
Abstract
Intense stress has the potential to produce traumatic memories that are core features of chronic mental disorders. However, encountering even intense stress most often does not have a persisting negative impact on health. Stress outcomes appear to involve complex interactions of sleep, learning, stressor qualities, and individual differences in resilience and vulnerability. This chapter will discuss how these interactions can impact the formation of traumatic memories, with a focus on factors that can differentially lead to normal and pathological stress outcomes. It will discuss the potential roles of different types of learning, stress resilience and vulnerability, and the neurobiological substrates that regulate interactions of stress, sleep, and the formation of traumatic memories. A case will be made that, given its role in learning and the processing of emotion, sleep may be key to fully understanding normal and pathological outcomes of intense stress.
The views expressed in this article do not represent those of the Department of Veterans Affairs or the US Government.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
7.1 Introduction
Real and perceived danger evoke a coordinated behavioral, neurobiological, and physiological stress response that provides resources for organisms to cope with an ongoing challenge and that enables physiological homeostasis to be restored when the threat is removed (Chrousos 1998; Chrousos et al. 2000). By definition, the stress response includes arousal (Chrousos 1998), and virtually all stressors are associated with significant alterations in sleep in the early post-stress period. Stressful events also provide the opportunity for learning and the formation of stress-related and fear memories that can impact the ability to respond to future challenges. Experimental evidence indicates that stress-related memories can themselves induce a stress response and can have much the same effects on behavior and sleep as the original stressor.
The stress response is normally adaptive and important for survival, and learning associated with successful coping can improve the ability to deal with subsequent stressors (Chrousos 1998). However, traumatic stress can overwhelm an individual’s ability to cope, resulting in a stress response that is compromised or fails. In such instances, trauma-related memories have the potential to contribute to psychopathology and also are often a defining symptom.
Sleep is emerging as a significant biomarker of differential stress responses and as a putative mediator of stress outcomes. Indeed, sleep disturbances both before (Bryant et al. 2010; Gehrman et al. 2013) and after (Koren et al. 2002; Lavie 2001) a traumatic event may be predictive of emotional and physical disorders. Additionally, sleep has long been implicated in learning and memory consolidation, and recent studies have suggested that sleep, in particular rapid eye movement sleep (REM), is important for processing emotion (Goldstein and Walker 2014) and adapting to stress (Mellman et al. 2002, 2007; Sanford et al. 2010). REM can be increased or decreased in association with similar stress system activation and fear behavior (Sanford et al. 2010; Machida et al. 2013; Yang et al. 2011; Wellman et al. 2016, 2017), indicating complex relationships among sleep, stress, and learning that currently are poorly understood.
In this chapter, we will provide an overview of the relationships of stress, sleep, learning, and the formation of trauma-related memories, with the goal of delineating critical gaps in our knowledge of how traumatic stress can produce significant negative effects on emotional and physical health.
7.2 Stress Response
Stress is broadly defined as a nonspecific physiological response to a situation or event that is psychologically or physiologically demanding. In response to stressors, neurochemical mediators are released and act acutely to promote adaptive physiological and behavioral responses (McEwen 2007). These include activation of the hypothalamo-pituitary-adrenal (HPA) axis and the autonomic nervous system (sympathoadrenalmedullary (SAM) branch) to initiate and regulate behavioral and physiological responses and adaptations to challenge (Chrousos 1998, 2009; Chrousos et al. 2000; Nezi et al. 2000). Other processes work to prevent over-responses of the stress systems (Chrousos 1998). Problems can arise when the stress response is insufficient or the stress system is overwhelmed by an intense or prolonged challenge (Chrousos 1998). Indeed, stress is implicated in a number of neuropsychiatric diseases as well as a variety of physical health ailments and risks. Traumatic stress leads to the development of posttraumatic stress disorder (PTSD) in a substantial minority of individuals and can be associated with depression as well.
7.3 Effects of Stress on Sleep
Essentially all stressors that have been examined produce alterations in sleep (for reviews, see Pawlyk et al. 2008; Sanford et al. 2015). Animal experiments have repeatedly demonstrated that stressful experiences during wakefulness can significantly impact subsequent sleep. Sleep has been recorded after a range of stressors, including avoidable footshock, restraint, water maze, exposure to novel objects, open field, ether exposure, cage change, and social stress (reviewed in Pawlyk et al. 2008; Sanford and Tang 2009). This work has described the effects of a variety of stressors on sleep and demonstrated that changes in arousal and sleep vary with stressor type and intensity. Effects also depend on the duration of stress exposure, with significant differences in the effects of acute compared to repeated or chronic stress (reviewed in Sanford et al. 2015). Repeated and chronic stress can produce alterations in sleep related to disruptions in homeostatic and circadian drive in addition to effects specific to stress (Sanford et al. 2015). For this reason, we will concentrate our discussion on the effects of discrete, temporally limited stressors, which enable clearer identification and definition of the stressful experiences.
Exposure to an acute stressor typically produces a period of arousal followed by subsequent increases in REM and/or non-REM (NREM) that occur at various latencies after the stressor is removed. In some cases, the amount of post-stress sleep can be larger than the amount lost; for example, the increase in NREM can be larger after an encounter with an aggressive conspecific than after an equal period of sleep deprivation (Meerlo et al. 1997; Meerlo and Turek 2001). The increase in sleep also can be significantly delayed even when the opportunity to sleep is available. While this delay can occur with a variety of stressors, it is perhaps best exemplified by restraint stress, in which case the application of restraint in the light period can produce an enhancement of REM in the following dark period (Meerlo et al. 2001; Rampin et al. 1991).
A pattern of initial arousal followed by recovery sleep is observed with minor and mild stressors (e.g., handling, novelty, open field) and stressors that animals may repeatedly experience (e.g., cage change); this suggests that this response pattern is not indicative of developing pathology. Relatively intense controllable stress (modeled by escapable shock (ES)) can also be followed by a significant increase in sleep, particularly an increase in REM, which can occur soon after the stressor is removed. We (LDS and LLW) have suggested that the increases in sleep after many stressors may reflect restoration of homeostasis as the stress response follows its normal course (reviewed in Sanford and Tang 2009). The fact that sleep amount after stress can be greater than that lost is consistent with a significant role of sleep in the stress response. It has been suggested that REM plays a role in “decoupling” memory from its emotional charge (Baran et al. 2012; van der Helm et al. 2011; Walker and van der Helm 2009) and that intact REM may aid in the processing of the memory for trauma (Mellman et al. 2002, 2007). Based on work in animals, we (Sanford et al. 2010; Tang et al. 2005) and others (Suchecki et al. 2012) also have suggested that REM may have an adaptive function in recovery from stress. Some stressors (e.g., social stress (Meerlo et al. 1997; Meerlo and Turek 2001)) seem to preferentially promote NREM, suggesting that it as well may be important for recovering from certain types of stress. This would be consistent with the finding that both visually scored delta sleep and EEG delta amplitude may be reduced in individuals with PTSD (reviewed in Neylan et al. 2006).
7.4 Effects of Stress on Learning and Memory
Although stress can have a significant negative impact on health (Shalev 2000; Van den Berg et al. 1998; Van Dijken et al. 1992; Adamac and Shallow 1993; Pynoos et al. 1996), most stressors do not produce persisting or pathological changes. Even the extreme stress associated with traumatic life events gives rise to PTSD in only a minority of individuals (Yehuda and LeDoux 2007; Cohen et al. 2003; Kerns et al. 2004); most adequately cope with such experiences with only transitory detrimental effects. The difference between successful and unsuccessful coping with stress, including whether stress has transitory or lasting effects, can vary with characteristics of the stressful event including its controllability (Bolstad and Zinbarg 1997; Foa et al. 1992), predictability (Adell et al. 1988; Abbott et al. 1984), duration, and intensity (Buydens-Branchey et al. 1990; Natelson 2004). An individual’s relative resilience and vulnerability are also of great importance (Yehuda et al. 2006). How these factors alter the potential pathological impact of stress is poorly understood, but it likely involves their impact on trauma-related learning and memory.
Stressful events can engage associative (operant (instrumental) and classical conditioning) and nonassociative (sensitization and habituation) learning processes; these different types of learning can occur concurrently, with tremendous importance for mediating stress outcome. Effective methods of avoiding long-term consequences of stress involve learning, with the formation of successful coping strategies. From an evolutionary perspective, this relationship between stress and memory is important as survival success depends on both the ability to respond to a current threat and the ability to use knowledge gained from prior experiences to meet future similar challenges (Salehi et al. 2010). An experimental example is found in studies of stressor controllability, which have demonstrated that controllable and uncontrollable stress of the same magnitude can have significantly different impacts on behavioral and physiological outcomes (Bolstad and Zinbarg 1997; Foa et al. 1992). Uncontrollable stress has been linked to negative outcomes, including deficits in learning and in motivational and emotional functioning, and it can induce significant alterations in a variety of neurochemical systems. By comparison, controllable stress has been associated with neutral or positive outcomes. The ability, or inability, to learn and remember a successful coping response likely determines the different outcomes of controllable and uncontrollable stress.
Controllable stress, which can enable stress-related operant learning, can guide successful responses to future challenges. Conversely, uncontrollable stress has the potential to impede useful operant learning and can negatively impact the ability to respond to subsequent stress. Perhaps the best known paradigm for distinguishing the outcomes of exposure to controllable and uncontrollable stress is learned helplessness (Anisman and Merali 2009; Overmier and Seligman 1967; Seligman and Beagley 1975; Seligman and Maier 1967; Seligman et al. 1975). In one variant of this paradigm, experimentally yoked animals receive equal amounts of footshock, but one member of the yoked pair can terminate the footshock simply by moving to the safe side of the shock chamber (controllable stress), while the other member cannot act to influence the shock presentation (uncontrollable stress). Rodents that receive inescapable shock (IS) can show deficits in the ability to learn a subsequent escape response, whereas those that are able to escape from shock can show attenuated responses to subsequent uncontrollable shock presentations (reviewed in Anisman and Merali 2009). Interestingly, uncovering learning deficits in rodents that have experienced uncontrollable stress may require implementing a test with a more difficult escape contingency or one that requires a longer active response than that used in the original uncontrollable stress paradigm (Anisman and Merali 2009).
Stressful events may also engage classical conditioning processes. The most studied is fear conditioning, a widely used experimental model of learned fear and anxiety, with relevance to the development of mental disorders in humans, PTSD in particular (Foa et al. 1992; Davis 1990; Grillon et al. 1996; Shalev et al. 1992; Charney and Deutch 1996; Pitman et al. 2001). In experimental fear conditioning, an explicit neutral stimulus (generally a light or auditory stimulus) or situational context comes to induce fear through an association with an aversive stimulus (usually footshock) (Davis 1990; Davis and Whalen 2001). After the association is made, subsequent exposure to the newly fear-conditioned cue or context can elicit behavioral and physiologic responses similar to those elicited by the unconditioned aversive stimulus. These include behavioral freezing (absence of all movement except respiration) (e.g., Blanchard and Blanchard 1969; Paylor et al. 1994), a stress response (Yang et al. 2011; Wellman et al. 2016, 2017), a variety of physiological signals (e.g., increased heart rate and respiration) indicative of fear (reviewed in Davis 1992a), and a fear-potentiated increase in startle amplitude (Davis 1990, 1992b).
After training, fear-conditioned memories provide a pathway by which reminders of traumatic events can produce maladaptive changes in behavior. However, conditioned fear also can underlie adaptive behavior that typically is extinguished when the fear-inducing stimulus is no longer presented (Pitman et al. 2001; Kishimoto et al. 2000). Indeed, it is the failure of fear extinction that has been linked to persisting symptoms of PTSD (Myers and Davis 2007), though the qualities of a stressful event that mediate adaptive and maladaptive fear responses are poorly understood. Contextual reminders of ES and IS, models of controllable and uncontrollable stress, respectively, can produce differential activation in brain stress regulatory regions (Liu et al. 2009a) and different sleep responses (Sanford et al. 2010; Yang et al. 2011, discussed below), whereas behavioral fear and stress indices can be virtually identical (Sanford et al. 2010; Machida et al. 2013; Yang et al. 2011). This suggests that successfully learning an escape response can differentially mediate several stress outcomes even though standard indices of fear and stress do not vary. Such learning, and the impact it would have on immediate stress outcomes and its potential for increasing the probability of successful responses to subsequent stressors, would provide a clear advantage to the animal.
Different from conditioning, sensitization is defined as enhanced responding upon repeated presentations of a stimulus, and habituation is defined as reduced responding with repeated stimulus presentations (Rahn et al. 2013). Exposure to extreme stressors has the potential to sensitize an organism’s response to future stressors (Smid et al. 2012). Sensitization of various stress-related systems (e.g., HPA axis (Yehuda 2001), noradrenergic (NA) system (Southwick et al. 1994) and arousal/hyperarousal systems more generally (Rahn et al. 2013)), has been implicated in the development of PTSD (Shalev 2000). By comparison, habituation is important for reducing responses to repeated stressors of a similar type, thereby, for example, limiting the harmful effects of sustained glucocorticoid release (Herman 2013). Variants of exposure therapy are thought to rely partly on habituation (Sripada and Rauch 2015; Jaycox et al. 1998), as well as extinction learning (Hofmann 2007), to reduce fear responses.
It has been suggested that the pathophysiology of PTSD depends on complex interactions between associative and nonassociative learning arising from traumatic events (Siegmund and Wotjak 2006). Siegmund and Wotjak (2006) proposed a “Dual-Branch Hypothesis of PTSD” that incorporates fear conditioning and sensitization as mediators of associative and nonassociative fear memory, respectively. In this model, classical conditioning mediates associative fear memory and related processes including fear generalization, whereas sensitization mediates fear incubation. There is also evidence that sensitization can impact conditioned fear in some instances and that sensitization and habituation may play roles in mediating the magnitude of fear-induced freezing (Kamprath and Wotjak 2004).
In addition to the potential interactions or parallel roles of classical conditioned fear and sensitization in the formation of traumatic memories, our work with ES and IS demonstrates that differences in operant learning can differentially mediate several outcomes of acute stress even though standard measures of stress and fear may be the same across conditions (Sanford et al. 2010; Machida et al. 2013; Yang et al. 2011). For example, even in the IS condition, the animal typically attempts to escape or engage in other behaviors to try to lessen stressor intensity. Failed escape attempts and inadequate behavioral responses may contribute to the formation and intensity of traumatic memories, whereas successful escape may ameliorate some effects of the stressful experience. In summary, the formation of traumatic memories potentially involves the collective effects of failed coping (operant) responses, intense fear conditioning, and stress-enhanced sensitization. These collective effects cross learning modalities and may make traumatic fear memories highly resistant to extinction. Unfortunately, the potential compound effects of, or interactions between, associative and nonassociative learning associated with stress have received little attention. Similarly, the role that sleep may play in processing traumatic memories and other posttraumatic behaviors has barely been explored.
7.5 Stress, Sleep, and Learning
There is considerable experimental support for a role for sleep in the consolidation of certain types of memories (see Born and Wilhelm 2012; Graves et al. 2003; Poe et al. 2010; Rolls et al. 2011; Stickgold 2005; Stickgold and Walker 2007; van Dongen et al. 2012; Walker 2009; for opposing opinions, see Siegel 2001, 2011; Vertes 2004a; Vertes and Siegel 2005). Most experiments have focused on the role that sleep may play in mediating performance on memory-related tasks in subsequent wakefulness. Less studied, and perhaps even less acknowledged, are the significant effects that emotional memories can have on sleep. However, answering complementary questions regarding the potential interactions between waking experiences and subsequent sleep is critical for fully understanding both the early effects of trauma and the development and persisting effects of traumatic memories.
7.5.1 Relationship Between Associative Learning and Memory and Sleep
Numerous studies using a variety of behavioral paradigms have demonstrated that learning experiences may be followed by alterations in subsequent sleep. One classical line of work employed shock avoidance training in a shuttle box, in which animals are signaled of imminent shock presentation and can learn to jump to safety preemptively. Successful avoidance is typically followed by a significant increase in REM at various times post-training, so-called REM “windows” (Smith and Butler 1982; Smith et al. 1974, 1980; Smith and Lapp 1986). These increases in REM have been viewed as evidence of a role for REM in memory consolidation. Consistent with this interpretation is the finding that selective post-training REM deprivation can adversely affect subsequent performance (Smith and Butler 1982; Smith and Lapp 1986; Smith and Kelly 1988). More recent work has suggested that pontine waves (the pontine component of ponto-geniculo-occipital (PGO) waves, a neural signature of REM) may be the critical REM mechanism (Datta 2000; Mavanji and Datta 2003). Although shock avoidance generally has been viewed in the context of learning and memory, it is also a controllable stress paradigm that provides animals the opportunity to acquire a coping response to an aversive stimulus; an increase in REM follows successful acquisition of the avoidance response (Smith et al. 1980). Thus, shock avoidance is an excellent example of the impact of stress-related operant learning on sleep and of the potential role of sleep in mediating the formation and influence of stress-related memories.
Shock paradigms that model uncontrollable stress also can produce significant alterations in sleep. In an early study, Adrien et al. (1991) presented rats with 60 trials of IS at relatively high intensity (0.8 mA) and long duration (15 s) over the course of an hour. Compared to rats that experienced the shock chamber alone without receiving shock, rats trained with IS showed a greater REM latency and reduced REM amount during the 3 h after training. Subsequently, REM returned to the control amount, but no REM rebound was observed in recordings in the following dark or light periods. Light NREM amount was increased from baseline sleep and compared to the control group. This study demonstrates that strong uncontrollable stressful experiences can produce significant alterations in subsequent sleep. It also demonstrates a difference in sleep after avoidable shock, as well as many other stressors (discussed above), viz., lost REM was not recovered. Unfortunately, such studies typically do not examine the effects of stressful memories on sleep. Also, they usually focus on one type of learning, although as noted above, the response to intensely stressful experiences likely involves multiple types of associative and nonassociative learning.
One clear example of the effects of stress-related memory on sleep can be found in work using experimental fear conditioning paradigms. Fear conditioning models are important for examining the development and effects of traumatic memories as they can engage fear memory and induce fear and stress responses, and impact sleep, without requiring a full reexperiencing of the initiating stressful event. Indeed, various studies have used variations of cued and contextual fear conditioning to examine the effects of both fear conditioning and fear memories on sleep (e.g., Wellman et al. 2017; DaSilva et al. 2011; Laitman et al. 2014; Liu et al. 2002; Madan et al. 2008; Sanford et al. 2003a, b). However, general fear conditioning models, as currently conceived, are inadequate as they cannot fully explain the effects of stressful learning and memories on sleep, thereby indicating a significant gap in our understanding of how traumatic experiences can lead to persisting dysfunction in fear, stress, and arousal systems.
Although conditioned fear is thought to be important in the development of psychopathology, it is generally studied in animals using mild or limited shock presentations as the aversive stimulus. Such brief stressful experiences are not likely to produce the lasting changes necessary for the development of psychopathology in humans. Indeed, as indicated above, fear-conditioned responses typically extinguish when the fear-inducing situation is removed, and such extinction is thought to represent a form of successful adaptation to stress (Pitman et al. 2001; Kishimoto et al. 2000; Bouton 2004). On the other hand, DaSilva et al. (2011) have reported that fear conditioning in the stress-sensitive Wistar–Kyoto (WKY) rat strain can produce the REM fragmentation similar to that reported in PTSD, particularly early in the course of the evolving PTSD symptom complex (Mellman et al. 2014; Ross 2014). Laitman et al. (2014) have provided preliminary validation of this model with their observation that prazosin, arguably the most effective treatment for the nightmare disturbance in PTSD, enhanced REM continuity in fear-conditioned WKY rats.
Mild conditioning produces relatively small effects on sleep. Using a single shock training paradigm, Hellman and Abel (2007) found that, in fear-conditioned mice compared to non-shocked mice as well as mice that experienced a footshock unassociated with conditioning, NREM was increased by approximately 1 h over the 24 h after training. However, the amount of training that an animal receives is an important parameter of the response to footshock stress. There appears to be a graded response in post-stress sleep that varies with number of stimulus-shock pairings. For example, the initial presentation of fearful cues after 4 days of IS training produced an 85% and a 55% reduction in REM and NREM, respectively, in the first hour after presentation (Sanford et al. 2003a), while the presentation of fearful cues after a single day of training produced a 34% and a 19% reduction in REM and NREM, respectively, in that time window (Sanford et al. 2003c). In contrast, REM and NREM in mice trained with a single cue-shock pairing did not significantly differ from baseline levels after the presentation of a single cue (Sanford et al. 2003c). Thus, multiple trial training appears to be required to produce alterations in sleep in response to fear-conditioned stimuli (Sanford et al. 2003c).
7.5.2 Stress Mediators and Sleep
Factors that can impact stress outcomes, such as stressor controllability and individual differences in resilience and vulnerability, can influence post-stress sleep. For example, controllable stress that is associated with positive or neutral outcomes can be followed by a significant increase in REM, whereas uncontrollable stress can decrease REM (Sanford et al. 2010; Machida et al. 2013).
The REM increase after controllable stress could be viewed as support for the oft-made argument that REM is needed for successful operant learning (Smith and Butler 1982; Smith et al. 1974, 1980; Smith and Lapp 1986; Smith and Kelly 1988), and REM may be involved in differences in learning. We (LDS and LLW) have recently found that outbred Wistar rats can show different REM responses to uncontrollable footshock stress. Some rats show pronounced decreases in REM during the first 4 h post-training, whereas others show no change or even an increase in REM (Wellman et al. 2016, 2017). These different REM responses (which we have called vulnerable and resilient REM responses) are independent of freezing and of stress-induced hyperthermia (SIH), a stress index that parallels the time course of the corticosterone response to stress (Groenink et al. 1994; Veening et al. 2004; Vinckers et al. 2009). Thus, REM may be a marker of differences in the stress response that are not captured by standard behavioral and physiological measures of fear memory and stress (Wellman et al. 2016; 2017) or of operant learning.
7.6 Sleep as a Mediator of Memory and Stress Outcomes
The effects of experiences in waking on subsequent sleep have most often been examined in the context of the role sleep may play in forming associations and learning. Sleep deprivation after training can impair fear memory for a single shock training session (Graves et al. 2003; Hagewoud et al. 2010). A recent study in a rat model of circadian desynchrony found that fragmentation of NREM and REM without total sleep loss produced deficits in single-trial contextual fear conditioning, but not in cued fear conditioning or spatial learning (Lee et al. 2016). These and other studies (e.g., Cai et al. 2009; Fu et al. 2007) suggest that sleep may have a role in forming memories of transitory fearful events, which is consistent with the importance of sleep for adaptive learning.
There is evidence that REM promotes the consolidation of emotional memories (Genzel et al. 2015; Wagner et al. 2001). Menz et al. (2013) showed that, in healthy individuals, REM improved the recall of fear learned in a Pavlovian conditioning paradigm. Although these investigators emphasized the negative emotional consequences of REM-enhanced fear recall, Walker and van der Helm (2009) posited that REM following an aversive experience could reduce the negative emotional consequences of such fear recall. This is consistent with the suggestion of Bennion et al. (2015) that sleep-based facilitation of emotional memory processing involves a “restriction and refinement of the neural processes needed for successful [italices are the authors’] retrieval.” Similarly, Rasch and Born (2013) suggested that, in traumatized individuals, a failure of the normal attenuation by REM of the negative tone associated with fear memories could produce a nightmare disturbance.
Using an experimental laboratory trauma protocol in healthy young women, Kleim et al. (2016) found that sleep posttrauma protected against the occurrence of intrusive trauma memories. Interestingly, it was NREM, including NREM fast parietal spindles, that was correlated with reduced intrusion frequency; REM density (no. rapid eye movements/total REM time) also was negatively correlated with frequency of intrusions. In a clinical study of accident survivors, REM fragmentation in the aftermath of trauma predicted the development of PTSD (Mellman et al. 2002), suggesting that uninterrupted REM is necessary for the effective processing of an emotional experience and the prevention of posttraumatic memories and other PTSD symptoms. The effects of REM on memory consolidation may extend beyond emotional memories. Studying healthy young adults, Whitehurst et al. (2016) found evidence that autonomic nervous system activity during REM, specifically vagally mediated activity measured as high frequency heart rate variability, played an important role in associative memory consolidation.
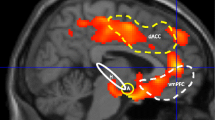
REM is marked by prominent electroencephalographic (EEG) activity in the theta band (4–12 Hz). Stujenske et al. (2014) have reviewed the evidence that theta band oscillations in the basolateral amygdala (BLA), medial prefrontal cortex (mPFC), and hippocampus promote communication among these brain regions in response to aversive stimuli. In a polysomnographic study of healthy young adults who had been exposed to an environmental trauma, Cowdin et al. (2014) found that high right prefrontal theta power in REM was associated with resiliency. They concluded that theta power in this brain region could be a biomarker of a capacity for adaptive emotional memory processing. This interpretation is consistent with the earlier report by Nishida et al. (2009) that, in healthy young adults studied with a nap paradigm, high right prefrontal theta power in REM predicted improved consolidation of emotional, but not neutral, memories. There also is a report that memory for fear conditioning in rats trained in a relatively mild cued fear paradigm is associated with theta coherence in the amygdala, mPFC, and hippocampus during REM (Popa et al. 2010).
Stress and the stress hormone cortisol also are reported to influence memory consolidation (Bennion et al. 2015). There is evidence, although no consensus, that both enhance the consolidation of emotional memories (reviewed in Bennion et al. 2015). Cortisol level may be an important parameter (Lupien and Lepage 2001), with large elevations, that might occur during severe stress, impairing emotional learning. On the other hand, Zohar et al. (2011) found that administering a single dose of hydrocortisone to human subjects with symptoms of acute traumatic stress diminished the development of posttraumatic stress symptoms, i.e., possibly enhanced effective emotional learning. Similarly, van Marle et al. (2013) demonstrated a prioritization of emotional over neutral memory consolidation in healthy young males administered hydrocortisone; of particular interest, there was an attenuation of amygdalar activation during memory retrieval in these subjects, again suggesting that cortisol could enhance adaptive emotional learning.
An interaction between cortisol and sleep processes may be necessary for the consolidation of negative emotional memories (Bennion et al. 2015). Consistent with this hypothesis, Bennion et al. (2015) reported that cortisol was essential for sleep-facilitated memory consolidation in a population of healthy young adults. This dependence was especially strong when an aversive item was well attended at the time of encoding. Wagner and Born (2008) have suggested that the normal rise in cortisol late in the sleep period, when REM predominates, may “counteract an overshooting consolidation of emotional memories;” in hypocortisolemic conditions, such as PTSD has been construed, removing this cortisol “brake” may release intrusive distressing memories.
The above discussion illustrates the often conflicting results and hypotheses regarding the potential role of sleep and stress in mediating the formation of traumatic memories that may have other pathological consequences. Indeed, stress and fear learning systems may mediate adaptive responses that enable individuals to cope successfully with ongoing challenges as well as maladaptive responses that have the potential to contribute to pathology linked to traumatic memories. It is essential in both basic and clinical studies to distinguish adaptive from maladaptive stress responses and to determine the factors underlying each.
7.7 Neurobiological Distinctions Between Adaptive vs. Maladaptive Traumatic Memories
Memory formation depends on synaptic plasticity (Josselyn et al. 2015). The widely accepted synaptic plasticity and memory hypothesis states that “Activity-dependent synaptic plasticity is induced at appropriate synapses during memory formation, and is both necessary and sufficient for the information storage underlying the type of memory mediated by the brain area in which that plasticity is observed” (Martin et al. 2000). Formation of a memory trace, engram, involves changing synaptic weights within a neuronal circuit. Encoding of information during memory formation requires conversion of labile changes to more enduring changes in synaptic weight called synaptic/cellular consolidation. Consolidation of memory, in particular explicit associative memory, may also involve the distribution of the engram to different brain areas, often termed system consolidation. Memory also includes recall and reconsolidation of memory engrams. Thus, there are multiple opportunities for stress and sleep to have adaptive or maladaptive influences on memory processes.
7.7.1 Stress and Synaptic Plasticity
To limit our discussion, we will focus on how stress may influence the best characterized form of synaptic plasticity, NMDA receptor-dependent long-term potentiation (LTP) and long-term depression (LTD) of CA1 hippocampal neurons. In CA1, acute stress-evoked corticosteroids and catecholamines enhance LTP via mechanisms that include insertion of AMPA receptors into the postsynaptic site (O’Dell et al. 2015; Takeuchi et al. 2016; Groc et al. 2008). However, chronic stress, with elevated corticosteroid levels, may produce opposite effects, reducing AMPA and NMDA receptor levels (Alfarez et al. 2006); this leads to a decrease in dendritic spine size or density, a correlate of LTD. In contrast to the hippocampus, neurons in BLA, but not the central nucleus of the amygdala (CNA), undergo hypertrophy after chronic stress, exhibiting a region-specific response (Qin et al. 2011; Vyas et al. 2006). As discussed later, these are critical brain regions for linking fear memory and sleep.
In addition to the extensively studied corticosteroid- and catecholamine-mediated mechanisms and their signaling pathways, the integrated stress response that encompasses cellular responses to possibly all forms of stress is gaining increasing attention. It is an evolutionary conserved cellular mechanism for coping with stress, and it couples stressful components of a learning situation to synaptic plasticity. Interference with the integrated stress response pathway alters both synaptic plasticity and learning outcomes (Sekine et al. 2015; Jian et al. 2014). The molecular differences between adaptive and maladaptive responses to stress remain undetermined. However, it is intriguing that the integrated stress response involves a global reduction in translation initiation, including synaptic plasticity genes, but preferential translation initiation of stress remediation transcripts (Young and Wek 2016). It is tempting to speculate that adaptive responses to stress involve faster stress remediation and less suppression of plasticity genes.
7.7.2 Sleep and Synaptic Plasticity
An increase in synaptic strength during learning and memory processes correlates with increased synapse numbers and synaptic size. However, physical constraints, such as the limited space within the adult cranium, and synaptic saturation, when efficacy of synaptic transmission is maximized, pose limits to increased synapse density and size as a lifelong learning mechanism. To counteract saturation of synaptic strength/size, there are synaptic homeostatic mechanisms. One of the possible benefits of sleep could be to restore synaptic homeostasis (Tononi and Cirelli 2014). During sleep, synaptic downscaling results in a net decrease in synaptic strength while maintaining relative differences between strongly vs. weakly potentiated synapses (de Vivo et al. 2017) in the neocortex, thus maintaining memory engrams.
Sleep may play a complementary plasticity inducing role in extrahippocampal cortical regions during hippocampus-dependent learning. Rat CA1 pyramidal neurons that are sequentially activated during spatial behavior repeat the same order of firing during subsequent NREM (Born and Wilhelm 2012). Such replay of this information in each NREM cycle, with information transfer from the hippocampus to extrahippocampal regions, induces plasticity in these regions, leading to extraction of semantic content of episodic memories. REM may also have a role in this process. Neuronal circuits reactivated in NREM are primed for LTP in the ensuing REM period, supporting plasticity-related gene expression (Ribeiro et al. 1999; Ulloor and Datta 2005). Thus, sleep interacts with plasticity processes that relate to memory formation in multiple ways. Sleep may contribute to the lifelong capacity for learning by facilitating homeostatic processes and system consolidation of memories. At the same time, learning experiences affect sleep parameters, probably using overlapping cellular mechanisms, potentially in ways that differentiate adaptive and maladaptive memories.
7.8 Neurocircuitry Linking Sleep, Stress, and Memory
Major components of the neurocircuitry linking stress, fear learning, and REM are known, and the roles of several brain regions have been established. These include the amygdala, hippocampus, and mPFC, which are important structures in fear memory circuitry and linked to brain stem regions involved in the response to stress and the regulation of REM.
The amygdala is critical for emotion. It is central in all models of fear conditioning (Davis 1992b; LeDoux 1992; LeDoux and Muller 1997) and important for the expression and extinction of fear (Buchel and Dolan 2000; LaBar et al. 1998; Linnman et al. 2011; Phelps et al. 2004; Sehlmeyer et al. 2009). It has been linked to mood and anxiety disorders as well as PTSD. Neuronal activity of the amygdala varies across the sleep-wake states, with increased activity during REM and less activity during NREM in comparison to wakefulness (Nofzinger et al. 2002; Braun et al. 1997), findings consistent with its significant role in modulating arousal and sleep in both normal and stressful conditions (Bernard et al. 1993; Krettek and Price 1978; Petrov et al. 1994; Peyron et al. 1998; Price et al. 1987; Sanford et al. 1995, 2002; Smith and Miskiman 1975). Our (LDS and LLW) recent work has demonstrated a role for the amygdala in regulating the impact of fearful memories on sleep, i.e., whether REM is increased or decreased following stress and the activation of stress-related fear memories (Wellman et al. 2016, 2017).
Hippocampal activity has been observed during fear behavior in imaging studies, and it has been linked to the contextual features associated with fear conditioning and expression (Sehlmeyer et al. 2009; Kalisch et al. 2006; Knight et al. 2009; Milad et al. 2007). It is also implicated in extinction training and recall (Milad et al. 2007, 2009), and there is evidence that sleep is important for consolidating hippocampal-dependent memory (Lee et al. 2016; Cai et al. 2009; Fu et al. 2007; Ruskin et al. 2004; Ruskin and Lahoste 2008). In humans, activity in the mPFC has been reported to be increased during extinction of fear behavior and recall of extinction (Phelps et al. 2004) and to be positively correlated with post-fear REM (Spoormaker et al. 2014). However, these paradigms used relatively brief training protocols that employed shock applied to the hand or wrist that was titrated based on the subject’s perception to be “uncomfortable,” rather than “painful.” Thus, their relevance for the role of mPFC activity in mediating the relationship between sleep and traumatic memories is not fully clear.
The circuitry regulating stress and fear (Chrousos 2009; Sanford et al. 2015; Davis and Whalen 2001; LeDoux 1993, 2000; Pare et al. 2004) has significant overlap with, and impact on, brain stem regions that regulate arousal and sleep (e.g., REM regulatory and generator regions in the pons: locus coeruleus (LC), dorsal raphe nucleus (DRN), nucleus subcoeruleus (SubC), laterodorsal and pedunculopontine tegmental nuclei (LDT/PPT), and the reticularis pontis oralis (RPO) (Morrison et al. 2000; Xi et al. 2011; Zhang et al. 2012)). These same brain stem regions also have significant roles in mediating the stress response. Noradrenergic (NA) and serotonergic (5-HT) neurons in the stress-responsive LC and DRN, respectively, are virtually silent during REM, and their activation has long been thought to inhibit its generation (reviewed in Steriade and McCarley 1990). Essentially all current conceptions of REM generation and control involve models of the interactions and mutual inhibition among these pontine and mesopontine regions and neurochemical systems (e.g., McCarley 2004; McCarley and Hobson 1975; Datta 2010; Lu et al. 2006; Fuller et al. 2007; Dunmyre et al. 2014; Scammell et al. 2017). These models include inhibitory effects of REM-off neurons (LC and DRN), excitatory effects of REM-on neurons (LDT and PPT), and generation of REM phenomena (RPO) (McCarley 2007). Some models of REM regulation also consider descending inputs to pontine/mesopontine areas from more rostral regions, primarily cell groups located in the hypothalamus (Dunmyre et al. 2014; Ramaligam et al. 2013). There is also more limited evidence of roles for the amygdala and mPFC (Ramaligam et al. 2013; Saper et al. 2010), which may have particular importance in mediating the effects of stress and fear memory on REM.
7.8.1 Amygdalar Modulation of Sleep, Fear, and Stress
The amygdala projects (via efferents from CNA or the lateral division of the bed nucleus of the stria terminalis (BNST), both considered extended amygdala) to areas that control sleep and arousal including the thalamus, hypothalamus, and brain stem regions. Functional studies in animal models have shown that the amygdala has a strong influence on REM and that it regulates the effects of stress, fear, and fear memory on REM.
The CNA appears to directly regulate REM and to mediate the effects of stress and fear memory on REM. For example, functional inactivation of the CNA with microinjections of the GABAA agonist muscimol produced a selective decrease in REM, whereas blocking GABAergic inhibition with the GABAA antagonist bicuculline increased REM (Sanford et al. 2002). That stress-induced inactivation of CNA is involved in stress-induced reduction in REM is also suggested by the absence of Fos expression (a marker of neural activation (Chowdhury et al. 2000; Cullinan et al. 1995; Watanabe et al. 1994; Zangenehpour and Chaudhuri 2002)) in CNA with conditioned fear (Liu et al. 2003) and by the finding that bicuculline microinjected into CNA attenuated the IS-induced reduction in REM (Liu et al. 2009b). Blocking CNA inhibition also reduced activation, as indicated by c-Fos activity, in the LC, consistent with the role of this nucleus in inhibiting REM. In contrast, microinjection of the GABAA agonist muscimol into the CNA did not alter the REM reduction typically observed following IS nor did it change c-Fos activity in the LC following fear conditioning (Liu et al. 2009b), suggesting that inactivation of CNA regulates the reduction in REM after IS.
The BLA appears critical for determining how fear memories affect sleep, likely via descending projections from the CNA and/or BNST. Inactivation of the BLA with microinjections of muscimol prior to IS blocked the post-training reduction in REM and attenuated freezing and the subsequent reduction in REM when animals were reexposed to the stressful environment (Wellman et al. 2014). However, microinjections of muscimol immediately following IS or prior to context reexposure blocked the reduction in REM without altering fear behavior or the stress response. BLA also appears to be a critical area for regulating the differences between vulnerable and resilient animals with respect to stress and fear-induced alterations in REM. This is indicated by the fact that inactivation of BLA prior to reexposure to the shock context attenuated the REM reduction in vulnerable rats, but did not significantly alter REM in resilient rats (Wellman et al. 2017).
Corticotropin-releasing hormone (CRH), a major mediator of the brain’s response to stress, acts in the amygdala to regulate the alterations in sleep observed following stress. Microinjection of the CRH antagonist antalarmin into the CNA of rats prior to context reexposure blocked the fear-induced reduction in REM and attenuated c-Fos expression in regions important for REM generation and regulation (LC and DRN) and the stress response (paraventricular nucleus of the hypothalamus) (Liu et al. 2011). When microinjected into the BLA prior to IS, antalarmin blocked the IS-induced reduction in REM without blocking fear memory as indicated by contextual freezing (Wellman et al. 2013). In vivo microdialysis in BLA of rats showed an increase in the CRH level following fear conditioning, and this corresponded to freezing behavior during later cue presentations (Mountney et al. 2011). The effects of stress also involve descending CRH projections. Both the CNA (Van Bockstaele et al. 1998) and the BNST (Van Bockstaele et al. 1999) contain CRH efferents to the LC that increase the firing rate of LC neurons and subsequently the release of NA on upstream targets (including the PFC (Curtis et al. 1997) and hippocampus (Page and Abercrombie 1997; Palamarchouk et al. 2002)).
7.8.2 The Role of Medial Prefrontal Cortex in Modulating Sleep, Fear, and Stress
The mPFC has an established role in the perception of stressor control and the mediation of stressor consequences. For example, past exposure to a controllable stressor is generally protective during future stressful experiences, an effect believed to be mediated by the mPFC. Blocking activation of the ventral mPFC (mPFCv) with muscimol produced failure in escape learning in rats presented with ES, and greater fear conditioning in rats provided an opportunity to escape shock in a shuttle box. By comparison, mPFCv activation with the GABA antagonist picrotoxin prior to IS promoted escape learning, indicating that mPFCv activity could increase self-protective behavior even when the stressor is not controllable (Maier et al. 2006).
The protective effect of mPFC activation during controllable stress is thought to involve inhibition of the DRN (Amat et al. 2005). Electrical stimulation of projection neurons in mPFC led to inhibition of DRN 5-HT neurons, at least partially through GABA interneurons (Celada et al. 2001). IS compared to ES produced significantly greater activation of DRN 5-HT cells, as measured by c-Fos activity (Amat et al. 2005; Grahn et al. 1999). This increased activity subsequently induced a greater efflux of 5-HT into the mPFCv inhibiting local pyramidal neurons (Puig et al. 2005) and further contributing to differential activation of the mPFCv by stressors of differing controllability (Amat et al. 2005).
The mPFC has also been found to influence REM. A recent study found that lesions of the mPFCv in rats decreased REM, increased sleep fragmentation, and shortened REM latency (Chang et al. 2014). A possible role of the mPFCv in modulating fear-conditioned sleep is suggested by the report of a positive correlation between mPFCv activity during conditioning and subsequent REM (Spoormaker et al. 2014). This influence on REM likely involves connections between the mPFCv and REM-off brain stem regions (Chang et al. 2014), although projections to BLA and CNA, or to GABAergic neurons in the intercalated nuclei that have inhibitory control over CNA output, could also play a role (Vertes 2004b).
Interestingly, projections from the LC and DRN to the mPFC promote wakefulness (Cid-Pellitero and Garzon 2011a, b), and CRH plays a role in mediating these effects. Injections of CRH into the LC increased NA release in the mPFC, an action blocked by co-administration of a CRH antagonist (Smagin et al. 1995). The release of 5-HT in the mPFC induced by stimulation of CNA was blocked by administration of a CRH2 antagonist into the DRN (Forster et al. 2008).
7.9 Neurocircuitry Underlying the Complex Relationship Between Fear Memory and Sleep
Despite clear linkages between the circuitries that regulate conditioned fear and REM, current models based on studies of immediate fear responses (i.e., freezing and autonomic responses) do not sufficiently explain the relationship between fear memory and sleep or the dissociation that can occur between fear behaviors in wakefulness and fear-induced alterations in sleep. There is a clear discrepancy regarding the role of CNA in regulating fear behavior in wakefulness and fear-induced alterations in REM, which can either be increased or decreased after fearful events. In current fear models, activation of CNA induces the generation of fear behavior and related physiological responses via descending brain stem projections (Duvarci et al. 2011). However, inhibition of CNA suppresses REM, and its activation (e.g., with electrical stimulation (Smith and Miskiman 1975)) can promote REM in some situations. Another discrepancy is found in the fact that inactivating BLA prior to recall of contextual fear can block fear-induced reductions in REM without altering fear behavior or the stress response (Wellman et al. 2017). Thus, significant work is needed to delineate the neural circuits and substrates that link stress, sleep, and fear memory.
7.10 Conclusions
Traumatic stress has the potential to produce chronic mental disorders, including PTSD, and to increase susceptibility to physical diseases. However, even intense stress is often encountered with no more than a transitory negative impact. Interactions between stressor parameters, sleep, and learning are likely important determinants of differential stress outcomes and whether or not PTSD develops. Stressful memories can increase or decrease REM in much the same way that the original stressor does, suggesting that this sleep state has a unique relationship with the type of stressful memories that are formed. Whether it plays an active role in the adaptive processing of stressful experiences, or rather is an epiphenomenon, needs to be determined.
References
Abbott BB, Schoen LS, Badia P (1984) Predictable and unpredictable shock: behavioral measures of aversion and physiological measures of stress. Psychol Bull 96:45–71
Adamac R, Shallow T (1993) Lasting effects on rodent anxiety of a single exposure to a cat. Physiol Behav 54:101–109
Adell A, Trullas R, Gelpi E (1988) Time course of changes in serotonin and noradrenaline in rat brain after predictable or unpredictable shock. Brain Res 459:54–59
Adrien J, Dugovic C, Martin P (1991) Sleep-wakefulness patterns in the helpless rat. Physiol Behav 49:257–262
Alfarez DN, Wiegert O, Krugers HJ (2006) Stress, corticosteroid hormones and hippocampal synaptic function. CNS Neurol Disord Drug Targets 5:521–529
Amat J, Baratta MV, Paul E, Bland ST, Watkins LR, Maier SF (2005) Medial prefrontal cortex determines how stressor controllability affects behavior and dorsal raphe nucleus. Nat Neurosci 8:365–371
Anisman H, Merali Z (2009) Learned helplessness induced in mice. In: Gould TD (ed) Mood and anxiety related phenotypes in mice. Humana Press, New York, pp 177–196
Baran B, Pace-Schott EF, Ericson C, Spencer RM (2012) Processing of emotional reactivity and emotional memory over sleep. J Neurosci 32:1035–1042
Bennion KA, Mickley Steinmetz KR, Kensinger EA, Payne JD (2015) Sleep and cortisol interact to support memory consolidation. Cereb Cortex 25:646–657
Bernard JF, Alden M, Besson JM (1993) The organization of the efferent projections from the pontine parabrachial area to the amygdaloid complex: a Phaseolus vulgaris leucoagglutinin (PHA-L) study in the rat. J Comp Neurol 329:201–229
Blanchard RJ, Blanchard DC (1969) Crouching as an index of fear. J Comp Physiol Psychol 67:370–375
Bolstad BR, Zinbarg RE (1997) Sexual victimization, generalized perception of control, and posttraumatic stress disorder symptom severity. J Anxiety Disord 11:523–540
Born J, Wilhelm I (2012) System consolidation of memory during sleep. Psychol Res 76:192–203
Bouton ME (2004) Context and behavioral processes in extinction. Learn Mem 11:485–494
Braun AR, Balkin TJ, Wesenten NJ, Carson RE, Varga M, Baldwin P, Selbie S, Belenky G, Herscovitch P (1997) Regional cerebral blood flow throughout the sleep-wake cycle. An H2(15)O PET study. Brain 120(Pt 7):1173–1197
Bryant RA, Creamer M, O’Donnell M, Silove D, McFarlane AC (2010) Sleep disturbance immediately prior to trauma predicts subsequent psychiatric disorder. Sleep 33:69–74
Buchel C, Dolan RJ (2000) Classical fear conditioning in functional neuroimaging. Curr Opin Neurobiol 10:219–223
Buydens-Branchey L, Noumair D, Branchey M (1990) Duration and intensity of combat exposure and posttraumatic stress disorder in Vietnam veterans. J Nerv Ment Dis 178:582–587
Cai DJ, Shuman T, Gorman MR, Sage JR, Anagnostaras SG (2009) Sleep selectively enhances hippocampus-dependent memory in mice. Behav Neurosci 123:713–719
Celada P, Puig MV, Casanovas JM, Guillazo G, Artigas F (2001) Control of dorsal raphe serotonergic neurons by the medial prefrontal cortex: involvement of serotonin-1A, GABA(A), and glutamate receptors. J Neurosci 21:9917–9929
Chang CH, Chen MC, Qiu MH, Lu J (2014) Ventromedial prefrontal cortex regulates depressive-like behavior and rapid eye movement sleep in the rat. Neuropharmacology 86:125–132
Charney D, Deutch A (1996) A functional neuroanatomy of anxiety and fear: implications for the pathophysiology and treatment of anxiety disorders. Crit Rev Neurobiol 10:419–446
Chowdhury GM, Fujioka T, Nakamura S (2000) Induction and adaptation of Fos expression in the rat brain by two types of acute restraint stress. Brain Res Bull 52:171–182
Chrousos GP (1998) Stressors, stress, and neuroendocrine integration of the adaptive response. Ann N Y Acad Sci 851:311–335
Chrousos GP (2009) Stress and disorders of the stress system. Nat Rev Endocrinol 5:374–381
Chrousos G, Vgontzas AN, Kritikou I (2000) HPA axis and sleep. In: De Groot LJ, Beck-Peccoz P, Chrousos G, Dungan K, Grossman A, Hershman JM, Koch C, McLachlan R, New M, Rebar R, Singer F, Vinik A, Weickert MO (eds) Endotext. South Dartmouth. http://www.ncbi.nlm.nih.gov/pubmed/25905298
Cohen H, Zohar J, Matar M (2003) The relevance of differential response to trauma in an animal model of posttraumatic stress disorder. Biol Psychiatry 53:463–473
Cowdin N, Kobayashi I, Mellman TA (2014) Theta frequency activity during rapid eye movement (REM) sleep is greater in people with resilience versus PTSD. Exp Brain Res 232:1479–1485
Cullinan WE, Herman JP, Battaglia DF, Akil H, Watson SJ (1995) Pattern and time course of immediate early gene expression in rat brain following acute stress. Neuroscience 64:477–505
Curtis AL, Lechner SM, Pavcovich LA, Valentino RJ (1997) Activation of the locus coeruleus noradrenergic system by intracoerulear microinfusion of corticotropin-releasing factor: effects on discharge rate, cortical norepinephrine levels and cortical electroencephalographic activity. J Pharmacol Exp Ther 281:163–172
DaSilva JK, Lei Y, Madan V, Mann GL, Ross RJ, Tejani-Butt S, Morrison AR (2011) Fear conditioning fragments REM sleep in stress-sensitive Wistar-Kyoto, but not Wistar, rats. Prog Neuropsychopharmacol Biol Psychiatry 35:67–73
Datta S (2000) Avoidance task training potentiates phasic pontine-wave density in the rat: a mechanism for sleep-dependent plasticity. J Neurosci 20:8607–8613
Datta S (2010) Cellular and chemical neuroscience of mammalian sleep. Sleep Med 11:431–440
Davis M (1990) Animal models of anxiety based on classical conditioning: the conditioned emotional response (CER) and the fear-potentiated startle effect. Pharmacol Ther 47:147–165
Davis M (1992a) The role of the amygdala in conditioned fear. In: Aggleton J (ed) The amygdala: neurobiological aspects of emotion, memory, and mental dysfunction. Wiley-Liss, New York, pp 255–305
Davis M (1992b) The role of the amygdala in fear and anxiety. Annu Rev Neurosci 15:353–375
Davis M, Whalen PJ (2001) The amygdala: vigilance and emotion. Mol Psychiatry 6:13–34
de Vivo L, Bellesi M, Marshall W, Bushong EA, Ellisman MH, Tononi G, Cirelli C (2017) Ultrastructural evidence for synaptic scaling across the wake/sleep cycle. Science 355:507–510
Del Cid-Pellitero E, Garzon M (2011a) Hypocretin1/orexinA-containing axons innervate locus coeruleus neurons that project to the Rat medial prefrontal cortex. Implication in the sleep-wakefulness cycle and cortical activation. Synapse 65:843–857
Del Cid-Pellitero E, Garzon M (2011b) Medial prefrontal cortex receives input from dorsal raphe nucleus neurons targeted by hypocretin1/orexinA-containing axons. Neuroscience 172:30–43
Dunmyre JR, Mashour GA, Booth V (2014) Coupled flip-flop model for REM sleep regulation in the rat. PLoS One 9:e94481
Duvarci S, Popa D, Pare D (2011) Central amygdala activity during fear conditioning. J Neurosci 31:289–294
Foa EB, Zinbarg R, Rothbaum BO (1992) Uncontrollability and unpredictability in post-traumatic stress disorder: an animal model. Psychol Bull 112:218–238
Forster GL, Pringle RB, Mouw NJ, Vuong SM, Watt MJ, Burke AR, Lowry CA, Summers CH, Renner KJ (2008) Corticotropin-releasing factor in the dorsal raphe nucleus increases medial prefrontal cortical serotonin via type 2 receptors and median raphe nucleus activity. Eur J Neurosci 28:299–310
Fu J, Li P, Ouyang X, Gu C, Song Z, Gao J, Han L, Feng S, Tian S, Hu B (2007) Rapid eye movement sleep deprivation selectively impairs recall of fear extinction in hippocampus-independent tasks in rats. Neuroscience 144:1186–1192
Fuller PM, Saper CB, Lu J (2007) The pontine REM switch: past and present. J Physiol 584:735–741
Gehrman P, Seelig AD, Jacobson IG, Boyko EJ, Hooper TI, Gackstetter GD, Ulmer CS, Smith TC (2013) Predeployment sleep duration and insomnia symptoms as risk factors for new-onset mental health disorders following military deployment. Sleep 36:1009–1018
Genzel L, Spoormaker VI, Konrad BN, Dresler M (2015) The role of rapid eye movement sleep for amygdala-related memory processing. Neurobiol Learn Mem 122:110–121
Goldstein AN, Walker MP (2014) The role of sleep in emotional brain function. Annu Rev Clin Psychol 10:679–708
Grahn RE, Will MJ, Hammack SE, Maswood S, McQueen MB, Watkins LR, Maier SF (1999) Activation of serotonin-immunoreactive cells in the dorsal raphe nucleus in rats exposed to an uncontrollable stressor. Brain Res 826:35–43
Graves LA, Heller EA, Pack AI, Abel T (2003) Sleep deprivation selectively impairs memory consolidation for contextual fear conditioning. Learn Mem 10:168–176
Grillon C, Southwick SM, Charney DS (1996) The psychobiological basis of posttraumatic stress disorder. Mol Psychiatry 1:278–297
Groc L, Choquet D, Chaouloff F (2008) The stress hormone corticosterone conditions AMPAR surface trafficking and synaptic potentiation. Nat Neurosci 11:868–870
Groenink L, van der Gugten J, Zethof T, van der Heyden J, Olivier B (1994) Stress-induced hyperthermia in mice: hormonal correlates. Physiol Behav 56:747–749
Hagewoud R, Whitcomb SN, Heeringa AN, Havekes R, Koolhaas JM, Meerlo P (2010) A time for learning and a time for sleep: the effect of sleep deprivation on contextual fear conditioning at different times of the day. Sleep 33:1315–1322
Hellman K, Abel T (2007) Fear conditioning increases NREM sleep. Behav Neurosci 121:310–323
Herman JP (2013) Neural control of chronic stress adaptation. Front Behav Neurosci 7:61
Hofmann SG (2007) Enhancing exposure-based therapy from a translational research perspective. Behav Res Ther 45:1987–2001
Jaycox LH, Foa EB, Morral AR (1998) Influence of emotional engagement and habituation on exposure therapy for PTSD. J Consult Clin Psychol 66:185–192
Jian M, Luo YX, Xue YX, Han Y, Shi HS, Liu JF, Yan W, Wu P, Meng SQ, Deng JH, Shen HW, Shi J, Lu L (2014) eIF2alpha dephosphorylation in basolateral amygdala mediates reconsolidation of drug memory. J Neurosci 34:10010–10021
Josselyn SA, Kohler S, Frankland PW (2015) Finding the engram. Nat Rev Neurosci 16:521–534
Kalisch R, Wiech K, Critchley HD, Dolan RJ (2006) Levels of appraisal: a medial prefrontal role in high-level appraisal of emotional material. Neuroimage 30:1458–1466
Kamprath K, Wotjak CT (2004) Nonassociative learning processes determine expression and extinction of conditioned fear in mice. Learn Mem 11:770–786
Kerns JG, Cohen JD, MacDonald AW 3rd, Cho RY, Stenger VA, Carter CS (2004) Anterior cingulate conflict monitoring and adjustments in control. Science 303:1023–1026
Kishimoto T, Radulovic J, Radulovic M, Lin CR, Schrick C, Hooshmand F, Hermanson O, Rosenfeld MG, Spiess J (2000) Deletion of crhr2 reveals an anxiolytic role for corticotropin-releasing hormone receptor-2. Nat Genetics 24:415–419
Kleim B, Wysokowsky J, Schmid N, Seifritz E, Rasch B (2016) Effects of sleep after experimental trauma on intrusive emotional memories. Sleep 39:2125–2132
Knight DC, Waters NS, Bandettini PA (2009) Neural substrates of explicit and implicit fear memory. NeuroImage 45:208–214
Koren D, Arnon I, Lavie P, Klein E (2002) Sleep complaints as early predictors of posttraumatic stress disorder: a 1-year prospective study of injured survivors of motor vehicle accidents. Am J Psychiatry 159:855–857
Krettek JE, Price JL (1978) Amygdaloid projections to subcortical structures within the basal forebrain and brainstem in the rat and cat. J Comp Neurol 178:225–254
LaBar KS, Gatenby JC, Gore JC, LeDoux JE, Phelps EA (1998) Human amygdala activation during conditioned fear acquisition and extinction: a mixed-trial fMRI study. Neuron 20:937–945
Laitman BM, Gajewski ND, Mann GL, Kubin L, Morrison AR, Ross RJ (2014) The alpha1 adrenoceptor antagonist prazosin enhances sleep continuity in fear-conditioned Wistar-Kyoto rats. Prog Neuropsychopharmacol Biol Psychiatry 49:7–15
Lavie P (2001) Sleep disturbances in the wake of traumatic events. N Engl J Med 345:1825–1832
LeDoux J (1992) In: Aggleton J (ed) Emotion and the amygdala in the amygdala: neurobiological aspects of emotion, memory and mental dysfunction. Wiley-Liss, New York, pp 339–351
LeDoux JE (1993) Emotional memory systems in the brain. Behav Brain Res 58:69–79
LeDoux JE (2000) Emotion circuits in the brain. Annu Rev Neurosci 23:155–184
Ledoux JE, Muller J (1997) Emotional memory and psychopathology. Philos Trans R Soc Lond Ser B Biol Sci 352:1719–1726
Lee ML, Katsuyama AM, Duge LS, Sriram C, Krushelnytskyy M, Kim JJ, de la Iglesia HO (2016) Fragmentation of rapid eye movement and nonrapid eye movement sleep without total sleep loss impairs hippocampus-dependent fear memory consolidation. Sleep 39:2021–2031
Linnman C, Rougemont-Bucking A, Beucke JC, Zeffiro TA, Milad MR (2011) Unconditioned responses and functional fear networks in human classical conditioning. Behav Brain Res 221:237–245
Liu X, Tang X, Sanford LD (2002) Strain differences in sleep architecture of mice after repeated presentations of fear conditioned cues. Sleep 25:283
Liu X, Tang X, Sanford LD (2003) Fear-conditioned suppression of REM sleep: relationship to Fos expression patterns in limbic and brainstem regions in BALB/cJ mice. Brain Res 991:1–17
Liu X, Tang X, Sanford LD (2009a) Stressor controllability and Fos expression in stress regulatory regions in mice. Physiol Behav 97:321–326
Liu X, Yang L, Wellman LL, Tang X, Sanford LD (2009b) GABAergic antagonism of the central nucleus of the amygdala attenuates reductions in rapid eye movement sleep after inescapable footshock stress. Sleep 32:888–896
Liu X, Wellman LL, Yang L, Ambrozewicz MA, Tang X, Sanford LD (2011) Antagonizing corticotropin-releasing factor in the central nucleus of the amygdala attenuates fear-induced reductions in sleep but not freezing. Sleep 34:1539–1549
Lu J, Sherman D, Devor M, Saper CB (2006) A putative flip-flop switch for control of REM sleep. Nature 441:589–594
Lupien SJ, Lepage M (2001) Stress, memory, and the hippocampus: can’t live with it, can’t live without it. Behav Brain Res 127:137–158
Machida M, Yang L, Wellman LL, Sanford LD (2013) Effects of stressor predictability on escape learning and sleep in mice. Sleep 36:421–430
Madan V, Brennan FX, Mann GL, Horbal AA, Dunn GA, Ross RJ, Morrison AR (2008) Long-term effect of cued fear conditioning on REM sleep microarchitecture in rats. Sleep 31:497–503
Maier SF, Amat J, Baratta MV, Paul E, Watkins LR (2006) Behavioral control, the medial prefrontal cortex, and resilience. Dialogues Clin Neurosci 8:397–406
Martin SJ, Grimwood PD, Morris RG (2000) Synaptic plasticity and memory: an evaluation of the hypothesis. Annu Rev Neurosci 23:649–711
Mavanji V, Datta S (2003) Activation of the phasic pontine-wave generator enhances improvement of learning performance: a mechanism for sleep-dependent plasticity. Eur J Neurosci 17:359–370
McCarley RW (2004) Mechanisms and models of REM sleep control. Arch Ital Biol 142:429–467
McCarley RW (2007) Neurobiology of REM and NREM sleep. Sleep Med 8:302–330
McCarley RW, Hobson JA (1975) Neuronal excitability modulation over the sleep cycle: a structural and mathematical model. Science 189:58–60
McEwen BS (2007) Physiology and neurobiology of stress and adaptation: central role of the brain. Physiol Rev 87:873–904
Meerlo P, Turek FW (2001) Effects of social stimuli on sleep in mice: non-rapid-eye-movement (NREM) sleep is promoted by aggressive interaction but not by sexual interaction. Brain Res 907:84–92
Meerlo P, Pragt BJ, Daan S (1997) Social stress induces high intensity sleep in rats. Neurosci Lett 225:41–44
Meerlo P, Easton A, Bergmann BM, Turek FW (2001) Restraint increases prolactin and REM sleep in C57BL/6J mice but not in BALB/cJ mice. Am J Physiol Regul Integr Comp Physiol 281:R846–R854
Mellman TA, Bustamante V, Fins AI, Pigeon WR, Nolan B (2002) REM sleep and the early development of posttraumatic stress disorder. Am J Psychiatry 159:1696–1701
Mellman TA, Pigeon WR, Nowell PD, Nolan B (2007) Relationships between REM sleep findings and PTSD symptoms during the early aftermath of trauma. J Trauma Stress 20:893–901
Mellman TA, Kobayashi I, Lavela J, Wilson B, Hall Brown TS (2014) A relationship between REM sleep measures and the duration of posttraumatic stress disorder in a young adult urban minority population. Sleep 37:1321–1326
Menz MM, Rihm JS, Salari N, Born J, Kalisch R, Pape HC, Marshall L, Buchel C (2013) The role of sleep and sleep deprivation in consolidating fear memories. Neuroimage 75:87–96
Milad MR, Wright CI, Orr SP, Pitman RK, Quirk GJ, Rauch SL (2007) Recall of fear extinction in humans activates the ventromedial prefrontal cortex and hippocampus in concert. Biol Psychiatry 62:446–454
Milad MR, Pitman RK, Ellis CB, Gold AL, Shin LM, Lasko NB, Zeidan MA, Handwerger K, Orr SP, Rauch SL (2009) Neurobiological basis of failure to recall extinction memory in posttraumatic stress disorder. Biol Psychiatry 66:1075–1082
Morrison AR, Sanford LD, Ross RJ (2000) The amygdala: a critical modulator of sensory influence on sleep. Biol Signals Recept 9:283–296
Mountney C, Anisman H, Merali Z (2011) In vivo levels of corticotropin-releasing hormone and gastrin-releasing peptide at the basolateral amygdala and medial prefrontal cortex in response to conditioned fear in the rat. Neuropharmacology 60:410–417
Myers KM, Davis M (2007) Mechanisms of fear extinction. Mol Psychiatry 12:120–150
Natelson BH (2004) Stress, hormones and disease. Physiol Behav 82:139–143
Neylan TC, Otte C, Yehuda R, Marmar CR (2006) Neuroendocrine regulation of sleep disturbances in PTSD. Ann N Y Acad Sci 1071:203–215
Nezi M, Mastorakos G, Mouslech Z (2000) Corticotropin releasing hormone and the immune/inflammatory response. In: De Groot LJ, Beck-Peccoz P, Chrousos G, Dungan K, Grossman A, Hershman JM, Koch C, McLachlan R, New M, Rebar R, Singer F, Vinik A, Weickert MO (eds) Endotext. South Dartmouth. http://www.ncbi.nlm.nih.gov/pubmed/25905246
Nishida M, Pearsall J, Buckner RL, Walker MP (2009) REM sleep, prefrontal theta, and the consolidation of human emotional memory. Cereb Cortex 19:1158–1166
Nofzinger EA, Buysse DJ, Miewald JM, Meltzer CC, Price JC, Sembrat RC, Ombao H, Reynolds CF, Monk TH, Hall M, Kupfer DJ, Moore RY (2002) Human regional cerebral glucose metabolism during non-rapid eye movement sleep in relation to waking. Brain 125:1105–1115
O’Dell TJ, Connor SA, Guglietta R, Nguyen PV (2015) Beta-adrenergic receptor signaling and modulation of long-term potentiation in the mammalian hippocampus. Learn Mem 22:461–471
Overmier JB, Seligman ME (1967) Effects of inescapable shock upon subsequent escape and avoidance responding. J Comp Physiol Psychol 63:28–33
Page ME, Abercrombie ED (1997) An analysis of the effects of acute and chronic fluoxetine on extracellular norepinephrine in the rat hippocampus during stress. Neuropsychopharmacology 16:419–425
Palamarchouk VS, Swiergiel AH, Dunn AJ (2002) Hippocampal noradrenergic responses to CRF injected into the locus coeruleus of unanesthetized rats. Brain Res 950:31–38
Pare D, Quirk GJ, Ledoux JE (2004) New vistas on amygdala networks in conditioned fear. J Neurophysiol 92:1–9
Pawlyk AC, Morrison AR, Ross RJ, Brennan FX (2008) Stress-induced changes in sleep in rodents: models and mechanisms. Neurosci Biobehav Rev 32:99–117
Paylor R, Tracy R, Wehner J, Rudy J (1994) DBA/2 and C57BL/6 mice differ in contextual fear but not auditory fear conditioning. Behav Neurosci 108:810–817
Petrov T, Krukoff TL, Jhamandas JH (1994) Chemically defined collateral projections from the pons to the central nucleus of the amygdala and hypothalamic paraventricular nucleus in the rat. Cell Tissue Res 277:289–295
Peyron C, Petit JM, Rampon C, Jouvet M, Luppi PH (1998) Forebrain afferents to the rat dorsal raphe nucleus demonstrated by retrograde and anterograde tracing methods. Neuroscience 82:443–468
Phelps EA, Delgado MR, Nearing KI, LeDoux JE (2004) Extinction learning in humans: role of the amygdala and vmPFC. Neuron 43:897–905
Pitman RK, Shin LM, Rauch SL (2001) Investigating the pathogenesis of posttraumatic stress disorder with neuroimaging. J Clin Psychiatry 62(Suppl 17):47–54
Poe GR, Walsh CM, Bjorness TE (2010) Both duration and timing of sleep are important to memory consolidation. Sleep 33:1277–1278
Popa D, Duvarci S, Popescu AT, Lena C, Pare D (2010) Coherent amygdalocortical theta promotes fear memory consolidation during paradoxical sleep. Proc Natl Acad Sci U S A 107:6516–6519
Price J, Russchen F, Amaral D (1987) The limbic region. II: the amygdaloid complex. In: Swanson L (ed) Handbook of chemical neuroanatomy. Integrated systems of the CNA, Part I. Elsevier, New York, pp 279–375
Puig MV, Artigas F, Celada P (2005) Modulation of the activity of pyramidal neurons in rat prefrontal cortex by raphe stimulation in vivo: involvement of serotonin and GABA. Cereb Cortex 15:1–14
Pynoos R, Ritzmann R, Steinberg A, Goenjian A, Prisecaru I (1996) A behavioral animal model of posttraumatic stress disorder featuring repeated exposure to situational reminders. Biol Psychiatry 39:129–134
Qin M, Xia Z, Huang T, Smith CB (2011) Effects of chronic immobilization stress on anxiety-like behavior and basolateral amygdala morphology in Fmr1 knockout mice. Neuroscience 194:282–290
Rahn EJ, Guzman-Karlsson MC, David Sweatt J (2013) Cellular, molecular, and epigenetic mechanisms in non-associative conditioning: implications for pain and memory. Neurobiol Learn Mem 105:133–150
Ramaligam V, Chen MC, Saper CB, Lu J (2013) Perspectives on the rapid eye movement sleep switch in rapid eye movement sleep behavior disorder. Sleep Med 14:707–713
Rampin C, Cespuglio R, Chastrette N, Jouvet M (1991) Immobilisation stress induces a paradoxical sleep rebound in rat. Neurosci Lett 126:113–118
Rasch B, Born J (2013) About sleep's role in memory. Physiol Rev 93:681–766
Ribeiro S, Goyal V, Mello CV, Pavlides C (1999) Brain gene expression during REM sleep depends on prior waking experience. Learn Mem 6:500–508
Rolls A, Colas D, Adamantidis A, Carter M, Lanre-Amos T, Heller HC, de Lecea L (2011) Optogenetic disruption of sleep continuity impairs memory consolidation. Proc Natl Acad Sci U S A 108:13305–13310
Ross RJ (2014) The changing REM sleep signature of posttraumatic stress disorder. Sleep 37:1281–1282
Ruskin DN, Lahoste GJ (2008) Aspects of learned fear related to the hippocampus are sleep-dependent. Behav Brain Res 191:67–71
Ruskin DN, Liu C, Dunn KE, Bazan NG, LaHoste GJ (2004) Sleep deprivation impairs hippocampus-mediated contextual learning but not amygdala-mediated cued learning in rats. Eur J Neurosci 19:3121–3124
Salehi B, Cordero MI, Sandi C (2010) Learning under stress: the inverted-U-shape function revisited. Learn Mem 17:522–530
Sanford LD, Tang X (2009) Effect of stress on sleep and its relationship to PTSD. In: Shiromani P, Keane T, LeDoux J (eds) Neurobiology of PTSD. Humana Press, Totowa, pp 231–253
Sanford LD, Tejani-Butt SM, Ross RJ, Morrison AR (1995) Amygdaloid control of alerting and behavioral arousal in rats: involvement of serotonergic mechanisms. Arch Ital Biol 134:81–99
Sanford LD, Parris B, Tang X (2002) GABAergic regulation of the central nucleus of the amygdala: implications for sleep control. Brain Res Bull 956(2):276–284
Sanford LD, Tang X, Ross RJ, Morrison AR (2003a) Influence of shock training and explicit fear-conditioned cues on sleep architecture in mice: strain comparison. Behav Genet 33:43–58
Sanford LD, Yang L, Tang X (2003b) Influence of contextual fear on sleep in mice: a strain comparison. Sleep 26:527–540
Sanford LD, Fang J, Tang X (2003c) Sleep after differing amounts of conditioned fear training in BALB/cJ mice. Behav Brain Res 147:193–202
Sanford LD, Yang L, Wellman LL, Liu X, Tang X (2010) Differential effects of controllable and uncontrollable footshock stress on sleep in mice. Sleep 33:621–630
Sanford LD, Suchecki D, Meerlo P (2015) Stress, arousal, and sleep. Curr Top Behav Neurosci 25:379–410
Saper CB, Fuller PM, Pedersen NP, Lu J, Scammell TE (2010) Sleep state switching. Neuron 68:1023–1042
Scammell TE, Arrigoni E, Lipton JO (2017) Neural circuitry of wakefulness and sleep. Neuron 93:747–765
Sehlmeyer C, Schoning S, Zwitserlood P, Pfleiderer B, Kircher T, Arolt V, Konrad C (2009) Human fear conditioning and extinction in neuroimaging: a systematic review. PLoS One 4:e5865
Sekine Y, Zyryanova A, Crespillo-Casado A, Fischer PM, Harding HP, Ron D (2015) Stress responses. Mutations in a translation initiation factor identify the target of a memory-enhancing compound. Science 348:1027–1030
Seligman ME, Beagley G (1975) Learned helplessness in the rat. J Comp Physiol Psychol 88:534–541
Seligman ME, Maier SF (1967) Failure to escape traumatic shock. J Exp Psychol 74:1–9
Seligman ME, Rosellini RA, Kozak MJ (1975) Learned helplessness in the rat: time course, immunization, and reversibility. J Comp Physiol Psychol 88:542–547
Shalev AY (2000) Biological responses to disasters. Psychiatr Quart 71:277–288
Shalev AY, Ragel-Fuchs Y, Pitman RK (1992) Conditioned fear and psychological trauma. Biol Psychiatry 31:863–865
Siegel JM (2001) The REM sleep-memory consolidation hypothesis. Science 294:1058–1063
Siegel JM (2011) REM sleep: a biological and psychological paradox. Sleep Med Rev 15:139–142
Siegmund A, Wotjak CT (2006) Toward an animal model of posttraumatic stress disorder. Ann N Y Acad Sci 1071:324–334
Smagin GN, Swiergiel AH, Dunn AJ (1995) Corticotropin-releasing factor administered into the locus coeruleus, but not the parabrachial nucleus, stimulates norepinephrine release in the prefrontal cortex. Brain Res Bull 36:71–76
Smid GE, van der Velden PG, Lensvelt-Mulders GJ, Knipscheer JW, Gersons BP, Kleber RJ (2012) Stress sensitization following a disaster: a prospective study. Psychol Med 42:1675–1686
Smith C, Butler S (1982) Paradoxical sleep at selective times following training is necessary for learning. Physiol Behav 29:469–473
Smith C, Kelly G (1988) Paradoxical sleep deprivation applied two days after end of training retards learning. Physiol Behav 43:213–216
Smith C, Lapp L (1986) Prolonged increases in both PS and number of REMS following a shuttle avoidance task. Physiol Behav 36:1053–1057
Smith CT, Miskiman DE (1975) Increases in paradoxical sleep as a result of amygdaloid stimulation. Physiol Behav 15:17–19
Smith C, Kitahama K, Valatx JL, Jouvet M (1974) Increased paradoxical sleep in mice during acquisition of a shock avoidance task. Brain Res 77:221–230
Smith C, Young J, Young W (1980) Prolonged increases in paradoxical sleep during and after avoidance-task acquisition. Sleep 3:67–81
Southwick SM, Bremner D, Krystal JH, Charney DS (1994) Psychobiologic research in post-traumatic stress disorder. Psychiatr Clin North Am 17:251–264
Spoormaker VI, Gvozdanovic GA, Samann PG, Czisch M (2014) Ventromedial prefrontal cortex activity and rapid eye movement sleep are associated with subsequent fear expression in human subjects. Exp Brain Res 232:1547–1554
Sripada RK, Rauch SA (2015) Between-session and within-session habituation in Prolonged Exposure Therapy for posttraumatic stress disorder: a hierarchical linear modeling approach. J Anxiety Disord 30:81–87
Steriade M, McCarley R (1990) Brainstem control of wakefulness and sleep. Plenum Press, New York
Stickgold R (2005) Sleep-dependent memory consolidation. Nature 437:1272–1278
Stickgold R, Walker MP (2007) Sleep-dependent memory consolidation and reconsolidation. Sleep Med 8:331–343
Stujenske JM, Likhtik E, Topiwala MA, Gordon JA (2014) Fear and safety engage competing patterns of theta-gamma coupling in the basolateral amygdala. Neuron 83:919–933
Suchecki D, Tiba PA, Machado RB (2012) REM sleep rebound as an adaptive response to stressful situations. Front Neurol 3:41
Takeuchi T, Duszkiewicz AJ, Sonneborn A, Spooner PA, Yamasaki M, Watanabe M, Smith CC, Fernandez G, Deisseroth K, Greene RW, Morris RG (2016) Locus coeruleus and dopaminergic consolidation of everyday memory. Nature 537:357–362
Tang X, Yang L, Sanford LD (2005) Rat strain differences in freezing and sleep alterations associated with contextual fear. Sleep 28:1235–1244
Tononi G, Cirelli C (2014) Sleep and the price of plasticity: from synaptic and cellular homeostasis to memory consolidation and integration. Neuron 81:12–34
Ulloor J, Datta S (2005) Spatio-temporal activation of cyclic AMP response element-binding protein, activity-regulated cytoskeletal-associated protein and brain-derived nerve growth factor: a mechanism for pontine-wave generator activation-dependent two-way active-avoidance memory processing in the rat. J Neurochem 95:418–428
Van Bockstaele EJ, Colago EE, Valentino RJ (1998) Amygdaloid corticotropin-releasing factor targets locus coeruleus dendrites: substrate for the co-ordination of emotional and cognitive limbs of the stress response. J Neuroendocrinol 10:743–757
Van Bockstaele EJ, Peoples J, Valentino RJ (1999) A.E. Bennett Research Award. Anatomic basis for differential regulation of the rostrolateral peri-locus coeruleus region by limbic afferents. Biol Psychiatry 46:1352–1363
Van den Berg C, Lamberts R, Wolterink G, Wiegant V, Van Ree J (1998) Emotional and footshock stimuli induce differential long-lasting behavioural effects in rats; involvement of opioids. Brain Res 799:6–15
van der Helm E, Yao J, Dutt S, Rao V, Saletin JM, Walker MP (2011) REM sleep depotentiates amygdala activity to previous emotional experiences. Curr Biol 21:2029–2032
Van Dijken H, Mos J, van der Heyden J, Tilders F (1992) Characterization of stress-induced long-term behavioural changes in rats: evidence in favor of anxiety. Physiol Behav 52:945–951
van Dongen EV, Takashima A, Barth M, Zapp J, Schad LR, Paller KA, Fernandez G (2012) Memory stabilization with targeted reactivation during human slow-wave sleep. Proc Natl Acad Sci U S A 109:10575–10580
van Marle HJ, Hermans EJ, Qin S, Overeem S, Fernandez G (2013) The effect of exogenous cortisol during sleep on the behavioral and neural correlates of emotional memory consolidation in humans. Psychoneuroendocrinology 38:1639–1649
Veening JG, Bouwknecht JA, Joosten HJ, Dederen PJ, Zethof TJ, Groenink L, van der Gugten J, Olivier B (2004) Stress-induced hyperthermia in the mouse: c-fos expression, corticosterone and temperature changes. Prog Neuropsychopharmacol Biol Psychiatry 28:699–707
Vertes RP (2004a) Memory consolidation in sleep; dream or reality. Neuron 44:135–148
Vertes RP (2004b) Differential projections of the infralimbic and prelimbic cortex in the rat. Synapse 51:32–58
Vertes RP, Siegel JM (2005) Time for the sleep community to take a critical look at the purported role of sleep in memory processing. Sleep 28:1228–1229 discussion 30–3
Vinckers CH, van Oorschot R, Olivier B, Groenink L (2009) Stress-induced hyperthermia in the mouse. In: Gould TD (ed) Mood and anxiety-related phenotypes in mice: characterization using behavioral tests. Humana Press, New York, pp 139–152
Vyas A, Jadhav S, Chattarji S (2006) Prolonged behavioral stress enhances synaptic connectivity in the basolateral amygdala. Neuroscience 143:387–393
Wagner U, Born J (2008) Memory consolidation during sleep: interactive effects of sleep stages and HPA regulation. Stress 11:28–41
Wagner U, Gais S, Born J (2001) Emotional memory formation is enhanced across sleep intervals with high amounts of rapid eye movement sleep. Learn Mem 8:112–119
Walker MP (2009) The role of slow wave sleep in memory processing. J Clin Sleep Med 5:S20–S26
Walker MP, van der Helm E (2009) Overnight therapy? The role of sleep in emotional brain processing. Psychol Bull 135:731–748
Watanabe Y, Stone E, McEwen BS (1994) Induction and habituation of c-fos and zif/268 by acute and repeated stressors. Neuroreport 5:1321–1324
Wellman LL, Yang L, Ambrozewicz MA, Machida M, Sanford LD (2013) Basolateral amygdala and the regulation of fear-conditioned changes in sleep: role of corticotropin-releasing factor. Sleep 36:471–480
Wellman LL, Fitzpatrick ME, Machida M, Sanford LD (2014) The basolateral amygdala determines the effects of fear memory on sleep in an animal model of PTSD. Exp Brain Res 232:1555–1565
Wellman LL, Fitzpatrick ME, Kuzmina OY, Sutton AM, Williams BL, Sanford LD (2016) Individual differences in animal stress models: considering resilience, vulnerability and the amygdala in mediating the effects of stress and conditioned fear on sleep. Sleep 39:1293–1303
Wellman LL, Fitzpatrick ME, Hallum OY, Sutton AM, Williams BL, Sanford LD (2017) The basolateral amygdala can mediate the effects of fear memory on sleep independently of fear behavior and the peripheral stress response. Neurobiol Learn Mem 137:27–35
Whitehurst LN, Cellini N, McDevitt EA, Duggan KA, Mednick SC (2016) Autonomic activity during sleep predicts memory consolidation in humans. Proc Natl Acad Sci U S A 113:7272–7277
Xi M, Fung SJ, Sampogna S, Chase MH (2011) Excitatory projections from the amygdala to neurons in the nucleus pontis oralis in the rat: an intracellular study. Neuroscience 197:181–190
Yang L, Wellman LL, Ambrozewicz MA, Sanford LD (2011) Effects of stressor predictability and controllability on sleep, temperature, and fear behavior in mice. Sleep 34:759–771
Yehuda R (2001) Biology of posttraumatic stress disorder. J Clin Psychiatry 62(Suppl 17):41–46
Yehuda R, LeDoux J (2007) Response variation following trauma: a translational neuroscience approach to understanding PTSD. Neuron 56:19–32
Yehuda R, Flory JD, Southwick S, Charney DS (2006) Developing an agenda for translational studies of resilience and vulnerability following trauma exposure. Ann N Y Acad Sci 1071:379–396
Young SK, Wek RC (2016) Upstream open reading frames differentially regulate gene-specific translation in the integrated stress response. J Biol Chem 291:16927–16935
Zangenehpour S, Chaudhuri A (2002) Differential induction and decay curves of c-fos and zif268 revealed through dual activity maps. Brain Res Mol Brain Res 109:221–225
Zhang J, Xi M, Fung SJ, Sampogna S, Chase MH (2012) Projections from the central nucleus of the amygdala to the nucleus pontis oralis in the rat: an anterograde labeling study. Neurosci Lett 525:157–162
Zohar J, Juven-Wetzler A, Sonnino R, Cwikel-Hamzany S, Balaban E, Cohen H (2011) New insights into secondary prevention in post-traumatic stress disorder. Dialogues Clin Neurosci 13:301–309
Acknowledgment
Portions of this work were supported by NIH research grant MH64827 (L.D.S).
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2019 Springer Nature Singapore Pte Ltd.
About this chapter

Cite this chapter
Sanford, L.D., Wellman, L.L., Lonart, G., Ross, R.J. (2019). Sleep, Stress, and Traumatic Memory. In: Jha, S., Jha, V. (eds) Sleep, Memory and Synaptic Plasticity. Springer, Singapore. https://doi.org/10.1007/978-981-13-2814-5_7
Download citation
DOI: https://doi.org/10.1007/978-981-13-2814-5_7
Published:
Publisher Name: Springer, Singapore
Print ISBN: 978-981-13-2813-8
Online ISBN: 978-981-13-2814-5
eBook Packages: Biomedical and Life SciencesBiomedical and Life Sciences (R0)