
Abstract
Numerous evidence revealed that climate change could have adverse effects on human health, while in developing countries, especially in China, less evidence covering different climatic zones is available due to data unavailability. We searched studies which investigated the association between ambient temperature and mortalities in six databases. We performed random-effects model to calculate pooled estimated for mortalities in association with per 1 °C increase (or decrease). We finally included 17 in 819 identified articles. Short-term exposures to inappropriate temperature were significantly associated with mortalities, per 1 °C increase corresponded to a 1.2% (95% CI: 1.1%, 1.3%) increase in all-cause mortality, a 2.6% (95% CI: 2.4%, 2.9%) increase in cardiovascular mortality, and a 1.2% (95% CI: 1.0%, 1.3%) increase in respiratory mortality. And each 1 °C decrease caused a 3.1% (95% CI: 2.7%, 3.5%) in all-cause mortality, a 1.5% (95% CI: 1.2%, 1.9%) increase in cardiovascular mortality, and a 3.3% (95% CI: 2.8%, 3.9%) increase in respiratory mortality. Our findings indicated that the increase and decrease in ambient temperature have relationships with mortalities among Chinese population and cold effect was more durable and pronounced than hot effect.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
2.1 Introduction
In the last 130 years, the world has warmed by approximately 0.85 °C. Since 1850, temperatures have been significantly warmer than previous decade [1]. Although global warming can bring some local benefits, such as reduced winter deaths in temperate climes and increased food production in some areas, climate change has adverse effects on overall health. Extreme high air temperatures contribute directly to deaths from cardiovascular and respiratory disease, particularly among elderly people. For example, more than 70,000 excess deaths were recorded in the heat wave of summer 2003 in Europe [2].
Existing evidence shows that meteorological factors have apparent association with death, such as temperature, relative humidity, atmospheric pressure, wind velocity, etc. Study area was mainly located in coastal area and economic developed area in China; few studies have focused on the effects of meteorological factors on mortality among county-level city and economically backward area.
With global warming, ambient temperature has the greatest impact on death among the meteorological factors. Increasing evidence indicated that exposure to inappropriate temperature could have adverse effects on human health worldwide. Most of these studies demonstrated that the relationship between temperature and mortality was generally U-, V-, or J-shaped, with higher risks of mortality in extreme cold and hot temperature. However, the associations vary among different studies due to differences in geographic locations, population characteristics, and weather conditions, so more comprehensive studies with a wider variety of climate zone and population structure are needed to assess the overall association among Chinese population [3,4,5].
Cardiovascular disease and respiratory disease are one of the leading causes of death worldwide. An estimated 17.3 million people died from cardiovascular disease in 2008, representing 30% of all global deaths. Low- and middle-income countries are disproportionally affected: over 80% of cardiovascular disease deaths take place in low- and middle-income countries and occur almost equally in men and women [6]. Respiratory disease includes asthma, chronic obstructive pulmonary disease (COPD), pneumonia, etc. According to the latest World Health Organization (WHO) estimates, currently 64 million people have COPD, and three million people died of COPD. WHO predicts that COPD will become the third leading cause of death worldwide by 2030 [7]. A lot of studies demonstrated cardiovascular disease and respiratory disease were related to meteorological factors, especially to temperature.
Many recent epidemiological studies have investigated that extreme temperatures have various adverse effects on human health in China [8, 9], while most studies were limited to a single city or a small number of cities in China [10, 11]. However, these results cannot fully show the real effects due to the wide range of climatic, sociodemographic, and cultural characteristics of China. Therefore, a study overview to summarize the relationship between ambient temperature and mortality among Chinese population is warranted.
In this chapter, we examined the ambient temperature and mortality in Chinese population including Mainland China, Hong Kong, Taiwan, and Macao. This study will provide useful information to develop intervention strategies for cold and hot temperature exposures in China.
2.2 Materials and Methods
2.2.1 Literature Search and Data Extraction
We searched the major electronic databases including MEDLINE database, PubMed database, Ovid database, China National Knowledge Infrastructure (CNKI) database, Chinese Wanfang database, and Chinese VIP database. We used the following combinations of keywords: (1) temperature, weather, climate change, heat, cold, and season and (2) adverse effect, health, disease, death, and mortality. In order to reflect the health effects of exposure to inappropriate temperature among Chinese populations, we searched potential articles on temperature over the China published between January 2000 and December 2017. References of all included articles were searched for any additional studies.
We converted the effect estimates reported in each study into the ER in deaths per 1 °C increase (or decrease) in daily average temperature if different scales or indicators were used. And we contacted authors to apply for additional data as necessary. Two investigators have extracted data independently, and conflicts were adjudicated by a third investigator.
2.2.2 Study Selection Criteria
Eligible studies fell into following categories:
-
1.
All epidemiological studies, in both English and Chinese, involved the health impacts of exposure to temperature.
-
2.
Original studies provided quantitative exposure-response relationships between ambient temperature and health outcomes (e.g., relative risk, odds ratios, excess risk [ER], or hazard ratios and their 95% confidence intervals [95% CI]).
-
3.
At least 1 year of daily data relating to a general population.
-
4.
Studies were not identical or similar in terms of location or study period.
-
5.
Study location must be located in Mainland China, Hong Kong, Taiwan, and Macao.
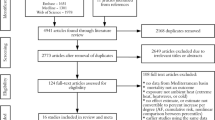
We selected the most recent studies if more than two published articles have the same study period, location, and population. We presented a flow diagram of the study selection process (Fig. 2.1).

Procedure for literature search
2.2.3 Statistical Analysis
We used random-effects meta-analysis to estimate the overall association between ambient temperature and mortality as well as the corresponding 95% confidence interval. The excess risk was used as a summary statistic. To check the robustness of the effect estimation, we conducted a sensitivity analysis by individually excluding the studies with the largest and the smallest effect estimates from the meta-analyses.
We applied I2 test to examine heterogeneity. I2 statistic was used to estimate the percentage of total variation across studies because of heterogeneity rather than chance. I2 can be calculated as the following formula: I2 = 100%*(Q – df)/Q (Q, Cochrane’s heterogeneity statistics; df, degree of freedom). We defined more than 50% heterogeneity as substantial heterogeneity. If no substantial heterogeneity exits in the combined data, we used fixed-effects model to calculate overall estimate, and if substantial heterogeneity is present, a random-effects model is more appropriate [12]. To further confirm the robustness of the results, we have showed the results with both fixed- and random-effects models.
Finally, publication bias was evaluated using funnel plots and Egger’s linear regression method. All analysis was done and performed using R version 2.13.0 (R Foundation for Statistical Computing, Vienna, Austria). A value of p < 0.05 was considered significant.
2.3 Results
The process of study selection is shown in Fig. 2.1. Our search stratifies and initially identified a total of 819 articles, among which 768 were excluded as they were irrelevant to the study topic by examining the abstract. The remaining 51 underwent in-depth review, 19 of them were excluded due to their estimated effect based on extreme climate change such as cold spells and heat waves; 11 studies were excluded based on the special meteorological indicators (diurnal temperature range; universal thermal climate index; temperature changes between neighboring days; apparent temperature); and 4 studies showed, at the same time, geographical area with similar information removed. The remaining 17 studies were included in the meta-analysis. Among them, 12 articles examined the relationships between all-cause mortality and temperature, 12 reported the effects of temperature on cardiovascular mortality, and 10 estimated the associations between ambient temperature and respiratory mortality.
2.3.1 Short-Term Effects on All-Cause Mortality
We systematically searched for all articles containing the association between temperature and mortality. A total of 12 studies reporting the short-term effects of temperature on all-cause mortality were finally included after excluding studies from the same study area (Table 2.1).
The pooled associations between temperature exposure and mortalities were separately reported for the heat and cold exposure. For hot effects, 51 of the 84 estimates of all-cause mortality were statistically significant; and for cold effects, 71 of the 84 estimates were statistically significant. Based on random-effects models in the meta-analyses, we estimated that a 1 °C increase was related to a 1.2% increase (95% CI: 1.1%, 1.3%) in all-cause mortality, and 1 °C decrease was corresponded to a 2.6% increase (95% CI: 2.4%, 2.9%) in all-cause mortality.
We observed significant heterogeneity across the study areas. For hot effects, one study in Fuzhou reported a considerable positive association between heat exposure and all-cause mortality (ER = 21.7%, 95% CI: 12.0%, 32.3%) [13], while negative effect was observed in Lhasa (ER = 7.9%, 95% CI: –16.6%, 39.6%) and in Urumqi (ER = 0.9%, 95% CI: –1.9%, 3.7%) [14]. For cold effects, study from Hong Kong reported a positive but nonsignificant association between cold exposure and all-cause mortality (ER = 2.1%, 95% CI: –2.3%, 4.6%) [15]; however, a large positive effect was reported in Guangzhou (ER = 9.6%, 95% CI: 7.5%, 11.7%) [16].
2.3.2 Short-Term Effects on Cardiovascular Mortality
A total of 70 individual effect estimates were identified by our literature search for the short-term effects on cardiovascular mortality (Table 2.2).
Statistically significant associations between temperature and cardiovascular mortality were reported in most of the study cities. For hot effects, 44 of the 72 estimates of all-cause mortality were statistically significant; and for cold effects, 56 of the 72 estimates were statistically significant. We observed pooled ER for cardiovascular mortality for each 1 °C increment was 1.2% (95% CI: 1.0%, 1.3%); the pooled ER was 3.1% (95% CI: 2.7%, 3.5%) for each 1 °C decrement.
Between-city heterogeneity was observed in the short-term cardiovascular mortality effects of temperature. For hot effects, studies from Changsha reported a positive but nonsignificant association between heat exposure and cardiovascular mortality (ER = 8.2%, 95% CI: –14.1%, 36.4%) [17], and another study in Harbin also reported the same results (ER = 2.1%, 95% CI: –0.3%, 4.6%) [13], while a large effect was observed in Kunming (ER = 14.3%, 95%CI: 3.8%, 25.8%) and Guangzhou (ER = 22.6%, 95% CI: 10.2%, 36.4%) [17]. For cold effects, the positive relationships were observed between cold exposure and cardiovascular mortality in Nanjing (ER = 5.1%, 95% CI: 1.6%, 16.4%) and Chengdu (ER = 3.5%, 95% CI: 1.0%, 12.8%) [18], while large but nonsignificant results were found in Zhuhai (ER = 10.3%, 95% CI: –6.5%, 30.0%) [17].
2.3.3 Short-Term Effects on Respiratory Mortality
We finally included 60 individual effect estimates in our meta-analysis to investigate the short-term effects on respiratory mortality (Table 2.3).
A number of study cities presented significant relationships between temperature and respiratory mortality. For hot effects, 29 of the 60 estimates of all-cause mortality were statistically significant; and for cold effects, 45 of the 60 estimates were statistically significant. The short-term effects of heat exposure on the respiratory mortality were 1.5% (95% CI: 1.2%, 1.9%), and the short-term effects of cold exposure on the respiratory mortality were 3.3% (95% CI: 2.8%, 3.9%).
Different regions show heterogeneity on the short-term respiratory mortality effects of temperature. For example, the estimated effect of a 1 °C increment on respiratory mortality was 13.4% (95% CI: 6.3%, 19.8%) in Fuzhou, while another study in Hong Kong found non-statistically significant association (ER = 1%, 95% CI: –4.1%, 6.4%) [13, 15]. In addition, one study demonstrated a large significant cold effect on respiratory mortality (ER = 9.3%, 95% CI: 1.7%, 17.4%) in Tianjin [10], while one study in Taiwan has not found statistically significant association between cold temperature and respiratory mortality (ER = 1.5%, 95% CI: –0.1%, 3.2%) [19].
2.4 Discussion
In recent years there has been a great increase in interest in time-series studies of temperature and mortality. Increasing evidence showed statistically significant associations between temperature and mortality. While less attention has been paid to the effects of temperature in China, most of studies have focused on the effects of temperatures in a single city or only a few cities. In this meta-analysis, we identified 18 studies on the short-term associations between temperature and mortality among Chinese population. We aim to identify and quantify the association between temperatures and mortality among Chinese population through a systematic review and meta-analysis.
To our knowledge, this is the first meta-analysis to quantitatively assess the estimates of ambient temperature effects on mortality among Chinese population. In this analysis, we combined 84, 72, and 60 individual effect estimates on the all-cause mortality, cardiovascular disease, and respiratory disease. The results reveal a statistically significant increase of mortalities associated with a 1 °C increase (or decrease) in ambient temperature.
Our estimates indicated that both hot and cold temperature exposures have adverse effects on mortalities. The pooled results show that a 1 °C increase on hot days was related to a 1.2% (95% CI: 1.1%, 1.3%) increase in all-cause mortality, a 1.2% (95% CI: 1.0%, 1.3%) increase in cardiovascular mortality, and a 1.5% (95% CI: 1.2%, 1.9%) increase in respiratory mortality, respectively. And a 1 °C decrease was associated with a 2.6% increase (95% CI: 2.4%, 2.9%) in all-cause mortality, 3.1% (95% CI: 2.7%, 3.5%) increase in cardiovascular mortality, and 3.3% (95% CI: 2.8%, 3.9%) increase in respiratory mortality, respectively. The results show a statistically significant increase of mortalities associated with a 1 °C increase or a 1 °C decrease in ambient temperature among Chinese population.
We found that hot effects and cold effects were different, in which heat temperatures have a smaller effect on mortality than cold temperatures. Furthermore, the hot effects of all-cause mortality, cardiovascular disease, and respiratory disease were the same, while the cold effects show differences, with the largest cold effects on respiratory disease.
The pooled estimates from this meta-analysis are consistent with same previous studies. For example, a meta-analysis published in 2013 summarized that cold effects were relatively larger than hot effects, which reported an ER of all-cause mortality increased by 2.0% (95% CI: 1.0%, 3.0%) for the heat exposure and 4.0% (95% CI: 2.0%, 7.0%) for the cold exposure [20]. And another systematic review and meta-analysis were conducted; the risk of cardiovascular mortality increased by 5.5% (95% CI: 5.0%, 6.0%) for the cold exposure and 1.3% (95% CI: 1.1%, 1.5%) for the heat exposure [21]. Conversely, few studies observed larger hot effect than cold effect. For example, Zhang’s study in Wuhan observed larger hot effect on mortalities than cold effect (all-cause mortality, 25.2% vs. 1.7%; cardiovascular mortality, 34.1% vs. 3.0%; respiratory mortality, 24.3% vs. 1.1%) [22].
The results of our meta-analysis reveal relatively stronger association between cold exposure and respiratory mortality. Series of studies also reported the same results, for example, a study in Dublin observed larger effects on respiratory mortality than all-cause mortality and cardiovascular mortality [23]. The underlying mechanism was still unclear and may be due to a synergy between temperature and air pollution on the respiratory system but not on the cardiovascular system. This result suggests that we should strengthen the protection and prevention among people suffering from chronic cardiovascular or respiratory diseases in China.
We conducted a number of sensitivity analyses to examine the robustness of the effect estimation; the results were shown in Table 2.4. When excluding single study with the largest or smallest effect, we observed generally consistent associations between short-term exposure to heat (or cold) temperature and mortalities. For example, when excluding the largest hot effect of all-cause mortality, the estimate still stables (ER = 1.2%, 95% CI: 1.1%, 1.3%). We also obtained robust effects when we alternatively used fixed-effect meta-analysis.
All outcomes showed substantial (I2 = 67.31–94.17%) and statistically significant heterogeneity in the point estimates for temperature among included studies. The results of Egger’s tests revealed that there was significant publication bias in the meta-analyses (Table 2.5).
Previous epidemiologic evidence showed that climatological, socioeconomic, demographic, community-level, and individual factors have a role in modification of the association between temperature and mortality [24, 25].
A great number of studies demonstrated that age group might modify the relationship between temperature and mortality. One study in China reported larger mortality effect of temperature in older age group than younger age group [24]. This evidence has also been observed in several previous studies [26,27,28]. For example, Ma’s study in Shanghai reported increasing trend in risk with age in temperature, which clarifies the elderly to be the most vulnerable to the short-term exposure of temperature. The underlying reasons might be that pre-existing disorders and difficulty in thermoregulation come with age [29, 30].
Gender was usually considered a potential effect modifier. One study in China found higher risk of dying among females than males [24]. Another study in Australia reported effect estimate among females was even more than 20 times that among males [28]; and one study in Suzhou also support this view [31]. One previous experimental study reported that one possible mechanism might be that female were more heat intolerant than male possibly due to sex-specific differences in thermoregulatory and physiological mechanisms [32].
A series of evidence demonstrated that community-level factors could modify the relationship between temperature and mortality [14, 25, 33], such as population density, green coverage, economic situation, educational level and adaptive capacity. For example, Huang’s study observed higher mortality risk in areas with a lower educational level, which is consistent with previous studies [34, 35]. One possible reason might be that higher educated people tend to pay more attention to their health.
One interesting finding was that 1-degree change for latitude could influence the relationship between ambient temperature and mortality. A great number of studies observed that higher-latitude countries demonstrated higher effects of heat temperature on the risk of mortality, while it showed lower effects of cold temperature on the risk of mortality [36, 37]. The underlying reason might be that residents in high-latitude regions usually live in colder environment for longer time compared with those in low-latitude regions, so they are better adapted to low temperatures, and are more vulnerable to high temperatures.
2.5 Conclusion
Climate change could lead to serious public health problems in China. This chapter quantitatively estimated the effects of ambient temperature exposures on mortalities among Chinese population; the pooled estimates were found to be statistically significant for both heat and cold exposures and mortality categories. For both hot and cold effects, this study provided evidences to support the associations between heat and cold exposures and the risk of mortality from all-cause, cardiovascular, and respiratory mortality. In addition, we found the cold effects were larger than hot effects among Chinese population. We also found the pooled cold effect on respiratory mortality was obviously greater than all-cause and cardiovascular mortality. This meta-analysis suggests that more attention should be paid to the health effects caused by cold weather, especially for people suffering from cardiovascular and respiratory diseases in China.
References
IPCC. Climate change 2013: the physical science basis. In: Stocker TF, Qin D, Plattner G-K, Tignor M, Allen SK, Boschung J, Nauels A, Xia Y, Bex V, Midgley PM, editors. Contribution of working group I to the fifth assessment report of the intergovernmental panel on climate change. Cambridge: Cambridge University Press; 2013. 1535p.
Robine JM, Cheung SL, Le RS, Van OH, Griffiths C, Michel JP, Herrmann FR. Death toll exceeded 70,000 in Europe during the summer of 2003. C R Biol. 2008;331(2):171–8.
Castillejos M, Borja-Aburto VH, Dockery DW, Gold DR, Loomis D. Airborne coarse particles and mortality. Inhal Toxicol. 2000;12(Supp 1):61–72.
Gasparrini A, Guo Y, Hashizume M, Lavigne E, Zanobetti A, Schwartz J, Tobias A, Tong S, Rocklöv J, Forsberg B. Mortality risk attributable to high and low ambient temperature: a multicountry observational study. Lancet. 2015;386(9991):369–75.
Guo Y, Antonio G, Armstrong BG, Benjawan T, Aurelio T, Eric L, Pan X, Ho K, Masahiro H. Temperature variability and mortality: a multi-country study. Environ Health Perspect. 2016;124(10):1554–9.
Wang H, Naghavi M, Allen C, Barber RM, ZA B. Global, regional, and national life expectancy, all-cause mortality, and cause-specific mortality for 249 causes of death, 1980-2015: a systematic analysis for the Global Burden of Disease Study 2015. Lancet. 2016;388(10053):1459.
Bousquet J, Khaltaev N, Bousquet J, Khaltaev N. Global surveillance, prevention and control of chronic respiratory diseases: a comprehensive approach. J Pharm Technol. 2008;24(2):122.
Yuan J, Lau EH, Li K, Leung YH, Yang Z, Xie C, Liu Y, Liu Y, Ma X, Liu J. Effect of live poultry market closure on Avian Influenza A(H7N9) virus activity in Guangzhou, China, 2014. Emerg Infect Dis. 2015;21(10):1784.
Ma W, Wang L, Lin H, Liu T, Zhang Y, Rutherford S, Luo Y, Zeng W, Zhang Y, Wang X. The temperature-mortality relationship in China: an analysis from 66 Chinese communities. Environ Res. 2015;137:72.
Guo Y, Barnett AG, Pan X, Yu W, Tong S. The impact of temperature on mortality in Tianjin, China: a case-crossover design with a distributed lag nonlinear model. Environ Health Perspect. 2011;119(12):1719–25.
Yang J, Ou CQ, Yan D, Zhou YX, Chen PY. Daily temperature and mortality: a study of distributed lag non-linear effect and effect modification in Guangzhou. Environ Health. 2012;11(1):63.
Higgins JP, Thompson SG. Quantifying heterogeneity in a meta-analysis. Stat Med. 2002;21(11):1539.
Pei D, Li L. Threshold analysis of ambient temperature in five cities based on population daily mortality. Chin J Dis Control Prev. 2011;15(5):372–6.
Huang Z, Lin H, Liu Y, Zhou M, Liu T, Xiao J, Zeng W, Li X, Zhang Y, Ebi KL. Individual-level and community-level effect modifiers of the temperature–mortality relationship in 66 Chinese communities. BMJ Open. 2015;5(9):e009172.
Chan EYY, Goggins WB, Kim JJ, Griffiths SM. A study of intracity variation of temperature-related mortality and socioeconomic status among the Chinese population in Hong Kong. J Epidemiol Community Health. 2012;66(4):322–7.
Wu W, Xiao Y, Li G, Zeng W, Lin H, Rutherford S, Xu Y, Luo Y, Xu X, Chu C. Temperature–mortality relationship in four subtropical Chinese cities: a time-series study using a distributed lag non-linear model. Sci Total Environ. 2013;449(449):355–62.
Zeng W, Li G, Xiao Y, Xu Y, Xu X, Liu T, Luo Y, Xiao J, Ma W. The impact of temperature on cardiovascular disease deaths in 4 cities, China: a time-series study. Chin J Epidemiol. 2012;33(10):1021–5.
Ma X, Li R, Luo K, Zhang R, Wang Z, Xu Q. Association between temperature and mortality in three cities in China. Basic Clin Med. 2016;36(6):805–10.
Chung JY, Honda Y, Hong YC, Pan XC, Guo YL, Kim H. Ambient temperature and mortality: an international study in four capital cities of East Asia. Sci Total Environ. 2009;408(2):390–6.
Hu M, Ma W, Zhang Y, Liu T, Lin H, Luo Y, Xiao J. Relationship between temperature and the risks of mortality in China: a meta-analysis. Chin J Epidemiol. 2013;34(9):922–6.
Moghadamnia MT, Ardalan A, Mesdaghinia A, Keshtkar A, Naddafi K, Yekaninejad MS. Ambient temperature and cardiovascular mortality: a systematic review and meta-analysis. PeerJ. 2017;5(8):e3574.
Zhang Y, Li C, Feng R, Zhu Y, Wu K, Tan X, Ma L. The short-term effect of ambient temperature on mortality in Wuhan, China: a time-series study using a distributed lag non-linear model. Int J Environ Res Public Health. 2016;13(7):722–34.
Goodman PG, Dockery DW, Clancy L. Cause-specific mortality and the extended effects of particulate pollution and temperature exposure. Environ Health Perspect. 2004;112(2):179–85.
Ma W, Zeng W, Zhou M, Wang L, Rutherford S, Lin H, Liu T, Zhang Y, Xiao J, Zhang Y. The short-term effect of heat waves on mortality and its modifiers in China: an analysis from 66 communities. Environ Int. 2015;75:103–9.
Zanobetti A, Oneill MS, Gronlund CJ, Schwartz J. Susceptibility to mortality in weather extremes: effect modification by personal and small-area characteristics. Epidemiology. 2013;24(6):809–19.
Ma W, Yang C, Tan J, Song W, Chen B, Kan H. Modifiers of the temperature-mortality association in Shanghai, China. Int J Biometeorol. 2012;56(1):205–7.
Ryti NRI, Guo Y, Jaakkola JJK. Global association of cold spells and adverse health effects: a systematic review and meta-analysis. Environ Health Perspect. 2016;124(1):12–22.
Yu W, Vaneckova P, Mengersen K, Pan X, Tong S. Is the association between temperature and mortality modified by age, gender and socio-economic status? Sci Total Environ. 2010;408(17):3513–8.
Hajat S, Kovats RS, Lachowycz K. Heat-related and cold-related deaths in England and Wales: who is at risk? J Occup Environ Med. 2007;64(2):93.
Stafoggia M, Forastiere F, Agostini D, Caranci N, De’Donato F, Demaria M, Michelozzi P, Miglio R, Rognoni M, Russo A. Factors affecting in-hospital heat-related mortality: a multi-city case-crossover analysis. J Epidemiol Community Health. 2008;62(3):209–15.
Wang C, Chen R, Kuang X, Duan X, Kan H. Temperature and daily mortality in Suzhou, China: a time series analysis. Sci Total Environ. 2013;466-467(1):985.
Barnett AG. Temperature and cardiovascular deaths in the US elderly: changes over time. Epidemiology. 2007;18(3):369–72.
Reid CE, Oneill MS, Gronlund CJ, Brines SJ, Brown DG, Diezroux AV, Schwartz J. Mapping community determinants of heat vulnerability. Environ Health Perspect. 2009;117(11):1730–6.
O’Neill MS, Ebi KL. Temperature extremes and health: impacts of climate variability and change in the United States. J Occup Environ Med. 2009;51(1):13.
Zeka A, Zanobetti A, Schwartz J. Individual-level modifiers of the effects of particulate matter on daily mortality. Am J Epidemiol. 2006;163(9):849–59.
Kim J, Shin J, Lim YH, Honda Y, Hashizume M, Guo YL, Kan H, Yi S, Kim H. Comprehensive approach to understand the association between diurnal temperature range and mortality in East Asia. Sci Total Environ. 2016;539:313–21.
Shaposhnikov D, Revich B, Gurfinkel Y, Naumova E. The influence of meteorological and geomagnetic factors on acute myocardial infarction and brain stroke in Moscow, Russia. Int J Biometeorol. 2014;58(5):799.
Acknowledgements
We are grateful for the support of National Key R&D Program of China (Grant No: 2018YFA0606200).
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2019 Springer Nature Singapore Pte Ltd.
About this chapter

Cite this chapter
Wang, X. et al. (2019). Ambient Temperature and Mortality in Chinese Population. In: Lin, H., Ma, W., Liu, Q. (eds) Ambient Temperature and Health in China. Springer, Singapore. https://doi.org/10.1007/978-981-13-2583-0_2
Download citation
DOI: https://doi.org/10.1007/978-981-13-2583-0_2
Published:
Publisher Name: Springer, Singapore
Print ISBN: 978-981-13-2582-3
Online ISBN: 978-981-13-2583-0
eBook Packages: MedicineMedicine (R0)