
Abstract
Objective: Patients after cardiac arrest from suffocation (airway obstruction caused by foreign body aspiration) or hanging could not have improved prognoses even after undergoing targeted temperature management (TTM). Therefore, to obtain characteristics of such patients, we retrospectively evaluated patients’ data including other pathologies.
Methods: Sixty patients, who suffered cardiopulmonary arrest inside or outside our hospital from June 2009 to July 2016 and received TTM, were assessed. The patients were classified into the two groups: CPC1–CPC2 and CPC3–CPC5 at hospital discharge for parameter comparisons. JMP7.0 was used for statistical analysis, while the Wilcoxon rank sum test and χ 2 test were used for testing statistical significance.
Results: Among 60 patients receiving TTM, 40 were male and 20 female. The average age was 64. Nine patients had airway obstructions due to foreign body aspiration or hanging, while 51 patients died due to other diseases such as ventricular fibrillation, cardiac infarction, and bronchial asthma. The overall average pH upon arrival was 6.99, while the overall average serum potassium was 4.68 mEq/L. In two cases, the airway obstruction and hanging were witnessed, while four patients received bystander CPR. None of the nine patients with airway obstruction due to foreign body aspiration or hanging was evaluated as CPC1–CPC2, while 16 (31%) out of 51 patients with other diseases were neurologically favorable. All nine patients with airway obstructions were determined as poor outcomes (CPC3–CPC5), while those in the other causes were 35 out of 51 subjects (100 vs. 68%, p = 0.0497).
Discussion: From the results of our hospital, we assume that TTM resulted in no improvements in the outcomes of patients who suffered airway obstruction due to foreign body aspiration or hanging. In general, some facilities do not actively indicate TTM for patients who suffered airway obstructions. However, improved prognoses have been reported in some case reports (“The 53-year-old man who was out-of-hospital asystole recovered without a problem neurologically.” Intern Emerg Med 2009;4:445–7. “A case in which TTM was used successfully in a patient with coma after cardiorespiratory arrest induced by hanging.” Resuscitation 2005;67:143–4. “Neurologically uneventful 2 hanging cases.” Med J Niigata City General Hospital 2015;36(1)), suggesting the need for further accumulation of subjects to select indicated victims for TTM.
Access provided by CONRICYT-eBooks. Download chapter PDF
Similar content being viewed by others


Keywords
- Cardiac arrest due to suffocation/hanging
- TTM (targeted temperature management)
- pH at admission (arrival)
- Bystander CPR
4.1 Introduction
According to the 2015 JRC (Japan Resuscitation Council) guidelines for cardiopulmonary resuscitation, TTM (targeted temperature management) at a temperature level choosing from 32 to 36 °C is recommended for patients in a coma after cardiac arrest. However, the cause of cardiac arrest and the time required for spontaneous circulation to return may possibly affect the outcome. For inpatients after cardiac arrest even without VF/pVT, shockable rhythms (2015 JRC treatment recommendation: We suggest. Level of evidence: very low) are indicated for TTM. However, it is unclear whether TTM should be carried out for outpatients who suffered airway obstruction due to foreign body aspiration or hanging.
4.2 Objective
Patients in a state of post-cardiac arrest due to suffocation or hanging may not have improved prognoses even after undergoing targeted temperature management (TTM). Therefore, to obtain characteristics of such patients, we retrospectively evaluated patients’ data including other pathologies.
4.3 Methods
We retrospectively evaluated 60 patients who suffered cardiopulmonary arrest inside or outside our hospital and received TTM from June 2009 to July 2016. They were divided into the two groups for parameter comparisons: CPC1–CPC2 and CPC3–CPC5 at hospital discharge. JMP7.0 was used for statistical analysis, while the Wilcoxon rank sum test and χ 2 test were used for testing statistical significance. Data were shown in mean ± SD. **Depicted as statistical significance. *CPC cerebral performance categories; outcome of brain-injured patients: the Glasgow-Pittsburgh cerebral performance and overall performance categories.
4.4 Results
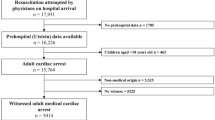
As shown in Fig. 4.1, 40 male and 20 female subjects were included in this study. The classification of diseases is given in Fig. 4.2: patients with acute myocardial infarction made up the majority of 33.3%, while the rate of patients suffered suffocation or hanging was 15%. TTM was carried out in all cases of this study.

TTM was carried out in all cases of this study. The number of males and females are shown

*VSA vasospastic angina. Patients with acute myocardial infarction accounted for the majority, at 33.3%, while 15% suffered suffocation or hanging
Table 4.1 showed the comparisons in parameters between the groups of CPC1–CPC2 and CPC3–CPC5 in all 60 cases. Table 4.2 described the comparison between the groups of suffocation/hanging and cardiac arrests from other origins.
Tables 4.3 and 4.4 demonstrated the demographic data of the suffocating cases (abbreviations: FBO, foreign body obstruction; ROSC, return of spontaneous circulation).
4.5 Case Reports
4.5.1 Case 1. Age: 38 Female Hanging
The patient had been regularly visiting the Department of Psychosomatic Medicine for depression for 10 years. She was found unconscious at home by a family member 5 min after a sound was heard. An emergency service team received a call and transported the patient to hospital in 18 min. With a bystander CPR, adrenaline 2 mg resulted in the resumption of heartbeat. Upon arrival in the ER, light reflex was observed with both pupils having a diameter of 3.5 mm. Her body temperature was 36.4 °C; blood gas analysis showed that pH 6.675, B.E. −25.6 mEq/L, HCO3 13.5 mmol/L, PCO2 118.5 Torr, PO2 62 Torr, and K 6.1 mEq/L. GOT 155 IU/L GPT 185 IU/L. LDH 410 IU/L. CPK 100 IU/L. Her outcome was CPC5 on day 74 after pseudomonas aeruginosa septicemia.
4.5.2 Case 2. Age: 82 Male Foreign Body Aspiration During Alcohol Intoxication
The patient suffered from foreign body aspiration twice, resulting in CAP, followed by a bystander CPR and then was transferred with continued CPR to a hospital by an ambulance. It took 27 min for transportation to the hospital. Upon arrival, no light reflex was observed with pupil diameters of rt. 4 mm/left 5 mm. Upon arrival, his body temperature was 36.9 °C. Blood gas analysis showed that pH 6.915, B.E. −13.9 mEq/L, HCO3 21.4 mmol/L, PCO2 107.8 Torr. PO2 1.2 Torr, K 6.6 mEq/L, GOT 61 IU/L, GPT 34 IU/L, LDH 314 IU/L, and CPK 78 IU/L. Blood ethanol level: 172.0 mg/dL. His outcome was CPC4, eventually, CPC5 with DNAR on day 16.
4.5.3 Case 3. Age: 58 Male Foreign Body Aspiration from During Eating Meat and Alcohol Drinking
The patient had a history of smoking but no particular disease history. While eating and drinking at a steak house, he choked on a piece of meat, resulting in cardiac arrest. He did not receive bystander CPR at the site. At 1:23, PEA was confirmed. At 1:24, his heartbeat resumed after sternal compressions. A 6 cm piece of meat was removed. E1VTM2. Within a period of 24 h, his maximum body temperature was 38.9 °C. It took 24 min for the emergency team to transport the patient to the hospital after receiving the call. Pupil diameter: 1.5 (+)/1.5 (+). Upon arrival, his blood gas analysis showed that pH 6.922, B.E. −17.5 mEq/L, HCO3 17.4 mmol/L, PCO2 86.4 Torr, PO2 250.6 Torr, K 3.2 mEq/L, GOT 46 IU/L, GPT 30 IU/L, LDH 279 IU/L, and CPK 276 IU/L. Blood ethanol concentration was 266.2 mg/dL. His outcome was intractable myoclonic epilepsy being difficult to treat. We could not stop his epileptic seizures using anti-epilepsy medicine alone and could not evaluate his consciousness level accurately for a long time due to the use of sedative agents. He was transferred to another hospital on day 56.
4.5.4 Analysis of Suffocating Cases
The mean ambulance transportation time was 22.8 ± 3.76 min. Two cases were witnessed. The four patients received bystander CPR (Table 4.3). Spontaneous heartbeats in three cases resumed before reaching the hospital (Table 4.4). The average time until ROSC was 34.8 ± 8.53 min. All 9 patients suffering from airway obstruction or hanging were evaluated as poor outcome (CPC3–CPC5), while 16 out of 51 patients showed neurologically favorable outcomes (CPC1–CPC2) (p = 0.0497) (Table 4.1). The cases of hanging were mostly suffering from psychosomatic medical diseases (five cases), while cases of airway obstruction due to foreign body aspiration were those who had drunk a considerable amount of alcohol (three cases). Nielsen et al. [1] showed that there were differences in the TTM management procedures depending on attending physicians in ICU at the time of arrival, and in some cases, it took 30 h to get 34 °C targeted temperature. In our hospital, there is a variety of doctors on shift duty including heart surgeons, cardiologists or nephrologists, which might be a cause of delayed induction for TTM.
4.6 Discussion
The present results suggest that TTM might not be able to improve the outcomes of patients who suffered from airway obstruction due to foreign body aspiration or hanging.
Case 3 in this report had a high fever of 38.9 °C upon arrival. If TTM had been initiated in the early stage, myoclonus epilepsy might not have been so difficult to treat [2,3,4,5,6,7,8]. Possibly it might cause abrupt sympathetic hyperactivity after the insult [9, 10]. In this case, we did not perform TTM because of patient’s family intension. The final prognosis might be influenced by the decision for the treatment by patient families’ intension based on the underlying diseases or explanations of attending physicians. Certain hospitals do not introduce TTM for patients suffering from airway obstruction due to the foreign body aspiration or hanging. However, improved prognoses have been reported in some studies. Murata et al. reported on a 16-year-old boy who suffered incomplete hanging (some part of the body is touching the ground) and cardiac arrest for 18 min without bystander CPR, but eventually he was discharged with CPC2 [11]. His initial rhythm was VF, and his heartbeat was restarted by the defibrillation using AED. Spontaneous respiration regained during transportation. He had GCS 3 upon arrival at the emergency department. Both pupil diameters were 2.5 mm with no light reflex. His body temperature was 34 °C. So, he was undergoing TTM for 24 h at 34 °C and then was rewarmed to 36 °C for 48 h after the insult. From day 24, he had a sustained fever up to 38–39 °C, and consciousness disturbance continued. Since NSAIDs or others were ineffective in decreasing his fever, on day 49, amantadine 150 mg/day was administered for the purpose of activating the patient activity. The patient recovered gradually to a state such that he could look after himself on day 56. Thus, even some cardiac arrest victims after hanging might recover at CPC1 or CPC2. Therefore, in the future, we need to establish the neuromonitoring for evaluating the brain function even in the early phase of post-cardiac arrest for selecting the right victims to be treated.
Ola et al. reported on the outcomes of cases of near hanging treated in two ICUs in Sweden from 2003 to 2006 [12]. Among a total of 13 cases of near hanging, 10 cases did not go into cardiac arrest. Five patients who underwent TTM treatment and all three patients who did not receive TTM were discharged with CPC1–CPC2. Interestingly, only one patient of three subjects in cardiac arrest who received TTM was discharged with CPC1–CPC2. The most important outcome predictors after near hanging were suspension time, depth of coma, and whether or not CA had occurred. The estimated cardiac arrest time of our cases was for 24–56 min (an average duration, 34.8 min). The good recovery case was reported to have a short cardiac arrest time (as described in the paper of Kashif M et al. 15 min [13]) and also with the initial wave form VF (relatively short time expecting with a little damage to the heart), the cases without comorbidities with good overall status. But in the present study, there were no VF forms as the initial wave at the site. The initial wave form VF could be expected to be correlated with a good outcome, so even a hanging case may be an indication of TTM if fulfilled the conditions stated above [12].
Baldursdottir et al. have reported 14 cardiac arrest cases due to hanging and suffocation including carbon monoxide poisoning and drowning. Among them, six cases of cardiac arrests due to hanging underwent TTM: three of the patients were discharged from the hospital at CPC1. The pHs of the patients on admission were 7.31, 7.38, and 7.27, respectively [14].
Jung Hee Wee et al. examined 111 cardiac arrest cases admitted from January 1, 2007 to December 31, 2012. The average age of the patients was 65.8 ± 16.3, with 70.3% of cases suffering cardiac arrest due to clogging of the airway with a foreign body. All patients underwent TTM at 32–34 °C, among 52 patients survived, and 6 of them were discharged with CPC1–CPC2. Light reflex, corneal reflex, and time to ROSC were reportedly to be potential predictors for survival [15].
Min Joung Kim et al. demonstrated that among 159 patients who suffered hanging but were not in cardiac arrest, 12 cases of CPC3–CPC5 did not receive TTM, suggesting that TTM might have led to different results depending on each patient condition. As characteristics of the hanging cases with cardiac arrest who received TTM getting CPC1–CPC2, the authors reported the following: (1) CPR time before hospital transfer was short as approximately 5 min; (2) pH was greater than 7.28; (3) the base excess was higher than −4.7 mEq/L; and (4) HCO3 − was greater than 20.5 mEq/L. pH and HCO3 − could be useful as prognostic predictors; in our study, all cases had a pH less than 7.0 [16].
Two cases of hanging who were not in cardiac arrest were reported. A patient was a 40-year-old male with E1V2M4, and his bladder temperature was 39.0 °C on admission. He received TTM management and was discharged on the 52nd day with CPC1. Although the other patient was discovered in a state of his left foot submerging 2 m under the floor, he was rescued by family members to recover both respiration and circulation when emergency personnel arrived. Upon arrival at the emergency department, the patient was E2V2M4 with an axillary temperature of 36.4 °C and received TTM; eventually he regained his consciousness even before discharge with CPC1 on the 14th day [17].
In some cases, there were actually no cardiac arrests in a group who were thought to have cardiac arrest. According to the home page for citizens by the Japanese Circulation Society (http://www.j-circ.or.jp/cpr/call.html), confirmation of a pulse is not required. It is recommended to compress the chest if there is no consciousness nor respiration. Therefore, some patients who suffered airway obstruction from foreign body aspiration or hanging might not experience cardiac arrest, but cerebral hypoxia could occur, so TTM should not suspend for cases of airway obstruction such from hanging. Patients who do not respond to verbal command after cardiac arrest are indicated for TTM. Cooling starts earlier; less brain damage could be expected [18]. We had a drowned woman of 50s with cardiac arrest: her pH was 6.94, the duration of arrest was approximately 40 min, but her body temperature on arrival was 34.4 °C. After 4 days, she was discharged with CPC1 [19]. In this study, no cases had a body temperature around 34 °C on admission (Table 4.3).
The mechanisms of cardiac arrest due to airway obstruction caused by foreign body aspiration or hanging may vary. Suzutani et al. reported that the mechanisms of cardiac arrest due to hanging are as follows: (1) obstruction of the airway; in typical dead cases by hanging, the base part of the tongue is pushed back and upward and tightly adhered to the posterior pharyngeal wall, resulting in closure of the airway at the pharynx part (external suffocation); (2) obstruction of the cervical blood vessels, wherein the cervical blood vessels are externally compressed by hanging and their lumens are collapsed, blood circulation to the cranial cavity instantaneously stops, and then oxygen deficiency occurs in the brain (internal suffocation); (3) compression of the cervical nerve; and (4) cervical vertebral fracture and transection of the neck or a combination of them. The simultaneous occurrence of (3) and (4) is reported to be rare [20]. In this study, there were no cases involving the mechanism (4). If either (1) or (2) occurs, oxygen is not delivered to the brain. Therefore, they are causes of cardiac arrest due to hypoxic mechanisms. In the current cases whose ROSC could not be obtained, PCO2 levels were over 110 Torr, so it is likely that they are a group of inadequate ventilation.
4.6.1 Study Limitation
This study was a retrospective evaluation at a single facility. One of the causes for cardiac arrest from suffocation and airway obstruction is hypoxemia, while the mechanism of cardiac arrest in hanging cases may be due to internal/external suffocation, cervical nerve compression, or carotid sinus/vagal activations; thus there would be complication. Therefore, it is possible that the mechanisms of cardiac arrest may vary among cases suffering from airway obstruction due to foreign body aspiration or hanging leading to cardiac arrest.
4.7 Conclusions
Patients who suffered from airway obstruction due to foreign body aspiration or hanging without cardiac arrest are reported to mostly recover to CPC1–CPC2. However, in some cases on arrival, it is difficult to determine whether such patients did have cardiac arrest or not. In such situation, pH upon arrival, at least in part, might offer information regarding the possibility of cardiac arrest, thereby potentially predicting prognoses. TTM might have reduced brain damage after cardiac arrest due to suffocation mechanisms. However, since there has been very limited evidence, we could neither recommend nor refute TTM for post-cardiac arrest patients after suffocation. Therefore, we need to accumulate more data and elaborate to allow us to determine subjects who would recover to neurologically favorable outcomes.
References
Nielsen N, et al. Targeted temperature management at 33°C versus 36°C after cardiac arrest. N Engl J Med. 2013;369(23):2197–206.
Liu Z, et al. Effect of temperature on kainic acid-induced seizures. Brain Res. 1993;17(631):51–8.
Jiang W, et al. The neuropathology of hyperthermic seizures in the rat. Epilepsia. 1999;40:5–19.
Lundgren J, et al. Hyperthermia aggravates and hypothermia ameliorates epileptic brain damage. Exp Brain Res. 1994;99:43–55.
Wang Y, et al. Hypothermia reduces brain edema, spontaneous recurrent seizure attack, and learning memory deficits in the kainic acid treated rats. CNS Neurosci Ther. 2011;17:271–80.
Maeda T, et al. Effect of hypothermia on kainic acid-induced limbic seizures: an electro-encephalographic and 14C-deoxyglucose autoradiographic study. Brain Res. 1999;13(818):228–35.
Schmitt FC, et al. Anticonvulsant properties of hypothermia in experimental status epilep-ticus. Neurobiol Dis. 2006;23:689–96.
Kowski AB, et al. Deep hypothermia terminates status epilepticus—an experimental study. Brain Res. 2012;29(1446):119–26.
Rabinstein AA. Paroxysmal sympathetic hyperactivity in the neurological intensive care unit. Neurol Res. 2007;29:680–2.
Perkes I, Baguley IJ, Nott MT, et al. A review of paroxysmal sympathetic hyperactivity after acquired brain injury. Ann Neurol. 2010;68:126–35.
Murata Y, et al. A patient who received amantadine for consciousness disturbance after cardiac arrest/heartbeat resumption by hanging. Jpn Soc Intensive Care Med. 2015;22:536–9.
Borgquist O, et al. Therapeutic hypothermia for comatose survivors after near-hanging-a retrospective analysis. Resuscitation. 2009;80(2):210–2.
Kashif M, et al. Early recognition of foreign body aspiration as the cause of cardiac arrest. Case Rep Crit Care. 2016;2016:1329234.
Baldursdottir S, et al. Induced hypothermia in comatose survivors of asphyxia: a case series of 14 consecutive cases. Acta Anaesthesiol Scand. 2010;54(7):821–6.
Wee JH, et al. Outcomes of asphyxia cardiac arrest patients who were treated with therapeutic hypothermia: a multicentre retrospective cohort study. Resuscitation. 2015;89:81–5.
Kim MJ, et al. Neurologic outcome of comatose survivors after hanging: a retrospective multicenter study. Am J Emerg Med. 2016;34(8):1467–72.
Aso Y. Two cases of hanging who got back into society. Med J Niigata City General Hospital. 2015;36(1):86–7.
Brian EG, et al. Targeted temperature management after out-of-hospital cardiac arrest: who, when, why, and how? Can Fam Physician. 2015;61(2):129–34.
Nagama M, et al. A patient who drowned at sea and suffered hypothermia with bystander CPR but was able to re-enter society without aftereffects. Jpn Assoc Acute Med. 2017:170.
Suzutani T. Discussion on the mechanisms and causes of death by hanging. Hokkaido J Med Sci. 1982;57(5):642–8.
Acknowledgments
The authors have no conflicts of interest directly relevant to the content of this article.
Author information
Authors and Affiliations
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2018 Springer Nature Singapore Pte Ltd.
About this chapter

Cite this chapter
Sakuda, Y., Nagama, M., Yamauchi, S., Iraha, T., Kinjoh, K., Sakugawa, K. (2018). Indications for Targeted Temperature Management in Patients After Choking or Suicide Hanging. In: Aibiki, M., Yamashita, S. (eds) A Perspective on Post-Cardiac Arrest Syndrome. Springer, Singapore. https://doi.org/10.1007/978-981-13-1099-7_4
Download citation
DOI: https://doi.org/10.1007/978-981-13-1099-7_4
Published:
Publisher Name: Springer, Singapore
Print ISBN: 978-981-13-1098-0
Online ISBN: 978-981-13-1099-7
eBook Packages: MedicineMedicine (R0)