
Abstract
The current guidelines emphasize that early prognostication of outcome is an essential component of post-cardiac arrest care. Lactate has been studied as an indicator of critical illness severity. Several studies reported that initial lactate level obtained immediately after hospital arrival was an independent predictor of survival and neurological outcomes in patients with post-cardiac arrest syndrome (PCAS). Recent studies also described that serial lactate measurements in early after-hospital admission could be more useful than a single lactate measurement as a predictor of outcome in those patients. Thus, we conducted an ad hoc analysis of the prospective, multicenter observational study to test the hypothesis that early lactate reduction within 6 h after admission could be a prognostic factor for the outcomes in PCAS. Among the eligible patients (n = 1482), the overall 30-day proportions for survival and good neurological outcome were 29.7% and 16.7%, respectively. Among the study patients, there were significant differences in age, ROSC prior to hospital arrival, epinephrine usage during ACLS, mechanical circulatory support, therapeutic hypothermia, and lactate levels at 0 and 6 h among the lactate clearance quartiles. Of note, patients in the quartile 4 group had the highest initial lactate level. Multivariate logistic regression analyses showed that lactate clearance quartile was an independent predictor of the 30-day survival and good neurologic outcome. In the Cox proportional hazards model, the frequency of mortality during 30 days was markedly higher for patients with lactate clearance in the 1st (hazard ratio, 3.12; 95% CI, 2.14–4.53), 2nd (2.13; 1.46–3.11), and 3rd quartile (1.49; 1.01–2.19) than those in the 4th quartile. In summary, effective lactate reduction over the first 6 h of post-cardiac arrest care was associated with survival and good neurologic outcome independent of the initial lactate level.
Access provided by CONRICYT-eBooks. Download chapter PDF
Similar content being viewed by others

Keywords
3.1 Introduction
Sudden cardiac arrest is one of the leading causes of death worldwide [1]. Despite advances in the management of cardiac arrest patients, improvement in the rates of survival to hospital discharge has been extremely limited, and more than half of the survivors exhibit lasting neurologic deficits [2, 3]. The current guidelines emphasize that early prognostication of outcome is an essential component of post-cardiac arrest care [4]. Early and accurate prediction of cardiac arrest outcome can help clinicians and families to make a better-informed decision for the patient’s healthcare. Thus, the main objective of predictive test of survivors with PCAS immediately after return of spontaneous resuscitation (ROSC) is to establish the survival to discharge with intact neurological function [5].
3.2 Pathophysiology and Current Treatment for Post–Cardiac Arrest Syndrome
The PCAS is characterized as systemic illness from ischemic-reperfusion injury combined with the pathophysiologic derangements. The greatest proportion of post-cardiac arrest mortality and morbidity is caused by global ischemic brain injury [6]. The pathophysiological mechanisms responsible for brain injury after ROSC include excitotoxicity, free radical formation, pathological activation of proteases, and cell death signaling [2, 7]. Managements for PCAS patients include optimizing oxygenation and organ perfusion, targeted temperature management (TTM), and treating the underlying etiology of arrest. Current guidelines regarding PCAS management recommend measuring serial lactate levels in postarrest patients to ensure adequate perfusion, based on evidence from other diseases such as sepsis [4].
3.3 Prognostication After Cardiac Arrest
Early and accurate prognostication after cardiac arrest can help with the optimal management after hospital admission for patients with PCAS and minimize related emotional and financial costs for their families. Over the last few decades, several studies have shown the utility of several prognostic tools of PCAS outcome, such as clinical examination, biochemical markers, electrophysiological testing, and neuroimaging. Clinical findings such as the absence of motor response, presence of myoclonus status epilepticus, and lack of brainstem reflexes have been widely used for the prognostication after successful CPR. Blood biomarkers (e.g., neuron-specific enolase [NSE] and soluble 100-β protein) are useful for coma prognostication, but results vary among commercial laboratory assays, and applying one single cutoff level for poor prognostication is not recommended. Electroencephalogram monitoring after resuscitation can contribute to the prediction of both good and poor neurological outcome. Neuroimaging tests such as computer tomography (CT) (e.g., the loss of distinction between gray and white matter), position emission tomography (PET) (e.g., reduced glucose metabolism), and diffusion MRI are emerging as promising tools for prognostication. However their precise roles need further study. This multimodal approach might offer the best outcome predictive performance for prognostication of comatose survivors from PCAS [8].
3.4 Role of Lactate Metabolism in Cellular Stress and Recovery
In the critical care setting, lactate is frequently measured in several diseases, usually with the goal of detecting tissue hypoxia. Lactate is a crucial metabolite in the glycolysis and oxidative phosphorylation. Under stable conditions, glycolysis and oxidative phosphorylation steadily metabolize glucose. Because the rate of glycolysis can increase two to three times faster than oxidative phosphorylation, glycolysis can quickly provide far more adenosine triphosphate (ATP). Excess pyruvate will rapidly accumulate and is converted to lactate in order for glycolysis to proceed. Under recovery conditions, lactate is diverted into pyruvate. These reactions (both directions) are catalyzed by the lactate dehydrogenase (LDH). Thus, LDH catalyzes the conversion of lactate to pyruvic acid and back, as it converts NAD+ to NADH and back (Fig. 3.1). When rapidly large amounts of energy are required, such as under circumstances of cellular stress, lactate serves as a critical buffer that allows glycolysis to accelerate.

Metabolic pathways of Pyruvate/Lactate. PFK phosphofructokinase; F-1,6-BP fructose 1,6-bisphosphate; NADH nicotinamide adenine dinucleotide; LDH lactate dehydrogenase; PDH pyruvate dehydrogenase
Increased lactate levels may represent tissue hypoxia, accelerated aerobic glycolysis driven by excess adrenergic stimulation, or decreased clearance due to hepatic dysfunction. Several experimental studies have confirmed the relationship between the production of lactate and tissue hypoxia by reducing the components of systemic oxygen delivery (cardiac output, oxygen saturation, and hemoglobin level) until the extraction of oxygen can no longer maintain oxygen availability to the cells to meet their demands [9, 10]. When oxygen delivery reduced at a critical level, oxygen consumption becomes limited by oxygen delivery with the concomitant increase of blood lactate levels. In an experimental study of cardiac tamponade by Zhang and colleagues [10], it was demonstrated that resolution of the supply-dependent state of oxygen consumption by resolving the tamponade was associated with an increment of oxygen consumption to baseline levels and normalization of lactate levels. Moreover, impaired aerobic metabolism and aggravation of oxidative stress caused by mitochondrial dysfunction have been implicated as causes of neurological deficits following cardiac arrest [11,12,13]. Pyruvate dehydrogenase (PDH) is the critical rate-limiting mitochondrial matrix enzyme linking glycolysis to the tricarboxylic acid (TCA) cycle. PDH is inhibited stimulated by NADH and acetyl-CoA. (Fig. 3.1). In tissue hypoxia, lactate is overproduced and underutilized as a result of impaired mitochondrial oxidation. Even if systemic oxygen delivery recovers to normal range, microcirculatory dysfunction can cause tissue hypoxia and hyperlactatemia. Hyperoxia-induced oxidative inactivation of PDH has been suggested as a culprit in the loss of cerebral aerobic metabolism and neurological deficit after cardiac arrest [11, 14]. Although there are still ongoing discussions, a recent science has focused on the presence of mitochondrial dysfunction in critically ill that could limit pyruvate metabolism (and thus increase lactate levels) in the absence of limited oxygen availability [15, 16].
3.5 Role of Lactate in the Critical Care Setting
Blood lactate concentration is generally recognized as a hemodynamic indicator and target for resuscitation in the critically ill for decades. In several critical illnesses, increased blood lactate levels have been related to morbidity and mortality. The measurement of lactate levels both in the emergency department and in the ICU is shown to be helpful for risk stratification [17]. In addition, Jansen and colleagues demonstrated that the duration and area under the curve of increased lactate levels are related to both morbidity and mortality in heterogeneous intensive care unit patients [18]. Several clinical conditions have been associated with impaired clearance of lactate. Nguyen and colleagues showed a significant association between lactate clearance and biomarkers of pro- and anti-inflammation, coagulation, apoptosis, and further with multiorgan dysfunction and mortality in severe sepsis and septic shock [19]. Also, lactate clearance has been shown to be impaired in patients with liver dysfunction [20] and after cardiac surgery [21]. A body of evidence suggests that global tissue hypoxia plays a crucial role in the complex mechanisms leading to the endothelial response in severe sepsis and septic shock rather than a terminal event. Further, given the well-established relationship with the inadequate tissue oxygenation and with morbidity and mortality, lactate levels could represent a useful goal of initial resuscitation in many clinical conditions.
3.6 Lactate Levels After Successful Resuscitation from Cardiac Arrest
Circulatory arrest and the hypocirculatory state during cardiopulmonary resuscitation (CPR) can contribute to lactic acidosis. Oxygen deficiency leads to anaerobic metabolism and therefore to lactate overproduction. Concurrently, the impaired liver function due to profound ischemia state results in reduced lactate clearance [22]. Carden and colleagues reported in detail the time course of linear increase in blood lactate level during CPR in an animal cardiac arrest model, suggesting that delayed ROSC and/or poor quality of CPR may lead to an increased blood lactate concentration [23]. Decrease in lactate is a surrogate marker for adequate tissue perfusion after ROSC and potentially serves as an endpoint for resuscitation. Two retrospective studies have demonstrated that effective clearance was associated with decreased mortality [24, 25]. Starodub and colleagues measured lactate levels at time of hospital admission and 12 and 24 h after ROSC in PCAS patients treated with therapeutic hypothermia [26]. They observed no difference in initial lactate levels between survivors and nonsurvivors; however, lactate levels at 12 and 24 h after ROSC were significantly lower in survivors. Donnino and colleagues reported that lower lactate levels at 0, 12, and 24 h as well as a greater lactate reduction at 12 h were associated with improved survival and good neurologic outcomes in patients with PCAS in a four-center prospective observational study [27]. Furthermore, Ikeda and colleagues have demonstrated that pyruvate dehydrogenase (PDH) activity was markedly depressed in post-cardiac arrest patients [28]. Taken together, it is reasonable to hypothesize that effective lactate reduction early after hospital admission can be a prognostic factor for outcomes and a target for resuscitation in PCAS patients.
3.7 Can Early Lactate Clearance Predict the Outcomes in Patients with PCAS?
Based on the abovementioned backgrounds, we sought to verify the hypothesis that early lactate reduction is a prognostic factor for outcomes and a target for resuscitation in PCAS patients. To determine whether early lactate reduction during PCAS care can be associated with improved survival and good neurologic outcome at 30 days after ROSC in patients who suffered OHCA, we conducted an ad hoc data analysis of a prospective, multicenter observational study [29].
3.7.1 Study Design and Settings
We performed the survey of survivors after OHCA in the Kanto area, including the Tokyo Prefecture of Japan in 2012 (SOS-KANTO 2012 study). Briefly, SOS-KANTO study was a prospective, multicenter observational study consisting of 16,452 patients who suffered OHCA and were transported to the 67 emergency hospitals by emergency medical service (EMS) personnel between January 2012 and March 2013.
The inclusion criteria of the present study were (1) hospital admission after achieving ROSC and (2) lack of severe disability as activities of daily living before cardiac arrest. The exclusion criteria were (1) admission to hospitals where the frequency of serial lactate measurements after ICU admission was less than 20%, (2) age was less than 18 years, and (3) cardiac arrest was caused by the following diseases: acute aortic dissection/rupture, subarachnoid hemorrhage, and obvious exogenous factor including trauma, burn, asphyxia, drowning, accidental hypothermia, and drug overdose, because these can affect liver metabolism and/or hypoxic mechanism and production and clearance of lactate.
The primary endpoint was 30-day survival, and the secondary endpoint was good neurologic outcome 30 days after cardiac arrest. The cerebral performance category (CPC) scale was used to categorize neurologic outcomes: CPC 1, good performance; CPC 2, moderate disability; CPC 3, severe disability; CPC 4, comatose or persistent vegetative status; and CPC 5, brain death or death. CPC 1 and 2 were defined as good neurologic recovery. CPC scores were further dichotomized into good (CPC 1 or 2) and poor (CPC 3, 4, or 5) outcomes. To collect 1-month follow-up data, the institutional researchers collected inhospital information including survival and neurologic outcome. If the patients were discharged from the hospitals or transferred out to rehabilitation hospitals, the institutional researchers collected the information by phone.
3.7.2 Definition of Early Lactate Clearance
Early lactate clearance was defined as the percent change in lactate level 6 h after a baseline measurement. It was calculated using the following formula: lactate at hospital admission (hour 0) minus lactate at hour 6, divided by lactate at hospital admission (hour 0), which is then multiplied by 100. A positive value denotes a decrease or clearance of lactate, whereas a negative value denotes an increase in lactate after 6 h of intervention.
3.7.3 Data Collection
Pre- and inhospital data were prospectively collected. Prehospital information was collected by EMS providers and included age, sex, preadmission functional status, witness status, presence of bystander CPR, location of cardiac arrest, cause of cardiac arrest (coded as cardiogenic or noncardiogenic), initial cardiac rhythm, airway management by EMS personnel, prehospital automated external defibrillator (AED) attempt, time interval from EMS call to arrival at the hospital, and achievement of ROSC prior to hospital arrival. The inhospital information was collected by institutional researchers: ROSC subsequent to arrival at the hospital, hospital admission, laboratory data obtained immediately after hospital arrival, medications and post-resuscitation treatment, duration of hospital stay, and neurologic outcome at 30 days after CA. Post-resuscitation interventions included therapeutic hypothermia, renal replacement therapy, and mechanical circulatory support. In this SOS-KANTO 2012 study, physicians were encouraged to measure lactate levels at 0 and 6 h if they deemed it appropriate in each individual case.
3.7.4 Statistical Analyses
Distributions of continuous variables were compared and evaluated with the use of the t-test (or analysis of variance). The chi-square test or Fisher exact test was used for comparisons of binary variables. The linear trend across the levels of a variable was tested by the Cochran-Armitage trend test. The study population was sorted by increasing lactate clearance values and divided into four groups by lactate clearance quartiles (Table 3.1). For primary analyses, multivariate logistic regressions were used for adjusting selected covariates to assess the associations between lactate clearance quartiles and primary and secondary outcomes. Independent variables were selected as follows: lactate clearance quartiles, lactate concentration at hospital admission, age, sex, witness status, CPR initiated by bystander, initial shockable rhythm, cardiac etiology, airway management by EMS, AED attempted by EMS, time interval from EMS call to hospital arrival, ROSC achieved prior to hospital arrival, epinephrine usage during advanced cardiovascular life support (ACLS), and treatments after hospital admission including therapeutic hypothermia, mechanical circulatory support, renal replacement therapy, steroids usage, anticonvulsants usage, and antipyretics usage. Receiver operating characteristic (ROC) curve analyses were performed for evaluating the accuracy of lactate clearance in differentiating between survivors and nonsurvivors at 30 days. The area under curves (AUCs) in the ROC and their 95% CIs was calculated.
As a secondary analysis, the Kaplan-Meier method and logrank tests were used to compare the four lactate clearance quartiles. The Cox proportional hazards regression model was used to investigate whether lactate clearance was associated with all-cause death. All abovementioned covariates were included in the model.
All statistical tests used a significance level of 0.05 and were two-sided. All data were analyzed with SPSS version 23.0 (SPSS, Chicago, IL).
3.8 Results
3.8.1 Characteristics of Study Patients
The study flowchart is presented in Fig. 3.2. A total of 16,452 OHCA patients were identified during the study period. Of those, 1482 PCAS patients were eligible according to the inclusion criteria. The overall 30-day survival proportion and good neurologic outcome were 29.7% and 16.7%, respectively. After excluding 409 patients had data missing for mandatory elements which were included in the multivariate regression model; 543 PCAS patients were included in the final analyses (Fig. 3.2). Table 3.1 shows the characteristics by lactate clearance quartile. The lactate clearance quartiles were − 23.0% ± 69.0%, 41.6% ± 10.2%, 67.1% ± 5.4%, and 84.2% ± 5.0%, respectively. There were significant differences in age, ROSC prior to hospital arrival, epinephrine usage during ACLS, mechanical circulatory support, therapeutic hypothermia, and lactate levels at 0 and 6 h among the lactate clearance quartiles (Table 3.1). The distribution of lactate clearance is shown in Fig. 3.3. Among the final analyzed patients, the 30-day survival was observed in 256 of 543 patients (47.1%) and good neurologic outcome in 149 of 543 patients (27.4%).

Patient selection. AA rupture acute aortic rupture; AAD acute aortic dissection; ACLS advanced cardiovascular life support; AED automated external defibrillator; AHT accidental hypothermia; CA cardiac arrest; EMS emergency medical service; SAH subarachnoid hemorrhage; VT/VT ventricular fibrillation and pulseless ventricular tachycardia

Distribution of early lactate clearance among survivors and non-survivors
3.8.2 Early Lactate Clearance Is Associated with Improved Outcomes in Patients with PCAS
The increasing lactate clearance is significantly associated with the increasing survival proportion (quartile 1, 29.4%; quartile 2, 42.6%; quartile 3, 51.5%; quartile 4, 65.2%; Cochran-Armitage trend test, p < 0.001) (Fig. 3.4). Multivariate analysis showed that lactate clearance in quartiles 3 and 4 was an independent predictor of survival (Table 3.2). Similarly, a significant trend was found for a good neurologic outcome with increasing lactate clearances (quartile 1, 14.0%; quartile 2, 30.1%; quartile 3, 32.4%; quartile 4, 33.3%; Cochran-Armitage trend test, p < 0.001) (Fig. 3.5). Multivariate analysis revealed that lactate clearances were significant predictors of good neurologic outcome (Table 3.3).

Association between the quartiles of lactate clearance and the 30-day survival proportion after cardiac arrest and successful cardiopulmonary resuscitation

Association between the quartiles of lactate clearance and the proportion of 30-day good neurologic outcome after cardiac arrest and successful cardiopulmonary resuscitation
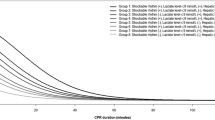
The Kaplan-Meier survival analysis showed a survival benefit during 30 days for patients in the higher lactate clearance quartiles (logrank test, p < 0.001) (Fig. 3.6). In the Cox proportional hazards regression model, the cumulative proportional hazards were significantly higher for patients with lactate clearance in the 1st (hazard ratio [HR], 3.12; 95% CI, 2.14–4.53; p < 0.001), 2nd (HR, 2.13; 95% CI, 1.46–3.11; p < 0.001), and 3rd (HR, 1.49; 95% CI, 1.01–2.19; p = 0.04) than those with lactate clearance in the 4th quartile (Fig. 3.7).

The Kaplan-Meier analysis based on lactate clearance quartile (Q; log-rank test; p < 0.001). *p < 0.001 vs. Q1, †p < 0.05 vs. Q2, ‡p < 0.001 vs. Q3, §p < 0.01 vs. Q1

The Cox proportional hazards model of mortality during follow-up according to the quartiles of early lactate clearance. HR hazard ratio
In a receiver operating characteristic (ROC) analysis, the area under the curve (AUC) revealed that lactate clearance cutoff of 51.8% provided optimal sensitivity and specificity for predicting 30-day survival (AUC, 0.65; 95% CI, 0.60–0.70; sensitivity, 67.2%; specificity, 57.1%).
In summary, our study suggested that effective lactate clearance within the first 6 h during post-cardiac arrest management was significantly associated with survival and good neurologic outcomes in patients with PCAS independently of initial lactate concentration [29]. Our results also provide evidence that the design and interpretation of future clinical studies should consider the early stages of post-cardiac arrest care. Further research is required to clarify the mechanisms underlying the role of lactate and its clearance, such as the complex interaction between increased removal, decreased production, and lactate dilution.
3.8.3 Limitation of this Study
There were several limitations in this study. First, 63.4% (939/1482) of the eligible patients had missing data, resulting in a reduced statistical power. Given that patients with data missing had an older age, a lower proportion of initial shockable rhythm, cardiac etiology, and received substantial treatments after ICU admission, it is possible that mortality within 6 h after admission led to a lack of lactate measurement at 6 h in these patients and that the role of lactate clearance could be limited to some patients with a good prognosis. It is conceivable that the use of lactate clearance might be applicable to a population of successfully resuscitated adult patients with nontraumatic OHCA. Second, healthcare providers were not blinded to clinical lactate measurements; therefore, care might have been altered based on the available data. Third, we could not obtain clinical data related to the causes of hyperlactatemia. Lactate clearance might be affected by underlying comorbidities such as sepsis, liver disease, and acute/chronic kidney injury in patients. Finally, as with any observational study, the association between effective lactate reduction and good outcomes does not necessarily prove causality and might be confounded by unmeasured factors.
3.9 Conclusions
Greater percentage of lactate reduction within 6 h after admission is associated with improved survival and good neurological outcome in patients with PCAS. Although the early lactate clearance during post-CA care as a target of resuscitation warrants further research, the serial measurement of blood early after admission can be a promising tool for prognostication and should be included in the routine management in patients with PCAS.
References
Field JM, Hazinski MF, Sayre MR, Chameides L, Schexnayder SM, Hemphill R, Samson RA, Kattwinkel J, Berg RA, Bhanji F, Cave DM, Jauch EC, Kudenchuk PJ, Neumar RW, Peberdy MA, Perlman JM, Sinz E, Travers AH, Berg MD, Billi JE, Eigel B, Hickey RW, Kleinman ME, Link MS, Morrison LJ, O’Connor RE, Shuster M, Callaway CW, Cucchiara B, Ferguson JD, Rea TD, Vanden Hoek TL. Part 1: executive summary: 2010 American Heart Association guidelines for cardiopulmonary resuscitation and emergency cardiovascular care. Circulation. 2010;122:S640–56.
Neumar RW, Nolan JP, Adrie C, Aibiki M, Berg RA, Bottiger BW, Callaway C, Clark RS, Geocadin RG, Jauch EC, Kern KB, Laurent I, Longstreth WT Jr, Merchant RM, Morley P, Morrison LJ, Nadkarni V, Peberdy MA, Rivers EP, Rodriguez-Nunez A, Sellke FW, Spaulding C, Sunde K, Vanden Hoek T. Post-cardiac arrest syndrome: epidemiology, pathophysiology, treatment, and prognostication. A consensus statement from the International Liaison Committee on Resuscitation (American Heart Association, Australian and New Zealand Council on Resuscitation, European Resuscitation Council, Heart and Stroke Foundation of Canada, InterAmerican Heart Foundation, Resuscitation Council of Asia, and the Resuscitation Council of Southern Africa); the American Heart Association Emergency Cardiovascular Care Committee; the Council on Cardiovascular Surgery and Anesthesia; the Council on Cardiopulmonary, Perioperative, and Critical Care; the Council on Clinical Cardiology; and the Stroke Council. Circulation. 2008;118:2452–83.
Nichol G, Thomas E, Callaway CW, Hedges J, Powell JL, Aufderheide TP, Rea T, Lowe R, Brown T, Dreyer J, Davis D, Idris A, Stiell I. Regional variation in out-of-hospital cardiac arrest incidence and outcome. JAMA. 2008;300:1423–31.
Callaway CW, Donnino MW, Fink EL, et al. Part 8: post-cardiac arrest care: 2015 American Heart Association guidelines update for cardiopulmonary resuscitation and emergency cardiovascular care. Circulation. 2015;132:S465–82.
Becker LB, Aufderheide TP, Geocadin RG, Callaway CW, Lazar RM, Donnino MW, Nadkarni VM, Abella BS, Adrie C, Berg RA, Merchant RM, O’Connor RE, Meltzer DO, Holm MB, Longstreth WT, Halperin HR. Primary outcomes for resuscitation science studies: a consensus statement from the American Heart Association. Circulation. 2011;124:2158–77.
Laver S, Farrow C, Turner D, Nolan J. Mode of death after admission to an intensive care unit following cardiac arrest. Intensive Care Med. 2004 Nov;30(11):2126–8.
Neumar RW. Molecular mechanisms of ischemic neuronal injury. Ann Emerg Med. 2000;36(5):483–506.
Asgari S, Moshirvaziri H, Scalzo F, Ramezan-Arab N. Quantitative measures of EEG for prediction of outcome in cardiac arrest subjects treated with hypothermia: a literature review. J Clin Monit Comput. 2018. https://doi.org/10.1007/s10877-018-0118-3. [Epub ahead of print].
Cain SM. Appearance of excess lactate in anesthetized dogs during anemic and hypoxic hypoxia. Am J Phys. 1965;3:604–8.
Zhang H, Vincent JL. Oxygen extraction is altered by endotoxin during tamponade-induced stagnant hypoxia in the dog. Circ Shock. 1993;3(3):168–76.
Boaert Y, Sheu K, Hof P, et al. Neuronal subclass-selective loss of pyruvate dehydrogenase immunoreactivity following canine cardiac arrest and resuscitation. Exp Neurol. 2000;161:115–26.
Vaagenes P, Ginsberg M, Ebmeyer U. Cerebral resuscitation from cardiac arrest: pathophysiologic mechanisms. Crit Care Med. 1996;24:S57–68.
Pulsinelli W, Levy D, Duffy T. Regional cerebral blood flow and glucose metabolism following transient forebrain ischemia. Ann Neurol. 1982;11:499–502.
Zaidan E, Sims N. Selective reductions in the activity of the PDH complex in mitochondria isolated from brain subregions following forebrain ischemia in rats. J Cereb Blood Flow Metab. 1993;13:98–104.
Brealey D, Brand M, Hargreaves I, Heales S, Land J, Smolenski R, Davies NA, Cooper CE, Singer M. Association between mitochondrial dysfunction and severity and outcome of septic shock. Lancet. 2002;360(9328):219–23.
Crouser ED, Julian MW, Blaho DV, Pfeiffer DR. Endotoxin-induced mitochondrial damage correlates with impaired respiratory activity. Crit Care Med. 2002;30(2):276–84.
Jansen TC, van Bommel J, Bakker J. Blood lactate monitoring in critically ill patients: a systematic health technology assessment. Crit Care Med. 2009;37(10):2827–39.
Jansen TC, van Bommel J, Woodward R, Mulder PG, Bakker J. Association between blood lactate levels, sequential organ failure assessment subscores, and 28-day mortality during early and late intensive care unit stay: a retrospective observational study. Crit Care Med. 2009;37(8):2369–74.
Nguyen HB1, Loomba M, Yang JJ, Jacobsen G, Shah K, Otero RM, Suarez A, Parekh H, Jaehne A, Rivers EP. Early lactate clearance is associated with biomarkers of inflammation, coagulation, apoptosis, organ dysfunction and mortality in severe sepsis and septic shock. J Inflamm. 2010;7:6. https://doi.org/10.1186/1476-9255-7-6.
Almenoff PL, Leavy J, Weil MH, Goldberg NB, Vega D, Rackow EC. Prolongation of the half-life of lactate after maximal exercise in patients with hepatic dysfunction. Crit Care Med. 1989;3(9):870–3.
Mustafa I, Roth H, Hanafiah A, Hakim T, Anwar M, Siregar E, Leverve XM. Effect of cardiopulmonary bypass on lactate metabolism. Intensive Care Med. 2003;3(8):1279–85.
Teasdale G, Jennett B. Assessment of coma and impaired consciousness: a practical scale. Lancet. 1974;2:81–4.
Carden DL, Martin GB, Nowak RM, Foreback CC, Tomlanovich MC. Lactic acidosis during closed-chest CPR in dogs. Ann Emerg Med. 1987;16:1317–20.
Kliegel A, Losert H, Sterz F, et al. Serial lactate determinations for prediction of outcome after cardiac arrest. Medicine. 2004;83(5):274–9.
Donnino MW, Miller J, Goyal N, et al. Effective lactate clearance is associated with improved outcome in post-cardiac arrest patients. Resuscitation. 2007;75(2):229–34.
Starodub R, Abella BS, Grossestreuer AV, et al. Association of serum lactate and survival outcomes in patients undergoing therapeutic hypothermia after cardiac arrest. Resuscitation. 2013;84:1078–82.
Donnino MW, Andersen LW, Giberson T, et al. National Post-Arrest Research Consortium: initial lactate and lactate change in postcardiac arrest: a multicenter validation study. Crit Care Med. 2014;42:1804–11.
Ikeda K, Liu X, Kida K, Marutani E, Hirai S, Sakaguchi M, Andersen LW, Bagchi A, Cocchi MN, Berg KM, Ichinose F, Donnino MW. Thiamine as a neuroprotective agent after cardiac arrest. Resuscitation. 2016;105:138–44. https://doi.org/10.1016/j.resuscitation.2016.04.024. Epub 2016 May 13.
Hayashida K, Suzuki M, Yonemoto N, Hori S, Tamura T, Sakurai A, Tahara Y, Nagao K, Yaguchi A, Morimura N, SOS-KANTO 2012 Study Group. Early lactate clearance is associated with improved outcomes in patients with Postcardiac arrest syndrome: a prospective, multicenter observational study (SOS-KANTO 2012 study). Crit Care Med. 2017;45(6):e559–66.
Author information
Authors and Affiliations
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2018 Springer Nature Singapore Pte Ltd.
About this chapter

Cite this chapter
Hayashida, K. (2018). Prognostic Value of Early Lactate Clearance in Patients with Post-Cardiac Arrest Syndrome. In: Aibiki, M., Yamashita, S. (eds) A Perspective on Post-Cardiac Arrest Syndrome. Springer, Singapore. https://doi.org/10.1007/978-981-13-1099-7_3
Download citation
DOI: https://doi.org/10.1007/978-981-13-1099-7_3
Published:
Publisher Name: Springer, Singapore
Print ISBN: 978-981-13-1098-0
Online ISBN: 978-981-13-1099-7
eBook Packages: MedicineMedicine (R0)