
Abstract
Among cardiac interstitial cells, the recently described telocytes (TCs) display the unique ability to build a supportive three-dimensional network formed by their very long and thin prolongations named telopodes. Cardiac TCs are increasingly regarded as pivotal regulators in intercellular signaling with multiple cell types, such as cardiomyocytes, stem/progenitor cells, microvessels, nerve endings, fibroblasts and immune cells, thus converting the cardiac stromal compartment into an integrated system that may drive either heart development or maintenance of cardiac homeostasis in post-natal life. Besides direct intercellular communications between TCs and neighboring cells, different types of TC-released extracellular vesicles (EVs), namely exosomes, ectosomes and multivesicular cargos, may act as shuttles for paracrine molecular signal exchange between cardiac TCs and cardiomyocytes or putative cardiomyocyte progenitors. In this review, we summarize the recent research findings on cardiac TCs and their EVs. We first provide an overview of the general features of TCs, including their peculiar morphological traits and immunophenotypes, intercellular signaling mechanisms and possible functional roles. Thereafter, we describe the distribution of TCs in normal and diseased hearts, as well as their role as intercellular communicators via the release of exosomes and other types of EVs. Finally, the involvement of cardiac TCs in cardiovascular diseases and the potential utility of TC transplantation and TC-derived exosomes in cardiac regeneration and repair are discussed.
Access provided by CONRICYT-eBooks. Download chapter PDF
Similar content being viewed by others


Keywords
1 Introduction
Intercellular crosstalk is essential to survival and maintenance of tissue and organ homeostasis within a multicellular system [1]. The communication between living cells may occur by different modalities, which include either intercellular contacts, such as adhesion molecules, gap junctions and nanotubes, or the exchange of a variety of cell-released factors including cytokines, growth factors and hormones acting in an autocrine, paracrine, or endocrine manner [2].
Of note, an additional intercellular signaling mechanism that can act over both short and long distances has recently emerged, based on the release and uptake of membrane-bound vesicles which are referred to as extracellular vesicles (EVs) [1,2,3,4]. These circular membrane fragments enriched for mRNAs, small, single-stranded RNAs called microRNAs (miRNAs), long non-coding RNAs, proteins, and bioactive lipids may be released by exocytosis from the intracellular endosomal compartment or are formed by budding from the cell surface membrane [1,2,3,4,5]. Increasing evidence indicates that EVs may play important roles in a variety of physiological processes, including stem cell self-renewal and differentiation, tissue repair, immune surveillance and vascular homeostasis [2, 6, 7]. Furthermore, EVs appear to be implicated in several pathologies, such as cancer, neurodegenerative, cardiovascular, and metabolic disorders [1,2,3, 6, 7]. Nowadays, the importance of EVs is further highlighted by the evidence that they can also be considered as disease biomarkers, as well as possible drug, vaccine, or gene vector delivery tools with potential therapeutic applications [2, 3, 6,7,8,9,10]. Among the different types of EVs, the term ‘exosomes’ specifically refers to nano-sized EVs deriving from the endosomal compartment [3, 5, 6]. Exosomes are released and taken up by most cell types, thereby playing a pivotal role in the maintenance of tissue and organ homeostasis via horizontal transfer of cargos between cells [3, 5, 6]. Thus, the properties and roles of exosomes are now being increasingly investigated in a variety of physiological and pathological settings, with a main focus on their possible diagnostic and therapeutic utility in different conditions [1, 6, 9,10,11].
In this context, EVs and, in particular, exosomes are being increasingly implicated in multiple biological effects possibly exerted by a recently identified interstitial (stromal) cell type known as telocytes (TCs) [2, 12]. TCs, firstly identified by Popescu’s group in 2005 as interstitial Cajal-like cells and officially renamed in 2010, have been described in the stromal compartment of many organs in humans and other vertebrates [13, 14]. As distinctive morphological features, TCs are characterized by a small cell body from which extremely long and slender processes, named telopodes (Tps), originate [13, 14]. The latter typically display a moniliform silhouette conferred by the alternation of thin segments (podomers) and small dilations (podoms) which accommodate caveolae, mitochondria and endoplasmic reticulum cisternae [13, 14]. Within the stromal compartment, Tps make a three-dimensional labyrinthine system establishing multiple intercellular communications by direct homocellular and heterocellular junctions [14, 15]. Moreover, Tps may release different types of EVs either in vivo or in vitro suggesting that TCs may profoundly influence the activity of neighboring cells by vesicular paracrine signals [2, 12].
In the heart, TCs have been reported to be ubiquitously distributed in the epicardium, myocardial interstitium, endocardium and in cardiac valves, where they are supposed to participate in the regulation of cardiac homeostasis and regeneration [16,17,18,19,20,21,22]. TCs appear to be in close contact with virtually all cell types in the human heart, such as cardiomyocytes, cardiac stem cells, blood capillaries, nerve endings and other cells found in the stromal compartment [16, 23, 24]. Noteworthy, it has been demonstrated that cardiac TCs are able to release at least three different types of EVs, namely exosomes, ectosomes and the so-called multivesicular cargos [2, 12, 25]. Indeed, the heart seems characterized by a complex intercellular shuttle mechanism which involves EV-mediated bidirectional paracrine signals either between TCs and tissue-resident stem cells or between TCs and cardiomyocytes [26]. In particular, TC-released exosomes, containing a cell-specific cargo of proteins, lipids and nucleic acids, seem to play a pivotal role in the crosstalk between TCs and other cardiac cells, thus making substantial contribution to cardiac physiology and response to injury [26]. In addition, TCs have been proposed to guide or ‘nurse’ putative stem cells and cardiomyocyte progenitors within cardiac stem cell niches [27, 28]. Of note, a number of studies have indicated that the TC interstitial network is reduced and impaired during myocardial infarction either in humans or in animal models [29]. Interestingly, there is also experimental evidence that transplantation of cardiac TCs in the infarcted and border zones of the heart may be effective in decreasing the infarction size and improving myocardial function [30].
This review summarizes the recent research findings on cardiac TCs and their EVs. We first provide an overview of the general features of TCs, including their morphological traits and immunophenotypes, intercellular signaling mechanisms and possible functional roles. Thereafter, we describe the distribution of TCs in the cardiac stromal compartment and the emerging role of cardiac TCs as intercellular communicators via the release of different EVs with particular focus on exosomes. Finally, the involvement of TCs in cardiovascular diseases and the potential utility of TC-derived exosomes in cardiac regeneration and repair are discussed.
2 General Characteristics of Telocytes
2.1 Morphological Features and Immunophenotypes of Telocytes
TCs are a novel type of stromal cells widely distributed in the interstitium of many tissues and organs [14, 31]. The shortest possible definition of TCs is ‘cells with Tps’ [14]. In fact, TCs display unique ultrastructural features characterized by a small piriform-, spindle- or triangular-shaped cell body (9–15 μm) giving rise to a variable number of extremely long (10–1000 μm) and thin prolongations which have been named Tps and distinguish them from ‘classical’ stromal cells, such as fibroblasts [13, 14, 32]. The cellular nucleus occupies about 25% of the cell body and contains clusters of heterochromatin attached to the nuclear envelope, while the surrounding scarce cytoplasm accommodates mitochondria, endoplasmic reticulum and Golgi apparatus. The Tps display an uneven caliber (mostly below 0.2 μm under light microscopy, and about 0.1–0.5 μm under transmission electron microscopy) with a distinctive moniliform appearance due to the alternation of thin segments (podomers) (~80 nm) and small dilated portions (podoms) (250–300 nm) containing mitochondria, endoplasmic reticulum cisternae and caveolae [14, 32]. In the interstitial space, Tps are typically organized to form a three-dimension labyrinthine network and establish multiple intercellular communications either between TCs through homocelullar junctions or between TCs and other cell types through heterocellular junctions [14, 15, 32]. Moreover, TCs and their Tps can release different types of EVs, which act as important transporters involved in intercellular signaling, including the transfer of genetic material consisting mainly of miRNAs [2, 12, 33].
Electron microscopy is commonly considered the gold standard method to identify TCs [14]. However, double immunolabeling for CD34 and c-kit/CD117, vimentin, platelet-derived growth factor receptor (PDGFR)-α or PDGFR-β may help in distinguishing TCs from other stromal cells under light microscopy [14, 26, 32]. Even if TCs do not display a unique antigenic profile, CD34 and PDGFR-α are currently regarded as the most suitable markers for their in situ identification by immunohistochemistry [14]. In fact, coexpression of CD34 and PDGFR-α has been extensively found in TCs from different tissues and organs [14, 34, 35]. However, there is also increasing evidence that the immunophenotypical features of TCs may vary among different organs/systems and that TC subtypes characterized by the expression of different markers may even coexist within the same organ [36, 37]. For instance, TCs may exhibit either CD34, PDGFR-α or c-kit/CD117 in some organs, such as the heart, while they are CD34/PDGFR-α double-positive and c-kit-negative in others, such as the gastrointestinal tract [34, 35, 38]. A growing number of studies also indicate that TCs display gene expression and proteomic profiles and miRNA signatures that are rather different from those of ‘classical’ fibroblasts [14, 39,40,41,42,43].
2.2 Telocytes as Intercellular Communicators: Telocyte’s Contacts and Telocyte-Derived Extracellular Vesicles
In a variety of either cavitary or non-cavitary organs, TCs make a three-dimensional interstitial network which consists of their long Tps establishing either homocellular contacts between Tps or heterocellular contacts with other neighboring cell types, such as tissue-specific parenchymal cells, vessels, nerve endings, stem/progenitor cells, and other stromal cells including fibroblasts and immunoreactive cells like macrophages and mast cells [14, 15].
In particular, the homocellular contacts may be of several types and are formed by either simple appositions of the plasma membranes of contiguous TCs or by complex junctional areas accomplishing mechanical functions or allowing functional intercellular exchanges [15]. Junctional complexes with a mechanical function can be found in all the TCs and, since they resemble various types of the adherens junctions, have been named ‘puncta adhaerentia minima’ and ‘processus adhaerens’, which usually connect the overlapping Tps, and ‘recessus adhaerens’ or ‘manubria adhaerentia’ having a cuff-like appearance [15]. Instead, junctional complexes that functionally allow intercellular exchanges and signaling are mostly represented by gap junctions. Heterocellular contacts between TCs and other cell types consist mainly of minute junctions (e.g. point contacts, nanocontacts and planar contacts) typically with an inter-membrane distance of 10–30 nm, but more often by variably extended simple apposition of the contiguous TC plasma membranes [15].
Furthermore, increasing evidence indicates that TCs may participate in intercellular signaling through the release of a variety of EVs which regulate multiple neighboring cell functions [2, 12]. In fact, EVs are currently regarded as a new important way of communication for either short- or long-distance intercellular signaling events. EVs, characterized by a lipid bilayer membrane, carry a rich cargo of various bioactive materials including DNAs, RNAs, proteins, and lipids that are released into the extracellular space during both physiological and pathological processes [3, 5, 7, 44]. These EVs can interact with different cell types by ligand-receptor interactions, membrane fusion, and subsequent internalization via receptor-mediated endocytosis or macropinocytosis [44]. According to the classification criteria based on biogenesis mechanisms, different types of EVs can be distinguished, namely exosomes, ectosomes (also known as shedding microvesicles, microparticles or plasma membrane-derived vesicles), apoptotic bodies as well as a recently described novel EV type termed multivesicular cargos [1,2,3, 5, 7, 12, 25, 44].
Among the aforementioned EV subtypes, exosomes have been most extensively studied and characterized in recent years. These nano-sized vesicles are originated from the fusion of the plasma membrane with the multivesicular bodies, which are large cytoplasmic endosomal structures characterized by multiple intraluminal vesicles [1, 3, 5, 6, 44]. In fact, multivesicular bodies can either traffic to lysosomes for degradation or, alternatively, to the plasma membrane where, upon fusion, they may release their contents into the surrounding extracellular space. Once released into the extracellular space by exocytosis, the multivesicular body-derived vesicles are referred to as ‘exosomes’ [1, 3, 5, 6]. These exosomes, released into tissue interstitial spaces and bodily fluids, appear as multiple homogenous vesicles of around 30–150 nm in diameter containing numerous macromolecules including mRNAs, miRNAs, long non-coding RNAs, cytokines, chemokines, growth factors and various endosomal proteins such as tetraspanins (e.g. CD9, CD63, CD81), ALG-2 interacting protein X (Alix), tumour susceptibility gene 101 (TSG101), and annexin A5 (ANXA5), which are commonly used as markers for exosomal identification [1, 3, 5, 6, 12].
Unlike exosomes, ectosomes are small EVs with a diameter of about 50–1000 nm which originate directly from the plasma membrane by outward budding [1, 2, 5, 7, 44]. The molecular composition of ectosomes is still poorly characterized, although they seem to contain matrix metalloproteinases, glycoproteins (e.g. GPIb, GPIIb–IIIa and P-selectin), and integrins (e.g. Mac-1), depending on the ectosome-releasing cell type. Apoptotic bodies are instead heterogeneous vesicles (50 nm–5 μm) released upon programmed cell death via outward blebbing of the cell membrane [1, 2]. Finally, multivesicular cargos (0.4–1 μm) are large EVs which contain tightly packed endomembrane-bound smaller vesicles and have been recently reported to be secreted by cardiac TCs [2, 12, 25, 33]. Under transmission electron microscopy, multivesicular cargos appear frequently clustered in the subplasmallemal space of TCs, bulging from the plasma membrane of either the cell body or Tps, and released in an envelope formed by the plasma membrane [25]. The subsequent disruption of this envelope results in the release of individual or grouped small vesicles into the extracellular space [25]. Consistent with these electron microscopy observations, a peculiar structure with a cup-shaped or ellipsoid morphology, usually containing between 60 and 500 tightly packed endomembrane vesicles of varying shapes and dimensions, has been highlighted for multivesicular cargos by electron tomography [25].
2.3 Potential Roles of Telocytes
According to the distinctive morphological features, distribution and intercellular communications of the three-dimensional network-building Tps either in normal or in diseased tissues, multiple potential biological functions have been suggested for the TCs [14, 26, 29]. It is commonly believed that TCs may be functionally committed to the maintenance of local tissue homeostasis, as well as the regulation of tissue differentiation and renewal by short- and long-distance intercellular crosstalk mechanisms [14, 26, 29]. In particular, it has been proposed that during organ morphogenesis TCs might act as inductors and regulators of cell differentiation due to their capability to release paracrine molecular signals and to structurally build the three-dimensional scaffold driving parenchymal organization, while in the adulthood, these cells might behave as mesenchymal stromal cells with stemness properties and the potential to differentiate toward different mature cell types [14, 16, 21, 26, 45]. TCs have also been proposed to participate in immunomodulation and immunosurveillance, and possibly in the regulation of the activity of neighboring stromal cells, such as fibroblasts [29]. Moreover, TCs might be essential for the maintenance, proliferation, differentiation, maturation and guidance of the local stem/progenitor cells found within the niches of various organs, eventually stimulating and sustaining tissue regenerative and reparative processes [14, 26, 28]. Interestingly, increasing evidence also suggests that TCs may be involved in different pathologies including cancers, liver fibrosis, systemic sclerosis, inflammatory bowel diseases, and cardiovascular diseases [29, 45,46,47,48,49,50,51,52]. Therefore, currently there is growing research interest on the possible applications of TCs in regenerative medicine [26, 53].
3 Cardiac Telocytes and Their Extracellular Vesicles
The cardiac stroma plays a fundamental role in the building and maintenance of the normal heart architecture, as well as in any changes occurring in a variety of cardiac diseases [16]. Numerous electron microscopy studies have demonstrated that the heart contains typical TCs (Fig. 16.1) which are found in the epicardium, myocardial interstitium, endocardium, and cardiac valves [16,17,18,19,20,21,22,23,24]. Noteworthy, TCs were also identified in epicardial stem cell niches, where they appear located in close relationship with tissue-resident stem cells and putative cardiomyocyte progenitors, possibly contributing to form an interstitial scaffold which supports cardiomyocyte precursors during their self-renewal process and differentiation into new mature cardiomyocytes [27, 28]. During heart morphogenesis, TCs may even guide the process of cardiac tissue compaction from the embryonic myocardial trabeculae [16, 21, 54]. In addition, considering that cardiac TCs and epicardial progenitor cells share the expression of some stemness markers (e.g. c-kit/CD117), it has also been suggested that TCs might represent a subpopulation of progenitor cells which could therefore be directly implicated in cardiac development and regenerative processes [21, 53]. Of note, it also appears that both TCs and tissue-resident stem cells are decreased in the adult heart compared with newborns, which might contribute to the reduced cardiac regenerative capacity during aging [26, 55]. A recent experimental study in mice also reported that the number of cardiac TCs was significantly increased following physical exercise training, which is consistent with the evidence that exercise-induced cardiac growth is an important way to promote cardiac regeneration and repair [56].

Representative scanning electron micrograph of monkey left ventricular myocardium. The image shows a typical telocyte located across the cardiomyocytes. The three-dimensional view reveals close interconnections of the telocyte body and telopodes with cardiomyocytes and blood capillaries (Reproduced with permission from Kostin and Popescu [19])
At present, cardiac TCs are clearly the best ex vivo, in vitro and in vivo characterized TCs. In the adult heart, TCs display immunopositivity for different markers, such as CD34, c-kit/CD117 (Fig. 16.2), vimentin, PDGFR-α or PDGFR-β [26, 30, 35, 38]. Moreover, cardiac TCs in primary culture have been reported to express the embryonic stem cell marker Nanog and the myocardial stem cell marker Sca-1, suggesting that these cells may possess pluripotent properties [26, 38]. In addition, cardiac TCs exhibit a distinctive miRNA signature that further differentiates them from other interstitial cells. In particular, at variance with cardiac fibroblasts, cardiac TCs do not express miR-193, which has been shown to repress the expression of c-kit/CD117 [42]. Interestingly, this seems consistent with the evidence that cardiac TCs display c-kit/CD117 immunopositivity either ex vivo or in vitro [30, 38, 42]. Furthermore, miRNAs which are usually expressed by cardiomyocytes and other muscle cells (e.g. miR-133a, miR-208a) are undetectable in cardiac TCs [42]. Cultured cardiac TCs also behave differently from fibroblasts in terms of adherence, spreading, and extension of their cell prolongations when seeded on various matrix proteins [57]. Overall, these data clearly support the notion that TCs are a unique type of cardiac interstitial cells definitely distinct from ‘classical’ fibroblasts [58].

Identification of rat cardiac telocytes in culture. (a) Primary culture of isolated cardiac telocytes reveals that under phase-contrast microscopy cardiac telocytes display piriform/spindle/triangular cell bodies and very long and slender telopodes formed by the alternation of small dilated segments (podoms, arrows) and thin segments (podomers, dotted line arrows). (b) Cardiac telocytes with unique morphology are c-kit+ and CD34+ (Adapted with permission from Zhao et al. [30])
Although it appears that TCs represent a small fraction of interstitial cells in the human heart, their very long and convoluted Tps form a dynamic and extensive three-dimensional network within the cardiac stroma [24, 53, 55]. In addition to transmission electron microscopy studies, three-dimensional reconstruction of cardiac TCs has been recently performed by focused ion beam scanning electron microscopy (FIB-SEM) tomography, which confirmed that these cells have very long, slender and flattened (ribbon-like) Tps, with humps along their length due to the presence of podoms [59]. FIB-SEM tomography also highlighted that TCs make a network in the cardiac interstitium through wide adherens junctions connecting Tps [59]. Moreover, TCs build a supportive network in the myocardial interstitium and may communicate with the surrounding cells, namely cardiomyocytes, stem/progenitor cells, blood vessels, nerve endings, fibroblasts and immune cells (Fig. 16.3) [26, 55]. In particular, heterocellular connections between Tps and cardiomyocytes consist mainly of small point junctions with electron-dense nanocontacts, presumably forming a ‘functional unit’ which might help in mediating the electrical coupling of cardiomyocytes [26, 60,61,62]. Consistent with the well-documented spatial relationship between TCs and stem cell niches in cardiac tissue, different types of junctions have also been observed between cardiac TCs and cardiac stem cells in vitro [27, 28, 63].

(a–c) Representative transmission electron micrographs of human atrial interstitium. (a, b) General views of human atrial interstitium showing the distribution of telocytes and their telopodes. (c) A telopode is enfolding a putative stem cell with very few mitochondria and numerous ribosomes in the cytoplasm. TC telocyte, Tp telopode, CM cardiomyocyte, E endothelial cell, P pericyte, N nerve ending, pSC putative stem cell, coll collagen (Adapted with permission from Popescu et al. [55])
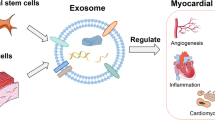
Besides intercellular contacts, paracrine signaling also plays an important role in the crosstalk between different cardiac cells, contributing substantially to cardiac physiology, responses to injury, regeneration and repair [26]. One pivotal component of this paracrine signaling machinery is represented by different specialized subtypes of EVs, such as exosomes and shedding microvesicles [2, 12, 26]. Indeed, growing evidence indicates that both types of EVs may function as shuttles to translocate genetic material (e.g. mRNAs and miRNAs) between cells over a long distance thereby modulating the gene expression and phenotype of the recipient cells [2, 12, 26]. In particular, recent studies demonstrated the importance of exosome-encased miRNAs in multiple intercellular communications within the cardiovascular system [6]. This specific exchange mechanism may be of crucial importance in cardiac tissue regeneration and remodeling [6, 11, 26]. For instance, it has been shown that post-mytotic cardiomyocytes are capable to deliver miRNAs to cardiac stem cells promoting their differentiation [64]. Moreover, stem cell-derived exosomes contain cardioprotective enzymes, which may exert beneficial effects on cardiomyocytes as demonstrated in a rat model of myocardial infarction and reperfusion [6, 65]. Noteworthy, it also appears that different types of TC-released EVs may act as important transporters for paracrine molecular signal exchange between cardiac TCs and cardiomyocytes or tissue-resident progenitor cells [25, 26, 33]. Using transmission electron microscopy and electron tomography, it could be demonstrated that cardiac TCs in culture release at least three different types of EVs, namely exosomes released from intracellular endosomes, ectosomes budding directly from the plasma membrane, and multivesicular cargos, these latter containing tightly packaged endomembrane-bound vesicles (Fig. 16.4) [25]. Electron tomography further highlighted that such endomembrane vesicles are released into the extracellular space as a cargo enclosed by plasma membranes [25]. These different types of EVs, which are also released in situ by TCs within the cardiac tissue, likely represent an essential component of the intercellular signaling machinery of cardiac TCs and may be directly involved in the complex physiological and regenerative mechanisms of the heart [26]. Of note, in vitro studies have shown that the secretome of myocardial TCs may modulate the activity and increase the self-renewal capacity of cardiac stem cells [41]. Using fluorescent labeling of cells and EVs with calcein and Cy5-miR-21 oligos, it could be demonstrated that cardiac TCs deliver EVs loaded with miRNAs to cardiac stem cells [33]. Similarly, cardiac stem cells were found to deliver miRNA-loaded EVs to TCs, suggesting the existence of a reciprocal (bidirectional) post-transcriptional signaling between cardiac TCs and stem cells (Fig. 16.5) [33]. Collectively, the aforementioned observations support the notion that cardiac TCs may exert an epigenetic control over stem and progenitor cells, thus contributing to the regulation of post-natal cardiac tissue homeostasis and renewal. Depending of the specific types of miRNAs delivered by EVs, cardiac TCs might contribute substantially to the local balance between quiescent and proliferative states of stem cells, as well as between self-renewal and differentiation of putative cardiomyocyte progenitors [26, 33].

(a) Schematic representation of the three types of extracellular vesicles released by cardiac telocytes, namely exosomes, ectosomes and multivesicular cargos. (b–d) Electron microscopy of cardiac telocytes in culture demonstrates: (b) the presence of numerous intraluminal vesicles (small arrows) in two multivesicular bodies, precursors of exosomes; (c) the ectosome budding (arrow) from the plasma membrane of a telopode; (d) a multivesicular cargo emerging (arrow) from a telopode. TC telocyte, Tp telopode, mvb multivesicular bodies, m mitochondria, er endoplasmic reticulum, r ribosome (Adapted with permission from Fertig et al. [25])

Cardiac telocytes and stem cells exchange microRNAs by extracellular vesicles (Reproduced with permission from Cismaşiu and Popescu [33])
4 Telocytes in Cardiovascular Diseases
The infarcted myocardium experiences a loss of cardiomyocytes via ischemia-induced necrosis and apoptosis followed by neoangiogenesis and fibrotic changes, resulting into pathological tissue remodeling and, eventually, end-stage organ failure [26]. Recently, it has been demonstrated that the number of myocardial TCs is also dramatically decreased during heart failure due to dilated, ischemic or inflammatory cardiomyopathy [29, 66]. In particular, in the failing human heart TCs exhibit several ultrastructural degenerative changes culminating into apoptotic cell death [66]. It was also shown that the composition of the extracellular matrix may substantially influence the distribution of TCs within the cardiac interstitium [66]. Indeed, in fibrotic areas of the failing myocardium which were characterized by the deposition of tightly packed collagen fibers, the TCs and Tps were severely reduced or even almost completely undetectable. Moreover, the few remaining TCs exhibited a variety of ultrastructural alterations, such as cytoplasmic vacuolization and shrinkage/shortening of the Tps along with the loss of the typical Tp labyrinthine arrangement [66]. On the contrary, in interstitial areas rich in amorphous material, TCs were more numerous and displayed typical morphological features and organization of Tps. As further evidenced by semiquantitative analysis, the number of cardiac TCs and Tps was negatively correlated to the amount of mature fibrillar collagens [66]. Therefore, the interstitial distribution of TCs and Tps appear to closely reflect any quantitative and qualitative changes in the extracellular matrix composition of the failing human myocardium. Of note, TCs might also be involved in the formation of cardiac amyloid deposits in patients with long-standing atrial fibrillation [67]. In particular, Tps were found to intimately surround the amyloid deposits, likely in the attempt to prevent their expansion in the adjacent areas of the cardiac interstitium [67].
The pathophysiological consequences of the TC reduction and loss in the failing human heart are not completely understood, but it has been proposed that such a severe impairment of the TC interstitial network could largely contribute to the disruption of the normal three-dimensional myocardial organization and complex intercellular signaling mechanisms [29, 66]. Besides building a supportive structural network within the myocardial stroma, in the adult heart TCs have also been detected in the cardiogenic niches, where they establish close communications and may exchange paracrine signals through EVs with the tissue-resident stem cells possibly acting as nursing and guiding cells [27, 28, 33]. Therefore, the extensive damage and reduction of TCs occurring in the failing heart may profoundly hamper the TC ability to maintain stem cell niches with consequent impairment and loss of the pool of cardiac stem cells and putative cardiomyocyte progenitors [29]. Of note, experimental studies in a rat model of myocardial infarction showed that TCs were strongly reduced in fibrotic zones of the myocardium, while exogenous transplantation of cardiac TCs in the infarcted and border zones effectively decreased the infarction size with significant improvement of post-infarcted cardiac function [30, 68]. Histological analyses further revealed that a reconstruction of the stromal network of TCs paralleled by an impressive reduction in tissue fibrosis occurred in the exogenous TC-injected myocardium [30, 68]. The aforementioned beneficial effects could also depend on the ability of transplanted cardiac TCs to promote the expansion, recruitment and differentiation of local cardiomyocyte progenitors [26, 30, 68]. In another study, transplantation of human induced pluripotent stem cell-derived mesenchymal stem cells was able to reduce myocardial infarction improving cardiac function in mice, and this positive effect was accompanied by the rebuilding of the interstitial network of TCs within the infarcted myocardium [69]. Interestingly, TCs may also behave as key players in neoangiogenesis after experimental acute myocardial infarction [70]. In fact, it was demonstrated that TCs are markedly increased in the border zone of the infarcted myocardium during the post-infarction neoangiogenesis phase, with multiple Tps exhibiting numerous close intercellular connections either with pre-existing or neoformed microvessels [70]. Besides such physical contacts, TCs may presumably contribute to neoangiognesis through paracrine secretion of proangiogenic factors, including VEGF, NOS2 and several proangiogenic miRNAs (e.g. let-7e, 10a, 21, 27b, 100, 126-3p, 130a, 143, 155, and 503) [70].
Overall, the currently available experimental data support the possible therapeutic application of exogenous TC transplantation in the treatment of cardiac diseases. Nevertheless, further preclinical in vivo studies and the use of in vitro cardiac tissue engineering will help to better decipher the specific roles exerted by TCs during cardiac repair and regenerative processes [53, 62]. In this context, it is worth mentioning that a recent study highlighted the importance of TCs in the architectural organization of three-dimensional engineered heart tissue [71]. Indeed, electron microscopy revealed that typical TCs surrounded and contacted the cardiomyocytes with their long Tps exhibiting cardiomyocyte nursing properties during the construction of engineered heart tissue. Thus, engineered heart tissues may represent a very useful model system to clarify the specific functions of TCs during cardiac morphogenesis and post-injury regeneration [71].
5 The Potential Utility of Telocyte-Derived Exosomes in Cardiac Homeostasis, Regeneration and Repair
Exosomes seem to play a preferential role in the paracrine crosstalk between different cardiac cells, making substantial contribution to cardiac physiology, response to injury, regeneration and repair [6, 11, 26]. Therefore, exosomes are now being increasingly investigated for their possible diagnostic and therapeutic use in cardiovascular diseases [6, 11, 26, 72]. Interestingly, intramyocardial delivery of stem cell-derived exosomes resulted in the reduction of cardiomyocyte apoptosis and fibrosis, stimulated neoangiogenesis, and ameliorated cardiac function after experimental myocardial infarction [73,74,75,76]. In this experimental setting, the cardioprotective effects of exosomes were mostly ascribed to their enriched content in a variety of angiogenic and anti-apoptotic miRNAs [73, 74].
Besides tissue-resident stem cell-derived exosomes, either electron microscopy or electron tomography studies provided direct evidence that cardiac TCs are an additional important source of exosomes within the heart microenvironment [25, 26, 33]. As already mentioned, increased numbers of cardiac TCs were observed in the proangiogenic phase of the post-infarcted heart, with numerous secreted exosomes being detectable around the TC cell bodies and Tps [70]. Of note, TC-derived exosomes bear a cocktail of molecular signals (e.g. proangiogenic miRNAs) which may regulate the activity of neighboring vascular endothelial cells with consequent promotion of angiogenesis via an epigenetic paracrine mechanism [70]. In vitro studies further suggest that cardiac TCs could influence mesenchymal stem cell functions via exosomes [33, 41]. Considering that intramyocardial injection of cardiac TCs showed therapeutic utility in reducing the infarction size and myocardial fibrosis in rodent models, further research is required to elucidate the possible implication of TC-secreted exosomes in cardiac response to injury [30, 68]. An in-depth molecular characterization of cardiac TC-derived exosomes will also be of fundamental importance to decipher the TC paracrine machinery and its possible targeting in cardiovascular diseases. Anticipating a new avenue for potential therapeutic applications, TC-derived exosomes could be employed in the not-too-distant future as novel therapeutic nanovectors to deliver specific biological signals that may foster cardiomyocyte survival, cardiac neovascularization, and tissue-resident progenitor cell activation/differentiation to promote myocardial regeneration and repair [26, 72, 77].
6 Conclusions and Future Perspectives
Growing evidence supports a pivotal role of TCs in cardiac pathophysiology [16, 26, 29, 47]. Among cardiac interstitial cells, TCs appear to possess the unique ability to organize a proper three-dimensional scaffold consisting of their cell bodies and very long and convoluted Tps, and stimulate the growth and differentiation of putative cardiomyocyte progenitors to build the complex multicellular architecture of the heart [16, 21]. In fact, due to their close spatial relationship and intimate connections with other cell types, TCs are seen as ‘connecting cells’ mostly specialized to orchestrate the intercellular signaling mechanisms that constitute the basis for either a proper heart development or the maintenance of cardiac homeostasis in post-natal life [16, 21, 26]. In this context, recent studies have highlighted that multiple paracrine signaling effects possibly exerted by TCs in the adult heart largely depend on the secretion of EVs and, in particular, exosomes [2, 25, 26, 33, 41]. On the basis of the current knowledge, it is believed that the exogenous transplantation of TCs or the delivery of TC-derived exosomes might have great potential as future therapeutic strategies to foster cardiac regeneration and repair [26, 30, 33, 41, 68]. Given their biophysical properties, among the various types of EVs exosomes are particularly easy to isolate and their mRNA, miRNA and protein contents can be easily manipulated for therapeutic purposes [6]. Therefore, the possible use of exosomes, either natural exosomes or exosome-mimetic nanovesicles, as carriers/vectors of biological or synthetic therapeutics might be a promising strategy to allow efficient delivery of drugs across different physiological barriers to specific target cells [6]. Interestingly, beneficial effects of stem cell-derived exosomes for ischemic myocardial tissue regeneration and repair have already been reported in different preclinical studies [6, 78, 79]. As far as cardiac TCs are concerned, the specific molecular cargo of their exosomes and the mechanisms that promote their secretion still require a thorough characterization. The exact biodistribution of cardiac TC-derived exosomes also remains to be established. Finally, whether the manipulation of cardiac TC-released exosomes might represent a novel therapeutic strategy to counteract heart failure and other cardiovascular diseases will need to be comprehensively addressed in future translational studies.
References
Vader P, Breakefield XO, Wood MJ (2014) Extracellular vesicles: emerging targets for cancer therapy. Trends Mol Med 20(7):385–393
Cretoiu D, Xu J, Xiao J, Cretoiu SM (2016) Telocytes and their extracellular vesicles—evidence and hypotheses. Int J Mol Sci 17(8):1322
Corrado C, Raimondo S, Chiesi A, Ciccia F, De Leo G, Alessandro R (2013) Exosomes as intercellular signaling organelles involved in health and disease: basic science and clinical applications. Int J Mol Sci 14(3):5338–5366
Ratajczak J, Wysoczynski M, Hayek F, Janowska-Wieczorek A, Ratajczak MZ (2006) Membrane-derived microvesicles: important and underappreciated mediators of cell-to-cell communication. Leukemia 20(9):1487–1495
Camussi G, Deregibus MC, Bruno S, Cantaluppi V, Biancone L (2010) Exosomes/microvesicles as a mechanism of cell-to-cell communication. Kidney Int 78(9):838–848
Emanueli C, Shearn AI, Angelini GD, Sahoo S (2015) Exosomes and exosomal miRNAs in cardiovascular protection and repair. Vasc Pharmacol 71:24–30
EL Andaloussi S, Mäger I, Breakefield XO, Wood MJ (2013) Extracellular vesicles: biology and emerging therapeutic opportunities. Nat Rev Drug Discov 12(5):347–357
Zhang B, Yeo RW, Tan KH, Lim SK (2016) Focus on extracellular vesicles: therapeutic potential of stem cell-derived extracellular vesicles. Int J Mol Sci 17(2):174
Batrakova EV, Kim MS (2015) Using exosomes, naturally-equipped nanocarriers, for drug delivery. J Control Release 219:396–405
Ren J, He W, Zheng L, Duan H (2016) From structures to functions: insights into exosomes as promising drug delivery vehicles. Biomater Sci 4(6):910–921
Zhang Y, Hu YW, Zheng L, Wang Q (2017) Characteristics and roles of exosomes in cardiovascular disease. DNA Cell Biol 36(3):202–211
Ratajczak MZ, Ratajczak D, Pedziwiatr D (2016) Extracellular microvesicles (ExMVs) in cell to cell communication: a role of telocytes. Adv Exp Med Biol 913:41–49
Popescu LM, Faussone-Pellegrini MS (2010) Telocytes—a case of serendipity: the winding way from interstitial cells of Cajal (ICC), via interstitial Cajal-like cells (ICLC) to telocytes. J Cell Mol Med 14(4):729–740
Cretoiu SM, Popescu LM (2014) Telocytes revisited. Biomol Concepts 5(5):353–369
Faussone-Pellegrini MS, Gherghiceanu M (2016) Telocyte’s contacts. Semin Cell Dev Biol 55:3–8
Bani D (2016) Telocytes in cardiac tissue architecture and development. Adv Exp Med Biol 913:127–137
Popescu LM, Manole CG, Gherghiceanu M, Ardelean A, Nicolescu MI, Hinescu ME, Kostin S (2010) Telocytes in human epicardium. J Cell Mol Med 14(8):2085–2093
Gherghiceanu M, Manole CG, Popescu LM (2010) Telocytes in endocardium: electron microscope evidence. J Cell Mol Med 14(9):2330–2334
Kostin S, Popescu LM (2009) A distinct type of cell in myocardium: interstitial Cajal-like cells (ICLCs). J Cell Mol Med 13(2):295–308
Kostin S (2010) Myocardial telocytes: a specific new cellular entity. J Cell Mol Med 14(7):1917–1921
Bani D, Formigli L, Gherghiceanu M, Faussone-Pellegrini MS (2010) Telocytes as supporting cells for myocardial tissue organization in developing and adult heart. J Cell Mol Med 14(10):2531–2538
Yang Y, Sun W, Wu SM, Xiao J, Kong X (2014) Telocytes in human heart valves. J Cell Mol Med 18(5):759–765
Gherghiceanu M, Popescu LM (2012) Cardiac telocytes—their junctions and functional implications. Cell Tissue Res 348(2):265–279
Rusu MC, Pop F, Hostiuc S, Curca GC, Jianu AM, Paduraru D (2012) Telocytes form networks in normal cardiac tissues. Histol Histopathol 27(6):807–816
Fertig ET, Gherghiceanu M, Popescu LM (2015) Extracellular vesicles release by cardiac telocytes: electron microscopy and electron tomography. J Cell Mol Med 18(10):1938–1943
Bei Y, Zhou Q, Sun Q, Xiao J (2016) Telocytes in cardiac regeneration and repair. Semin Cell Dev Biol 55:14–21
Gherghiceanu M, Popescu LM (2010) Cardiomyocyte precursors and telocytes in epicardial stem cell niche: electron microscope images. J Cell Mol Med 14(4):871–877
Popescu LM, Gherghiceanu M, Manole CG, Faussone-Pellegrini MS (2009) Cardiac renewing: interstitial Cajal-like cells nurse cardiomyocyte progenitors in epicardial stem cell niches. J Cell Mol Med 13(5):866–886
Ibba-Manneschi L, Rosa I, Manetti M (2016) Telocyte implications in human pathology: an overview. Semin Cell Dev Biol 55:62–69
Zhao B, Chen S, Liu J, Yuan Z, Qi X, Qin J, Zheng X, Shen X, Yu Y, Qnin TJ, Chan JY, Cai D (2013) Cardiac telocytes were decreased during myocardial infarction and their therapeutic effects for ischaemic heart in rat. J Cell Mol Med 17(1):123–133
Xiao J, Bei Y (2016) Decoding telocytes. Adv Exp Med Biol 913:23–39
Faussone-Pellegrini MS, Popescu LM (2011) Telocytes. Biomol Concepts 2(6):481–489
Cismaşiu VB, Popescu LM (2015) Telocytes transfer extracellular vesicles loaded with microRNAs to stem cells. J Cell Mol Med 19(2):351–358
Vannucchi MG, Traini C, Manetti M, Ibba-Manneschi L, Faussone-Pellegrini MS (2013) Telocytes express PDGFRα in the human gastrointestinal tract. J Cell Mol Med 17(9):1099–1108
Zhou Q, Wei L, Zhong C, Fu S, Bei Y, Huică RI, Wang F, Xiao J (2015) Cardiac telocytes are double positive for CD34/PDGFR-α. J Cell Mol Med 19(8):2036–2042
Vannucchi MG, Faussone-Pellegrini MS (2016) The telocyte subtypes. Adv Exp Med Biol 913:115–126
Cretoiu D, Radu BM, Banciu A, Banciu DD, Cretoiu SM (2016) Telocytes heterogeneity: from cellular morphology to functional evidence. Semin Cell Dev Biol 64:26–39
Chang Y, Li C, Lu Z, Li H, Guo Z (2015) Multiple immunophenotypes of cardiac telocytes. Exp Cell Res 338(2):239–244
Sun X, Zheng M, Zhang M, Qian M, Zheng Y, Li M, Cretoiu D, Chen C, Chen L, Popescu LM, Wang X (2014) Differences in the expression of chromosome 1 genes between lung telocytes and other cells: mesenchymal stem cells, fibroblasts, alveolar type II cells, airway epithelial cells and lymphocytes. J Cell Mol Med 18(5):801–810
Zheng Y, Cretoiu D, Yan G, Cretoiu SM, Popescu LM, Wang X (2014) Comparative proteomic analysis of human lung telocytes with fibroblasts. J Cell Mol Med 18(4):568–589
Albulescu R, Tanase C, Codrici E, Popescu DI, Cretoiu SM, Popescu LM (2015) The secretome of myocardial telocytes modulates the activity of cardiac stem cells. J Cell Mol Med 19(8):1783–1794
Cismaşiu VB, Radu E, Popescu LM (2011) miR-193 expression differentiates telocytes from other stromal cells. J Cell Mol Med 15(5):1071–1074
Zheng Y, Zhang M, Qian M, Wang L, Cismasiu VB, Bai C, Popescu LM, Wang X (2013) Genetic comparison of mouse lung telocytes with mesenchymal stem cells and fibroblasts. J Cell Mol Med 17(4):567–577
Yoon YJ, Kim OY, Gho YS (2014) Extracellular vesicles as emerging intercellular communicasomes. BMB Rep 47(10):531–539
Diaz-Flores L, Gutierrez R, Garcia MP, Sáez FJ, Díaz-Flores L Jr, Valladares F, Madrid JF (2014) CD34+ stromal cells/fibroblasts/fibrocytes/telocytes as a tissue reserve and a principal source of mesenchymal cells. Location, morphology, function and role in pathology. Histol Histopathol 29(7):831–870
Ibba-Manneschi L, Rosa I, Manetti M (2016) Telocytes in chronic inflammatory and fibrotic diseases. Adv Exp Med Biol 913:51–76
Kostin S (2016) Cardiac telocytes in normal and diseased hearts. Semin Cell Dev Biol 55:22–30
Zheng Y, Bai C, Wang X (2012) Telocyte morphologies and potential roles in diseases. J Cell Physiol 227(6):2311–2317
Manetti M, Rosa I, Messerini L, Ibba-Manneschi L (2015) Telocytes are reduced during fibrotic remodelling of the colonic wall in ulcerative colitis. J Cell Mol Med 19(1):62–73
Milia AF, Ruffo M, Manetti M, Rosa I, Conte D, Fazi M, Messerini L, Ibba-Manneschi L (2013) Telocytes in Crohn’s disease. J Cell Mol Med 17(12):1525–1536
Manetti M, Guiducci S, Ruffo M, Rosa I, Faussone-Pellegrini MS, Matucci-Cerinic M, Ibba-Manneschi L (2013) Evidence for progressive reduction and loss of telocytes in the dermal cellular network of systemic sclerosis. J Cell Mol Med 17(4):482–496
Fu S, Wang F, Cao Y, Huang Q, Xiao J, Yang C, Popescu LM (2015) Telocytes in human liver fibrosis. J Cell Mol Med 19(3):676–683
Bei Y, Wang F, Yang C, Xiao J (2015) Telocytes in regenerative medicine. J Cell Mol Med 19(7):1441–1454
Faussone-Pellegrini MS, Bani D (2010) Relationships between telocytes and cardiomyocytes during pre- and post-natal life. J Cell Mol Med 14(5):1061–1063
Popescu LM, Curici A, Wang E, Zhang H, Hu S, Gherghiceanu M (2015) Telocytes and putative stem cells in ageing human heart. J Cell Mol Med 19(1):31–45
Xiao J, Chen P, Qu Y, Yu P, Yao J, Wang H, Fu S, Bei Y, Chen Y, Che L, Xu J (2016) Telocytes in exercise-induced cardiac growth. J Cell Mol Med 20(5):973–979
Niculite CM, Regalia TM, Gherghiceanu M, Huica R, Surcel M, Ursaciuc C, Leabu M, Popescu LM (2015) Dynamics of telopodes (telocyte prolongations) in cell culture depends on extracellular matrix protein. Mol Cell Biochem 398(1–2):157–164
Bei Y, Zhou Q, Fu S, Lv D, Chen P, Chen Y, Wang F, Xiao J (2015) Cardiac telocytes and fibroblasts in primary culture: different morphologies and immunophenotypes. PLoS One 10(2):e0115991
Cretoiu D, Hummel E, Zimmermann H, Gherghiceanu M, Popescu LM (2014) Human cardiac telocytes: 3D imaging by FIB-SEM tomography. J Cell Mol Med 18(11):2157–2164
Gherghiceanu M, Popescu LM (2011) Heterocellular communication in the heart: electron tomography of telocyte-myocyte junctions. J Cell Mol Med 15(4):1005–1011
Shim W (2016) Myocardial telocytes: a new player in electric circuitry of the heart. Adv Exp Med Biol 913:241–251
Zhou J, Zhang Y, Wen X, Cao J, Li D, Lin Q, Wang H, Liu Z, Duan C, Wu K, Wang C (2010) Telocytes accompanying cardiomyocyte in primary culture: two- and three-dimensional culture environment. J Cell Mol Med 14(11):2641–2645
Popescu LM, Fertig ET, Gherghiceanu M (2016) Reaching out: junctions between cardiac telocytes and cardiac stem cells in culture. J Cell Mol Med 20(2):370–380
Hosoda T, Zheng H, Cabral-da-Silva M, Sanada F, Ide-Iwata N, Ogórek B, Ferreira-Martins J, Arranto C, D’Amario D, del Monte F, Urbanek K, D'Alessandro DA, Michler RE, Anversa P, Rota M, Kajstura J, Leri A (2011) Human cardiac stem cell differentiation is regulated by a mircrine mechanism. Circulation 123(12):1287–1296
Lai RC, Arslan F, Lee MM, Sze NS, Choo A, Chen TS, Salto-Tellez M, Timmers L, Lee CN, El Oakley RM, Pasterkamp G, de Kleijn DP, Lim SK (2010) Exosome secreted by MSC reduces myocardial ischemia/reperfusion injury. Stem Cell Res 4(3):214–222
Richter M, Kostin S (2015) The failing human heart is characterized by decreased numbers of telocytes as result of apoptosis and altered extracellular matrix composition. J Cell Mol Med 19(11):2597–2606
Mandache E, Gherghiceanu M, Macarie C, Kostin S, Popescu LM (2010) Telocytes in human isolated atrial amyloidosis: ultrastructural remodelling. J Cell Mol Med 14(12):2739–2747
Zhao B, Liao Z, Chen S, Yuan Z, Yilin C, Lee KK, Qi X, Shen X, Zheng X, Quinn T, Cai D (2014) Intramyocardial transplantation of cardiac telocytes decreases myocardial infarction and improves post-infarcted cardiac function in rats. J Cell Mol Med 18(5):780–789
Miao Q, Shim W, Tee N, Lim SY, Chung YY, Ja KP, Ooi TH, Tan G, Kong G, Wei H, Lim CH, Sin YK, Wong P (2014) iPSC-derived human mesenchymal stem cells improve myocardial strain of infarcted myocardium. J Cell Mol Med 18(8):1644–1654
Manole CG, Cismaşiu V, Gherghiceanu M, Popescu LM (2011) Experimental acute myocardial infarction: telocytes involvement in neo-angiogenesis. J Cell Mol Med 15(11):2284–2296
Zhou J, Wang Y, Zhu P, Sun H, Mou Y, Duan C, Yao A, Lv S, Wang C (2014) Distribution and characteristics of telocytes as nurse cells in the architectural organization of engineered heart tissues. Sci China Life Sci 57(2):241–247
Ong SG, Wu JC (2015) Exosomes as potential alternatives to stem cell therapy in mediating cardiac regeneration. Circ Res 117(1):7–9
Barile L, Lionetti V, Cervio E, Matteucci M, Gherghiceanu M, Popescu LM, Torre T, Siclari F, Moccetti T, Vassalli G (2014) Extracellular vesicles from human cardiac progenitor cells inhibit cardiomyocyte apoptosis and improve cardiac function after myocardial infarction. Cardiovasc Res 103(4):530–541
Wang Y, Zhang L, Li Y, Chen L, Wang X, Guo W, Zhang X, Qin G, He SH, Zimmerman A, Liu Y, Kim IM, Weintraub NL, Tang Y (2015) Exosomes/microvesicles from induced pluripotent stem cells deliver cardioprotective miRNAs and prevent cardiomyocyte apoptosis in the ischemic myocardium. Int J Cardiol 192:61–69
Khan M, Nickoloff E, Abramova T, Johnson J, Verma SK, Krishnamurthy P, Mackie AR, Vaughan E, Garikipati VN, Benedict C, Ramirez V, Lambers E, Ito A, Gao E, Misener S, Luongo T, Elrod J, Qin G, Houser SR, Koch WJ, Kishore R (2015) Embryonic stem cell-derived exosomes promote endogenous repair mechanisms and enhance cardiac function following myocardial infarction. Circ Res 117(1):52–64
Teng X, Chen L, Chen W, Yang J, Yang Z, Shen Z (2015) Mesenchymal stem cell-derived exosomes improve the microenvironment of infarcted myocardium contributing to angiogenesis and anti-inflammation. Cell Physiol Biochem 37(6):2415–2424
Chistiakov DA, Orekhov AN, Bobryshev YV (2016) Cardiac extracellular vesicles in normal and infarcted heart. Int J Mol Sci 17(1):63
Ibrahim AG, Cheng K, Marban E (2014) Exosomes as critical agents of cardiac regeneration triggered by cell therapy. Stem Cell Reports 2(5):606–619
Ong SG, Lee WH, Huang M, Dey D, Kodo K, Sanchez-Freire V, Gold JD, Wu JC (2014) Cross talk of combined gene and cell therapy in ischemic heart disease: role of exosomal microRNA transfer. Circulation 130(11 Suppl 1):S60–S69
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2017 Springer Nature Singapore Pte Ltd.
About this chapter
Cite this chapter
Marini, M., Ibba-Manneschi, L., Manetti, M. (2017). Cardiac Telocyte-Derived Exosomes and Their Possible Implications in Cardiovascular Pathophysiology. In: Xiao, J., Cretoiu, S. (eds) Exosomes in Cardiovascular Diseases. Advances in Experimental Medicine and Biology, vol 998. Springer, Singapore. https://doi.org/10.1007/978-981-10-4397-0_16
Download citation
DOI: https://doi.org/10.1007/978-981-10-4397-0_16
Published:
Publisher Name: Springer, Singapore
Print ISBN: 978-981-10-4396-3
Online ISBN: 978-981-10-4397-0
eBook Packages: Biomedical and Life SciencesBiomedical and Life Sciences (R0)