
Abstract
Nowadays, there are different tools to understand geometric distribution of tumors in bones. Preoperative virtual planning (PVP) is an asset within the field of oncologic surgery. Surgeons are able to perform osteotomies with intraoperative virtual navigation (IVN) that shows the plan that was previously planned. These tools have started a brand-new paradigm in oncologic orthopedic: it is possible to reproduce a 3D osteotomy before the intervention and execute it with meticulous accuracy in a virtual platform. It opens a new field in medicine called “computerized assisted surgery” (CAS). The pelvis is geometrically complex; the use of PVP and IVN is an asset to improve potentially safety and quality during osteotomies. Moreover, these tools contribute potentially to decrease tumoral recurrence.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others

Keywords
- Preoperative virtual planning
- Intraoperative virtual navigation
- Computed-assisted surgery
- Virtual scenarios
- Bone tumor navigation
1 Introduction
Orthopedic oncologic literature has demonstrated that CAS is a useful and novel tool. PVP and IVN can potentially improve resection of tumors located in the pelvis (1,2,3,4,5) due to its geometrical complexity.
Formerly, surgeons planned their pelvic tumor surgery with a bidimensional printed slice image from computerized tomography (CT) and magnetic resonance image (MRI). Surgeons study the films and integrate CT and MRI, taking the oncologic margin into account. For years, this method has been the only alternative presenting insufficient accuracy and tumor recurrence due to wrong cutting margins. However, poor preoperative information led to wider resections as to achieve oncologic security.
Recently, technological developments allow physicians to manipulate digital medical images. In this way, integration of CT and MRI in a virtual simulation scenario is possible (6, 7). This virtual environment has the ability to include 3D bone tumor reconstructions. Specialists use a virtual simulation scenario to plan the cuts before the intervention and then execute it under IVN. That is to say that physicians have greater knowledge of the tumor area, improving the accuracy of the intervention (8, 9). The aim of this chapter describes the basics of PVP and its execution in pelvis sarcomas under IVN.
2 Preoperative Virtual Planning
PVP works in a virtual simulation scenario where it is possible to merge digital medical images. This platform is potentially reliable for physicians in order to decide about further surgical techniques for a better quality intervention.
Moreover, PVP is a tool that can be used to plan a case and address possible surgical techniques. PVP is a platform where many specialists of different areas can see the case’s approach together and interact before the real intervention.
Image acquisition protocols (CT and MRI) with cuts of 1 mm (millimeters) or less thickness were used.
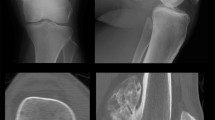
The requested CT and MRI are merged (image fusion), and the oncologic margins are defined within the virtual scenario. The oncologic margin is calculated with dots in the healthy bone tissue and tumor limits. Specialists, depending on the tumor histology, measure the distances and determine the safe margins. In tumors such as in low-grade chondrosarcoma cases without edema, the oncologic margin limit is easy to define between healthy and pathologic bone tissue (Fig. 5.1), whereas in other histological types such as Ewing tumors, the dots are more difficult to fix (Fig. 5.2).

This MRI slice shows that the limit between healthy and pathologic bone is clear since there is no edema

This image shows a case where the tumoral limit is difficult to determine. This is frequent in Ewing tumors
Each oncologic margin distance is unique according to the histological type and the definition of tumor limits. As general criteria in low-degree chondrosarcomas with no edema, the plan is done with a 5 mm margin, in osteosarcomas 1 cm, and in tumors with undefined limits 2 cm or more.
After the process of defining the margins of the tumor, physicians start planning the type of osteotomy they will perform in the OR. Each case is given a name after the number of planes in which it is going to be performed: uniplanar if it is only one plane, biplanar if there are two planes, and multi-planar if there are more than two planes (Fig. 5.3).

Planar configurations: each configuration receives a different nomenclature. (a) Uniplanar, (b) biplanar, and (c) multi-planar
The surgical approach is decided according to the proposed osteotomy; afterward, it is possible to perform a virtual resection. Specialists of different fields are able to actually see detailed features of the patient’s pelvis and its tumor after virtual resection previous to the real intervention (Fig. 5.4).

A virtual resection is shown. The surgical approach is decided after a resection plan is built and evaluated in the virtual scenario
Finally, after virtually resecting the tumor with its planned margins, physicians are able to foresee different reconstructive alternatives. Having access to the virtual library of banked allografts, bones allow to practice numerous reconstructions using structural bones (Fig. 5.5).

Nonregular structural bone reconstructions using allografts bone models digitally stored in the virtual bone bank
2.1 PVP Summary
-
1.
Study the tumor in MRI.
-
2.
Delineate margins according to histology.
-
3.
Determine the conformation of planar osteotomy: uni-, bi-, or multi-planar.
-
4.
Perform a virtual resection.
3 Intraoperative Virtual Navigation
Intraoperative virtual navigation (IVN) is the tool that executes PVP osteotomies.
This type of navigation is the optical navigation based on images, a system of infrared cameras (emission lights) found in specific instruments. The instrument is a tracker fixed on the patient and a pointer held by the surgeon. In this case, it has been used as active instrumental (powered by lithium batteries), although there is also passive instrumental (without batteries). The navigator has two monitors, one for technicians and other one for surgeons; both screens display the same (Fig. 5.6).

A navigation pointer in the front. In the back, the navigator screen showing the location of the tumor and the tip and angle of the pointer
The first important aspect to mention is the place we are going to designate to the physical navigator in the operating room. It is important to place the device in the operating room after the sterile fields have been placed so as not to disturb the surgeon and avoid contamination.
The device is placed opposite to the surgeon so he can see the camera 2 m from surgical approach.
It must be determined in PVP the fixing site of the registrar. The fixing is the insertion of two pins between 3 and 4 cm diameter in the bone. It is of great importance to dispose such pins far from the tumor area so as not to disturb the surgeon during the intervention as well as disposing the pins where the camera can visualize them. Once the tracker is fixed, specialists proceed with registration process. Through this process, the virtual bone from planning and the real bone of the patient are compared and matched. Registration process can be divided in two parts, a primary and a secondary.
During primary registration, it is numerically determined those recognized bones from 3D reconstruction which can be visualized after the approach. At least three landmarks are set. Then secondary registration consists of adding more landmarks to refine the area. This last step allows specialists to match completely 3D image with the real bone. In order to verify the accuracy of the process, specialists have to dispose the pointer over three different bone landmarks and corroborate visually that the pointer seen in 3D representation is found in air-bone interface (Fig. 5.7).

The pointer is used to visually verify the registration process. This is done by checking the air-bone interface area in well-known locations
The following step is to mark the cut path in the bone with methylene blue that also resembles with PVP.
After marking the bone, the osteotomy is done with the saw blade. The saw blade thickness is foreseen in PVP, so it is left a 2 mm cut thickness.
When osteotomy is initiated, IVN is an asset in order to guide the procedure. The pointer is placed in the created slot, visualizing the exact position on the navigator screen and trajectory by three bidimensional windows.
Finally, an ultimate control can be done with the pointer after tumor resection. It is pointed to the remnant defect in order to verify visually the exactness of the osteotomy.
3.1 IVN Summary
-
1.
Place the navigator device.
-
2.
Tracker fixation.
-
3.
Primary registration and secondary registration.
-
4.
Air-bone check over three spots.
-
5.
PVP navigation.
-
6.
Defect control.
4 Accuracy in PVP and IVN
An experimental design scans the surgically removed specimen in a CT in order to determine the accuracy of the above-described procedure. The following procedure is to reconstruct three-dimensionally the surgical specimen and superimpose it to PVP (Fig. 5.8). This allows physicians to perform a comparative study between osteotomies virtually planned and those executed.

The accuracy evaluation workflow. (a) The surgical specimen is CT scanned; (b) the preoperative plan is registered against the surgical specimen; (c) the distances from the osteotomy surface to the planar cut are measured; (d) the measured data is displayed so the surgeon can perform adjustments
Although the first impression of the comparative study is a visual appreciation, virtual reconstructions and planes can be transformed into a map of dots (Fig. 5.8). This enables physicians to measure dot to dot, obtaining as a result a numeric value. A comparative study informs physicians quantitatively the accuracy between planned and executed.
The values can be expressed by colored graphs (colorimetric). For instance, green color is given when planned and executed osteotomy match. Red color is given when the osteotomy dangerously approached the tumor, and blue color is given when osteotomy shifted away from the tumor. Colorimetric graphics depict cut pathways behavior tridimensionally (Fig. 5.8).
5 Conclusion
PVP and IVN are tools used in the novel field of computerized assisted surgery area. They are important assets to perform pelvic sarcomas resections as they provide potentially optimal surface approach before surgery. Furthermore, these tools give specialists the necessary instruments to study a case in depth before the intervention and to prevent unexpected situations. Executing what was previously planned supported by accurate tridimensional images potentially improves safeness, quality, and, foremost important, predictability in osteotomies during oncologic surgery.
References
Cho HS, Kang HG, Kim HS, et al. Computer-assisted sacral tumor resection. A case report. J Bone Joint Surg. 2008;90-A:1561–6.
So T, Lam YL, Mak KL. Computer-assisted navigation in bone tumor surgery: seamless workflow model and evolution of technique. Clin Orthop Relat Res. 2010;468:2985–91.
Jeys L, Matharu GS, Nandra RS, Grimer RJ. Can computer navigation-assisted surgery reduce the risk of an intralesional margin and reduce the rate of local recurrence in patients with a tumour of the pelvis or sacrum? Bone Joint J. 2013 Oct;95-B(10):1417–24. https://doi.org/10.1302/0301-620X.95B10.31734.
Wong K-C, Kumta S-M. Use of computer navigation in orthopedic oncology. Curr Surg Rep. 2014;2:47. https://doi.org/10.1007/s40137-014-0047-0.
Bird JE. Advances in the surgical management of bone tumors. Curr Oncol Rep. 2014;16:392. https://doi.org/10.1007/s11912-014-0392-2.
Wong K, Kumta S, Antonio G, et al. Image fusion for computer assisted bone tumor surgery. Clin Orthop Relat Res. 2008;466:2533–41.
Aponte-Tinao L, Ritacco LE, Ayerza MA, Luis Muscolo D, Albergo JI, Farfall GL. Does intraoperative navigation assistance improve bone tumor resection and allograft reconstruction results? Clin Orthop Relat Res. 2015;473(3):796–804.
Ritacco LE, et al. Accuracy of 3-D planning and navigation in bone tumor resection. Orthopedics. 2013;36(7):e942–50.
Cho HS, Oh JH, Han I, Kim HS. The outcomes of navigation-assisted bone tumour surgery: minimum three-year follow-up. J Bone Joint Surg Br. 2012;94(10):1414–20.
Acknowledgments
To Florencia Figar Laborde for translating and editing this manuscript.
Disclosure: Dr. Aponte-Tinao is a paid consultant for Stryker. Drs. Ritacco, Milano, Farfalli, Ayerza, and Muscolo have no relevant financial relationships to disclose.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2020 Springer Nature B.V.
About this chapter

Cite this chapter
Ritacco, L.E., Milano, F.E., Farfalli, G.L., Ayerza, M.A., Muscolo, D.L., Aponte-Tinao, L.A. (2020). Staging, Preoperative, and Surgical Planning. In: Guo, W., Hornicek, F., Sim, F. (eds) Surgery of the Pelvic and Sacral Tumor. Springer, Dordrecht. https://doi.org/10.1007/978-94-024-1945-0_5
Download citation
DOI: https://doi.org/10.1007/978-94-024-1945-0_5
Published:
Publisher Name: Springer, Dordrecht
Print ISBN: 978-94-024-1943-6
Online ISBN: 978-94-024-1945-0
eBook Packages: MedicineMedicine (R0)