
Abstract
Background
Child sexual and physical abuse types were studied more extensively than emotional abuse and neglect. In recent years an increasing amount of community based studies on the long term outcomes of emotional abuse and neglect were published. However, only few studies compared between the risk for psychopathology associated with different types of child abuse.
Aim
To review the current knowledge on the long term effects of child abuse as indicated in epidemiological studies.
Methods
A review of the literature published since year 2000–2012. The chapter will include population based studies of any type of abuse. As an outcome we will focus on three types of psychopathologies: mood and anxiety disorders, representing Axis I (DSM-IV), and personality disorders, representing Axis II disorders.
Conclusions
The review of the evidence suggests strong and reliable relationship between child abuse and psychopathology in adulthood. Emerging evidence indicate that child neglect and emotional abuse may be as harmful as sexual and physical abuse.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others

Keywords
- Anxiety Disorder
- Child Abuse
- Obsessive Compulsive Disorder
- Personality Disorder
- Generalize Anxiety Disorder
These keywords were added by machine and not by the authors. This process is experimental and the keywords may be updated as the learning algorithm improves.
Introduction
The 1989 United Nations Convention on the Rights of the Child states that children should be protected from all forms of physical or mental violence, injury or abuse, neglect or negligent treatment, maltreatment or exploitation (Art. 19). As repeatedly documented, the failure of such protection is a risk factor for psychopathology early in life (cf. Herrenkohl and Herrenkohl 2007) and even years later (Caspi et al. 2008; Chapman et al. 2004; Duncan et al. 1996; Gal et al. 2011; Green et al. 2010; Kessler et al. 1997, 2010; MacMillan et al. 2001; Molnar et al. 2001; Mullen et al. 1996; Stein and Barrett-Connor 2000; Widom et al. 2007). Most of these studies, though, either considered only a single type of child abuse (CA), such as sexual or physical abuse, or employed a composite measure that was not sensitive to differential effects of specific abuse type. Only a few studies compared associations of CAs with different types of mental disorders or examined changes in CA effects over the life course.
The current approach to child abuse refers to 4 categories: sexual-, physical-, emotional-abuse, and neglect. Each of these types of abuse can occur singly or in combination with other types of abuse, as well as other childhood adversities (CAs). By and large, child sexual abuse (CSA) and physical abuse (CPA) were studied more extensively than emotional abuse and neglect. In addition, while some studies reported on outcomes of emotional abuse and neglect, they were mostly based on specific, mainly clinical, populations which do not allow firm conclusions. However, in recent years an increasing amount of attention is being placed on the adverse effects of emotional abuse and neglect and their life-long outcomes were studied in community-based, samples as well.
The current chapter will present data on the long term outcomes of all types of abuse. Methodological attention will be given to specific aspects. First, although most studies used retrospective designs a few prospective cohort studies were published, giving additional support to the findings. Second, theoretical propositions were made regarding gender differences in the vulnerability to long term outcomes following child abuse (Cutler and Nolen-Hoeksema 1991). Some reports on the short term impact of CA indicated that boys are more prone to develop externalizing behaviors such as aggression, impulsivity and defiance in response to abuse, whereas girls are at risk for internalizing problems, including depression, low self-confidence, somatic complains and social withdrawal (Darves-Bornoz et al. 1998; Herrenkohl and Herrenkohl 2007; Widom 1999). However, investigations into sex differences with regard to long-term outcomes in adulthood related to child abuse are missing (Herrenkohl et al. 2008). Third, most studies considered adult Axis I disorders of the DSM-IV (APA 2000) such as mood, anxiety, impulse control, and substance use disorders. Fewer studies focused on the link between childhood adversity and Axis II personality disorders (PDs), which are generally persistent overtime and are often represented by patterns of behaviours and experiences that can negatively impact areas of cognition, affect, and interpersonal functioning (American Psychiatric Association 2000).
Objectives
To review the current knowledge on the long term effects of child abuse as indicated in the epidemiological field of research. We will review literature published since year 2000–2012. The chapter will include studies focusing on CSA, CPA, emotional abuse and neglect, as well as studies combining these types. As an outcome we will focus on 3 types of common psychopathologies: mood and anxiety disorders, representing Axis I, and PDs, representing Axis II disorders.
Methods
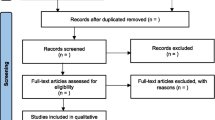
We conducted a systematic review of available studies published between January 1st 2000 and December 31st 2012.
Child Sexual Abuse
Mood Disorders
This is probably the most robust finding on the long-term effects of child abuse. The majority of these studies applied retrospective methodology and 4 were prospective. Most studies reported lifetime prevalence, while 5 studies reported current (mainly 12-months) mood disorders. Eleven retrospective and two prospective studies have indicated increased risk for lifetime mood disorders (OR range 1.4–3.9). No significant associations were reported by 2 studies (retrospective and prospective). Five studies investigated the risk for 12-months mood disorders, yielding inconsistent findings. Hovens et al. (2010) reported on increased risk for both seldom (OR = 1.9) and frequent (OR = 3.4) mood and anxiety disorders, while the 2 other studies indicated a mild significant association (OR range 1.1–1.3) (Gal et al. 2011; Chapman et al. 2004; Hanson et al. 2001; Spatz-Widom et al. 2007).
Five studies differentiated between male and female subjects (Afifi et al. 2008; Chapman et al. 2004; Dinwiddie et al. 2000; Macmillan et al. 2001; Molnar et al. 2001). Although similar range were indicated among females (OR range 1.8–3.9) and males (OR range 1.8–3.9), the studies were inconsistent in determining differential risk to develop mood disorders between genders. Based on 2 replications of the National Comorbidity Survey in the USA, as well as the US ACE study, similar associations were reported for females and males for CSA and lifetime mood disorders (Afifi et al. 2008; Chapman et al. 2004; Molnar et al. 2001), as well as current mood disorders (OR females 2.0, males 1.6) (Chapman et al. 2004). However, 2 other studies reported that although significant associations were present for both genders, they were more robust in either males or females. Based on a Canadian sample, Macmillan et al. (2011) observed a higher risk among females (OR = 3.9) than males (OR = 1.9). In contrast, based on an Australian sample, Dinwiddie et al. (2000) reported a lower risk among females (OR = 2.2) than males (OR = 3.9).
Anxiety Disorders
Some studies explored the impact of CSA on the risk for lifetime anxiety disorders (Lindert 2014). Several studies (Gal et al. 2011; Green et al. 2010) found significant associations, while other studies (Fujiwara and Kawakami 2011) did not find a such associations. Some studies differentiated between males and females (Afifi et al. 2008; Cougle et al. 2010; Macmillan et al. 2001). Other studies (Afifi et al. 2008; Macmillan et al. 2001) reported significant findings between sexual abuse and anxiety disorders (OR = 1.6; 2.4, respectively) but not among males (OR = 1.5; 1.2, respectively).
Posttraumatic Stress Disorder
Both Cougle et al. (2010) and Molnar et al. (2001) reported gender effects on the association between CSA and PTSD. Cougle et al. (2010) reported an increased risk for PTSD among both females (OR = 2.6) and males (OR = 2.4). A more robust effect was indicated by Molnar et al. (2001) both among females (OR = 10.2) and males (OR = 5.3).
Panic Disorder
Six studies referred to panic disorder (Cougle et al. 2010; Dinwiddie et al. 2000; Goodwin et al. 2005; Jonas et al. 2011; Kendler et al. 2000; and Molnar et al. 2001) and yielded significant associations (OR range: 1.9–5.0) with the exception of Molnar et al. (2001). Two studies, one in the USA (Cougle et al. 2010) and the other in Australia (Dinwiddie et al. 2000) found an increased risk for panic disorder following CSA both in females (OR = 2.0; 3.5) and males (OR = 1.9; 5.0), respectively. Drawing on an earlier US survey, Molnar et al. (2001) did not indicate a significant association among both genders (OR females 1.4; males 0.8). Goodwin et al. (2005) were alone in exploring the risk of experiencing panic attacks, reporting a strong relationship (OR = 4.1).
Two studies explored social phobia and have reported inconsistent results. Cougle et al. (2010) indicated increased risk among both females (OR = 1.6) and males (OR = 2.3), while, Dinwiddie et al. (2000) found a strong association for females (OR = 3.4) but not for males (OR = 1.0). Jonas et al. (2011) were the only study exploring the association between CSA and phobia and OCD, and found significant increases in risk for both (OR = 2.1; 1.8 respectively).
Personality Disorders
Two studies explored long term outcomes of CSA on personality disorders (PDs). Afifi et al. (2011) indicated an increased risk for Cluster A (OR = 1.2), Cluster B (OR = 1.6), but not for Cluster C (OR = 1.1) PDs. However, Moran et al. (2011) have indicated an increased risk for PDs as a function of the number of CSA episodes: for Cluster A (single event OR = 1.0, multiple OR = 2.7), Cluster B (single event OR = 1.9, multiple OR = 2.3), and Cluster C (single event OR = 0.9, multiple OR = 1.8).
Child Physical Abuse
Mood Disorders
Several studies investigated the effects of CPA on the risk of developing lifetime mood disorders in adulthood (Lindert et al. 2014). Some (Fujiwara and Kawakami 2011; Green et al. 2010; Wainwright and Surtees 2002) reported an increased risk for lifetime mood disorder following CPA (OR range 1.8–3.9). One study did not indicate significant associations (Gal et al. 2011).
Anxiety Disorders
Several studies explored the relationship between CPA and the risk of developing anxiety disorders (Lindert et al. 2014). Of them, 7 studies related to lifetime anxiety disorders. Some retrospective studies (Gal et al. 2011; Green et al. 2010; Macmillan et al. 2001 and some (Scott et al. 2010) reported on a significant increase in the risk for lifetime anxiety disorders following CPA (OR range 1.6–2.7), However, others (Fujiwara and Kawakami 2011) did not yield significant results. CPA, anxiety and gender.
Two studies reported on differential gender effects. Afifi et al. (2008) found an increased risk among males (OR = 2.3), but not among females (OR = 1.2). However, Macmillan et al. (2001) indicated an increased risk both among females (OR = 2.2) and males (OR = 1.7).
Panic Disorders
One study referred only to the risk of developing panic disorders (Goodwin et al. 2005), and found a significantly elevated risk following CPA (OR = 3.0). One study controlled for gender effects for various lifetime anxiety disorders (Cougle et al. 2010). Among females an elevated risk was observed for PTSD (OR = 1.7), generalized anxiety disorder (GAD) (OR = 1.4), and panic disorder (OR = 1.5), while among males an increased risk was found for post-traumatic stress disorder (PTSD) (OR = 2.4) and social anxiety (OR = 1.5).
Personality Disorders
Only one study (Afifi et al. 2008) explored the associations between CPA and personality disorder (PD). The risk of developing Cluster B PDs (OR = 1.4) was increased, while Cluster A and C PDs were not significantly associated (both ORs = 1.1) (Table 5.2).
Child Neglect
We identified several studies exploring the associations between childhood neglect and psychopathology in adulthood. Three studies explored the associations between PDs and childhood neglect. Johnson et al. (2001) reported on increased risk for Cluster A PD (OR = 3.5), while the other studies (Afifi et al. 2011; Cohen et al. 2001) found no such association (ORs = 1.1; 0.7, respectively). Similarly, a significant association between neglect and Cluster B PD was indicated in one study (OR = 1.3) (Afifi et al. 2011), but not in the 2 other studies (ORs = 1.7; 1.8) (Cohen et al. 2001; Johnson et al. 2001). Two studies (Afifi et al. 2011; Johnson et al. 2001) reported no significant association with Cluster C PD (ORs = 1.1; 1.8) (Table 5.3).
Child Emotional Abuse
Epidemiological research exploring the association between emotional abuse and psychopathology in adulthood is scarce (Table 5.1).
Two studies (Chapman et al. 2004; Ritchie et al. 2009) explored the association between emotional abuse and mood disorders. Ritchie et al. (2009) differentiated between 2 types of emotional abuse and indicated significant associations: verbal abuse (OR = 2.9) and humiliation (OR = 4.3). Chapman et al. (2004) explored the effects of insult or fear and controlled for gender, indicating an increased risk for both females and males: lifetime (ORs females 2.7; males 2.5) and 12-month (ORs F 3.1; M 3.3) disorders. Hovens et al. (2010) defined psychological abuse as being verbally abused, receiving undeserved punishment, being subordinated to siblings and being blackmailed. They reported on an increased risk for seldom (OR = 4.6), as well as frequent e (OR = 7.5) 12-months mood or anxiety disorders. A single report on the association of neglect with PDs (Afifi et al. 2011) indicated a significant increase of cluster A (OR = 1.3) and B (OR = 1.3), but not C (OR = 1.1) (Table 5.4).
Child Abuse and Psychopathology in Adulthood
We based this chapter on population based studies on the associations between child abuse and psychopathology in adulthood. The most consistent finding referred to the associations between CAs and lifetime mood disorders. A recent meta-analysis on the effects of child abuse indicated that across studies, physical abuse, emotional abuse and neglect lead to an increased risk for mood disorders (Norman et al. 2012; Lindert et al. 2014). According to our review, only few studies diverged from this pattern: 2 on CSA and 1 each on CPA and neglect. The studies which yielded negative outcomes following CSA were a retrospective study from Japan (Fujiwara and Kawakami 2011) and a prospective study from the USA (Spatz-Widom et al. 2007), a retrospective study from Israel on CPA (Gal et al. 2011) and a retrospective study from France on the associations with neglect (Ritchie et al. 2009). The Japanese study (Fujiwara and Kawakami 2011) reported on a very low rate of CSA, suggesting that the study did not have sufficient power to obtain significant results. However, the point estimation (i.e., the OR) itself was also very low representing only 30.0 % increase. The Israeli study (Gal et al. 2011) shares some common facts with the former Japanese study: they are both part of the World Mental Health Survey (WMHS) and are single reports from these countries. The rate of reported CPA in the Israeli study was relatively low (3.0 %) and although the point estimation indicated an elevated risk, the variability was too high to reach significance. It is more difficult to explain the lack of findings of Spatz-Widom et al. (2007) with regard to CSA since they did show significant increase following CPA and neglect. This negative finding could not be attributed to lack of power, since power was sufficient to yield a significant association with PTSD (Widom 1999). The French study (Ritchie et al. 2009) sampled an aged population of 65+ years and found no association between sexual and physical abuse, which both showed a very low rate. This same study indicated no association with childhood neglect, maybe due to the fact that it focused on late life psychopathology, while the outcome is more probable to appear earlier in life (Table 5.5).
In addition, the studies using AEs combinations arrive to the same conclusion, although not as definitively as those tat addresed each type of abuse separately. However, the larger variability of findings should be considered. One explanation of the heterogeneity of these findings is that it is not clear which adverse events (AEs) was included in the combination of some of the studies. Samples of interviewees reporting several CA exposures are more heterogeneous. However, the additive effect of CAs consistently indicates that subjects with a greater variety of maltreatment history are at greater risk for mood disorders.
A different picture is revealed when the effects on 12-months mood disorders are considered. Here, for most CAs the associations are not consistent and it is difficult to determine the nature of the association. For example, with regard to CSA 4 out of 5 studies did not indicate significant associations. It is possible that since, by definition less cases are defined with current compared to lifetime disorders, the number of diagnosed cases is small. Indeed, the only study that did observe significant findings (Hovens et al. 2010) lumped together mood and anxiety disorders and by that increased the number of the diagnosed sample. A similar pattern was observed with regard to CPA. Interestingly, a more consistent association was reported with regard to emotional abuse and neglect, but the number of studies is much smaller compared to CSA and CPA and that precludes drawing firm conclusions.
Anxiety Disorders
Lindert et al. (2014) and Norman et al. (2012) have indicated elevated risk of lifetime anxiety disorders following CPA and emotional abuse, but not neglect. According to the meta-analysis and the review of the associations with CSA ranged from an increase of 90–130 %, CPA studies showed a more consistent range of 60–170.0 %. However, only one study tested anxiety disorders following neglect, and no reports on emotional abuse were found. Only 2 studies on the associations between any of the CAs and current anxiety disorders were found and therefore it would be difficult to draw conclusions from the literature.
Further complexity was seen when specific types of anxiety disorders were considered. This was seen mainly with regard to CSA (8 studies), and to a lesser degree following CPA (2 studies). Relatively consistent findings were observed with regard to increased risk for PTSD and panic disorders, while the findings on GAD, social phobia, obsessive compulsive disorder (OCD) and panic attack were either scarce or inconsistent. Thus it would be difficult to draw conclusions with regard to specific composition of anxiety disorders which show elevated risk following CAs.
Personality Disorders
We identified 4 studies exploring the outcome of PDs, representing Axis II diagnoses, personality disorders (PD). The results widely differed between these studies, suggesting that the outcomes were not consistent across specific CAs. Afifi et al. (2011) have indicated that the risk for cluster B PDs was consistently elevated following CSA, CPA, emotional abuse and neglect. The findings were associated mainly with specific increase of borderline, antisocial and to a lesser degree narcissistic PDs. However, Moran et al. (2011) reported an increased risk of cluster B PDs only if repeated exposure to CSA was reported. The 2 other studies on neglect found no associations with cluster B PDs (Cohen et al. 2001; Johnson et al. 2001). This inconsistent pattern may be explained by the relatively large sample (N = 34,653) used by Afifi et al. (2011) which could enable the power to yield the associations between relatively infrequent events. Alternatively they could suggest a cohort effect in this report (Afifi et al. 2011). Associations with cluster A PDs were reported by 3 studies following CSA (Afifi et al. 2011; Moran et al. 2011) and neglect (Johnson et al. 2001), but not following CPA (Afifi et al. 2011) as well as the other studies on neglect (Afifi et al. 2011; Cohen et al. 2001). Thus the pattern of findings does not allow drawing conclusions. A significant association with cluster C PDs was reported by one study following repeated exposure to CSA (Moran et al. 2011), but not in all other studies exploring the associations between any type of CA and this cluster of PDs.
Gender Differences in Outcomes
Some of the studies differentiated between females and male outcomes following CAs. The findings were inconsistent. A review on the associations between gender and psychiatric outcomes following CSA, CPA and neglect has concluded that the associations among adult samples are complex (Gershon et al. 2008).
While Gershon et al. (2008) concluded that adult samples either show greater risk in females than males, or that there are no gender differences, our findings point to a different conclusion. Thus, according to studies reported here males after exposure to CSA and CPA are at greater risk for both, mood and anxiety disorders, compared to females. Similarly, such findings were reported on mood disorders following either CSA (Dinwiddie et al. 2000) or CPA (Afifi et al. 2008), anxiety and social anxiety following CPA (Afifi et al. 2008; Cougle et al. 2010), and anxiety following CSA or CPA (Gal et al. 2011). Taken together the current data are heterogeneous and need further careful investigation.
Theoretical Considerations
The studies reviewed here provide evidence of a dose–response relationship between child maltreatment and psychopathology, such that those experiencing more CAs were at greater risk of developing mental disorders than those experiencing lesser maltreatment (Chapman et al. 2004; Green et al. 2010; Moran et al. 2011; Perez-Fuentes et al. 2012). However, it is important to note that while some of the studies reported on the accumulating effects of similar AEs (e.g., CSA), other have reported on sum of events which could be different in nature (e.g., parental death or divorce). With regard to the former, Perez-Fuentes et al. (2012) have clearly indicated that an increase of exposure to CSA is associated with an increased risk for mood from OR of 2.8 following a single event to 4.2 following 4 events, and anxiety from 2.7 to 5.2. The study of Moran et al. (2011) has shown same pattern of increased risk on PDs.
Consistent dose–response relationships with repeated types of AEs have been reported for mood (Afifi et al. 2008; Anda et al. 2006; Chapman et al. 2004; Green et al. 2010) and anxiety (Afifi et al. 2008; Anda et al. 2006; Fujiwara and Kawakami 2011; Green et al. 2010) disorders. Interestingly, 2 studies have indicated that that the addition of CAs becomes less significant with the increase of CAs (Green et al. 2010; Kessler et al. 2010). This has an important implication for intervention. It means that prevention or amelioration of a single type of AEs among individuals exposed to many is probably not enough to yield a positive outcome. Thus, early intervention to reduce all types of maltreatment should be carried out in order to significantly reduce the negative outcomes of such AEs.
While most studies focused on the severity or frequency of AEs, Hovens et al. (2010) have enquired on the severity of the outcome. Since psychopathology in community samples is mostly reported in binary terms of present/not present it is not possible to identify cases on the basis of the severity of mental health outcomes (Table 5.4).
Outlook
Both prospective and retrospective studies were invetigated for the association between exposure to child adversities and psychiatric outcomes. The availability of prospective studies could provide conclusive evidence of a temporal relationship between exposure to child maltreatment and the later development of mental health outcomes. However, only 5 studies were prospective, and 2 additional studies had both prospective and retrospective directionality. Thus, the majority of the studies were cross-sectional and relied on adult retrospective report of abuse and neglect in childhood. By definition, these studies cannot prove a temporal relationship between exposure to child maltreatment and the onset of health outcomes.
Furthermore, retrospective, self-reported information regarding AEs may be subject to recall bias. In many cases participants were asked to report on events that occurred many years before, and the issue of potentially unreliable recall threatens the validity of the published literature on child maltreatment. At least with respect to child sexual abuse, Kendler et al. (2000) noted that it is unlikely that people reporting symptoms are more prone to report other events when the latter refers to a highly undesirable experience. In addition, it has been suggested that biases are probably towards under-reporting rather than over-reporting of abuse (Maughan and Rutter 1997). If the latter proposition is correct then the results probably underestimated the true association with regard to the overall rates (Fergusson et al. 2000).
Conclusion
This overview of the evidence suggests a strong and reliable relationship between CAs and psychopathology in adulthood. There is also emerging evidence that neglect and emotional abuse in childhood may be as harmful as sexual and physical abuse. While such conclusions have been drawn before from single empirical studies, the current chapter demonstrates more communal and replicable effects.
This review contributes to a better understanding and measurement of mental health impact of child maltreatment. All forms of child maltreatment should be considered as part of the cluster of interpersonal violence risk factors in global risk assessments for adult mental health.
Attributable burden is likely to be substantial, given the high prevalence of CAs, the strong associations indicated in our review, and the fact that the mental health outcomes are relatively frequent and among the leading causes of disease burden globally. Despite the magnitude of the problem and increasing awareness of its high social costs, preventing child maltreatment is not a political priority in most countries. It is imperative that public health studies will find their proper place leading national and international efforts to understand and prevent all variants of child maltreatment.
References
Afifi, T. O., Enns, M. W., Cox, B. J., Asmundson, G. J., Stein, M. B., & Sareen, J. (2008). Population attributable fractions of psychiatric disorders and suicide ideation and attempts associated with adverse childhood experiences. American Journal of Public Health, 98, 946–952.
Afifi, T. O., Boman, J., Fleisher, W., & Sareen, J. (2009). The relationship between child abuse, parental divorce, and lifetime mental disorders and suicidality in a nationally representative adult sample. Child Abuse & Neglect, 33, 139–147.
Afifi, T. O., Mather, A., Boman, J., Fleisher, W., Enns, M. W., MacMillan, H., & Sareen, J. (2011). Childhood adversity and personality disorders: Results from a nationally representative population-based study. Journal of Psychiatric Research, 45, 814–822.
American Psychiatric Association. (2000). Diagnostic criteria from DSM-IV-TR. Washington, DC: American Psychiatric Association.
Anda, R. F., Felitti, V. J., Bremner, J. D., Walker, J. D., Whitfield, C. H., Perry, B. D., Dube, S. R., & Giles, W. H. (2006). The enduring effects of abuse and related adverse experiences in childhood. European Archives of Psychiatry and Clinical Neuroscience, 256, 174–186.
Caspi, A., Vishne, T., Sasson, Y., Gross, R., Livne, A., & Zohar, J. (2008). Relationship between childhood sexual abuse and obsessive compulsive disorder: Case control study. Israel Journal of Psychiatry and Related Sciences, 45, 177–182.
Chapman, D. P., Whitfield, C. L., Felitti, V. J., Dube, S. R., Edwards, V. J., & Anda, R. F. (2004). Adverse childhood experiences and the risk of depressive disorders in adulthood. Journal of Affective Disorders, 82, 217–225.
Cohen, P., Brown, J., & Smailes, E. (2001). Child abuse and neglect and the development of mental disorders in the general population. Development and Psychopathology, 13, 981–999.
Cougle, J. R., Timpano, K. R., Sachs-Ericsson, N., Keough, M. E., & Riccardi, C. J. (2010). Examining the unique relationships between anxiety disorders and childhood physical and sexual abuse in the National Comorbidity Survey-Replication. Psychiatry Research, 177, 150–155.
Cutler, S. E., & Nolen-Hoeksema, S. (1991). Accounting for sex differences in depression through female victimization: Childhood sexual abuse. Sex Roles, 24, 425–438.
Darves-Bornoz, J. M., Choquet, M., Ledoux, S., Gasquet, I., & Manfredi, R. (1998). Gender differences in symptoms of adolescents reporting sexual assault. Social Psychiatry and Psychiatric Epidemiology, 33, 111–117.
Dinwiddie, S., Heath, A. C., Dunne, M. P., Bucholz, K. K., Madden, P. A. F., Slutske, W. S., Statham, D. B., & Martin, N. G. (2000). Early sexual abuse and lifetime psychopathology: A co-twin-control study. Psychological Medicine, 30, 41–52.
Duncan, R. D., Saunders, B. E., Kilpatrick, D. G., Hanson, R. F., & Resnick, H. S. (1996). Childhood physical assault as a risk factor for PTSD, depression, and substance abuse: Findings from a national survey. American Journal of Orthopsychiatry, 66, 437–448.
Fergusson, D. M., Woodward, L. J., & Horwood, L. J. (2000). Risk factors and life processes associated with the onset of suicidal behaviour during adolescence and early adulthood. Psychological Medicine, 30, 23–39.
Fujiwara, T., & Kawakami, N. (2011). Association of childhood adversities with the first onset of mental disorders in Japan: Results from the World Mental Health Japan, 2002–2004. Journal of Psychiatric Research, 45, 481–487.
Gal, G., Levav, I., & Gross, R. (2011). Psychopathology among adults abused during childhood or adolescence: Results from the Israel-based world mental health survey. The Journal of Nervous and Mental Disease, 199, 222.
Gershon, A., Minor, K., & Hayward, C. (2008). Gender, victimization, and psychiatric outcomes. Psychological Medicine, 38, 1377–1391.
Goodwin, R. D., Fergusson, D. M., & Horwood, L. J. (2005). Childhood abuse and familial violence and the risk of panic attacks and panic disorder in young adulthood. Psychological Medicine, 35, 881–890.
Green, J. G., McLaughlin, K. A., Berglund, P. A., Gruber, M. J., Sampson, N. A., Zaslavsky, A. M., & Kessler, R. C. (2010). Childhood adversities and adult psychiatric disorders in the national comorbidity survey replication I: Associations with first onset of DSM-IV disorders. Archives of General Psychiatry, 67, 113.
Hanson, R. F., Saunders, B., Kilpatrick, D., Resnick, H., Crouch, J. A., & Duncan, R. (2001). Impact of childhood rape and aggravated assault on adult mental health. American Journal of Orthopsychiatry, 71, 108–119.
Herrenkohl, T. I., & Herrenkohl, R. C. (2007). Examining the overlap and prediction of multiple forms of child maltreatment, stressors, and socioeconomic status: A longitudinal analysis of youth outcomes. Journal of Family Violence, 22, 553–562.
Herrenkohl, T. I., Sousa, C., Tajima, E. A., Herrenkohl, R. C., & Moylan, C. A. (2008). Intersection of child abuse and children’s exposure to domestic violence. Trauma, Violence & Abuse, 9, 84–99.
Hovens, J. G. F. M., Wiersma, J. E., Giltay, E. J., Van Oppen, P., Spinhoven, P., Penninx, B. W. J. H., & Zitman, F. G. (2010). Childhood life events and childhood trauma in adult patients with depressive, anxiety and comorbid disorders vs. controls. Acta Psychiatrica Scandinavica, 122, 66–74.
Johnson, J. G., Cohen, P., Smailes, E. M., Skodol, A. E., Brown, J., & Oldham, J. M. (2001). Childhood verbal abuse and risk for personality disorders during adolescence and early adulthood. Comprehensive Psychiatry, 42, 16–23.
Jonas, S., Bebbington, P., McManus, S., Meltzer, H., Jenkins, R., Kuipers, E., Cooper, M. K., & Brugha, T. (2011). Sexual abuse and psychiatric disorder in England: Results from the 2007 Adult Psychiatric Morbidity Survey. Psychological Medicine, 41, 709–719.
Kendler, K. S., Bulik, C. M., Silberg, J., Hettema, J. M., Myers, J., & Prescott, C. A. (2000). Childhood sexual abuse and adult psychiatric and substance use disorders in women: An epidemiological and cotwin control analysis. Archives of General Psychiatry, 57, 953.
Kessler, R. C., Davis, C. G., & Kendler, K. S. (1997). Childhood adversity and adult psychiatric disorder in the US National Comorbidity Survey. Psychological Medicine, 27, 1101–1119.
Kessler, R. C., McLaughlin, K. A., Green, J. G., Gruber, M. J., Sampson, N. A., Zaslavsky, A. M., Aguilar-Gaxiola, S., Alhamzawi, A. O., Alonso, J., Angermeyer, M., Benjet, C., Bromet, E., Chatterji, S., de Girolamo, G., Demyttenaere, K., Fayyad, J., Florescu, S., Gal, G., Gureje, O., Haro, J. M., Hu, C. Y., Karam, E. G., Kawakami, N., Lee, S., Lépine, J. P., Ormel, J., Posada-Villa, J., Sagar, R., Tsang, A., Ustün, T. B., Vassilev, S., Viana, M. C., & Williams, D. R. (2010). Childhood adversities and adult psychopathology in the WHO World Mental Health Surveys. British Journal of Psychiatry, 197, 378–385.
Lindert, J., von Ehrenstein, O., Grashow, R., Gal, G., Braehler, E., Weiskopf, M. G. (2014). Sexual and physical abuse in childhood is associated with depression and anxiety over the life course: Systematic review and meta-analysis. International Journal of Public Health, 59, 359–72.
MacMillan, H. L., Fleming, J. E., Streiner, D. L., Lin, E., Boyle, M. H., Jamieson, E., Duku, E. K., Walsh, C. A., Wong, M. Y., & Beardslee, W. R. (2001). Childhood abuse and lifetime psychopathology in a community sample. American Journal of Psychiatry, 158, 1878–1883.
Maughan, B., & Rutter, M. (1997). Retrospective reporting of childhood adversity: Issues in assessing long-term recall. Journal of Personality Disorders, 11, 19–33.
Molnar, B. E., Buka, S. L., & Kessler, R. C. (2001). Child sexual abuse and subsequent psychopathology: Results from the National Comorbidity Survey. American Journal of Public Health, 91, 753–760.
Moran, P., Coffey, C., Chanen, A., Mann, A., Carlin, J. B., & Patton, G. C. (2011). Childhood sexual abuse and abnormal personality: A population-based study. Psychological Medicine, 41, 1311–1318.
Mullen, P. E., Martin, J. L., Anderson, J. C., Romans, S. E., & Herbison, G. P. (1996). The long-term impact of the physical, emotional, and sexual abuse of children: A community study. Child Abuse & Neglect, 20, 7–21.
Nelson, E. C., Heath, A. C., Madden, P. A., Cooper, M. L., Dinwiddie, S. H., Bucholz, K. K. (2002). Association between self-reported childhood sexual abuse and adverse psychosocial outcomes: Results from a twin study. Archives of General Psychiatry, 59, 139–145.
Norman, R. E., Byambaa, M., De, R., Butchart, A., Scott, J., & Vos, T. (2012). The long-term health consequences of child physical abuse, emotional abuse, and neglect: A systematic review and meta-analysis. PLoS Medicine, 9, e1001349.
Perez-Fuentes, G., Olfson, M., Villegas, L., Morcillo, C., Wang, S., & Blanco, C. (2013). Prevalence and correlates of child sexual abuse: A national study. Comprehensive Psychiatry, 54, 16–27.
Reinherz, H. Z., Paradis, A. D., Giaconia, R. M., Stashwick, C. K., & Fitzmaurice, G. (2003). Childhood and adolescent predictors of major depression in the transition to adulthood. American Journal of Psychiatry, 160, 2141–2147.
Ritchie, K., Jaussent, I., Stewart, R., Dupuy, A. M., Courtet, P., Ancelin, M. L., & Malafosse, A. (2009). Association of adverse childhood environment and 5-HTTLPR genotype with late-life depression. The Journal of Clinical Psychiatry, 70, 1281–1288.
Scott, K. M., Smith, D. R., & Ellis, P. M. (2010). Prospectively ascertained child maltreatment and its association with DSM-IV mental disorders in young adults. Archives of General Psychiatry, 67, 712–719.
Slopen, N., Williams, D. R., Seedat, S., Moomal, H., Herman, A., & Stein, D. J. (2010). Adversities in childhood and adult psychopathology in the South Africa Stress and Health Study: Associations with first-onset DSM-IV disorders. Social Science & Medicine, 71, 1847–1854.
Spatz Widom, C., DuMont, K., & Czaja, S. J. (2007). A prospective investigation of major depressive disorder and comorbidity in abused and neglected children grown up. Archives of General Psychiatry, 64, 49–56.
Stein, M., & Barrett-Connor, E. (2000). Sexual assault and physical health: Findings from a population-based study of older adults. Psychosomatic Medicine, 62, 838–843.
Wainwright, N. W. J., & Surtees, P. G. (2002). Childhood adversity, gender and depression over the life-course. Journal of Affective Disorders, 72, 33–44.
Widom, C. S. (1999). Posttraumatic stress disorder in abused and neglected children grown up. American Journal of Psychiatry, 156, 1223–1229.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2015 Springer Science+Business Media Dordrecht
About this chapter
Cite this chapter
Gal, G., Basford, Y. (2015). Child Abuse and Adult Psychopathology. In: Lindert, J., Levav, I. (eds) Violence and Mental Health. Springer, Dordrecht. https://doi.org/10.1007/978-94-017-8999-8_5
Download citation
DOI: https://doi.org/10.1007/978-94-017-8999-8_5
Published:
Publisher Name: Springer, Dordrecht
Print ISBN: 978-94-017-8998-1
Online ISBN: 978-94-017-8999-8
eBook Packages: MedicineMedicine (R0)