
Abstract
A unified approach for modeling shelter needs and health impacts caused by earthquake damage which integrates social vulnerability into the physical systems modeling approaches has been developed. The shelter needs and health impact models discussed here bring together the state-of-the-art casualty and displaced population estimation models into a comprehensive modeling approach based on multi-criteria decision support, which provides decision makers with a dynamic platform to capture post-disaster emergency shelter demand and health impact decisions. The focus in the shelter needs model is to obtain shelter demand as a consequence of building usability, building habitability and social vulnerability of the affected population rather than building damage alone. The shelter model simulates households’ decision-making and considers physical, socio-economic, climatic, spatial and temporal factors in addition to modeled building damage states. The health impact model combines a new semi-empirical methodology for casualty estimation with models of health impact vulnerability, and transportation accessibility to obtain a holistic assessment of health impacts in the emergency period after earthquakes.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
These keywords were added by machine and not by the authors. This process is experimental and the keywords may be updated as the learning algorithm improves.
4.1 Integrated Framework for Modeling Socio-economic Impacts
4.1.1 Introduction
Recent decades have seen an exponential growth in the physical impacts and losses from earthquakes throughout the world. The Great Wenchuan Earthquake in May 2008, the Haitian Earthquake of 2010, and the 2011 Great East Japan Earthquake provide poignant reminders of the susceptibility of communities to devastating loss of lives, livelihoods, and property from earthquake events. These disasters, plus many other smaller ones, illustrate how earthquakes adversely impact people and the communities in which they live, and the impacts of such events occur across geographic boundaries and at multiple scales affecting governments, institutions, economic sectors, livelihoods, and people.
There is a consensus within the scientific community that disasters associated with earthquakes are not wholly the product of the physical impacts of natural hazard events. Rather, these disasters are the outcome of the interaction between the earth’s biophysical systems, the engineered environment, and the social conditions inherent at particular places (Hewitt and Burton 1971; Mileti 1999; Wisner et~al. 2004). It is increasingly becoming clear that some people and groups are impacted differentially by damaging events, react differently in an event’s aftermath, adjust to its circumstances in dissimilar ways, and recover in a differential manner. These circumstances have stimulated great interest in understanding how to manage the associated seismic risk, adverse impacts, and loss.
The current state-of-the-art in earthquake loss estimation (ELE) software provides several parameters of direct socio-economic consequences which are needed to support effective decision making. These include parameters such as casualties, displaced persons, and business failures by industry, for example. However, poor linkages between damage to physical systems and resultant social consequences remain a significant limitation with existing hazard loss estimation models (Bostrom et~al. 2008). A new direction with earthquake loss estimation software, which has been developed by researchers of the Mid America Earthquake Center, is the inclusion of social vulnerability (Elnashai et~al. 2009). Although definitions and applications of social vulnerability vary within the literature (Cutter 1996), the concept is often described as the potential for harm and the ability of an individual or community to protect itself from damaging events (Cutter et~al. 2003; Wood et~al. 2010). Given equal exposure to seismic threats, two groups may vary in their social vulnerability due to internal societal characteristics where differences according to wealth, gender, race, class, history, and socio-political organization influence the patterns of loss, mortality, and the ability of communities to reconstruct following a disaster (Burton and Cutter 2008). Inclusion of social vulnerability into quantitative loss estimation frameworks allows for a more holistic measurement of risk. However, more work is needed to develop a systemic approach that quantitatively brings together these disparate research areas in social vulnerability research into a comprehensive modeling tool, which provides decision makers with a dynamic platform to capture post-disaster decisions, interactions and changes over time.
At the core of the SYNER-G project are the development of state-of-the-art modeling capabilities and a suite of software tools that can be utilized for the assessment and communication of earthquake risk through the integration of both physical and social vulnerability. Thus, one of the main aims in SYNER-G was to compute social losses (displaced population, shelter needs and health impacts) as an integrated function of hazard intensity, systemic vulnerability of physical systems and the social vulnerability of the population at risk. This way of conceptualizing integrated risk emphasizes the importance of understanding the interrelations between physical and social systems. In other words, how direct physical losses can potentially aggravate existing vulnerabilities in society and how vulnerabilities in society can ultimately lead to greater impacts from physical damage and losses.
4.1.2 Integrated Evaluation of Physical and Socio-economic Models
The impact of an earthquake on the infrastructure evolves in space with the time elapsed from the event. Different stakeholders have different interests and play distinct roles in the various phases of the disaster. Correspondingly they look at impact assessments according to their own particular needs and mandates. These three dimensions (time, space, stakeholders) are represented in Fig. 4.1, which allows the vulnerability and impacts on infrastructure systems to be operationalized. In particular, along the time-dimension three periods of a disaster – emergency, recovery and reconstruction – can be identified. The first period constitutes the immediate aftermath of the event and its short-term consequences where the damaged infrastructure operates in a state of emergency. In this phase emergency managers must deal with the demand generated by damaged infrastructure in terms of temporary shelter needs or hospitalization and treatment of victims. In the midterm recovery period, while the infrastructure progressively returns to a new state of normal functionality, the disruptions to businesses might be of interest to stakeholders in the insurance sector. In the long-term reconstruction period, national governments and multi-lateral organizations have to grapple with the costs of permanently rebuilding or upgrading/retrofitting damaged infrastructure, and mitigate the risk from the next event. From the perspective of systemic studies there are two distinct phases which are commonly addressed:

The three dimensions in an infrastructure vulnerability and impact studies
-
Emergency phase: short-term (a few days/weeks) at the urban/regional scale (e.g. Franchin et~al. 2006; Nuti and Vanzi 1998)
-
Economic recovery phase: medium to long-term, at the regional/national scale (e.g. Karaca 2005)
Furthermore, the position on the “time axis” of the analyst/observer with respect to the time-frame changes the goal of the systemic study:
-
Outside/before the time-frame: the goal of the system analyst is to forecast the impact in order to set-up preparedness, planning and mitigation measures. It is important to underline how the information basis in this case can be considered as constant.
-
Within the time-frame: the goal of the system analyst is that of providing the managers with a real-time decision support system, which updates the Infrastructure state based on the continuously incoming flow of information.
-
After the time-frame: the goal of the system analyst is to validate the models against occurred events.
The general methodology developed within the SYNER-G Project focuses on the short-term only, with emergency managers as the reference stakeholders, and with the goal of forecasting, before the event occurs, the expected impact in terms of dead, injured and displaced population, for the purpose of planning and implementing risk mitigation measures. The goal of the methodology developed within the SYNER-G project is to assess the seismic vulnerability of an infrastructure of urban/regional extension, accounting for all relevant and meaningful inter- and intra-dependencies among infrastructural components, as well as of uncertainties. As described in Chap. 2 (see Fig. 2.1), the model for the infrastructure consists of both physical models of the systems making up the infrastructure (e.g. building and building aggregates, transportation network, lifeline systems) as well as socio-economic models that take as an input the output of the physical models and provide the socio-economic consequences of the event. Thus, the integrated approach proposed in SYNER-G provides a framework to link the degree of damage and performance of inter-related physical systems to vulnerabilities and coping capacities in society to assess: (1) Impacts on displaced populations and their shelter needs, and (2) Health impacts on exposed populations and their health-care needs. Furthermore, disruption to transportation and lifeline networks (roads, pipelines, electricity and water supply) have important consequences on the recovery process and contribute to increased social disruptions within both shelter and health sectors.
There are various possible interactions of socio-economic models with physical vulnerability/loss estimation models. Figure 4.2 shows three possible entry points for socio-economic models. In many earthquake loss estimation models socio-economic models are brought in at the third entry point as linear “damage-consequence functions” for the estimation of direct social and economic losses from physical system parameters, such as, level of building damage. Bringing in socio-economic models at the first entry point shown in Fig. 4.2 as empirical models, requires the systematic collection of post-event social and economic post-earthquake data which is typically not feasible, given the perishable nature of such data and that it is currently not being collected in a systematic and coordinated fashion.

Possible interaction of socio-economic models with physical vulnerability/loss estimation models
In SYNER-G the socio-economic models are being brought in at the second entry point depicted in Fig. 4.2. Here, new methods have been developed to compute social losses (e.g., number of displaced people and casualties) as an integrated function of hazard intensity, vulnerability of physical systems and the social vulnerability of the population at risk. In this framework design it is assumed that interactive and causal processes take place between society and the physical systems it interacts with. For example, the loss of building habitability (derived from physical building and utility damage models) will play a major role in the decision to evacuate one’s domicile and seek public shelter. Here the interaction between building habitability, environmental factors (e.g., weather conditions) and social factors such as the occupants tenure status (home owner vs. renter), whether the occupant lives in a single family home or a multi-family apartment structure, the level of anxiety of aftershocks, etc., will ultimately form the integrated model that is used to determine an estimate of displaced populations after an earthquake.
4.1.3 Multi-criteria Decision Analysis Framework
The integration of multiple dimensions of vulnerability with diverse and complex linkages constitutes some of the most challenging questions in store for interdisciplinary research. Contributing to this is the fact that social vulnerability is a fundamentally relative phenomenon and not something that can be directly observed and measured (Birkmann 2006). Thus, one of the main objectives has been the adoption of an indicator system and common nomenclature which posits social vulnerability in relational terms with respect to both shelter and healthcare systems. In this regard, indicators are pieces of information that summarize the characteristics of a system or highlight what is happening in a system. An indicator is a quantitative or qualitative measure derived from observed facts that simplify and communicate the reality of a complex situation (Freudenberg 2003). Indicators reveal the relative position of the phenomena being measured and when evaluated over time, can illustrate the magnitude of change (a little or a lot) as well as direction of change (up or down; increasing or decreasing). The mathematical combination (or aggregation as it is termed) of a set of indicators is often termed an index or a composite indicator. Consequently, transparent and validated indicator systems, which characterize the different aspects sectors addressed here (i.e., shelter, health, transportation) have been defined.
The theoretical framework for integration of physical and social performance indicators is founded on the work of Cardona (2005). It provides an overview of not only the expected direct damages, but also the potential for aggravating impact of the direct damages by the social fragility and lack of resilience of the different sectors analyzed here. As shown in Fig. 4.3 a physical performance index is obtained, for each unit of analysis by interacting with the physical infrastructure models, whereas the total social impact index is obtained by multiplying the direct physical performance indices by an indirect impact factor, based on variables associated with the socio-economic conditions of each unit of analysis. In order to reduce the complexity of the total system for applied purposes, vulnerability in each system is operationalized by a set of discrete indicators, representing social vulnerability and coping capacities. The indicators and sub-indicators have been chosen according to the vulnerability factors and decision criteria identified for each system and are described in the subsequent sections.

Structure of the integrated framework for assessment of social impacts
The process of developing an integrated indicator framework for assessment of overall social impacts depicted in Fig. 4.4 consists of five main steps which should be passed in an iterative manner (Nardo et~al. 2005). These development steps are very similar to the main phases of the multi-criteria decision theory (MCDA) or multi-attribute-value theory (MAVT). Therefore, for the development of a hierarchical indicator framework for the shelter needs and health impacts models in SYNER-G, the methodological approaches used within a MAVT-Analysis were transferred to the vulnerability for each of the two sectors – shelter and health – analyzed. The MCDA/MAVT framework also provides the basis for developing the software system in SYNER-G as a decision-support tool for emergency planning by taking into account a broader range of expert judgment through the interactive modeling of indicator weights or complementing the existing system of indicators with additional available data (e.g., for the assessment of additional vulnerability dimensions).

Methodological steps of the development of a hierarchical indicator framework
4.2 Shelter Needs Model
4.2.1 Population Displacement Following Historic Earthquakes
For the planning of public shelter provisions in the aftermath of earthquakes the expected number of homeless persons and people seeking public shelter is an essential input for emergency managers. Few models exist that estimate the displaced or homeless population and the number of displaced persons seeking public shelter in an earthquake. Most Earthquake Loss Estimation (ELE) software providing input for displaced population are based on the HAZUS methodology which computes both displaced population as a linear consequence of building damage. For example 90 % of all occupants in severely damaged multi-family homes and 100 % of all occupants in extensively and completely damaged multi-family and single-family homes are assumed to be displaced according to the HAZUS model default conditions (FEMA 2003).
Looking at data from 457 historic earthquakes from 1900 to 2012 with destroyed or heavily damaged building data in the CATDAT Damaging Earthquakes Database (Daniell et~al. 2011), a linear trend (on a logarithmic scale) of displacement and building damage can indeed be observed (Fig. 4.5). This data shows that the number of displaced persons is generally a little less than one order of magnitude larger than the number of destroyed or severely damaged buildings. However, the data in Fig. 4.5 also shows that in many past events the number of displaced persons is much larger than can be accounted for only through the number of occupants in severely damaged or collapsed buildings. Observations from past earthquake events found in the literature show that the number of displaced persons after an earthquake not only depend on external factors like building damage, loss of utilities, and weather conditions but also from household internal socioeconomic and individual factors such as safety concerns or fear of aftershocks (see full literature review of factors influencing displacement in Khazai et~al. 2011a). The intention to leave can also be undermined through feasibility restraints, e.g. if the next shelter is too far away, if people are disabled or lack mobility. Even if households decide to leave their homes the final question is where they will find accommodation. Alternatives to public shelter are for example to stay with friend and family or in hotels. Thus, only a subset of the total population should be considered in computing demand for public shelter.

Relationship between severely damaged and destroyed buildings and displaced persons after earthquakes (n = 457 earthquakes from 1900 to 2012)
4.2.2 Shelter Demand Models
To determine shelter needs in Earthquake Loss Estimation, most software follow the HAZUS methodology, where displaced population (determined only from building damage) is multiplied by a factor that considers age, ownership, ethnicity and income to determine demand for public shelters. These four parameters were originally developed by the American Red Cross and were based on expert opinion along with historical data from the 1994 Northridge earthquake (Harrald et~al. 1992). New approaches have recently been developed which simulates households’ decision-making in seeking shelter and considers socio-economic, temporal and spatial factors in addition to housing damage and lifeline loss to estimate displaced and shelter seeking populations (Chang et~al. 2009; Wright and Johnston 2010; Khazai et~al. 2011c). For example, the model by Chang et~al. (2009) adopts an agent-based approach that utilizes census microdata on households and simulates households’ decision-making about post-earthquake shelter on the basis of their dwelling condition, risk perception, mobility, and resources.
A new approach is presented for modeling emergency shelter demand in SYNER-G by integrating shelter-seeking logic models into a systemic seismic vulnerability analysis and earthquake loss estimation software tool (Khazai et~al. 2012a). The selection of socio-economic vulnerability indicators and other factors in the shelter logic model are based on an in-depth literature survey of historic earthquakes and are derived and validated using statistical models. Thus a new advancement to shelter estimation methodology is being explored through three types of key inputs: (1) the “habitability” of buildings which combines inputs from the physical models (building usability, utility loss and climate factors) to provide information on the habitability of a building and can be used as a better determinant in influencing the decision to evacuate than building damage alone; (2) GIS-based shelter accessibility analysis as an input to the shelter seeking model – not discussed here; and (3) a multi-criteria decision model for implementing a shelter-seeking logic model based on complex socio-economic factors which ultimately lead to the decision to evacuate and seek public shelter. These three inputs are combined into a dynamic shelter model and software tool developed within the SYNER-G software platform to provide stakeholders an interactive framework in decision-making process for shelter planning and preparedness as well as resource allocation.
4.2.2.1 Building Habitability Model
The first step in the decision to evacuate after an earthquake is based on the structural stability of a building and functional lifeline structures, such as access to water gas and electric power services. Weather conditions can further aggravate potential displacement from damaged buildings with disrupted lifeline services. If a building is only slightly damaged and it is very cold and there are no possibilities to heat, that home will be uninhabitable. During other seasons and weather conditions the same building might be habitable. In a rare study surveying post-earthquake survivors about their shelter preferences, Chien et~al. (2002) found evidence that under normal weather conditions 67 % of the interviewees after the 1999 Chi-Chi earthquake chose to stay in nearby open fields or under a tent, whereas under wet or cold weather conditions only 17 % showed a preference for staying there. Similar to the Chi-Chi earthquake, cold weather played a major role in the choices of occupants who sought shelter in both of the last two major earthquakes: The 2011 Tohoku earthquake (Khazai et~al. 2011b) and the 2012 Van earthquake in Turkey (Wenzel et~al. 2012).
Building habitability is determined as a combination of the functionality of buildings (building usability), utility services and impending weather conditions and constitutes the first decision step in leaving or staying at home after an earthquake. Building usability is derived from a simplified semi-empirical approach as a function of the severity of observed damage to structural and non-structural elements of buildings. The usability model was developed based on a detailed survey of 305 buildings in the densely packed suburb of Pettino obtained from the Italian Department of Civil Protection after the 2009 L’Aquila earthquake. The six usability classes considered during the survey were reduced in this model to just three: buildings which are immediately non-usable (NU), partially usable (PU) or fully usable (FU). Using the Pettino database, Usability Ratios (UR) for buildings were derived for each of the three usability classes as a function of the damage data, reported according to six damage states (DS0 to DS5), which were also reduced to three damage states (none, yield, collapse). Usability ratios can be used then to estimate the number of persons in each of the three building usability classes (NFU, NPU, NNU). Using the Usability Ratios in Table 4.1, the number of persons in each of the three building usability classes can be obtained using the following expression:
where:
-
i = damage level (i = 1, …, 3)
-
N i = number of buildings having damage level i,
-
NO i = number of occupants (at the time of the event) in each building for each damage level i,
-
UR i = usability ratio (UR) for damage level i for each usability class
To determine building habitability the usability of buildings is considered together with utility loss in a systemic seismic vulnerability analysis (Cavalieri et~al. 2012). Non-usable buildings (NU) are also non-habitable. If a building is fully or partially usable, depending on the level of residual service in the utilities and the prevailing weather conditions at the time of impact, it can be habitable (H) or non-habitable (NH). For each utility, the level of residual service is satisfactory when the Utility Loss (UL), defined as one minus the ratio of satisfied to required demand, is lower than a threshold value (ULi < ULTi). The threshold values depend on Weather conditions and Building Usability and due to the subjective nature of perceptions, the Utility Loss Threshold (ULTi) should be established on a context-specific basis by the analyst. The total Utility Loss is a weighted average of ULi on each of the utilities, with weights wi provided by the analyst:
where:
-
j = utility systems (j = 1, …N UN with N UN = 2 in this application)
-
UL j = Utility Loss in system j
-
w j = weight associated with the importance of loss in utility system j in making the building uninhabitable
The percentage fully or partially usable buildings that are non-habitable (NH FU or NH PU ) is thus determined as the portion of buildings which have utility losses greater than the utility loss threshold value (UL ≥ UL T ). The Uninhabitable Building Index (UBI) is computed as the ratio of occupants of buildings that are uninhabitable to the total population (N) according to the following relationship:
where:
-
N FU , N PU , N NU = number of occupants in buildings that are fully, partially and non-usable
-
NH FU = percentage of fully usable buildings that are non-habitable, where UL ≥ ULT
-
NH PU = percentage of partially usable buildings that are non-habitable, where UL ≥ ULT
-
N d = number of dead persons estimated in a selected casualty model
4.2.2.2 Shelter-Seeking Decision Model
The basic elements of the logic model for the shelter demand model are based on the ideas of Chang et~al. (2009). The shelter model combines each of the decision steps (represented as an output indicator) shown in Fig. 4.6 in a weighted multi-criteria decision analysis framework according to the following scheme: D1 is given by an output indicator as the proportion of population residing in uninhabitable buildings criteria; D2 and D3 are a combination of a number of internal and external factors and given by an output indicator representing the desirability to evacuate criteria; and D4 is given by an output indicator representing the desirability to seek public shelter based on the access to resources criteria.

Proposed model framework for shelter seeking logic model
The decision to evacuate one’s home after an earthquake and to utilize public shelter is correlated with a variety of social and demographic factors (Tierney 2006). These decisions are also usually made at the household level; however, as was seen in the case of the L’Aquila earthquake the decision to evacuate can also be imposed by government authorities that make an evacuation of homes mandatory. A survey of disaster literature regarding post-earthquake sheltering demand provided an initial basis for selection of relevant socio-economic indicators related to the desirability to evacuate (Khazai et~al. 2012a; Braun 2011). The main factors influencing evacuation behavior were derived from 18 key studies and are shown in Fig. 4.7.

Number of nominations found for indicators influencing post-earthquake evacuation behavior in 18 studies surveyed
While the literature survey provides for a comprehensive wish list of indicators, an important requirement for operationalizing the approach is that it should be possible to quantitatively populate the socio-economic indicators based on an approach that can be harmonized at the European level for the urban scale of analysis; one of the aims of this study. As such, data was compiled from the EUROSTAT Urban Audit for European cities at the sub-city districts (SCD) level and used as a next step to pre-select the most relevant indicators from the Urban Audit that were found in the literature survey. In order to narrow down the selection of the most influential indicators from the Urban Audit and to assign a set of default weights a factor analysis was conducted with the Urban Audit data. Out of the 338 indicators described in the Urban Audit, data is available for only 44 indicators at the SCD level. The 44 indicators were analyzed for two periods: 1999–2002 (7,856 districts in 321 cities in 30 European countries); and 2003–2006 (2,972 districts in 173 cities in 24 European Countries). Principal component analysis (PCA) was used to calculate the inter-correlation between variables and a new set of transformed variables was created where the importance of each of the new variables in terms of the variability of the data is identified. It was found that close to 75 % of variation in data is represented by 8 dimensions shown in Table 4.2. Additionally, the PCA provides a possibility to model the relative influence of all data in terms of their explanatory power (i.e., how much of the statistical variation can be explained by each indicator).
The literature survey and the statistical models provide a set of candidates for operationalizing the shelter-seeking decision model presented in Fig. 4.6. The first step (D1) is determined through the building habitability analysis as discussed above. The following presents the methodology and indicator framework related to desirability to evacuate (D2 and D3) and desirability to seek public shelter (D4).
4.2.2.2.1 Desirability to Evacuate
The desirability to evacuate is a combination of factors related to a set of internal factors which is a reflection of perceived security and safety, as well as external factors forcing residents to leave (Table 4.3). Feeling safe at home (or the feeling that it is safer to leave) is subjective and depends on a large range of factors each with different perceived importance values and cultural contexts. As mentioned above the perception of weather conditions is compounded with the building damage and utility services disruptions. The resistance to evacuation is also influenced by sociological and economic factors, such as having strong social networks, belonging to a minority or being disabled, having enough knowledge and financial resources to protect oneself, and knowing where to obtain information. Other factors influencing the perceived security are conditions such as fear and anxiety of aftershocks or mistrust in safety evaluation of one’s home (green, yellow and red tags) which are more difficult to describe and define quantitatively through indicators. Thus, the desirability to leave is a combination of a complex set of social factors and is ultimately determined by the individual’s perception of the importance of each one of these factors in driving the decision to evacuate. While desirability to leave represents an internal driver to evacuation, the resistance to evacuation is also driven by external decisions imposed on the affected population, which in some cases may force them to evacuate (e.g., mandatory evacuation of an entire city centre as in 2009 L’Aquila earthquake, or a radiation advisory and evacuation radius, as in the aftermath of the 2011 Tohoku earthquake and tsunami). The equation for the desirability to evacuate (DE) is given as
where:
-
DE = Desirability to evacuate
-
w i = overall weight given to each indicator
-
I i = indicators representing the desirability to evacuate
-
EF = External Factors, derived from a GIS analysis and/or different evacuation scenarios
4.2.2.2.2 Desirability to Seek Public Shelter
Not all displaced population will seek public shelter, and some may find alternative shelter accommodation (e.g., rent motel rooms or apartments), stay with family and friends, or leave the affected area. For estimations of shelter demand it is necessary to account various factors that lead to populations seeking public shelter. Desirability to seek public shelter in this study is given by an indicator model related to the “Access to Resources” which accounts for both “push” factors (such as low income, lack of mobility or having no social networks) and “pull” factors (such as being too far from the shelter sites). The “push” factors are determined in terms of socio-economic drivers, while the “pull” factor is an input from a GIS-based shelter accessibility model (Khazai et~al. 2011a). The question of accessibility relates mostly to residents who are able to choose between different destinations (Table 4.4). The proximity and ease of access of shelter locations might be a key criteria for these households whose decision of leaving is not founded on aspects of vulnerability but on individual preferences. The Shelter Seeking Index (SSI) is then derived as an additive weighted sum of each of the indicators constituting the shelter seeking population and multiplied by how accessible each of the designated shelter sites are, according to:
where:
-
SSI = Shelter Seeking Index
-
w i = overall weight given to each indicator
-
I i = indicators representing shelter seeking population
-
AI = Accessibility Index, derived from a GIS distance-cost analysis to shelter sites
4.2.2.3 Multi-criteria Shelter Model
The integrated shelter needs model developed here is based on a multi-criteria decision theory (MCDA) framework which allows the bringing together of parameters influencing the physical inhabitability of buildings, with social vulnerability (and coping capacity) factors of the at-risk population to determine as well as external factors to determine the desirability to evacuate and seek public shelter. As shown in Fig. 4.8, the multi-criteria framework can be described schematically as composed of the two main criteria: overall population at risk of being displaced after an earthquake (DPI) and the proportion of this population likely to seek public shelter (SSI). Subsequently, the total demand for public shelter for a particular location (i.e., city district) can be described as a product of the population at risk of being displaced (D1, D2 and D3) to the population likely to seek public shelter (D4). This can be expressed by the equation below where w DPI and w SSI are the weights assigned to DPI and SSI, respectively:
where:
SSI is derived from a weighted index related to lack of access of resources indicators in a community or neighborhood, and DPI is given as occupants in uninhabitable buildings amplified by external and internal factors related to desirability to evacuate according to the following expression:

Decision criteria for computing Shelter Needs Index (SNI)
4.2.3 Shelter Demand Model Implementation
To demonstrate the shelter methodology it has been applied to the 2009 L’Aquila earthquake, where detailed data on post-earthquake Building Usability (AEDES Survey of 1,667 buildings); Socio-economic data for 106 fractions (ISTAT data); and Shelter Population data from April to August 2009 for 107 shelter sites (Italian Civil Defence) was used to validate the model (Khazai et~al. 2012c). For each Mixed Operations Centres (COM), information was collected about the number of shelter sites, the total number of shelters, and the population in the shelters. When shelter population evolution is compared between the different COMs as shown in Fig. 4.9, it can be seen that in most COMs a drop in shelter population is observed after the first month. The most drastic development is observed in COM 5, where there is a drop of almost 60 % in shelter population from April to May. Contrary is the development in COM 1 with an increase in people in shelter until end of June. This increase could partly account for the loss in COM 5 supporting the assumption that migration may have taken place between displaced populations of the different COMs.

Shelter population evolution in each COM after the 2009 L’Aquila event
The shelter model methodology was implemented into the Multi-Criteria Decision Analysis (MCDA) which is the basis of the software developed in SYNER-G (Khazai et~al. 2012b). The tool will allow stakeholders to display the Shelter Needs ranking of different neighborhoods using various output and visualization formats. The user can assign different importance (weights) to selected indicators and the tool can be used to discuss the weighting outcomes and interactively examine the variability of shelter demand in different areas for different weighting schemes, or for different earthquake scenarios. The rankings for shelter demand after the L’Aquila earthquake are shown in Fig. 4.10 for the eight COMs which had the overall coordinating role in their own territories for all rescue and shelter provision operations. First the Displaced Persons Index (DPI) is obtained as the number of occupants living in uninhabitable buildings (BHI) amplified by the Desirability to Evacuate Criteria. In this case, the proportion of persons in uninhabitable buildings was not modelled following the methodology but taken directly based on observed values of partially usable and non-usable buildings in each of the eight COMs from the AEDES Survey. Furthermore, in the calibration of the shelter model people living in the historical city centre were recommended to evacuate without consideration of unique building stability due to historical buildings and narrow alleys. Accordingly, the Desirability to Evacuate criteria accounts for forced evacuations in COM1, 2 and 5 (Fig. 4.10b).

Ranking of the displaced persons (left, 6a–c) based on the Building Habitability Index (BHI) and the desirability to evacuate criteria. Ranking of the Shelter Needs Index (right, 6d–f) based on the Desirability to Seek Shelter (SSI) criteria and the Displaced Persons Index. (a) Desirability to Evacuate. (b) Desirability to Evacuate (DE) given forced evacuation of city centre. (c) Displaced Persons Index (DPI). (d) Desirability to Seek Shelter. (e) Desirability to Seek Shelter (SSI) given Shelter Accessibility. (f) Shelter Needs Index (SNI)
To obtain the Shelter Needs Index shown in Fig. 4.10f, the Desirability to Seek Shelter Indicators (Fig. 4.10d) were obtained and amplified based on accessibility to shelter sites in the eight COMs (Fig. 4.10e). Finally, the Shelter Needs Index (SNI) is obtained as the interaction between the Displaced Persons Index and Shelter Seeking Index (SSI). Fig. 4.11 shows how the modeling approach can be used to capture the actual shelter demand conditions (given as the observed number of people in shelter camps normalized by total population in each COM). For example, based on building usability alone, COM 3 should have a lower shelter demand than COM 6 and 4. However, given the high desirability to evacuate and seek shelter based on socio-economic indicators, COM3 obtains a more realistic ranking.

Ratio of actual population in shelters (observed data) shown against the ranking of displaced persons and shelter needs in the eight COMs
4.3 Health Impact Model
4.3.1 Health and Healthcare System Impacts of Earthquakes
Health impacts after earthquakes include mortality and morbidity in term of injuries, disability, psychological effects, inadequate treatment of non-communicable and chronic diseases (e.g. problem with drug procurement), and increased transmission of infectious diseases (e.g., caused by parallel systems dysfunction such as water and sanitation). Health impacts are the result of direct consequences of the physical impact of the earthquake (collapsing buildings, falling objects, falls due to shaking, traffic accidents, secondary hazards such as tsunami or landslides), and additionally, systemic failures of healthcare systems and parallel infrastructure (water and sanitation system, emergency housing system, transport and communication system) can as well lead to increased secondary fatalities (Gunn 1995; Howard et~al. 1996; Ramirez and Peek-Asa 2005; Aldrich and Benson 2008).
Studies, models, and guidelines related to health impacts in earthquake engineering have focused largely on casualty estimation methodologies (Coburn and Spence 2002; FEMA 2006), and hospital performance largely in terms of physical damage to structural systems and in some cases nonstructural systems and equipment (e.g., HAZUS model, FEMA 2003). Casualty estimation methodologies generally exclude casualties due to secondary causes, and do not account for injuries which can digress to fatalities as a result of systemic failures of healthcare systems and parallel infrastructure (e.g., transport, power, etc.). Systemic failures in healthcare delivery and lack of access to food and shelter can also lead to the exaggeration of baseline diseases and increased transmission of communicable infectious diseases. Several researchers, have proposed methods to assess interrelated systems – structural, nonstructural, lifelines, and personnel – according to performance levels indicating functionality (Chang et al. 2009; Lupoi et~al. 2008; Yavari et~al. 2010). Furthermore, systemic vulnerabilities in the healthcare or infrastructure systems can aggravate the overall health impact after earthquakes beyond the direct fatalities, for example, by the exaggeration of baseline diseases and increased transmission of communicable infectious diseases.
Health impacts (mortality and morbidity, population in need of medical treatment) after earthquakes are also influenced or aggravated by social factors that are best described using the term social vulnerability. This includes latent vulnerability conditions in the at-risk population and systemic failure in the healthcare delivery system. Although there is wide evidence that social vulnerability is a key component for influencing health outcome of disasters (see Sect. 4.3.2.3), it is seldom linked to common formal and quantitative seismic loss estimates of injured people which provide direct impact on emergency health care services. To link social impacts of health and health-care services to a systemic seismic vulnerability analysis, a conceptual model on health and the health care systems has been developed in SYNER-G.
4.3.2 Basic Elements of the Health Impact Model
The aim of the Health Impact Model is to extend earthquake casualty estimation methods by developing a combined engineering and social science approach for modeling earthquake health impacts. As such, the approach presents a new method for modeling health impacts caused by earthquakes by linking casualty estimation methods typically used in Earthquake Loss Estimation (ELE) to key factors of individual health and health-care systems. The methodology provides an operational framework for implementing the different factors into an analytical hierarchical process model, and deploying them using indicators following the principles of Multi-criteria Decision Analysis. The integrated approach for estimating post-earthquake health impact with a special focus on social vulnerability is composed of the following basic components which are described in the following sections.
4.3.2.1 Casualty Estimation Model
Casualty estimation methodologies in earthquake engineering (Kawasumi 1954; Whitman et~al. 1975; Wiggins 1977; Christoskov and Samardjieva 1984, 2013; Coburn and Spence 2002; FEMA 2006, etc.) following earthquakes provide estimates of both injuries and fatalities, which is a key input to assist planners in determining the resources required to deal with the increased surge in the patients. Most models provide “in-door” casualty estimates from structural building collapse and some provide non-structural casualties as a ratio of structural damage. It has been observed that 80 % of fatalities attributed to earthquakes have been caused by the collapse of buildings (Coburn and Spence 2002). This has changed significantly with the past earthquakes in the last decade but the overall percentage has stayed around the same (77 %) with Marano et~al. (2010) from 749 fatal events from 1968 to 2008 and Daniell et~al. (2012) from 2020 fatal events from 1900 to 2012 that 71 % of deaths are due to earthquake shaking. As the construction of RC buildings is increasing, the portion of casualty victims in RC buildings is rapidly increasing. This can also be attributed to the fact that RC structures built in the poorer countries are highly vulnerable and when they collapse they are considerably more lethal and kill a higher percentage of their occupants than masonry buildings.
Starting with the first casualty model by Kawasumi (1954), earthquake casualty methodologies seek to define a relationship between a ground motion parameter and/or damaged buildings and the potential number of fatalities. In addition to models that rely on expert opinion (Whitman et~al. 1975; Wiggins 1977), others have attempted to empirically derive relationships between casualties and a form of magnitude, PGA or other ground motion parameters (Christoskov and Samardjieva 1984; Coburn 1986; RGELFE 1992 and Surahman 2000). Other approaches (Alexander 1982; Ohta et~al. 1983; de Bruycker et~al. 1985; Coburn and Spence 1992; Zuccaro and Cacace 2010) have used the damage state of a building after the event to estimate the potential casualties via empirically derived data.
The difficulty of correlating casualties to a ground motion parameter is due to the fact that different parts of the world design buildings and structures differently, thus there can be a large discrepancy in the damage patterns seen between two countries for the same PGA and such models are generally not transferrable to another region or context. There are also many difficulties in correlating casualties against building damage states, including: damage states are notoriously difficult to classify into correct brackets; non-structural or furniture related deaths are generally not taken into account; and the fact that in-depth fatality counts are generally not known for each building post-event with only scattered studies detailing these fatalities.
Many new and old methodologies are based primarily on intensity with Berberian (1978), Ohashi and Ohta (1983) and Coburn et~al. (1987) to name a few. Recent models of authors such as So (2009), Jaiswal and Wald (2010), Maqsood and Schwarz (2011) have concentrated on earthquake intensity as the hazard metric vs. population ratios or by the population in collapsed buildings using expert opinion related collapse ratios using historical data. By definition, intensity links hazard and damage in one measure and this method attempts to alleviate some of the key uncertainties in casualty estimation, which include:
-
Casualty statistics (types and numbers) from past earthquakes are often inconsistent and unreliable (i.e., lack of standardization of injury data and established methodologies for reporting casualty data).
-
Casualty statistics very often do not provide information about cause of death (e.g., structural, non-structural, other causes)
-
Casualty statistics do not discern which building type (e.g., RC, Masonry, etc.) the casualty figures come from
-
Lethality Ratios used in CEMs are often engineering factors and not based on empirical/historic data
-
Uncertainties in population per building (i.e., uncertainties and incompleteness of data relating occupants to building volume)
-
Uncertainties in building occupancy at the time of earthquake (day and night variability as well as seasonal variability due to inflow of tourists or students)
As a result of the many uncertainties existing casualty models have failed to convey the degree of confidence to which estimates are given. This is extremely important in any decision making process as administrators or policy makers must be aware of the margins of error to make informed decisions. The seismic community has so far failed to disseminate data and stimulate responses from national and government organizations effectively (Spence 2007).
4.3.2.1.1 Casualty Estimation Model in SYNER-G
As casualty ratios (CR) used in casualty loss estimation depend on the particular building typologies, building practices and living arrangements in each region, a global or pan-european casualty model is not feasible. The casualty model developed in SYNER-G provides an initial (direct) casualty estimate for occupants of buildings at the time of earthquake based on an original idea developed by Coburn and Spence (1992). However, the casualty model developed in SYNER-G has several new components and considerations compared to available casualty models. The features of the SYNER-G casualty model are described below:
-
The model estimates casualties from all damage states. Most casualty models determine casualty as a function of building collapse only. While building collapse is the dominant factor, So and Spence (2013) show using historic data (Pakistan, Indonesia and Peru) that casualties can also occur in moderate and low damage states.
-
The model estimates casualties using semi-empirical casualty ratios. The process of determining casualty ratios is often unclear and in many cases it is an engineering judgement based on historic evidence. The model optimizes casualty ratios for regions with comparable building construction.
-
In addition to determining casualty ratios as a function of building damage, the model also considers Seismic Intensity.
-
The model estimates casualties by proposing a “Building-Casualty” Super-class based on the propensity of different building typologies in producing casualties.
In the SYNER-G casualty model, casualty and building damage data has been collected for two large Italian earthquakes: 214 municipalities (deaths and injured) for Irpinia 1980 and 26 municipalities (deaths) in Friuli 1976. Based on the building type designations in the survey data, 3 “Superclasses” of building typologies have been defined and shown in Table 4.5. The choice of the superclasses are based on casualties produced by different building types in Italian earthquakes and knowledge of the reduction of volume in different building types which influences the number of trapped people and hence casualties (References). It should be emphasized that building vulnerability classes (e.g., EMS classes A-F) do not represent the potential to produce casualties in buildings and only represent the vulnerability of buildings to damage. Hence a novelty in this methodology are the superclasses, which discern between different building classes of equal damage state (e.g. slight or collapse) in terms of the relative casualty level which can be produced in each of the building classes. However, as no empirical data as such is available to validate the choice of the superclasses, a sensitivity analysis is performed to determine the influence of change in superclasses.
The aim is to produce a semi-empirical approach by which Casualty Ratios would be derived from empirical data on building damage classes and Super classes of building typologies. In this approach Casualty Ratios (CR) for an Italian model are obtained by optimization with casualty and damage data for the selected Italian earthquakes which occur in comparable settings and are night-time events. The approach of estimating casualty ratios can be described in the following steps:
-
1.
The building stock of any region is grouped in terms of its distribution in Building-Casualty super classes (Table 4.5) and 6 EMS Vulnerability Classes (A-F) at the event year.
-
2.
A database for each historic earthquake event is constructed, where for each administrative unit (e.g., municipality) the following parameters are captured: (a) Number of dead and injured in each Municipality; (b) Number of total buildings in each Municipality, and (c) Population at time of event for each Municipality
-
3.
Distribution of Building Damage states (none, slight, moderate, severe, collapse) in each Municipality
-
4.
Distribution of Seismic Intensity (EMS scale) in each Municipality
-
5.
Allocation of Building Damage states for each Building-Casualty superclass (1-BC, 2-BC and 3-BC) and Building Vulnerability EMS class (A-F).
-
6.
Allocation of Seismic Intensity for each Building-Casualty superclass (1-BC, 2-BC and 3-BC) and Building Vulnerability EMS class (A-F).
-
7.
Allocation of Total Building Occupancy for each Building-Casualty superclass (1-BC, 2-BC and 3-BC) and Building Vulnerability EMS class (A-F).
-
8.
Using the above parameters the number of dead is simulated in an initial run with an assumed Casualty Ratio matrix using values published in the literature Coburn and Spence (2002), So and Spence (2013) and ATC 13.
-
9.
Casualty ratios are optimized in subsequent iterations using an optimization algorithm so that a best-fit is achieved between simulated and surveyed casualty numbers (Table 4.6).
Table 4.6 Casualty ratios derived from optimization algorithm
The optimization algorithms use constraints and restrictions which are derived from common assumptions (e.g., the casualty ratio for moderate damage state should not be greater than casualty ratio for collapsed damage state). Lower and Upper boundary functions are also defined based Coburn and Spence (2002), So and Spence (2013), ELER (Erdik et~al. 2011), and ATC-13 (HAZUS). Using the optimized Casualty Ratios for the region, the number of deaths are determined for that region, using the mean inhabitants by building type, and occupancy rate by day and night. Combining the death records for the Friuli and Irpinia events according to seismic intensity, the casualty model proposed here was compared against the 2008 Coburn and Spence casualty model developed for LessLoss (Casualty Ratios only in D5 damage state) and recorded deaths (Fig. 4.12). As the graph is plotted on a logarithmic scale, the relative comparison of both models is best seen through the average error bars. It can be seen that Coburn and Spence overestimate deaths at low seismic intensities, while they at higher intensities the average error is comparable.
where:
-
t = building-casualty type (t = 1-BC. 2-BC. 3-BC)
-
d = damage level (d = D0, D1, D2, D3, D4, D5)
-
i = seismic intensity level (i = VI, VII, VIII, IX, X)
-
Nt,d,i = number of buildings of type t having damage level d at seismic intensity level i
-
CRt,i = proportion of deaths by building type, damage level and seismic intensity
-
NOt = number of occupants (at the time of the event) by building type t

Comparison of SYNER-G and Coburn and Spence (Less Loss) casualty models for Italy
4.3.2.2 Transportation Accessibility Model
Health impacts of earthquakes like mortality and morbidity in term of injuries, disability, inadequate treatment of non-communicable and chronic diseases (e.g., problem with drug procurement), and increased transmission of infectious diseases (e.g., caused by parallel systems dysfunction such as water and sanitation, communication and transport) is directly related to transport accessibility to healthcare facilities. Transport accessibility basically refers to ability to reach health care services by using various travel costs on the considered road network. As many factors affect transport accessibility, different aspects and measures of accessibility are found in the literature (Litman 2011). However, in order to better assess accessibility to healthcare facilities it is essential to use network-based accessibility analyses. When emergency healthcare accessibility is considered, use of Geographical Information Systems (GIS) becomes essential to assess spatially accessibility zones in terms of emergency services, and help medical emergency service providers determine the extent to which a city is ready for any medical emergency. For example, physical accessibility of medical emergency services can be measured to check if urban/rural areas are highly accessible by medical emergency vehicles (ambulances) within 5 or 10 min of critical time threshold.
The analysis of healthcare accessibility has inherent complexity (Pedigo and Odoi 2010). Pedigo and Odoi (2010) refer to Guagliardo (2004) and Higgs (2009) as the researchers who defined -accessibility to healthcare as the ability to obtain potential healthcare that may be impeded by both spatial, like travel impedances, and non-spatial factors like the ability to pay. However, in the case of earthquakes, physical accessibility, which is assessed spatially, to healthcare services, has direct relation to health impacts. Pedigo and Odoi’s (2010) work is a typical example of healthcare accessibility analysis related to health impact dimension of socio-economic vulnerability, where spatial accessibility to emergency care for stroke and Myocardial Infarction (MI) in the East Tennessee Appalachian Region is evaluated within a GIS to identify the spatial extent of regions which have inadequate accessibility to emergency care units for stroke and MI. McGrail (2012) provides a methodology for determining primary healthcare services accessibility by considering the volume of healthcare services provided relative to the population’s size and the proximity of health services provided relative to the location of the population. The proposed methodology by McGrail (2012) is based on two-step floating catchment area (2SFCA) method, which includes a distance-decay function within a catchment area together with variable catchment sizes. Yiannakoulias et~al. (2013) investigate effect of two different travel cost measures on health care service accessibility. They compare simple network travel cost metric (requiring only data on speed limit and road segment length) and a more complex network travel cost metric (requiring estimates of traffic congestion and intersection turn costs) on a gravity-based measure of accessibility to primary healthcare services. Yiannakoulias et~al. (2013) find that the city center is less sensitive to change in travel cost matrix as compared to outlying regions and more complex network travel cost metric (requiring estimates of traffic congestion and intersection turn costs) provides more realistic accessibility results. Ertugay and Duzgun (2011) present health service accessibility based on a stochastic approach, where uncertainties related to the catchment boundaries are considered and probabilistic catchment boundaries are determined instead of crisp catchment boundaries in the deterministic model. Düzgün et~al. (2011) provide a framework for vulnerability assessment of urban environment in neighborhood scale where in addition to building fragility and socio-economic vulnerability, the accessibility of neighborhoods by the critical services like fire brigades, ambulances etc. are modeled as one of the vulnerability component of the neighborhoods. Horner and Widener (2011) investigate the impacts network failures, which are predicted by simulations made based on various hurricane disaster scenarios, on disaster relief planning strategies, for Florida City. They report that the modest disruptions to the transportation network yields marked changes in the number and spatial configuration of relief facilities. Bono and Eugenio (2011) suggest a method based on combining simple graph theory and GIS-based spatial analyses to define the urban accessibility landscape in the aftermath of earthquake damage. They use open source data for Port Au Prince and evaluate difference between the undamaged and damaged networks to measure potential decrease in transport performance as a result of the earthquake.
4.3.2.2.1 Transportation Accessibility Model in SYNER-G
In SYNER-G two accessibility analysis approaches for healthcare services in case of earthquake are developed at the urban scale. The first method is based on evaluating accessibility by using indicators of accessibility, which can be obtained from publically available socio-economic data in Europe (e.g., EUROSTAT Urban Audit Database). A comprehensive overview of factors affecting transport accessibility provided by Litman (2011), include: transportation demand and activity, mobility, transportation options, user Information, integration-terminals-parking, affordability, mobility substitutes, land use factors, transportation network connectivity, roadway design and management, prioritization, value of inaccessibility. Among the various ‘Urban Audit’ data groups investigated the following show a high degree of relevance to the indicators listed by Litman (2011) for assessing accessibility in urban environments: population structure (population of working age, proportion of children and elderly, demographic dependency, migrant population) which indicates transportation demand and activity; economic aspects (labor market, economic activity, income disparities and poverty), which forms the basis of various transportation option’s affordability; travel patterns (vehicle ownership, mode of journey to work, percentage of commuters, length of public transportation network), which relates to transportation options and integration-terminals-parking; information society (user and infrastructure, local government and ICT sector), which is relevant to express user information. Hence by using these indicators relative accessibility levels of various urban environments can be assessed by using multi criteria decision approach.
The second approach is based on use of transportation data in GIS with prediction of road closure for various earthquake scenarios, following a three-step procedure: (1) data acquisition and integration; (2) traveling cost calculation; and (3) accessibility modeling and visualization. Data acquisition and integration phase includes compilation of data related to road network as well as supply and demand. Transportation network data also have attributes of road segments indicating their type and hence capacity such as main roads, secondary roads etc. The supply data constitutes locations of healthcare service and their capacities. The demand data involves boundaries of administrative zones and centroids of these zones so that accessibility of each administrative zone can be calculated. Usually these data are obtained in various formats, which require integration in GIS environment. Traveling cost calculation phase involves determination of traveling costs for each road segment on the transportation network according to road closure probabilities. The road closure probabilities can be obtained based on either the structural analysis of the road segments or prediction of road closure due to building collapse, which is estimated by structural analyses of buildings or both. Finally, accessibility modeling and visualization phase is computation of health service accessibility scores and their visualization in a GIS environment.
The health-care accessibility model is implemented as a pilot application for the city of Thessaloniki based on three different accessibility modeling techniques: isochronal-based technique (travel time measure); zone-based technique (cumulative time from each health service to each administrative district centroid without considering the scale of the health service); and zone-based technique (gravity measure). The basic data used in the model are:
-
Transportation network (line): The main transportation network data which is considered to be important in case of emergency (the city of Thessaloniki as case study example). The local roads, which are expected to have higher blockage probability due to building collapses, are not taken into account.
-
Supply locations (point): The locations of healthcare services (Thessaloniki as a case study) and scale of healthcare service data are also taken into account. The scale of healthcare service indicates the capacity of the healthcare service and hence used as gravity measure where high capacity healthcare services attract more healthcare seekers.
-
Demand locations (area): The administrative districts of the urban areas (Thessaloniki in this case) as defined by the sub-city district boundaries of the EUROSTAT Urban Audit.
-
Road closure probabilities due to building collapses, soil liquefaction, bridge damages and overpass bridge collapses were calculated. The average number of damages over 10,000 runs are presented for the estimating road closure probabilities which are described in Chap. 7.
-
Depending on the road closure probability different average speeds were assigned to the road segments to compute the traveling costs (Table 4.7). For the road segments that have road closure probability scores greater than zero, the scores are first normalized to have a range of 0 and 1, then classified into four categories as shown in Table 4.7 and used in calibration of the transportation network costs.
Table 4.7 Reduction in average traveling speed as function of road closure probability
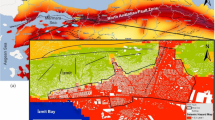
As the performance of the network is affected at the same time from all of the different types of damages, the results are aggregated into one group in order to provide a more complete view of the accessibility. In particular, the results that include the road closure probabilities due to liquefaction, building collapses, bridge and overpass damages are aggregated into a new group which is named as “overall” accessibility. When there is an overlay case during aggregation process, the maximum of the probability scores is considered in calculation of the transportation network costs. Five minutes (300 s) cost is accepted as a critical time threshold for the health service accessibility. An example accessibility analysis result is given in Fig. 4.13, the results for the combined health service accessibility are shown for both the isochrones-based and zone-based techniques.

Combined healthcare accessibility example results for Thessaloniki using the isochrones-based technique (top) and zone based techniques (bottom)
4.3.2.3 Social Vulnerability Factors Influencing Health Issues
Beyond the parameters used in earthquake casualty estimation to assess and describe expected mortalities and injuries (earthquake intensity, building class, occupancy, time of day, building damage state), social vulnerability and health care system vulnerability can aggravate the overall health impact after a disaster. To identify the most critical factors determining post-earthquake health impacts and to deduce appropriate indicators representing these factors, a literature research focusing on case studies on impacts of earthquakes on individual health and on the health care system was carried out and supplemented by publications giving a general overview on health and health care system impacts from earthquakes and other disasters (Gunn 1995; Alexander 1996; Howard et~al. 1996; Ramirez and Peek-Asa 2005; Watson et~al. 2007; Aldrich and Benson 2008; Bartels and VanRooyen 2011).
The case studies used to identify the most critical factors cover 15 earthquakesFootnote 1 worldwide and rely on various research designs:
-
epidemiological studies that analyze earthquake-related mortality and injury, trauma, infectious diseases studies (Chan 2008; Shi et~al. 2010; Guha-Sapir and van Panhuis 2009; Phalkey et~al. 2011; Karmakar et~al. 2008; Matsuoka et~al. 2000; Tanaka et~al. 1999),
-
studies that combine an epidemiological approach with socio-economic variables to identify risk factors for mortality and morbidity (Chou et~al. 2004a; Liang et~al. 2001; Peek-Asa et~al. 2003),
-
studies dealing with particular injuries such as burns (Nakamori et~al. 1997) or crush syndrome (Vanholder et~al. 2007; Erek et~al. 2002; Oda et~al. 1997), infectious diseases (Guha-Sapir and van Panhuis 2009; Karmakar et~al. 2008; Vahaboglu et~al. 2000; Schneider et~al. 1997), impacts on mental health (Başoğlu et~al. 2002; Chan et~al. 2012), or on reproductive health (Liu et~al. 2010; Hibino et~al. 2009; Chang et~al. 2002),
-
studies that consider pre-existing health conditions such as chronic disease (Mori et~al. 2007),
-
studies that investigate long-term health impact outcome (Zhang et~al. 2011; Seplaki et~al. 2006; Oda et~al. 2002; Dobalian et~al. 2011; Armenian et~al. 1997),
-
studies that focus on challenges and limitations faced in medical emergency response immediately after earthquakes (Roy et~al. 2002, 2005; Chan 2008; Shi et~al. 2010; Phalkey et~al. 2011; McCurry 2011).
Correspondingly, the data analyzed in the case studies is rather heterogeneous. It ranges from hospital records (Guha-Sapir and van Panhuis 2009; Phalkey et~al. 2011; Tanaka et~al. 1999), laboratory tests (Karmakar et~al. 2008; Vahaboglu et~al. 2000), field observations (Chan 2008) or rapid assessments (Takahashi et~al. 2011; McCurry 2011), and surveys among survivors (Kun et~al. 2010; Roy et~al. 2002), to data of statistical offices and national and international health organizations (Chou et~al. 2004b; Muramatsu and Akiyama 2011; Guha-Sapir and van Panhuis 2009).
Analyzing and comparing the results of the case studies with respect to individual, social, health and health care system factors by carefully taking into ac-count the heterogeneity of the studies and limitations in generalizability of case studies, a number of recurring variables emerged across several earthquakes that influenced the health impact of earthquakes and that can be considered classified as contributing to risk factors for negative health outcomes after earthquakes. The variables were categorized in five factors that potentially aggravate health impact and that were later on used to define indicators for the further analysis: social vulnerability, environmental health, baseline health status, health care capacity, infrastructure (Table 4.8). Three of them (social vulnerability, baseline health status, health care capacity) represent different facets of social vulnerability conditions (socially vulnerable groups, health and health care status, hospital health care capacities) and should therefore be integrated in the further model development and implementation.
The factor social vulnerability subsumes a number of socio-demographic and socio-economic variables that were associated with higher mortality and morbidity rates: age (elderly and children) (elderly and children), gender, and socioeconomic status, physical disability. Across most of the 15 earthquakes covered in the literature research, higher mortality rates among elderly were reported in the majority of the case studies that considered age as variable or risk factor (Muramatsu and Akiyama 2011; Suzuki and Kim 2012; Alexander 2011; Chan 2008; Sullivan and Hossain 2010; Chou et~al. 2004a; Liang et~al. 2001; Osaki and Minowa 2001; Tanaka et~al. 1999; Peek-Asa et~al. 2003), but also higher rates for injuries (Nakamori et~al. 1997; Peek-Asa et~al. 2003), pneumonia and heart diseases in the immediate phase after the earthquake (Matsuoka et~al. 2000). Also for children higher mortality and injury rates were observed (Chan 2008; Sullivan and Hossain 2010; Roy et~al. 2002; Chou et~al. 2004b; Liang et~al. 2001). Concerning gender, the literature includes a significant number of case studies that reported higher female rates in mortality (Kun et~al. 2010; Chou et~al. 2004b; Liang et~al. 2001), injuries (Roy et~al. 2002; Armenian et~al. 1997; Peek-Asa et~al. 2003; Nakamori et~al. 1997) and mental impact rates such as posttraumatic stress disorder syndrome PTSD (Tural et~al. 2004). Regarding the socio-economic status, being divorced,/widowed or living alone turned out to be a negative factor for physical and mental health outcome (Kun et~al. 2010; de Bruycker et~al. 1985), and also low income, relying on social welfare or living in low-cost buildings were observed as variables associated with higher mortality rates (Chou et~al. 2004b; Alexander 2011) or more emotional distress (Dobalian et~al. 2011).
Environmental health factors cover characteristics of the natural and build environment that have an immediate impact on health in the emergency phase after earthquakes and that can aggravate the health situation. Examples from the case studies are cold and harsh weather conditions that impede immediate medical help (Chadda et~al. 2007; Noji et~al. 1993) or may lead to a higher rate of Acute Respiratory Infections (Matsuoka et~al. 2000), warm weather conditions that favor the spreading of vector borne infections such as the Valley Fever (Coccidioidomycosis) outbreak after the Northridge earthquake (Jibson 2002; Schneider et~al. 1997). Also interruption of access to clean water and sanitation has been reported as factor across the case studies that had an influence on increasing gastro-intestinal infection rates (Kun et~al. 2010; Liu et~al. 2010; Karmakar et~al. 2008; Guha-Sapir and van Panhuis 2009; Matsuoka et~al. 2000). Finally, changed living conditions in crowed shelters has been observed as factor associated with increased death rates, pneumonia and heart disease (Matsuoka et~al. 2000).
The factor pre-earthquake baseline health status as influencing factor refers to constrained individual health conditions (people with chronic diseases, functional limitations, bedridden people) which may lead to increased mortality and an increased rate of negatively aggravated health effects of an earthquake (Muramatsu and Akiyama 2011; Suzuki and Kim 2012; Osaki and Minowa 2001; Dobalian et al. 2011; Chou et~al. 2004a), but also to indicators such as a general high rate of major infections (Wen et~al. 2009) or a low vaccination status against Tetanus (Chan 2008) as factors that could aggravate the health impact of earthquakes. Results subsumed to this factor include also an increased risk due to hospitalization in the month before the earthquake (Chou et~al. 2004a) and pre-quake emotional distress (Dobalian et~al. 2011).
The factor health care capacity summarizes those characteristics that limit and hinder the health care sector to respond immediately and adequately to the medical needs of the injured: collapse of hospitals, partial non- functionality or disruption of normal functionalities due to the physical impact of the earthquake (McCurry 2011; Suzuki and Kim 2012; Rossetto et~al. 2011; Kuwagata et~al. 1997; Noji et~al. 1993; Roy et~al. 2002; Chan 2008), and lack of medical doctors, nurses and hospital beds compared to the high influx of patients in the first days after the earthquake (Shi et~al. 2010; Roy et~al. 2002; Liang et~al. 2001; Tanaka et~al. 1998, 1999).
The factor infrastructure finally refers mainly to interruptions of roads, bridges, and railway tracks that are necessary to access the affected area and that, on the one hand, hamper the transportation of injured in due time to functioning hospitals for medical treatment (Takahashi et~al. 2012; Shi et~al. 2010; Wen et~al. 2009; Vanholder et~al. 2007; Chadda 2007; Roy et~al. 2002; Liang et~al. 2001; Noji et~al. 1993), and that, on the other hand, can lead to an interruption in supply of necessary medical equipment and drugs (Suzuki and Kim 2012).
4.3.3 Health Impact Model Implementation and Conclusions
The integrated health impacts model developed here is based on a multi-criteria decision theory (MCDA) framework which allows the bringing together of parameters influencing the direct social losses represented through estimates of casualties and injuries, with factors related to overall health impact of the population at risk in an earthquake. As shown in Fig. 4.14, the multi-criteria framework can be described schematically as composed of the two main criteria: overall population at risk of mortality in an earthquake (represented by casualties) and an Impact Factor (IF). Subsequently, the overall health impact for a particular location (i.e., city district, county or country) can be described as the population at risk of mortality, amplified by the set of conditions that can aggravate the health impacts following a disaster which are derived as a weighted index of a set of indicators in four main categories of: social vulnerability, baseline health status, environmental parameters and healthcare accessibility. This can be expressed by:
where:
-
HII = Health Impact Index.
-
C = Indicator representing the mortality ratio from an event. When using a casualty estimation model this is taken as the ratio of the fatalities to occupants at a given location.
-
IF = Impact Factor.
-
AI = Accessibility Index, derived from accessibility model.
-
w j = overall weight given to each indicator.
-
VF j = represented as the weighted sum of indicators representing the categories social vulnerability, baseline health status and environmental health and healthcare capacity.
According to the overall aim to implement a combined engineering and social science approach the next steps would have been to combine the developed Casualty estimation model with the hospitality accessibility index and the social vulnerability factors as aggravating factors on a sub-city level. Unfortunately this was not possible due to lack of data in the European Urban Audit on sub-city level for data on baseline health status and health care capacities that could have been combined with the Casualty Estimation for Italy or the transportation accessibility model developed for Thessaloniki, Greece as example. In order to test the approach at least in principle, it was decided to apply it on national level. Based on the literature research presented in Sect. 4.3.2.3, the identified 22 indicators that represent all of the main factors influencing health impact developed in the framework, with the exception of accessibility, were implemented in a multi-criteria hierarchical model (See Fig. 4.14 Multi-Criteria Framework with indicators).

Multi-criteria framework for health impact analysis, application on national level
To demonstrate the health impact methodology at the national level of analysis it has been applied to 12 South West European Countries representing the greatest seismic risk in Europe. The mortality ratio was obtained using detailed data on the number of dead persons from 244 events affecting 35 European countries from 1900 till 2012, which were reduced to the top 12 with the highest casualty estimates. Indicators representing the different categories of the impact factor were compiled from various sources including EUROSTAT, UNDP, WHO, World Bank, and CIA. All indicators were derived for the year 2012. It can be observed in Fig. 4.15 that Turkey, for example, has the highest potential for overall health problems following an event due to lack of health care capacities, comparatively lower baseline health status and social vulnerabilities in addition to a very high historic earthquake fatality. Figure 4.15 also shows how impact factor is derived as weighted average of a number of indicators including representing social vulnerability, baseline health status, environmental health and healthcare capacity. The assigning of weights to each of these indicators is a subjective process and their elicitation should be carried out in a participatory approach with a group of experts or other stakeholders using the model. Similarly the weight assigned to each category of the Impact Factor (IF) can be different and should also be determined in a participatory approach. In this analysis equal weights were given to all criteria.

Overall health impact (c) obtained as a product of fatalities (a) and impact factors (b)
The model is readily extendable to other scales (provincial, municipal, sub-municipal) where individual indicators are selected based on the specific context of the scale and availability of data. The preferred approach for application of models in SYNER-G is the sub-city level of geography. However, based on the principle that only European-wide public available data should be used, application at this scale was not possible as the Urban Audit database does not contain enough relevant factors for criteria identified in this study.
Notes
- 1.
Tohoku earthquake 2011 (Japan), L’Aquila 2009 (Italy), Wenchuan 2008 (China), Noto Peninsula 2007 (Japan), Kashmir 2005 (India, Pakistan), Sumatra 2004 (Indonesia), Niigata-Chuetsu 2004, Japan, Gujarat 2001 (India), Chi-Chi 1999 (Taiwan), Izmit 1999 (Turkey), Kobe 1995 (Japan), Northridge 1994 (USA), Loma Prieta 1989 (USA), Spitak 1988 (Armenia), Irpinia 1980 (Italy).
References
Aldrich N, Benson, FW (2008) Disaster preparedness and the chronic disease needs of vulnerable older adults. Prev Chronic Dis 5. http://www.cdc.gov/pcd/issues/2008/jan/07_0135.htm. Accessed 18 June 2013
Alexander D (1982) Disease epidemiology and earthquake disaster: the example of southern ltaly after the 23 November 1980 earthquake. Soc Sci Med 16:1959–1969
Alexander D (1996) The health effects of earthquakes in the mid-1990s. Disasters 20:231–247
Alexander D (2011) Mortality and morbidity risk in the L’Aquila, Italy earthquake of 6 April 2009 and lessons to be learned. In: Spence R, So E, Scawthorn C (eds) Human casualties in earthquakes, vol 29, Advances in natural and technological hazards research. Springer, Berlin. ISBN 978-90-481-9455-1
Armenian HK, Melkonian A, Noji EK, Hovanesian AP (1997) Deaths and injuries due to the earthquake in Armenia: a cohort approach. Int J Epidemiol 26:806–813
Bartels SA, VanRooyen MJ (2011) Medical complications associated with earthquakes. Lancet. doi:10.1016/S0140-6736(11)60887-8
Başoğlu M, Şalcioğlu E, Livanou M (2002) Traumatic stress responses in earthquake survivors in Turkey. J Trauma Stress 15:269–276
Berberian M (1978) Tabas-e-Golshan (Iran) catastrophic earthquake of September 16, 1978; a preliminary field report. Disaster 2(4):207–219
Birkmann J (2006) Measuring vulnerability to natural hazards: towards disaster resilient societies. United Nations University Press, New York
Bono F, Eugenio G (2011) A network-based analysis of the impact of structural damage on urban accessibility following a disaster: the case of the seismically damaged Port Au Prince and Carrefour urban road networks. J Transp Geogr 19:1443–1455
Bostrom A, French SP, Gottlieb SJ (2008) Risk assessment, modeling and decision support: strategic directions. Springer, Berlin
Braun J (2011) Post-earthquake vulnerability indicators of shelter and housing in Europe: Masters Thesis. University of Trier
Burton C, Cutter SL (2008) Levee failures and social vulnerability in the Sacramento-San Joaquin Delta area, California. Nat Hazards Rev 9(3):136–149
Cardona OD (2005) Indicators of disaster risk and risk management: program for Latin America and the Caribbean. Summary Report (No. 30718), Inter-American Development Bank
Cavalieri F, Franchin P, Khazai B, Gehl P (2012) Quantitative assessment of buildings habitability based on physical damage and functional interaction with infrastructural systems. Earthq Eng Str Dyn EQE-11-0153
Chadda RK, Malhotra A, Kawa N, Singha J, Sethia H (2007) Mental health problems following the 2005 earthquake in Kashmir: findings of community-run clinics. Prehosp Disaster Med 22:541–545
Chan E (2008) The untold stories of the Sichuan earthquake. Lancet 372:359–362
Chan CL, Wang C-W, Ho AH, Qu Z-Y, Wang X-Y, Ran M-S, Mao W-J, Lu BQ-B, Zhang BQ, Zhang X-L (2012) Symptoms of posttraumatic stress disorder and depression among bereaved and non-bereaved survivors following the 2008 Sichuan earthquake. J Anxiety Disord 26:673–679
Chang H-L, Chang T-C, Lin T-Y, Kuo S-S (2002) Psychiatric morbidity and pregnancy outcome in a disaster area of Taiwan 921 earthquake. Psychiatry Clin Neurosci 56:139–144
Chang SE, Pasion C, Yavari S, Elwood K (2009) Social impacts of lifeline losses: modeling displaced populations and health care functionality. In: Oakland California proceedings of 2009 Technical Council on Lifeline Earthquake Engineering (TCLEE) conference
Chien S, Chen L, Chang S, Cui G, Chu C (2002) Development of an after earthquake disaster shelter evaluation model. J Chin Inst Eng 25(5):2
Chou FHC, Chou P, Su TTP, Ou Yang WC, Chien IC, Lu MK, Huang M-W (2004a) Quality of life and related risk factors in a Taiwanese village population 21 months after an earthquake. Australian and New Zealand. J Psyc 38:358–364
Chou YJ, Huang N, Lee CH, Tsai SL, Chen LS, Chang HJ (2004b) Who is at risk of death in an earthquake. Am J Epidemiol 160:688–695
Christoskov L, Samardjieva E (1984) An approach for estimation of the possible number of casualties during strong earthquakes. Bulg Geophys J X 4:94–106
Coburn AW (1986) Seismic vulnerability and risk reduction strategies for housing in Eastern Turkey. University of Cambridge, PhD Dissertation
Coburn A, Spence R (1992) Earthquake protection. John Wiley & Sons Ltd, Chichester
Coburn A, Spence R (2002) Earthquake protection. Wiley, Chichester
Coburn AW, Ohashi Murakami H, Ohta Y (1987) Factors affecting fatalities and injuries in earthquakes, chair for engineering seismology and earthquake disaster prevention planning. Department of Architectural Engineering, Hokkaido University, Japan
Cutter SL (1996) Societal vulnerability to environmental hazards. Int Soc Sci J 47(4):525–536
Cutter SL, Boruff B, Shirley JWL (2003) Social vulnerability to environmental hazards. Soc Sci Q 84:242–261
Daniell JE, Khazai B, Wenzel F, Vervaeck A (2011) The CATDAT damaging earthquakes database. Nat Hazards Earth Syst Sci 11:2235–2251
Daniell JE, Vervaeck A, Khazai B, Wenzel F (2012) Worldwide CATDAT damaging earth-quakes database in conjunction with Earthquake-report.com – Presenting past and present socio-economic earthquake data. 15th WCEE, Lisbon, Portugal, Paper no. 2025
de Bruycker M, Greco D, Lechat MF (1985) The 1980 earthquake in Southern Italy – morbidity and mortality. Int J Epidemiol 14:113–117
Dobalian A, Stein JA, Heslin KC, Riopelle D, Venkatesh B, Lanto AB, Simon B, Yano EM, Rubenstein LV (2011) Impact of the Northridge earthquake on the mental health of veterans: results from a panel study. Disaster Med Public Health Preparedness 5:S220–S226
Düzgün HSB, Yücemen MS, Kalaycioglu HS, Celik K, Kemec S, Ertugay K, Yilmaz N (2011) An integrated earthquake vulnerability assessment framework for urban areas. Nat Hazards 59:917–947
Elnashai AS, Jefferson T, Friedrich F, Cleveland LJ, Gress T (2009) Impact of new Madrid seismic zone earthquake on the central USA, vol. I. MAE Center report no 09-03
Erdik M, Şeşetyan K, Demircioğlu MB, Hancılar U, Zülfikar C (2011) Rapid earthquake loss assessment after damaging earthquakes. Soil Dynam Earthquake Eng 31(2):247–266
Erek E, Sever M, Serdengeçti K, Vanholder R, Akoğlu E, Yavuz M, Ergin H, Tekçe M, Duman N, Lameire N, Turkish Study Group of Disaster (2002) An over-view of morbidity and mortality in patients with acute renal failure due to crush syndrome: the Marmara earthquake experience. Nephrol Dial Transplant 17(1):33–40
Ertugay K, Duzgun S (2011) GIS-based stochastic modeling of physical accessibility using GPS-based floating Car data and Monte Carlo simulation. Int J Geogr Inform Sci 25(9):1491–1506
FEMA (2003) Chapter 14: Direct social losses: displaced households due to loss of housing habitability and short term shelter needs. HAZUS-MH MR4 Technical Manual, Washington, DC
Federal Emergency Management Agency (FEMA) (2006) HAZUS-MH MR2 technical manual. Federal Emergency Management Agency, Washington, DC
Franchin P, Lupoi A, Pinto PE (2006) On the role of road networks in reducing human losses after earthquakes. J Earthquake Eng 10(2):195–206
Freudenberg M (2003) Composite indicators of country performance: a critical assessment. Organisation for Economic Co-operation and Development (OECD), Paris
Guagliardo MF (2004) Spatial accessibility of primary care: concepts, methods and challenges. Int J Health Geogr 3:1–13
Guha-Sapir D, van Panhuis WG (2009) Health Impact of the 2004 Andaman Nicobar earth-quake and Tsunami in Indonesia. Prehosp Disaster Med 24:493–499
Gunn S (1995) Health effects of earthquakes. Disaster Prev Manag 4:6–10
Harrald JR, Fouladi B, Al-Hajj SF (1992) Estimates of demand for mass care services in future earthquakes affecting the San Francisco bay region. Prepared by George Washington University for the American Red Cross Northern California Earthquake Relief and Preparedness Project (NCERPP)
Hewitt K, Burton I (1971) The hazardousness of a place: a regional ecology of damaging events. Research publication 6. University of Toronto Press, Toronto
Hibino Y, Takaki J, Kambayashi Y, Hitomi Y, Sakai A, Sekizuka N, Ogino K, Nakamura H (2009) Health impact of disaster-related stress on pregnant women living in the affected area of the Noto Peninsula earthquake in Japan. Psychiatry Clin Neurosci 63:107–115. Wiley Online Library
Higgs G (2009) The role of GIS for health utilization studies: literature review. Health Serv Outcom Res Methodol 9:119–139
Horner MW, Widener MJ (2011) The effects of transportation network failure on people’s accessibility to hurricane disaster relief goods: a modeling approach and application to a Florida case study. Nat Hazards 59:1619–1634
Howard MJ, Brillmann JC, Burkle FM (1996) Infectious disease emergencies in disasters. Emerg Med Clin North Am 14:413–428
Jaiswal K, Wald D (2010) An empirical model for global earthquake fatality estimation. Earthquake Spectra 26(4):1017–1038
Jibson RW (2002) A public health issue related to collateral seismic hazards: the valley fever outbreak triggered by the 1994 Northridge, California earthquake. Surv Geophys 23:511–523
Karaca E (2005) Regional earthquake loss estimation: role of transportation network, sensitivity and uncertainty, and risk mitigation. PhD dissertation. MIT, Cambridge, MA
Karmakar S, Rathore AS, Kadri SM, Dutt S, Khare S, Lal S (2008) Post-earthquake outbreak of rotavirus gastroenteritis in Kashmir (India): an epidemiological analysis. Public Health 122:981–989
Kawasumi H (1954) Intensity and magnitude of shallow earthquakes. Bureau Central Seism Intern, Scr A Trav Sci 19:99–114
Khazai B, Braun J, Vangelsten BV (2011a) Definition of a group of output indicators representing socio-economic impact from displacement in emergency/temporary shelter. Tech report D4.1 of the SYNER-G project. http://www.syner-g.eu
Khazai B, Daniell JE, Wenzel F (2011b) The March 2011 Japan earthquake – analysis of losses impacts, and implications for the understanding of risks posed by extreme events. Technikfolgenabschätzung – Theorie und Praxis, 20. Jg., Heft, 3 Nov 2011
Khazai B, Vangelsten B, Duzgun S, Braun J, Daniell J (2011c) Social impacts of emergency shelter provision in the aftermath of earthquakes. Geophys Res Abs 13: EGU 2011-7374
Khazai B, Daniell JE, Franchin P, Cavalieri F, Vangelsten B, Iervolino I, Esposito S (2012a) A new approach to modeling post-earthquake shelter demand in the aftermath of earthquakes: integrating social vulnerability in systemic seismic vulnerability analysis. In Proceedings of the 15th WCEE. Paper no. 2105, Lisbon, Portugal, 24–28 Sept 2012
Khazai B, Schaefer D, Mueller T (2012b) MCDA software tool. Tech report D7.1 of the SYNER-G project. http://www.syner-g.eu
Khazai B, Vangelsten B, Duzgun S, Daniell J, Braun J, Plapp-Kunz T, Iervolino I, Esposito S, Elefante L (2012c) Framework for integrating physical and socio-economic models for estimating shelter needs. Tech report D4.7 of the SYNER-G project. http://www.syner-g.eu
Kun P, Wang Z, Chen X, Le H, Gong X, Zahng L, Yao L (2010) Public health status and influence factors after 2008 Wenchuan earthquake among survivors in Sichuan province, China: cross-sectional trial. Public Health 124:573–580
Kuwagata Y, Oda J, Tanaka H, Iwai A, Matsuoka T, Takaoka M, Kishi M, Morimoto F, Ishikawa K, MizushimaY MY, Yamamura H, Hi-raide A, Shimazu T, Yoshioka T (1997) Analysis of 2,702 traumatized patients in the 1995 Hanshin-Awaji earthquake. J Trauma 43:427–432
Liang N-J, Shihs Y-T, Shihs F-Y, Wu H-M, Wang H-J, Shi S-F, Liu M-Y, Wang BB (2001) Disaster epidemiology and medical response in the Chi-Chi earthquake in Taiwan. Ann Emerg Med 38:549–555
Litman T (2011) Evaluating accessibility for transportation planning. Victoria Transport Policy Institute. http://www.vtpiorg. A shorter version of this paper was presented at the 87th Transportation Research Board annual meeting (www.trb.org) on January 2008
Liu S, Han J, Xiao D, Ma C, Chen B (2010) A report on the reproductive health of women after the massive 2008 Wenchuan earthquake. Int J Gynaecol Obstet 108:161–164
Lupoi G, Franchin P, Lupoi A, Pinto PE, Calvi GM (2008) Probabilistic seismic assessment for hospitals and complex-social systems. IUSS Press, Pavia
Marano KD, Wald DJ, Allen TI (2010) Global earthquake casualties due to secondary effects: a quantitative analysis for improving rapid loss analyses. Nat Hazards 52(2):319–328
Maqsood ST, Schwarz J (2011) Estimation of human casualties from earth-quakes in Pakistan – an engineering approach. Seismol Res Lett 82(1):32–41
Matsuoka T, Yoshioka T, Oda J, Tanaka H, Kuwagata Y, Sugimoto H, Sugimoto T (2000) The impact of a catastrophic earthquake on morbidity rates for various illnesses. Public Health 114:249–253
McCurry J (2011) Japan: the aftermath. Lancet 377:1061–1062
McGrail (2012) Spatial accessibility of primary health care utilising the two step floating catchment area method: an assessment of recent improvements, International J Health Geogr 11:50. doi:10.1186/1476-072X-11-50, http://www.ij-healthgeographics.com/content/11/1/50
Mileti DS (1999) Disasters by design: a reassessment of natural hazards in the United States. National Academies Press, Washington, DC
Mori K, Ugai K, Nonami Y, Kirimura T, Kondo C, Nakamura T, Motoki E, Kaji H (2007) Health needs of patients with chronic diseases who lived through the great Hanshin earthquake. Disaster Manag Response 5:8–13
Muramatsu N, Akiyama H (2011) Japan: Super-Aging Society preparing for the future. Gerontologist 51:425–432
Nakamori Y, Tanaka H, Oda J, Kuwagata Y, Matsuoka T, Yoshioka T (1997) Burn injuries in the 1995 Hanshin-Awaji earthquake. Burns 23:319–322
Nardo N, Saiana M, Saltelli A, Tarantola S, Hoffmann A, Giovannini E (2005) Handbook on constructing composite indicators: methodology and user guide. OECD statistics working paper
Noji EK, Armenian HK, Oganessian A (1993) Issues of rescue and medical care following the 1988 Armenian earthquake international. J Epidemiol 22:1070–1076
Nuti C, Vanzi I (1998) Assessment of post‐earthquake availability of hospital system and upgrading strategies. Earthquake Eng Struct Dynam 27(12):1403–1423
Oda J, Tanaka H, Yoshioka T, Iwai A, Yamamura H, Ishikawa K, Sugimoto H (1997) Analysis of 372 patients with crush syndrome caused by the Hanshin-Awaji earthquake. J Trauma-Injury Infect Crit Care 42(3):470–476
Ohashi H, Ohta Y (1983) Distribution characteristics of structural damage and casualty at several recent earthquakes in turkey and its factor analysis. In: A comprehensive study on earthquake disasters in Turkey in view of seismic risk reduction. Hokkaido University, Sappro, pp 131–166
Ohta Y, Ohashi H, Tabban A (1983) Macro statistical analysis on earth-quake damage in Turkey. In: A comprehensive study on earthquake disasters in Turkey in view of seismic risk reduction. Hokkaido University, Sapporo, pp 5–21
Osaki Y, Minowa M (2001) Factors associated with the earthquake deaths in the Great Hanshin-Awaji Earthquake, 1995. Am J Epidemiol 153:153–156
Pedigo AS, Odoi A (2010) Investigation of disparities in geographic accessibility to emergency stroke and myocardial infarction care in East Tennessee using geographic information systems and network analysis. Ann Epidemiol 20(12):924–930
Peek Asa C, Ramirez M, Seligson H, Shoaf K (2003) Seismic, structural, and individual factors associated with earthquake related injury. Inj Prev 9:62–66
Phalkey R, Rheinhardt JD, Marx M (2011) Injury epidemiology after the 2001 Gujarat earth-quake in India: a retrospective analysis of injuries treated at a rural hospital in the Kutch district immediately. Glob Health Action 4:7169
Ramirez M, Peek-Asa C (2005) Epidemiology of traumatic injuries from earthquakes. Epidemiol Rev 27:47–55
RGELFE (Research Group for Estimating Losses from Future Earthquakes) (1992) Estimating Losses from Earthquakes in China in the forthcoming 50 years. State Seismological Bureau, Seismological Press, Beijing
Rossetto T, Peiris N, Alarcon J, So E, Sargeant S, Free M, Sword-Daniels V, Re DD, Libberton C, Verrucci E, Sammonds P, Walker JF (2011) Field observations from the Aquila, Italy earthquake of April 6, 2009. Bull Earthq Eng 9:11–37
Roy N, Shah H, Patel V, Coughlin RR (2002) The Gujarat earthquake (2001) experience in a seismically unprepared area: community hospital medical response. Prehosp Disaster Med 17:186–195
Roy N, Shah H, Patel V, Bagalkote H (2005) Surgical and psychosocial outcomes in the rural injured – a follow-up study of the 2001 earthquake victims injury. Int J Care Inj 36:927–934
Schneider E, Haijeh RA, Spiegel RA, Jibson RW, Harp EL, Marshall GA, Gunn RA, McNeil MM, Pinner RW, Baron RC, Burger RC, Hurtwanger LC, Crump C, Kaufman L, Reef SE, Feldman GM, Pappagianis D, Werner SB (1997) A coccidioidomycosis outbreak following the Northridge, Calif, earthquake. J Am Med Assoc 277:904–908
Seplaki CL, Goldman N, Weinstein M, Lin YH (2006) Before and after the 1999 Chi-Chi earthquake: traumatic events and depressive symptoms in an older population. Soc Sci Med 62:3121–3132
Shi YK, Wang LI, Lin YD, Pe FX, Kang Y (2010) Challenges for rear hospital care of Wenchuan earthquake casualties: experience from West China Hospital. Chin J Traumatol 13:131–136
So E (2009) The assessment of casualties for earthquake loss estimation. PhD dissertation, University of Cambridge, Cambridge, UK
So E, Spence R (2013) Estimating shaking-induced casualties and building damage for global earthquake events: a proposed modelling approach. Bull Earthquake Eng 11(1):347–363
Spence R (ed) (2007) Earthquake disaster scenario prediction and loss modelling for urban areas. IUSS Press, University of Pavia
Sullivan KM, Hossain SM (2010) Earthquake mortality in Pakistan. Disasters 36:176–183
Surahman A (2000) Earthquake Vulnerability evaluation of buildings in Bandung Municipality In: Proceedings of the 12th WCEE, Auckland, New Zealand, 30 January-4 February 2000.
Suzuki Y, Kim Y (2012) The Great East Japan earthquake in 2011, toward sustainable mental health care system. Epidemiol Psych Sci 21:7–11
Takahashi T, Goto M, Yoshida H, Sumino H, Matsui H (2011) Infectious diseases after the 2011 Great East Japan earthquake. J Exper Clin Med 4:20–23
Takahashi T, Goto M, Yoshida H, Sumino H, Matsui H (2012) Infectious diseases after the 2011 Great East Japan earthquake. J Exper Clin Med 4:20–23
Tanaka H, Iwai A, Oda J, Kuwagata Y, Matsuoka T, Shimazu T, Yoshioka T (1998) Overview of evacuation and transport of patients following the 1995 Hanshin-Awaji earthquake. Disaster Med 16:439–444
Tanaka H, Oda J, Iwai A, Kuwagata Y, Matsuoka T, Takaoka M, Kishi M, Morimoto F, Ishikawa K, Mizushima Y, Nakata Y, Yamamura H, Hiraide A, Shimazu T, Yoshioka T (1999) Morbidity and mortality of hospitalized patients after the 1995 Hanshin-Awaji-earthquake. Am J Emerg Med 17:186–191
Tierney KJ (2006) Social inequality, hazards, and disasters. In: Daniels RJ (ed) On risk and disaster: lessons from Hurricane Katrina. National symposium on risk and disasters. University of Pennsylvania Press, Philadelphia, pp 110–128
Tural Ü, Coşkun B, Önder E, Çoarpçioğlu A, Yildiz M, Kesepara C, Karakaya I, Aydin M, Erol A, Torun F, Aybar G (2004) Psychological consequences of the 1999 earthquake in Turkey. J Trauma Stress 17:451–459
Vahaboglu H, Gundes S, Karandenizli A, Mutlu B, Cetin S, Kolayli F, Coskunkan F, Dündar V (2000) Transient increase in diarrheal diseases after the devastating earthquake in Kocaeli, turkey: results of an infectious disease surveillance study. Clin Infect Dis 31:1386–1389
Vanholder R, vander Tol A, Smet MD, Hoste E, Koç M, Hussain A, Khan S, Sever M (2007) Earthquake and crush syndrome casualties: lessons learned from the Kashmir disaster. Kidney Int 71:17–23
Watson JT, Gayer M, Conolly MA (2007) Epidemics after natural disasters. Emerg Infect Dis 13:1–5
Wen J, Shi YK, Li YP, Wang L, Cheng L, Gao Z, Li L (2009) Risk factors of earthquake inpatient death: a case control study. Crit Care 13:R24
Wenzel F, Daniell, J, Khazai, B, Kunz-Plapp, T (2012) The CEDIM forensic earthquake analysis and the test case of the 2011 Van earthquake. In: Proceedings of the 15th WCEE, 24–28 Sept 2012, Lisbon, Portugal
Whitman RV, Biggs JM, Brennan JE III, Cornell CA, De Neufville RL, Vanmarcke EH (1975) Seismic design analysis. J Struct Div, ST5, ASCE:1067–1084
Wiggins HH (1977) National losses and mitigation effects for air, earth and waterborne natural hazards. In: Proceedings of the second conference designing to survive severe hazards, IIT Research Institute, Chicago, pp 47–97
Wisner B, Blaikie P, Cannon T, Davies I (2004) At risk – natural hazards, people’s vulnerability and disasters, 2nd edn. Routledge, London
Wood NJ, Burton CG, Cutter SL (2010) Community variations in social vulnerability to Cascadia-related tsunamis in the US Pacific Northwest. Nat Hazards 52(2):369–389
Wright KC, Johnston DM (2010) Post-earthquake sheltering needs, how loss of structures and services affects decision making for evacuation. NZSCE conference, Wellington, New Zealand
Yavari S, Chang SE, Elwood K (2010) Modeling post-earthquake functionality of regional health care facilities. Earthquake Spectra 26(3):869–892
Yiannakoulias N, Bland W, Svenson LW (2013) Estimating the effect of turn penalties and traffic congestion on measuring spatial accessibility to primary health care. Appl Geog 39:172–182
Zhang Z, Shi Z, Wang L, Liu M (2011) One year later: mental health problems among survivors in hard-hit areas of the Wenchuan earthquake. Public Health 125:293–300
Zuccaro G, Cacace F (2010) Seismic casualty evaluation: the Italian model, an application to the L’Aquila 2009 event. In: Spence R, So E, Scawthorn C (eds) Human casualties in earthquakes, vol 29, Advances in natural and technological hazards research. Springer, Berlin. ISBN 978-90-481-9455-1
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2014 Springer Science+Business Media Dordrecht
About this chapter
Cite this chapter
Khazai, B., Daniell, J.E., Düzgün, Ş., Kunz-Plapp, T., Wenzel, F. (2014). Framework for Systemic Socio-economic Vulnerability and Loss Assessment. In: Pitilakis, K., Franchin, P., Khazai, B., Wenzel, H. (eds) SYNER-G: Systemic Seismic Vulnerability and Risk Assessment of Complex Urban, Utility, Lifeline Systems and Critical Facilities. Geotechnical, Geological and Earthquake Engineering, vol 31. Springer, Dordrecht. https://doi.org/10.1007/978-94-017-8835-9_4
Download citation
DOI: https://doi.org/10.1007/978-94-017-8835-9_4
Published:
Publisher Name: Springer, Dordrecht
Print ISBN: 978-94-017-8834-2
Online ISBN: 978-94-017-8835-9
eBook Packages: Earth and Environmental ScienceEarth and Environmental Science (R0)