
Abstract
The seismic performance of a regional Health-Care System (HCS) is investigated. The earthquake effects both on hospitals and on the Road Network (RDN), connecting towns to hospitals, are evaluated and the interaction among them accounted for. Victims move to hospitals until their request for a bed or for a surgical treatment is satisfied, if possible. A novel “dynamic” model for hospitalization is developed and implemented. The road network is modelled in connectivity terms. The vulnerability of hospitals and bridges is expressed by pre-evaluated fragility curves. Seismic hazard is described by a state-of-the-art model. The reliability problem is solved by Monte Carlo simulation. The un-hospitalized victims, the risk that hospitals are unable to provide medical care, the demand of medical care on hospitals, the hospitalization travel time, are among the useful results of the analysis. The methodology is exemplified with reference to a case-study region, with population of 877,000, 20 towns, 5 hospitals and 32 bridges.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
These keywords were added by machine and not by the authors. This process is experimental and the keywords may be updated as the learning algorithm improves.
11.1 Introduction
This study presents the probabilistic seismic assessment of a Health-Care System at regional scale. The response of hospitals and of the road network connecting them to neighboring towns jointly contribute to satisfy the demand of assistance by the victims of an earthquake. Damaged hospitals and collapsed bridges reduce and/or delay the capability of providing medical care to the victims. In addition, it is well known that the mortality rate is substantially reduced if those injured receive medical care in a short time; in fact, transportation of the victim plays a crucial role.
The evaluation of the reduced performances of the vulnerable elements is affected by a large uncertainty, which has to be added to the uncertainty associated to the seismic hazard. Thus, a probabilistic approach to tackle the problem is here used.
The short-term, emergency period after the seismic event (24/48 h) is the reference time-frame of the study. The main goal is to forecast the expected impact in terms of: (a) the number of un-hospitalized victims; (b) the risk of hospitals not being capable to provide the medical care required by the victims; (c) the demand of medical care on hospitals; (d) the travel time to hospitals.
The Emergency managers (e.g. Civil Protection), the hospital managers as well as all the authorities in charge of managing the emergency phase are the stakeholders which may be interested in the results of this study. The proposed methodology may also serve as a tool for planning risk mitigation measures, by considering alternative strategies (new hospitals, field hospitals, retrofitting bridges, etc.) and comparing the corresponding performances of upgraded systems.
This study follows the line of similar works by Nuti and Vanzi (1998) and Franchin et al. (2006).
11.2 Methodology
11.2.1 Hospital Facility and Treatment Capacity
The seismic assessment of a single hospital facility is studied in (Lupoi et al. 2008); results are employed in this study, which extends the analysis to a regional scale. The probabilistic procedure developed in the cited paper is briefly illustrated in this section.
The hospital is described as a system made of three vulnerable components: physical, human and organizational. These components jointly contribute in providing the medical services for the treatment of patients.
The physical component is the building where the medical services are delivered. It is made of structural elements and non-structural elements (architectural elements, basic contents and equipment). While the former are critical to preserve the life-safety of the occupants, the latter are fundamental to preserve hospital functionality.
The human component is the hospital staff: doctors, nurses and in general whoever plays an active role in providing medical care.
The organizational component is the set of standardized procedures established to ensure that medical services are delivered under appropriate conditions.
The study of the hospital’s functioning under emergency conditions has led to the identification of a sub-set of medical services that have to stay operative in order to guarantee, after a seismic event, adequate treatment of patients and victims. These are classified as essential medical services and typically are: Emergency department; Operating theatres; Intensive care unit; Diagnostics; Blood bank; Hemodialysis; Urology; Neonatology; Gynecology/Obstetrics; Pediatrics; Laboratory; Pharmacy. In addition, it has to be considered that the hospital layout (i.e. the location of medical services) during an emergency can be modified with respect to the “standard” one, i.e. the one developed for daily routine.
Previous experiences have shown that surgery is the bottleneck of medical care services after a mass-casualty event that produces trauma victims. Therefore, the number of surgical treatments that can be operated is selected as the seismic performance measure of a hospital. The number of functioning operating theatres is of primarily importance, of course, but other factors have to be also accounted for. In fact, the proposed “hospital treatment capacity” index, HTC, is given by the expression:
where: α accounts for the efficiency of the emergency plan (organizational component), β accounts for the quality, training and preparation of the operators (human component), t m is the mean duration of a surgical operation, γ 1 is the number of operating theatres which remain operative after the hazardous event, γ 2 is a Boolean function equal to 1 if the system “survives” and nil otherwise. The survival condition is defined as follows:
-
(a)
the “operational” limit state has to be satisfied for the areas of the building devoted to the essential medical services;
-
(b)
the “safeguard of human life” limit state has to be satisfied for all other areas.
Condition (a) depends on the response of both structural and non-structural elements, while condition (b) depends on the response of structural elements only.
It is noted that all components “contribute” to the determination of the HTC index. At the current stage of development, the influence of the organizational and human components on HTC is empirically estimated by expert judgment. The quality of the emergency plan provides the elements for the estimate of the coefficient α; its value typically ranges from 0.5, for very poor emergency plans, up to 1 for excellent and complete ones. The exam of the available resources and of the operators’ skill to put in practice the emergency plan provides the elements for the estimate of the β factor; its value may range from 0.5, for poorly trained and understaffed operators, up to 1, for well-trained and adequately-staffed operators.
The γ 1 and γ 2 factors are instead evaluated analytically on the basis of engineering methods. The number of functioning operating theatres, γ 1 , is derived from the results of structural analysis, taking into accounts also the effects on the non-structural elements.
The Boolean factor γ 2 is estimated building up a fault-tree of the physical component, which schematically depicts the vulnerable elements (columns, beams, joints, portioning walls, ceiling, windows, furniture, machineries, equipment, pipelines, etc.) and their functional interrelationship. The fault-trees of sub-systems (electrical power, medical gasses, water, elevators, etc.) are appropriately “assembled” to build up the “system” fault-tree of the whole physical component. This is hospital-dependent and has to be customized on a case-by-case basis. A preliminary, thorough examination of the vulnerable elements is recommended in order to reduce as much as possible the branches of the system fault-tree. The fault-tree analysis establishes the relationship between the state of the vulnerable elements and the state of the system.
The fragility curve of the physical component is calculated employing an “advanced” structure-specific approach, which splits in two the reliability problem (Pinto et al. 2004) in order to reduce the computational burden. Uncertainties related to structural properties (strength of materials, amounts of reinforcement, capacity models, etc.) and to the seismic hazard are both taken into account. First, a relationship between the structural response quantities D (forces, displacements and deformations) and the ground motion intensity measure, IM, is derived by means of a reduced number of numerical analyses carried out for the mean values of the structural random variables. Then, a standard Monte Carlo simulation is performed without carrying out any further structural analysis since, at each run, the response of the structure for the sampled r.v.’s is obtained from the D(IM) relationship. The state of the system is evaluated at each run of the simulation: if it fails, i.e. γ 2 = 0, no surgical treatment can be operated, and hence HTC is also nil.
The final outcome of the methodology is the fragility curve for the hospital performance index: HTC = f(IM).
11.2.2 Casualty Model and Hospital Treatment Demand
The demand for hospitalization is estimated combining casualty models and epidemiological studies.
Casualty models provide a rapid estimate of the earthquake impact on population for the purpose of response planning and mitigation. Engineers have developed them from limited, anedoctal and historical data. The model by Coburn and Spence (1992), as simplified by Nuti and Vanzi (1998), is here employed. The casualties, C, understood as the “Severely-Injured” (SI) and the deaths, are estimated as a percentage of the population through the following expression:
where I is the intensity measure of the seismic event,Footnote 1 k and I min are model parameters which take into account the occupancy rate and the vulnerability of the building stock, respectively. The model parameters have to be calibrated as function of the environmental conditions. The “Lightly-Injured” (LI) people, defined as those not requiring hospitalization, are not included in the estimate given by Eq. (11.2).
In this study an error term having lognormal distribution, unit median and coefficient of variation, ε cas , equal to 0.3, is applied to the expression in Eq. (11.2) in order to account for the large uncertainties that affect the model. The number of casualties is then given by:
where N pop is the population of the area affected by the earthquake.
The estimate of the people requiring hospitalization, N SI , is of interest for the scope of this study. The proportion of people severely injured and the deaths can be derived from epidemiological studies, which investigate the patterns of disease and injury in human population and provide information of the type and amount of resources needed to treat casualties. The types and numbers of casualties vary with the characteristics of the earthquake, the building stock in the struck area, the demography and also with the time of the day when the earthquake occurs. The “medical severity” of a hazardous event is assessed by two severity indexes:
which gives an indication of the overall severity of the event (deaths over all injured), and
which measures the severity of the injuries caused by the event (“Severely-Injured” over “Lightly-Injured”). The larger is S 2 , the greater is the demand of medical care. Data from past earthquakes show that S 1 is comprised between 0.1 and 0.5, while S 2 between 0.15 and 0.6. The ratio deaths/“Severely-Injured” is obtained combining Eqs. (11.4) and (11.5):
Finally, the number of victims requiring hospitalization, N SI , is obtained by combining Eqs. (11.6) and (11.3):
The Hospital Treatment Demand, HTD, is defined as the sub-set of the Severely-Injured that require a surgical treatment:
The coefficient ζ is defined on a case-by-case basis by expert opinion; it typically ranges between 1/3 and 1/2.
The complement of HTD is the number of victims to whom it is sufficient to assign a bed to administer the necessary medical care:
11.2.3 Road Network
In this study the function of the road network is to allow the transportation of the injured to hospitals. The primary interest is to identify the portions of the network that may be critical with respect to connectivity as a consequence of the seismic damages eventually experienced by its vulnerable elements.
The analysis is carried out in terms of pure connectivity, i.e. traffic flows are not modeled. This is coherent with the time-frame of the study, which is limited to rescue operations in the aftermath of the seismic event. This approach requires a simple description of the network based on basic graph theory. The road network is represented as a graph consisting of n nodes or vertices, connected by n a arcs, or links or edges. The relationship between nodes and arcs is described by the adjacency matrix B = [b ij ], which is an n × n Boolean square matrix, whose terms are either 0, when no connection exists between nodes i and j, or 1 when a connection exists. A free-flow travel speed is assigned to each arc of the graph.
Towns within the region are “concentrated” at the graph’s nodes; each node is called TAZ (Traffic Analysis Zone). Hospitals are “housed” within towns. A zero-distance/zero-travel time connection is assumed for a hospital and its “hosting” town.
It is assumed that the highways free-flow speed does not change after a seismic event, while a 50 % reduction in speed is considered for the urban portions of the road network in order to account for potential road blockages.
11.2.4 Transportation and Medical Treatment Model of the Victims
Transportation is assumed to take place by private vehicles on the damaged road network. The selection of the hospital, made by users, is affected by both objective constraints and subjective choices. The closure of a road represents one of the former; the user “familiarity” with a specific facility is one of the latter. This section briefly addresses the proposed model for the transportation of casualties to the hospitals of the region of interest.
The implemented hospitalization algorithm is “dynamic”: the process follows a chain of events, which are scheduled in ascending order based on their time of occurrence, elapsed from the earthquake time. Victims are allocated based on their arrival time, i.e. following the “first-come, first-served” criterion.
At the very beginning of the process, for each TAZ an event is created to allow its casualties, if present, to be moved to the closest hospital, i.e. the one which can be reached within the minimum travel time. All events are stored in an event matrix, recording the occurrence time, the origin TAZ, the destination hospital and the number of estimated victims which are going to move.
Before starting to go through all the events, the health-care capacity of all the regional hospitals is checked, both in terms of \( \overline{HTD} \) (by counting the number of available beds) and in terms of HTD (verifying that the HTC of the damaged hospitals is greater than zero). “Unavailable” hospitals are excluded.
Successively, the single events are analyzed in their order of occurrence. For each event, in case the destination hospital is able to receive all incoming victims, its capacity is reduced and the next scheduled event is taken into consideration. On the contrary, if the destination hospital is severely damaged (not operative, γ2 = 0) or has its capacity saturated, separately for the two types of victims (in terms of number of available beds or number of functioning operating theatres), all or a portion of the victims cannot be hospitalized and, hence, these are forced to move to the closest hospital facility (which has not been visited yet). In this case, in the event matrix is added a further event, with an occurrence time given by the travel time needed to reach the destination hospital at hand plus the travel time to the next hospital. The event matrix is then sorted again.
The iterative process is concluded either when all the casualties are hospitalized or when all the functioning hospitals in the region are saturated (all available beds are assigned or HTC ≤ HTD).
An alternative modeling choice could be to assume that the injured victims that do not need a surgical treatment, i.e. \( \overline{HTD} \), always receive medical assistance at the first operative hospital reached. This assumption of “infinite” beds capacity is justifiable in view of the emergency procedures’ activation, where the number of beds may be doubled with respect to the standard, “every-day” condition (eventually by field hospitals).
11.2.5 System’s Performance Indicators
A number of results which are useful primarily for hospital disaster managers and civil protection can be inferred from this study. We have selected the following ones: (a) the mean annual frequency of un-hospitalized victims, subdivided into those requiring a surgical treatment and those requiring a bed, as performance measure of the regional health-care system; (b) the risk that a hospital is not capable of providing the required surgical treatment (HTC < HTD), as performance indicator for a single facility; (c) the (expected) demand of medical care on each hospital, an essential information to get prepared and to cope with the emergency; (d) the (expected) number of un-hospitalized victims subdivided by towns, a useful information for policy makers; (e) the (expected) maximum travel time for hospitalization, an indicator of the adequateness of the road network and an indication for future upgrade and/or seismic retrofit. All the above information may be useful for the allocation of resources.
11.3 Treatment of Uncertainties
The regional system under assessment is affected by many and large uncertainties of different types, from those related to the regional seismic activity and the (corresponding) local intensity at each site, to those related to the physical damage state as a function of local intensity, to the uncertainty on the parameters (or even the form) of the fragility models employed.
Uncertainty on the seismic hazard is modeled through two models, the event model and the local intensity model (Franchin and Cavalieri 2013). The event model starts with a continuous variable M for the event magnitude, continues with a discrete random variable Z for the active zone, with as many states as the number of seismo-genetic zones, and ends with a random variable L for the epicenter location within the active source. Distributions vary according to the adopted sampling scheme, but that of Z is conditional on the sampled value of M, and that of L is conditional on the sample zone Z.
The local intensity measure at the sites of vulnerable components is described with a vector of IMs that are needed as an input to the corresponding fragility model. A scalar random field of a so-called “primary IM”, e.g. peak ground acceleration (PGA) on rock (no amplification yet), is first sampled as a function of the sampled M and L on a regular grid covering the study region, employing a ground motion prediction equation (GMPE) with inter- and intra-event error terms η and ε. In the application to follow the employed GMPE is that by Akkar and Bommer (2010). Intra-event residuals ε are modeled as a spatially correlated random field (Jayaram and Baker 2009) by means of an exponential auto-correlation function derived for Italian events and consistent with the Akkar and Bommer GMPE in (Esposito et al. 2010). The need for sampling on a regular grid first arises to avoid singularity problems in the covariance matrix of intra-event residuals, since sites usually occur in clusters with very similar source-to-site distances. The primary IM is then interpolated to all sites and “secondary IMs” (all other components in the intensity vector at a site) are sampled from their distribution conditional on the primary IM value (postulating joint lognormality of the IMs, see e.g. Bazzurro and Cornell 2002, and using inter-IM correlation values from Baker and Cornell 2006).
The uncertainty related to the vulnerable components, i.e. hospitals and bridges, is accounted for by means of pre-evaluated fragility functions. Its derivation is out of the scope of this study; therefore these are taken from previous studies. The derivation of the fragility curve for a hospital is illustrated in Sect. 11.2.1.
The uncertainty in the estimation of the victims is accounted for by the random variable ε cas as described in Sect. 11.2.2.
The reliability problem is solved employing a standard simulation-based method. A simulation run is carried out as part of either a plain (robust) Monte Carlo simulation or a more (computationally) effective importance sampling scheme (e.g. Jayaram and Baker 2010). The state of all components is sampled as a function of the input intensity measures; once this is known, the functional analysis of the regional system is carried out to determine its performance. Interactions among components are considered at this stage such as, for instance, detour to reach hospitals from area districts due to closure of damaged portions of roads.
11.4 Example Application
11.4.1 The Case Study Area
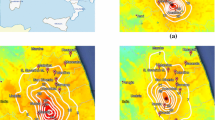
A hypothetical region composed of towns, hospitals and a road network is shown in Fig. 11.1. The architecture is developed from the application example in Kang et al. (2008), with some modifications and additions in order to form an infrastructure that is subjected to a distributed seismic hazard and in which the road network and hospital care system (RDN/HCS) interaction is taken into account. The seismo-genetic area sources that can generate events affecting the region are also shown in Fig. 11.1, together with their corresponding activity parameters for the truncated Gutenberg-Richter recurrence law: lower and upper magnitude limits M L and M U , magnitude slope β, and mean annual rate of events with M > M L in the source λ.

The regional study area
The transportation network connects 20 towns by highways with 32 bridges. A pure connectivity approach is employed, i.e. no traffic flows are computed in the damaged network. For simplicity, given the illustrative character of the application, it is assumed that no other roads aside from the highways exist between cities and that the bridges are the only vulnerable components, whose earthquake-induced damage may cause paths to be disconnected.
The 20 towns have populations ranging from 22,000 to 70,000 inhabitants, for a regional population equal to 877,000. The towns centroids (TAZs) are taken as the RDN nodes.
The HCS comprises five hospitals, located in towns #5, 8, 12, 16 and 18. The total number of beds is taken as 0.4 % of population; an occupancy, pre-earthquake rate equal to 80 % is assumed. Hospitals relevant data are summarized in Table 11.1.
The fragility curves employed for the hospitals in the region are relative to an existing RC hospital located in Italy (Lupoi et al. 2008). These have been computed as described in Sect. 11.2.1, introducing uncertainties in both structural and non-structural elements. The factors α and β in Eq. (11.1) have been taken equal to 1 and 0.8, respectively. The reference hospital is equipped with eight operating theatres; the mean duration of a surgical treatment has been taken equal to t m = 2 h. It was assumed that in emergency condition a theatre works 24 h continuously; 24 h is also the maximum time that a severely injured patient can wait for the surgical treatment. The maximum HTC for the undamaged configuration of the reference hospital is then: HTC undamaged = [(1 × 0.8 × 1 × 1)/2] × 24 × 8 = 77 treatments per day.
Figure 11.2 shows three HTC fragility curves, expressing the damaged or residual (post-seismic conditions) HTC as a function of the ground motion PGA. The displayed curves, corresponding to the mean and the mean minus/plus one standard deviation fragility curves, are indicated as curves #1, #2 and #3, and have been assigned to the five hospitals as indicated in Table 11.1.

HTC fragility curves for hospitals
Two types of bridge are included in the road network: single-bent and two-bent overpasses. The corresponding fragility curves, expressing the conditional probability of attaining or exceeding the collapse limit state for a given value of PGA, are shown in Fig. 11.3. At each run of the Monte Carlo simulation, the state of a bridge can be “collapsed” or “survived”; no “intermediate” states are considered.

Fragility curve for bridges
The casualty model parameters k and I min in Eq. (11.2) are taken equal to 0.05 and 4, respectively; the severity indexes S 1 and S 2 in Eq. (11.7) are taken equal to 0.154 and 0.625, respectively (FEMA 1999).
11.4.2 Simulation Results
A plain Monte Carlo simulation with 10,000 runs is carried out to test the proposed methodology.
The global performance of the regional Health-Care System is measured in terms of the number of victims that cannot receive the medical care. The Mean Annual Frequency (MAF) of exceedance curves for un-hospitalized victims subdivided by HTD and \( \overline{HTD} \), normalized to the regional population, are shown in Fig. 11.4. The same curves can also be referred in terms of return period. This latter is commonly used to better communicate the actual risk to stakeholders. For example, the return period of an event where 0.1 % of the regional population cannot receive the (needed) surgical treatment is about 40 years.

MAF curves of normalized victims (divided in two categories) that are not allocated in hospitals
The performance of the hospitals in the region is expressed in terms of the probability of not being able to provide the required surgical treatments to victims if an earthquake strikes the region (i.e. the risk), as shown by the bar plot in Fig. 11.5. The risk is higher for the hospitals located in TAZ #8 and #12, because their “tributary” area is greater than the one of the three other hospitals and also because of the proximity to the central seismic source #3.

P(HTD ≥ HTC), for the five hospitals
The (expected) demands of medical care on hospitals are indicated in the area plot of Fig. 11.6. This is the basic information which is needed by hospital disaster managers and civil protections to set up adequate emergency strategies. The higher demand is registered for the central hospital in TAZ #12 for the same reason given above: the (expected) number of victims requiring a surgical treatment that reach the hospital in TAZ #12 is 222. It is noted that this number includes also those that can not be hospitalized in this hospital for “saturation” of its capacity (damaged HTC) and have to move to the closest one, the selection of the latter depending on the state of damaged road network. The hospitalization process of the victims takes place within the first 24 h after the event, or in an even shorter period.

(Expected) demand of medical care on hospitals
The (expected) number of victims not able to receive medical care is indicated in the area plot of Fig. 11.7; victims are referred to their town of origin. These data give indication of the critical (worst-served) towns, information that can be useful to policy makers for the planning of new facilities and/or for the retrofit of existing ones.

(Expected) victims not able to receive medical care
Finally, the (expected) maximum hospitalization travel time for the investigated region is about 70 min. The moving average μ and moving standard deviation σ are computed at each simulation run. Corresponding curves of μ and μ ± σ are shown in Fig. 11.8. The mean of the indicator becomes stable after about 1,000 runs; this justifies the adopted number of runs.

Evolution of maximum travel time for hospitalization
11.5 Conclusions
A methodology for the seismic assessment of a regional Health-Care System is illustrated in this study. The system is composed of hospitals, towns and a road network. The road network is deputed to connect towns to hospitals allowing the transportation of the injured people.
A probabilistic approach has been employed to model the large uncertainties that affect the problem. The vulnerability of the main components of the system, i.e. hospitals and bridges, is accounted for as well as their interaction. In particular, the hospitals’ capacity and the bridges’ physical damage are represented by fragility curves. Uncertainties in the evaluation of the casualties are also introduced. A state-of-the-art model to compute the seismic hazard is also employed. Finally, a “dynamic” model for the hospitalization of the victims has been developed and implemented: the path of the victims from the town of origin to the hospital of destination through the road network is considered. Hospitalization, for each homogenous type of victims, is accorded on a “first-come, first-served” criterion. This model represents a novelty of the proposed methodology with respect to other similar applications available in the literature.
The reliability problem is solved by Monte Carlo simulation. A number of interesting results are provided by the analysis: the number of un-hospitalized victims expressed either as mean annual frequency of exceedance or as return period; the risk of not being able to provide the required medical care for each hospital of the region; the (expected) demand of medical care on each hospital; the (expected) un-hospitalized victims for each town in the region; the (expected) maximum hospitalization travel time. These results are certainly of great value to emergency managers, policy makers and authorities involved in planning emergency operations and in developing mitigation strategies.
The capability of the proposed methodology is successfully tested through the application to a realistic study region.
Notes
- 1.
In the original model the intensity measure is the Modified Mercalli Intensity (MMI); the relationship in (Wald et al. 1999) is employed to convert MMI into PGA.
References
Akkar S, Bommer JJ (2010) Empirical equations for the prediction of PGA, PGV and spectral accelerations in Europe, the Mediterranean region and the Middle East. Seismol Res Lett 81(2):195–206
Baker JW, Cornell CA (2006) Correlation of response spectral values for multicomponents ground motions. Bull Seismol Soc Am 96(1):215–227
Bazzurro P, Cornell CA (2002) Vector-valued probabilistic seismic hazard analysis (VPSHA). In: 7th U.S. national conference on earthquake engineering, Boston, MA, 21–25 July 2002, Paper no. 61
Coburn A, Spence R (1992) Earthquake protection. Wiley, Chichester
Esposito S, Iervolino I, Manfredi G (2010) PGA semi-empirical correlation models based on European data. In: 14th European conference on earthquake engineering, Ohrid, FYROM
FEMA (1999) Earthquake loss estimation methodology Hazus99 SR2: Technical Manual. Federal Emergency Management Agency, Washington, DC
Franchin P, Cavalieri F (2013) Seismic vulnerability of a complex interconnected infrastructure. In: Tesfamariam S, Goda K (eds) Handbook of seismic risk analysis and management of civil infrastructure systems. Woodhead Publishing Limited, Cambridge. ISBN 978-0-85709-268-7 (Not yet published)
Franchin P, Lupoi A, Pinto PE (2006) On the role of road networks in reducing human losses after earthquakes. J Earthq Eng 10(2):195–206
Jayaram N, Baker JW (2009) Correlation model of spatially distributed ground motion intensities. J Earthq Eng Struct Dyn 38(15):1687–1708
Jayaram N, Baker JW (2010) Efficient sampling and data reduction techniques for probabilistic seismic lifelines assessment. Earthq Eng Struct Dyn 39(10):1109–1131
Kang W-H, Song J, Gardoni P (2008) Matrix-based system reliability method and applications to bridge networks. Reliab Eng Syst Saf 93(11):1584–1593
Lupoi G, Franchin P, Lupoi A, Pinto PE, Calvi GM (2008) Probabilistic seismic assessment for hospitals and complex-social systems, Rose School technical report 2008/02. IUSS Press, Pavia. ISBN 978-88-6198-017-4
Nuti C, Vanzi I (1998) Assessment of post-earthquake availability of hospital system and upgrading strategies. Earthq Eng Struct Dyn 27(12):1403–1423
Pinto PE, Giannini R, Franchin P (2004) Seismic reliability analysis of structures. IUSS Press, Pavia
Wald DJ, Quitoriano V, Heaton TH, Kanamori H (1999) Relationships between peak ground acceleration, peak ground velocity, and modified Mercalli intensity in California. Earthq Spectra 15(3):557–564
Acknowledgements
The contribution of Dr Giorgio Lupoi for the development of hospitals’ fragility curves is gratefully acknowledged.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2014 Springer Science+Business Media Dordrecht
About this chapter
Cite this chapter
Lupoi, A., Cavalieri, F., Franchin, P. (2014). Application to a Network of Hospitals at Regional Scale. In: Pitilakis, K., Franchin, P., Khazai, B., Wenzel, H. (eds) SYNER-G: Systemic Seismic Vulnerability and Risk Assessment of Complex Urban, Utility, Lifeline Systems and Critical Facilities. Geotechnical, Geological and Earthquake Engineering, vol 31. Springer, Dordrecht. https://doi.org/10.1007/978-94-017-8835-9_11
Download citation
DOI: https://doi.org/10.1007/978-94-017-8835-9_11
Published:
Publisher Name: Springer, Dordrecht
Print ISBN: 978-94-017-8834-2
Online ISBN: 978-94-017-8835-9
eBook Packages: Earth and Environmental ScienceEarth and Environmental Science (R0)