
Abstract
With a median survival period of approximately 19 months, therapeutic options for patients with castration-resistant prostate cancer (CRPC) remain limited. In a multicenter phase II trial, 65 patients with histologically confirmed CRPC continuously received a biomodulatory regimen during the 6-month core period for redirecting tumor-promoting normative notions, i.e. angiogenesis, inflammation, immune response and the osteoplastic process. Treatment comprised daily doses of imatinib mesylate, pioglitazone, etoricoxib, treosulfan, and dexamethasone. The primary endpoint was prostate-specific antigen (PSA) response, defined as a confirmed reduction in serum PSA of ≥ 50 % in patients with a baseline value of ≥ 5 ng/mL. Responders could enter an extension phase until disease progression or presence of intolerable toxicity. Mean PSA was 45.3 ng/mL at baseline, and 77 % of the patients had a PSA doubling time of < 3 months. Twenty three (37.7 %) out of the 61 evaluable patients were PSA responders, who showed a mean PSA decrease from 278.9 ± 784.1 ng/mL at baseline to 8.8 ± 11.6 ng/mL at the final visit (24 weeks or LOCF). The remaining 38 non-responders included 14 patients (23.0 %) with stable disease. In one center, 6 out of 16 patients showed nearly complete resolution of bone metastases. Out of the 947 adverse events observed, 57.6 % were suspected to be drug-related, 13.8 % led to dose adjustment or permanent discontinuation of the study medication, and 40.2 % required concomitant medication. Twenty seven patients experienced serious adverse events. This novel multi-targeted approach led to an impressive PSA response rate of 37.7 % in CRPC patients despite the fact that individual components had shown limited efficacy when applied on their own. The good PSA response rate and the manageable toxicity profile suggest that this combination may offer an alternative treatment option to present therapeutic regimens.
Clinical trial registration: NCT00427999 (http://clinicaltrials.gov/ct2/show/NCT00427999)
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others

Keywords
- Imatinib Mesylate
- Eastern Cooperative Oncology Group Performance Status
- Abiraterone Acetate
- Normative Notion
- Core Trial
These keywords were added by machine and not by the authors. This process is experimental and the keywords may be updated as the learning algorithm improves.
Introduction
The natural history of metastatic prostate cancer may be divided into two phases: the castration-sensitive stage and the castration-resistant stage, the latter stage requiring a complete change of treatment strategy (Fig. 5.1).

During progression from the organ-confined stage to the clinical metastatic stage, tumors acquire multifold asynchronous chromosomal and molecular-genetic aberrations. Applied systems biology in metastatic tumors may meet this therapeutic challenge by targeting a tumor’s normativity, thereby simultaneously and equally targeting tumor and stroma cells
In recent years, a variety of novel compounds have shown a survival benefit in castration-resistant prostate cancer (CRPC), for instance, the vaccine taxane cabazitaxel (Sipuleucel-T) and the androgen biosynthesis inhibitor abiraterone acetate [1, 2]. Further agents are currently under investigation [3], for example, androgen receptor inhibitors (MDV3100), androgen biosynthesis inhibitors, immune-modulating compounds (PROSTVAC-VF), as well as angiogenesis inhibitors (thalidomide, lenalidomine, aflibercept, tasquinimod), orteronel (TAK-700), and radium-223 chloride (Alpharadin). The availability of these new therapeutic approaches allows the exploration of sequential treatment regimens in an attempt to balance the risks and benefits of novel compounds for individual patients with CRPC.
After exploiting novel therapy strategies for achieving hormonal ablation, the standard therapy during the castration-refractory stage is chemotherapy (docetaxel) combined with prednisone. Our novel biomodulatory therapy approach aimed at achieving at least the same efficacy levels (PSA response rate) as chemotherapy while simultaneously avoiding particularly grade 3 and 4 toxicity levels that are commonly associated with pulsed chemotherapy.
We report the findings of a phase II, single-arm, multicenter trial, in which patients with CRPC received a combination of biomodulatory agents. In contrast to conventional treatment strategies, our multi-targeted therapy exploited the molecular and genetic heterogeneity of both tumor and stroma cells in CRPC [4–6]: A biomodulatory approach of this type aims at comprehensively targeting the pathogenic mechanisms of CRPC, including some of the classic ‘hallmarks’ of cancer, such as tumor-associated inflammation, angiogenesis, and immune response. Each of these conditions is highly relevant in prostate cancer: Inflammation plays a crucial role in its pathogenesis [7–9], tumor-associated angiogenesis is obligate, and prostate cancer is known to principally be an immunogenic tumor [8–12]. In addition, the current regimen targets the contribution to tumor growth in CRPC made by osteoblasts because osteoblastic metastases represent up to 80 % of organ metastases in prostate cancer [13]. The aim of the multi-targeted treatment regimen in this trial is to modulate and redirect the tumor and stroma cells via ubiquitous and non-oncogene-addicted targets including PDGFR (imatinib) [14, 15], the PPARalpha/gamma receptor (pioglitazone) [16–21], the glucocorticoid receptor (dexamethasone) [20, 21], and the cyclooxygenase-2 inhibitor (etoricoxib) [24, 25]. Such effects are coupled with the pleiotropic/immunomodulatory and angiostatic activity of metronomic low-dose chemotherapy using treosulfan via regulatory T-cells and thrombospondin-1 [26, 27] (Table 5.1). In the current regimen, these drugs were administered to achieve concerted biomodulatory activity by imposing therapeutic boundary conditions in the normative growth of CRPC. Two of the drugs, dexamethasone [22, 23, p. 223] and metronomic low-dose chemotherapy with alkylating agents [28–30], have previously shown mono-activity in CRPC (Fig. 5.2). Other drugs have shown activity in in vitro or animal models but have failed to induce a response in vivo (pioglitazone [20]) or to improve response when added to taxotere (imatinib [15]).

Patients received the all-oral biomodulatory therapy during the core phase. In case of stable disease or > 50 % PSA response, patients were allowed to proceed to the extension phase until disease progression
Patients and Methods
Study Design and Conduct
This single-arm, open-label, 6-month phase II trial was conducted at 11 German oncology centers. Patients with CRCP received imatinib mesylate, pioglitazone, etoricoxib, treosulfan, and dexamethasone until progression of the prostate-specific antigen (PSA) (Fig. 5.3). At the end of the core 6-month trial, patients responsive to study medication (defined at a PSA decrease of ≥ 30 % from baseline and a 24-week treatment period without any signs of disease progression) proceeded to an extension phase until disease progression or presence of intolerable toxicity levels. The study protocol had been approved by the institutional review board of the participating centers and by the health authorities. Written informed consent from patients had been obtained before enrolment.

Quality of life scores remained stable throughout the core phase for all patients regardless of response behavior
The trial was sponsored by Novartis Pharma GmbH and registered at ClinicalTrials.gov (NCT: NCT00427999).
Study Population
Male patients aged ≥ 18 years were included, who had histologically confirmed prostate cancer with proven progression after androgen deprivation therapy (surgical or medical castration). For inclusion, patients had to have total serum testosterone of < 1.72 nmol/L (50 ng/dL). Patients also had to be castration-resistant, which needed to be confirmed by three consecutive elevated (≥ 50 % above nadir) serum PSA tests separated by at least two weeks, and the last 2 PSA measurements had to be ≥ 5.0 ng/mL despite secondary hormonal manipulations (according to the European Association of Urology (EAU)) [31]. Additional inclusion criteria were a performance status of ≤ 2 according to the Eastern Cooperative Oncology Group (ECOG), an adequate hematological status (defined as absolute neutrophil count > 1,500/mm3, platelet count > 75,000/mm3), normal hepatic, renal, and cardiac function, and a life expectancy of at least 6 months. Key exclusion criteria included use of chemotherapy, treatment with imatinib or other tyrosine kinase inhibitors, concomitant therapy with other tumor treatments except for LHRH agonists, concomitant warfarin, phenprocoumon or other oral anticoagulant treatment, radiotherapy of > 25 % of the bone marrow, systemic radioisotope therapy, uncontrolled brain metastases, regular blood transfusions, and previous secondary malignant disease within the past 5 years. Patients with the following comorbidities were excluded: Symptomatic congestive heart failure, unstable angina or recent myocardial infarction, uncontrolled diabetes, chronic hepatic or renal disease, active uncontrolled infection, chronic inflammatory intestinal disease, autoimmune disease or a known diagnosis of HIV, or hepatitis B or C infection.
Interventions
Eligible patients received oral doses of imatinib mesylate (400 mg daily), pioglitazone (60 mg daily), etoricoxib (60 mg daily), treosulfan (250 mg twice daily), and dexamethasone (1 mg daily) until PSA progression. Patients with PSA progression were switched to a dose of 400 mg imatinib twice daily and treosulfan 250 mg daily; in case of further progression, patients were withdrawn from the trial. Dose reductions were permitted for intolerable non-hematologic or hematologic grade 2 toxicity or any grade 3 or 4 toxicity. Study medication was restarted after the toxicity of the respective drug(s) had resolved or decreased to less than grade 2 or less than grade 3, depending on the toxicity and respective drug. If toxicity recurred despite dose reduction(s), the relevant drug was withdrawn. Dose reductions, if required, were specified as follows: Reduced dose for imatinib depending on dose and toxicity grade (between 200–600 mg/day, 60 mg every second day for etoricoxib, 45 mg/day for pioglitazone, 0.5 mg/day for dexamethasone, and 250 mg/day for treosulfan). Study participation was discontinued if medication could not be maintained at a minimum of treosulfan 250 mg/day in addition to one biomodulator (etoricoxib or pioglitazone or imatinib) plus dexamethasone after a 4-week interruption because of grade 2–4 toxicity. Patients were also to discontinue the trial if they refused to continue therapy, in response to protocol violations, or administrative problems (Table 5.2).
Concomitant use of bisphosphonates was allowed.
Evaluation
During screening, all patients underwent imaging by CT, MRI, or plain radiography as necessary to confirm metastatic sites. A radioisotope bone scan was conducted for patients with bone metastases. Pre-treatment evaluations included medical history, ECOG performance status and vital signs, physical examination, electrocardiogram laboratory screening including PSA and testosterone levels, coagulation assessment, urinalysis, electrocardiography, and assessment of quality of life (EORTC-30 questionnaire). During the 6-month core trial, PSA values, ECOG performance status, and quality of life were assessed monthly. Physical examination, vital signs, and blood tests were conducted after 1, 2, 4, 8, 12, and 16 weeks, and coagulation was measured after 4 weeks and subsequently, if clinically indicated. Urinalysis and imaging by CT, MRI, plain radiography, or bone scanning were conducted as clinically indicated. At the final visit of the core trial, ECOG performance status, vital signs, and concomitant medication and therapies were recorded, and physical examination, laboratory screening including PSA, coagulation and urinalysis, quality of life assessment, and imaging (if clinically indicated) were conducted. Adverse events were monitored throughout the trial and graded according to the Common Terminology Criteria for adverse events established by the National Cancer Institute (version 3.0).
Study Endpoints
The primary endpoint was PSA response, defined as a reduction in serum PSA of ≥ 50 % compared to baseline value; confirmation was obtained by a second PSA value 3–4 weeks later. Patients who did not fulfill these criteria were defined as PSA non-responders and were categorized as having PSA progression or stable disease. PSA progression was defined as a PSA increase of at least 50 % over baseline or an increase of at least 25 % over baseline with an absolute PSA increase of 5 ng/L, which had to be confirmed 3–4 weeks later. PSA non-responders were considered to have stable disease if they did not meet the criteria for progressive disease. Tumor response was evaluated by the Response Evaluation Criteria in Solid Tumors (RECIST) [13], if adequate imaging data were available for follow-up.
Secondary endpoints included the time to PSA response (defined as the time from the first administration of the study drugs to the first confirmed PSA response), progression-free survival (defined as the time from the first administration of the study drugs to the first date of PSA progression, overall survival during the extension phase of the trial, quality of life including pain response (EORTC-30 questionnaire), and safety and tolerability of the combined therapy.
Statistical Analysis
The sample size calculation estimated that 46 evaluable patients would be required to distinguish between the two rates 40 % (p 1) and 25 % (p 0) with a one-sided alpha of 10 and 80 % power under the assumption of a 20 % dropout rate [2]. Sample size was estimated according to exact binomial probabilities. The first design (and hence the lowest number) that satisfied the design criteria (alpha and power constraints) was chosen.
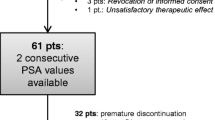
The intent-to-treat (ITT) population was defined as patients who received at least one dose of the study medication and who provided two consecutive post-baseline PSA values. The number of PSA responders is presented with the corresponding 95 % confidence interval for ITT populations. Data on quality of life as assessed by the EORTC-30 questionnaire are presented descriptively.
Results
Patients
Between February 2007 and October 2009, 65 patients received at least one treatment with the study medication; 61 out of these 65 patients provided two consecutive PSA values and were thus included into the ITT population (Table 5.3). Thirty-two patients discontinued the trial prematurely, mostly because of disease progression (n = 13), consent withdrawal (n = 9), or withdrawal of medication because of side effects (n = 6). The mean time in the core trial was 141 days, and the mean duration of at least minimal therapy was 121 days.
Eighteen patients entered the extension phase of the trial, which is still ongoing. One patient has been followed in the extension trial since June 2008 without any disease progression or occurrence of intolerable toxicity levels. Mean PSA at baseline was 45.3 ng/mL with values ranging from 5 to 3603 ng/mL. Approximately 78 % of the patients had bone metastases, 34 % had measurable lymph node involvement, and 8 % had measurable organ involvement (Table 5.1).
Combined Modularized Therapy
PSA response
Twenty three patients showed PSA response (37.7 %, 95 % CI 50.1, 74.5). Among responders, mean PSA levels decreased from 278.9 ± 784.1 ng/mL at baseline to 8.8 ± 11.6 ng/mL at the last visit. The remaining 38 patients (62.3 %, 95 % Cl 25.5, 49.9) were considered PSA non-responders, and 14 of them (14/61, 23.0 %) showed stable disease. Altogether, 37 patients (60.6 %) responded or had stable PSA levels during the trial. The evolution of PSA level in these three categories of patients is presented in Fig. 5.1. In total, 26 patients (42.6 %) had a PSA decline of ≥ 50 %, and a further 12 patients (19.6 %) had a PSA reduction of < 50 % during the 6-month core trial at one measured time point. A PSA reduction of > 50 % was also observed in five patients with a baseline PSA doubling time of < 3 months.
Twelve patients received an imatinib dose increased from 400 to 800 mg as per protocol because of PSA progression, but this increase did not improve PSA response in any of the patients. PSA response occurred independent of the presence of distant metastases and the metastatic site.
Seventy-seven percent of the patients required some type of dose modification or a temporary interruption of the study drug because of a non-hematologic or hematologic toxicity grade 2 or because of adverse events. Nevertheless, over 60 % of the study population either showed a PSA response or maintained a stable disease course.
Neither median time to PSA response nor overall or progression-free survival could be achieved.
Time to doubling of the PSA level at baseline (ITT population)
For correctly estimating the PSA response rate, it should be mentioned that 77 % of the patients had a PSA doubling time of < 3 months.
Adverse events and serious adverse events
Each of the 65 patients experienced one or more adverse event (Table 5.2). The majority of adverse events (97.1 %; n = 919) did not result in a permanent discontinuation of the study medication. Out of the 947 adverse events reported, 545 (57.6 %) were suspected to be drug-related, 131 (13.8 %) led to dose adjustment or temporary interruption, 27 (2.9 %) led to permanent discontinuation, and 381 (40.2 %) required concomitant medication or non-drug therapy.
The most frequently reported drug-related adverse events (> 20 % of the patients) were peripheral edema (56.9 %), nausea (38.5 %), edema (36.9 %), fatigue (35.4 %), dyspnea (35.4 %), anemia (33.8 %), leukopenia (29.2 %), diarrhea (23.1 %), vomiting (23.1 %), facial edema (23.1 %), muscle spasms (21.5 %), and increased weight (21.5 %). In total, 98 serious adverse events were reported in 27 patients (41.5 %); 32 of these events that occurred in 14 patients were drug-related and led to permanent discontinuation of the study drug in five patients. The most frequent drug-related serious adverse events (> 2 % of the patients) were general disorders and administration site conditions (7.7 %), blood and lymphatic system disorders (6.2 %), infections and infestations (4.6 %), nervous system disorders (4.6 %), and gastrointestinal disorders (3.1 %) (Table 5.4 and 5.5).
Four patients (6.2 %) died during the core trial, either as a result of tumor progression [1], acute respiratory insufficiency because of progression of prostate cancer [1], acute respir atory distress syndrome because of pneumonia [1], or cardiac arrest and pulmonary arrest [1].
Quality of life (EORTC-30 questionnaire)
Quality of life assessment showed that social, emotional, and physical function scores remained stable throughout the core phase of the trial (Fig. 5.3).
Redirecting and Modulating Tumor-Immanent Normative Functions
Clinically, the trial shows the modulation and redirection of important normative functions maintained by castration-resistant prostate cancer.
Immunmodulation
Rapid tumor response and recovery from tumor-associated lupus erythematodes could be shown after metronomic low-dose chemotherapy in addition to combined transcriptional modulation with pioglitazone and dexamethasone. This therapy was followed by an objective response in liver metastases (Fig. 5.4).

The immunmodulatory activity of the schedule is underlined by the rapid control of paraneoplastic lupus erythematodes before the onset of objective tumor response
Marked reduction of technetium up-take after biomodulatory therapy
A marked reduction or disappearance of bone metastases in control bone scans could be observed at one center during 6 out of 16 examinations (according to protocol, routine diagnostic investigations did not include follow-up bone scans). Figure 5.5 shows the example of a patient who experienced a steep decrease in the PSA level (from 2137 to 0.73 ng/mL at month 12) accompanied by an impressive decrease in bone metastases. Two patients with extensive lymphatic metastases showed calcifications in the lymph node tissue and partial remission according to the RECIST criteria.

Steep PSA decrease was accompanied by the resolution of skeletal lesions visible from the missing technetium up-take in the bone scan. Strong antiosteoplastic activity is assumed on the background that pioglitazone may inhibit the maturation of mesenchymal cell to osteoblasts
Induction of a biological memory
In 3 patients, the study medication was discontinued after a PSA response of > 50 % due to hip or knee replacement (degenerative diseases). The PSA doubling time was up to 10-fold higher (12.5–15 months) compared to baseline (Fig. 5.6). All patients responded to retreatment. One patient who had been progressive during retreatment responded again to additional treatment with a gonadotropin-releasing hormone (GnRH) agonist.

The rapid base-line PSA doubling time of < 3 months was up to ten times prolonged after the discontinuation of the study medication due to surgeries. Retreatment again was efficacious
These results indicate that the biomodulatory therapy approach may induce a biological memory for tumor growth control, presumably based on epigenetic changes mediated by the preceding combined transcriptional modulation with pioglitazone plus dexamethasone (Fig. 5.7).

Combined transcriptional modulation is assumed to induce stable epigenetic alterations in a tumor that might be responsible for maintaining response
Are there different rationalizations for tumor-associated normative functions?
Biomodulatory therapies are useful to uncover different rationalization processes for tumor-immanent normative functions, because they simply implement non-normative boundary conditions in a tumor system to force the system to start communicative activities by modularly rearranging tumor-associated systems functions.
Sixty percent of the patients responded to biomodulatory therapy with disease stabilization or a > 50 % PSA response. However, 40 % of the patients did not respond, although the frequency of osteoblastic metastases in this group was the same (80 %). Therefore, normative notions in the latter patient population are differentially rationalized and not accessible by the administered combined modularized therapy approach. Figure 5.8 presents PSA changes by patient from baseline.

The combined modularized therapy approach may control the osteoplastic metastases in about 60 % of the patients. Although non-responders had the same percentage of bone involvement, therapy was inefficacious in about 40 % of non-responders. This inefficacy indicates that the osteoplastic process in prostate cancer is differently rationalized
Discussion: Top-Down Strategy
The results of this phase II trial suggest that the combination therapy with the oral biomodulatory active drugs imatinib, treosulfan, etoricoxib, pioglitazone, and dexamethasone induces PSA responses of ≥ 50 % in almost 40 % of patients when used as a first-line therapy for CRPC. This response rate is comparable with that achieved with standard chemotherapies, such as docetaxel (45 %) or mitoxantrone (32 %) [32–34] and presumably much higher than in ‘low-risk‛ patients receiving glucocorticoids only (7 % up to 67 %) [22, 23]. Phase II trials on abiraterone achieved PSA response rates between 36 to 67 % [2], again indicating that response is dependent on disease characteristics of included patients. Moreover, this encouraging finding was accompanied by a low rate of acute toxicity of the study regimen, as indicated by patient-reported outcomes (quality of life assessments). Early dose reductions as a response to increased toxicity levels allowed the continuation of the treatment regimen over an extended period. These findings increase the possibility that this biomodulatory strategy could achieve long-term tumor control with a very low tumor burden.
Previous phase II trials have shown that dexamethasone 2 mg daily or metronomic low-dose cyclophosphamide or combinations can achieve a PSA response (again defined as ≥ 50 % decrease in PSA from baseline) in more than 50 % of asymptomatic patients [26]. However, the novel regimen used in the current trial may induce an objective response even in patients with rapid PSA doubling times (a majority of patients in the present study population) and extensive tumor load (Fig. 5.5). In addition, a marked reduction or nearly complete disappearance of bone metastases was observed in bone scans at one center in 6 out of 16 patients (the patients were not systematically screened during the follow-up). These patients experienced long-term tumor control at a low tumor burden. Two out of 16 patients at one center showed tumor necrosis with saponification as indicated by lymph node calcification.
Our therapeutic schedule did not include any classic cytotoxic agent, thus drug-related toxicity levels of standard chemotherapy regimens could be avoided [32, 33]. Although all patients experienced at least one adverse event, drug-related toxicity was generally manageable after prompt dose modifications for events of grade 1 or 2 toxicity. These changes did not appear to markedly limit the efficacy of the regimen: Although 77 % of the patients required some type of dose modification or a temporary interruption of the study drug, over 60 % of the study population showed either a PSA response or maintained a stable disease course. In addition, quality of life was maintained throughout the trial.
The combined activity of individual compounds in this regimen and particularly the concerted effect of metronomic low-dose chemotherapy and other biomodulators has been proven previously [28]. Using a similar therapeutic strategy by combining etoricoxib, pioglitazone, dexamethasone, and metronomically administered capecitabine after first-line chemotherapy, a high PSA response rate was observed (41 %), which was superior to that of standard-dose capecitabine alone in historical controls (12 %) [30, 35]. In biomodulatory regimens, the activity of one single drug cannot be defined, because mono-activity is not a prerequisite for concerted activity. The combination, however, must facilitate non-normative boundary conditions to redirect tumor-promoting action norms. Monitoring biomodulatory activity requires serum analytics of the secretome derived from specific cellular compartments in the tumor and could provide novel functional signatures [36, 37]. Such an analysis could determine which components of the cocktail are redundant or essential and which have additive or synergistic effects. Moreover, this analysis may also provide clues for repurposing drugs and for establishing adaptive trial designs [38–41].
The central therapeutic problem of tumor heterogeneity, particularly in CRPC [42–44], may be addressed by targeting selected normative notions, including particularly the ‘hallmarks’ of cancer by a ‘top-down’ approach (Fig. 5.9). Such a novel therapy strategy aims at redirecting the communicative expression of tumor-promoting systems participators, pathways, communication lines, etc. by modulating their communicative ‘background’. Such an approach primarily necessitates a multi-track approach to facilitate concerted biomodulatory drug activity, aiding the inclusion of drugs with poor or no mono-activity in the respective tumor type.

Finally, either the top-down approach or the bottom-up approach has to redirect or modulate rationalizations of normative notions to attenuate tumor growth. The modes how the approaches achieve this aim are rather different: The traditional bottom-up approach tries to knock-down the function of assumed tumor-promoting pathways with single-track or combined single-track methods, irrespective of their communicative expression in the concert of additional tumor-relevant aberrations. The top-down approach aims at targeting a tumor’s normativity with a primarily multi-track approach by redirecting the communicative background of assumed tumor-promoting pathways
Particularly the combined transcriptional modulation opens up completely new therapeutic strategies, such as the implementation of a presumably epigenetically maintained biological memory. Additionally, biomodulatory therapies contribute to uncovering differently organized rationalizations for tumor-specific normative functions.
Promising clinical data indicate that combined modularized therapies that modulate tumor-associated angiogenesis, inflammation, and immune response in CRPC need to be explored further. In addition, biomodulatory therapies targeting tumor-immanent normative notions may also be effective for the large and expanding group of elderly and frail patients because of its favorable toxicity profile [45–47]. Finally, biomodulatory therapy schedules offer the important opportunity of combining tumor-specific medications with relatively mild mono-activity to achieve synergistic effects.
References
Osanto S, Van Poppel H (2012) Emerging novel therapies for advanced prostate cancer. Ther Adv Urol 4:3–12
Ryan CJ, Smith MR, de Bono JS et al (2013) COU-AA-302 Investigators. Abiraterone in metastatic prostate cancer without previous chemotherapy. N Engl J Med 368(2):138–48. doi: 10.1056/NEJMoa1209096. Epub 2012 Dec 10
Logothetis CJ, Basch E, Molina A et al (2012) Effect of abiraterone acetate and prednisone compared with placebo and prednisone on pain control and skeletal-related events in patients with metastatic castration-resistant prostate cancer: exploratory analysis of data from the COU-AA-301 randomised trial. Lancet Oncol 13(12):1210–1217. doi: 10.1016/S1470–2045(12)70473-4. Epub 2012 Nov 9
Reichle A, Vogt T (2008) Systems biology: a therapeutic target for tumor therapy. Cancer Microenviron 1:159–170
Reichle A, Hildebrandt GC (2009) Principles of modular tumor therapy. Cancer Microenviron 2(Suppl 1):227–237
Reichle A (2009) Tumor systems need to be rendered usable for a new action-theoretical abstraction: the starting point for novel therapeutic options. Curr Cancer Ther Rev 5:232–242
Mimeault M, Johansson SL, Batra SK (2012) Pathobiological implications of the expression of EGFR, pAkt, NF-Φ#186;B and MIC-1 in prostate cancer stem cells and their progenies. PLoS ONE 7:e31919
Azevedo A, Cunha V, Teixeira AL et al (2011) IL-6/IL-6R as a potential key signaling pathway in prostate cancer development. World J Clin Oncol 2:384–396
Jain G, Cronauer MV, Schrader M et al (2012) NF-κB signaling in prostate cancer: a promising therapeutic target? World J Urol 30:303–310
Huber ML, Haynes L, Parker C et al (2012) Interdisciplinary critique of sipuleucel-T as immunotherapy in castration-resistant prostate cancer. J Natl Cancer Inst 104:273–279
Kantoff PW, Higano CS, Shore ND et al (2010) Sipuleucel-T immunotherapy for castration-resistant prostate cancer. New Engl J Med 363:411–422
Tang S, Moore ML, Grayson JM et al (2012) Increased CD8 + T cell function following castration and immunization is countered by parallel expansion of regulatory T cells. Cancer Res 72:1975–1985
Scher HI, Halabi S, Tannock I et al (2008) Design and end points of clinical trials for patients with progressive prostate cancer and castrate levels of testosterone: recommendations of the Prostate Cancer Clinical Trials Working Group. J Clin Oncol 26:1148–1159
Ustach CV, Huang W, Conley-LaComb MK et al (2010) A novel signaling axis of matriptase/PDGF-D/ß-PDGFR in human prostate cancer. Cancer Res 70:9631–9640
Mathew P, Thall PF, Jones D et al (2004) Platelet-derived growth factor receptor inhibitor imatinib mesylate and docetaxel: a modular phase I trial in androgen-independent prostate cancer. J Clin Oncol 22:3323–3329
Meyer S, Vogt T, Landthaler M et al (2010) Cyclooxygenase 2 (COX2) and peroxisome proliferator-activated receptor gamma (PPARG) are stage-dependent prognostic markers of malignant melanoma. In: Reichle A (ed) From molecular to modular tumor therapy. Springer, Berlin, pp 433–465
Nakamura Y, Suzuki T, Sugawara A et al (2009) Peroxisome proliferator-activated receptor gamma in human prostate carcinoma. Pathol Int 59:288–293
Lyles BE, Akinyeke TO, Moss PE et al (2009) Thiazolidinediones regulate expression of cell cycle proteins in human prostate cancer cells via PPARgamma-dependent and PPARgamma independent pathways. Cell Cycle 8:268–277
Matsuyama M, Yoshimura R (2008) Peroxisome proliferator-activated receptor-gamma is a potent target for prevention and treatment in human prostate and testicular cancer. PPAR Res 2008:249849
Smith MR, Manola J, Kaufman DS et al (2004) Rosiglitazone versus placebo for men with prostate carcinoma and a rising serum prostate-specific antigen level after radical prostatectomy and/or radiation therapy. Cancer 101:1569–1574
Shockley KR, Lazarenko OP, Czernik PJ et al (2009) PPARgamma2 nuclear receptor controls multiple regulatory pathways of osteoblast differentiation from marrow mesenchymal stem cells. J Cell Biochem 106:232–246
Storlie JA, Buckner JC, Wiseman GA et al (1995) Prostate specific antigen levels and clinical response to low dose dexamethasone for hormone-refractory metastatic prostate carcinoma. Cancer 76:96–100
Nishimura K, Nonomura N, Yasunaga Y et al (2000) Low doses of oral dexamethasone for hormone-refractory prostate carcinoma. Cancer 89:2570–2576
Khor LY, Bae K, Pollack A et al (2007) COX-2 expression predicts prostate-cancer outcome: analysis of data from the RTOG 92-02 trial. Lancet Oncol 8:912–920
Meyer S, Vogt T, Landthaler M et al (2009) Cyclooxygenase 2 (COX2) and peroxisome proliferator-activated receptor gamma (PPARG) are stage-dependent prognostic markers of malignant melanoma. PPAR Res 2009:848645
Emmenegger U, Chow A, Bocci G (2010) The biomodulatory capacities of low-dose metronomic chemotherapy: complex modulation of the tumor microenvironment. In: Reichle A (ed) From molecular to modular tumor therapy. Springer, Berlin, pp 433–465
Feyerabend S, Feil G, Krug J et al (2007) Cytotoxic effects of treosulfan on prostate cancer cell lines. Anticancer Res 27(4B):2403–2408
Nelius T, Rinard K, Filleur S (2011) Oral/metronomic cyclophosphamide-based chemotherapy as option for patients with castration-refractory prostate cancer: review of the literature. Cancer Treat Rev 37:444–455
Glode LM, Barqawi A, Crighton F et al (2003) Metronomic therapy with cyclophosphamide and dexamethasone for prostate carcinoma. Cancer 98:1643–1648
Walter B, Rogenhofer S, Vogelhuber M (2010) Modular therapy approach in metastatic castration-refractory prostate cancer. World J Urol 28:745–750
Heidenreich A, Aus G, Bolla M et al (2008) EAU guidelines on prostate cancer. Eur Urol 53:68–80
Berthold DR, Pond GR, Soban F et al (2008) Docetaxel plus prednisone or mitoxantrone plus prednisone for advanced prostate cancer: updated survival in the TAX 327 study. J Clin Oncol 26:242–245
Tannock IF, de Wit R, Berry WR et al (2004) Docetaxel plus prednisone or mitoxantrone plus prednisone for advanced prostate cancer. N Engl J Med 351:1502–1512
Petrylak DP, Tangen CM, Hussain MH et al (2004) Docetaxel and estramustine compared with mitoxantrone and prednisone for advanced refractory prostate cancer. N Engl J Med 351:1513–1520
Morant R, Bernhard J, Dietrich D et al (2004) Capecitabine in hormone-resistant metastatic prostatic carcinoma—a phase II trial. Br J Cancer 90:1312–1317
Pitteri SJ, Kelly-Spratt KS, Gurley KE et al (2011) Tumor microenvironment-derived proteins dominate the plasma proteome response during breast cancer induction and progression. Cancer Res 71:5090–5100
Paulitschke V, Kunstfeld R, Gerner C et al (2010) Secretome proteomics, a novel tool for Biomarkers discovery and for guiding biomodulatory therapy approaches. In: Reichle A (ed) From molecular to modular tumor therapy. Springer, Berlin, pp 405–431
Bundscherer A, Hafner C (2010) Breathing new life into old drugs. Indication discovery by systems-directed therapy. In: Reichle A (ed) In from molecular to modular tumor therapy. Springer, Berlin
Oprea TI, Bauman JE, Bologa CG et al (2011) Drug repurposing from an academic perspective. Drug DiscovToday Ther Strateg 8(3–4):61–69
Berry DA (2011) Adaptive clinical trials in oncology. Nat Rev Clin Oncol 9:199–207
Reichle A, Hildebrandt GH (2010) The comparative uncovering of tumor systems biology by modularly targeting tumor-associated inflammation. In: Reichle A (ed) From molecular to modular tumor therapy. Springer, Berlin, pp 287–303
Ashida S, Orloff MS, Bebek G et al (2012) Integrated analysis reveals critical genomic regions in prostate tumor microenvironment associated with clinicopathologic phenotypes. Clin Cancer Res 18:1578–1587
Squire JA, Park PC, Yoshimoto M et al (2011) Prostate cancer as a model system for genetic diversity in tumors. Adv Cancer Res 112:183–216
Gu G, Brothman AR (2011) Cytogenomic aberrations associated with prostate cancer. Cancer Genet 204:57–67
Bellmunt J (2008) Chemotherapy for prostate cancer in senior adults: are we treating the elderly or the frail? Eur Urol 55:1310–1312
Walter LC, Covinsky KE (2001) Cancer screening in elderly patients: a framework for individualized decision making. JAMA 285:2750–2756
Koroukian SM, Murray P, Madigan E (2006) Comorbidity, disability, and geriatric syndromes in elderly cancer patients receiving home health care. J Clin Oncol 24:2304–2310
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2013 Springer Science+Business Media Dordrecht
About this chapter
Cite this chapter
Vogelhuber, M. et al. (2013). Redirecting and Modulating Rationalizations of Tumor-Immanent Normative Functions in Castration-Resistant Prostate Cancer. In: Reichle, A. (eds) Evolution-adjusted Tumor Pathophysiology:. Springer, Dordrecht. https://doi.org/10.1007/978-94-007-6866-6_5
Download citation
DOI: https://doi.org/10.1007/978-94-007-6866-6_5
Published:
Publisher Name: Springer, Dordrecht
Print ISBN: 978-94-007-6865-9
Online ISBN: 978-94-007-6866-6
eBook Packages: Biomedical and Life SciencesBiomedical and Life Sciences (R0)