
Abstract
When LDL is oxidized by a free radical generating system, both cholesterol and fatty acyl moieties within the LDL are modified. Oxidized low density lipoprotein (oxLDL) can induce alterations in the Ca2+ transients in isolated cardiomyocytes. It is unclear if oxidation of the LDL fatty acyl chains (in phospholipids, triglycerides and cholesteryl esters) or oxidation of the LDL unesterified cholesterol is more important in producing the oxLDL-induced alteration in cellular calcium transients. Therefore, we investigated the possible role of oxidized cholesterol and fatty acyl chain peroxidation in the effects of LDL on Ca2+ transients. Cholesterol oxidase (CO) treatment of LDL produced oxidized cholesterol plus H2O2. The H2O2 peroxidized the LDL fatty acyl chains, as indicated by an increased malondialdehyde (MDA) content. The cell systolic [Ca2+] was significantly increased after incubation with CO-treated LDL. Diastolic [Ca2+] was unchanged. MDA content in the CO-treated LDL correlated with the change in systolic [Ca2+] of treated cells. Catalase, a scavenger of H2O2, inhibited MDA formation in the CO-treated LDL and prevented the increment in systolic [Ca2+] in the treated cells. A similar stimulatory effect on the Ca2+ transient was observed if cells were treated with LDL after exposure to only H2O2 and not CO. Direct exposure of myocytes to H2O2 (without LDL) failed to produce a stimulatory effect on the calcium transient but caused an increment in cellular diastolic Ca2+. Exposure of myocytes to CO alone (without LDL) produced a significant increment in diastolic [Ca2+] and this effect was not prevented by catalase. These results suggest that fatty acid peroxidation in the LDL moiety is more important than oxidized cholesterol in the generation of ox-LDL-induced increases in Ca2+ transients in isolated cardiomyocytes. Further, oxidation of in situ cell membrane cholesterol will destroy cell integrity. Our data also underline the importance of adding extracellular lipid in any study of the effects of oxygen free radicals on cellular function. Under conditions of radiologic or chemically-induced generation of oxygen-derived free radicals, cardiac dysfunction and damage may be induced by this process.
Access provided by Autonomous University of Puebla. Download conference paper PDF
Similar content being viewed by others


Keywords
- High Performance Liquid Chromatography
- Calcium Transient
- Cholesterol Oxidase
- Fatty Acyl Chain
- Cholesterol Acyl Transferase
These keywords were added by machine and not by the authors. This process is experimental and the keywords may be updated as the learning algorithm improves.
1 Introduction
The generation of oxygen-derived free radicals is proposed to increase during hypoxia/reoxygenation and ischemia/reperfusion injuries to the heart [3, 4, 22]. Chemical, biological and radiological conditions can also induce damaging and even lethal levels of oxygen-derived free radicals. One of the targets of the free radicals is thought to be the cardiomyocyte itself. Free radicals increase the resting intracellular [Ca2+] and thereby contribute to cell damage and death [6, 20]. However, another important target of the free radicals is circulating lipids like LDL (low density lipoprotein). LDL can be extensively oxidized by free radicals [38]. Since LDL is in contact with cardiomyocytes in relative high concentrations [21], and free radicals present in the interstitial space may have been shown to oxidize LDL there [15, 40, 46], it is possible that oxidized LDL (oxLDL) may exert an effect of its own on the cardiomyocytes. Recently, we observed that oxLDL can significantly alter the Ca2+ transient in isolated cardiomyocytes [27]. The oxLDL greatly potentiated the effects of free radicals on their own. In view of the significance of free radical-induced damage to the heart [3, 4, 22], and the potential role of ox-LDL as a mediator in this action, it was important to investigate the mechanism whereby oxLDL exerts its effects on the cardiomyocyte Ca2+ transients.
The purpose of the present study was to investigate which part of the oxLDL particle is most important for producing the effects of oxLDL on the Ca2+ transient of the isolated cardiomyocyte. Three major parts of the LDL lipoprotein moiety (apoprotein, fatty acyl chain and cholesterol) can be oxidized [1, 42]. If the fatty acyl chain present in LDL phospholipids, cholesterol esters and triglycerides is oxidized extensively, a broad spectrum of shorter chain aldehydes (conjugated dienes, malondialdehyde and 4-hydroxynonenal) is generated [11, 17, 42]. The unesterified cholesterol in LDL can also be oxidized into several cholesterol oxide derivatives [1, 28, 29]. Currently, it is difficult to evaluate which lipid in the oxLDL moiety plays the most important role in modifying the Ca2+ transport characteristics [24]. We decided, therefore, to examine if oxidized cholesterol in LDL may be responsible for the effects of oxLDL on the cardiomyocyte Ca2+ levels. In the present investigation, cholesterol oxidase was employed to specifically oxidize the cholesterol in the LDL.
2 Materials and Methods
2.1 Materials
All chemicals were of standard reagent grade (Sigma Chemical Co., St. Louis, MO). Cholesterol oxidase (CO) (Pseudomonas fluorescens) and catalase (bovine liver) were obtained from Sigma Chemical Co. Other selected cholesterol derivatives which were used as standards for the high performance liquid chromatography (HPLC) analysis were purchased from Steraloids, Inc., Wilton, NH. Fura-2AM was purchased from Molecular Probes Inc., Junction City, Oregon. Collagenase was obtained from Worthington Biochemicals (Freehold, New Jersey). The cholesterol supplemented rabbit chow was purchased from ICN Biochemicals Inc. (Cleveland, OH). Lazaroid (U74500A) was kindly provided by The Upjohn Co.
2.2 Cardiomyocyte Isolation
Calcium tolerant, contractile, single cardiomyocytes were prepared according to a procedure which has been described in detail previously [26, 30]. In brief, the hearts from 2.5 kg male albino New Zealand rabbits were quickly excised, the ascending aorta cannulated, and the heart retrogradely perfused with a Ca2+-free then minimal Ca2+ containing solution supplemented with 1.3 mg/ml collagenase and 0.5 mg/ml hyaluronidase. The heart was then removed from the isolation apparatus after ~30 min perfusion and the cells gently minced free in a petri dish. Myocytes were harvested at 1 xg and viable cardiomyocytes adhered to coverslips which had been previously coated for ~20 min with a 0.2 mg/ml laminin. More than 70 % of the myocytes were rod-like shaped, calcium-tolerant, free of membrane blebs, possessed clear sarcomere striation, did not spontaneously contract and excluded trypan blue. Myocytes were studies in a Kreb’s perfusion solution containing (in mM): NaCl 120; NaHCO3 25, KCl 4; KH2PO4 1.2; MgSO4 1.2; dextrose 5.5; CaCl2 1.8; (pH 7.4). All experiments were performed at a temperature of 37 °C.
2.3 Lipoprotein Isolation
LDL (density 1.019–1.063 g/ml) was prepared by sequential ultracentrifugation from the plasma of male albino New Zealand rabbits fed a 1 % cholesterol-supplemented diet [34]. Dithiobisnitrobenzoic acid (1.5 mM), phenylmethylsulphonyl fluoride (2 mM), thimerosal (0.08 mg/ml) were added to the plasma after separation of the blood cells to inhibit lecithin:cholesterol acyl transferase, proteolysis and bactericides, respectively [25]. Ascorbic acid (50 μM) and EDTA (1 mM) were added throughout the isolation to prevent oxidation of LDL [25, 30]. The LDL fraction was extensively dialyzed against 0.15 M NaCl, 1 mM EDTA (pH 7.4) and stored at 4 °C. The protein content of LDL was determined by Lowry’s method [32], and cholesterol (free and esterified) was measured enzymatically as described [37]. The absence of LDL oxidization during isolation or prior to their use in experiments was estimated by an absence of malondialdehyde (MDA) reactive products [13, 27, 28] and oxidized cholesterol [28, 31, 41].
2.4 Preparation and Measurement of Lipid Oxidation
Lipoprotein oxidation was induced by incubation with CO ± catalase at 37 °C for 60 min. CO and catalase concentrations used were 1 mg/ml each throughout the experiments or as otherwise indicated. An aliquot of oxidized LDL was then applied to the medium bathing the experimental myocyte (tenfold dilution). Lipid peroxidation of LDL was assessed by measuring the MDA content of LDL using the thiobarbituric acid reactive substances (TBARS) method [13, 28]. Freshly diluted malondialdehyde bis (dimethyl acetal 1,1,3,3-tetra-methoxypropane) was used as a reference standard. TBARS were expressed as MDA equivalents. Oxidized cholesterol species in myocytes treated with oxLDL were identified and quantified using HPLC. A modification of the technique of Sevanian and McLeod [41] was employed, as described in detail elsewhere (18, 24, 28). Briefly, myocytes were treated with various agents in M199 solution for 60 min at 37 °C followed by washing the cells three times. The treated cells were then homogenized in a solution containing 0.5 % Triton X-100, 3 mM sodium cholate and 0.1 M Tris (pH 6.6), transferred to 5 ml of 2:1 chloroform:methanol, and extracted overnight at 4 °C in the dark. After the samples were lipid extracted as described in detail elsewhere [24, 28], the lipids were then suspended in 20 μl of methylene chloride of which 10 μl was used for HPLC analysis. The HPLC used included a Waters 501 HPLC pump, 116 solvent delivery system, Waters 484 tunable absorbance detector and a Waters Nova-Pak Silica column (3.9 × 150 mm). Flow rate was kept at 2.0 ml/min and the mobile phase was 99:1 hexane:isopropanol. UV detection of the peaks was carried out at an absorbance of 208 nm. The Waters Baseline 810 chromatography workstation was employed in operating the process.
2.5 Measurement of Cellular Ca2+ Transients
The fluorescent Ca2+ indicator dye fura-2 was used to measure intracellular Ca2+ transients [10, 18]. Briefly, myocytes were loaded with 2 μM fura-2AM (acetoxymethylester) for 15 min at 22 °C, then were gently washed twice with Kreb’s solution. These cells were then studied in a chamber on the stage of a Nikon Diaphot epifluorescent microscope which was attached to a SPEX Fluorolog spectrofluorometer (SPEX Industries, Edison, NJ) [10, 27, 30]. Cardiomyocytes were sequentially excited at 340 and 380 nm wavelength light and the emitted fluorescent images of the myocyte at 505 nm were recorded and quantitated with photomultiplier tubes coupled to a computer. Calibration of the monocytes’ fluorescent ratio was carried out with the in situ method of Grynkiewicz et al. [14] using 20 μM 4-bromo-A23187 to obtain maximal fluorescence and 10 mM EGTA to determine the minimum fluorescence [6, 14].
For each experiment, a single cardiomyocyte was selected under the phase contrast bright field microscopy and then stimulated by passing currents via two platinum electrodes spaced ~8 mm apart. The cell contracted in response to this field stimulation which was set at a frequency of 0.5 Hz with biphasic pulses of 3 ms in duration. Stimulation voltage across the electrodes as determined in air was 8–12 V.
2.6 Statistical Analysis
All results are expressed as mean ± SEM. Data was analyzed statistically with one-way analysis of variance followed by a Duncan’s post hoc test [25]. The level of significance was arbitrarily set at P < 0.05.
3 Results
LDL was pre-incubated with 0.1 mg/ml CO in the absence of catalase. The incubation of LDL with CO alone will result in an oxidation of LDL cholesterol and the generation of H2O2. An aliquot was removed and placed in a solution bathing the cardiomyocytes and the intracellular calcium transient of isolated cardiomyocytes was measured. In the control cells, the Ca2+ transient is stable for more than 60 min of stimulation [30]. Fig. 7.1 shows representative results of calcium transients over time in cardiomyocytes incubated with CO treated LDL ± catalase. Recordings were paused after 25 s every 2 min in order to avoid photo bleaching the dye which could have occurred during long exposure times to light. This protocol was used throughout the experiments. A slow and steady increment in the Ca2+ transient was observed after oxLDL was incubated with the cardiomyocyte (Fig. 7.1a). A striking increment in peak systolic [Ca2+] during the transient was noticeable during the treatment whereas the diastolic Ca2+ level was unaltered. An inexcitability of treated cells was consistently observed after ~16 min treatment with oxLDL (Fig. 7.1a). When the above treatment was applied to cells but in the presence of 0.1 mg/ml catalase to in-activate the H2O2 (Fig. 7.1b), the amplitude of the Ca2+ transient was not significantly increased. A number of experiments were carried out to investigate the effects of varying concentrations of oxLDL ± catalase on the Ca2+ transients in cardiomyocytes (Table 7.1). The systolic level of the Ca2+ transients was not significantly increased until the oxLDL concentration reached 50 μg cholesterol/ml oxLDL. This effect required at least 16 min before statistical significance was achieved. This effect was not observed when catalase was present during the treatment of oxLDL. The diastolic [Ca2+] was not significantly altered at any of the concentrations applied.

Representative recordings of calcium transients in cardiomyocytes treated with 0.1 mg cholesterol/ml LDL oxidized by 0.1 mg/ml cholesterol oxidase (CO) (a) or 0.1 mg cholesterol/ml LDL oxidized by 0.1 mg/ml CO in the presence of 0.1 mg/ml catalase (b). The recordings here are not continuous but for 25 s then stopped. At the second minute, another 25 s recording was resumed, followed by another 25 s recording at the fourth minute, etc. Note the increase in the size of calcium transient induced after the cell was exposed to 0.1 mg/ml oxLDL treatment (a) and the relative stability in the calcium transient recording in the cell treated with 0.1 mg/ml oxLDL but in the presence of 0.1 mg/ml catalase (b)
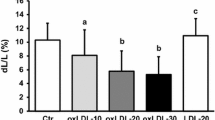
To understand the mechanism of action of oxLDL on the Ca2+ transient of treated cardiomyocytes, the association of lipid peroxidation within the LDL to the change in the intracellular Ca2+ transient was investigated. MDA products within the LDL were determined as an index of lipid peroxidation. A good correlation between the oxLDL MDA content and the percentage increase in systolic Ca2+ transient was observed in Fig. 7.2.

The effects of varying the oxLDL concentration on the cellular calcium transient and the LDL MDA content. Panel a shows the MDA production as a function of the oxLDL concentration. *P < 0.05 vs. MDA value at 10 μg/ml LDL. Panel b shows the percentage change in the systolic calcium transient vs. oxLDL concentration. *P < 0.05 vs. control untreated LDL. Values represent the mean ± S.E.M. from 4 to 6 experiments using different cells in both panels. Panel c presents the correlation between the MDA content of oxLDL and the percentage change of systolic calcium transients in cardiomyocytes treated with oxLDL
The efficacy of antioxidants in preventing the effects of cholesterol oxidase on LDL was compared. Catalase I in a ratio of 1:1 (w:w) to cholesterol oxidase completely inhibited MDA formation in the oxLDL (Fig. 7.3a). Lazaroid, a novel antioxidant, and vitamin E also prevented the production of MDA in the oxLDL but less efficiently compared to catalase (Fig. 7.3b).

The effects of catalase and other antioxidants on MDA production in oxLDL. Panel a presents the effect of catalase n the MDA production. Panel b shows influence of vitamin E and lazaroid on the MDA production. Values are the mean ± S.E.M. from 4 to 6 different experiments. If standard error bars are not present, then the symbol size was greater than the standard error of the mean
Cholesterol oxidase (CO) itself may have a strong influence on the cardiomyocyte Ca2+ transient. Therefore, in order to exclude the possibility that CO itself may be inducing a direct effect rather than the oxLDL, the effect on the Ca2+ transient of varying the concentration of CO ± catalase was examined in the absence of LDL (Fig. 7.4, n = 4–6). Figure 7.4 shows representative calcium transients in the cardiomyocytes after treatment with 1 mg/ml cholesterol oxidase (CO) (A), 1.5 mg/ml CO (B), 2 mg/ml CO (C), 0.5 mg/ml catalase (D) and 2 mg/ml CO + 0.5 mg/ml catalase (E). Recordings were only for 25 s, then stopped and the data saved before reinitiating the recording again for 25 s two minutes later. The CO was added at the time point indicated by the arrow. Note the stability in the calcium transient recorded from cells treated with 1 mg/ml CO (A) and the striking elevation in the diastolic component of the calcium transient induced by 1.5 and 2 mg/ml CO treatment (B and C). Note the steadiness of Ca2+ transient in the cells treated with 0.5 mg/ml catalase (D) and the complete loss of excitability in the cells treated with 2 mg/ml CO + 0.5 mg/ml catalase (E). When 1 mg/ml CO was applied to cardiomyocytes, no noticeable alteration in the myocyte Ca2+ transient was observed except an inexcitability appeared at 18 min (Fig. 7.4a). However, when the CO concentration was increased to 1.5 mg/ml, a striking increment in the diastolic component of the Ca2+ transient of treated myocytes was observed (Fig. 7.4b). An immediate increment in the diastolic component of the Ca2+ transient appeared when the CO concentration applied to the cardiomyocyte was increased to 2 mg/ml (Fig. 7.4c). The possible protective role of catalase against this effect produced by CO was also examined. The Ca2+ transient of cardiomyocytes remained stable after 0.5 mg/ml catalase was incubated with cardiomyocytes for 20 min (Fig. 7.4d). However, catalase at this concentration failed to protect against the effects of 2 mg/ml CO on the cell Ca2+ transient (Fig. 7.4e).

Representative recordings of calcium transients in the cardiomyocytes
HPLC was used to determine if CO was indeed oxidizing cell membrane cholesterol (Fig. 7.5). Cholesterol is a major component of the cell membrane (Fig. 7.5b). One oxidized cholesterol species, 20 α-OH, was also detectable in the control cardiomyocyte. This may be due to the presence of some necrotic cells in the preparation. Our cell isolation yield is about 70–80 % rod shaped, live, viable cells and 20–30 % rounded, necrotic cells (Fig. 7.5b). The most striking change in membrane cholesterol after CO treatment was the appearance of 4-cholesten-3-one (Fig. 7.5c, d). 4-cholesten-3-one became very prominent when the CO concentration was increased to 2 mg/ml and cholesterol disappeared (Fig. 7.5d).

Representative HPLC recordings of cholesterol species in the cardiomyocytes ± cholesterol oxidase treatment. (a) Standard cholesterol and oxidized cholesterol species, peak 1:4-cholesten-e-one; peak 2: cholesterol; peak 3: 20 α-OH cholesterol; (b) Control cardiomyocytes. (c) Cardiomyocytes were incubated with 1 mg/ml CO for 60 min at 37 °C; (d) Cardiomyocytes were incubated with 2 mg/ml CO for 60 min at 37 °C. Catalase was present at ratio of 1:1 (mg/ml) with CO in (c) and (d)
The by-product of cholesterol oxidation by cholesterol oxidase is hydrogen peroxide [43]. The possibility exists, therefore, that the effects on the cardiomyocyte Ca2+ transient produced by oxLDL may be due to the presence of H2O2 rather than oxLDL itself. Therefore, the effect of varying the H2O2 concentration on the Ca2+ transient of cardiomyocytes was investigated (Fig. 7.6). A significant increment in the diastolic Ca2+ concentration of treated cardiomyocytes was observed. The greater the [H2O2] that was applied to the cell, the faster the diastolic [Ca2+] increased (Fig. 7.6a–c). 10 mM H2O2 treatment produced a rapid (4 ± 1 min, n = 4) increment in the diastolic [Ca2+] of treated cardiomyocytes (Fig. 7.6a). 1 mM and 0.1 mM H2O2 also produced an increment in diastolic [Ca2+] in treated cardiomyocytes but it required a longer time to develop (10 ± 2 and 28 ± 2 min, respectively, n = 4–6) (Fig. 7.6b, c). However, the effects of H2O2 on the cell Ca2+ transient were very different if LDL was present. If LDL was preincubated with 0.1 mM H2O2 and then this oxLDL was incubated with cardiomyocytes, an increment (54.4 ± 4 %) of the systolic Ca2+ transient of cardiomyocytes was observed (Fig. 7.6d) (n = 4).

Representative recordings of calcium transients in myocytes after exposure to 10 mM H2O2 (a), 1 mM H2O2 (b), 0.1 mM H2O2 (c) or 0.1 mg/ml oxLDL oxidized by 0.1 mM H2O2 (d). Note the difference in the time to a change in diastolic [Ca2+] after addition of various concentrations of H2O2 (a–c) and the increment in the calcium transient after cells were treated with 0.1 mg/ml LDL oxidized by 0.1 mM H2O2 (d)
The time to contracture of cardiomyocytes after treatment with varying concentrations of H2O2 was also measured. The cells first lost excitability and then suddenly shortened to a rounded state indicative of contracture. A very rapid contracture (2.4 ± 0.3 min) of cardiomyocytes was produced by 20 mM H2O2 treatment (Fig. 7.7). When the concentration of H2O2 was decreased to 0.1 mM, a much longer time was required for cardiomyocytes to develop a contracture (28 ± 2 min).

Average time to contracture in myocytes exposed to varying H2O2 treatments. Values represent mean ± S.E.M. of 4–6 separate cell measurements
4 Discussion
The treatment of LDL by CO alone will oxidize LDL cholesterol and generate H2O2, which in turn can oxidize lipids in the LDL moiety [29, 43]. By including catalase in the incubation of LDL with CO, we can negate the effects of H2O2 and separately define the roles of cholesterol oxidation and fatty acyl chain peroxidation in the effects of oxLDL on Ca2+ transients. Several lines of evidence suggest that it is fatty acyl chain peroxidation rather than oxidized cholesterol in the LDL moiety which plays the primary role in the oxLDL-induced alteration of Ca2+ transients. First, a good correlation was observed between the MDA content in the oxLDL and the in-crease of systolic [Ca2+] in the treated cells. MDA is an indicator of lipid peroxidation [2, 19]. Secondly, catalase effectively protected LDL from lipid peroxidation and also protected against the change in Ca2+ transients in the treated cells. This would further support the conclusion that an interaction of the lipid peroxidation products in the oxLDL with cardiomyocytes may play an important role in modifying the Ca2+ transient. The protective effect of catalase against the MDA production in the oxLDL was more efficient than that of lazaroid and vitamin E. This would suggest that LDL peroxidation was primarily induced by H2O2 since catalase is a more efficient chelator of H2O2 [9, 39]. Lazaroid and vitamin E are good general free radical scavengers [8, 12, 35, 36, 45]. The peroxidation of LDL lipids by H2O2 may also have been potentiated by presence of μM Fe2+. Lazaroid has some metal chelating antioxidant properties [5] and its ability to inhibit MDA formation would give an indication that Fe2+ may have had a small contributory role in the H2O2 effect. Third, H2O2 treatment of LDL induced the same increase in systolic [Ca2+] in the cell that CO treatment of LDL (− catalase) did (Fig. 7.5d). Together, these data strongly suggest that H2O2 induced fatty acyl chain peroxidation in the LDL and it was these products which caused the change in systolic Ca2+ levels. Conversely, when LDL cholesterol was selectively oxidized by CO in the presence of catalase, no change in systolic [Ca2+] was observed. This clearly rules out oxidized LDL cholesterol as a mechanistic factor.
The effects of CO treated LDL on the cell [Ca2+] were very different than the effects of CO or H2O2 in the absence of LDL. Exposure of cells to CO without LDL produced a loss of excitability, an increase in diastolic [Ca2+] and eventually cell contracture. Systolic [Ca2+] was not increased as was the case when cells were exposed to oxLDL. It is very likely that oxidation of cell membrane cholesterol by CO produced nonspecific membrane damage resulting in a leakage of Ca2+ into the cell. HPLC data showed the generation of 4-cholesten-3-one in the membrane with a corresponding decrement of membrane cholesterol after the cardiomyocytes were treated with CO. In isolated cardiac sarcolemmal membranes, oxidation of membrane cholesterol resulted in significant changes in the Ca2+ flux and an increase in passive Ca2+ permeability characteristics [24]. Catalase, the specific chelator of H2O2, did not provide any protection against the effects of CO on cell contracture.
At higher concentrations, H2O2 also has its own effect on the intracellular diastolic Ca2+ level and can cause cardiomyocyte contracture. Our results agree with other studies that this effect of H2O2 is time and concentration dependent [16, 20]. There are several mechanisms for the increase in the diastolic [Ca2+] caused by H2O2. These include: (1) an inhibition of sarcolemmal Na+-K+ ATPase, resulting in intracellular Ca2+ overload via Na+-Ca2+ exchange [23]; (2) nonspecific membrane damage caused by sarcolemmal lipid peroxidation which renders the sarcolemma leaky to Ca2+ [44]; (3) H2O2 might depress the sarcoplasmic reticulum Ca2+ pump function which may lead to Ca2+ overload in the treated cardiomyocytes; (4) accelerated calcium influx through voltage gated calcium channels [20, 27].
The findings of the current study have significant pathological implications for the heart. Cardiac dysfunction and damage produced by oxygen derived free radicals may be important in ischemia/reperfusion or hypoxia/reoxygenation conditions [7, 33]. Chemical, biological or radiological challenges from the environment due to pollution, accidents or warfare may also increase the generation of oxygen-derived free radicals in the body and ultimately lead to the cardiac dysfunction and damage shown in the present work. Previous work has demonstrated that LDL can potentiate the effects on Ca2+ transients of oxygen derived free radicals on their own [27]. Lipid peroxidation is thought to play a critical role in in vivo situations where oxygen radical mediated tissue damage is important [2, 17, 42]. Our study suggests the fatty acyl groups found in LDL phospholipids, triglycerides and cholesteryl esters are the most important component in oxLDL for stimulating the Ca2+ transient of isolated cardiomyocytes. Oxidation of LDL free cholesterol does not account for the effect on the Ca2+ transient produced by oxLDL. Protection against LDL peroxidation by antioxidants like lazaroid, vitamin E and especially catalase may have important clinical applications. Clearly, in view of the differences we observed in the effects of H2O2 on cell function in the absence or presence of LDL, the present data demonstrate the importance of studying free radical effects in a medium which contains circulating lipids. These data provide important mechanistic information to help explain how damage to the heart can be induced when oxygen-derived free radicals are generated under conditions of excessive exposure to chemical, biological and radiological compounds. The data also demonstrate the importance of using antioxidant agents to prevent this damage.
References
Aviram M (1993) Modified forms of low density lipoprotein and atherosclerosis. Atherosclerosis 98:1–9
Bird RP, Draper HH (1984) Comparative studies on different methods of malondialdehyde determination. Methods Enzymol 105:299–305
Bolli R (1988) Oxygen-derived free radicals and postischemic myocardial dysfunction (“stunned myocardia”). JACC 12:239–249
Bolli R, Jeroudi MO, Patel BS et al (1989) Direct evidence that oxygen-derived free radicals contribute to postischemic myocardial dysfunction in the in-tact dog. Proc Natl Acad Sci USA 86:4695–4699
Braughler JM, Pregenzer JF, Chase RL et al (1987) Novel 21-amino steroids as potent inhibitors of iron-dependent lipid peroxidation. J Biol Chem 262:10438–10440
Burton KP, Morris AC, Massey KD et al (1990) Free radicals alter ionic calcium levels and membrane phospholipids in cultured rat ventricular myocytes. J Mol Cell Cardiol 22:1035–1047
Burton KP (1988) Evidence of direct toxic effects of free radicals on the myocardium. Free Rad Biol Med 4:15–24
Carrea FP, Lesnefsky EJ, Kaiser DG et al (1992) The lazaroid U74006F, a 21-aminosteroid inhibitor of lipid peroxidation, attenuates myocardial injury from ischemia reperfusion. J Cardiovasc Pharmacol 20:230–235
Chance B, Sies H, Boveris A (1979) Hydroperoxide metabolism in mammalian organs. Physiol Rev 59:527–605
Cheung JY, Tillotson DL, Yelamarty RV (1989) Cytosolic free calcium concentration in individual cardiac myocytes in primary culture. Am J Physiol 256:C1120–C1130
Esterbauer H, Jurgens G, Quehenberger O et al (1987) Autoxidation of human low density lipoprotein: loss of polyunsaturated fatty acids, vitamin E, and generation of aldehydes. J Lipid Res 28:495–509
Fisher M, Levine PH, Doyle EM et al (1991) A 21-aminosteroid inhibits oxidation of human low density lipoprotein by human monocytes and copper. Atherosclerosis 90:197–202
Fogelman AM, Shechter I, Seager J et al (1980) Malondialdehyde alteration of low density lipoproteins leads to cholesterol ester accumulation in human monocytes-macrophages. Proc Natl Acad Sci USA 77:2214–2218
Grynkiewicz G, Poenie M, Tsien RY (1985) A new generation of Ca2+ indicators with greatly improved fluorescent properties. J Biol Chem 260:3440–3450
Haberland ME, Fong D, Cheng L (1988) Malondialdehyde-altered protein occurs in atheroma of Watanabe heratable hyperlipidimic rabbit. Science 241:215–218
Hayashi H, Miyata H, Watannabe H et al (1989) Effects of hydrogen peroxide on action potentials and intracellular Ca2+ concentration of guinea pig heart. Cardiovasc Res 23:767–773
Heinecke JW, Rosen H, Chait A (1984) Iron and copper promote modification of low density lipoprotein by human arterial smooth muscle cells in culture. J Clin Invest 74:1890–1894
Hohl CM, Li Q (1991) Compartmentation of cAMP in adult canine ventricular myocytes relation to single-cell free Ca2+ transients. Circ Res 60:1369–1379
Janero DR (1990) Malondialdehyde and thiobarbituric acid-reactivity as diagnostic indices of lipid peroxidation and peroxidative tissue injury. Free Rad Biol Med 9:515–540
Josephson RA, Silverman HS, Lakatta EG et al (1991) Study of mechanism of hydrogen peroxide and hydroxyl free radical-induced cellular injury and calcium overload in cardiac myocytes. J Biol Chem 266:2354–2361
Julien P, Downer E, Angel A 1993(1981) Lipoprotein composition and transport in the pig and dog cardiac lymphatic system. Circ Res 49: 248–254
Khalid MA, Ashraf M (1993) Direct detection of endoge-nous hydroxyl radical production in cultured adult cardiomyocytes during anoxia and reoxygenation. Circ Res 72:725–736
Kramer JH, Tong Mak I, Weglicki WB (1984) Differential sensitivity of canine cardiac sarcolemmal and microsomal enzymes to inhibition by free radical-induced lipid peroxidation. Circ Res 55:120–124
Kutryk MJB, Maddaford TG, Ramjiawan B et al (1991) Oxidation of membrane cholesterol alters active and passive transsarcolemmal calcium movement. Circ Res 68:8–26
Kutryk MJB, Pierce GN (1991) Effects of low-density lipoprotein on calcium ion movements in cultured vascular smooth muscle cells. Coronary Artery Dis 2:1093–1101
Langer GA, Frank JS, Orner FB (1987) Calcium exchange, structure, and function in cultured adult myocardial cells. Am J Physiol 252:H214–H324
Liu KZ, Massaeli H, Pierce GN (1993) The action of oxidized low density lipoprotein on calcium transients in isolated rabbit myocytes. J Biol Chem 268:4145–4151
Liu KZ, Cuddy TE, Pierce GN (1992) Oxidative status of lipoproteins in coronary disease patients. Am Heart J 123:285–290
Liu KZ, Ramjiawan B, Kutryk MJB et al (1991) Effects of oxidative modification of cholesterol in isolated low density lipoproteins on cultured smooth muscle cells. Mol Cell Biochem 108:49–56
Liu KZ, Pierce GN (1993) The effect of low density lipoprotein on calcium transients in isolated rabbit cardiomyocytes. J Biol Chem 268:3767–3775
Liu KZ, Maddaford TG, Ramjiawan B et al (1992) Effects of cholesterol oxidase on cultured vascular smooth muscle cells. Mol Cell Biochem 108:39–48
Lowry OH, Rosebrough NJ, Farr AL, Randall AJ (1951) Protein measurement with folin phenol reagent. J Biol Chem 193:265–275
McCord JM (1985) Oxygen-derived free radicals in postischemic tissue injury. New Engl J Med 312:159–163
Mills GL, Lane PA, Weech PK (1984) A guidebook to lipoprotein technique. Elsevier Science Publisher BV, Dordrecht
Morel DW, DiCorleto PE, Chisolm GM (1984) Endothelial and smooth muscle cells alter low density lipoprotein in vitro by free radical oxidation. Arterioslcerosis 4:357–364
Negre-Salvayre A, Alomar Y, Troly M et al (1991) Ultraviolet-treated lipoproteins as a model for the study of the bio-logical effects of lipid peroxidates on cultured cells. III The protective effect of antioxidants (probucol, Catechin, and vitamin E) against the cytotoxicity of oxidized LDL occurs in two different ways. Biochem Biophys Acta 1096:291–300
Omodea SF, Marchesini S, Fishman PH et al (1984) A sensitive enzymatic assay for determination of cholesterol in lipid extracts. Anal Biochem 142:347–350
Parthasarathy S, Steinberg D, Witztum JL (1992) The role of oxidized low density lipoprotein in the pathogenesis of atherosclerosis. Annu Rev Med 43:219–225
Roos D, Weening RS, Wyss SR et al (1980) Interaction between human neutrophils by endogenous catalase: studies with cell from catalase-deficient individuals. J Clin Invest 65:1515–1522
Rosenfeld ME, Palinski W, Ylä-Herttuala S et al (1990) Protein B in atherosclerotic lesions of varying severity from WHHL rabbits. Arteriosclerosis 10:336–349
Sevanian A, McLeod LL (1987) Cholesterol autooxidation in phospholipid membrane bilayers. Lipid 22:627–636
Steinberg D, Parthasarathy S, Carew TE et al (1989) Beyond cholesterol modification of low density lipoprotein that increase atherogenesis. N Engl J Med 320:915–924
Thurnhofer H, Gains N, Mutsch B et al (1986) Cholesterol oxidase as a structural probe of biological membrane: its application to brush-border membrane. Biochem Biophys Acta 856:174–181
Tones MA, Poole-Wilson PA (1985) α-Adrenoceptor stimulation, lysophosphoglycerides, and lipid peroxidation in reoxygenation induced calcium uptake in rabbit myocardium. Cardiovasc Res 19:228–236
Van Hinsbergh VW, Scheffer M, Havekes L et al (1986) Role of endothelial cells and their products in the modification of low density lipoproteins. Biochem Biophys Acta 878:49–64
Ylä-Herttuala S, Palinski W, Rosenfeld ME et al (1989) Evidence for the presence of oxidatively modified low density lipoprotein in atherosclerotic lesions of rabbit and man. J Clin Invest 84:1086–1095
Acknowledgements
This work was supported by grants from the Canadian Institutes of Health Research and the Heart and Stroke Foundation of Manitoba. K.Z. Liu was a Trainee of the Manitoba Health Research Council. The assistance of Mr. Charles Labun, previously of the UpJohn Co. of Canada, is gratefully acknowledged.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2013 Springer Science+Business Media Dordrecht
About this paper
Cite this paper
Liu, Kz., Massaeli, H., Ramjiawan, B., Pierce, G.N. (2013). Oxidation of Selected Lipids in Low Density Lipoprotein: Effects on Calcium Transients in Isolated Rabbit Cardiomyocytes. In: Pierce, G., Mizin, V., Omelchenko, A. (eds) Advanced Bioactive Compounds Countering the Effects of Radiological, Chemical and Biological Agents. NATO Science for Peace and Security Series A: Chemistry and Biology. Springer, Dordrecht. https://doi.org/10.1007/978-94-007-6513-9_7
Download citation
DOI: https://doi.org/10.1007/978-94-007-6513-9_7
Published:
Publisher Name: Springer, Dordrecht
Print ISBN: 978-94-007-6512-2
Online ISBN: 978-94-007-6513-9
eBook Packages: Biomedical and Life SciencesBiomedical and Life Sciences (R0)