
Abstract
This chapter concerns the idea that Subjective Wellbeing (SWB) is managed by a system of psychological devices which have evolved for this purpose. It is proposed that this management is actually directed at the protection of Homeostatically Protected Mood, as the major component of SWB. We normally experience HPMood as a combination of contentment, happiness and arousal. A theoretical description of this construct is offered that can account for many of the commonly observed empirical characteristics of SWB data. It is further proposed that when homeostasis fails, due to the overwhelming nature of a negative challenge, people lose contact with HPMood and experience the domination of negative rather than positive affect. If this condition is chronic, people experience the clinical condition we call depression.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
1 Introduction
The purpose of this chapter is to draw together three threads that have been occupying our research over the past decade or so. The first of these is the composition and character of Subjective Wellbeing (SWB). The second is homeostatic process by which SWB is normally held within a narrow range of values. And the third is the nature of the relationship between SWB, homeostasis and depression. Each of these areas will now be addressed and the nature of their integration explained.
The single most important thing about Subjective Wellbeing is that it is positive. It is normal for people to feel good about themselves. This feature of SWB data is evident in the results of all publications that investigate the construct, and very explicitly in data gathered by the Australian Unity Wellbeing Index project (Cummins et al. 2003). This project measures the SWB of the Australian population several times each year. Each survey involves a telephone interview of 2,000 new respondents, nation wide. The project commenced in April 2001 and the accumulated data from the 21 surveys conducted to April 2009 provide much of the data for this chapter.
The scale used to measure and conceptualize SWB is the Personal Wellbeing Index (International Wellbeing Group 2006) which has a unique construction. It is designed as the first-level deconstruction of the highly abstract question ‘How satisfied are you with your life as a whole’. In order to achieve this design aim, each of the eight items has two important characteristics. The first lies in the semi-abstract nature of each question, such as ‘How satisfied are you with your relationships’. This format is deliberately non-specific. It allows the response that people give to be dominated by non-specific mood affect (the essence of SWB, see later), slightly flavored with cognitions attached to relationships. A more specific question, such as ‘How satisfied are you with your friends’, would elicit a more cognitively driven response.
The second characteristic of the eight items (domains) that comprise the Personal Wellbeing Index is that when they are regressed together against ‘Satisfaction with life as a whole’, each one contributes unique variance. These matters of theoretical construction are elaborated in the test manual.
Each item is rated on an end-defined 0–10 scale (Jones and Thurstone 1955) that is anchored by ‘completely dissatisfied’ and ‘completely satisfied’ (see Cummins and Gullone 2000 for an argument as to why this form of scale is superior to a Likert scale). The data are then averaged across the eight domains for each respondent and the result transformed onto a 0–100 scale. The cumulative results for the Australian population can be found in Cummins et al. (2009) and show the distribution of SWB in this population. The distribution of SWB is approximately normal within the positive (satisfied) sector of the response scale. The mean is 75 points and only 4.4 % of respondents score 50 or below. It is, thus, normal to feel positive about oneself.
1.1 Subjective Wellbeing Stability
The second intriguing feature of SWB is its stability. This can be demonstrated by two kinds of data. One uses the mean scores from population surveys and the other are data obtained from individuals.
To take the population data first, two reports (Cummins 1995, 1998) first demonstrated the extraordinary level of SWB stability, and therefore predictability, of population mean scores. The first of these chapters combined data from population surveys performed in various Western countries. It included highly diverse studies, each one having been conducted by different researchers, using different scales of measurement, at different times over the decades 1970–1990. When the results were transformed onto a 0–100 scale it was found that the mean of the 16 surveys was 75 points and their standard deviation was 2.5. Thus, using two standard deviations on either side of the mean to define a normal range, the SWB mean scores extend between 75 ± 5 or 70–80 points.
Of course, this estimate of the normal range is heavily contaminated with error variance resulting from the many methodological differences between the studies. Much greater stability is revealed by the 21 Australian Unity Wellbeing Index surveys. Over the nine-year period of these surveys (2001–2009) SWB varied over a total range of 3.1 points (73.2–76.3). Using these 21 values as data yields a mean of 74.93 points, a standard deviation of 0.75 and, therefore, a normative range of 73.43–76.43 points. In other words, the mean score of a random survey of people in Australia can be predicted, with 95 % certainty, to lie within a 3.0 % point range. There is no precedent in the literature for such extraordinary stability in measures of SWB.
The above analyses have been based on the use of sample means as data. When measures of SWB from individuals are used, the standard deviation is much larger, but is also very consistent. Using the data from the Australian population (Cummins et al. 2009) the mean is 74.93 points, the standard deviation is 12.36 and so the normal range is 50.21–99.64 points. It can be seen that this range rather neatly fits the positive sector of the distribution, however it is certainly too large to be regarded as the true normal range. This is because the calculation involves the 4.4 percent of people who fall below this range and, as will be argued later, this is considered to indicate the presence of pathology. So, a new range can be calculated omitting these values. This produces a mean of 76.45 and a standard deviation of 10.13. Using these new values, the normal range becomes 56.19–96.71.
A further slight adjustment can be made on the assumption that the true distribution is normal and that the 4.4 % of values that fall below 50 are overly representative of low values within the normative range. This idea is supported by the slightly higher frequency of scores above, compared to below the median of 75 points, over the range of 50–100 (see Cummins et al. 2009). So, if the above calculation is adjusted downward slightly it gives a normal range for SWB between 55 and 95 and a mean of 75 points. Of course, this is only an approximation and requires verification by other methodologies, but it is a reasonable basis for further theory-building.
2 How can these Data Patterns be Explained?
It is apparent from these results that SWB is exhibiting some determined characteristics as follows: (1) It is highly stable. (2) It is normally restricted to the positive half of the dissatisfied—satisfied continuum. (3) It shows a normal distribution consistent with what Psychologists refer to as an individual difference and is under strong genetic determination (e.g. Lykken and Tellegen 1996). That is, its distribution is consistent with SWB being an innate personal characteristic.
So what kind of a system might be responsible for such behavior? There is a substantial literature in which researchers describe the models they imagine responsible for SWB. The earliest of these were the ‘Physical and Spiritual Model’ (Liu 1975), the ‘Lewinian Lifespace Model’ (Campbell et al. 1976) and the ‘Two-Dimensional Conceptual Model’ (Andrews and Withey 1976) but all of these were mainly concerned with the composition of Quality of Life into its objective and subjective components. It took more than a decade for researchers to incorporate some of the psychometric characteristics described above into their models.
The first of these pioneers were two Australian researchers, Headey and Wearing (Headey et al 1984a, b; Headey and Wearing 1986, 1987, 1989). Using data from a panel study they observed that people appeared to have a ‘set-point’ for their SWB. That in the absence of significant life events, people tended to maintain a relatively steady level of SWB, and that if an event caused SWB to change then, over time, it tended to regain its previous level. They called this their ‘Dynamic Equilibrium Model’ and considered the management of SWB to be vested in a genetically-inbuilt psychological system, based in stable personality characteristics, which had the primary purpose of maintaining self-esteem. They characterized the positive sense of SWB as a ‘Sense of Relative Superiority’ because it had the consequence of making people feel that their subjective life experience is better than average for the population.
The second researchers to take up this challenge were Stones and Kozma (1991) who proposed their ‘Magical Model of Happiness’. Like Headey and Wearing, they depicted SWB as a self-correcting process that maintains stability around set-points that differ between individuals. They also regard SWB stability as a function of a dispositional system (Kozma et al. 2000 now referred to this as the ‘Propensity Model’). However, they also found that the propensity for stability could not be entirely explained through personality variables alone, and that the best predictor of future SWB was the level of past SWB.
All of these data are consistent with the idea, also proposed by other authors (Hanestad and Albrektsen 1992; Nieboer 1997; Ormel 1983; Ormel and Schaufeli 1991) that SWB is neurologically maintained in a state of dynamic equilibrium. However, these earlier models did not attempt to account for the nature of the relationship between SWB in dynamic equilibrium, and other demographic and psychological variables. This feature requires that theoretical attention be given to the processes of SWB management, which we call SWB homeostasis.
In 1998, Cummins first used the term ‘homeostasis’ to describe the basic mechanism underpinning SWB management. The term implies an analogy between the physiological management of internal body states, such as body temperature, and the management of SWB. While the homeostatic management of body temperature lies within the autonomic system, SWB is considered to be managed by dispositional, genetically pre-wired, neurological systems.
The term, ‘homeostasis’, is charged with meaning. Describing management in these terms makes very clear predictions concerning the relationship between SWB and other variables. The variable being managed, SWB, must conform to the standard performance requirements of homeostatic systems, and these include the three characteristics that have been previously listed. In addition to these, other characteristics should also be displayed if SWB management may be considered homeostatic. These include the following:
-
1.
There must be a threshold value which is being defended by the homeostatic processes. There must also be evidence that, as this value is approached, the system works harder than normal to retain control. Then, as the threshold value is exceeded, there must be evidence that homeostasis has failed and is no longer controlling the level of SWB.
-
2.
Following homeostatic defeat, over time the system should act to regain control. If this is successful, the level of SWB should return to a stable approximation of its set-point.
-
3.
The aim of homeostasis is to maintain the variable it is managing within a narrow range of values. Thus, SWB must evidence a ‘set-point-range’ which reflects the moment-to-moment range in which SWB will normally be found for each individual. The magnitude of this range may also be an individual difference, with some ranges being more tightly controlled than others.
-
4.
SWB should respond to variables that either enhance or challenge the operation of the homeostatic system. But the nature of the relationship with such variables should be consistent with the operation of a homeostatic system. The implications of these requirements are illustrated with the aid of Fig. 5.1.
Fig. 5.1 
Changing levels of SWB as homeostasis is challenged

This Figure comprises several parts as follows:
-
1.
The vertical axis shows the 0–100 scale of SWB and includes an illustrative set-point-range of 70–80 points.
-
2.
The lower horizontal axis shows the strength of a negative challenge to SWB, such as might be delivered by poverty or anxiety.
-
3.
The upper horizontal axis shows the dominant source of control. The source of control changes depending on whether the strength of the challenging agent is weak or strong.
-
4.
The curving ‘response line’ depicts the changes in SWB due to changes in the strength of challenge. The upper (80 point) and lower (70 point) margins of the set-point-range are identified as ‘thresholds’ and indicated by vertical arrows.
-
5.
An important limitation in this depiction is that the position of the response line will vary between people, determined by their set-point-range. Thus, for people who have a lower set-point, the response line will also be lower.
-
6.
A second limitation in this depiction is that it shows the theoretical outcome of the combined influences of supportive and challenging agents acting on the homeostatic system at any one time. Due to such multiple influences, any empirical investigation of the relationship between SWB and its sources of influence can only be expected to approximate the pattern that is shown
The predictions derived from Fig. 5.1 are as follows:
-
1.
Under conditions of zero threat, SWB will average to its set-point, which in this case is 75 points.
-
2.
As mild sources of threat are experienced, the level of SWB will vary within its set-point-range. Moreover, its position within the range will be a probability statement determined by the balance of good and bad momentary experience and the resilience of the homeostatic system. Thus, a sustained environment where good experience dominates, will allow SWB to average within the upper portion of the set-point-range. A sustained challenge will cause SWB to average within the lower portion of the set-point-range. However, the extent of such fluctuations is predicted to be quite modest. Since the magnitude of the set-point-range is calculated to be around 10–12 % points (Cummins et al. 2008, Sect. 3.8.1), the total movement of SWB due to such influences will not be more than a few percentage points on either side of the set-point. This phase is shown in Fig. 5.3a.
-
3.
As the strength of threat intensifies, the strength of the homeostatic defence also increases in an attempt to maintain stable levels of SWB. The result is phase (b) in which homeostasis manages to hold-the-line and prevents SWB from decreasing below its lower threshold value of 70 points. The evidence for this lower threshold to be located at about 70 points, on average, is presented in Cummins (2003). Importantly during this phase (b), the value of SWB is insensitive to changing levels of the challenging agent. That is, although the strength of the challenge is increasing, SWB will be held steady at the value of the lower threshold. This phase will continue as long as the homeostatic system is effective. However, at some higher strength of challenge, homeostasis will be overwhelmed.
-
4.
Once the strength of the challenging agent becomes too strong for homeostatic management, the value of SWB enters phase (c). In this phase the dominant source of control has shifted from homeostatic processes to the challenging agent. Now the value of SWB is sensitive to the strength of the challenging agent and, as the strength of the challenge increases, the value of SWB will sharply fall.
Within this theoretical and predictive background, two kinds of elaboration will now be presented. The first concerns the nature of the homeostatic system itself. The second examines empirical evidence for the proposition that the relationship between SWB and challenging agents conforms to the outcomes predicted by this homeostatic model.
3 The Mechanisms of Homeostasis
It is proposed that the mechanism of homeostasis comprises two kinds of buffers as External an Internal. The two major External buffers are wealth and relationships.
3.1 The External Buffers
There are serious misconceptions as to what money can and cannot do in relation to personal wellbeing. Most importantly, it cannot shift the set-point to create a perpetually happier person. Set-points for SWB are proposed to be under genetic control (Cummins et al. 2003; Lykken and Tellegen 1996), so in this sense money cannot buy happiness. No matter how rich someone is, their average level of SWB cannot be sustained higher than their set-point range. People adapt readily to luxurious living standards, so genetics trumps wealth after a certain level of income has been achieved.
The real power of wealth is to protect wellbeing through its capacity to be used as a flexible resource to assist homeostasis (Cummins 2000). It does this by allowing people to minimize the unwanted challenges they experience in their daily life. Wealthy people pay others to perform tasks they do not wish to do themselves. Poor people, who lack such financial resources, must fend for themselves to a much greater extent. As a consequence their level of SWB is far more at the mercy of their environment. Because of this influence, SWB rises with income, but only up to a certain level. In Australia SWB rises with gross household income up to about $91,000–$120,000, but at higher incomes no further systematic rise in SWB can be detected (Cummins et al. 2009).
This pattern of the relationship between SWB and wealth is much the same when comparisons are made between countries (e.g World Bank 1997). It is what the economists refer to as Decreasing Marginal Utility; that rising income has its strongest effect to raise wellbeing at low income levels.
This curvilinear, asymptotic relationship is a typical output from a management system that can be saturated. That is, supplying more of some relevant resource (money) may or may not cause an increase in output. The effect of the resource is dependent on the level of deprivation. Thus, for poor people or countries, all other things being equal, increased wealth will increase SWB. But this will continue only up to some ceiling value for SWB (about 80 points), which reflects full and unrestricted functioning of the system in relation to that resource.
These results are also convergent evidence that the power of money lies in its usefulness as a flexible resource, which can be used to diminish the probability of encountering chronic negative life events. In terms of Fig. 5.1, this represents a shift from being dominantly at (c) and (b) to being dominantly at (a) and (b). That is, the resource of money has an effect in two stages. The first is the most obvious. As income rises, fewer people within the sample experience homeostatic defeat due to some factor that can be ameliorated through the resource of money. This represents the significant rise in SWB up to $91,000–$120,000. Above this level of income there will be a continued, but gradual rise in average SWB, as progressively more of the sample experience a lifestyle that allows their SWB to inhabit the upper portion of their set-point-range. However, of course, in any population sample there will always be some people with a level of SWB that lies below its set-point irrespective of the financial situation. The cause will be attributable to situations, such as parenting unpleasant children, which are not amenable to resolution through money.
A further observation from Fig. 5.1 is that SWB plateaus at about 80 points. There are two reasons for this. First it reflects limitations to the upward movement of SWB due to resource saturation of the homeostatic system. Second it reflects the normal distribution of set-points within any population sample.
A second major external resource is a relationship with another adult that involves mutual sharing of intimacies and support. Almost universally, the research literature attests to the power of such relationships to moderate the influence of potential stressors on SWB (for reviews see Henderson 1977; Sarason et al. 1990). It might be expected that the power of the two external buffers to protect SWB is additive, and this is demonstrated by the interaction between income and household structure in Fig. 5.2. These results are drawn from Cummins et al. (2009).

The interaction between income and household composition
The top line shows the effect of income on the SWB of people living only with their partner. It can be seen that this living arrangement makes people very resilient. Even at the lowest household income, SWB lies in the middle of the normal range. Notably, it does not change very much as income increases, rising only 3.7 points across the entire income range. This is another example of the ceiling created by homeostasis—that money as a resource cannot be used to chronically increase SWB beyond the set-point range for each individual. Thus, since the mean SWB of this group is already in the normal range at the lowest income level, the only influence of higher income is to increase the probability that SWB lies towards the top of its set-point-range.
The second line in this figure shows partners who are living with one or more children. Their resilience is lower because children drain the emotional and financial resources of their parents. Thus, at the lowest income level, SWB lies well below the normal range. This reflects the demands made by children exceeding the resources available to some parents. However, at a gross household income of $31,000–$60,000 the financial and relationship resources become sufficient for homeostatic control to be returned. Thereafter, rises in income do not statistically differ between the couples with and without children.
The situation for single parents is more extreme. Since they lack the resource of an adult partnership, they require an income of $61,000–$90,000 to regain homeostatic control. It is also informative to observe that the three-person household (partners plus child) on low income has higher SWB than the two-person household (one parent plus child). This is quite the reverse of the relative wellbeing normally assumed by Economists (see Trigger 2003). They usually calculate household wellbeing as income discounted by the number of people in the household. This method is incorrect in relation to SWB. The increased consumption of goods by the additional adult is more than offset by the instrumental and emotional support they are able to provide.
In summary, both income and relationship support are highly effective external buffers for SWB homeostasis, and their combined influence appears to be additive, as expected. Moreover, the relationship between SWB and both of the external buffers conforms fairly well to the predictions of homeostasis. But this is only the external aspects of homeostatic control. There is an additional set of buffers to assist homeostasis that are internal to each person.
3.2 Internal Buffers
When the external buffers are not strong enough to prevent something bad happening, all is not lost. At the heart of homeostasis is a set of genetically programmed internal buffers. These comprise protective devices that are brought into action because SWB is being threatened. At the simplest level these involve the automatic processes of adaptation and habituation. These act over time to make us less aware of challenging experiences. An example of this phenomenon can be observed in relation to the gradual loss of motor functioning with age. Because people adapt both their behavior and expectations to fit the reality of their diminishing motor capacity, the loss of functioning only weakly engages awareness, and so fails to threaten SWB. The extent to which this can happen is amazing. Many people with Multiple Sclerosis, which induces a gradual loss of motor functioning, report normal levels of SWB even when they lose the capacity to independently breathe and require mechanical ventilation (Bach et al. 1991).
We propose that this kind of adaptation is assisted by a set of cognitive buffers. These use cognition to restructure reality and so to minimize the impact of unavoidable negative experiences. The ways that the cognitive buffers do this are highly varied. For example, one can find meaning in the event (‘God is testing me’), fail to take responsibility for the failure (‘it was not my fault’) or regard the failure [dropping a vase] as useful (‘I did not like that old vase anyway and now I can buy another’). There are many such devices that essentially involve maintaining a sense of control, collectively called Secondary Control techniques (Rothbaum et al. 1982).
There are other ways of restructuring reality that do not involve the sense of control. One is protection of self-esteem through ‘splintering’. For example, when dropping the vase, one may think ‘Well, so I am a bit clumsy, but it doesn’t matter because I am so good at [making friends, cooking, writing, etc.]. Here, the cause of the bad event has been relegated to some aspect of performance that the person regards as unimportant to their sense of identity. People may also employ optimistic temporal restructuring, e.g “Well this has been a bad day, but tomorrow will be better”. And so on.
No doubt there are many more such cognitive devices but they all serve the same purpose. Some explanation or reason for the negative experience has been found that allows the person to feel that their sense of self and ability to understand the world is intact. Their sense of threat has been dissipated and SWB is assisted to return within its set-point range. A detailed discussion of these internal buffering systems is provided in Cummins and Nistico (2002) and Cummins et al. (2002).
It is important to note, in relation to all this, that the homeostatic system, as described, has the role of maintaining a positive sense of wellbeing that is both non-specific and highly personalized. It is concerned only with the abstract core feelings that the individual has about themselves and only in the most general sense. One consequence of this is to imbue people with a ‘positivity bias’ in relation to themselves. So, people generally feel they are ‘superior’ to others, or better than average (Diener et al. 1999; Headey and Wearing 1988, 1989). They believe they are luckier, happier and more moral (Andrews and Withey 1976). This is all part of the general positive bias that is ‘value added’ by the brain to such thought processes and which leads, under the normal circumstances of living, to a generalized positive self-view (Taylor and Brown 1988; Weinstein 1989).
It is these characteristics that allow the personal sense of wellbeing to be so defendable against the slings and arrows of misfortune. Because these self-beliefs are held at such an abstract level, specific instances of personal bad-luck or incompetence that might otherwise damage the sense of personal wellbeing, can be dismissed by the internal buffers in order to maintain the abstract belief. This general idea is not novel. For example, Tesser et al. (1989) provide empirical support for a model of Self-Evaluation Maintenance, in which the self recognizes good performance on a variety of dimensions, yet aspires to ‘be good at’ (or personally values) only a few such dimensions. Thus, one’s own performance is not threatening to self-evaluation provided that failures are confined to non-valued dimensions in life. Such processes assist people who are deaf, for example, to maintain a positive self-view (Bat-Chava 1994).
So, SWB is heavily defended and this hints at the importance of maintaining positive feelings about the self. But SWB is generally acknowledged to be a mixture of affect and cognition. So is this what homeostasis is actually defending?
4 What is Homeostasis Defending?
Most contemporary theorists regard the measurement of SWB, obtained through a verbal or written response, to involve both affective and cognitive processes. This was first recognized by Campbell et al. (1976) who suggested that this amalgam should be measured through questions of ‘satisfaction’. This form of question has since become standard for SWB measurement. However, relatively little research has been directed to examining the relative contribution of affect and cognition. Certainly the two components are separable (Lucas et al. 1996) but whether, as claimed by Diener et al. (2004), SWB represents a dominantly cognitive evaluation, is moot. To the contrary, recent research (Davern et al. 2007) points to the essence of SWB as a construct these authors call ‘Core Affect’.
The term Core Affect was coined by Russell (2003) to describe a neurophysiological state that is experienced as a feeling and which may be conceptualized as a deep form of trait affect, or mood. He describes it as analogous to felt body temperature in that it is always there, can be accessed when attention is drawn to it, extremes are most obvious, and it exists without words to describe it. Naturally enough, Russell regarded Core Affect in conformity with the circumplex model of affect, comprising a blend of hedonic (pleasant–unpleasant) and arousal values (activation–deactivation).
The reason Davern et al. were attracted to adopt this term was Russell’s determined description of Core Affect as a biologically influenced mood, rather than an emotion. Specifically, he made it clear that while the feeling of Core Affect can be consciously accessed, it is not tied to any specific object in the manner of an emotional response. Instead it is a mood-state, which refers to how the individual senses themselves in an abstract but personal way. If the perception of the Core Affect feeling becomes linked to a cause, then the feeling state makes the transition from mood to emotion.
A more recent account of Core Affect, however, has muddied this distinction. Russell (2009) makes it clear that Core Affect may be involved in either moods or emotions. He proposes that Core affect may become directed at something and, indeed, that Core Affect may itself be changed by a variety of other influences. Thus a new term is required that describes the mood affect associated with homeostasis. We propose the term Homeostatically Protected Mood (HPMood) to describe a feeling state with the following characteristics:
-
1.
It is a biologically determined positive mood that comprises the most basic experienced feeling. It is hard-wired for each individual, comprising the tonic state of affect that provides the activation energy, or motivation, for behavior.
-
2.
HPMood is not only the dominant affective constituent of SWB, as determined by Davern et al., but also the basic steady-state, set-point that homeostasis seeks to defend.
-
3.
HPMood perfuses all higher process, including personality (for a review of the neurobiology of personality see Depue and Collins 1999), memory and momentary experience. It perfuses all cognitive processes to some degree, but most strongly the rather abstract notions of self (e.g. I am a good person). These self-perceptions are held at strength of positivity that approximates the set-point HPMood.
Consistent with this fundamental role, we hypothesise that the process of evolution has advantaged the survival of individuals who experience a level of HPMood corresponding to 70–80 points pleasant or positive. Notably, SWB values above and below this range are associated with different forms of cognitive functioning, which each have their own advantages and disadvantages. For example, higher SWB is associated with enhanced friendliness and problem solving (Lyubomirsky et al. 2005), but has the downside of poor information processing, an exaggerated sense of control, and therefore enhanced risk-taking. Lower SWB, on the other hand, leads to more careful information processing (for a review see Forgas 2008) and greater preparedness for threat (Sweeny et al. 2006) but carries the risk of low motivation and even depression if it becomes chronic. Thus, we propose, 75 points is a trade-off between the advantages and disadvantages of higher and lower values. This level then, on average, constitutes the optimum set-point range for SWB, corresponding to the most adaptive range of mood affect.
As measured by Davern et al. (2007), HPMood can be parsimoniously represented as the combined affects of happiness, contentment, and excitement. These represent the activated and deactivated pleasant quadrants of the affective circumplex (for a review of affect see Cropanzano et al. 2003). Davern et al. tested the relative strength of HPMood, cognition, and all five factors of personality, as predictors of SWB. The cognitive component of SWB was measured using 7 items derived from Multiple Discrepancies Theory (Michalos 1985). These items address the perceived gap between what the respondent currently has and general life aspirations, what age-matched others have, the best one has had in the past, expected to have 3 years ago and expects to have after 5 years, deserves and needs.
Consistent with previous research, all three components correlated significantly with SWB and with one another. However, when the variances were controlled by structural equation modelling, it was demonstrated that affect and MDT are the dominant components of SWB. Indeed, after accounting for both of these, personality made only a very small contribution to the explanation of SWB variance. The simplified model from this chapter is reproduced in Fig. 5.3. The personality factors are designated as: N—Neuroticism, E—Extraversion, O—Openness, A—Agreeableness, C—Conscientiousness.

Simplified affective-cognitive model of SWB (Davern et al. 2007)
This finding has been replicated using independent data (Blore 2008), from which we deduce that mood is the dominant component of SWB. We also propose HPMood as the driving force behind individual set point levels in SWB homeostasis.
Over the past few years, there have been several critics of set-point theory (e.g. Fujita and Diener 2005; Headey 2008; Lucas 2007) based on observed changes in the SWB of individuals over time. The first two of these chapters report data from the German Socio-Economic Panel Study from 1984 to 2000. For example, Fujita and Diener showed that, over this 16 year period, about 10 % of the sample showed a change in satisfaction of about 30 points. They conclude that SWB “can and does change for some people.”
All of these authors interpret changes in SWB over time as indicative that the set-point has changed. However, homeostasis theory and HPMood offers an alternative possibility. We propose that when people report a level of SWB outside their set-point range, they have simply lost contact with their set-point mood-affect. That is, at the time of data collection, their level of SWB was being controlled by a powerful emotional state which overwhelmed homeostasis, and so dominated their awareness. Within this alternative conception, each person’s HPMood and set-point remains unaltered and the abnormal level of SWB reflects attention to the dominating emotional state.
This alternative conception also predicts that, over time, external and internal resources will be directed to the restoration of homeostasis, as has been discussed. If these resources are sufficient, they will reduce the perceived level of challenge to the point that that homeostatic control is restored. When this occurs, the person regains contact with their HPMood, and their reported SWB returns to its set-point-range.
An alternative and interesting possibility is that set-points do, in fact, change systematically over the life span (Land, personal communication). Results from the Framingham Heart Longitudinal Study has found that a number of physiological parameters that must be maintained within homeostatic bounds for survival–such as blood pressure–have “optimal” values that change with age. Such changes are adaptive, in that individuals who deviate far from the optimal values are at higher risk of mortality. Through analogy, is possible that SWB set-points also change over the life-span, quite possibly in an upward direction to compensate for functional loss. We certainly find (Cummins et al. 2005) that the highest levels of SWB occur in old age.
5 SWB and Depression
From all of the above, SWB can be predominantly characterized as a stable positive mood that is normally held within a narrow range of values for each individual. The level of this set-point-range is genetically determined and a homeostatic system acts to defend our perception of Homeostatically Protected Mood as our normal sense of affective self. SWB is an approximation of HPMood, which is why, under normal conditions, SWB approximates the set-point-range. However, if the level of challenge to SWB becomes too great, homeostasis fails. When this occurs, our affective experience is redirected from HPMood to the dominating emotion, either positive or negative.
Under such conditions, SWB no longer conforms to the set-point-range of HPMood. If it is made to be higher, due to the induction of an acute positive emotion, then the processes of adaptation and habituation soon return the dominant affective experience back to HPMood. Whether, as claimed by Positive Psychology, it is possible to maintain a substantially higher level of positive affect than the set-point-range on a chronic basis is moot. As of this writing no reliable empirical evidence is available to support such a view, which is also counter to homeostatic theory.
If SWB is made to be lower, through the induction of a negative emotion, then the same processes of adaptation and habituation, together with secondary control, will normally allow recovery back to the set-point-range of HPMood. However, if the negative challenge is chronic and strong, recovery may not take place. The homeostatic system has a limited capacity to recover normal functioning and if this capacity is chronically exceeded, recovery will not occur. Under such conditions, homeostasis will be persistently defeated, and the loss of positive affect will remain as the dominating experience. This is the reason that poor countries have such low SWB. They contain a high proportion of their population who are living under conditions of chronic homeostatic defeat. We have recently reported the same phenomenon in Australia through a study of 4,000 people providing care for a disabled family member at home (Cummins et al. 2007). Their mean level of SWB was 59 points.
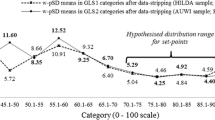
We propose that this loss of positive mood is the essence of depression. The relationship between SWB and the Depression sub-scale of the Depression, Anxiety and Stress Scale (Lovibond and Lovibond 1995) is shown below using cumulative data from our surveys.
Figure 5.4 is based on DASS increments of 3.0 points. This increment size is the smallest range for our cumulative sample that allows an N > 20 per group. The group Ns range from 785 for depression group (0.1–3.0) to 23 for group (33.1–36.0) The Figure reveals a clearly inverse relationship between the falling PWI and rising depression scores. However, two observations pertain. First, the rate of SWB decrease is far less than the rate of depression score increase. This is consistent with resistance to SWB change. Second, the rate at which PWI falls appears to slow at a depression score of 15.1–18 (moderate) through to 24.1–27.0 (severe), with these depression categories defined by reference to the scale manual. The amount of change between these four contiguous scores, which differ sequentially by <2 points, can be contrasted with the amount of change in the four immediately higher and lower scores, which all differ sequentially by >2 point, as shown below.

PWI and DASS depression means across increments of depression scores
Table 5.1 shows the changing rate of PWI decrease and the appearance of the homeostatic plateau over the middle grouping. As the level of challenge (depression score) increases from 0 to 18, the value of SWB moves down in a linear fashion to approximate the start of the homeostatic plateau. This is phase (a) in Fig. 5.1. Then, over the depression rating of 18–27, homeostasis ‘holds-the-line’ and SWB remains relatively unchanged (Phase b). However, at a depression score of 27 or greater, homeostasis is overwhelmed; control of SWB passes from the homeostatic system to the challenging agent, and SWB drops markedly (Phase c).
A more detailed description of these results in relation to Homeostatic Theory is as follows.
-
1.
In reference to Fig. 5.4, the fact that the highest PWI value corresponds to a depression score of zero is logical. Moreover, the value of 82.8 points is consistent with theory, based on two assumptions, both of which have been previously argued. The first is that the normal range for individual set-points is 55–95, and the second is that the normal set-point-range is 5–6 points on either side of the mean. Then, if zero depression is taken as implying that each SWB value approximates the top of each set-point-range, then this SWB distribution extends from (55 + 6) = 61 to (95 + 6) ≈ 100. The half-way point on this range is 80.5 points, which is a reasonable approximation to the measured value of 82.8 points.
-
2.
The start of the plateau in Fig. 5.4 occurs at a PWI of 63.2 and it ends at 58.5 points. This is also consistent with theoretical prediction. In a previous report using population sample mean scores from 19 different countries as data, the overall mean was found to be 74.4 and the standard deviation 5.1 points (Cummins 2003). It was also calculated that 70 points, corresponding to about one standard deviation below the mean, was the lowest value on the plateau, below which the value SWB fell sharply.
The current data set uses the scores of individuals rather than population mean scores. The overall mean is 73.40 and the standard deviation is much larger as 14.54. One standard deviation below the mean is 58.9 points, which approximates the lower end of the plateau in Fig. 5.4. Thus, the results using either population mean scores as data, or the scores of individuals as data, converge to yield a common finding. This is that SWB values lying one standard deviation below the normative mean approximate the boundary between homeostatic maintenance and homeostatic defeat. Thus, SWB values that lie much further from the normative mean than one standard deviation are likely under the control of the challenging agent rather than homeostasis (refer to Fig. 5.1).
Perhaps the most interesting question raised by these results, is why plotting the PWI against the DASS shows this plateau effect. The DASS items measure the extent of negative affect (down-hearted and blue), life being meaningless, low personal self-worth, etc. In other words, even quite strong negative feelings about the self can co-exist with normal or even high levels of SWB. There is, thus, a degree of disconnection between negative and positive feelings about the self as long as homeostasis is functional. This is highly adaptive in allowing negative feeling to be acknowledged while also maintaining normal levels of SWB. However, once the level of challenge becomes overwhelming, positive feelings about the self evaporate and it is possible that true depression sets-in.
6 Summary and Conclusions
It has been argued that Subjective Wellbeing (SWB) is managed by a system of psychological devices which have evolved for this purpose. Further, that this management is actually directed at the protection of Homeostatically Protected Mood, which is the major component of SWB. We experience HPMood as a combination of contentment, happiness and arousal thus giving us a normally positive view of ourselves. It is further proposed that when homeostasis fails, due to the overwhelming nature of a negative challenge, people lose contact with HPMood and experience the dominance of negative rather than positive affect. When this condition is chronic, people experience depression.
References
Andrews FM, Withey SB (1976) Social indicators of well-being: American’s perceptions of life quality. Plenum Press, New York
Bach JR, Campagnolo DI, Hoeman S (1991) Life satisfaction of individuals with Duchenne Muscular Dystrophy using long-term mechanical ventilatory support. Am J Phys Med Rehabil 70:129–135
Bat-Chava Y (1994) Group identification and self-esteem of deaf adults. Personality Soc Psychology Behav 20(5):494–502
Blore JD (2008) Subjective wellbeing: an assessment of competing theories. Unpublished Doctoral Thesis. Deakin University, Geelong
Campbell A, Converse PE, Rodgers WL (1976) The quality of American life: perceptions, evaluations, and satisfactions. Russell Sage Foundation, New York
Cropanzano R, Weiss HM, Hale JMS, Reb J (2003) The structure of affect: reconsidering the relationship between negative and positive affectivity. J Manage 29(6):831–858
Cummins RA (1995) On the trail of the gold standard for life satisfaction. Soc Indic Res 35:179–200
Cummins RA (1998) The second approximation to an international standard of life satisfaction. Soc Indic Res 43:307–334
Cummins RA (2000) Personal income and subjective well-being: a review. J Happiness Stud 1:133–158
Cummins RA (2003) Normative life satisfaction: measurement issues and a homeostatic model. Soc Indic Res 64:225–256
Cummins RA, Eckersley R, Pallant J, Van Vugt J, Misajon R (2003) Developing a national index of subjective wellbeing: the Australian unity wellbeing index. Soc Indic Res 64:159–190
Cummins RA, Gullone E (2000) Why we should not use 5-point Likert scales: the case for subjective quality of life measurement. In: Paper presented at the second international conference on quality of life in cities. National University of Singapore, Singapore. http://www.deakin.edu.au/research/acqol/instruments/PWI/2000-QOL_in_Cities-Likert_Scales-ss.doc
Cummins RA, Gullone E, Lau ALD (2002) A model of subjective well being homeostasis: the role of personality. In: Gullone E, Cummins RA (eds) The universality of subjective wellbeing indicators: social indicators research series. Kluwer, Dordrecht, pp 7–46
Cummins RA, Hughes J, Tomyn A, Gibson A, Woerner J, Lai L (2007) Australian Unity Wellbeing Index: Report 17.1 The Wellbeing of Australians—Carer Health and Wellbeing. Melbourne: Australian Centre on Quality of Life, School of Psychology, Deakin University. Retrieved 30 June 2009, from http://www.deakin.edu.au/research/acqol/index_wellbeing/index.htm
Cummins RA, Nistico H (2002) Maintaining life satisfaction: the role of positive cognitive bias. J Happiness Stud 3:37–69
Cummins RA, Woerner J, Gibson A, Lai L, Weinberg M, Collard J (2008) Australian Unity Wellbeing Index: Report 19.0. The Wellbeing of Australians—Links with exercise, nicotine and alcohol. Australian Centre on Quality of Life, School of Psychology, Deakin University, Melbourne. ISBN 978 1 74156 113 5. Retrieved 30 June 2009, from http://www.deakin.edu.au/research/acqol/index_wellbeing/index.htm
Cummins RA, Woerner J, Gibson A, Weinberg M, Collard J, Chester M (2009) Australian Unity Wellbeing Index: Report 21.0. The Wellbeing of Australians—Gambling, Chocolate and Swine Flu. Australian Centre on Quality of Life, School of Psychology, Deakin University, Melbourne. ISBN 978 1 74156 125 8. Retrieved 2 Sept 2009, from http://www.deakin.edu.au/research/acqol/index_wellbeing/index.htm
Cummins RA, Woerner J, Tomyn A, Knapp T, Gibson A (2005) Australian unity wellbeing index: Report 14.0—”The Wellbeing of Australians—Personal Relationships”. Australian Centre on Quality of Life, School of Psychology, Deakin University, Melbourne. Retrieved, 30 June 2009, from http://www.deakin.edu.au/research/acqol/index_wellbeing/index.htm
Davern M, Cummins RA, Stokes M (2007) Subjective wellbeing as an affective/cognitive construct. J Happiness Stud 8(4):429–449
Depue RA, Collins PF (1999) Neurobiology of the structure of personality: dopamine facilitation of incentive motivation and extraversion. Behav Brain Sci 22:491–569
Diener ED, Napa Scollon CN, Lucas RE (2004) The evolving concept of subjective well-being: the multifaceted nature of happiness. In: Costa PT, Siegler IC (eds) Recent advances in psychology and aging. Elsevier Science BV, Amsterdam, pp 187–219
Diener ED, Suh EM, Lucas RE, Smith HL (1999) Subjective well-being: three decades of progress. Psychol Bull 125(2):276–302
Forgas JP (2008) The strange cognitive benefits of mild dysphoria: on the evolutionary advantages of not being too happy. In: Forgas JP, Haselton MG, von Hippel W (eds) Evolutionary psychology and Social cognition. Psychology Press, New York, pp 107–121
Fujita F, Diener E (2005) Life satisfaction set point: stability and change. J Pers Soc Psychol 88(1):158–164
Hanestad BR, Albrektsen G (1992) The stability of quality of life experience in people with Type 1 diabetes over a period of a year. J Adv Nurs 17:777–784
Headey B (2008) The set-point theory of well-being: negative results and consequent revisions. Soc Indic Res 85(3):389–404
Headey B, Holmstrom E, Wearing A (1984a) The impact of life events and changes in domain satisfactions on well-being. Soc Indic Res 15:203–227
Headey B, Holmstrom E, Wearing A (1984b) Well-being and ill-being: different dimensions? Soc Indic Res 14:115–139
Headey B, Wearing A (1986) The sense of relative superiority—central to well-being. University of Melbourne, Melbourne
Headey B, Wearing A (1987) A theory of life satisfaction and psychological distress. University of Melbourne, Melbourne
Headey B, Wearing A (1988) The sense of relative superiority—central to well-being. Soc Indic Res 20:497–516
Headey B, Wearing A (1989) Personality, life events, and subjective well-being: toward a dynamic equilibrium model. J Pers Soc Psychol 57:731–739
Henderson S (1977) The social network, support and neurosis. the function of attachment in adult life. Br J Psychiatry 131:185–191
International Wellbeing Group (2006) Personal wellbeing index manual. Deain University, Melbourne. Retrieved 30 June 2009, from http://www.deakin.edu.au/research/acqol/instruments/wellbeing_index.htm
Jones LV, Thurstone LL (1955) The psychophysics of semantics: an experimental investigation. J Appl Psychology 39(1):31–36
Kozma A, Stone S, Stones MJ (2000) Stability in components and predictors of subjective well-being (SWB): implications for SWB structure. In: Diener E, Rahtz DR (eds) Advances in quality of life: theory and research. Kluwer Academic Publishers, Great Britain, pp 13–30
Liu B (1975) Quality of life: concept, measure and results. Am J Econ Sociology 34:1–13
Lovibond SH, Lovibond PF (1995) Manual for the depression anxiety stress scales. Psychology Foundation, Sydney
Lucas RE (2007) Adaptation and the set-point model of Subjective Well-Being: Does happiness change after major life events? Curr Directions Psychological Sci 16(2):75–79
Lucas RE, Diener E, Suh E (1996) Discriminant validity of well-being measures. J Pers Soc Psychol 71:616–628
Lykken D, Tellegen A (1996) Happiness is a stochastic phenomenon. Psychol Sci 7:186–189
Lyubomirsky S, King L, Diener E (2005) The benefits of frequent positive affect: does happiness lead to success? Psychol Bull 131(6):803–855
Michalos AC (1985) Multiple discrepancies theory (MDT). Soc Indic Res 16:347–413
Nieboer AP (1997) Life events and well-being: a prospective study on changes in well-being of elderly people due to a serious illness event or death of the spouse. Thesis Publishers, Amsterdam
Ormel J (1983) Neuroticism and well-being inventories. Measuring traits or states? Psychol Med 13:165–176
Ormel J, Schaufeli WB (1991) Stability and change in psychological distress and their relationship with self-esteem and locus of control: a dynamic equilibrium mode. J Pers Soc Psychol 60:288–299
Rothbaum F, Weisz JR, Snyder SS (1982) Changing the world and changing the self: a two-process model of perceived control. J Pers Soc Psychol 42:5–37
Russell JA (2003) Core affect and the psychological construction of emotion. Psychol Rev 110(1):145–172
Russell JA (2009) Emotion, core affect, and psychological construction. Cognition Emotion 23(7): 1259–1283. ISSN: 1464–0600
Sarason IG, Sarason BR, Pierce GR (1990) Social support: the search for theory. J Soc Clin Psychol 9:137–147
Stones MJ, Kozma A (1991) A magical model of happiness. Soc Indic Res 25:31–50
Sweeny K, Carroll PJ, Sheppard JA (2006) Is optimism always best? Future outlooks and preparedness. Curr Directions Psychological Sci 15(6):302–306
Taylor SE, Brown JD (1988) Illusion and well-being: a social psychological perspective on mental health. Psychol Bull 103:193–210
Tesser A, Pilkington CJ, McIntosh WD (1989) Self-evaluation maintenance and the mediational role of emotion: the perception of friends and strangers. J Pers Soc Psychol 57:442–456
Trigger D (2003) Does the way we measure poverty matter? National Centre for Social and Economic Modelling, University of Canberra
Weinstein ND (1989) Optimistic biases about personal risks. Science 246:1232–1233
World Bank (1997) World Values Surveys; GNP/capita purchasing power estimates from World Bank, World Development Report, 1997. Retrieved 30 June 2009, from http://margaux.grandvinum.se/SebTest/wvs/articles/folder_published/article_base_56
Acknowledgments
I thank Ann-Marie James for her assistance in the preparation of this manuscript and Australian Unity for their continued support of this research. We also acknowledge the key role played by Renee Bear, Wendy Kennedy and Melissa Weinberg in coining the term Homeostatically Protected Mood.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2013 Springer Science+Business Media Dordrecht
About this chapter
Cite this chapter
Cummins, R.A. (2013). Subjective Well-Being, Homeostatically Protected Mood and Depression: A Synthesis. In: Delle Fave, A. (eds) The Exploration of Happiness. Happiness Studies Book Series. Springer, Dordrecht. https://doi.org/10.1007/978-94-007-5702-8_5
Download citation
DOI: https://doi.org/10.1007/978-94-007-5702-8_5
Published:
Publisher Name: Springer, Dordrecht
Print ISBN: 978-94-007-5701-1
Online ISBN: 978-94-007-5702-8
eBook Packages: Humanities, Social Sciences and LawSocial Sciences (R0)