
Abstract
The practice of stratification based on variables or indicators such as race, ethnicity, gender and socioeconomic position has been integral in the development of a substantial body of the social epidemiologic literature demonstrating significant and persistent inequalities in health outcomes. However, it is time for social epidemiologists to recognize that mere demonstration of gradients is no longer enough. The identification of gaps and gradients based on these variables flags the presence of a potential problem but does not explain the underlying mechanisms. Yet these proxies are often treated as if they are the exposures responsible for the gaps in outcomes. In this chapter, we will explore how the practice of stratification in epidemiologic research can evolve to identify the real causes of the gaps and to inform interventions and evaluations of interventions that target identified health inequities. The key recommendations of this chapter are to:
-
1.
Draw from strong theories about causal mechanisms, which must take into consideration the relational aspects of the groups we are comparing;
-
2.
Undertake measurement of, and stratification by, the modifiable societal and contextual factors that lead to hierarchical power relations between socially defined groups; and
-
3.
Undertake measurement of variables that accurately explain the heterogeneity of experiences within socially defined groups to ensure that groups or individuals are not essentialized, with a particular focus on the solution-linked variables responsible for the heterogeneity.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
These keywords were added by machine and not by the authors. This process is experimental and the keywords may be updated as the learning algorithm improves.
1 Introduction
A fundamental strategy employed in epidemiology is to stratify study populations to investigate differences between groups such as those distinguished by age, sex or gender and race or ethnic group (Shim 2002). With a growing interest in social and health inequities and the emergence of the sub-discipline of social epidemiology, many epidemiologists have focussed in on the differential impact of social, economic and demographic variables on health-related processes and outcomes (Berkman 2009; Putnam and Galea 2008). This practice of stratification has been integral in the development of a substantial body of international literature that has demonstrated significant and persistent inequalities in health outcomes based on variables such as race, ethnicity, gender and socioeconomic position (e.g. income and education) (Berkman 2009; Hofrichter 2006; Shim 2002).
However, social epidemiology is becoming increasingly at risk of stagnation unless researchers acknowledge that the demonstration of gaps and gradients is no longer enough, in part, because they only flag the presence of a potential problem and do not explain why a problem exists or how to address that problem. For example, knowing that infant mortality is two times higher among African Americans compared to Whites does not yield information about which interventions should be implemented to reduce the gap. As has been argued throughout this book, social epidemiologists need to move the emphasis of the field away from problem description and toward identifying actionable mechanisms and the generation of evidence to inform the development of viable interventions (see Chap. 1). Although it is commonplace to see a discussion on action that could be taken to reduce the identified inequity in many social epidemiologic papers, these discussions are often speculative and not based in strong theory or direct evidence regarding the causes or contributors of the gaps. In order to determine the best actions to take to reduce inequities, one requires a firm basis in the underlying and modifiable mechanisms that lead to these same inequities, and this foundation is often where social epidemiology is still lacking (Engel 2002; Krieger 2001; Krieger et al. 1993, 1997; Randall 2006; Syme 2008).
The increased level of distress experienced by many homosexuals upon coming to terms with their own sexuality when compared to heterosexuals realizing their sexuality provides one example. This marked distress was at one time viewed as a mental disorder (listed as “ego dystonic homosexuality” in The Diagnostic and Statistical Manual of Mental Disorders, 3rd edition), instead of as a fairly predictable result of the prospect of having to deal with both internalized and societal homophobia (Zucker and Spitzer 2005). One can imagine two markedly different paths towards ameliorating this mental distress based on these two explanations, one focussed on changing the individual, e.g. the use of fluoxetine to suppress sexual activity (Elmore 2002), the other focussed on changing societal biases and/or helping those affected with coping mechanisms and de-stigmatization strategies (Lamont 2009). Clearly, it is only through direct exploration of causes of distress level gaps (i.e., societal-level discrimination toward homosexuals) that we arrive at feasible ways to begin to close the gaps (i.e., not to feel the need to fix the individual).
In this chapter, we seek to view stratification through a realist lens (see Chap. 2). We aim to encourage social epidemiologists to rethink the current reflexive practice of stratification based on variables or indicators such as race or income, as it does little to explain why gaps exist or shed light on achievable solutions to the gaps observed. As they are currently conceptualized and operationalized, some of these stratification variables are often uninformative, serving as poor proxies for the true mechanisms that underlie health inequities (Coburn 2004; Gravlee 2009; Manly 2006; Sayer 1992). Yet we regularly treat these poor proxies as if they are the exposures responsible for the gaps in outcomes. “Race” itself is almost never the reason a gap exists; instead it is the exposure to interpersonal racism or being subjected to institutional racial discrimination, the intergenerational transmission of its effects or particular experiences that are associated with race that lead to inequities. Indicators, in other words, are proxies of something, and it is imperative that social epidemiology have a clear explanation of what that something is (see Chap. 2). Moreover, when such proxies are used, the reader can insert their own interpretation as to whether it is a cultural, genetic (e.g., Muntaner et al. 1996), economic or discriminatory practice that has lead to the observed gaps, resulting in confusion as to the real causes of the inequities. Further evidence of the weakness of these proxies is apparent when we consider that many are measured cross-sectionally; yet, the life course and legacy effect literature tell us that the cumulative and intergenerational effects of social deprivation could be much more revealing (David and Collins 2007; Love et al. 2010; Singh-Manoux et al. 2004; Smith et al. 1997).
In this chapter, we will explore how, using new and complementary indicators and methods, stratification can evolve to inform interventions and evaluations of interventions that target identified health inequities. We aim to move social epidemiology from only examining the who of health inequities to a focus on how to change health inequities. In particular, our recommendations are threefold: (1) draw from strong theories about causal mechanisms, which must take into consideration the relational aspects of the groups we are comparing; (2) undertake measurement of, and stratification by, the modifiable societal and contextual factors that lead to hierarchical power relations between socially defined groups; and (3) undertake measurement of variables that accurately explain the heterogeneity of experiences within socially defined groups to ensure that groups or individuals are not essentialized, with a particular focus on solution-focused variables responsible for the heterogeneity.
We begin the chapter with a discussion of the need for supporting theories. Such information is currently sparse in the literature but is essential to inform attainable solutions to the problems identified when we demonstrate gaps by race, gender or class.
2 The Need for Theory
Epidemiology and public health, as applied fields, have tended to de-emphasize theory or relied on implicit biomedical and biological-based theories that predominate within the field to explain health and health inequities. Yet all research, and especially all causal claims, including those concerned with social, economic, racial and gender inequities, are based upon explicit or implicit theory. Epidemiology and public health in the twentieth century have relied heavily on biomedical theories to explain the occurrence of and inequities in health and well-being (Engel 2002; Krieger 2001; Stallones 1980; Susser 1985). Thus, despite much research challenging the scientific validity of the categories of “race” or “ethnicity” as they are typically used in public health studies (American Anthropological Association 1998; Gunaratnam 2003; Stanfield and Dennis 1993) and ample evidence dispelling the myth that racial groups reflect inherent biological or genetic homogeneity (American Anthropological Association 1998; U.S. Department of Energy Office of Science 2003), we still encounter studies that invoke such explanations for demonstrated racial or ethnic gaps (Cooper et al. 2003).
At the other end of the spectrum, there are those who argue that race and ethnicity are socially determined categories shaped by societal processes like slavery, colonization, discrimination and/or privilege (Fujishiro 2009; Muntaner et al. 1996; Randall 2006). Thus, examination of racial differences should be explained by historical, materialist or cultural processes (Gunaratnam 2003). There is even the suggestion that the categories of race be abandoned in favour of the study of the processes that contribute to so-called racial gaps (Stanfield and Dennis 1993).
While we focus on “race” here as an example, it is important to note that stratification by race is primarily an American practice. Race, and in particular African American race, is a proxy for the history of slavery and continuous discrimination unique to this population and is not applicable in other settings such as neighbouring Canada. Historical differences between the United States and Canada means that references to Black race would represent an entirely different set of circumstances and is very rarely used in Canadian epidemiologic research. Because of the history of immigration in Canada, the term “visible minority” has been used instead by federal agencies to represent “persons, other than Aboriginal people, who are non-Caucasian in race or non-white in colour” (Statistics Canada 2009). Visible minority status was developed to study labour market disadvantages of this group (Statistics Canada 2009). Thus, the evolution of these variables used for stratification often reflects a historical context that is rarely made explicit.
3 The Risks of Essentialism
To progress in our understanding of why inequalities by race or ethnicity exist and, therefore, to reduce the gaps, we must avoid essentializing categories such as race, ethnicity, sex or gender and even poverty. When we essentialize we “impute a fundamental, basic, absolutely necessary constitutive quality to a person, social category, ethnic group, religious community, or nation” (Werbner 2003). At the same time, we are not likely to discard the use of race, ethnicity or the other categories in our research as they reflect socially relevant groupings of populations (more so in some countries, such as the United States, than others). Moreover, even when using variables such as “racial identity,” or discrimination, epidemiologists seek to simplify their categories, thus contributing to continued essentialism.
If we accept that the theories of inherent biological or genetic differences by race are invalid and that using race or ethnicity as a proxy for social explanations is too limiting in its ability to explain complex gaps, then how should epidemiologists approach the examination of inequities by race or ethnicity? To avoid essentialism, Gunaratnam (2003) recommends that our research: (1) take into account the relational nature of the categories being compared; (2) connect the categories to their context; and (3) focus on heterogeneity within categories of difference to ensure that groups or individuals are not defined by a single category.
Our theories of inequities must take into consideration the relational aspects of the groups we are comparing. Thus, rather than categorizing or stratifying groups into, for example, low or high income, we must articulate how wealth matters to health and also investigate the ways in which individual and institutional practices, through power, status, resources and connections, serve to maintain the wealth gap and maintain poverty (Wright 2008). Although individuals on both ends of the spectrum may not be aware of these institutionalized practices, competition and control for scarce resources where the wealthy consume more than their fair share, exploitation of those with less power by the wealthy, such that those in power benefit while the powerless suffer, and the ability of the wealthy to utilize power and connections to maintain their wealth at the expense of those with less wealth, are meaningful relations that should be incorporated into our research to explain why the gaps exist. Currently, strata or categories of income are devoid of such acknowledgements. Class-based measures (O’Campo and Burke 2004; Wright 2008) incorporate the relations between classes or potential “warfare” between the class strata and provide a theoretical explanation for why gaps exist. Measures on inequities by gender in the workplace, as reported in a study illustrating unique indicators of employment-based gender discrimination for income, job strain, job demands and control that were informed by strong theories, suggests that these factors illustrate large disparities in these areas even when controlling for occupation and are important predictors of health (O’Campo and Burke 2004).
The idea that we must connect the categories to the larger contexts is the second recommendation of Gunaratnam. The larger contexts that have contributed to the differences observed between groups will be discussed at length in the following section. Focussing on heterogeneity within groups being compared is a third strategy. This, too, will be discussed in the section on heterogeneity below. This acknowledgement of heterogeneity not only prevents groups from being reduced to simple homogeneous categories but also ensures that research reflects the multiple identities and experiences that can simultaneously shape risks and determine health. Thus, using strong theory to inform the key stratification variables and measuring indicators that avoid essentializing these groups will lead to progress in ensuring that epidemiologic evidence begins to point to appropriate interventions that move beyond the simple demonstration of disparities.
4 The Importance of Context
4.1 The Misguided Focus on Individual-Level Factors
Our second key recommendation for stratification in social epidemiology is to measure modifiable contextual factors that underlie the gradients and gaps we frequently observe. Too often within social epidemiology research, the analyses of the determinants of inequalities have focussed at the level of the individual. Consequences of this misguided focus have included epidemiology’s long history of reductionist genetic and biological explanations for racial and ethnic health inequities (although it must be noted that a misconstruction of race as a biological classification has also strongly contributed to these misguided explanations) as well as suppositions such as “downward drift” (the hypothesis that mental disorders are more represented in lower social classes because individual weaknesses in mental functioning lead to low social class attainment (Perry 1996)) and similar individually focussed explanations for socioeconomic health inequities. While more recently there has been a growth in the inclusion of societal-level factors in research concerning health inequities, determinants are still primarily focussed on an individual’s lifestyle and perceived choices without the requisite examination of the context of how power is embedded in the society around that individual (Krieger 2000; Muntaner et al. (2011); Putnam and Galea 2008; Shankardass et al. 2010a; Syme 2008). The subsequent explanations and range of interventions emerging from this evidence are therefore targeted at changing the behaviours of the individual, not at changing the contextual problems that shape and determine behaviours and the health of the individual.
For example, a major risk factor for the leading cause of mortality, cardiovascular disease, is physical activity. As physical activity rates have been suggested by some authors to be lower among people of lower income compared to their more well-to-do counterparts, proposed solutions are often focussed around ways to increase motivation of disadvantaged individuals to exercise more often (Hallal et al. 2005; McMurray et al. 2000). Factors such as accessibility of opportunities to exercise (e.g., time, cost, geographic proximity) are often ignored. Similarly, many of the discussions about poverty and low income frequently focus on individual-level characteristics such as employment readiness or educational attainment, which are modeled as determinants of low-income status. Factors such as labour markets, state or federal employment and minimum wage policies or business practices of cutting wages to increase profits, to name a few examples, are rarely considered in the examination of health inequities despite being the drivers of income levels. Similarly, more immediately actionable contextual factors such as the local availability of employment, employment training programs or traditional and alternative educational opportunities are rarely considered. Tellingly, in a review of how health inequities are addressed in the American media, Kim et al. (2010) found that behavioural explanations dominated the discourse.
The choice to frame health inequities as individual-level issues and to explain them with individual-level behaviours can be a counterproductive one. This choice often encourages, whether intended or not, the practice of “blaming the victim” (Green and Darity 2010; Wallace 2008) and encourages the erroneous use of resources on inappropriate interventions. In the case of physical activity, if the appropriate action is believed to be to encourage the individual to exercise, then the implicit (or even explicit) suggestion is that the individual has chosen to be lazy or does not have the knowledge or intelligence to recognize that they are lazy. If we focus on the demographic characteristics of low-income individuals, then we are choosing to not focus on the larger economic and political context that exclude them from obtaining quality education and employment training. This example illustrates how the wrong solutions, or solutions that will do little to ameliorate the true causes, will be implemented if contextual factors are not taken into consideration.
4.2 The Role of Power Relations
As social epidemiologists we can no longer afford to ignore that, on a global level, the wealthy or those of the lightest shade of skin color consistently have access to both micro- and macro-level privileges that have been determined by social, historical and economic societal-level contexts. Correspondingly, the poor and those of darker shades of skin color are consistently and actively excluded from receiving these same privileges (O’Campo 2007; Wallace 2008). In fact, many of the determinants of health and social inequalities observed the world over emanate from the societal processes of White privilege or privilege of the majority group, inequitable access to quality education, unjust labour markets, unjust financial policies and neo-liberalist economies and/or political systems. Researchers need to examine these processes, especially those that are more readily actionable with community-based interventions (Green and Darity 2010; James 2009; Krieger 2003; Manly 2006; Wallace 2008).
The magnitude of the effects of the unequal distribution of power was captured in words by the African American physician, Charles Roman, in 1917 and still hold truth over 90 years later, once we interpret “strength of the white man” to represent the political power of the dominant social class: “The greatest difficulties confronting us from a sanitary and hygienic standpoint arise not from the physiological weakness of the colored man but from the psychological strength of the white man” (Roman 2010). Yet the aforementioned article by Kim et al. (2010) tells us that less than 5% of media articles on health inequities invoked a social justice explanation. To truly advance the field of social epidemiology, researchers need to constantly challenge the implicit idea that particular socially defined groups do not do well because they are not allowing themselves to integrate into the mainstream and instead develop explanations that incorporate the role that institutionalized power relations created by larger society play in actively perpetuating health inequities (Muntaner et al. 2011; Putnam and Galea 2008; Shankardass et al. 2010a; Syme 2008). These power relations are manifested not only at the larger level (national, state, provincial) but also at the more local level (neighbourhood, district), suggesting that the route to change will not only require widespread political upheaval but also community-based interventions that researchers can undertake immediately.
To unearth the true mechanisms generating inequities and to develop effective interventions, the contexts that generate the social inequalities must be measured and incorporated into our research. In essence, instead of comparing the number of calories that an individual from an empowered group is burning versus the number of calories an individual from a disempowered group is burning, we need to compare: the walkability of their neighbourhoods; whether each feels safe walking or cycling in their neighbourhood; the ability of their local schools to incorporate physical education into their curriculums based on their resources; and the availability of local community recreation centres with free activities, while explicitly acknowledging that a difference in political and societal empowerment exists. We need to recognize that if race is a socially defined construct, then racial inequities must be socially defined as well and are, consequently, socially actionable.
4.3 Measures Reflective of Context
So if current stratification variables do not represent the all-important societal context, what are examples of variables that could? Income level, possibly the single most commonly used stratification variable in social epidemiology in one form or another, does not accurately capture the underlying causes of health inequities by social class, in part because income levels themselves are the end result, not the cause, of larger societal processes that also contribute to health inequities. However, depending on the research question and specific context, there are many other variables that are directly reflective of underlying processes that researchers could consider. If the association between income and detrimental dietary practices are being questioned, exploration of access (both geographical and financial) to healthy and high-quality foods and the processes by which there might be systematic exclusion or diminished access to such health promoting resources becomes necessary. It is well documented that many foods available in high-income neighbourhoods tend to be of better quality, healthier and cheaper (Cummins and Macintyre 2002; Glazier et al. 2007; James 2009; Krieger et al. 1997). If the relationship between socioeconomic status and chronic stress is being studied, the ability to participate in the same recreational and family activities to which those of higher socioeconomic position are privy to becomes an important factor to measure (Krieger et al. 1997).
Race and ethnicity are also commonly used stratification variables in the social epidemiology literature, and many large and persistent health inequities based on race and/or ethnicity have been unearthed as a result. However, in addition to measuring race or ethnicity, at a minimum, epidemiologists should measure experiences of discrimination. As we have discussed above, the use of race/ethnicity in epidemiologic studies can be problematic, in part because it is routinely the inequitable race relations to which one is subjected to due to race that are the cause of inequalities and not one’s race itself (Krieger 2003; Krieger et al. 1993; Wright 2008). For example, high blood pressure has been found to be associated with one’s perceived and culturally ascribed color but not with one’s measured skin pigmentation (Gravlee 2009), suggesting that it is one’s place in the social hierarchy, as determined by the dominant group, that matters and not the geographic location from which one’s ancestors originate. Although both attitudinal and institutionalized discrimination are important to acknowledge and measure, and although most people think first of attitudinal discrimination when they think of racism, discrimination and prejudice, we recommend a particular emphasis on the latter.
In the section above, we discussed the importance of power relations, many of which negatively impact racialized groups. The concept of institutionalized or structural discrimination is closely related and consists of systems in which public policies, institutional practices and/or societal norms interact to actively maintain inequities (Putnam and Galea 2008; Randall 2006). Instances of institutionalized discrimination are numerous, some of which have been mentioned before, and include: the under-representation of minorities in the health professions; the disproportionate marketing of tobacco and alcohol to racial minorities; name-based discrimination in the workforce; active maintenance of segregation from education and employment opportunities and from safe, healthy environments; and health care systems that are structured to disadvantage particular marginalized groups (O’Campo 2007; Randall 2006). This discrimination has far-reaching repercussions. For instance, discrimination in housing and lending markets leads to segregated neighbourhoods (Farley et al. 1993). These neighbourhoods, specifically those neighbourhoods in which disempowered groups live, are often subject to under-resourced schools and an inability to provide an adequate education to their students, limited employment opportunities, particularly for males, and a subsequent shift to illicit forms of earning money as other viable options rapidly disappear (Krieger 2000; Putnam and Galea 2008). Similarly, inability to access high quality, culturally competent medical care because of structural discrimination within the health care system can lead to a long-term deterioration in health for socially excluded groups (James 2009). The concept of cultural safety in health care, which recognizes that it is a group’s position within society that is most relevant as opposed to the specific things members think or do, and that every health care interaction is influenced both by the cultural mindset of the provider and by the cultural context in which it occurs, is a direct response to this discrimination within the health system (Polaschek 1998).
We have emphasized the measurement of institutionalized discrimination because it has implications over and above any particular individual (Gravlee 2009; Krieger 2003) and, inevitably, also involves recognizing the contextual factors that actively maintain oppression based on race and/or ethnicity. As a result, it has the potential to lend itself more easily to movement into solution-focused research than does exclusively focusing on attitudinal discrimination; the former means acknowledging that we are all either active or passive participants, and the latter suggests that some mysterious and distant “they” are racists (Randall 2006). Therefore, we re-emphasize that the focus of social epidemiologists should be on measures of institutionalized discrimination that more readily lend themselves to action and toward targeted interventions. For example, as a direct result of a research report by Germany’s Institute for the Study of Labor, which found that otherwise equivalent applications with German-sounding names had a 14% greater chance of landing an interview than those with foreign-sounding names, five major corporations agreed in 2010 to participate in a 1-year pilot project where personal information is removed before job applications are processed (Donath 2010). By using an actionable measure of institutionalized discrimination, instead of simply measuring employment based on ethnicity, the authors were able to directly affect an intervention targeted at some of the processes that underlie differences in employment based on ethnicity.
Importantly, whereas attitudinal prejudices are usually relatively easy to discern, institutionalized discrimination may not always be perceived by those toward whom it is targeted or, indeed, by those who are perpetuating it (Green and Darity 2010; Krieger 2003; Randall 2006). For instance, employers may not be aware of their name-based biases, and potential employees may not be aware that they are being passed over for interviews because of their perceived ethnicity. However, the effects are just as damaging, regardless of perception. Therefore, in studies where perceived discrimination has not been found to have a significant effect on health outcomes, but where health inequities still remain partially unexplained (Albert et al. 2010; Barnes et al. 2008), actionable processes of institutionalized discrimination should be strongly considered.
5 Heterogeneity
Our third and final recommendation is for researchers to address meaningful sources of heterogeneity within socially defined groups as a further method to elucidate underlying mechanisms of health inequalities. Socially defined groups, although so categorized because of some common characteristic, are not homogeneous and consist of many subpopulations with differing cultural, historical and societal experiences (Ruffin 2010). The sources of this experiential heterogeneity within any particular marginalized population become crucial to explore in a researcher’s quest for moving toward solution-focused research. By investigating heterogeneity, we may discover important but more subtle inequities that can further hone in on whom action and intervention are most needed, help to further demystify the root causes of the inequities and subsequently facilitate the movement toward action (Kramer and Hogue 2009; Krieger 1992; Krieger et al. 1993, 1997; O’Campo et al. 2004; Wallace 2008).
5.1 Heterogeneity Within Common Socially Defined Groups
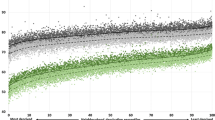
Two examples illustrate the importance of exploring heterogeneity within socially defined groups as well as of defining a meaningful referent group. A routine practice in epidemiology is to examine health outcomes by race or socioeconomic position such as those presented for low birthweight by race and education in Fig. 5.1. When examined separately, we see a familiar pattern of non-White and less educated individuals having the worst outcomes. Yet, when we combine race and education, as is shown in Fig. 5.2, we see the heterogeneity within and between races more clearly. We see just how much improvement is required across all races in order to bring all groups up to the standard of health experienced by the most privileged subgroup, namely White women with more than a high school education.

Low birthweight by race and education separately, based on vital records data for a U.S. state

Low birthweight by race and education together
As a second example, Bleich et al. (2010) found that the well-known racial disparities in obesity among women in the United States, where African American women are significantly more likely to be obese, do not exist among poor, urban women subject to the same social context. Among these women, race had no significant bearing on obesity rates. These findings suggest that policies to target the obesity disparity should focus on social aspects of the environment around a woman, such as availability of healthy yet affordable foods and availability of an environment that promotes safe and regular physical activity as mentioned above, instead of focus on trying to change the cultural dietary choices of that woman. They also suggest that policies to fight obesity should not exclude non-African American women. However, without examining both race and social class and without identifying a meaningful referent group, the researchers would likely have produced misguided and erroneous recommendations for addressing the obesity problem.
These examples demonstrate an important point to remember. Variables that lead to heterogeneity within marginalized groups may not only act independently, they may also be variables that act synergistically. There are individuals who are simultaneously members of several marginalized groups, and the oppression that they experience as a result is more than additive (Krieger 2000; Krieger et al. 1993; Randall 2006). Author Vernellia Randall (2006) has described the impact of the intersection of race and gender in the United States with the phrase “all women are white, all blacks are men” to illustrate how African American women are often excluded from both gender and racial issues. Neglecting the potential synergistic effects of socially defined characteristics for an individual or group is unacceptable when we are concerned with targeting the social determinants of health. Therefore, social epidemiologists must not only simultaneously examine the effects of multiple variables in their analyses but must also examine their interactions (Wallace 2008). Through an exploration of heterogeneity and use of an appropriate referent group, and bearing in mind the possibility of synergistic effects, we can highlight the most vulnerable subgroups where action is most urgently needed and ensure the best use of resources for ameliorating inequities.
5.2 Heterogeneity Through a Realist Lens
However, it must be stressed that researchers need to be thoughtful on the sources of heterogeneity that they choose to investigate. Again, we need to ensure that we approach heterogeneity with a realist lens. Acknowledgement of heterogeneity within strata is not a new concept, but studies usually focus on individual-level factors that may serve as a source of distraction if used in isolation and rarely concurrently investigate the solution-focused variables responsible for the heterogeneity. When we explore the heterogeneity within disadvantaged groups, we must continue to address the contextual and societal factors that could be the basis of action to reduce inequities. For example, differential access to, eligibility for and participation in the financial arena (e.g., home ownership, ability to get credit) and various social services may explain differences in health or well-being among low-income populations in a more meaningful way than only sub-categorizing by race or ethnicity and in a way that guides us toward underlying mechanisms for heterogeneity within groups (Krieger 2000; Krieger et al. 1997; Manly 2006). Gender differences within an income stratum might be better explained by also exploring differences based on childcare responsibilities and age and number of family members in the household (Krieger et al. 1993, 1997). Underlying mechanisms such as unequal access to political power, lack of accommodation for child-rearing responsibilities within the work force and the need to distribute the same amount of income over multiple household members need to be addressed (O’Campo et al. 2004). Within any particular racialized or ethnic group, important differences in experiences may exist based on level of acceptance by the privileged group, perceived threat by the privileged group, exposure to segregation, exposure to quality education and employment opportunities (Krieger 2003; Manly 2006). For example, babies born to African-born Black women have been found to have identical distributions of birth weight as babies born to American-born White women and higher than that of babies born to American-born Black women. Within one generation, this advantage disappears (Gravlee 2009). If we want to explore the underlying causes for these differences, is birthplace the only appropriate source of heterogeneity to target? Or should we also consider potential underlying mechanisms such as social supports, feelings around sense of self, sense of empowerment and chronic exposure to discrimination, segregation and stress? Tellingly, African American neonatal mortality has been independently associated with less relative political power (Krieger 2000).
A related example illustrates how the investigation of heterogeneity can directly inform evidence-based intervention. With the knowledge that infant mortality and low birth weight are more common in non-White ethnic groups, Norbeck et al. (1996) examined the effects of high stress, low social supports and high anxiety as sources of heterogeneity on pregnancy outcomes for African American, Hispanic and White women. The authors found that low social support from the woman’s partner or mother was of especial importance for birth complications for African American women only. As a result of their findings, the authors created a social support intervention aimed at preventing low birth weight among African American women with known low social support. The intervention was designed to provide the support usually provided by mothers or partners and was effective in reducing the rate of low birth weight. By exploring actionable sources of heterogeneity within racial groups and not stopping at simply describing the differences in pregnancy outcomes by racial group, the authors were able to create an effective intervention targeted at an underlying mechanism for an observed inequity.
6 Conclusion
Epidemiologists may be hesitant to approach stratification in the way we have suggested for fear of appearing as advocates instead of scientists or for fear of appearing to lack subjectivity (Krieger 2003). Yet, it is advocacy groups, not academics, who have traditionally been most likely to propose solutions to health inequities (Kim et al. 2010). As well, the changes we propose to the approach to stratification may be difficult for peer reviewers and editors to accept (Syme 2008). However, the development of strong theoretical frameworks to guide the research may help to assuage some of these fears. Researchers should also consider, however, that a conscious choice to not acknowledge the underlying mechanisms that lead to health inequities is in itself a political decision based on implicit assumptions about the root cause of inequities (see Chap. 3). Finally, though reviewers and editors may be reticent to accept these changes, we suspect that interested policy makers will appreciate the advent of measures that will be directly transferable to action.
References
Albert MA, Cozier Y, Ridker PM et al (2010) Perceptions of race/ethnic discrimination in relation to mortality among Black women: results from the Black Women’s Health Study. Arch Intern Med 170:896–904
American Anthropological Association (1998) Statement on “race”. http://www.aaanet.org/stmts/racepp.htm. Accessed 25 Mar 2011
Barnes LL, de Leon CF, Lewis TT et al (2008) Perceived discrimination and mortality in a population-based study of older adults. Am J Public Health 98:1241–1247
Berkman LF (2009) Social epidemiology: Social determinants of health in the United States: are we losing ground? Annu Rev Public Health 30:27–41
Bleich SN, Thorpe RJ, Sharif-Harris H et al (2010) Social context explains race disparities in obesity among women. J Epidemiol Community Health 64:465–469
Coburn D (2004) Beyond the income inequality hypothesis: class, neo-liberalism, and health inequalities. Soc Sci Med 58:41–56
Cooper R, Kaufman J, Ward R (2003) Race and genomics. N Engl J Med 348:1166–1170
Cummins S, Macintyre S (2002) A systematic study of an urban foodscape: the price and availability of food in greater Glasgow. J Urban Stud 39:2115–2130
David R, Collins J (2007) Disparities in infant mortality: what’s genetics got to do with it? Am J Public Health 97:1191–1197
Donath J (2010) Anonymous job applications: German pilot project aims to reduce discrimination. Spiegel Online International. http://www.spiegel.de/international/business/0,1518,713711,00.html. Accessed 30 Dec 2010
Elmore JL (2002) Fluoxetine-association remission of ego-dystonic male homosexuality. Sex Disabil 20:149–151
Engel G (2002) The need for a new medical model – a challenge for biomedicine. In: Marks D (ed) The health psychology reader. Sage, London
Farley R, Steeh C, Jackson T et al (1993) Continued racial residential segregation in Detroit: “Chocolate city, vanilla suburbs” revisited. J Hous Res 4:1–38
Fujishiro K (2009) Is perceived racial privilege associated with health? Findings from the Behavioral Risk Factor Surveillance System. Soc Sci Med 68:840–844
Glazier R, Booth G, Gozdyra P et al (2007) Neighbourhood environments and resources for healthy living – a focus on diabetes in Toronto: ICES Atlas. Institute for Clinical Evaluative Sciences, Toronto
Gravlee CC (2009) How race becomes biology: embodiment of social inequality. Am J Phys Anthropol 139:47–57
Green TL, Darity WA Jr (2010) Under the skin: using theories from biology and the social sciences to explore the mechanisms behind the black-white health gap. Am J Public Health 100:S36–S40
Gunaratnam Y (2003) Researching race and ethnicity: methods, knowledge and power. Sage, London
Hallal PC, Azevedo MR, Reichert FF et al (2005) Who, when, and how much? Epidemiology of walking in a middle-income country. Am J Prev Med 28:156–161
Hofrichter R (2006) Tackling health inequities through public health practice: a handbook for action. The National Association of County and City Health Officials, Washington, DC
James SA (2009) Epidemiologic research on health disparities: some thoughts on history and current developments. Epidemiol Rev 31:1–6
Kim AE, Kumanyika S, Shive D et al (2010) Coverage and framing of racial and ethnic health disparities in US newspapers, 1996–2005. Am J Public Health 100:S224–S231
Kramer MR, Hogue CR (2009) Is segregation bad for your health? Epidemiol Rev 31:178–194
Krieger N (1992) The making of public health data: paradigms, politics, and policy. J Public Health Policy 13:412–427
Krieger N (2000) Discrimination and health. In: Berkman LF, Kawachi I (eds) Social epidemiology. Oxford University Press, Oxford
Krieger N (2001) Theories for social epidemiology in the 21st century: an ecosocial perspective. Int J Epidemiol 30:668–677
Krieger N (2003) Does racism harm health? Did child abuse exist before 1962? On explicit questions, critical science, and current controversies: an ecosocial perspective. Am J Public Health 93:194–199
Krieger N, Rowley DL, Herman AA et al (1993) Racism, sexism, and social class: implications for studies of health, disease, and well-being. Am J Prev Med 9:82–122
Krieger N, Williams DR, Moss NE (1997) Measuring social class in US public health research: concepts, methodologies, and guidelines. Annu Rev Public Health 18:341–378
Lamont M (2009) Responses to racism, health, and social inclusion as a dimension of successful societies. In: Hall PA, Lamont M (eds) Successful societies: how institutions and culture affect health. Cambridge University Press, New York
Love C, David RJ, Rankin KM et al (2010) Exploring weathering: effects of lifelong economic environment and maternal age on low birth weight, small for gestational age, and pre-term birth in African-American and white women. Am J Epidemiol 172:127–134
Manly JJ (2006) Deconstructing race and ethnicity: implications for measurement of health outcomes. Med Care 44:S10–S16
McMurray RG, Harrell JS, Deng S et al (2000) The influence of physical activity, socioeconomic status, and ethnicity on the weight status of adolescents. Obes Res 8:130–139
Muntaner C, Nieto J, O’Campo P (1996) The bell curve: on race, social class, and epidemiologic research. Am J Epidemiol 144:531–536
Muntaner C, Borell C, Ng E et al (2011) Politics, welfare regimes, and population health: controversies and evidence. Sociology of Health & Illness 33(6):946–964
Norbeck JS, DeJoseph JF, Smith RT (1996) A randomized trial of an empirically-derived social support intervention to prevent low birthweight among African American women. Soc Sci Med 43:947–954
O’Campo P (2007) Equity and Distributive Justice. Background paper prepared for the 10th International Medical Workforce Conference, Vancouver, Canada 2006
O’Campo P, Burke J (2004) Recommendations on the use of socioeconomic position indicators to better understand racial inequalities in health. In: Ver Ploeg M, Perrin E (eds) Eliminating health disparities: measurement and data needs. National Academies Press, Washington, DC
O’Campo P, Eaton W, Muntaner C (2004) Labor market experience, work organization, gender inequalities and health status: results from a prospective analysis of US employed women. Soc Sci Med 58:585–594
Perry M (1996) The relationship between social class and mental disorder. J Prim Prev 17:17–30
Polaschek NR (1998) Cultural safety: a new concept in nursing people of different ethnicities. J Adv Nurs 27:452–457
Putnam S, Galea S (2008) Epidemiology and the macrosocial determinants of health. J Public Health Policy 29:275–289
Randall V (2006) Dying while Black: an indepth look at a crisis the American healthcare system. Seven Principles Press, Dayton
Roman CV (2010) Fifty years’ progress of the American Negro in health and sanitation. Am J Public Health 100:S66–S68
Ruffin J (2010) The science of eliminating health disparities: embracing a new paradigm. Am J Public Health 100:S8–S9
Sayer A (1992) Method in social science: a realist approach, 2nd edn. Routledge, London
Shankardass K, Solar O, Murphy K et al (2010a) Health in all policies: a snapshot for Ontario. Results of a realist-informed scoping review of the literature. In: Getting started with Health in All Policies: a resource pack. Report to the Ministry of Health and Long-Term Care (Ontario). Centre for Research on Inner City Health, St. Michael’s Hospital, Toronto. http://www.stmichaelshospital.com/knowledgeinstitute/search/details.php?id=18218&page=1. Accessed 12 May 2011
Shim J (2002) Understanding the routinised inclusion of race, socioeconomic status and sex in epidemiology: the utility of concepts from technosicence studies. Sociol Health Illn 24:129–150
Singh-Manoux A, Ferrie J, Chandola T et al (2004) Socioeconomic trajectories across the life course and health outcomes in midlife: evidence for the accumulation hypothesis? Int J Epidemiol 33:1072–1079
Smith GD, Hart C, Blane D et al (1997) Lifetime socioeconomic position and mortality: prospective observational study. Br Med J 314:547–552
Stallones R (1980) To advance epidemiology. Ann Rev Public Health 1:69–82
Stanfield J, Dennis R (1993) Race and ethnicity in research methods. Sage, Newbury Park
Statistics Canada (2009) Visible minority population and population group reference guide, 2006 Census. Catalogue no. 97-562-GWE2006003. http://www12.statcan.gc.ca/census-recensement/2006/ref/rp-guides/visible_minority-minorites_visibles-eng.cfm. Accessed 25 Mar 2011
Susser M (1985) Epidemiology in the United States after World War II: the evolution of technique. Epidemiol Rev 7:147–177
Syme L (2008) Reducing racial and social-class inequalities in health: the need for a new approach. Heal Aff 27:456–459
U.S. Department of Energy, Office of Science (2003) Exploring genetics issues relevant to minority communities. http://www.ornl.gov/hgmis/elsi/minorities.html. Accessed 25 Mar 2011
Wallace B (2008) Toward equity in health: a new global approach to health disparities. Springer, New York
Werbner P (2003) A “treacherous bind”: working with and against racial categories. In: Gunaratnam Y (ed) Researching race and ethnicity: methods, knowledge and power. Sage, London
Wright E (2008) Logics of class analysis. In: Lareau A, Conley D (eds) Social class: how does it work? Russell Sage, New York
Zucker KJ, Spitzer RL (2005) Was the gender identity disorder of childhood diagnosis introduced into DSM-III as a backdoor maneuver to replace homosexuality? A historical note. J Sex Marital Ther 31:31–42
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2012 Springer Science+Business Media B.V.
About this chapter
Cite this chapter
Lofters, A., O’Campo, P. (2012). Differences That Matter. In: O’Campo, P., Dunn, J. (eds) Rethinking Social Epidemiology. Springer, Dordrecht. https://doi.org/10.1007/978-94-007-2138-8_5
Download citation
DOI: https://doi.org/10.1007/978-94-007-2138-8_5
Published:
Publisher Name: Springer, Dordrecht
Print ISBN: 978-94-007-2137-1
Online ISBN: 978-94-007-2138-8
eBook Packages: Biomedical and Life SciencesBiomedical and Life Sciences (R0)