
Abstract
Glioblastoma multiforme (GBM) is the most common adult malignant brain tumor and is comprised of a heterogeneous population of cells. Despite advanced surgical and medical therapies, the 2-year survival rate for patients with GBM remain only 10–25%. Recently, increasing evidence suggest that the progression of GBM is driven by a small subpopulation of tumor cells, termed cancer stem cells. These cancer stem cells have capability of self-renewal, proliferation, and differentiation into the phenotypically diverse populations of cells similar to those present in the original GBM. Furthermore, these cancer stem cells are able to form tumors and generate both neuron-like and glial-like progenies after implantation into the brains of SCID mice. Here, we summarize the methods of isolating cancer stem cells from GMB, and discuss the implications of the cancer stem cell hypothesis for understanding the origin and growth of GBM and development of new therapeutic strategies for the treatment of brain tumors.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
Introduction
Glioblastoma multiforme (GBM) is typically comprised of morphologically diverse cells within the tumor mass. Despite current advances in therapy, the morbidity and mortality of GBM remain very high with a 2-year survival rate of only 10–25% (Stupp et al., 2005). This is due, at least in part, to the focus of most treatments on the tumor mass. However, the diverse cells within GBM may play different roles in tumorogenesis. There is increasing evidence that cancers might contain and arise from stem cells. Studies on leukemia and breast carcinoma have demonstrated that a small group of cells within the tumor mass is responsible for tumor formation and maintenance. This subpopulation of stem-like cells plays an important role in the tumorogenic process (Lapidot et al., 1994). GBMs contain cells that express neural markers as well as cells that express glial markers, indicating that there may be multipotent neural stem cell like cells (Ignatova et al., 2002).
The cell origin of glioblastomas may develop from neural stem cells (NSCs) or from differentiated cell types that acquired multipotential stem cell-like properties by either reprogramming or de-differentiating in response to oncogenic mutation (Bachoo et al., 2002; Kondo and Raff, 2000). This plasticity of central nervous system (CNS) cells has already been reported as normal oligodendrocyte precursor cells can be induced to acquire stem cell-like properties (Kondo and Raff, 2000; Nunes et al., 2003). Recent evidence suggests that brain tumors contain small numbers of cells with neural stem cell properties. These cells may be important for the malignancy (Galli et al., 2004; Hemmati et al., 2003; Singh et al., 2003, 2004; Yuan et al., 2004). To clarify the concept, Dirks and others have established a functional definition of brain cancer stem cells (Dirks, 2008; Vescovi et al., 2006). First, brain cancer stem cells should be highly proliferative, multipotent, and capable of self-renewal. Second, a brain cancer stem cells should be tumorigenic; that is, capable of giving rise to a histologically appropriate tumor following transplantation into an SCID mouse brain. Last, brain cancer stem cells should give rise to a tumor that is capable of propagation, whether by dissociation and cell culture of the transplanted tumor mass, or by serial transplantation into an immunocompromised host.
For the past several years in our laboratory, we have demonstrated that a subpopulation of cells exist within adult GBM (Yuan et al., 2004). We have also successful isolated tumor stem-like cells from benign brain tumors, including pituitary adenomas (Xu et al., 2009). These cells may represent a general source of cancer stem cells in adult brain tumor and need to be targeted for more effective and specific cancer therapy. Here, we discuss the procedures of isolation and characterization of cancer stem cells from brain tumors, highlight some of the central questions that remain to be answered and potential strategies for the development of cancer stem cells specific therapies.
Primary Culture of Glioblastoma Cells and Spheres
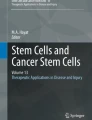
Tumor specimens from GBM patients were collected within 30 min after the surgical resection. Under a biohazard hood, tumor tissues were washed three times with PBS to eliminate blood eventually present. The tissue was then transferred onto a new culture dish and dissected in a dissection medium containing catalase, deferoxamine, N-acetyl cysteine, and superoxide dismutase using sterile scissors and forceps. The dissected tissue was then centrifuged to remove supernatant. After digestion in trypsin, tumor tissues were triturated by passing them in a tissue sieve, the cell suspension was recovered by passing a 70 mm cell strainer. Tumor cells were suspended in DMEM/F12 medium containing 10% fetal bovine serum (FBS) as growth medium and plated at 2×106 cells per 75 cm2 flasks. The cells attached and grew as a monolayer in flasks. After growing for 24–48 h, the monolayer-growing tumor cells were switched into a defined serum free neural stem cell medium (Yuan et al., 2004), containing DMEM/F12, EGF (20 ng/ml), and bFGF (20 ng/ml), B27, penicillin/streptomycin (200 U/ml), fungizone (250 ng/ml). Neurosphere-like colonies appeared in the cultures after 1–2 weeks and formed floating spheres after continuing culture (Fig. 14.1a).

Primary cultures of adult GBM form glioblastoma spheres that can self-renew. (a) Primary neurosphere-like colony, glioblastoma sphere, developing from monolayer tumor cells. Scale bar = 50 μm. (b) Subsphere derived from a single cell of primary sphere. Scale bar = 50 μm
Neurosphere-Forming Assay for Glioblastoma Cells
After primary spheres formed and reached about 50–200 cells per sphere in the culture, the sphere cells were harvested, dissociated into single cells and plated into a 96-well plate for the subsphere-forming assay by limiting dilution (Kabos et al., 2002; Yuan et al., 2004). The cells in single-cell suspension were diluted and plated at 1–2 cells/well. In parallel, the monolayer cell remaining in the flasks after harvesting of the spheres was also plated. Cells were fed by changing half of the medium every 2 days. After plating, the cells were observed and only wells containing a single cell were considered. The wells were scored for sphere formation after 14 days. Subspheres can form in the wells seeded with individual sphere cells with efficiency between 1 and 10% varying among different tumor samples (Fig. 14.1b). However, sphere formation will be not evident in the wells seeded with monolayer cells. When compared with normal human NSCs that were grown with the similar passage number, there were usually <1% cells with subsphere-forming ability. This observation indicates that the glioblastoma spheres have a self-renewing ability. This ability can be confirmed by harvesting the subspheres and performing further rounds subsphere-forming assay. The efficiency of subsphere formation is usually maintained.
Glioblastoma Spheres Express NSC Markers as Well as Lineage Markers
The self-renewal capability of glioblastoma spheres indicates that sphere cells isolated from GBM primary cultures share this property with the NSC. To investigate whether the glioblastoma spheres could express genes characteristic of NSC, spheres derived from a single mother cell and isolated by subsphere-forming assay were dissociated and expanded following by gene expression analysis. For staining the primary cultured tumor cells and differentiated glioblastoma sphere or normal neurosphere, the cells growing in precoated chamber slides were fixed with 2% paraformaldehyde for 15 min at room temperature, treated with 1% donkey serum, and then stained with the following primary antibodies: anti-CD133, anti-nestin, anti-β-tubulinIII, anti-GFAP, and anti-myelin/oligodendrocyte. The primary antibodies were detected with Tex-Red or FITC-conjugated secondary antibodies. The cells were counterstained with 4, 6-diamidino-2-phenylindole (DAPI) to identify all nuclei. For immunostaining of glioblastoma spheres, the spheres or dissociated sphere cells were freely floated in “U”-bottom wells of a 96-well plate during the staining process. Then, the cells were resuspended into the mounting medium containing DAPI and mounted on microslides. Quantification of cells positive for a specific marker was carried out by counting all the stained cells within 20 randomly selected microscope fields per specimen, and the percentage was calculated based on the total number of nuclei counted. Two NSC markers were chosen to characterize the expanded spheres: CD133, a cell surface marker of normal human NSCs; and nestin, a cytoskeletal protein associated with NSCs and progenitor cells in the developing CNS. For all GBMs studied, daughter spheres derived from one mother cell were positive for both CD133 and nestin (Fig. 14.2). Several lineage markers were also chosen for clarifying the characteristics of the spheres: anti-β-tubulinIII is a neuronal marker; anti-GFAP is an astocyte marker, and anti-myelin/ oligodendrocyte is an oligodendrocyte marker. Some cells within tumor spheres were also found to be positive for lineage markers β-tubulinIII and myelin/oligodendrocyte. The cells in non-sphereforming monolayer cultures predominantly expressed the three lineage markers of CNS, β-tubulinIII (30–50%), GFAP (10–25%), and myelin/oligodendrocyte (20–40%). The pattern was clearly different from that of the glioblastoma sphere with 5–15% for β-tubulinIII, 1–5% for GFAP, and 10–20% for myelin/oligodendrocyte. The observed phenotypic variation of stained cells within spheres from one mother cell indicates that the mother cells have the potential to produce the terminal cell types specific to the tumor tissue.

Single-mother-cell-derived glioblastoma spheres express NSC markers. Glioblastoma spheres derived from a single mother cell were stained by NSC markers CD133 (red) and Nestin (green). Cells were located by counterstaining with DAPI (blue). Scale bar = 50 μm
Differentiation Assay of Glioblastoma Spheres
To test whether glioblastoma spheres derived from one mother cell have multipotent ability and produce progenies of different lineages, the spheres were subjected to a differentiation assay. Glioblastoma sphere derived from one mother cell in the subsphere-forming assay was trypsinized into single-cell suspension and seeded into chamber slides for differentiation assay. The cells were grown in medium devoid of growth factors but permissive for differentiation for 14 days, and processed for immunocytochemistry staining for various lineage markers. The results demonstrate that glioblastoma spheres were predominantly differentiated into b-tubulinIII (80%), myelin/oligodendrocyte (25%) and GFAP (10%)-positive cells that recapitulated the parental tumor phenotype. In contrast, the phenotype pattern was different from that of normal human NSC, which was cultured for the same period of time as that of glioblastoma spheres. The differentiated progeny of normal NSCs was characterized with 50–60% GFAP-positive cells, 20–30% β-tubulinIII-positive cells, myelin/oligodendrocyte-positive cells accounting for 10%, and less than 5% cells positive for CD133 or nestin, respectively. These results reveal that glioblastoma spheres are multipotent for the three neural cell types, but different from normal human neurospheres regarding the phenotype of their progenies.
Distinctions Between Glioblastoma Spheres and Normal Neurospheres
To further determine that glioblastoma spheres are cancer stem cells and not derived from contaminating normal NSC, we conducted a differentiation experiment for both glioblastoma spheres and normal human neurospheres by dissociating individual spheres into a single-cell suspension and subjecting the cells to differentiation conditions. After 2 weeks of differentiation, all cells were attached and growing as a monolayer. Cells were then switched into NSC growth medium. New spheres started to form in the GBM differentiated monolayers after 1 week and were positive for nestin and CD133. No spheres were observed in the normal human neurosphere-differentiated monolayer even after 4 weeks.
We also did karyotype analysis of the glioblastoma sphere cells as compared to normal human neurospheres. The spectral karyotype analysis identified chromosome loss, gain, and translocation events in glioblastoma sphere cells, but not in normal human neurospheres (Yuan et al., 2004). Taken together, both cellular analysis and genetic data support the hypothesis that glioblastoma spheres isolated from primary GBM cultures are not normal NSCs migrated into the tumor mass. Rather, these glioblastoma spheres possess abnormal characteristics including enhanced self-renewal and altered differentiation abilities, which may be responsible for maintaining the tumor stem cell pool and also for generating the differentiated progeny.
Glioblastoma Spheres are Capable of Forming Tumors into the Brains of SCID Mice
To address whether glioblastoma spheres and nonsphere-forming monolayer cells differ in their abilities to form tumor in vivo, the isolated glioblastoma spheres or non-sphere-forming monolayer cells were implanted into the brains of the SCID mice. The implanted mice were killed after 6 weeks to 6 months, and then the brains were harvested and examined for tumors on the brain sections after hematoxylin–eosin staining. There was no tumor detected in the brains after implantation of non-sphere-forming monolayer cells. However, all the mice developed brain tumors after implanting with the same number of glioblastoma sphere cells. The tumors, which developed in mice brains after implantation of human glioblastoma spheres, were stained positively by human-specific antibodies against nestin and CD133 (Fig. 14.3), the NSC related markers. Also, the tumor cells were stained positive for anti-GFAP, anti-myelin/oligodendrocyte, and anti-β-tubulinIII, suggesting that the implanted glioblastoma spheres can generate both glial cells and neurons in vivo. Thus, the malignance of the human adult GBM apparently depends on the insolated glioblastoma spheres, the cancer stem cells.

The isolated glioblastoma spheres were able to form brain tumors in nude mice after intracranial implantations. The tumors developed in the mice brain could be stained with human-specific antibodies against NSC markers, nestin (a, b) and CD133 (d–f). The sections were labeled also with DAPI (blue) to identify nuclei (c, e). The merged images were also shown (f). Scale bar = 1000 μm (a–c); Scale bar = 250 μm (d–f)
Relationship Between Neural Stem Cells and Cancer Stem Cells
Stem cells are functionally defined as self-renewing, multipotent cells that exhibit multilineage differentiation (Weissman, 2000). Over the past decade, several groups have succeeded in isolating NSCs from various regions of the adult human brain, including the anterior subventricular zone (SVZ) (Sanai et al., 2004) and the subgranular zone (SGZ) of the dentate gyrus (Roy et al., 2000). These stem cells in the adult SVZ and SGZ reside in tightly controlled environments, known as niches, which maintain the complement of stem cells and regulate stem cell proliferation and differentiation (Quinones-Hinojosa et al., 2007). In addition, it is thought that the niche can adapt to the brain’s need for new cells in the conditions of brain injury (Thored et al., 2006) or neurodegenerative diseases, such as Parkinson’s disease (Hoglinger et al., 2004) and amyotrophic lateral sclerosis (Liu and Martin, 2006).
The application of principles used for studying the NSCs to tumor biology indicates a link between normal neurogenesis and brain tumorigenesis (Holland et al., 2000; Kabos et al., 2002). The concept of cancer stem cells arose from the observation of striking similarities between stem cells and cancer cells, including the self-renewal mechanisms, activation of DNA repair mechanisms, and expression of drug transporters (Pardal et al., 2003). Normal somatic stem cells must self-renew and maintain a relative balance between self-renewal and differentiation, cancer can be contextualized as a disease of unregulated self-renewal (Reya et al., 2001). The presence of cancer stem cells in both primary GBMs and medulloblastomas was initially reported independently by several groups (Al-Hajj et al., 2003; Galli et al., 2004; Singh et al., 2004; Yuan et al., 2004) with different approaches for isolating these cells. Galli et al. and our group isolated cancer stem cells from adult human GBMs based on neurospheres assay (Galli et al., 2004; Yuan et al., 2004). The neurospheres were detected in all cultures established from GBMs from both groups. Sphere-forming frequency was between 0.5 and 31% of the total cells plated for GBM in Galli’s group, as compared to that of 1–10% in our group. The GBM cells were not only capable of self-renewal, but were also multipotent, and tumorigenic. Tumors derived from transplantation of these cells into SCID mice recapitulated the histopathological phenotype of the parent tumors. Singh et al. isolated a subpopulation of cells from human GBMs and medulloblastomas by use of cell sorting technique based on selection for the cell surface marker CD133, a transmembrane glycoprotein found on numerous adult stem cell populations, including those in the adult human brain (Singh et al., 2004). In culture, this subpopulation of cells demonstrated properties of NSCs, including sphere-forming capability, self-renewal, and multipotentiality. The CD133+ cell content ranged from 19 to 29% among GBMs and from 6 to 21% among medulloblastomas. Implantation of 100 CD133+ cells into SCID mice produced a tumor that could be serially transplanted, whereas injection of 1×105 CD133– cells produced engraftment but not tumor progression. The tumors arising from CD133+ cells recapitulated the histopathological phenotype of the parent tumors, suggesting that the CD133+ subpopulation is capable of giving rise to the full heterogeneous complement of cells present in the tumor. However, Beier et al. reported that CD133 expression does not always appear to mark the cancer stem cells in gliomas (Beier et al., 2007). Indeed, glioblastomas could be propagated from CD133– cells, although these cells were cultured as adherent spheres and cell lines before transplantation. In this study, CD133– cells were similarly tumorigenic to CD133+ cells in nude mice, although CD133– tumour cells appeared to have a distinct molecular profile (Beier et al., 2007). Up to now, there is no appropriate marker for isolating cancer stem cells, especially for distinguishing cancer stem cells from NSCs. It is a fundamental step to identify and isolate cancer stem cells, so that elucidating the pathways that account for tumorigenic potential and developing effective and specific anticancer strategy may be realized.
Recently, several studies reported isolation of cancer stem cells from human glioblastoma cell lines (Fukaya et al., 2009; Qiang et al., 2009) and rat glioma cell lines (Kondo et al., 2004). These cells possess the properties of cancer stem cells, and may be useful for analyzing molecular and functional characteristics of cancer stem cells because of the ease of handling and their high yield.
Therapeutic Implications of Brain Cancer Stem Cells
Cancer stem cells have been implicated in brain tumor initiation, progression and recurrence. It was reported that CD133+ cells was significantly elevated in recurrent gliomas compared with newly diagnosed gliomas in the same patients. These CD133+ cells were more resistant than other tumor cells to treatment with a panel of chemotherapeutics, suggesting that their role in tumor recurrence is likely to be mediated by their relative resistance to chemotherapy (Liu et al., 2006). Increased expression of ATP-binding cassette transporters, including ABCG2 and ABCG5, is one of the possible mechanism underlying chemoresistance of cancer stem cells (Dean et al., 2005). Interestingly, expression of the drug transporter and chemoresistance mediator ABCB5 correlated with tumor progression.
In addition to chemoresistance, cancer stem cells exhibit enhanced resistance to radiation therapy. Bao et al. reported that cancer stem cells contribute to glioma radioresistance through preferential activation of the DNA damage checkpoint response and an increase in DNA repair capacity (Bao et al., 2006). CD133-expressing tumor cells isolated from both human glioma xenografts and primary patient glioblastoma specimens preferentially activate the DNA damage checkpoint in response to radiation, and repair radiation-induced DNA damage more effectively than CD133-negative tumour cells. In addition, the radioresistance of CD133-positive glioma stem cells can be reversed with a specific inhibitor of the Chk1 and Chk2 checkpoint kinases. Targeting DNA damage checkpoint response in cancer stem cells may overcome this radioresistance and provide a therapeutic model for malignant brain cancers (Bao et al., 2006).
There is increasing interest in exploiting the putative cancer stem cells niche for drug targeting. Cancer stem cells may dictate expansion of the normal niche as they proliferate, which may eventually lead to an altered niche as the cells become independent of normal regulatory signals and produce extrinsic factors that deregulate niche-forming cells. Cancer stem cells from glioblastoma and medulloblastoma appear to be maintained by signals from an aberrant vascular niche that mimics the normal stem cell niche. It was showed that freshly isolated CD133+ enriched cells but not CD133– glioblastoma cells formed highly vascular tumors in the brains of nude mice (Calabrese et al., 2007). Treatment of CD133+ cells with bevacizumab, a vascular endothelial growth factor monoclonal antibody, markedly inhibited their ability to initiate tumors in vivo and depleted both blood vessels and self-renewing CD133+ cells from tumour xenografts (Folkins et al., 2007). These studies suggest that anti-angiogenic therapy in conjunction with cytotoxic chemotherapy may prove effective in targeting cancer stem cells in glioblastomas.
A small subpopulation of radioresistant and chemoresistant cancer stem cells plays an important role in GBM initiation, progression and recurrence. The identification and characterization of these cells, as well as our increased understanding of molecular biology, offer an opportunity for the development of novel therapies for primary brain tumors.
References
Al-Hajj M, Wicha MS, Benito-Hernandez A, Morrison SJ, Clarke MF (2003) Prospective identification of tumorigenic breast cancer cells. Proc Natl Acad Sci USA 100:3983–3988
Bachoo RM, Maher EA, Ligon KL, Sharpless NE, Chan SS, You MJ, Tang Y, DeFrances J, Stover E, Weissleder R, Rowitch DH, Louis DN, DePinho RA (2002) Epidermal growth factor receptor and Ink4a/Arf: convergent mechanisms governing terminal differentiation and transformation along the neural stem cell to astrocyte axis. Cancer Cell 1:269–277
Bao S, Wu Q, McLendon RE, Hao Y, Shi Q, Hjelmeland AB, Dewhirst MW, Bigner DD, Rich JN (2006) Glioma stem cells promote radioresistance by preferential activation of the DNA damage response. Nature 444:756–760
Beier D, Hau P, Proescholdt M, Lohmeier A, Wischhusen J, Oefner PJ, Aigner L, Brawanski A, Bogdahn U, Beier CP (2007) CD133(+) and CD133(–) glioblastoma-derived cancer stem cells show differential growth characteristics and molecular profiles. Cancer Res 67:4010–4015
Calabrese C, Poppleton H, Kocak M, Hogg TL, Fuller C, Hamner B, Oh EY, Gaber MW, Finklestein D, Allen M, Frank A, Bayazitov IT, Zakharenko SS, Gajjar A, Davidoff A, Gilbertson RJ (2007) A perivascular niche for brain tumor stem cells. Cancer Cell 11:69–82
Dean M, Fojo T, Bates S (2005) Tumour stem cells and drug resistance. Nat Rev Cancer 5:275–284
Dirks PB (2008) Brain tumor stem cells: bringing order to the chaos of brain cancer. J Clin Oncol 26:2916–2924
Folkins C, Man S, Xu P, Shaked Y, Hicklin DJ, Kerbel RS (2007) Anticancer therapies combining antiangiogenic and tumor cell cytotoxic effects reduce the tumor stem-like cell fraction in glioma xenograft tumors. Cancer Res 67:3560–3564
Fukaya R, Ohta S, Yamaguchi M, Fujii H, Kawakami Y, Kawase T, Toda M (2009) Isolation of cancer stem-like cells from a side population of a human glioblastoma cell line, SK-MG-1. Cancer Lett 291:150–157
Galli R, Binda E, Orfanelli U, Cipelletti B, Gritti A, De Vitis S, Fiocco R, Foroni C, Dimeco F, Vescovi A (2004) Isolation and characterization of tumorigenic, stem-like neural precursors from human glioblastoma. Cancer Res 64:7011–7021
Hemmati HD, Nakano I, Lazareff JA, Masterman-Smith M, Geschwind DH, Bronner-Fraser M, Kornblum HI (2003) Cancerous stem cells can arise from pediatric brain tumors. Proc Natl Acad Sci USA 100:15178–15183
Hoglinger GU, Rizk P, Muriel MP, Duyckaerts C, Oertel WH, Caille I, Hirsch EC (2004) Dopamine depletion impairs precursor cell proliferation in Parkinson disease. Nat Neurosci 7:726–735
Holland EC, Celestino J, Dai C, Schaefer L, Sawaya RE, Fuller GN (2000) Combined activation of Ras and Akt in neural progenitors induces glioblastoma formation in mice. Nat Genet 25:55–57
Ignatova TN, Kukekov VG, Laywell ED, Suslov ON, Vrionis FD, Steindler DA (2002) Human cortical glial tumors contain neural stem-like cells expressing astroglial and neuronal markers in vitro. Glia 39:193–206
Kabos P, Ehtesham M, Kabosova A, Black KL, Yu JS (2002) Generation of neural progenitor cells from whole adult bone marrow. Exp Neurol 178:288–293
Kondo T, Raff M (2000) Oligodendrocyte precursor cells reprogrammed to become multipotential CNS stem cells. Science 289:1754–1757
Kondo T, Setoguchi T, Taga T (2004). Persistence of a small subpopulation of cancer stem-like cells in the C6 glioma cell line. Proc Natl Acad Sci USA 101:781–786
Lapidot T, Sirard C, Vormoor J, Murdoch B, Hoang T, Caceres-Cortes J, Minden M, Paterson B, Caligiuri MA, Dick JE (1994) A cell initiating human acute myeloid leukaemia after transplantation into SCID mice. Nature 367:645–648
Liu G, Yuan X, Zeng Z, Tunici P, Ng H, Abdulkadir IR, Lu L, Irvin D, Black KL, Yu JS (2006) Analysis of gene expression and chemoresistance of CD133+ cancer stem cells in glioblastoma. Mol Cancer 5:67
Liu Z, Martin LJ (2006) The adult neural stem and progenitor cell niche is altered in amyotrophic lateral sclerosis mouse brain. J Comp Neurol 497:468–488
Nunes MC, Roy NS, Keyoung HM, Goodman RR, McKhann G 2nd, Jiang L, Kang J, Nedergaard M, Goldman SA (2003) Identification and isolation of multipotential neural progenitor cells from the subcortical white matter of the adult human brain. Nat Med 9:439–447
Pardal R, Clarke MF, Morrison SJ (2003) Applying the principles of stem-cell biology to cancer. Nat Rev Cancer 3:895–902
Qiang L, Yang Y, Ma YJ, Chen FH, Zhang LB, Liu W, Qi Q, Lu N, Tao L, Wang XT, You QD, Guo QL (2009) Isolation and characterization of cancer stem like cells in human glioblastoma cell lines. Cancer Lett 279:13–21
Quinones-Hinojosa A, Sanai N, Gonzalez-Perez O, Garcia-Verdugo JM (2007) The human brain subventricular zone: stem cells in this niche and its organization. Neurosurg Clin N Am 18:15–20, vii
Reya T, Morrison SJ, Clarke MF, Weissman IL (2001) Stem cells, cancer, and cancer stem cells. Nature 414:105–111
Roy NS, Wang S, Jiang L, Kang J, Benraiss A, Harrison-Restelli C, Fraser RA, Couldwell WT, Kawaguchi A, Okano H, Nedergaard M, Goldman SA (2000) In vitro neurogenesis by progenitor cells isolated from the adult human hippocampus. Nat Med 6:271–277
Sanai N, Tramontin AD, Quinones-Hinojosa A, Barbaro NM, Gupta N, Kunwar S, Lawton MT, McDermott MW, Parsa AT, Manuel-Garcia Verdugo J, Berger MS, Alvarez-Buylla A (2004) Unique astrocyte ribbon in adult human brain contains neural stem cells but lacks chain migration. Nature 427:740–744
Singh SK, Clarke ID, Terasaki M, Bonn VE, Hawkins C, Squire J, Dirks PB (2003) Identification of a cancer stem cell in human brain tumors. Cancer Res 63:5821–5828
Singh SK, Hawkins C, Clarke ID, Squire JA, Bayani J, Hide T, Henkelman RM, Cusimano MD, Dirks PB (2004) Identification of human brain tumour initiating cells. Nature 432:396–401
Stupp R, Mason WP, van den Bent MJ, Weller M, Fisher B, Taphoorn MJ, Belanger K, Brandes AA, Marosi C, Bogdahn U, Curschmann J, Janzer RC, Ludwin SK,Gorlia T, Allgeier A, Lacombe D, Cairncross JG, Eisenhauer E, Mirimanoff RO (2005) Radiotherapy plus concomitant and adjuvant temozolomide for glioblastoma. N Engl J Med 352:987–996
Thored P, Arvidsson A, Cacci E, Ahlenius H, Kallur T, Darsalia V, Ekdahl CT, Kokaia Z, Lindvall O (2006) Persistent production of neurons from adult brain stem cells during recovery after stroke. Stem Cells 24:739–747
Vescovi AL, Galli R, Reynolds BA (2006) Brain tumour stem cells. Nat Rev Cancer 6:425–436
Weissman IL (2000) Stem cells: units of development, units of regeneration, and units in evolution. Cell 100:157–168
Xu Q, Yuan X, Tunici P, Liu G, Fan X, Xu M, Hu J, Hwang JY, Farkas DL, Black KL, Yu JS (2009) Isolation of tumour stem-like cells from benign tumours. Br J Cancer 101:303–311
Yuan X, Curtin J, Xiong Y, Liu G, Waschsmann-Hogiu S, Farkas DL, Black KL, Yu JS (2004) Isolation of cancer stem cells from adult glioblastoma multiforme. Oncogene 23:9392–9400
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2012 Springer Science+Business Media B.V.
About this chapter
Cite this chapter
Hu, J., Yuan, X., Xu, Q., Wang, H., Black, K.L., Yu, J.S. (2012). Cancer Stem Cells in Glioblastoma. In: Hayat, M. (eds) Stem Cells and Cancer Stem Cells, Volume 1. Stem Cells and Cancer Stem Cells, vol 1. Springer, Dordrecht. https://doi.org/10.1007/978-94-007-1709-1_14
Download citation
DOI: https://doi.org/10.1007/978-94-007-1709-1_14
Published:
Publisher Name: Springer, Dordrecht
Print ISBN: 978-94-007-1708-4
Online ISBN: 978-94-007-1709-1
eBook Packages: Biomedical and Life SciencesBiomedical and Life Sciences (R0)