
Abstract
High saturated fat intake contributes to insulin resistance, β-cell failure, and type 2 diabetes. Developmental programming refers to a stimulus or insult during critical periods of life which includes fetal and subsequent early neonatal life. Programming alters offspring physiology and metabolism with both immediate and lasting consequences. Maternal nutrition in gestation and lactation shapes offspring development and health. A high saturated fat diet ingested by mothers during gestation and/or lactation is a form of nutritional insult that induces diabetogenic changes in offspring physiology and metabolism. High fat programming is induced by maternal high saturated fat intake during defined periods of gestation and/or lactation and programs the physiology and metabolism of the offspring in early life. This more recently adopted form of developmental programming reflects society in both affluent and developing countries. High fat programming induces adverse changes in β-cell development and function in neonatal and weanling offspring. These changes are characterized by compromised β-cell development and function, evident by altered expression of key factors that maintain the β-cell phenotype. High fat programming is likely to result in β-cell failure and eventual type 2 diabetes.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
5.1 Introduction
Changes in lifestyle, such as consumption of a high-calorie diet and lack of exercise, have increased the global prevalence of obesity and diabetes [1]. Between 60 and 90% of cases of type 2 diabetes appear to be related to obesity [2] with a strong correlation between obesity and insulin resistance in both diabetic and nondiabetic subjects [3]. Developmental programming is defined as a stimulus or insult in utero or in early postnatal life (during suckling) that induces long lasting changes in progeny physiology and metabolism. High fat programming (HFP) is induced by maternal high saturated fat intake during defined periods of gestation and/or lactation and programs the physiology and metabolism of the offspring. This contrasts from previous studies focusing on protein deficiency in utero. Instead of mimicking famine as in protein restriction and undernutrition, which still exists in several parts of the world, HFP reflects current society in both affluent and developing nations. In affluent societies, there is an overabundance of food available. With economic improvement and migration in the developing world, there is a transition from the traditional way of life, where the diet comprises whole food and exercise is a regular routine in daily life, to a more Westernized lifestyle – characterized by the consumption of convenient processed and fast foods with high saturated fat content and a sedentary lifestyle due to a greater reliance on transport which reduces the need for exercise. With migration and changing economic status, people often switch diets which may be from whole food or a state of undernutrition to a diet that includes a high content of saturated fat and overnutrition. Disease risk is amplified by a greater mismatch between the prenatally predicted and actual adult environments [4]. As a result, societies in rapid economic transition are particularly vulnerable [5–8]. Long-term consumption of a high fat diet (HFD) concomitant with physical inactivity leads to obesity which is a major risk factor for inducing insulin resistance and β-cell failure and contributes to the increase in incidence of type 2 diabetes.
5.2 Critical Programming Windows
Both the intrauterine and lactational environments represent critical developmental periods that provide a platform for programming. The intrauterine environment influences the health of the fetus. The developing fetus is highly sensitive to its environment and nutrition is an important factor that affects both fetal growth and maturation [9]. The fetus makes adaptations that anticipate the postnatal nutrition which impacts its future metabolic status. A mechanism by which diet influences fetal growth is by altering circulating concentrations of key maternal metabolic hormones, which regulate placental nutrient transport and therefore fetal growth [10]. Lactation is a critical developmental stage for metabolic programming and later disease and for modifying the impact of prenatal challenges [11, 12]. Fluctuations in glycemic and saturated fatty acid levels have adverse effects on progeny. The level of nutrition available during pregnancy and lactation plays a major role in determining offspring metabolic phenotype [13]. The offspring adopts the nutrition it experienced during these critical developmental periods i.e., the diet that it is exposed to during fetal and early postnatal life. A high saturated fat diet is strongly associated with the pathogenesis of β-cell failure, insulin resistance, and type 2 diabetes [14]. In pregnant mothers, maintenance on an HFD results in the exposure of offspring to an insult during the critical period of fetal life. This, together with the changes in the metabolic profile and state of insulin resistance in the pregnant mother (which occurs in mothers during normal pregnancy), is likely to increase the risk of the offspring to develop metabolic disease.
5.3 HFP Concept
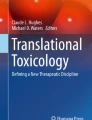
HFP can be described by maternal high saturated fat intake during defined periods of gestation and/or lactation which results in programming of the physiology and metabolism in the offspring in early life [15]. Offspring can be studied at various stages of life: as neonates, weanlings, young adults, and old age. In terms of experimental design, high saturated fat diets are administered to pregnant and/or lactating Wistar rats, thereby exposing progeny to this dietary insult. Specifically, mothers and their progeny were maintained on an HFD throughout gestation only (gestational high fat programming = HFG), throughout lactation only (lactational high fat programming = HFL), or throughout both gestation and lactation (gestational and lactational high fat programming = HFGL; Fig. 5.1a). These offspring are therefore programmed as high fat exposure during these critical developmental periods influences their metabolic status. The HFD used contained 40% energy as fat compared to 10% energy as fat in the standard laboratory diet. Similar protein levels were maintained in both diets to avoid the effects of protein deficiency on β-cell morphology and function.

High fat programming: basic experimental design. e, gestational day; d, postnatal day (lactational day), HFD, high fat diet; HFG, gestational high fat diet; HFL, lactational high fat diet; HFGL, gestational and lactational high fat diet; downward arrows denote time points; horizontal arrows denote period of high fat diet maintenance
Furthermore, HFP studies can be extended to include different time period interventions (Fig. 5.1b). In these studies, the nutritional trajectory of pregnant mothers was maintenance on an HFD for either the first, second, or third week of gestation (to mimic human trimesters) and throughout gestation [16]. Neonatal offspring, maintained on the HFD for those specified periods of fetal life, were studied. All of these neonatal groups were also studied at weaning (3 weeks of age) [17]. During lactation, these offspring were maintained on a standard laboratory (low fat) diet.

High fat programming: extended experimental design. e, gestational day; d, postnatal day (lactational day). Numerals refer to the specific day of gestation (e) or lactation (d). HFD, high fat diet; HF1, high fat diet for the first week of gestation; HF2, high fat diet for the second week of gestation; HF3, high fat diet for the third week of gestation; HFG, gestational high fat diet; HFGL1, high fat diet throughout gestation and for the first week of lactation; HFGL2, high fat diet throughout gestation and for the second week of lactation; HFGL3, high fat diet throughout gestation and for the third week of lactation; HFL, lactational high fat diet; HFGL, gestational and lactational high fat diet; downward arrows denote time points; horizontal arrows denote period of high fat diet maintenance
Further extension of the weanling groups included those maintained on a gestational HFD including either the first (HFGL1), or the second (HFGL2), or the final (HFGL3; Fig. 5.1b) week of lactation [18]. When the neonatal and weanling offspring were not maintained on a HFD, they were instead maintained on a standard laboratory diet.
These studies demonstrated that high fat consumption resulted in increased food intake in pregnant mothers which subsequently increased their body weights and induced hyperglycemia [16]. In terms of HFP, neonates displayed alterations in glycemia and in β-cell development [16], which persisted in weanlings [17]. HFP over different time periods of gestation and lactation also altered expression of key β-cell genes, including GLUT-2, glucokinase (GK), and to a lesser extent, Pdx-1 [18]. A gestational HFD-induced maternal hyperglycemia and the programming effects resulted in neonates with hyperglycemia [16]. Both the mothers and neonates displayed no changes in insulinemia. Different outcomes in β-cell development and function were evident in both neonatal and weanling offspring from dams maintained on an HFD during specified periods of gestation and/or lactation [16–18]. These alterations appear to be dependent on the specific period of exposure to the HFD.
5.4 β-Cell Regulation
The ability of an organism to maintain its β-cell mass during adulthood is critical for maintaining glucose homeostasis and preventing diabetes [19]. β-cell mass is increased by β-cell neogenesis (differentiation from precursor cells), β-cell proliferation or replication (from existing β-cells), and β-cell hypertrophy (increase in β-cell size), and is reduced by β-cell death, primarily through apoptosis and also via hypotrophy (decreased β-cell size) [19]. The balance between proapoptotic and anti-apoptotic (protective) processes determines the fate of β-cells [20]. ATF3, a stress-inducible proapoptotic gene, represses the expression of IRS2, a prosurvival gene, thus providing a direct link between the stress response and a potent prosurvival pathway [20]. Because ATF3 is induced by a variety of stress signals, it can function as a conduit for stress signals to dampen a potent prosurvival pathway in β-cells [20]. An early loss of β-cell mass might subsequently favor dysfunction of the residual β-cells, possibly due to overstimulation or toxic effects of even mild chronic hyperglycemia and/or hyperlipidemia [21]. Partial recovery of the lost mass may result from post-insult induction of β-cell regeneration and/or neogenesis and eventually with treatment with growth-stimulating pharmacological agents [22]. Hypertrophy and increased insulin responsiveness to glucose and free fatty acids (FFA) also occur in residual β-cells [22]. The adaptive response might be insufficient or temporary because of incomplete differentiation of newly formed β-cells and/or acquired dysfunction of residual β-cells chronically exposed to a metabolically altered environment [22]. An increased frequency of apoptosis due to prolonged overstimulation of residual β-cells, chronic hyperglycemia, and/or hyperlipidemia might accelerate decomposition [22].
An increase in β-cell mass usually takes place over a period of time for the endocrine pancreas to maintain glucose homeostasis when challenged by diabetogenic states such as obesity and insulin resistance. This allows the pancreas to cope, for a defined time, with the maintenance of glucose homeostasis. However, after a threshold is reached, the β-cells become exhausted and hyperglycemia is manifested usually along with an altered insulinemic profile. Initially hyperinsulinemia is exhibited, i.e., the β-cells secrete more insulin in order to restore glucose homeostasis, but eventually, the β-cells fail to secrete sufficient insulin resulting in hypoinsulinemia which often progresses to type 2 diabetes. Hypoinsulinemia is indicative of the more severe type 1 diabetes, which indicates how type 2 diabetes evolves to closely mimic type 1 diabetes, as it progresses to deteriorate to a state where exogenous insulin is required to counteract the elevated circulating glucose concentrations. Molecules, signaling pathways, and cellular machinery involved in the demise of β-cells under seemingly divergent pathophysiological conditions, i.e., type 1 and 2 diabetes are to a large extent the same [20]. Chronic high saturated fat consumption and persistent hyperglycemia contribute significantly to reducing β-cell mass.
5.5 HFP May Induce β-Cell Failure Via Glucolipotoxicity
Glucotoxicity can be described as the slow and progressively irreversible effects of chronic hyperglycemia on β-cell function [23]. Chronic hyperglycemia decreases β-cell mass by inducing apoptosis [24, 25] and adversely affects insulin secretion [23]. Lipotoxicity, characterized by chronic exposure to elevated FFA concentrations, impairs insulin secretion leading to hyperglycemia and β-cell failure [26]. Hyperglycemia is proposed to be a prerequisite for lipotoxicity to occur [27]. The glucolipotoxicity theory proposes that simultaneous elevation of glucose and lipids results in intracellular accumulation of lipids and lipid metabolites, which are ultimately detrimental to β-cell function and survival [28]. HFP may induce adverse effects on metabolism and physiology by elevating both circulating glucose and fatty acid levels in offspring. This impairs β-cell development and function resulting in loss of glucose homeostasis.
Chronic exposure of islets to elevated levels of nutrients induces β-cell dysfunction and triggers β-cell death. Exposure of isolated rodent islets to hyperglycemia for several days raises basal insulin secretion but impairs insulin secretion in response to stimulatory glucose concentrations [29, 30]. Similarly, exposure of islets to elevated levels of FFA does not impair glucose-stimulated insulin secretion (GSIS) unless the islets are cultured at or above a threshold concentration of glucose (about 8 mmol/l) [23, 31]. This suggests that β-cell failure is likely a consequence of glucolipotoxicity as opposed to either gluco- or lipotoxicity as separate entities [23, 31]. HFP may induce β-cell failure by a glucolipotoxic mechanism due to potential exposure of offspring to maternal hyperglycemic and hyperlipidemic intrauterine environments. In addition, the milk of hyperglycemic mothers may also contain elevated FFA concentrations which may have a glucolipotoxic effect on the suckling offspring. One hypothesis is that β-cells become sensitized to FFA and preferentially metabolize FFA rather than glucose as fuel, which may explain the reduced glucose-stimulated insulin release (GSIR) typically observed following prolonged exposure to FFA [27]. In HFP, it is therefore likely that preferential metabolism of FFA over glucose will further exacerbate hyperglycemia.
Elevated levels of glucose or saturated fatty acids can in their own capacity or synergistically induce β-cell failure. However, the presence of both gluco- and lipotoxicity, i.e., glucolipotoxicity will accelerate the impairment of β-cell function. This simultaneous dual insult will more rapidly increase the β-cell metabolic overload, inhibiting β-cell compensation and thus increase susceptibility to β-cell failure. In obese type 2 diabetic patients, their hyperglycemic state concomitant with the readily available fat stores for release of FFA, will place them in a glucolipotoxic state. Obese type 2 diabetic individuals who continuously ingest a high intake of harmful saturated fatty acids will further exacerbate this condition.
β-cells initially compensate for the insulin resistance associated with obesity by upregulating the secretion of insulin [1]. During β-cell compensation, β-cells are exposed to metabolic changes associated with obesity, so factors commonly associated with obesity such as insulin resistance, adipokines, FFA, reactive oxygen species, and ER-associated stress are likely inducers of β-cell failure [1]. β-cell failure in type 2 diabetes occurs when islets are unable to sustain β-cell compensation for insulin resistance [32]. The failure is progressive, particularly after hyperglycemia is established, which leads to poorly functioning, dedifferentiated β-cells and loss of β-cell mass from apoptosis [32]. β-cell destruction in various pathophysiological conditions can be viewed as a stress response [20]. The likely mechanisms of early β-cell failure include mitochondrial dysfunction, oxidative stress, ER stress, dysfunctional triglyceride/FFA (TG/FFA) cycling, and glucolipotoxicity [32]. Furthermore, β-cell failure is likely induced by a combination of chronic hyperglycemia, hyperlipidemia, and/or certain cytokines that interfere with the signaling pathways that maintain normal β-cell growth and survival [33]. This results in a reduction in functional β-cell mass in a diabetic state [33]. Other underlying mechanisms in β-cell failure include genetic susceptibility, β-cell metabolic overload and amyloid fibrils [34]. Once hyperglycemia has developed, which occurs in specific instances of HFP dependent on the period of exposure, additional processes linked to glucotoxicity and the diabetic milieu, such as islet inflammation, O-linked glycosylation, and amyloid deposition accelerate β-cell failure, resulting in severe β-cell phenotypic alterations and loss of β-cell mass by apoptosis [32].
Mice fed a diet rich in saturated fat develop overt diabetes characterized by hyperinsulinemia associated with hyperglycemia [35]. In offspring where the HFD was administered only during fetal life (similar to HFG) and during both fetal and neonatal life (similar to HFGL), the β-cell insult was severe evident by sustained hyperglycemia during adulthood [35]. Thus it seems feasible that the programming effects in both HFG and HFGL, and likely also in HFL weanlings, will further exacerbate as they reach adulthood. Obesity often leads to insulin resistance but only a subset of obese insulin-resistant individuals progress to type 2 diabetes [34], which may be due to genetic predisposition, poor dietary control, and physical inactivity. In both animals and humans, the triggering factor is β-cell failure, which involves a decrease in β-cell mass and a deterioration of key β-cell functions like GSIS [34]. The severity of HFP in inducing β-cell failure may be dependent on the stage of programming (gestational and/or lactational), the metabolic status of the mother, and the duration of the insult. It appears that limited exposure to programming effects, such as maintenance on an HFD for only a single gestational week, may have a reduced impact on adversely affecting β-cell function. This however makes the offspring susceptible to the predictive adaptive response whereby they cannot accurately anticipate future nutrition as it differs from the nutrition experienced in utero which is hypothesized to have adverse health consequences. Maintenance on an HFD throughout both gestation and lactation represents extreme HFP. It is hypothesized that if these progeny are maintained on an HFD, with time β-cell failure will ensue. Initially the β-cell may undergo compensation and adaptation to cope with the maintenance of glucose homeostasis. However, HFP coupled to chronic high fat feeding is likely to increase glucolipotoxicity resulting in eventual β-cell failure.
Chronic hyperglycemia can increase the rate of development of the early diabetic state by affecting the secretion capacity of pancreatic cells, which in turn, increases blood glucose concentrations [36] and ultimately leads to the total incapacity of β-cells to secrete insulin [37, 38]. HFP induces hyperglycemia and hypoinsulinemia, which is characterized by reduced β-cell volume, number, and sizes, with reduced expression of GK. Collectively, these adverse metabolic effects of programming would predispose these progeny to β-cell failure. Also, HFP may increase circulating FFA concentrations due to metabolism of the HFD which releases excess FFA. This may lead to reduced insulin secretion, which induces hyperglycemia resulting in β-cell failure. Apoptosis and oxidative stress are also likely candidates in the demise of β-cell integrity. HFP may follow a glucolipotoxic mechanism to impair β-cell function ultimately leading to the β-cell failure.
5.6 HFP Degrades β-Cell Integrity
A HFD is known to compromise glucose sensing and insulin signaling, evident by reduced expression of insulin, Pdx-1, GLUT-2, and GK after high fat feeding or exposure to FFA [39–42]. The percentage of l-type calcium channels that are considered most important for insulin secretion is reduced in neonatal rats, concomitant with reduced expression of GLUT-2 [43]. Preliminary results show that control neonates display a normal insulin secretory response to glucose stimulation, a function that was absent in HFG neonates – HFG neonates released reduced insulin at stimulatory 13 and 22 mmol/l glucose concentrations concomitant with reduced Pdx-1 and GK immunoreactivity (unpublished data). Chronic hyperglycemia adversely affects insulin secretion [23] and decreases β-cell mass by inducing apoptosis [24, 25]. As HFG neonates display reduced β-cell volume and numbers [5] and both Pdx-1 and GK immunoreactivity is reduced, the functional capacity of the HFG β-cells is reduced. These effects, concomitant with the reduced insulin release from HFG islets at stimulatory glucose concentrations, indicate that programming with an HFD during gestation impairs β-cell function.
An altered metabolic milieu decreases Pdx-1 transcription by mediating a cascade of epigenetic modifications which silences Pdx-1 [44]. In intrauterine growth retarded (IUGR) rats, Pdx-1 expression was permanently reduced in β-cells [44]. Gestational HFP reduced Pdx-1 immunoreactivity in the neonates which could adversely affect insulin gene expression and, in addition, appears to have contributed to the reduction in β-cell volume and number in HFG neonates.
Haploinsufficiency of β-cell specific GK (GK+/–) results in mild diabetes with impaired insulin secretion in response to glucose [45]. Wild-type mice fed an HFD showed marked β-cell hyperplasia, whereas GK+/–displayed insufficient β-cell hyperplasia despite a similar degree of insulin resistance [46]. Permanent exposure of weanlings to an HFD, i.e., during the entire duration of both gestation and lactation results in the reduction of mRNA expression of GLUT-2 and GK [18]. These HFGL weanlings displayed reduced circulating insulin concentrations suggesting impaired insulin secretion attributed partly to the reduced GK expression both at mRNA and protein level [18]. HFL, HFGL, and HFG weanlings display glucose intolerance in descending order of severity (unpublished data). Thus HFGL weanlings display impaired β-cell function which may predispose them to β-cell failure. Both HFG and HFGL weanlings were normoglycemic and hypoinsulinemic [18] but both groups were glucose intolerant, an effect that was more marked in HFGL weanlings. As the HFG and HFGL weanlings were normoglycemic yet glucose intolerant, it is thus important to assess β-cell function in the absence of hyperglycemia. In contrast, HFL weanlings were hyperglycemic and normoinsulinemic [18] and displayed the greatest severity in glucose intolerance. Glucose intolerance may represent an early event in the impairment of β-cell function and appears to be exacerbated by hyperglycemia.
5.7 HFP: Potential Mechanism of Induction of Type 2 Diabetes
Type 2 diabetes is associated with genetic and environmental factors (Fig. 5.2). Genetic factors include candidate genes (several are currently being characterized including TCF7L2 and KCNJ11) and MODY genes (mostly transcription factors, apart from GK), which result in offspring inheriting the disease from their parents. Environmental factors are more broadly defined as they include nutrition (e.g., malnutrition and overnutrition), developmental programming, level of physical activity, oxidative stress, cytokines, and glucolipotoxicity. High saturated fat diets, sedentary lifestyles, high oxidative stress levels, and cytokines all play a role in the pathogenesis of diabetes via different mechanisms. However, glucolipotoxicity may be strongly associated with HFP-induced β-cell failure.

The influence of HFP in the pathogenesis of type 2 diabetes. Apart from environmental and genetic factors, HFP can induce hyperglycemia as a stronger environmental insult. Glucolipotoxicity may be the mechanism whereby HFP induces β-cell failure. Hyperglycemia is the clinical hallmark of type 2 diabetes. Initially β-cells may compensate and adapt to the hyperglycemia (by hypertrophy and hyperplasia) by hypersecretion of insulin. This may still reflect normal glucose homeostasis. Eventually, β-cell exhaustion may set in resulting in reduced insulin secretion characterized by hypoinsulinemia which may lead to impaired glucose tolerance. This will further exacerbate hyperglycemia. In the endocrine pancreas, β-cell exhaustion eventually leads to β-cell failure characterized by impaired insulin secretion which may progress to overt type 2 diabetes. Skeletal muscle, liver and adipose tissue are the main sites of glucose uptake. Hyperglycemia, which is further aggravated by hypoinsulinemia, results in insulin resistance of these peripheral tissues due to their reduced ability to effectively clear glucose. Like β-cell failure, insulin resistance precedes overt type 2 diabetes
Developmental programming by feeding pregnant dams an HFD is an environmental insult that induces adverse changes in β-cell development and function in young offspring. HFP can be seen as a more robust environmental insult as high saturated fat intake (in its own capacity) and developmental programming (in its capacity) can strengthen the detrimental environmental influence of these combined insults.
Glucolipotoxicity proposes that simultaneous elevation of circulating glucose and FFA concentrations induces β-cell failure. HFP induces hyperglycemia and metabolism of the HFD may result in increased circulating FFA levels, particularly saturated fatty acids which have adverse effects on β-cells. HFP may therefore, via glucolipotoxic effects, induce β-cell failure.
Chronic hyperglycemia adversely affects insulin secretion [23] and decreases β-cell mass by inducing apoptosis [24, 25]. Furthermore, chronic hyperglycemia leads to progressive loss of β-cell mass with a prolonged increase in the rate of β-cell apoptosis without a compensatory increase in β-cell growth [47]. Hyperglycemia is central to type 2 diabetes and can be induced by environmental factors, genetic mutations, and by HFP. Apoptosis reduces β-cell mass thereby further aggravating hyperglycemia. With HFP, offspring are compromised at an early age, as normal β-cell development is impaired and they display reduced β-cell function. In the face of hyperglycemia, β-cell compensation and adaptation occurs to restore normoglycemia. This occurs by hyperplasia and hypertrophy of the β-cells, which temporarily maintain glucose homeostasis. However, if hyperglycemia recurs, β-cell exhaustion may ensue, resulting in subsequent β-cell failure. β-cell failure and insulin resistance are key events that contribute to the pathogenesis of type 2 diabetes. It is likely that HFP accelerates the onset of overt type 2 diabetes by inducing β-cell failure. Further studies are required to elaborate on this potential mechanism of HFP of β-cell failure and to determine the effects of HFP in the possible induction of insulin resistance in skeletal muscle, liver and adipose tissue.
5.8 Perspectives
HFP reduces β-cell integrity by impairing both β-cell development and function, therefore compromising future offspring health by predisposing them to metabolic disease. There may be a possible link between HFP and glucolipotoxicity. Nutrition during critical developmental periods shapes offspring health. The intrauterine milieu and the lactation period have a great influence on the health of the progeny. Dietary intervention to ensure adequate nutrition with the correct macronutrient balance, concomitant with sufficient levels of micronutrients and with the optimum ratios of fatty acids is a strategy to optimize the growth and health of the fetus and neonate. During fetal and early postnatal life, maintenance on an undesirable diet, such as a high saturated fat diet, is likely to induce adverse changes in offspring physiology and metabolism. Specifically HFP has been demonstrated to adversely affect β-cell function thus predisposing offspring to β-cell failure. The key for future research is to clearly elucidate the mechanisms such as glucolipotoxicity, followed by manipulation and correction of these changes in order to maintain a healthy β-cell phenotype that can cope with fluctuating metabolic demands and improve outcomes for β-cell survival.
References
Kasuga M. Insulin resistance and pancreatic beta cell failure. J Clin Invest 2006;116:1756–60.
Anderson JW, Kendall CW, Jenkins DJ. Importance of weight management in type 2 diabetes: review with meta-analysis of clinical studies. J Am Coll Nutr 2003;22:331–9.
Ludvik B, Nolan JJ, Baloga J, Sacks D, Olefsky J. Effect of obesity on insulin resistance in normal subjects and patients with NIDDM. Diabetes 1995;44:1121–5.
Godfrey KM, Lillycrop KA, Burdge GC, Gluckman PD, Hanson MA. Epigenetic mechanisms and the mismatch concept of the developmental origins of health and disease. Pediatr Res 2007;61:5R–10R.
Popkin BM. Nutrition in transition: the changing global nutrition challenge. Asia Pac J Clin Nutr 2001;10 Suppl:S13–8.
Gluckman PD, Hanson MA. The developmental origins of the metabolic syndrome. Trends Endocrinol Metab 2004;15:183–7.
Prentice AM, Moore SE. Early programming of adult diseases in resource poor countries. Arch Dis Child 2005;90:429–32.
Bhargava SK, Sachdev HS, Fall CH, Osmond C, Lakshmy R, Barker DJ, Biswas SK, Ramji S, Prabhakaran D, Reddy KS. Relation of serial changes in childhood body-mass index to impaired glucose tolerance in young adulthood. N Engl J Med 2004;350:865–75.
Gluckman PD, Hanson MA. Developmental origins of disease paradigm: a mechanistic and evolutionary perspective. Pediatr Res 2004;56:311–7.
Jansson N, Nilsfelt A, Gellerstedt M, Wennergren M, Rossander-Hulthen L, Powell TL, Jansson T. Maternal hormones linking maternal body mass index and dietary intake to birth weight. Am J Clin Nutr 2008;87:1743–9.
Heywood WE, Mian N, Milla PJ, Lindley KJ. Programming of defective rat pancreatic beta-cell function in offspring from mothers fed a low-protein diet during gestation and the suckling periods. Clin Sci (Lond) 2004;107:37–45.
Siebel AL, Mibus A, De Blasio MJ, Westcott KT, Morris MJ, Prior L, Owens JA, Wlodek ME. Improved lactational nutrition and postnatal growth ameliorates impairment of glucose tolerance by uteroplacental insufficiency in male rat offspring. Endocrinology 2008;149:3067–76.
Zambrano E, Bautista CJ, Deas M, Martinez-Samayoa PM, Gonzalez-Zamorano M, Ledesma H, Morales J, Larrea F, Nathanielsz PW. A low maternal protein diet during pregnancy and lactation has sex- and window of exposure-specific effects on offspring growth and food intake, glucose metabolism and serum leptin in the rat. J Physiol 2006;571:221–30.
Cerf ME. High fat diet modulation of glucose sensing in the beta-cell. Med Sci Monit 2007;13:RA12–7.
Cerf ME, Louw J. High fat-induced programming of beta-cell development and function in neonatal and weanling offspring. Kerala, India, Transworld Research Network; 2008, pp. 133–58.
Cerf ME, Williams K, Nkomo XI, Muller CJ, Du Toit DF, Louw J, Wolfe-Coote SA. Islet cell response in the neonatal rat after exposure to a high-fat diet during pregnancy. Am J Physiol Regul Integr Comp Physiol 2005;288:R1122–8.
Cerf ME, Williams K, Chapman CS, Louw J. Compromised beta-cell development and beta-cell dysfunction in weanling offspring from dams maintained on a high-fat diet during gestation. Pancreas 2007;34:347–53.
Cerf ME, Muller CJ, Du Toit DF, Louw J, Wolfe-Coote SA. Hyperglycaemia and reduced glucokinase expression in weanling offspring from dams maintained on a high-fat diet. Br J Nutr 2006;95:391–96.
Ackermann AM, Gannon M. Molecular regulation of pancreatic β-cell mass development, maintenance, and expansion. J Mol Endocrinol 2007;38:193–206.
Li D, Yin X, Zmuda EJ, Wolford CC, Dong X, White MF, Hai T. The repression of IRS2 gene by ATF3, a stress-inducible gene, contributes to pancreatic beta-cell apoptosis. Diabetes 2008;57:635–44.
Donath MY, Halban PA. Decreased beta-cell mass in diabetes: significance, mechanisms and therapeutic implications. Diabetologia 2004;47:581–89.
Masiello P. Animal models of type 2 diabetes with reduced pancreatic beta-cell mass. Int J Biochem Cell Biol 2006;38:873–93.
Poitout V, Robertson RP. Minireview: Secondary beta-cell failure in type 2 diabetes – a convergence of glucotoxicity and lipotoxicity. Endocrinology 2002;143:339–42.
Pick A, Clark J, Kubstrup C, Levisetti M, Pugh W, Bonner-Weir S, Polonsky KS. Role of apoptosis in failure of beta-cell mass compensation for insulin resistance and beta-cell defects in the male Zucker diabetic fatty rat. Diabetes 1998;47:358–64.
Donath MY, Gross DJ, Cerasi E, Kaiser N. Hyperglycemia-induced beta-cell apoptosis in pancreatic islets of Psammomys obesus during development of diabetes. Diabetes 1999;48:738–44.
Skelly RH, Bollheimer LC, Wicksteed BL, Corkey BE, Rhodes CJ. A distinct difference in the metabolic stimulus-response coupling pathways for regulating proinsulin biosynthesis and insulin secretion that lies at the level of a requirement for fatty acyl moieties. Biochem J 1998;331 (Pt 2):553–61.
Poitout V, Robertson RP. Glucolipotoxicity: fuel excess and beta-cell dysfunction. Endocr Rev 2008;29:351–66.
Ruderman N, Prentki M. AMP kinase and malonyl-CoA: targets for therapy of the metabolic syndrome. Nat Rev Drug Discov 2004;3:340–51.
Chen, C, Hosokawa, H, Bumbalo, LM, Leahy, JL: Regulatory effects of glucose on the catalytic activity and cellular content of glucokinase in the pancreatic beta cell. Study using cultured rat islets. J Clin Invest 94:1616–20, 1994
Khaldi MZ, Guiot Y, Gilon P, Henquin JC, Jonas JC. Increased glucose sensitivity of both triggering and amplifying pathways of insulin secretion in rat islets cultured for 1 wk in high glucose. Am J Physiol Endocrinol Metab 2004;287:E207–17.
Prentki M, Joly E, El-Assaad W, Roduit R. Malonyl-CoA signaling, lipid partitioning, and glucolipotoxicity: role in beta-cell adaptation and failure in the etiology of diabetes. Diabetes 51 Suppl 2002;3:S405–13.
Prentki M, Nolan CJ. Islet beta cell failure in type 2 diabetes. J Clin Invest 2006;116:1802–12.
Rhodes CJ. Type 2 diabetes-a matter of beta-cell life and death? Science 2005;307:380–84.
Muoio DM, Newgard CB. Mechanisms of disease: molecular and metabolic mechanisms of insulin resistance and beta-cell failure in type 2 diabetes. Nat Rev Mol Cell Biol 2008;9:193–205.
Gniuli D, Calcagno A, Caristo ME, Mancuso A, Macchi V, Mingrone G, Vettor R. Effects of high-fat diet exposure during fetal life on type 2 diabetes development in the progeny. J Lipid Res 2008;49:1936–45.
Brunner Y, Schvartz D, Priego-Capote F, Coute Y, Sanchez JC. Glucotoxicity and pancreatic proteomics. J Proteomics 2008, In press
LeRoith D. Beta-cell dysfunction and insulin resistance in type 2 diabetes: role of metabolic and genetic abnormalities. Am J Med 113 Suppl 2002;6A:3S–11S.
Dubois M, Vacher P, Roger B, Huyghe D, Vandewalle B, Kerr-Conte J, Pattou F, Moustaid-Moussa N, Lang J. Glucotoxicity inhibits late steps of insulin exocytosis. Endocrinology 2007;148:1605–14.
Kim Y, Iwashita S, Tamura T, Tokuyama K, Suzuki M. Effect of high-fat diet on the gene expression of pancreatic GLUT2 and glucokinase in rats. Biochem Biophys Res Commun 1995;208:1092–98.
Jorns A, Tiedge M, Ziv E, Shafrir E, Lenzen S. Gradual loss of pancreatic beta-cell insulin, glucokinase and GLUT2 glucose transporter immunoreactivities during the time course of nutritionally induced type-2 diabetes in Psammomys obesus (sand rat). Virchows Arch 2002;440:63–69.
Reimer MK, Ahren B. Altered beta-cell distribution of pdx-1 and GLUT-2 after a short-term challenge with a high-fat diet in C57BL/6 J mice. Diabetes 2002;51 Suppl 1:S138–3.
Gremlich S, Bonny C, Waeber G, Thorens B. Fatty acids decrease IDX-1 expression in rat pancreatic islets and reduce GLUT2, glucokinase, insulin, and somatostatin levels. J Biol Chem 1997;272:30261–9.
Navarro-Tableros V, Fiordelisio T, Hernandez-Cruz A, Hiriart M. Physiological development of insulin secretion, calcium channels and GLUT2 expression of pancreatic rat β-cells. Am J Physiol Endocrinol Metab 2007;292:E1018–29.
Park JH, Stoffers DA, Nicholls RD, Simmons RA. Development of type 2 diabetes following intrauterine growth retardation in rats is associated with progressive epigenetic silencing of Pdx1. J Clin Invest 2008;118:2316–24.
Terauchi Y, Sakura H, Yasuda K, Iwamoto K, Takahashi N, Ito K, Kasai H, Suzuki H, Ueda O, Kamada N. Pancreatic beta-cell-specific targeted disruption of glucokinase gene. Diabetes mellitus due to defective insulin secretion to glucose. J Biol Chem 1995;270:30253–6.
Terauchi Y, Takamoto I, Kubota N, Matsui J, Suzuki R, Komeda K, Hara A, Toyoda Y, Miwa I, Aizawa S, Tsutsumi S, Tsubamoto Y, Hashimoto S, Eto K, Nakamura A, Noda M, Tobe K, Aburatani H, Nagai R, Kadowaki T. Glucokinase and IRS-2 are required for compensatory beta cell hyperplasia in response to high-fat diet-induced insulin resistance. J Clin Invest 2007;117:246–57.
Sone H, Kagawa Y. Pancreatic beta cell senescence contributes to the pathogenesis of type 2 diabetes in high-fat diet-induced diabetic mice. Diabetologia 2005;48:58–67.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2010 Springer Science+Business Media B.V.
About this chapter
Cite this chapter
Cerf, M.E. (2010). High Fat Programming of β-Cell Failure. In: Islam, M. (eds) The Islets of Langerhans. Advances in Experimental Medicine and Biology, vol 654. Springer, Dordrecht. https://doi.org/10.1007/978-90-481-3271-3_5
Download citation
DOI: https://doi.org/10.1007/978-90-481-3271-3_5
Published:
Publisher Name: Springer, Dordrecht
Print ISBN: 978-90-481-3270-6
Online ISBN: 978-90-481-3271-3
eBook Packages: Biomedical and Life SciencesBiomedical and Life Sciences (R0)