
Access provided by Autonomous University of Puebla. Download chapter PDF
Keywords
These keywords were added by machine and not by the authors. This process is experimental and the keywords may be updated as the learning algorithm improves.
Incontinence
-
Urinary incontinence is more common in women, and it is related to pelvic organ prolapse and other pelvic floor abnormalities. It is commonly divided into three subtypes: stress, urge, and mixed.
-
MRI is acquiring a primary role in evaluating stress incontinence. Sagittal T2-weighted MRI identifies a cystocele as a posteriorly bulging bladder into the vagina. Ultrafast, large-field-of-view, T2-weighted sequences such as single-shot fast spin echo (SSFSE, GE Healthcare scanners) or half-Fourier acquisition turbo spin echo (HASTE, Siemens Medical Solutions scanners) are usually performed for a detailed dynamic pelvic floor visualization during straining; alternatively, true fast imaging in steady-state precession may be performed. Stress incontinence is associated with a greater vesicourethral angle and a larger retropubic space than found in continent women.
-
In men, incontinence is generally due to sphincter dysfunction, such as scarring or decreased contractions, after prostatectomy; these findings are evaluated with endourethral US.
Infarction, Bladder
-
Bladder overdistention can lead to ischemia and eventually to gangrene. It can also be secondary to a strangulated bladder in an inguinal hernia, generally in association with herniation of bowel loops and fat tissue.
-
CT: Bladder overdistention is often an incidental finding, especially in unconscious patients. Dome of bladder may extend above the level of the umbilicus.
Infarction, Renal
-
It is more often secondary to sudden occlusion of renal artery supply, but it can also be secondary to vessel compression by extrinsic tumors, artery thrombosis, emboli, vasculitides, and venous occlusions. One result of renal ischemia is renovascular hypertension, but in some patients, ischemia manifests primarily as renal failure (also called ischemic nephropathy).
-
CT: Contrast-enhanced CT is the best imaging tool. A focal infarction appears as a wedge-shaped region of decreased or absent contrast enhancement with sharply defined margins, most often extending to the capsule (Fig. 3a, b). Postcontrast CT of a total infarct shows a hypodense, nonfunctioning kidney; prominent capsular collaterals, called the cortical rim sign, often lead to surrounding vascular enhancement. If the infarction is chronic, it shows a small kidney with smooth or irregular contour, with no cortical rim sign.
Fig. 3 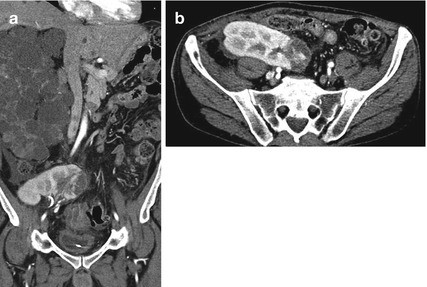
(a, b) Coronal and axial CT images showing a wedge-shaped region of decreased contrast enhancement with sharply defined margins, extending to the capsule on the medial aspect of a transplanted pelvic kidney, consistent with renal infarction
-
MRI: A focal infarction appears as a wedge-shaped region with low signal intensity both on T1 and T2; after contrast administration, it shows as a sharply demarcated, nonenhanced tissue. The cortical rim sign can be appreciated; however, this is only seen in around 50 % of the cases.

Infarction, Testis
-
It may result from torsion or trauma, but testicular infarction, although rare, has been also reported as a potential serious complication of a severe or unresolving epididymitis.
-
US is the imaging modality of choice; it shows a focal hypoechoic and avascular area on color Doppler.
Suggested Reading
Blaivas M, Sierzenski P and Lambert M. 2001. Emergency evaluation of patients presenting with acute scrotum using bedside ultrasonography. Acad Emerg Med.; 8:90–3.
Mazeh H, et al. 2008. Laparoscopic inguinal hernia repair on a general surgery ward: 5 years experience. J Laparoendosc Adv Surg Tech A. 18(3):373–6.
Yan ML, and Fielding JR. 2008. MRI of Pelvic Floor Dysfunction: Review. AJR Volume 191, Number 6.
Sue SR, Pelucio M and Gibbs M. 1998. Testicular infarction in a patient with epididymitis. Acad Emerg Med. 5: 1128–30.
Author information
Authors and Affiliations
Rights and permissions
Copyright information
© 2015 Springer-Verlag Italia
About this chapter
Cite this chapter
Panebianco, V., Fütterer, J.J. (2015). I. In: MDCT and MRI in Genitourinary Imaging. A-Z Notes in Radiological Practice and Reporting. Springer, Milano. https://doi.org/10.1007/978-88-470-5705-0_9
Download citation
DOI: https://doi.org/10.1007/978-88-470-5705-0_9
Published:
Publisher Name: Springer, Milano
Print ISBN: 978-88-470-5704-3
Online ISBN: 978-88-470-5705-0
eBook Packages: MedicineMedicine (R0)