
Access provided by Autonomous University of Puebla. Download chapter PDF
Keywords
These keywords were added by machine and not by the authors. This process is experimental and the keywords may be updated as the learning algorithm improves.
Oncocytoma, Renal
-
Oncocytoma is the second most common benign renal neoplasm after angiomyolipoma. It accounts for 3–7 % of solid renal masses. They appear to originate from the cortical part of collecting tubules. These tumors are often detected incidentally in asymptomatic individuals; some are multiple, bilateral, or metachronous in a minority of cases. In rare cases, presenting as hundreds of nodules scattered throughout both kidneys.
-
CT: they are solid, well-marginated, homogeneous, and often large tumors. Cystic changes and calcifications are rare. They have no specific imaging features (such as MRI), in fact imaging cannot differentiate it from a malignant renal mass, unlike which, hemorrhage and necrosis are not common. Oncocytomas tend to contain a central stellate scar that mimics the necrosis seen in a renal cell carcinoma.
-
MRI: The MR appearance is variable and nonspecific. They are hypointense on T1-weighted MR images (70 % of the cases) but vary in signal intensity on T2-weighted images (67 % high signal intensity), often with a well-defined capsule. The central scar (when present) can be seen as a stellate area of low signal intensity on T1-weighted images and high signal intensity on T2-weighted images; Fig. 4a, b. Postcontrast MR imaging reveals, in a minority of oncocytomas, a “spoke-wheel” enhancement pattern. However, this is a nonspecific sign, because a similar vascular arrangement has been described with renal cell carcinoma.
Fig. 4 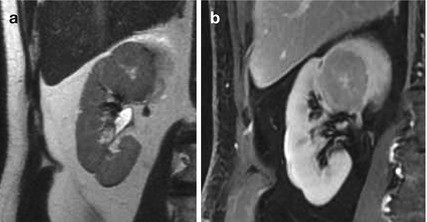
(a, b) Oncocytoma in a 40-year-old woman. T2-weighted imaging and delayed contrast-enhanced T1-weighted images, showing a large, round-shaped, well-definied, mass with heterogeneous signal intensity and a central cleft. Oncocytoma was confirmed at histopathology analysis performed after nefrectomy

Orchidopexy
-
Orchidopexy is the most succesful surgical treatment of cryptorchidism that is characterized by the failure of descent of one or both testicles in the scrotum. Surgical intervention is aimed at positioning and fixing of one or both testicles. The undescended testes is associated with a greater incidence of neoplasia at this level since the retention leads to degenerative phenomena of the gonad with arrest of spermatogenesis. This procedure should be performed after the twelfth month of life, the period during which the testicle could still end his physiological descent into the scrotum.
-
Several complications may occur including testicular retraction, atrophy or infarction, hematoma formation, ilio-inguinal nerve injuring, postoperative torsion, and damage to the vas deference.
-
MR imaging can be used in case ultrasound is inconclusive. Anatomical T1- and T2-weighted imaging can be applied for scrotal and pelvic evaluation. The testis is high signal intensity on T2 and intermediate signal intensity on T1.
Orchitis
-
Most episodes of orchitis result from extensions of acute epididymitis. In isolated orchitis, a viral infection, such as mumps, should be suspected. Causative agent in adolescent and men younger than 35 years are usually considered as Chlamydia trachomatis and Neisseria gonorrhoeae. Less common causes of epididymitis and orchitis include Granulomatous conditions such as Tuberculosis, Sarcoidosis, and Brucellosis and chemical epididymitis in reflux of sterile urine, amiodarone therapy, or prostate brachytherapy. In children less than 2 years of age, a predisposing condition is usually identified, such as imperforated anus, ureteral ectopia to seminal vesicles, bladder exstrophy, and posterior urethral valves.
-
Complications of epididymo-orchitis are abscess formation, pyocele, infarct, gangrene, infertility, atrophy and chronic pain.
-
MRI: In epididymo-orchitis, the testis and epididymis have heterogeneous low signal intensities on T2-weighted images. The epididymis will be enlarged and hyperenhancing with contrast on T1-weighted studies. The testis may show inhomogeneous enhancement with hypointense bands.
Ovarian, Functional Cyst
-
Ovarian cysts are seen in all age groups, and many of them are functional cysts. Functional ovarian cysts include follicular cyst and corpus luteal cyst. Follicular cysts results from a failure of the follicle to rupture and corpus luteum cysts derive from hemorrhage in corpus luteum. Simple cysts have in general a size less than 3 mm. Unilocular cysts have a diameter less than 3 cm. Corpus luteal cysts may be larger and tend to be more symptomatic than follicular cysts. Functional cysts may spontaneously regress over time, usually within two menstrual cycles, and they should be monitored by follow-up US at 6–8 weeks.
MRI: Most ovarian cysts show a thin wall, with a very high signal intensity on T2-weighted images and intermediate to low signal intensity on T1-weighted images because of simple fluid content. Similar imaging characteristics may be seen in benign ovarian cystic tumors. The most helpful feature in distinguishing functional cysts from ovarian neoplasms is the presence of papillary projections and nodular septa in the latter. Larger simple cysts cannot be differentiated from unilocular cystadenoma, but if the cyst is more than 10 cm, a tumorous condition should be considered. The most helpful feature in distinguishing functional cysts from ovarian cystic tumors is the presence of papillary projections and nodular septa in the latter. Corpus luteal cysts have thicker walls than follicular cysts and avid enhancement, due to the thick luteinized cell layer that lines the interior of the cyst. Corpus luteum cysts do not demonstrate the profound T2 shortening that is seen with many endometriomas (T2-shading).
Ovarian Mature Cystic Teratoma
-
Teratoma, also known as dermoid cyst, is the most common ovarian neoplasm in woman under 45 years of age. “Mature” means benign, as opposed to the immature, malignant teratoma. Ovarian teratomas derive from germ cells and are classified into three main categories, among which the mature cystic teratoma account for 99 %. Less common types of mature teratomas are the monodermal teratomas, which include the struma ovarii and carcinoid tumors.
-
They are slow-growing tumors and most tend to be asymptomatic. Therefore, they are discovered incidentally at imaging. The most commonly associated complication is ovarian torsion; in fact, even though benign, they are often resected; other complications are infection, rupture and, rarely, hemolytic anemia. Malignant transformation can occur but is also rare.
-
Up to 90 %, they are unilocular and their diameter is smaller than 10 cm. The cystic component is fluid fat, produced by sebaceous glands in cyst lining, and the presence of fat is diagnostic. Up to 60 % may contain calcifications.
-
The inner lining of every mature cystic teratoma contains single or multiple white shiny masses projecting from the wall toward the center of the cysts. When hair, other dermal appendages, bone, and teeth are present, they usually arise from this protuberance known as the Rokitansky protuberance that is a common site of malignant transformation.
-
CT images demonstrate fat, fat fluid level, sebum-rich fluid in the cyst cavity, calcification (sometimes tooth) may present or not present in the wall, Rokitansky protuberance (adipose tissue) and tufts of hair. Whenever the size exceeds 10 cm or soft tissue plugs and cauliflower appearance with irregular borders is seen, malignant transformation should be suspected; Fig. 5.
Fig. 5 
(a) Mature teratoma in a 28-year-old woman. Coronal image of a contrast-enhanced CT scan shows a large cystic tumor with fat and multiple toothlike calcification. (b) Axial image of the same CT

MRI: On T1-weighted images, the lipid-laden cyst fluids are hyperintense, while calcifications and fibrosis are hypointense. The fatty regions demonstrate intermediate signal intensity on T2-weighted images; Fig. 6.

Mucinous cystadenocarcinoma of right ovarian in a 61-year-old woman. Coronal image of a contrast-enhanced CT scan shows a large multilocular cystic tumor with some thick, enhancing septations and mural nodules. The locules are of different attenuation, consistent with varying protein content
Ovarian Cystadenoma
-
Ovarian cystadenoma is one of the most common benign ovarian tumors in the reproductive age and this frequency tends to increase with age. There are two different types that differ in pathology, prognosis, and disease: serous and mucinous cystadenoma.
-
Both are thin-walled unilocular or multilocular cystic lesions filled with water-like or higher proteinaceous contents. At imaging a serous cystadenoma is most often unilocular and anechoic on ultrasound, and may look like a simple cyst. Mucinous cyst adenomas tend to be filled with sticky gelatinous fluid and are typically multilocular with different contents of the loculi, separated by thin septations and tend to be larger than serous cyst adenomas (mean size of 10 cm). The finding of papillary projections should raise the suspicion of a possible borderline malignancy or a cystadenocarcinoma.
-
CT: Cystadenomas are well-circumscribed cystic tumors, with regular and thin (<3 mm) wall and internal septations, that show enhancement.
-
MRI: The cystic loculi of serous cystadenomas tend to be low in signal on T1 and high on T2-weighted images because of simple fluid content. The content of the different loculi of mucous cystadenoma varies from watery to proteinaceous to hemorrhagic, in fact have various signal intensities; the sticky gelatinous contents or mucin display intensity higher than water on T2 and lower on T2-weighted images relative to serous fluid.
Ovarian Cystadenofibroma
-
Ovarian cystadenofibroma is an uncommon benign epithelial ovarian tumor (1.7 % of ovarian tumors) that displays as cystic tumors with a variable amounts of fibrous stroma.
-
The imaging features are nonspecific and vary from purely cystic to a complex cystic tumor with one or more solid components.
-
MRI: typically appear as multilocular cystic masses with a solid fibrotic component of low signal intensity on T2-weighted images or cystic wall thickening with a low signal intensity on T2-weighted images without any definite solid component.
Ovarian Carcinoma
-
Ovarian cancer is the fifth most common cancer in women and is the leading cause of death from gynecological cancer. The prevalence increases with age, and the peak is reached in the VI-VII decade of life. Tumors arising from the surface epithelium account for 90 % of ovarian cancers and are pathologically designated as serous, mucinous, clear cell, endometrioid, or Brenner (transitional) tumors based on the cell type. Each histologic type is further classified as benign, borderline malignant (tumors of low malignant potential), or malignant, reflecting differences in clinical behavior.
-
Onset of symptoms is insidious, in fact 75 % of patients present with advanced (Stage III or IV) disease. Early symptoms are often vague, such as abdominal discomfort, abdominal distension, or bloating, urinary frequency or dyspepsia. It most commonly presents with a pelvic or abdominal mass that may be associated with pain. Often associated with ascites and metastasises to pelvic and periaortic lymph nodes, as well as over the pelvic and abdominal peritoneum.
-
Serous cystadenocarcinoma is the most common malignant epithelial tumor cell type, accounting for more than half of epithelial tumors: appears as a multiloculated cystic lesion in content serous or hemorrhagic cloudy or intracystic vegetation.
-
CT: Imaging findings that are suggestive of malignant tumors include: a thick, irregular wall, thick septa, papillary projections and a large soft-tissue component with necrosis; see Fig. 6. Ancillary findings of pelvic organ invasion, implants (peritoneal, omental, and mesenteric), ascites, and adenopathy increase diagnostic confidence for malignancy.
-
MRI: The cystic loculi tend to be low in signal on T1 and high on T2-weighted images because of simple fluid content. The content of the different loculi varies from watery to proteinaceous to hemorrhagic, in fact have various signal intensities; the solid components have intermediate signal on T1-weighted images and variable on T2-weighted images and post-MR contrast show enhancement.
Ovarian Metastases
-
Tumors may metastasize to the ovary by direct extension and through lymphatic, hematogenous, or transperitoneal spreads. Metastases to the ovaries account for 10 % of ovarian cancer. The most common primary tumors to involve the ovaries are gastrointestinal carcinoma and (in decreasing order of frequency) pancreatic, breast, and uterine carcinomas. The term “Krukenberg tumor” is reserved for metastases to the ovaries in which malignant signet ring cells invade an abundant and hypercellular stroma.
-
CT: The tumors are usually solid, but cystic areas are common. Ovarian metastases from colon cancer tend to be unilateral and cystic so can be difficult differentiate them from primary ovarian cancer.
-
MRI: The following features are suggestive: bilateral, predominantly solid masses, hypointense solid areas on T2-weighted images, and strong wall enhancement on contrast-enhanced study.
Ovarian Leydig Cell Tumor
-
Leydig cell tumors are very rare ovarian neoplasms (less than 0.5 % of all ovarian tumors), belong to the group of steroid cell tumors. They are usually benign and predominantly seen in postmenopausal women. These lesions contain Leydig cells, lutein cells, and adrenocortical cells in various amounts together with a fibrous stroma and are often associated with a virilization syndrome.
-
MRI shows small (<3 cm) and unilateral solid masses. The signal on T2 sequence is variable, depending on the extent of fibrous stroma and the lipid components appear as areas of elevated signal on T1- and T2-weighted images. Intense enhancement of the nonfibrotic portions after intravenous administration of gadolinium is usually displayed.
Ovarian Vein Thrombosis
-
Ovarian vein thrombosis is an uncommon disorder that may be associated with a variety of inflammatory and malignant conditions. Clinical signs and symptoms are often nonspecific, but prompt recognition and appropriate therapy is essential. Typically, it presents in the setting of postpartum sepsis.
-
Untreated, the condition can result in complications such as extension into the inferior vena cava, involvement of the renal veins, or pulmonary embolism.
-
CT or MRI may be used to demonstrate the thrombosed veins. Sonography, however, has relatively poor detection rates for OVT, because it may not show the entire length of the vein in most cases secondary to body habitus and overlying bowel gas.
-
CT: The thrombosed ovarian vein is visualized as a dilated tubular retroperitoneal structure that contains central low attenuation areas that represent the actual thrombus. Secondary signs associated with OVT are an enlarged uterus that contains fluid and inhomogeneously enhancing parauterine mass believed to be secondary to accompanying pelvic thrombophlebitis.
-
MRI can differentiate between acute and subacute thrombus; generally, the ovarian vein clot is subacute (between 1 week and 1 month), with shortened T1 and prolonged T2 relaxation time and, therefore, is hyperintense on both weightings. Time of flight sequence or contrast-enhanced magnetic resonance venography shows thrombus as filling defects.
Suggested Reading
Turgut AT, Bhatt S, Dogra VS. 2008. Acute painful scrotum, Ultrasound clinic; 3: 93–107.
Jung SE, Lee JM, Rha SE et al. 2002. CT and MRI of ovarian tumors with emphasis on the differential diagnosis. Radiographics; 22: 1305–1325
Montoriol PF, Mons A, Da Ines D, et al. 2013. Fibrous tumours of the ovary: Aetiologies and MRI features, Clinical Radiology; 68: 1276–1283
Iyer VR, Lee SI. 2010. MRI, CT, and PET/CT for Ovarian Cancer Detection and Adnexal Lesion Characterization, American Journal of Roentgenology; 194: 311–321
Park SB, Lee JB. 2014. MRI Features of Ovarian Cystic Lesions, Journal of magnetic resonance imaging; doi: 10.1002/jmri.24579
Rosenkrantz AB, Hindman N, Fitzgerald EF, et al. 2010. MRI Features of Renal Oncocytoma and Chromophobe Renal Cell Carcinoma. AJR; 195: 421–427
Virmani V, Kaza R, Sadaf A et al. 2012. Ultrasound, Computed Tomography, and Magnetic Resonance Imaging of Ovarian Vein Thrombosis in Obstetrical and Non obstetrical Patients. Canadian Association of Radiologists Journal; 69: 109–11
Kim W, Rosen MA, Langer JE et al. 2007. US MRI imaging correlation in pathologic conditions of the scrotum. Radiographics; 27: 1239–1253
Author information
Authors and Affiliations
Rights and permissions
Copyright information
© 2015 Springer-Verlag Italia
About this chapter
Cite this chapter
Panebianco, V., Fütterer, J.J. (2015). O. In: MDCT and MRI in Genitourinary Imaging. A-Z Notes in Radiological Practice and Reporting. Springer, Milano. https://doi.org/10.1007/978-88-470-5705-0_15
Download citation
DOI: https://doi.org/10.1007/978-88-470-5705-0_15
Published:
Publisher Name: Springer, Milano
Print ISBN: 978-88-470-5704-3
Online ISBN: 978-88-470-5705-0
eBook Packages: MedicineMedicine (R0)