
Abstract
The increasing number of industrial accidents, especially when security measures are not strict, renders rare axial injuries more frequent. In this type of injuries, the wrist is being divided into two or more columns with the respective metacarpals. Among fracture dislocations of the wrist, axial dislocations are more frequently associated with soft tissue damage, which is the main determining factor for the outcome; on the other hand, the functional results of the hand are usually unpredictable. The biomechanics of the transverse plane of the distal carpal row, as well as the incidence, the mechanism of injury and the clinical presentation of this rare type of injuries are also examined. In addition, these injuries result in mainly three types of axial dislocations, but the high-energy nature of the injuries could also produce unusual patterns of carpal derangement, which renders them difficult to classify. The management, outcome and complications of axial dislocations are also studied in this chapter.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others



Keywords
These keywords were added by machine and not by the authors. This process is experimental and the keywords may be updated as the learning algorithm improves.
1 Introduction
Malgaigne in 1855 stated that up to that time only three cases of dislocation of Carpometacarpal (CMC) joints had been reported. The first of these cases was an isolated dislocation of the base of the third MC, reported by Blandin in 1844. The second case, also an isolated dislocation of the base of the third MC, was reported by Roux in 1848; and the third case was an isolated dislocation of the base of the second MC reported by Bourguet in 1853. Vigouroux, in 1856, was the first to report a multiple CMC dislocation, involving the bases of the second, third, fourth and fifth MC; Rivington, in 1873, was the first to report a case of multiple dislocations of the bases of all five metacarpals (cited by Waugh and Yancey [1]).
In contradistinction to the thumb CMC joint, injuries of the four ulnar CMC joints are referred to as “finger carpometacarpal” [2] or as “medial four CMC” [3] injuries.
Although CMC injuries of the thumb are not uncommon, those of the base of one or more of the four medial metacarpals are rather rare. The clinical problems arising from injury of the 2nd to 5th CMC joints differ sufficiently from those of the thumb, to warrant separate consideration [4].
Dislocations of the CMC joints disrupt the normal transverse and longitudinal arches of the palm, impair grip strength, and can also affect the balance between intrinsic and extrinsic muscles when there is proximal displacement of the metacarpal. This displacement causes laxity of the extrinsic muscle tendons. Sterling Bunnell in 1944 [5] was the first to emphasize the importance of early anatomical reduction of all CMC dislocations, when he supported that “reduction is necessary to restore muscular balance and proper mechanics of the hand”.
Injuries of the CMC joints are rare and represent less than 1 % of all wrist and hand injuries [6, 7]. Dobyns et al. [8] reported only 3 such injuries in a series of 1,621 fractures and dislocations of the hand and wrist over 3 years at a military hospital (0.18 %).
In cases of CMC joint injuries, the coexistence of a distal carpal row fracture is quite frequent. Garcia-Elias [9] reported that out of 50 patients with traumatic fracture-dislocation of the CMC joints, 13 (26 %) also presented major fracture of the capitate, hamate or trapezoid, which resulted in subluxation or dislocation of the respective metacarpal base.
2 Anatomy
The CMC joints are anatomically stable and their stability is the result of: interlocking saddle joints, complex ligamentous support and dynamic protection by the long flexor and extensor tendons and intrinsic muscles [10].
The distal row of carpal bones forms a fixed transverse arch, while the ring and little fingers on the ulnar side of this arch and the thumb on the radial side, form two mobile longitudinal arches. Both longitudinal arches provide mobility about a fixed central unit comprising the index and middle fingers, whose metacarpals are firmly fixed to the distal carpal row [6] (Fig. 9.1). These bones establish the functional transverse and longitudinal arches of the hand.

The distal carpal row with the longitudinal arches of the index and middle fingers constitute the stable central unit of the hand. With permission from [132]
Experimental studies have indicated less than 1° of motion in the flexion–extension plane at the second ray and 3° at the third ray. Conversely, the flexion–extension motion for the 4th ray is approximately 10°–15° and 15°−30° for the 5th ray [6, 11, 12].
A kinematic analysis of the 2nd through 5th CMC joints using three-dimesional computerized imaging, revealed that the overall flexion–extension motions of the 2nd, 3rd, 4th, and 5th CMC joints, were found to be 11°, 7°, 20° and 27°, respectively; in radial-ulnar deviation 2°, 4°, 7°, and 13°, respectively and in pronation-supination motion 5°, 5°, 27°, and 22°, respectively [13]. This study moreover revealed that the range of motion of the 5th CMC joint reduces by 40 % when the 4th CMC joint is immobilized.
The anatomy of the ligaments and the formation of the articular surfaces of the CMC joints have not been sufficiently described, not only because literature reports are few, but also because there is a considerable number of anatomic varieties [6, 12, 14, 15]. Harwin et al. [12] reported seven dorsal CMC ligaments and eight palmar CMC ligaments of the 2nd through 5th CMC joint. Gurland [6] reported six dorsal CMC ligaments and six palmar CMC ligaments. Nakamura et al. [15] described nine dorsal CMC ligaments and seven palmar CMC ligaments and specifically: dorsally he reported two for the 5th, two for the 4th, three for the 3rd, and two for the 2nd CMC joint (Fig. 9.2) and volarly: one for the 5th, one for the 4th, four for the 3rd, and one for the 2nd CMC joint. Nanno et al. [16] in a three-dimensional analysis of the ligamentous attachments of the 2nd through 5th CMC joints, identified 9 dorsal and 11 palmar CMC ligaments.

The dorsal CMC and the three inter-metacarpal ligaments. With permission from [132]
Additional ligamentous restraint is provided by 3 dorsal and 3 palmar intermetacarpal ligaments that connect the bases of the metacarpals [15], while Nanno et al. [16] identified 4 dorsal and 4 palmar intermetacarpal ligaments of the 2nd through 5th CMC joints. In addition, one intraarticular ligament extending between the 3rd and 4th MC and capitate—hamate was also identified [15, 16], which secures stability even upon rupture of the dorsal and palmar ligaments. However, the role that these ligaments might play in the pathomechanics of axial disruptions and/or CMC dislocations and fracture-dislocations of the carpus has not been well described.
Of particular, importance is the pisometacarpal ligament extending between the pisiform and the ulnovolar base of the 5th metacarpal, through which the flexor carpi ulnaris exerts its effect (Fig. 9.3).

The volar CMC and the three volar inter-metacarpal ligaments. The pisometacarpal ligament is indicated with the asterisk. With permission from [132]
The strong periarticular ligamentous supports of the CMC joints render the anyway rare CMC fracture-dislocations, more frequent than pure dislocations. Although the dorsal ligaments are described as stronger and more distinct than their volar counterparts, dorsal dislocations are more frequent.
The extensor and flexor tendons of the wrist ensure dynamic stabilization by adhering to the base of the 2nd MC (flexor carpi radialis and extensor carpi radialis longus), the base of the 3rd MC (extensor carpi radialis brevis), and the base of the 5th MC (extensor carpi ulnaris and flexor carpi ulnaris via the pisometacarpal ligament) [6, 17] (Fig. 9.4a, b).

The relation of the extensors (a) and flexor (b) tendons with the CMC joints. (ECU Extensor carpi ulnaris, ECRB Extensor carpi radialis brevis, ECRL Extensor carpi radialis longus, FCR Flexor carpi radialis, FCU Flexor carpi ulnaris)
There is more variability and often multiple distinct joint surfaces forming the articulations between adjacent metacarpals and/or adjacent distal carpal bones. Nakamura et al. [15] recognized two types of articulation between the 2nd and 3rd MC, five types of articulation between the 3rd and 4th MCs, while the articulations between the 4th and 5th MCs, between the 2nd MC and the trapezium, and between the trapezoid and the trapezium were all single articulations. The authors also noticed that the area of the 2nd and 3rd CMC joints was found to have the highest incidence (18 %) of carpal coalition. Viegas et al. [18] reported that the joint surfaces between the 4th MC and the capitate and/or the hamate were variable and recognized 5 different types of articulation: A type I, with a single dorsal projection radially, a type II with a double projection radially, a type III with a narrow radioulnar dimension without any projection, a type IV with a narrow radioulnar dimension of the base and a separate small articular surface dorsoradially, and finally, a type V with a broad radioulnar dimension of the articular base of the 4th metacarpal.
The base of the 2nd MC has a cuneiform configuration and articulates with the corresponding surfaces of the trapezium-trapezoid. The 3rd metacarpal base has a dorsoradial styloid process that articulates with the base of the 2nd metacarpal, while ulnarly it has a double articular surface that articulates with the 4th MC and proximally with the capitate. The 4th and 5th metacarpals articulate with the saddle-shaped distal articular surface of the hamate. In general, CMC joints are saddle joints, where the metacarpal base is convex and the distal surface of the carpals is concave (Fig. 9.5). This relationship becomes less pronounced when progressing toward the ulnar column and is a major contributor to the decreased stability that the 4th and 5th metacarpals exhibit. This becomes a major factor in the relative frequency of CMC fracture-dislocations, with the 4th and 5th metacarpals being far more commonly involved [19].

The CMC joints opened dorsally and hinged volarly. The anatomic configuration is described in the text (Tm Trapezium, Td Trapezoid, C Capitate, H Hamate). With permission from [132]
3 Mechanism of Injury
Great and sudden force is required to disrupt the strong periarticular ligamentous supports of the CMC joints. The general consensus in the literature is that the dislocation of the CMC joints can occur either by a direct force on the bases of the metacarpals or by an indirect force transmitted via the metacarpal shafts [20].
These injuries are the result of traffic accidents, falls from heights or striking a hard object with a closed fist. However, a low-energy trauma has also been implicated [10, 21, 22].
In many cases, the axial force is transmitted along the metacarpal shaft, distally to proximally inducing a dislocation at the base of the metacarpal [9, 10, 17, 23–35]. This is the most likely of the mechanisms implicated in the dislocation of the 4th and/or 5th metacarpals, but also of the 2nd metacarpal [36], or of the 2nd to 4th metacarpals [37]. The actions of the ECU and the hypothenar muscles contribute to the deformity of this injury [38].
These injuries are also caused following the application of a force on the palmar surface of the wrist, while the wrist is dorsiflexed (dorsal dislocations), or the application of a force on the dorsal surface of the wrist, while the wrist is palmarflexed (palmar dislocations) [1, 2, 9, 12, 35, 39, 40].
Frequently, CMC injuries are produced after high-energy injuries (e.g., motorcycle accidents) in which, while gripping the handlebars at the time of collision, a significant amount of force is transmitted to the volar aspect of the metacarpal bases producing dorsal dislocations of the medial four CMC joints [2, 3, 20, 41]; in rare cases the handlebars act as a fulcrum causing the metacarpal base to dislocate volarly [42]. Kumar and Malhotra [43] described the need to apply a torsional force in a high-energy incident, to achieve a divergent variant of multiple CMC dislocations.
A rare type of injury, in which a palmarly dislocated 5th metacarpal is associated with a fracture of the hook of the hamate, has been described [44–48]. In this type of injury, a violent contraction of the FCU against a fixed wrist in dorsiflexion [45] or a direct mechanism of production [44, 46–48] has been implicated.
4 Clinical Evaluation
Clinical evaluation reveals either a blatant appearance with excessive swelling, pain, limited range of motion and signs of neurovascular dysfunction or in less severe injuries, mild swelling, and localized sensitivity above the affected joints. Sometimes splaying of the fingers is noted [49]. Waugh and Yansey [1] described the deformity of the more frequent dorsal dislocations as “dinner- fork”, while that of the volar dislocations as a “spade” type of deformity. Massive dorsal edema may obscure the characteristic clinical deformity and this, in combination with insufficient radiological control, are responsible for the high frequency of missed diagnosis [2, 6, 50–53]. Henderson and Arafa [27] reported that in 15 out of 21 cases with dorsal dislocations of the CMC joints, the diagnosis was missed at the emergency department, due to the swelling and use of routine radiographs. Garcia-Elias et al. [9] reported that 6 of their 13 patients had delayed or incorrect diagnosis. Shortening of the fingers, compared to the patient’s healthy hand, will arise suspicion for injury of the CMC joints, once simple radiological examination rules out injury of the fingers or metacarpals (Indian salutation test [54]). With injuries to the 4th or 5th CMC joint, function of the motor division of the ulnar nerve may be affected because of that nerve’s close proximity to the joint [6, 17, 52, 55–57]. This leads to weakness of the interossei and adductor pollicis, which manifests clinically as separation of the long and ring fingers when making a fist [10, 55]. Median nerve function may also be influenced in cases of palmar dislocations of the 2nd and 3rd CMC joints [9, 58], or of delayed reduction of central CMC joint dislocations or due to extensive swelling of the soft tissue. The close proximity of the deep palmar arterial arc with the palmar surface of the 3rd CMC joint must also be considered [17]. Another probable injury is the detachment of the flexor or extensor tendons of the wrist, which insert at the base of the affected metacarpal (Fig. 9.6a–f).

Male, 18 years old, motorcycle accident. A forearm fracture was associated with volar dislocations of the 2nd to 5th metacarpals (a); after forearm reduction, the attempt for closed reduction and pinning of the CMC joints was unsuccessful (b, c); exploration through a dorsal approach revealed the avulsion of the ECRB from the base of the 3rd metacarpal (arrow) (d); a bone anchor was used for tendon reattachment and K-wires were inserted to stabilize the CMC joints (e, f). With permission from [132]
5 Radiological Evaluation
Diagnosis of CMC joint injuries is usually delayed due to insufficient initial radiological control. Gunther [3] stated that subtle findings in the overlapping articular surfaces and minor loss of symmetry may escape the average orthopedic surgeon. He suggested four x-ray projections as being necessary for diagnosing injuries of the CMC joints, which are performed by gradual supination of the hand and wrist, starting with the hand flat and the wrist in neutral position. To the projections mentioned above we have added two more projections to fully demonstrate the CMC joints:
-
1.
Posteroanterior (PA) view with the palm attached to the cassette and the wrist in neutral position. The 3 medial CMC joints should be demonstrated without bony overlap and with their articular surfaces parallel to each other (Fig 9.7 a1–a2).
Fig. 9.7 
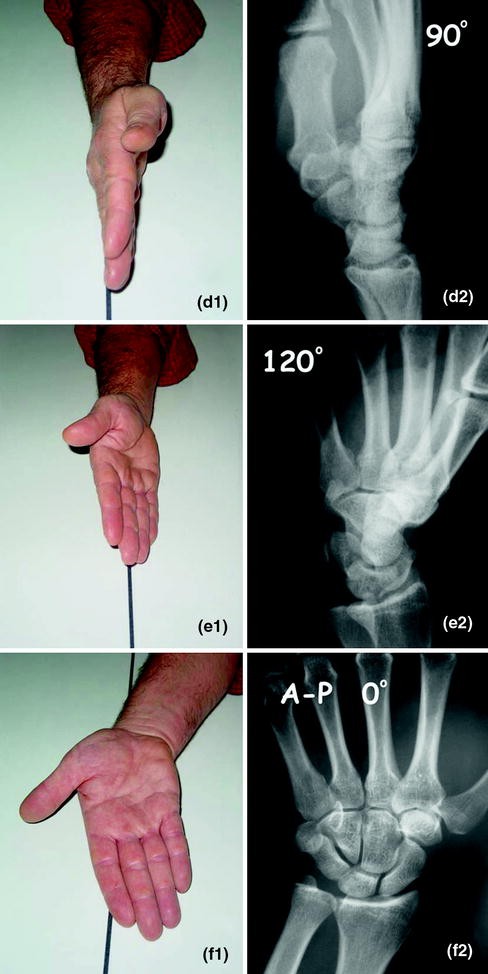
a1–f2 Six X-ray projections fully demonstrating the CMC joints. See text for description. With permission from [132]
-
2.
Elevation of the radial side of the wrist by 30°. This position shows the 2nd, as well as the 1st CMC joints adequately (Fig. 9.7b1–b2).
-
3.
Elevation of the radial side of the wrist by 60° clearly shows the lateral view of the 4th and 5th CMC joints (Fig. 9.7c1–c2).
-
4.
Further rotation to a true lateral projection and with the wrist in neutral, is in fact, a true lateral view of only the 3rd CMC joint (Fig. 9.7d1–d2).
-
5.
Further rotation of the wrist-hand unit by 30° beyond the lateral neutral position (120° from the starting position), is a suitable projection for the anteroposterior (AP) view of the 4th and 5th CMC joints (Fig. 9.7e1–e2).
-
6.
Finally, an AP view with the dorsum of the wrist attached to the cassette, clearly demonstrates the 2nd to 4th CMC joints in AP direction (Fig. 9.7f1–f2).


Parkinson and Paton [59] identified an increase in the angle formed by the long axis of the 2nd and 5th MC on a true lateral radiograph. In cases of dislocation of the 5th CMC joint the CMC angle is increased compared to controls (38.5° compared to 9.8°). A lesser increase in the CMC angle is suggestive of subluxation of this joint.
The PA projection must be performed with the palm attached to the cassette, since substandard positioning results in overlapping of the articular surfaces. Normally, the articular surfaces of any joint must be parallel to each other and the width of the 2nd through 5th joint spaces is uniform measuring 1–2 mm. It's been supported that on the PA radiograph two parallel lines approximating the letter M (parallel M lines) can be consistently drawn to define the normal 2nd through 5th CMC bone relationships. A break in the parallel M lines suggests an abnormality at that site [60–62]. Fisher et al. [61] stated that in simultaneous 4th and 5th CMC joint dislocations, an overlap was observed only at the 5th CMC joint since the flexor and extensor carpi ulnaris draw the dislocated 5th metacarpal proximally.
McDonald et al. [63] calculated the angles between the index and small metacarpal shaft (I-S IMA) and between the long and small metacarpal shaft (L-S IMA) in a lateral radiograph, in patients with ulnar-sided CMC fracture-dislocations. They concluded that both angles are useful screening measurements if they are greater than 10°.
Chmell et al. [64] in the PA view demonstrated the importance of the oblique line through the metacarpal heads for the evaluation of the MC shortening, which accompanies a CMC joint dislocation. This line is drawn tangentially across the distal articular surfaces of the heads of the 3rd, 4th, and 5th metacarpals (Fig. 9.8).

Tomography or computed tomography (CT) scans can also be useful, particularly when there are concomitant injuries to the carpal bones [65].
6 Classification
Although a generally accepted classification does not exist, injuries of the CMC joints can be classified based on different parameters, such as:
-
1.
The number of affected rays (isolated or multiple).
-
2.
The direction of injury (dorsal, palmar, ulnar, divergent).
-
3.
The type and severity of injury (sprain, subluxation, dislocation, fracture-dislocation).
-
4.
The location of the injury (MC base fracture, trans-articular, fracture of the distal carpal row or combinations).
Cain et al. [23] classified injuries of the ulnar CMC joints into 4 types based on the 5th CMC joint. This classification works on the basis that the primary injury is a fracture of the 4th metacarpal and the resulting shortening leads to the hamatometacarpal dislocation. In Type IA, subluxation or dislocation of the 5th MC is accompanied by dorsal CMC ligament disruption; in Type IB the dorsal dislocation of the 5th metacarpal is associated with an avulsion fracture of the dorsal rim of the hamate; in Type II a dorsal hamate comminution is present; and in Type III a coronal splitting of the hamate is present (Figs. 9.9a–d and 9.10a–d). The authors considered Type IB as the most frequent and correlated the type of injury to the stability. They regarded that Type II and III injuries, as grossly unstable requiring open reduction, while type I injuries were reduced, tested for stability and the treatment was adjusted accordingly. The main drawback of this classification is that it does not take into account the isolated dislocations of the 5th CMC joint without fracture of the 4th metacarpal.


However, since 4th and/or 5th metacarpal base intraarticular fractures are common findings that profoundly influence the treatment outcome, Lee et al. [30] recently suggested a new classification for the injuries of the ulnar CMC joints. This classification was based on the fractures of the bases of the 4th and/or 5th metacarpals and on the amount of articular surface of hamate fracture which was assumed as a fact. Three types of injuries were recognized: Type I was defined as less than one-third hamate articular surface involvement; Type II, more than one-third, and Type III, coronal splitting. Each type was divided into four subtypes: (1) absence of intraarticular MC base fracture; (2) fourth MC base fracture; (3) fifth MC base fracture; and (4) both fourth and fifth MC base fractures.
Garcia-Elias et al. [9] modified Cain’s original classification system to include the radial two CMC joints and they moreover considered the stability of the injury following closed reduction as an important factor for classification. It is a common sense that prognosis of stable post-reduction injuries is much better than that of unstable injuries.
According to this classification there are three types of instabilities (Fig. 9.11a–h):

Mayo Clinic’s classification of CMC joint injuries, presented by Garcia-Elias et al. [9]. Although only the central column is depicted, it can be applied to all the affected rays. Type I injuries are considered as transmetacarpal, type II injuries as carpometacarpal, and type III injuries as transcarpal instability. With permission from [132]
-
Type I (Transmetacarpal instability). Caused by fracture at the base of the metacarpal, which may be extrarticular (Ia) or intraarticular (Ib).
-
Type II (Carpometacarpal instability). Results after pure dislocation of the CMC joint (IIa) or a dislocation accompanied by a small chip avulsion fracture of the dorsal rim of the distal row carpal bones (IIb).
-
Type III (Transcarpal instability). This injury may involve only the dorsal and distal corner of the bone (IIIa) or it may be a fracture at the frontal plane of the bone affecting both the proximal and distal articulations (IIIb). Less frequently, the metacarpal along with the distal carpal row bone is dorsally subluxated with (IIIc) or without (IIId) fracture of the palmar surface of the bone. A case which could be classified as type IIId injury is illustrated in Fig. 9.12a–h.
Fig. 9.12 

Male, 46 years old. Five months prior to his examination he reported a left wrist injury, due to its entrapment in a garbage bin in hyperpronation position. He remained undiagnosed. Restriction of dorsal wrist extension, as well as painful osseous swelling at the dorsal side of the wrist, were noted during examination (a, b); radiological control revealed a widening of the lunocapitate joint in the P-A view (arrows) (c) and a dorsal midcarpal subluxation in the L view (d); MRI did not indicate further damage (e); dorsal approach revealed a fixed dorsal subluxation of the distal carpal row (f) (C Capitate, L Lunate, S Scaphoid); due to the difficulties of reduction and despite the good condition of the capitate head’s cartilage, the patient was subjected to a scapholunocapitate fusion; the postoperative X-rays (g, h); the radiological result 1 year later (i, j). This case was considered as type IIId injury according to Mayo Clinic classification [9]


This classification, has in addition a therapeutical importance, since type I (Ia and Ib) has been considered as a stable type and may be treated with longitudinal traction and cast support or percutaneous K-wires, while types II and III are inherently unstable and must be treated with open anatomical reduction.
It must be noted that delineation of these injuries using simple X-rays alone, is quite difficult. Tomography or CT scans at the sagittal plane are required.
7 Acute Injuries of the CMC Joints
Since acute injuries of the CMC joints are frequently the result of high-energy trauma, injuries to other parts of the body or even life-threatening injuries could probably coexist. In addition, complex injuries located at different levels of the same wrist (CMC, intercarpal, radiocarpal) have also been described [66, 67].
Almost every possible combination of injuries has been reported, including the divergent dislocation with some metacarpal bases being dorsally, while others being palmarly dislocated [19, 43, 68–71] (Fig. 9.13a–g). The divergence may have a different location in each case. In some cases, the divergence is localized and involves only two metacarpal bases, e.g., between 4th and 5th CMC joints [46, 72–74], while occasionally all the metacarpal bases are affected and the divergence could be located between the 2nd and 3rd [19, 43] or between the 3rd and 4th [68, 69] metacarpal bases.


Male, 28 years old, car accident. Divergent dislocations with the 2nd and 3rd metacarpals being dorsally dislocated, while the ulnar metacarpals were volarly displaced (a, b, c). With two longitudinal skin incisions dorsally, the dislocations were reduced and stabilized with K-wires (d, e); final radiographic appearance 6 months later (f, g). With permission from [132]
Frick et al. [75] in a retrospective study of 100 CMC dislocations found that in half the cases, lesions were located only within the 5th ray, while carpal or metacarpal fractures were associated with the majority of cases (88 %).
The most common of all CMC joint injuries is considered to be the isolated injury of the 5th CMC joint, which is followed by the simultaneous injury of the 4th and 5th CMC joints (Fig. 9.14a–d).

Case with fracture of the base of the 4th metacarpal and dislocation of the 5th CMC joint (a, b); closed reduction and percutaneous fixation with K-wires (c, d). With permission from [132]
The early recognition of these injuries is essential for satisfactory outcomes. The disability of the hand is severe in untreated cases or in those where treatment is delayed.
Management options include closed reduction and cast immobilization, closed reduction and K-wire fixation, or open reduction and internal fixation. The choice of treatment depends on the severity and stability of the CMC joints and the expertise of the attending physician [10].
7.1 Localized Injuries
Excluding the thumb, the most frequently injured CMC joints are the bases of the ring and small fingers, frequently described as hamatometacarpal fracture-dislocations [9, 23, 35, 76]. A limited number of pure dislocations of the 4th to 5th MC in dorsal [26, 61, 77, 78] (Fig. 9.15a, b) or in volar direction [49] or of a divergent type in different directions [46, 72–74] have been reported. Another rare combination of injuries is the coronal fractures of the body [29] or the dorsal pole of the hamate [25, 31, 76, 79–83] associated with injuries of the bases of the 4th and/or the 5th CMC joints (Fig. 9.16a–g).

Pure dorsal dislocations of the ulnar CMC joints (a), treated with closed reduction and stabilization with two K-wires (b). With permission from [132]


Male, 15 years old. Subluxation of the 5th CMC joint with a coronal fracture of the dorsal pole of the hamate (a, b); 3D CT-scan reconstruction images disclosed the extent of the injury (arrows) (c–d), while CT images disclosed the fracture of the hamate (arrows) (e–f) and in addition a fracture of the volar base of the 4th metacarpal (arrow) (g). The patient refused any further treatment
The most frequently affected isolated CMC joint is the 5th, which is mainly characterized as a dorsal fracture-dislocation. The displacement is analogous to a Bennett’s fracture of the thumb. Despite the fact that 4 types of intraarticular fractures at the base of the 5th MC have been described [33], the most common type involves a radiovolar bone fragment of different size, which remains attached with the 4th metacarpal through the intermetacarpal and palmar CMC ligaments, while the remainder of the 5th metacarpal is displaced ulnarly and dorsally to a varying degree, due to the action of extensor carpi ulnaris and the opponent digiti minimi muscle (Fig. 9.17a, b).

The most common type of fracture-dislocation of the 5th CMC joint. A small ulnovolar bone fragment remains attached to the 4th metacarpal through the ligaments, while the 5th metacarpal is ulnarly and dorsally displaced due to the action of ECU tendon and the direction of pull by the hypothenar muscles (ODM Opponent digiti minimi) (a); a clinical analogue of the injury (b). With permission from [132]
In addition, there are reported cases of isolated dislocations of the 5th CMC in dorsal [28, 84–88], or more rarely, in volar direction [45, 48, 60, 89] (Fig. 9.18a, b). There are two types of volar dislocations: radial and ulnar. In the radial type, which is the most common, all of the ligamentous and tendinous attachments are torn and usually open reduction is required using a volar-ulnar surgical approach. In the ulnar type, the pisometacarpal ligament remains intact preventing excessive displacement of the fifth metacarpal, which however overlaps the hamate and shortens the digit, due to the action of the flexor and extensor carpi ulnaris and the hypothenar muscles. Sometimes, the intact pisometacarpal ligament prevents excessive displacement, thus rendering stress radiographs necessary for correct diagnosis [89]. In this type of injury, the problem is usually not the reduction itself, but rather maintaining the reduction [6], thus percutaneous K-wire fixation of the joint is necessary.

Rare volar fracture-dislocation of the 5th CMC joint (a), which was treated with closed reduction (b). With permission from [132]
Closed reduction is accomplished with local or general anesthesia, longitudinal traction of the finger(s), direct pressure at the bases of the affected metacarpals and dorsal extension of the head of the MC, if the most common dorsal dislocations of the CMC joints are considered. Although successful stabilization of the wrist after the reduction has been suggested only with plaster [7, 90, 91], most authors advocate using percutaneous K-wires fixation. K-wires are percutaneously inserted from the base of the metacarpal to the hamate or the adjacent 4th metacarpal, from the dorsal and ulnar surface of the wrist, while taking care not to disrupt the function of the extension mechanism. Recently, Mozaffarian et al. [92] described a safe corridor for pinning of the 5th CMC joint to prevent iatrogenic injury to the ulnar nerve and tendons; it is located 2 cm distal to the joint at an angle of 20°–30° to the coronal plane, from 10° volar to dorsal to 20° dorsal to volar direction in the saggital plane. Once stable reduction has been achieved, a direct, active, and passive mobilization of the fingers and wrist must commence within 1–2 weeks. The K-wires will be maintained for at least 6 weeks, although keeping them for up to 12 weeks has also been suggested [11]. After the K-wires are removed, the patient starts grip strengthening exercises. The importance of early controlled mobilization has been emphasized [93] for reducing postinjury complications (stiffness of hand joints, tendon adhesions, and intrinsic muscle weakness).
Slutsky [94] described an arthroscopic technique for reduction and percutaneous fixation of 5th CMC fracture-dislocations. The technique is considered useful especially in cases where the articular fracture fragment is volar and difficult to visualize and reduced using a dorsal approach.
Rarer are the isolated injuries of the 2nd and/or 3rd CMC joint. In literature there are reported cases of dorsal [36, 95–97] or palmar dislocation [98, 99] of the 2nd CMC joint, dorsal non-reducible dislocation of the 2nd CMC joint due to interference of the extensor carpi radialis brevis [100, 101] and finally, palmar dislocations of the 2nd to 3rd CMC joint [12, 42, 58]. Although K-wire fixation is recommended to prevent recurrent dislocation, it has been suggested that it is not always necessary because of the intrinsic stability of the joint [101].
Open reduction and internal fixation, are clearly indicated in the following cases:
-
1.
Unsuccessful closed reduction.
-
2.
Irreducible dislocations due to interposed soft tissue or fracture fragments.
-
3.
In cases of delayed diagnosis, where the contraction of soft tissues hinders closed reduction.
-
4.
Complex fracture-dislocations.
Incision of the skin for the isolated injury of a CMC joint is usually dorsal curvilinear or of S type, with the transverse part of the incision located above the joint.
7.2 Multiple Injuries
In general, multiple injuries of the CMC joints cause significant swelling of soft tissue that obstructs closed reduction, which even if achieved, is difficult to maintain. The inability to achieve closed reduction is sometimes due to interposed joint capsule in the CMC joints [102]. There have been reported cases of dislocations or fracture-dislocations of all five CMC joints [103–112], dorsal dislocations of the 2nd to 5th CMC joint [22, 54, 67, 102, 113–118] (Figs. 9.19a–d and 9.20a–d), palmar dislocations of the 2nd to 5th CMC joint [90, 119–121], palmar dislocations of the 2nd to 4th CMC joint [122], or fracture of the base of the 3rd and dorsal dislocations of the 4th and 5th CMC joints [51].

A case of dorsal dislocations of the 2nd to 5th CMC joints associated with a fracture of the volar part of the capitate (arrows) (a, b); it was treated with open reduction and fixation with K-wires (c, d). With permission from [132]

Male, 40 years old, motorcycle accident. Dorsal dislocations of the 2nd to 5th CMC joints (a, b); he was treated with closed reduction and K-wires insertion, while the 4th CMC joint was reduced coincidently with the 3rd CMC joint (c, d). With permission from [132]
Garcia-Elias [2] stated that the treatment of choice for the relatively stable type II injuries (according to his classification) is early closed reduction, distal-to-proximal pin fixation, and specific cast support. Types I and III, by contrast, because of the presence of a displaced intraarticular fracture, are inherently unstable, thus open treatment, which allows identification and treatment of small osteochondral fractures, debridement of debris in the joints, accurate reduction and proper stabilization, is the method of choice. Rare cases have been reported with coronal fractures through the capitate and hamate [123] or through the capitate, hamate, and trapezoid [124], both of which necessitated a CT-scan for diagnosis. Both these cases probably constitute a type IIIb injury (according to Garcia-Elias classification) and were treated with open reduction and internal fixation.
A major distal carpal row bone fracture is frequently associated with CMC dislocations [9, 125] and in such cases open reduction and fixation of the fractured bone with K-wire(s) or with a compression screw is considered the treatment of choice (Fig. 9.21a–f).

Male, 30 years old, motorcycle accident. Dorsal dislocations of the 2nd to 5th CMC joints. The injuries of the 2nd and 3rd CMC joints were of IIa type, that of the 4th CMC joint was of Ia type and that of the 5th CMC joint was of IIIb type (associated with a fracture of the body of the hamate in the coronal plane) (arrows), according to the Mayo classification (a, b); he was treated with open reduction and K-wires stabilization including the hamate fracture (c, d); final radiographic appearance 4 years later (e, f). With permission from [132]
The dislocated joints are usually approached from the dorsal side and the skin incision may be longitudinal [17, 126] or transverse [46, 50, 69, 70, 115]. Alternatively, we may approach all 4 bases of the metacarpals, using two longitudinal skin incisions (between 2nd to 3rd and 4th and 5th CMC joint). Cutaneous nerves are protected and the extensor tendons are retracted to gain access to the dislocated joints. Reconstruction of the transverse carpal row starts with the reduction and stabilization of the base of the 3rd [6, 10, 39, 43, 121] or of the 2nd [67] metacarpal. When all 4 metacarpals are dislocated, stabilization of each joint separately is not necessary, as some of the interosseous ligaments usually remain intact, which helps to stabilize the adjacent metacarpal [3, 6, 68]. The wires must be placed so as to avoid the extensor tendons, since early mobilization is desirable.
The pins are removed at 4–6 weeks postoperatively. An alternative method to stabilize the dislocated joints with K-wires, avoiding the risk of damaging tendons and nerves, is the technique proposed by Foster [26], called “intramedullary stress sharing fixation” (originally described for ulnar CMC joints’ dislocations) (Fig. 9.22a–d).

Fosters’ [26] stabilizing method of a dislocated CMC joint using intramedullary K-wire: the dislocated joint (a); insertion of the K-wire from the proximal to the distal side into the intramedullary canal, exiting dorsally at the flexed MP joint and through the central portion of the extensor tendon (b); reduction of the dislocation and proximally advancing of the K-wire into the corresponding bone of the distal carpal row after excessive wrist palmarflexion (c); the pin is withdrawn proximally to disengage the head of the metacarpal; its proximal portion is curved and cut below the skin level (d)
8 Chronic Injuries of the Carpometacarpal Joints
There is no consensus for the definition of a chronic CMC dislocation. Most authors believe that an injury dated more than 3 to 6 months is defined as chronic [17, 127], while Ahmad and Plancher [128] defined CMC dislocations as chronic when there is a delay in diagnosis and treatment of at least 6-12 weeks. Usually, chronic cases are expressed with deformity, localized sensitivity, reduced muscle strength and in the long term, symptoms of arthritic changes (Figs. 9.23a, b and 9.24a–g).

Neglected dorsal CMC fracture-dislocations (a, b). The patient complained for dysfunction of the extensor tendons. With permission from [132]


Male, 29 years old, with a painful osseous swelling at the dorsal side of the wrist (a); radiographs revealed old unreduced dorsal dislocations, mainly of the 2nd to 3rd CMC joints (b, c); for the fusion of the affected joints and to regain the length of the shortened metacarpals, two small external fixators were used (d, e); radiographic appearance after the hardware removal (f, g)
Although there had been early reports that chronic dislocations or subluxations of the CMC joints do not result in any disability [1, 68], this view today has no advocates. Green [129] supported that injuries more than 3 weeks old do not require any treatment.
In cases with mild symptoms such as slight residual subluxation, conservative treatment is probably best [17], while in cases with marked deformity an attempt for delayed open reduction could be successful as late as 3–6 months postinjury [38]. Imbriglia [127] reported successful open reduction of the 2nd to 5th CMC joints 3 months post injury without the need for arthrodesis, due to the integrity of the articular cartilage. Prokuski and Eglseder [67] stated that delay of up to 4 weeks did not adversely affect results.
In any case, regardless of the time elapsed, the management will depend on the complaints, while if operative treatment is needed, the appropriate method will depend on the reducibility of the CMC joints, and the condition of articular cartilage.
9 Long-Term Results
Few reports document long-term follow-up in cases of multiple carpometacarpal dislocations. However, it is uniformly accepted that with early diagnosis and prompt treatment with restoration of normal anatomical reduction, excellent results may be expected [9, 10, 35, 41]. In addition, the outcome has generally been favorable as long as the reduction is maintained.
It has been suggested [10, 121] that delayed diagnosis and treatment will usually result in an undesirable outcome of pain, reduced grip strength and degenerative arthritis and that up to 43 % of patients with neglected single CMC joint injuries will experience residual pain and impaired function. However, with appropriate management, up to 87 % of patients with CMC joint injuries will return to full work and sporting activities with negligible pain.
Gunther [3] stated that open reduction with K-wire fixation results in excellent hand function. Grip strength returns to normal and the only residual symptoms of the fracture-dislocation are usually mild aching during changes of weather or during extremely heavy work.
Garcia-Elias et al. [9] reported that patient satisfaction when treated in the acute phase is high; on the contrary, delayed treatment, even with bone grafting and stabilization until fracture consolidation, had an increased incidence of mild residual symptoms, including weakness of grasp or pinch and tenderness at the CMC area. In addition, delayed diagnosis may lead to fracture nonunion due to vascular or mechanical factors, with adverse consequences (muscular imbalance, reduced grip strength, and arthritis).
Lawlis and Gunther [70] suggested that most adverse results concern patients with 2nd and 3rd MC injuries or those having additional injury of the ulnar nerve.
Lundeen and Shin [33] reported clinical results of 22 patients with intraarticular fractures of the base of the 5th MC treated by closed reduction and cast immobilization. After an average follow-up of 43 months, twenty patients reported excellent or good results and two reported fair or poor results. Nine of those patients (41 %) had mild arthrosis of the CMC joint. Yildiz et al. [112] supported that mild degenerative changes in the CMC joints may be present radiographically on long-term follow-up. However, the functional results appear to be good, provided that open reduction and internal fixation of the dislocations have been achieved.
10 Arthrodesis of CMC Joints
In cases of chronic instability or post-traumatic arthritis of CMC joints not responding to conservative treatment, arthrodesis constitutes the operation of choice [6, 50]. Arthrodesis of the 2nd, 3rd or both CMC joints does not result in any functional deficiency, because the motion range of these joints is limited, while the method has been suggested as a primary treatment for unstable fracture-dislocations [50, 70, 126]. In addition, the need for CMC arthrodeses tends to be higher among patients with more associated injuries [67]. Even arthrodesing the mobile 4th and 5th CMC joints will not cause any problems, provided that the joints are fused in sufficient flexion to maintain the normal curvature of the distal metacarpal arch when making a fist [6]. Because mobility of the 5th CMC joint is greater than the 4th, it should be fused in greater flexion. Arthrodesis is performed with the use of a sliding inlay graft, an iliac strut graft or a corticocancellous graft from the distal radius, which is stabilized with K-wires (Fig. 9.25a–g). Fusions usually heal within 8 weeks. As an alternative to arthrodesis, resectional arthroplasty with interposition of a rolled tendon spacer has been applied [130] or if the 5th CMC joint is involved, a “stabilized arthroplasty” suggested by Dubert and Khalifa [131] can be applied. The latter technique is based on the resection of the base of the 5th metacarpal, whereas the length of the fifth digit ray is restored by fusion to the adjacent 4th metacarpal.


Male, 35 years old, with a two-year-old malunion of the proximal 4th metacarpal, with arthritic changes of the dorsally subluxated 5th CMC joint (a, b); the disruption of the normal curvature of the metacarpal heads when making a fist, is showed (c); corrective osteotomy of the 4th metacarpal using a small plate and fusion of the 5th CMC joint (d, e); postoperative X-rays (f, g)
g
References
Waugh RL, Yancey AG (1948) Carpometacarpal dislocations. With particular reference to simultaneous dislocation of the bases of the fourth and fifth metacarpals. J Bone Joint Surg Am 30:397–404
Garcia-Elias M (2001) Carpometacarpal fractures and fractures dislocations. In: Watson K, Weinzweig J (eds) The wrist. Lippincott Williams & Wilkins, Philadelphia, pp 255–268
Gunther SF (1997) Medial four carpometacarpal joints. In: Lichtman DM, Alexander AH (eds) The wrist and its disorders, 2nd edn. WB Saunders Co, Philadelphia, pp 459–472
Watt N, Hooper G (1987) Dislocation of the trapezio-metacarpal joint. J Hand Surg [Br] 12(2):242–245
Bunnell S (1944) Fractures of metacarpals and phalanges. In: Bunnell S (ed) Surgery of the hand. JB Lippincott, Philadelphia, pp 528–531
Gurland M (1992) Carpometacarpal joint injuries of the fingers. Hand Clin 8:733
Mueller JJ (1986) Carpometacarpal dislocations: report of five cases and review of the literature. J Hand Surg [Am] 11(2):184–188
Dobyns JH, Linscheid RL, Cooney WP (1983) Fractures and dislocations of the wrist and hand, then and now. J Hand Surg [Am] 8:687–690
Garcia-Elias M, Bishop AT, Dobyns JH et al (1990) Transcarpal carpometacarpal dislocations excluding the thumb. J Hand Surg [Am] 15:531–540
Woon CYL, Chong KC, Low CO (2006) Carpometacarpal joint dislocations of the index to small finger: three cases and a review of the literature. Injury Extra 37:466–472
Gunther SF (1984) The carpometacarpal joints. Orthop Clin North Am 15:259–277
Harwin SF, Fox JM, Sedlin ED (1975) Volar dislocation of the bases of the second and third metacarpals. J Bone Joint Surg [Am] 57:849–851
El-Shennawy M, Nakamura K, Patterson RM et al (2001) Three-dimensional kinematic analysis of the second through fifth carpometacarpal joints. J Hand Surg [Am] 26:1030–1035
Joseph RB, Linscheid RL, Dobyns JH et al (1981) Chronic sprains of the carpometacarpal joints. J Hand Surg [Am] 6:172–180
Nakamura K, Patterson RM, Viegas SF (2001) The ligament and skeletal anatomy of the second through fifth carpometacarpal joints and adjacent structures. J Hand Surg [Am] 26:1016–1029
Nanno M, Buford WL, Patterson RM et al (2007) Three-dimensional analysis of the ligamentous attachments of the second through fifth carpometacarpal joints. Clin Anat 20:530–544
Rawles JG Jr (1988) Dislocations and fracture-dislocations at the carpometacarpal joints of the fingers. Hand Clin 4:103–112
Viegas SF, Crossley M, Marzke M et al (1991) The fourth carpometacarpal joint. J Hand Surg [Am] 16:525–532
Lewicky YM, Sheppard JE (2009) Closed-reduction percutaneous pinning of a complex divergent carpometacarpal fracture-dislocation involving the 4 ulnar carpometacarpal joints. Am J Orthop 38(4):191–193
Kirkham SG, Gray RJ (2004) Multiple carpometacarpal dislocations and an ipsilateral scapho-trapezium-trapezoid fracture-dislocation: a rare pattern of injury. J Orthop Surg 12(2):267–269
Griffiths MA, Moloney DM, Pickford MA (2005) Multiple carpometacarpal dislocations after a low-impact injury: a missed diagnosis. J Trauma 58(2):391–392
Oni O, Mackenny R (1986) Multiple dislocations of the carpometacarpal joints. J Hand Surg [Br] 11(1):47–48
Cain JE, Shepler TR, Wilson MR (1987) Hamatometacarpal fracture-dislocation: classification and treatment. J Hand Surg [Am] 12:762–767
Dunkerton M, Singer M (1985) Dislocation of the index metacarpal and trapezoid bones. J Hand Surg [Br] 10(3):377–378
Fakih RR, Fraser AM, Pimpalnerkar AL (1998) Hamate fracture with dislocation of the ring and little finger metacarpals. J Hand Surg [Br] 23(1):96–97
Foster RJ (1996) Stabilization of ulnar carpometacarpal dislocations or fracture dislocations. Clin Orthop 327:94–97
Henderson JJ, Arafa MA (1987) Carpometacaral dislocation: an easily missed diagnosis. J Bone Joint Surg [Br] 69:212–214
Laforgia R, Specchiulli F, Mariani A (1990) Dorsal dislocation of the fifth carpometacarpal joint. J Hand Surg [Am] 15:463–465
Langenhan R, Hohendorff B, Probst A (2011) Coronal fracture dislocation of the hamate and the base of the fourth metacarpal bone: a rare form of carpometacarpal injury. Handchir Mikrochir Plast Chir 43(3):140–146
Lee SU, Park IJ, Kim HM et al (2012) Fourth and fifth carpometacarpal fracture and dislocation of the hand: new classification and treatment. Eur J Orthop Surg Traumatol 22:571–578
Liaw Y, Kalnins G, Kirsh G et al (1995) Combined fourth and fifth metacarpal fracture and fifth carpometacarpal joint dislocation. J Hand Surg [Br] 20:249–252
Lilling M, Weinberg H (1979) The mechanism of dorsal fracture dislocation of the fifth carpometacarpal joint. J Hand Surg [Am] 4:340–342
Lundeen JM, Shin AY (2000) Clinical results of intraarticular fractures of the base of the fifth metacarpal treated by closed reduction and cast immobilization. J Hand Surg [Br] 25:258–261
Storm JO (1988) Traumatic dislocation of the fourth and fifth carpo-metacarpal joints: a case report. J Hand Surg [Br] 13(2):210–211
Topper S, Wood M (2010) Athletic injuries of the wrist. In: Cooney WP (ed) The Wrist. Diagnosis and operative treatment, 2nd edn. Wolters Kluwer/Lippincott Williams, Philadelphia, pp 1153–1186
Van der Lei B, Klasen HJ (1992) Dorsal carpometacarpal dislocation of the index finger: a report of three cases and a review of the English-language literature. J Trauma 32:789–793
Jameel J, Zahid M, Abbas M et al (2012) Volar dislocation of second, third, and fourth carpometacarpal joints: a rare and easily missed diagnosis. J Orthop Traumatol. doi:10.1007/s10195-012-0181-3
Bora F, Disizian NH (1974) The treatment of injuries to the carpometacarpal joint of the little finger. J Bone Joint Surg Am 56(7):1459–1463
Hartwig RH, Louis DS (1979) Multiple carpometacarpal dislocations. A review of four cases. J Bone Joint Surg [Am] 61(6):906–908
Mullan GB, Lloyd GJ (1980) Complete carpal disruption of the hand. The Hand 12(1):39–42
DeBeer JV, Maloon S, Anderson P (1989) Multiple carpo-metacarpal dislocations. J Hand Surg [Br] 14:105–108
Kumar P (2010) Dislocation of second and third carpometacarpal joints along with fracture of first metacarpal—possible mechanisms. J Hand Microsurg 2(2):85–86
Kumar R, Malhotra R (2001) Divergent fracture-dislocation of the second carpometacarpal joint and three ulnar carpometacarpal joints. J Hand Surg [Am] 26:123–129
Chen VT (1987) Dislocation of carpometacarpal joint of the little finger. J Hand Surg [Br] 12(2):260–263
Garcia-Elias M, Rossignani P, Cots M (1996) Combined fracture of the hook of the hamate and palmar dislocation of the fifth carpometacarpal joint. J Hand Surg [Br] 21:446–450
Moriya K, Saito H, Takahashi Y et al (2011) Divergent fracture-dislocation of the hamatometacarpal joint: case report. J Hand Surg [Am] 36(1):47–51
North ER, Eaton RG (1980) Volar dislocation of the fifth metacarpal: report of two cases. J Bone Joint Surg Am 62:657–659
Tountas AA, Kwok JM (1984) Isolated volar dislocation of the fifth carpometacarpal joint. Case report. Clin Orthop 187:172–175
Prokopis P, Weiland A (2008) Volar dislocation of the fourth and fifth carpometacarpal joints: a case report and review of the literature. HSSJ 4:138–142
Carroll RE, Carlson E (1989) Diagnosis and treatment of injury to the second and third carpometacarpal joints. J Hand Surg [Am] 14:102–107
Gaheer RS, Ferdinand RD (2011) Fracture dislocation of carpometacarpal joints: a missed injury. Orthopedics 34(5):399
Guimaraes RM, Benaissa S, Moughabghab M et al (1996) Carpometacarpal dislocations of the long fingers. Apropos of 26 cases with review of 20 cases. Rev Chir Orthop Reparatrice Appar Mot 82:598–607
Pullen C, Richardson M, McCullough K et al (1995) Injuries to the ulnar carpometacarpal region: are they being underdiagnosed? Aust N Z J Surg 65:257–261
Iqbal MJ, Saleemi A (2003) Indian salutation test in acute dorsal carpometacarpal joint dislocation of the ulnar four fingers. Am J Emerg Med 21:74–76
Gore DR (1971) Carpometacarpal dislocation producing compression of the deep branch of the ulnar nerve. J Bone Joint Surg Am 53:1387–1390
Pimpalnerkar AL, Fakih R, Thomas AP (1997) Carpometacarpal dislocation producing transient motor neurapraxia of the ulnar nerve. Injury 28:397–400
Sreedharan S, Chew W (2008) Re: Isolated fifth carpometacarpal joint volar dislocation with ulnar neuropathy. J Hand Surg [Br] 33(2):219–220
Weiland AJ, Lister GD, Villareal-Rios A (1976) Volar fracture dislocations of the second and third carpometacarpal joints associated with acute carpal tunnel syndrome. J Trauma 16:672–675
Parkinson RW, Paton RW (1992) Carpometacarpal dislocation: an aid to diagnosis. Injury 23:187–188
Fischer JW, Waseem M, Gambhir A et al (2002) Ulnopalmar dislocation of the fifth carpometacarpal joint. A rare injury. Acta Orthop Belg 68:175–177
Fisher MR, Rogers LF, Hendrix RW (1983) Systematic approach to identifying fourth and fifth carpometacarpal joint dislocations. Am J Roentgenol 140:319–324
Yin Y, Mann F, Gilula LA et al (1996) Roentgenographic approach to complex bone abnormalities. In: Gilula LA, Yin Y (eds) Imaging of the wrist and hand. Saunders, Philadelphia, pp 293–318
McDonald LS, Shupe PG, Hammel N et al (2012) The intermetacarpal angle screening test for ulnar-sided carpometacarpal fracture-dislocations. J Hand Surg [Am] 37(9):1839–1844
Chmell S, Light TR, Blair SJ (1982) Fracture and fracture dislocation of ulnar carpometacarpal joint. Orthop Rev 11:73–80
Gehrmann SV, Grassmann JP, Schneppendahl J et al (2011) Treatment strategy for carpometacarpal fracture dislocation. Unfallchirurg 114(7):559–564
Nourissat G, Mudgal C, Ring D (2008) Bridge plating of the wrist for temporary stabilization of concomitant radiocarpal, intercarpal, and carpometacarpal injuries: a report of two cases. J Orthop Trauma 22:368–371
Prokuski L, Eglseder W (2001) Concurrent dorsal dislocations and fracture-dislocations of the index, long, ring, and small (second to fifth) carpometacarpal joints. J Orthop Trauma 15(8):549–554
Agarwal A, Agarwal R (2005) An unusual farm injury: carpometacarpal joint dislocations. J Hand Surg [Br] 30(6):633–634
Gunther SF, Bruno PD (1985) Divergent dislocation of the carpometacarpal joints: a case report. J Hand Surg [Am] 10:197–201
Lawlis JF III, Gunther SF (1991) Carpometacaral dislocations: long-term follow-up. J Bone Joint Surg Am 73:52–59
Loudyi D, Amar MF, Chbani B et al (2009) Divergent carpometacarpal joint dislocations of the ulnar four fingers (a case report). Chir Main 28(3):168–170
Busa R, Internullo G, Caroli A (1998) Divergent dislocation of the fourth and fifth carpometacarpal joints. J Hand Surg [Am] 23(3):529–531
Chalidis B, Dimitriou C (2012) Treatment of neglected divergent dislocation of hamatometacarpal complex with a circular spider plate. J Hand Surg [Eur] 37(9):897–899
Dillon J, Street J, Mahalingham K (2005) Divergent dislocation of the ring and little finger carpometacarpal joints–a rare injury pattern. Acta Othop Belg 71(3):353–356
Frick L, Mezzadri G, Yzem I et al (2011) Acute carpometacarpal joint dislocation of the long fingers: study of 100 cases. Chir Main 30(5):333–339
Loth TS, McMillan MD (1988) Coronal dorsal hamate fractures. J Hand Surg [Am] 13(4):616–618
Helal B, Kavanagh TG (1977) Unstable dorsal fracture-dislocation of the fifth carpometacarpal jont. Injury 9:138–142
Vandeweyer E, Botero L, Coessens BC (2002) Dorsal carpometarcarpal dislocation of ulnar fingers. A case report. Acta Chir Belg 102:279–280
Bonacina P, Faggioli AM, Gaetani G et al (2005) Complex fracture-dislocation of the carpometacarpal joint associated with a fracture of the hamate: a case report. J Orthop Traumatol 6(2):98–100
Kaneko K, Ono A, Uta S et al (2002) Hamatometacarpal fracture-dislocation: distinctive three dimensional computed tomographic appearance. Chir Main 21(1):41–45
Kerr HD (1992) Hamate-metacarpal fracture dislocation. J Emerg Med 10(5):565–568
Schrott E, Wessinghage D (1983) Course of treatment of a luxation of the 4th and 5th carpometacarpal joint with hamate involvement. Handchir Mikrochir Plast Chir 15(1):25–28
Syed AA, Agarwal M, Giannoudis PV et al (2002) Dorsal hamatometacarpal fracture-dislocation in a gymnast. Br J Sports Med 36(5):380–382
Hennig K (1986) Isolated dislocation of the 5th carpometacarpal joint. A case report. Unfallchirurg 89:574–575
Khodadadyan C, Hoffmann R, Moazami-Goudarzi Y et al (1995) Double dislocation of the fifth metacarpal. J Hand Surg [Br] 20:253–254
Tingart M, Bathis H, Bouillon B et al (2000) Dorsal carpometacarpal dislocation of the fifth finger: discussion of diagnosis and therapy on two cases. Unfallchirurg 103:76–80
Valente M, Saggin G, Alecci V (2009) Pure isolated dorsal dislocation of the fifth carpometacarpal joint. Chir Organi Mov 93(2):97–100
Vijayasekaran VS, Briggs P (2000) Isolated dorsal dislocation of the 5th carpometacarpal joint. Hand Surg 5:175–180
Yamakado K, Hashimoto F, Nagata S et al (2000) Isolated palmar dislocation of the fifth carpometacarpal joint diagnosed by stress X-rays. Arch Orthop Trauma Surg 120(9):529–530
Bajekal RA, Kotwal PP, Menon D (1992) Closed volar dislocations of the four ulnar carpometacarpal joints. Injury 23:355–356
Storken G, Bogie R, Jansen EJP (2011) Acute ulnar carpometacarpal dislocations. Can it be treated conservatively? A review of four cases. Hand 6(4):420–423
Mozaffarian K, Vosoughi AR, Hedjazi A et al (2012) The safest direction of percutaneous pinning for achieving firm fixing of the fifth carpometacarpal joint. J Orthop Sci 17(6):757–762
Bell T, Chinchalkar SJ, Faber K (2010) Postoperative management of carpometacarpal joint fracture dislocation of the hand: a case report. Can J Plast Surg 18(3):e37–e40
Slutsky DJ (2011) Arthroscopic reduction and percutaneous fixation of fifth carpometacarpal fracture dislocations. Hand Clin 27(3):361–367
Benoit O, Polveche G, Barbier J et al (2001) Fracture-dislocation of the second carpometacarpal joint. Case report and review of the literature. Chir Main 20(5):397–402
Carneiro RS, Rancatore E (2000) Dorsal dislocation of the index carpometacarpal joint. J Emerg Med 18:21–22
Santini AJ, Douglas DL (1998) Second carpometacarpal joint dislocation: an impossible situation? Int J Clin Pract 52:517–518
Schutt RC, Boswick JA, Scott FA (1981) Volar fracture-dislocation of the carpometacarpal joint of the index finger treated by delayed open reduction. J Trauma 21:986–987
Thomas WO, Gottliebson WM, D’Amore TF et al (1994) Isolated palmar displaced fracture of the base of the index metacarpal: a case report. J Hand Surg [Am] 19:455–456
Ho PK, Choban SJ, Eshman SJ et al (1987) Complex dorsal dislocation of the second carpometacarpal joint. J Hand Surg [Am] 12:1074–1076
Köse O, Islam C (2008) Re: irreducible dorsal dislocation of the index carpometacarpal joint. J Hand Surg [Br] 33(2):217–218
Peace WJ, Abrams RA (2010) Simultaneous dorsal dislocations of the carpometacarpal joints of all four fingers. Orthopedics 33(2):121–123
Edwards A, Pike J, Bird J (2000) Simultaneous carpometacarpal joint dislocations of the thumb and all four fingers. Injury 31:116–118
Fayman M, Hugo B, de Wet H (1988) Simultaneous dislocation of all five carpometacarpal joints. Plast Reconstr Surg 82:151–154
Hsu KY, Wu CC, Wang KC et al (1993) Simultaneous dislocation of the five carpometacarpal joints with concomitant fractures of the tuberosity of the trapezium and the hook of the hamate: case report. J Trauma 35:479–483
Jebson PJ, Engber WD, Lange RH (1994) Dislocation and fracture-dislocation of the carpometacarpal joints. Orthop Rev 1994:19–28
Kneife F (2002) Simultaneous dislocations of the five carpometacarpal joints. Injury 33:846
Pérez-Serna AG, Figueroa-Cal y Mayor F (2009) Multiple carpometacarpal fracture-dislocation. Acta Ortop Mex 23(3):149–152
Petersen MB, Nielsen PT, Nielsen LS (1992) Simultaneous occurrence of trapezium-scaphoid-trapezoid dislocation and multiple carpometacarpal fracture dislocations. A case report. Acta Orthop Scand 63:104–105
Reznick SM, Greene TL, Roeser W (1985) Simultaneous dislocation of the five carpometacarpal joints. Clin Orthop 192:210–214
Schortinghuis J, Klasen HJ (1997) Open reduction and internal fixation of an unusual multiple carpometacarpal dislocation using one plate: a case report. Injury 28:701–703
Yildiz M, Baki C, Sener M (1995) Isolated dislocation of all five carpometacarpal joints. J Hand Surg [Br] 20:606–608
Mabee JR, Lee TJ, Halus S (1997) Dorsal dislocation of the four ulnar metacarpals. Am J Emerg Med 15:408–411
Mito K, Nakamura T, Sato K et al (2008) Dorsal dislocations of the second to fifth carpometacarpal joints: a case report. Hand Surg 13(2):129–132
Pankaj A, Malhotra R, Bhan S (2005) Isolated dislocation of the four ulnar carpometacarpal joints. Arch Orthop Trauma Surg 125:541–544
Pansard E, Kaba A, Peyroux LM et al (2009) Combined carpometacarpal dislocations, hand lesions and fractures of the two bones of the forearm: a report of two cases. Chir Main 28(4):250–254
Siddiqui YS, Zahid M, Sabir AB (2011) Multiple carpometacarpal fracture dislocation of the hand – An uncommon pattern of injury which is often missed : a case report with review of literature. JCDR 5(3):618–620
Smith GR, Yang SS, Weiland AJ (1996) Multiple carpometacarpal dislocations. A case report and review of treatment. Am J Orthop 25(7):502–506
Kleinman WB, Grantham SA (1978) Multiple volar carpometacarpal joint dislocation. Case report of traumatic volar dislocation of the medial four carpometacarpal joint in a child and review of the literature. J Hand Surg [Am] 3:377–382
Kumar S, Arora A, Jain AK et al (1998) Volar dislocation of multiple carpometacarpal joints: report of four cases. J Orthop Trauma 12:523–526
Kahlon IA, Karim A, Khan Z (2011) Multiple carpometacarpal volar dislocation. J Coll Physicians Surg Pak 21(1):49–51
Woo CC (1988) Traumatic volar dislocation of the second, third and fourth carpometacarpal joints: mechanism and manipulation. JMPT 11:124–129
Robison JE, Kaye JJ (2005) Simultaneous fractures of the capitate and hamate in the coronal plane: case report. J Hand Surg [Am] 30:1153–1155
Kang SY, Song KS, Lee HJ et al (2009) A case report of coronal fractures through the hamate, the capitate, and the trapezoid. Arch Orthop Trauma Surg 129:963–965
Hazlett JW (1968) Carpometacarpal dislocations other than the thumb: a report of 11 cases. Can J Surg 11:315–323
Hanel DP (1996) Primary fusion of fracture dislocations of central carpometacarpal joints. Clin Orthop 327:85–93
Imbriglia JE (1979) Chronic dorsal carpometacarpal dislocation of the index, middle ring and little fingers: a case report. J Hand Surg 4:343–345
Ahmad S, Plancher K (1996) Carpometacarpal dislocations of the fingers. Oper Techn Sports Med 4(4):257–267
Green DP (1990) Dislocations and ligamentous injuries of the wrist. In: Evarts CM (ed) Surgery of the musculoskeletal system, 2nd edn. Churchill Livingstone, New York, pp 449–515
Gainor BJ, Stark HH, Ashworth CR (1991) Tendon arthroplasty of the fifth carpometacarpal joint for treatment of post-traumatic arthritis. J Hand Surg [Am] 16:520–524
Dubert T, Khalifa H (2009) “Stabilized arthroplasty” for old fracture dislocations of the fifth carpometacarpal joint. Techn Hand Upper Extrem Surg 13(3):134–136
Apergis E (2004) καταγματα-εξαρθρήματα του καρπου. Konstantaras Medical Books, Athens
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
Copyright information
© 2013 Springer-Verlag Italia
About this chapter
Cite this chapter
Apergis, E. (2013). Carpometacarpal (CMC) Dislocations or Fractures-Dislocations Excluding the Thumb. In: Fracture-Dislocations of the Wrist. Springer, Milano. https://doi.org/10.1007/978-88-470-5328-1_9
Download citation
DOI: https://doi.org/10.1007/978-88-470-5328-1_9
Published:
Publisher Name: Springer, Milano
Print ISBN: 978-88-470-5327-4
Online ISBN: 978-88-470-5328-1
eBook Packages: MedicineMedicine (R0)