
Abstract
Poor scholastic performance has immediate as well as lifelong adverse effects on a child and adolescent’s self-esteem and future growth. Psychosocial factors are one of the important causative factors for poor scholastic performance in the under privileged societies, and often remain unidentified. Poor scholastic performance is associated with poor concentration in studies and high dropout rate from schools, and thus has high social costs. A comprehensive assessment covering psychosocial and biological factors is needed to identify the exact cause and plan effective management at the earliest so as to avoid long-term complications. This chapter mainly focusses on psychosocial issues in assessment and management of poor scholastic performance.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
FormalPara Key Points-
Children and adolescents with poor scholastic performance need a detailed evaluation.
-
Poor scholastic performance can be due to variety of causes varying from developmental problems to undiagnosed physical illnesses and psychosocial factors.
-
Cause needs to be identified at the earliest and corrected, since otherwise the problem can have long-term adverse consequences.
1 Introduction
Education is crucial for multifaceted development. Every child should be getting an opportunity to use one’s potentials to the best. Poor scholastic performance has adverse effects on the self-esteem and future growth of the children and adolescents. Prevalence of poor scholastic performance is quite high, to the extent of about 20 % (Thacker 2007). It is very important to identify the children with poor scholastic performance at the earliest, and also those, who are at risk, so that early interventions may be instituted.
Starting of schooling involves the process of separation from parents and adjustment to new environment, and adaptation to new social contacts. The child has to deal with the issues of competition, assertion, and intimacy. A mastery of all these characteristics is important for an optimal performance at school. A child’s physical, cognitive, and emotional adjustment is important for success and acceptance at school, and a disturbance in adjustment at any of these areas may affect scholastic performance of the child.
India has made extraordinary progress over the past decade in increasing access to elementary education. Over 98 % of children in India are estimated to have access to primary schooling within 1 km of their residence, and almost 92 % to an upper primary school within 3 km of their residence (http://ssa.nic.in/quality-docs/RTE%20SSA%20Final%20Report.pdf). In India, out of 20.41 crores of children aged 6–13 years, 60.41 lakhs (2.97 %) are out of school. However, there has been a progressive decrease in this group of children from 6.94 % in 2006 to 4.28 % in 2009 to 2.97 % in 2014. But unfortunately, the rate of school dropout in India is very high. The number of children with special needs who are out of school is much higher at 28.07 % (http://ssa.nic.in/pabminutes-documents/NS.pdf).
Poor scholastic performance is one of the important reasons for school dropout, and may be the real unidentified culprit, while the dropout is attributed to the other more socially acceptable factors like lack of facilities or resources or the teachers’ attitude.
2 Causes of Poor Scholastic Performance
Poor scholastic performance may occur due to a variety of causes including pregnancy and birth complications, developmental disturbances, sensory impairments, nutritional deficiencies, physical illnesses, and psychosocial and environmental factors and specific psychiatric illnesses. Details are discussed as below.
Pregnancy and birth complications: Pregnancy and birth related complications and low birthweight leading to developmental delays are one of the important causes of scholastic backwardness (Karande et al. 2007).
Developmental disorders: Developmental disorders especially subnormal intelligence and specific learning disabilities are important causes of scholastic backwardness. Undiagnosed intellectual disability and borderline or low average intelligence can also adversely affect the scholastic functioning. Specific developmental disorders of reading, writing or speech can affect studies and learning and thus have a potential to lead to scholastic backwardness (Karande et al. 2007; Haneesh et al. 2013).
Sensory impairments: Sensory impairments especially undiagnosed visual and hearing impairments can affect learning, leading to scholastic backwardness (Haneesh et al. 2013; Shashidhar et al. 2009).
Nutritional deficiencies: Similarly nutritional deficiencies including malnutrition, anaemia, and deficiencies of vitamins A, B1, B2, B6, D3 and niacinamide can also contribute by affecting the physical health and growth, and further affecting the scholastic performance (Haneesh et al. 2013; Rashmi et al. 2015; Nair et al. 2003).
Physical illnesses: Both common as well as chronic physical illnesses, if not properly managed, increase the risk for scholastic backwardness. Physical illnesses like bronchial asthma, allergic rhinitis, and worm infestation are quite common in children, and if untreated, may affect scholastic performance. Children suffering from chronic medical illnesses like epilepsy, diabetes, hematological disorders, leukemia, and congenital hypothyroidism need regular long-term treatment, affecting their functioning at school. Some children may suffer from idiopathic short stature and growth hormone deficiency, which can also lead to scholastic backwardness. HIV infection is another emerging problem with a potential to affect scholastic skills (Haneesh et al. 2013; Florence et al. 2008).
Psychosocial and environmental factors: Psychosocial stressors in the family like disturbed relations with parents, family conflict, broken homes and parental neglect may all affect the child’s school performance. Adequate supervision by the parents is often required for optimal academic performance, which if lacking, can affect it adversely, leading to scholastic backwardness. Physical or sexual abuse also worsens the scholastic performance (Nair et al. 2003; Shenoy and Kapur 1996; Mogasale et al. 2012; Khurana 1980).
Sociocultural and environmental factors like low priority being given to education in the family, education level of parents, lack of basic facilities and overcrowding at home, absence of space for studying at home, and alcohol and drug abuse in the family may be in the background of scholastic backwardness. Many times, the child is burdened with the domestic work and does not get adequate time for studies.
Environmental factors, peer group, change of school, and language issues can also adversely affect scholastic performance. Sometimes a child is put in a high profile school which may not be keeping in with the general sociocultural background of the child, and adds to the child’s burden. This is likely to affect the child’s scholastic performance. Similarly overuse of computers, mobile phones and internet, and excessive watching of television may also adversely affect the child’s school performance (Nair et al. 2003; Shenoy and Kapur 1996).
Psychiatric illnesses: Any psychiatric illness like anxiety disorders, childhood depression, conduct disorders, attention deficit hyperactivity disorder (ADHD), Tourette disorder, or autism spectrum disorders occurring in childhood, can lead to scholastic backwardness.
Anxiety may prevent the child to respond to the questions asked by the teacher or prevent the child to ask questions to clarify his or her problems in the class. The affected child may also have constant concerns about the way others view him/her, and affect peer relations at school. All these can adversely affect child’s academic performance at school.
A child suffering from depression may feel low and start losing interest and motivation in studies. Both anxiety and depression can also affect concentration in the studies.
Children affected by ADHD and conduct disorders also suffer scholastic backwardness, because of the innate nature of these illnesses. Some children may have conflictual feelings about success and may fear the success, and its consequences. Tourette disorder may lead to reduced socialisation, and can be incapacitating. Autism spectrum disorders can cause scholastic backwardness by affecting communication (Haneesh et al. 2013; Karande and Kulkarni 2005).
3 Psychosocial Factors Important for Academic Functioning
Certain psychosocial factors are essential for optimal scholastic functioning. Some of these have been referred to in the previous section. Psychosocial factors may be grouped into child and parent related factors, and are discussed as below.
3.1 Child Related Factors
-
Motivation for studies. An optimal level of motivation is essential for satisfactory scholastic performance. If it is lacking, it is likely to cause scholastic backwardness.
-
Ability to apply oneself to studies at school and complete school’s assignments.
-
Regular attendance at school.
-
Average intelligence. An average IQ is required for an optimal performance, and above average intelligence is required for academic excellence.
-
Absence of any sensory deficits.
-
Absence of any chronic physical illnesses.
-
Ability to cope with stressful life events.
-
Perception of support from parents, teachers, and peers (Rashmi et al. 2015; Shenoy and Kapur 1996; Karande et al. 2013).
3.2 Parent-Related Factors
-
Parental encouragement and supervision
-
A stable marital relationship in the parents
-
Positive attitude for education
-
Provision of healthy environment and space to the child
-
Child not to be over burdened with the domestic responsibilities (Haneesh et al. 2013; Rashmi et al. 2015; Nair et al. 2003; Shenoy and Kapur 1996)
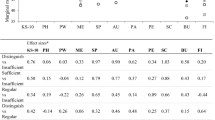
Refractory errors, not having help for study at home, not doing home work regularly, not solving question bank papers, and studying only before the examinations have been identified to be associated with poor scholastic performance in adolescents (Florence et al. 2008). Psychological disturbances, families lacking basic amenities, alcohol dependence in father, inconsistent disciplining and poor parental interaction, frequent school changes, and fewer hobbies have been reported to contribute to the poor scholastic performance in 5–8 year old children (Shenoy and Kapur 1996). Vision impairment, hearing impairment, physical disability, subnormal IQ and specific learning disabilities have been identified as common causes of scholastic backwardness in primary school children in Karnataka (Mogasale et al. 2012) (Table 21.1).
Similar findings have also been reported from other Asian countries. In a study from Malaysia conducted on 1470 children, poor academic achievement was identified in 14 % of the children (Ong et al. 2010). Cognitive ability, male gender, prematurity and lower socioeconomic status were associated with poor academic achievement. Children’s nutritional status, household socioeconomic background, and parental child feeding beliefs and practices have also been found to affect the children’s academic achievement (Lee et al. 2014; Mohd Nasir 2012). Living with one parent, parental divorce, and parents showing no interest in their child’s education and school system, low income, and smoking have also been identified as important contributors to poor scholastic performance in a study from the Middle East (Kamal and Bener 2009). The study also reported that frequent absence from school, incomplete homework, and hyperactivity, inattentiveness and disruptiveness in classroom were associated with poor scholastic performance. Most frequent psychological disorders contributing to school failure were examination phobia, anxiety, anger, fear and learning disability. The most prevalent health disorders included visual disturbances, asthma, anemia and hearing deficiency (Kamal and Bener 2009).
4 Epidemiology
Poor scholastic performance may be a manifestation of another underlying problem. The specific developmental disorders of scholastic skill (SDDSS), also known as specific learning disability (SLD) or disorder affect up to 10 % of the school children in the US (Altarac and Saroha 2007). Another study from the UK found specific arithmetic, arithmetic and reading, and specific reading difficulties in 1.3, 2.3, and 3.9 % of the children studied (Lewis et al. 1994). Reading disabilities have been reported more frequently in boys than in girls across various epidemiological studies (Rutter et al. 2004).
There have been a number of studies from India on the magnitude of poor scholastic performance and learning disorders. One of the earliest studies conducted in 1980s reported prevalence of learning disability as 20.61 % among school children studying in fourth and fifth standard (Venugopal and Raju 1988). In another study on primary school children from a rural area, 12.97 % of the children with IQ of 90 or more were found to have poor achievement in arithmetic and on teacher’s assessment. Children identified to have poor achievement had impaired perceptual maturity and conceptual grasp, and deficits in information processing (Agarwal et al. 1991). A large study from Bangalore on school children in the age group of 5–8 years reported prevalence of learning problems as 17.1 % and of scholastic backwardness as 10.23 %. Prevalence of the both was marginally higher in boys as compared to the girls. Rates of specific difficulties such as reading, writing, and arithmetic were 4.69, 5.15, and 15.96 %, respectively (Shenoy and Kapur 1996; Shenoy et al. 1998). A review of Indian studies conducted over two decades on prevalence of learning disability has reported a prevalence of 3–10 % of various specific learning disabilities (including scholastic abilities) among student population in the states of Karnataka, Kerala, and Tamil Nadu (Ramaa 2000).
A recent study conducted on scholastic backwardness on 1101 children found a prevalence of 24 % (Mogasale et al. 2012). The prevalence of specific learning disabilities was 15.17 %. Dysgraphia, dyslexia, and dyscalculia were specifically observed in 12.5, 11.2, and 10.5 % of the children, respectively. The study had used a six-level screening approach to identify scholastic backwardness. A stepwise exclusion of the subjects was done by excluding the common causes of scholastic backwardness like impaired vision and hearing, chronic medical conditions and subnormal intelligence among these children, and the remaining children were subjected to specific tests for reading, comprehension, writing, and mathematical calculation.
The results have however been highly variable, depending on the place of the study and the methodology used. A recent study from the city of Chandigarh in North India has reported a very low (1.58 %) prevalence of specific developmental disorder of scholastic skills in students of classes VII to XII. The study included a screening by teachers followed by detailed evaluation of the positives by NIMHANS Index for specific learning disability (Arun et al. 2013). A low prevalence of 0.5 % has also been reported in another study (Bansal and Berman 2011). One incidence study from India has reported incidence of specific developmental disorder of scholastic skills among school children at 1.8/1000/year (Malhotra et al. 2009).
The wide variations in the prevalence rates could be due to differences in the demographic profile of the general population, general standards of the school, population studied and methodology.
Table 21.2 summarizes some of the studies on prevalence of poor scholastic performance and learning problems.
5 Psychological Comorbidities
In the current examination conscious age, children are often categorized on the basis of their academic performance. Failure in examinations is viewed as a catastrophe. This results in stress and psychiatric problems in the child. At times, due to difficulty in coping with the examination stress and poor academic performance, many children develop psychological problems. Around one fourth of the children with scholastic backwardness have been reported to have psychological disturbances (Shenoy and Kapur 1996). About 20 % of adolescents with learning disabilities recollect being teased by classmates about their disability and being insulted by the teachers (Karande et al. 2009). A positive correlation between psychological disturbance and poor school achievement has also been reported from a Chinese study (Ekblad 1990).
Children with dyslexia are exposed to a higher risk of anxiodepressive and behavioural disorders. The affected children experience three times more behavioural disorders, and one-third of children with behavioural problems turn out to be affected by dyslexia. Though the literature reveals inconsistent findings about depression among children with dyslexia, evidence of a persistent increase in the rate of anxiety disorders has been observed. The environmental factors have an impact in precipitating these psychiatric comorbidities (Huc-Chabrolle et al. 2010). Youth with learning disabilities (LD) have been suggested to be at an increased risk for suicidal behavior (Bender et al. 1999). Students with LD express more loneliness, more victimization, and less social satisfaction (i.e., school integration) than their non-LD matched peers (Martínez and Semrud-Clikeman 2004).
Data from the National Longitudinal Study of Adolescent Health, which has followed up a nationally representative sample of adolescents in grades 7–12 in US, has found diminished scholastic achievement to be associated with attention problems, delinquency, and substance use, but not with depression (McLeod et al. 2012). Another study on the subject found neuropsychiatric comorbidity in 62.2 % of the children with learning disorders (Margari et al. 2013). The comorbid disorders in specific learning disorders subgroup included ADHD (33 %), anxiety disorders (28.8 %), developmental coordination disorder (17.8 %), language disorder (11 %) and mood disorders (9.4 %) (Margari et al. 2013).
Delayed school progression is associated with general mental health problems in adolescence, though this relationship is confounded by other factors (Tempelaar et al. 2014). Poor school performance has also been reported to be associated with increased rates of schizophrenia, schizoaffective disorder and other psychoses (MacCabe et al. 2008), though it may be difficult to differentiate the poor scholastic performance from the prodromal phase.
6 Assessment
Poor scholastic performance may be due to varied causes of medical and psychological nature. A detailed medical and developmental history should be taken and thorough physical and neurological examination should be conducted to identify the medical causes, if any, for the poor school performance. The possibility of having a chronic physical or psychiatric illness which might lead to prolonged school absenteeism and subsequent scholastic backwardness should be considered. Information should be obtained from multiple sources like the parents, class teacher, and school counselor to substantiate the diagnosis. Detailed information about psychosocial and environmental stressors should be taken. These may include alcohol use in parents, relationship with parents, marital disharmony in parents, adverse comparison with siblings, fear of teacher and examination, and battering by parents and teacher (Haneesh et al. 2013; Khurana 1980). For this the child should be interviewed in a nonjudgmental manner.
The inability to read and comprehend is a major obstacle to learning that may have long-term educational, social, and economic implications. Teaching children with reading difficulties is a big challenge for the teachers as well as the parents. It is also a great source of stress for the affected child. Because dyslexia can be both familial and heritable, the affected younger siblings can be identified earlier. A child should be observed for early indications of dyslexia if he or she has a family history of learning disabilities. An early history of language difficulties such as delay or difficulty in developing speech and language, learning rhymes, or recognizing letters and sound/symbol connections, may be an early indication of dyslexia (Handler et al. 2011).
If a child has any of the risk factors as discussed in the earlier sections, the child should be monitored for the learning difficulties. Identification at the initial stage can help in instituting early intervention and can so improve the prognosis.
To rule out medical causes of poor scholastic performance, hearing and visual acuity should also be tested, and must be attended to, if any problem was identified. As intellectual disability is a well-known cause of poor scholastic performances, IQ assessment by a clinical psychologist should also be done. A detailed psychiatric assessment should be done to screen for any psychiatric disorder.
In India, school teachers have a limited awareness and knowledge about LD (Kamala and Ramganesh 2013). It is recommended that all school teachers should be sensitized to suspect, and trained to screen for LD, when the child is in primary school. School managements should become proactive to setup resource rooms and employ special educators to ensure that these children receive regular and affordable remedial education. Teachers, parents, and the school management need to ensure that these children get the mandatory provisions both during school and board examinations (Karande et al. 2011).
7 Management
7.1 Management of the Identified Medical or Psychiatric Comorbidity, if Any
Treatment should be started as soon as the problem is identified. If any medical problem is identified, it should be treated promptly. If any visual or hearing impairment is detected, it should be corrected. Psychiatric comorbities, if diagnosed, should be managed using the standard psychotherapeutic or pharmacological approaches. Any sociocultural, familial, or environmental factors interfering with the scholastic performance identified during the assessment should be addressed. If need be, the class teacher of the student may also be contacted.
If a specific learning disorder is identified, remedial education is indicated (Coste-Zeitoun et al. 2005). One should not wait for implementing remedial measures, until the children are formally diagnosed with dyslexia or experience repeated failures (Vaughn et al. 2010). The treatment is tailored to the individual child’s cognitive function profile and severity of manifestations (Louis and Emerson 2014). Using specific teaching strategies and materials, the special educator formulates an individualized education program to reduce or modify the child’s deficiencies in specific learning areas such as reading, writing, and mathematics, as identified during the child’s educational assessment. During the remedial education sessions, the child undergoes systematic and highly structured training exercises to learn that words can be segmented into smaller units of sound (phoneme awareness), and that these sounds are linked with specific letters and letter patterns (phonics). The child also requires practice in reading stories, both to apply newly acquired decoding skills to reading words in context and to experience reading for meaning. The management of specific learning disorders is the more time demanding setting of secondary school is based more on providing provisions rather than remediation. The provisions include exemption from spelling mistakes, availing extra time for written tests, dropping a second language and substituting it with work experience, dropping algebra and geometry and substituting them with lower grade of mathematics and work experience; and are meant to help the child cope up in a regular mainstream school. With appropriate remedial education and provisions, most children can be expected to achieve academic competence (Karande and Kulkarni 2005).
7.2 Special Education
If the child is having intellectual disability or severe form of neurobehavioral deficits, he/she may need an open school or a special school. Recently, the Government of India has come out with the concept of ‘inclusive education’, in which such children (especially the less severe cases) can be educated in a regular mainstream school (Karande and Kulkarni 2005). Parents of children with “language barrier” should be advised to educate their children in their own language medium schools or to attend a facility for language stimulation (Silverstein et al. 2002).
Individualized education programme (IEP) has been shown to be effective for slow learners in school. The programme can be imparted on a daily basis or twice in week for 2–4 months. The training programme has been found to improve academic functioning as per the final test results and the parents’ reporting. It also improves the self-esteem of the children which is the first step towards successful remedial education. IEP can be integrated with the normal school curriculum (Krishnakumar et al. 2006, 2011).
Response to intervention (RTI) approach is another management method for LD. It includes eight central features and six common attributes. The central features include high-quality classroom instruction, research-based instruction, classroom performance measures, universal screening, continuous progress monitoring, research-based intervention, progress monitoring during intervention, and fidelity measures. The common attributes include use of concepts of multiple tiers, transition from instruction for all to increasingly intense interventions, implementation of differentiated curricula, instruction delivered by staff other than the classroom teacher, varied duration, time, and frequency of intervention, and categorical or non-categorical placement decisions (Grigorenko 2007).
Children at risk for reading difficulties can be identified in kindergarten (five years of age), and intervention programs started as a part of preventive measures. Classroom-based intervention programs that emphasize phonological awareness, vocabulary and reading strategies, if introduced early, have been found to benefit such children (Lesaux and Siegel 2003).
Schools also need to implement systemic models of prevention including primary, secondary, and tertiary prevention. Primary prevention would include provision of high-quality education for all children. Secondary prevention includes targeted, scientifically-based interventions for children who are not responding to primary prevention. As part of the tertiary prevention, provision of intensive individualized services needs to be created and interventions introduced for those children who do not respond to high-quality instruction or subsequent intervention efforts (Grigorenko 2007).
Parent involvement and advocacy, with assistance from pediatricians and knowledgeable school personnel, is necessary to ensure that appropriate resources available from various sectors are well coordinated and provided for children with learning disorder to improve their school performance and ongoing educational experience (Lambros and Leslie 2005).
8 Initiatives at the State Level
Long back, the Government of India had also constituted a committee under a famous educationist, Professor Yash Pal. The committee in its report “learning without burden” (1993) strongly raised the issue of noncomprehension in the class room. A significant fraction of children who drop out may be those who refuse to compromise with noncomprehension. These children may be potentially superior to those who just memorise and do well in examination, without comprehending very much. The National Curriculum Framework-2005 has pointed out “A majority of children have a sense of fear and failure in mathematics. Hence, they give up early on, and drop out of serious mathematical learning”. Keeping in view of these problems, a nationwide subprogram to the Sarva Shiksha Abhiyan (SSA), ‘Padhe Bharat, Badhe Bharat’ is planned to improve language development by creating an enduring interest in reading and writing with comprehension, and to create a natural and positive interest in mathematics related to the physical and social world (http://ssa.nic.in/pabminutes-documents/Padhe%20Bharat%20Badhe%20Bharat.pdf).
In the recent past, the Government of India has introduced some special provisions in examination system for children with LD. Such provisions have been shown to improve the academic performance at the board examinations (Kulkarni et al. 2006). Since 1999, the National Educational Boards, which conduct the Indian Certificate of Secondary Education (ICSE) and the Central Board of Secondary Education (CBSE) examinations, have also formally granted children with LD the benefit of availing the necessary provisions. Since 2010, the Government of India has also implemented the Right of Children to Free and Compulsory Education 2009 (RTE Act) which makes education free and compulsory to all children, including those with disabilities (Karande et al. 2011).
Sarva Shiksha Abhiyan (SSA) of the Government of India provides for a grant up to Rs. 1200/- per child per year for inclusion of disabled children. The interventions under SSA for inclusive education are identification, functional, and formal assessment, appropriate educational placement, preparation of individualized educational plan, provision of aids and appliances, teacher training, resource support, removal of architectural barriers, research, monitoring and evaluation, and a special focus on girls with special needs. SSA ensures that every child with special needs, irrespective of the kind, category, and degree of disability, is provided meaningful and quality education (http://ssa.nic.in/inclusive-education/overview-on-inclusiveeducation/Overview%20synopsis.pdf/view). As a part of the inclusive education, training modules have been developed for resource teachers for disabled children. With the help of training modules, teachers are sensitized to identify and pick up the children with early signs or symptoms of disability causing poor scholastic performance (http://ssa.nic.in/inclusive-education/training-module-for-resource-teachers-for-disable-children).
9 Conclusion
Poor scholastic performance in children and adolescents can be due to a number of causes including psychosocial, developmental and physical abnormalities. The children need to be assessed in details to find out the exact cause. Some of the causes like refractory errors or nutritional deficiencies can be easily corrected.
There is a need to sensitise the teachers to identify the common causes in the children with poor scholastic performance. The State needs to take adequate steps to introduce counselling facilities in all the schools so that the child can be offered psychosocial help in the school itself. Parents should be informed by the school at the earliest if the child is not performing satisfactorily, and advised to take remedial measures. A multilevel approach at the level of schools, counsellors, pediatricians, mental health professionals, parents, and the State is required.
References
Agarwal, K. N., Agarwal, D. K., Upadhyay, S. K., & Singh, M. (1991). Learning disability in rural primary school children. Indian Journal of Medical Research, 94, 89–95.
Altarac, M., & Saroha, E. (2007). Lifetime prevalence of learning disability among US children. Pediatrics, 119(Suppl 1), S77–S83.
Arun, P., Chavan, B. S., Bhargava, R., Sharma, A., & Kaur, J. (2013). Prevalence of specific developmental disorder of scholastic skill in school students in Chandigarh,India. The Indian Journal of Medical Research, 138, 89–98.
Bansal, P. D., & Berman, R. (2011). Psychopathology of school going children in the age group of 10–15 years. International Journal of Applied and Basic Medical Research, 1, 43–47.
Bender, W. N., Rosenkrans, C. B., & Crane, M. (1999). Stress, depression, and suicide among students with learning disabilities: Assessing the risk. Learning Disability Quarterly Journal, 22, 143–156.
Coste-Zeitoun, D., Pinton, F., Barondiot, C., Ducot, B., Warszawski, J., & Billard, C. (2005). Specific remedial therapy in a specialist unit: Evaluation of 31 children with severe, specific language or reading disorders over one academic year. Revue Neurologique, 161, 299–310.
Ekblad, S. (1990). The children’s behavior questionnaire for completion by parents and teachers in a Chinese sample. Journal of Child Psychology and Psychiatry, 31, 775–791.
Florence, M. D., Asbridge, M., & Veugelers, P. J. (2008). Diet quality and academic performance. Journal of School Health, 78, 209–215.
Grigorenko, E. L. (2007). Learning disabilities. In A. Martin & F. R. Volkmar (Eds.), Lewis’s Child and Adolescent Psychiatry: A Comprehensive Textbook (4th ed., pp. 410–148). Lippincott Williams & Wilkins.
http://ssa.nic.in/pabminutes-documents/Padhe%20Bharat%20Badhe%20Bharat.pdf. Accessed July 08, 2015
http://ssa.nic.in/quality-docs/RTE%20SSA%20Final%20Report.pdf. Accessed July 10, 2015.
http://ssa.nic.in/pabminutes-documents/NS.pdf. Accessed July 10, 2015
http://ssa.nic.in/inclusive-education/training-module-for-resource-teachers-for-disable-children. Accessed July 10, 2015
http://ssa.nic.in/inclusive-education/overview-on-inclusiveeducation/Overview%20synopsis.pdf/view. Accessed July 12, 2015
Handler, S. M., Fierson, W. M., et al. (2011). Learning disabilities, dyslexia, and vision. Pediatrics, 127, e818–e856.
Haneesh, K., Krishnakumar, P., Sukumaran, S. K., & Riyaz, A. (2013). Risk factors for scholastic backwardness in children. Indian Pediatrics, 50, 655–658.
Huc-Chabrolle, M., Barthez, M. A., Tripi, G., Barthélémy, C., & Bonnet-Brilhault, F. (2010). Psychocognitive and psychiatric disorders associated with developmental dyslexia. L’Encéphale, 36, 172–179.
Kamal, M., & Bener, A. (2009). Factors contributing to school failure among school children in very fast developing Arabian Society. Oman Medical Journal, 24, 212–217.
Kamala, R., & Ramganesh, E. (2013). Knowledge of specific learning disabilities among teacher educators in Puducherry, Union Territory in India. International Journal of Humanities and Social Science, 6, 168–175.
Karande, S., Doshi, B., Thadhani, A., & Sholapurwala, R. (2013). Profile of children with poor school performance in Mumbai. Indian Pediatrics, 50, 427.
Karande, S., & Kulkarni, M. (2005). Poor school performance. Indian Journal of Pediatrics, 72, 961–967.
Karande, S., Mahajan, V., & Kulkarni, M. (2009). Recollections of learning-disabled adolescents of their schooling experiences: A qualitative study. Indian Journal of Medical Sciences, 63, 382–391.
Karande, S., Satam, N., Kulkarni, M., Sholapurwala, R., Chitre, A., & Shah, N. (2007). Clinical and psychoeducational profile of children with specific learning disability and co-occurring attention-deficit hyperactivity disorder. Indian Journal of Medical Sciences, 61, 639–647.
Karande, S., Sholapurwala, R., & Kulkarni, M. (2011). Managing specific learning disability in schools in India. Indian Pediatrics, 48, 515–520.
Khurana, S. (1980). Non intellectual factors in learning disability. Indian Journal of Psychiatry, 22, 256–260.
Krishnakumar, P., Geeta, M. G., & Palat, R. (2006). Effectiveness of individualized education program for slow learners. Indian Journal of Pediatrics, 73, 135–137.
Krishnakumar, P., Jisha, A. M., Sukumaran, S. K., & Nair, M. K. (2011). Developing a model for resource room training for slow learners in normal schools. Indian Journal of Psychiatry, 53, 336–339.
Kulkarni, M., Karande, S., Thadhani, A., Maru, H., & Sholapurwala, R. (2006). Educational provisions and learning disability. Indian Journal of Pediatrics, 73, 789–793.
Lambros, K. M., & Leslie, L. K. (2005). Management of the child with a learning disorder. Pediatric Annals, 34, 275–287.
Lee, Y. Y., & Wan Abdul Manan, W. M. (2014). Nutritional status, academic performance and parental feeding practices of primary school children in a rural district in Kelantan, Malaysia. Progress in Health Science, 4, 144–152.
Lesaux, N. K., & Siegel, L. S. (2003). The development of reading in children who speak English as a second language. Developmental Psychology, 39, 1005–1019.
Lewis, C., Hitch, G. J., & Walker, P. (1994). The prevalence of specific arithmetic difficulties and specific reading difficulties in 9- to 10-year-old boys and girls. Journal of Child Psychology and Psychiatry, 35, 283–292.
Louis, P. T., & Emerson, I. A. (2014). Evaluating the cognition, behavior, and social profile of an adolescent with learning disabilities and assessing the effectiveness of an individualized educational program. Iranian Journal of Psychiatry and Behavioral Sciences, 8, 22–37.
MacCabe, J. H., Lambe, M. P., Cnattingius, S., Torrång, A., Björk, C., Sham, P. C., et al. (2008). Scholastic achievement at age 16 and risk of schizophrenia and other psychoses: a national cohort study. Psychological Medicine, 38, 1133–1140.
Malhotra, S., Kohli, A., Kapoor, M., & Pradhan, B. (2009). Incidence of childhood psychiatric disorders in India. Indian Journal of Psychiatry, 51, 101–107.
Margari, L., Buttiglione, M., Craig, F., Cristella, A., de Giambattista, C., Matera, E., et al. (2013). Neuropsychopathological comorbidities in learning disorders. BMC Neurology, 13, 198.
Martínez, R. S., & Semrud-Clikeman, M. (2004). Emotional adjustment and school functioning of young adolescents with multiple versus single learning disabilities. Journal of Learning Disabilities, 37, 411–420.
McLeod, J. D., Uemura, R., & Rohrman, S. (2012). Adolescent mental health, behavior problems, and academic achievement. Journal of Health and Social Behavior, 53, 482–497.
Mogasale, V. V., Patil, V. D., Patil, N. M., & Mogasale, V. (2012). Prevalence of specific learning disabilities among primary school children in a South Indian city. Indian Journal of Pediatrics, 7, 342–347.
Mohd Nasir, M. T., Norimah, A. K., Hazizi, A. S., Nurliyana, A. R., Loh, S. H., & Suraya, I. (2012). Child feeding practices, food habits, anthropometric indicators and cognitive performance among preschoolers in Peninsular Malaysia. Appetite, 58, 525–530.
Nair, M. K. C., Paul, M. K., & Padmamohan, J. (2003). Scholastic performance of adolescents. Indian Journal of Pediatrics, 70, 629–631.
Ong, L. C., Chandran, V., Lim, Y. Y., Chen, A. H., & Poh, B. K. (2010). Factors associated with poor academic achievement among urban primary school children in Malaysia. Singapore Medical Journal, 51, 247–252.
Ramaa, S. (2000). Two decades of research on learning disabilities in India. Dyslexia, 6, 268–283.
Rashmi, M. R., Shweta, B. M., Fathima, F. N., Agrawal, T., Shah, M., & Sequeira, R. (2015). Prevalence of malnutrition and relationship with scholastic performance among primary and secondary school children in two select private schools in Bangalore rural district (India). Indian Journal of Community Medicine, 40, 97–102.
Rutter, M., Caspi, A., Fergusson, D., Horwood, L. J., Goodman, R., Maughan, B., et al. (2004). Sex differences in developmental reading disability: new findings from 4 epidemiological studies. The Journal of the American Medical Association, 291, 2007–2012.
Shashidhar, S., Rao, C., & Hegde, R. (2009). Factors affecting scholastic performances of adolescents. Indian Journal of Pediatrics, 76, 495–499.
Shenoy, J., & Kapur, M. (1996). Prevalence of scholastic backwardness among five to eight year old children. Indian Journal of Psychiatry, 38, 201–207.
Shenoy, J., Kapur, M., & Kaliaperumal, V. G. (1998). Psychological disturbance among 5- to 8-year-old school children: a study from India. Social Psychiatry and Psychiatric Epidemiology, 33, 66–73.
Silverstein, M., Iverson, L., & Lozano, P. (2002). An English-language clinic-based literacy program is effective for a multilingual population. Pediatrics, 109, E76.
Tempelaar, W. M., Otjes, C. P., Bun, C. J., Plevier, C. M., van Gastel, W. A., MacCabe, J. H., et al. (2014). Delayed school progression and mental health problems in adolescence: a population-based study in 10,803 adolescents. BMC Psychiatry, 14, 244.
Thacker, N. (2007). Poor scholastic performance in children and adolescents. Indian Pediatrics, 44, 411–412.
Vaughn, S., Cirino, P. T., Wanzek, J., Wexler, J., Fletcher, J. M., Denton, C. A., et al. (2010). Response to intervention for middle school students with reading difficulties: effects of a primary and secondary intervention. School Psychology Review, 39, 3–21.
Venugopal, M., & Raju, P. (1988). A study on the learning disabilities among IV and V standard students. The Indian Journal of Psychological Medicine, 11, 119–123.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2016 Springer India
About this chapter
Cite this chapter
Chadda, R.K., Patra, B.N. (2016). Poor Scholastic Performance: Psychosocial Perspectives in Assessment and Management. In: Malhotra, S., Santosh, P. (eds) Child and Adolescent Psychiatry. Springer, New Delhi. https://doi.org/10.1007/978-81-322-3619-1_21
Download citation
DOI: https://doi.org/10.1007/978-81-322-3619-1_21
Published:
Publisher Name: Springer, New Delhi
Print ISBN: 978-81-322-3617-7
Online ISBN: 978-81-322-3619-1
eBook Packages: Behavioral Science and PsychologyBehavioral Science and Psychology (R0)