
Abstract
Mathematical modelling plays an important role in understanding the dynamics of transmissible infections, as information about the drivers of infectious disease outbreaks can help inform health care planning and interventions. This paper provides some background about the mathematics of infectious disease modelling. Using a common childhood infection as a case study, age structures in compartmental differential equation models are explored. The qualitative characteristics of the numerical results for different models are discussed, and the benefits of incorporating age structures in these models are examined. This research demonstrates that, for the SIR-type model considered, the inclusion of age structures does not change the overall qualitative dynamics predicted by that model. Focussing on only a single age class then simplifies model analysis. However, age differentiation remains useful for simulating age-dependent intervention strategies such as vaccination.
The original version of this chapter was revised: Equations were deleted. The erratum to this chapter is available at DOI 10.1007/978-4-431-55342-7_23
An erratum to this chapter can be found at http://dx.doi.org/10.1007/978-4-431-55342-7_23
Access provided by Autonomous University of Puebla. Download conference paper PDF
Similar content being viewed by others


Keywords
1 The Purpose and Applications of Infectious Disease models
In epidemiology, mathematical modelling is used to understand the dynamics of transmissible infections. This knowledge has important implications for health care planning and disease interventions. Mathematical models are tools that can help predict the impact of various control strategies on patterns of infection; can assist with understanding the groups of a population that are driving the transmission; and can allow control strategies to be tested and subsequently implemented effectively. For example, mathematical modelling techniques have been widely used in influenza pandemic planning [15, 16], in helping identify the drivers of seasonality in pre-vaccination measles epidemics [17, 18] and in understanding the dynamics of pertussis (whooping cough) outbreaks in young children [31].
This paper provides an overview of the mathematics of infectious disease modelling in the context of a common childhood respiratory infection. In particular, this work examines the extent to which age structures should be incorporated into the modelling, and shows how seasonality and waning immunity can be implemented in relatively simple compartmental models.
2 Introduction to the Mathematics of Infectious Disease Models
Mathematical models applied to infectious disease dynamics typically use deterministic, stochastic, or time series approaches. This paper will focus on a specific type of deterministic, ordinary differential equation model, employing the Susceptible-Infectious-Recovered (SIR) model approach. This model was first introduced by Kermack and McKendrick in 1927 [26] and has since been widely applied to model infectious disease dynamics.
The approach of the SIR framework is to divide a specified population into different compartments that correspond to the states of an infection. These compartments describe whether individuals are susceptible to an infection, infectious, or recovered. The basic SIR model is presented at Eqs. 1–4. Assuming a homogeneous, well-mixed population, S represents the number of individuals in a defined population who are susceptible, while I represents the number of individuals who are infectious and able to infect susceptible individuals. The class R represents the number of individuals who are ‘removed’ (recovered and immune to reinfection).
Demography is represented by the inclusion of a birth rate \(\mu \), which corresponds to an average life expectancy of \(1 / \mu \) years. In this example, the birth rate is assumed to equal the death rate, such that the total population, represented by N, remains constant over time t. Such an assumption is suitable for infectious diseases where the infection life cycle is relatively short compared to the average individual lifespan and the death rate due to the disease is negligible. The recovery rate is represented by \(\gamma \), where \(1/\gamma \) is the average duration of infection in years. A schematic representation of this structure is shown in Fig. 1. The differential equation model corresponding to such dynamics is given by

Schematic diagram for the SIR deterministic ordinary differential equation model
Though the SIR model is one of the simplest forms of a suite of compartmental models, it encapsulates the essence of many infectious disease situations with sufficient accuracy to be able to make useful predictions. Additional states may be included (such as a temporarily immune class) and complexities added (such as age structures). The SIR model and its variations are described extensively elsewhere [4, 11, 23, 25].
3 Respiratory Syncytial Virus
Respiratory syncytial virus (RSV) causes respiratory tract infections in young children. It is the most common pathogen found in children aged less than two years hospitalised with respiratory symptoms and studies indicate that almost all children will have been infected by the time they reach two years [19, 28, 32]. Because of the significant health care and economic burden of RSV (discussed for example in [12, 20, 38]), an improved understanding of its transmission dynamics is required to assist with health care planning. However, because the dynamics of RSV infection are poorly understood, there remains a need for representative models that are validated by the available data.
RSV dynamics have a clear age structure. RSV incidence is higher for children under 12 months than those between 12 and 24 months [29]. Peak incidence is observed in children between two and four months [32]. Newborn infants are typically protected from RSV infection by maternal antibodies until about six weeks of age (although infection can still occur in this early phase of life) [9, 13]. RSV infection data is usually collected from hospitalised cases, hence the cases observed are for severe infection only. However, the dynamics observed at the severe end of the disease spectrum may be representative of the dynamics in the broader community.
Few studies have been undertaken to examine the transmission of RSV among adults, but it is thought that repeated infection can occur throughout life [9, 22], and that in older children and adults, RSV symptoms present as those of a common cold [19]. Several studies have reported on outbreaks of RSV in aged care facilities and estimated the mortality caused by RSV in these older age groups [21, 35].
An important feature of RSV, in terms of understanding its transmission patterns and burden, is its seasonal behaviour. In temperate climates, RSV typically displays annual seasonal patterns, with high numbers of infections in winter and relatively low numbers in the summer months. In some temperate regions, biennial patterns of RSV infection have been detected. Such dynamics have been observed in Switzerland [14], Finland [36], Chile [7] and Australia [29].
Finally, immunity to RSV following recovery from infection is thought to be short-lived, averaging around 200 days [37]. Consequently, children can be infected in consecutive years.
Mathematical models of RSV must therefore take account of different patterns of severe illness with age, of seasonality in disease transmission, and must allow for the waning of disease immunity following recovery from infection.
4 An Age Structured Modelling Approach to RSV
Several models for RSV that implement the SIR approach have been published [10, 30, 37, 39, 40]. A time series approach has been examined by Spaeder et al. [33], and a network approach by Acedo et al. [2, 3]. Stochastic methods have been investigated by Arenas et al. [5].
In the work of Leecaster et al., an age-structured compartmental approach is used to distinguish between children less than two years old, and adults, with an additional ‘Detected’ class [27]. Acedo et al. divide the population into children under one year of age, and the remaining population, in order to model a vaccination strategy for RSV [1]. In recent work by Moore et al. [29], age structuring is used to fit a compartmental model to RSV detection data for children up to two years of age in Perth, Western Australia. The present paper builds upon the work presented published by Moore et al. [29], using parameters relevant to RSV dynamics in Western Australia.
In the following sections, compartmental models for RSV are presented. These models take into account the known clinical characteristics and epidemiological features of RSV, such as waning immunity, a latent period, and seasonal changes in the degree of transmission. The age-structured modelling approach is implemented for one, two and three age groups, in order to capture the transmission and susceptibility characteristics of different age groups. Numerical solutions are found and the resulting qualitative characteristics of the dynamics are discussed.
4.1 A Single Age Class Model for RSV
The simplest model for RSV transmission is that of a single age class. In this situation the age group was chosen to be the combined child and adult population, with no differentiation between age groups, and with the birth rate equal to the death rate. A latent disease class, represented by E, is included to reflect the state where an individual is infected with RSV, but not yet infectious. The disease states are presented as proportions of a population, such that \(S+E+I+R=N=1\). This model was first presented in [24] and the relevant equations are reproduced here as Eqs. 5–9.
To incorporate the effect of seasonal fluctuations in the number of infected cases, the transmission parameter \(\beta \) is replaced with a sinusoidal forcing function, shown at Eq. 9. The birth rate \(\mu \) was chosen based on birth and population data from Western Australia [6] and corresponds to a life expectancy of 74 years. The infectious rate \(\delta \) is based on previous studies and corresponds to a latent period of four days [37]. Similarly, the recovery rate \(\gamma \) is based on previous studies in the literature and corresponds to an infectious period of nine days [2, 27, 37].
The waning immunity parameter \(\nu \) is less well understood and is therefore chosen by fitting models to data from Western Australia, as demonstrated in [29], and corresponds to an immunity period of 230 days. The amplitude of seasonal forcing a was selected based on the same fitting routine, and the parameter b was allowed to vary. Parameter definitions and values are summarised at Table 1.
4.2 Multiple Age Class Models for RSV
There are two main approaches employed in the literature to simulate the ageing process in models for disease transmission. One is the continuous approach, where each compartment in the model is assumed to be a function of both age and time (see [25] for a concise explanation of this method), and the model can be represented as a system of partial differential equations. While realistic, this approach is complicated and the equations are more difficult to solve numerically.
A simpler approach is to treat age groups as compartments in the model, replicating the susceptible, infectious and removed states for each age class. While increasing the number of ordinary differential equations, the system remains straightforward to solve numerically. In this paper, we concentrate only on this second approach to age structures. Detailed examples of where the continuous approach has been used can be found elsewhere [8, 34, 41], although not for RSV.
The multiple age class compartmental model for three age classes is shown in Eqs. 10–17. The age classes are children up to 12 months of age; children aged between 12 and 24 months; and the remaining population. The model may also be adjusted for two age classes only. The seasonal forcing term for each age class is shown in Eqs. 18–19. In the following model, the youngest age class (denoted ‘1’) includes the birth term, with additional classes (denoted ‘i’) representing older age groups.
In comparison to the single age class model of Eqs. 5–9, the additional parameters in the model with multiple age classes are \(\sigma _i\), which represents the reduced transmissability for age class i, and \(\alpha _i\) which represents the reduced susceptibility in age group i. The extent to which transmission is reduced for older age classes is not well understood. Hence, transmission was not scaled for the 12–24 month old age class, but was selected as 0.6 for the older age group as in [29]. Similarly for the susceptibility scaling parameter \(\alpha \), the value for reduced susceptibility was selected for the second age group based on Western Australian data, and chosen to be 0.6 for the older age group. The parameter \(\eta _i\) represents the rate of ageing out of age group i, where \(1/\eta _i\) is the time spent in age group i. Infection-specific parameters are the same as those for the single age class model. The parameter values for the chosen age structure are presented at Table 1.

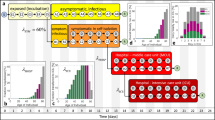
This figure shows two numerical solutions for compartmental RSV models, for each of a one, b two and c three age classes. For each model, the numerical output demonstrates that either an annual or biennial pattern may be produced, depending on the value of the transmission parameter b. The values of b are as follows: a 45, 49; b 3400, 3200; c 460, 530. Other parameter values are provided in Table 1
4.3 Numerical Solutions
The compartmental ordinary differential equation systems for one, two and three age classes, shown in Eqs. 5–19, were solved numerically using MATLAB’s inbuilt ode45 integrator. The values of the fixed parameters are given in Table 1.
The transmission parameter b was chosen to vary, in order to demonstrate different numerical solutions. The range of possible b values that produced plausible numerical solutions varied depending on the model age structure. This is a consequence of how the models were formulated. The model compartments (S, E, I, R), were assumed to be proportions of the chosen population, rather than numbers of individuals. For each age class, the compartments in that age classes summed to 1 at \(t=0\), and the total population did not remain constant as the birth rate and the ‘ageing out’ or death rate were not equal for all model structures; this changed the degree of transmission required to sustain annual epidemics. In practice, exact values of the transmission parameter b will vary according to the data the model is fitted to.
Depending on the value of b chosen, and holding other parameters constant, the model solutions produced either annual or biennial patterns. Examples of solutions for different values of the transmission parameter b are shown in Fig. 2. In this figure, the values of b were selected to be within a range that produced plausible solutions and so as to demonstrate markedly different dynamics.

This figure shows a bifurcation diagram for each of the compartmental RSV models, for a one, b two and c three age classes. The bifurcation parameter is the overall transmission b. For each model, the qualitative behaviour is similar, where there is a region of values of b that produces period two (biennial) solutions, and a region either side that produces period one (annual) solutions
In order to more clearly show the range of b values that produce either annual or biennial patterns of infection, a numerical bifurcation analysis was undertaken using XPP-AUT software. The analysis was conducted for each of the compartmental models, for one, two and three age classes, with bifurcation parameter b. The output is shown in Fig. 3. For each plot, the y-axis is the proportion of infectious individuals I at the seasonal peak, for the youngest age class. We can observe how the infectious peak changes as the value of transmission parameter increases, and whether the model dynamics are annual or biennial.
Figure 3 shows that for each model, there exists a region of solutions with biennial dynamics contained by two period doubling bifurcations. Either side of this region the solutions revert to annual seasonal dynamics. This analysis demonstrates the similar qualitative dynamics for the one, two and three age class models for RSV. A more detailed bifurcation analysis (for example, exploring other bifurcation parameters) is outside the scope of the present paper, but will be explored in a forthcoming publication.
5 Discussion
Mathematical modelling is an important tool for understanding the patterns of infectious disease transmission, and one use of these models is for simulation of disease-specific intervention strategies. Infectious disease interventions are often targeted for different age groups, particularly for children. The ability to implement age-structured modelling approaches is useful for studying the theoretical outcome of a vaccination strategy that is concentrated on specific age groups.
The purpose of this paper is to provide an overview of infectious disease modelling, with a focus on a common childhood respiratory infection. A series of ordinary differential equation models for RSV are presented, incorporating the known clinical characteristics of the infection. Age structures for one, two and three age classes are implemented using the compartmental approach, in order to examine the dynamics of the numerical solutions.
It is found that for the models considered, the qualitative dynamics of the numerical solutions are either annual or biennial, depending on the degree of transmission. Further, the dynamics of the solutions are qualitatively similar for the one, two and three age class systems. Despite adding the complexities of additional age classes, the overall patterns of disease transmission were the same, with a higher transmission rate in younger age groups producing a higher proportion of infectious cases.
This finding has useful implications for studying the dynamics of infectious disease models. It suggests that where the overall behaviour of a model is being investigated, and different possible patterns of disease transmission being considered, the age structuring may be ignored and the simplest single age class model considered. As the number of differential equations is reduced, numerical analyses (such as phase plane and bifurcation) are much simpler and often more readily interpreted. Age structures may of course be included at a later stage of model development, but considering only the single age class (here the younger population only) greatly simplifies analytical and numerical testing in situations where interventions are not being studied.
References
Acedo, L., Díez-Domingo, J., Moraño, J.-A., Villanueva, R.-J.: Mathematical modelling of respiratory syncytial virus (RSV): vaccination strategies and budget applications. Epidemiol. Infect. 138(6), 853–60 (2010)
Acedo, L., Moraño, J.-A., Díez-Domingo, J.: Cost analysis of a vaccination strategy for respiratory syncytial virus (RSV) in a network model. Math. Comp. Model. 52(7–8), 1016–1022 (2010)
Acedo, L., Moraño, J.-A., Villanueva, R.-J., Villanueva-Oller, J., Díez-Domingo, J.: Using random networks to study the dynamics of respiratory syncytial virus (RSV) in the Spanish region of Valencia. Math. Comp. Model 54(7–8), 1650–1654 (2011)
Anderson, R.M., May, R.M.: Infectious Diseases of Humans: Dynamics and Control. Oxford University Press, Oxford (1991)
Arenas, A.J., González-Parra, G., Moraño, J.-A.: Stochastic modeling of the transmission of respiratory syncytial virus (RSV) in the region of Valencia, Spain. BioSystems 96(3), 206–212 (2009)
Australian Bureau of Statistics.: Births, Australia, 2009, Table 2 Births, Summary, Statistical Divisions 2004 to 2009, time series spreadsheet, cat. no. 3301.0, viewed 20 September 2014. http://www.abs.gov.au/AUSSTATS/abs
Avendaño, L.F., Palomino, M.A., Larrañaga, C.: Surveillance for respiratory syncytial virus in infants hospitalized for acute lower respiratory infection in Chile (1989 to 2000). J. Clin. Microbiol. 41(10), 4879–4882 (2003)
Busenberg, S., Cooke, K., Iannelli, M.: Endemic thresholds and stability in a class of age-structured epidemics. SIAM J. Appl. Math. 48(6), 1379–1395 (1988)
Cane, P.A.: Molecular epidemiology of respiratory syncytial virus. Rev. Med. Virol. 11(2), 103–16 (2001)
Capistrán, M., Moreles, M., Lara, B.: Parameter estimation of some epidemic models. The case of recurrent epidemics caused by respiratory syncytial virus. Bull. Math. Biol. 71, 1890–1901 (2009)
Diekmann, O., Heesterbeek, H., Britton, T.: Mathematical Tools for Understanding Infectious Disease Dynamics. Princeton University Press, Princeton (2013)
Díez-Domingo, J., Pérez-Yarza, E.G., Melero, J.A., Sánchez-Luna, M., Aguilar, M.D., Blasco, A.J., Alfaro, N., Lázaro, P.: Social, economic, and health impact of the respiratory syncytial virus: a systematic search. BMC Infect. Dis. 14(1), 544 (2014)
Domachowske, J.B., Rosenberg, H.F.: Respiratory syncytial virus infection: immune response, immunopathogenesis, and treatment. Clin. Microbiol. Rev. 12(2), 298–309 (1999)
Duppenthaler, A., Gorgievski-Hrisoho, M., Frey, U., Aebi, C.: Two-year periodicity of respiratory syncytial virus epidemics in Switzerland. Infection 31(11–12), 75–80 (2003)
Ferguson, N.M., Cummings, D.A.T., Cauchemez, S., Fraser, C., Riley, S., Meeyai, A., Iamsirithaworn, S., Burke, D.S.: Strategies for containing an emerging influenza pandemic in Southeast Asia. Nature 437(7056), 209–214 (2005)
Germann, T.C., Kadau, K., Longini, I.M., Macken, C.A.: Mitigation strategies for pandemic influenza in the United States. Proc. Natl. Acad. Sci. USA 103(15), 5935–5940 (2006)
Grenfell, B.T., Bjørnstad, O.N., Kappey, J.: Travelling waves and spatial hierarchies in measles epidemics. J. Nat. 414, 716–723 (2001)
Grenfell, B.T., Bolker, B.M.: Population dynamics of measles. In: Scott, M.E., Smith, G. (eds.) Parasitic and Infectious Diseases: Epidemiology and Control, pp. 219–234. Academic Press, Orlando (1994)
Hall, C.B.: Respiratory syncytial virus. In: Feigin, R.D., Cherry, J.D. (eds.) Textbook of Paediatric Infectious Diseases, vol. II, pp. 1247–1267. W.B. Saunders Company, Philadelphia (1981)
Hall, C.B., Weinberg, G.A., Iwane, M.K., Blumkin, A.K., Edwards, K.M., Staat, M.A., Auinger, P., Griffin, M.R., Poehling, K.A., Erdman, D., Grijalva, C.G., Zhu, Y., Szilagyi, P.: The burden of respiratory syncytial virus infection in young children. N. Engl. J. Med. 360(6), 588–598 (2009)
Hardelid, P., Pebody, R., Andrews, N.: Mortality caused by influenza and respiratory syncytial virus by age group in England and Wales 1999–2010. Influenza Other Respir. Viruses 7(1), 35–45 (2013)
Henderson, F.W., Collier, A.M., Clyde Jr, W.A., Denny, F.W.: Respiratory-syncytial-virus infections, reinfection and immunity: a prospective, longitudinal study in young children. N. Engl. J. Med. 300(10), 530–534 (1979)
Hethcote, H.W.: The mathematics of infectious diseases. SIAM Rev. 42(4), 599–653 (2007)
Hogan, A.B., Mercer, G.N., Glass, K., Moore, H.C.: Modelling the seasonality of respiratory syncytial virus in young children. In: 20th International Congress on Modelling and Simulation, vol. 9, pp. 338–344. Adelaide, Australia (2013)
Keeling, M.J., Rohani, P.: Modeling Infectious Diseases in Humans and Animals. Princeton University Press, Princeton (2008)
Kermack, W.O., McKendrick, A.G.: A contribution to the mathematical theory of epidemics. Proc. R. Soc. Lond. A. 115, 700–721 (1927)
Leecaster, M., Gesteland, P., Greene, T., Walton, N., Gundlapalli, A., Rolfs, R., Byington, C., Samore, M.: Modeling the variations in pediatric respiratory syncytial virus seasonal epidemics. BMC Infect. Dis. 11(1), 105 (2011)
Moore, H.C., de Klerk, N., Keil, A.D., Smith, D.W., Blyth, C.C., Richmond, P., Lehmann, D.: Use of data linkage to investigate the aetiology of acute lower respiratory infection hospitalisations in children. J. Paediatr. Child Health 48(6), 520–528 (2012)
Moore, H.C., Jacoby, P., Hogan, A.B., Blyth, C.C., Mercer, G.N: Modelling the seasonal epidemics of respiratory syncytial virus in young children. PLoS ONE 9(6), e100422 (2014)
Paynter, S., Yakob, L., Simões, E.A.F., Lucero, M.G., Tallo, V., Nohynek, H., Ware, R.S., Weinstein, P., Williams, G., Sly, P.D.: Using mathematical transmission modelling to investigate drivers of respiratory syncytial virus seasonality in children in the Philippines. PLoS ONE 9(2), e90094 (2014)
Rohani, P., Zhong, X., King, A.A.: Contact network structure explains the changing epidemiology of pertussis. Science 330, 982–985 (2010)
Sorce, L.R.: Respiratory syncytial virus: from primary care to critical care. J. Pediatr. Health Care 23(2), 101–108 (2009)
Spaeder, M.C., Fackler, J.C.: A multi-tiered time-series modelling approach to forecasting respiratory syncytial virus incidence at the local level. Epidemiol. Infect. 140(4), 602–607 (2012)
Tudor, D.: An age-dependent epidemic model with application to measles. Math. Biosci. 147, 131–147 (1985)
van Asten, L., van den Wijngaard, C., van Pelt, W., van de Kassteele, J., Meijer, A., van der Hoek, W., Kretzschmar, M., Koopmans, M.: Mortality attributable to 9 common infections: significant effect of influenza A, respiratory syncytial virus, influenza B, norovirus, and parainfluenza in elderly persons. J. Infect. Dis. 206(5), 628–639 (2012)
Waris, M.: Pattern of respiratory syncytial virus epidemics in Finland: two-year cycles with alternating prevalence of groups A and B. J. Infect. Dis. 163(3), 464–469 (1991)
Weber, A., Weber, M., Milligan, P.: Modeling epidemics caused by respiratory syncytial virus (RSV). Math. Biosci. 172(2), 95–113 (2001)
Welliver, R.C.: Review of epidemiology and clinical risk factors for severe respiratory syncytial virus (RSV) infection. J. Pediatr. 143(5 Suppl), S112–S117 (2003)
White, L.J., Mandl, J.N., Gomes, M.G.M., Bodley-Tickell, A.T., Cane, P.A., Perez-Brena, P., Aguilar, J.C., Siqueira, M.M., Portes, S.A., Straliotto, S.M., Waris, M., Nokes, D.J., Medley, G.F.: Understanding the transmission dynamics of respiratory syncytial virus using multiple time series and nested models. Math. Biosci. 209(1), 222–239 (2007)
White, L.J., Waris, M., Cane, P.A., Nokes, D.J., Medley, G.F.: The transmission dynamics of groups A and B human respiratory syncytial virus (hRSV) in England & Wales and Finland: seasonality and cross-protection. Epidemiol. Infect. 133(2), 279–289 (2005)
Zhu, G.: Threshold and stability results for an age-structured epidemic model. Comput. Math. Appl. 42, 883–907 (2001)
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2016 Springer Japan
About this paper
Cite this paper
Hogan, A.B., Glass, K., Moore, H.C., Anderssen, R.S. (2016). Age Structures in Mathematical Models for Infectious Diseases, with a Case Study of Respiratory Syncytial Virus. In: Anderssen, R., et al. Applications + Practical Conceptualization + Mathematics = fruitful Innovation. Mathematics for Industry, vol 11. Springer, Tokyo. https://doi.org/10.1007/978-4-431-55342-7_9
Download citation
DOI: https://doi.org/10.1007/978-4-431-55342-7_9
Published:
Publisher Name: Springer, Tokyo
Print ISBN: 978-4-431-55341-0
Online ISBN: 978-4-431-55342-7
eBook Packages: EngineeringEngineering (R0)