
Abstract
The survey of early-onset dementia was done in five prefectures and two cities in all parts of Japan from 2006 to 2008. The estimated number of patients per 100,000 in the 18–64-year-old population was 47.6 (95% confidence interval (CI): 45.5–49.7). The estimated patient number in all of Japan was calculated to be 37,800 (95% CI: 36,100–39,400). As a result, we found that vascular dementia (VaD) was the most common illness causing dementia, followed by Alzheimer’s disease (AD), posttraumatic syndrome, and then frontotemporal degeneration.
The prevalence of late-onset dementia was surveyed with in ten areas in all parts of Japan from 2009 to 2012. From the results, the estimated national prevalence was 15%, with a standard error of 0.0136 and 95% CI of 0.12, 0.17. The number of people with dementia in all of Japan was estimated to be about 4.62 million out of a population of 30.79 million people (definite value) aged 65 years and older as of October 1, 2012. The number had probably reached 50 million by the end of 2014.
For the immediate future, both the prevalence and the total number of dementia patients are expected to rise steadily with the increase in the mean life expectancy.
Access provided by CONRICYT-eBooks. Download chapter PDF
Similar content being viewed by others

Keywords
1.1 Introduction
Japan is not the only country with an aging population. In Asia, for example, China is aging at a rate that surpasses Japan, with a current elderly population of about 12% which is predicted to reach 20% within 10 years. In the future, aging populations and the resulting growth in the number of people with dementia will become a major problem not only in China but also in South Korea, India, and the entire Asian region. The problem of dementia is also inevitable in Western countries, which were the first to experience aging populations.
Today, societies are aging and longevity is increasing on a global scale; therefore, dealing with dementia is not simply a medical issue but a fundamental policymaking challenge for each country. In November 2014, the G7 Dementia Summit was held in Japan, and knowledge on dementia care and prevention was presented and shared.
This article looks at the epidemiology of dementia and describes the number of patients and future trends in both early-onset (EOD) and late-onset dementia (LOD).
1.2 EOD
1.2.1 Definition
EOD is a popular term. Formally, dementia that first occurs between the ages of 18 and 44 is called juvenile dementia, while dementia that first occurs between the ages of 45 and 64 is called presenile dementia [1]. The upper limit, however, is taken to be 60 years in some cases and 65 years in others.
1.2.2 Epidemiology
(1) Number of patients
No data on the epidemiological status of early-onset dementia (EOD) in Japan existed until recently. The first nationwide epidemiological survey in Japan was the “Research on the present status of early onset dementia” (project leader: Naomichi Ichinowatari) [1]. The survey was conducted in 1996 in all of Aomori, Gunma, and Tottori Prefectures, plus the cities of Kitakyushu and Hachioji. The survey was done in two stages: the first was a screening, and the second was a more detailed examination. From the results, the number of EOD patients in all Japan was estimated to between 25,613 and 37,434.
We conducted an epidemiological survey on EOD in five prefectures and two cities in all parts of Japan from 2006 to 2008 [2, 3]. The purpose was to calculate the prevalence of EOD, defined as “people under the age of 65 years both at the time of onset and the time of the survey.” The survey areas were Kumamoto, Ehime, Toyama, Gunma, and Ibaraki [3] Prefectures, Kohoku Ward in the city of Yokohama, and all of Tokushima City. The survey was done following the same procedures in all areas. In each area, questionnaires were sent in two stages to all centers and institutions that were thought to be associated with medical care or public health and welfare for dementia. Responses were then collected and analyzed.
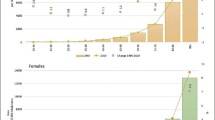
The mean inverse number of the product of the response rate in the first and second surveys was 1.49 (1.23–1.74). Based on the obtained data, the estimated number of patients per 100,000 in the 18–64-year-old population was 47.6 (95% confidence interval (CI): 45.5–49.7). The number of men was 57.9, greater than that of women (36.7). The estimated patient number in all of Japan was calculated to be 37,800 (95% CI: 36,100–39,400). As shown in Fig. 1.1, the global prevalence of dementia in those aged 65 or older is thought to double every 5 years, but this survey showed that this doubling phenomenon is seen from the 1930s.

Prevalence of early-onset dementia in terms of 5-year age strata
Oddly, the response rate was exactly the same in two surveys in Japan [1, 2]. It is also worth noting that the estimated number of patients was the same. This is because while EOD is said to be increasing in recent years, the obtained results show that it is in fact nearly the same. Estimates from these two surveys are similar to previously reported results from various countries [4,5,6,7,8,9,10,11,12] (Table 1.1).
1.2.3 Illnesses Causing Dementia
Summarizing reports from Western countries and Japan, Alzheimer’s disease (AD) is shown to be the most common form of dementia in a large majority of reports. Next is vascular dementia (VaD) or frontotemporal dementia, including Pick’s disease; these conditions account for about half as many cases as AD. They are followed by dementia with Lewy bodies (DLB) or Parkinson’s disease with dementia (PDD). Since these diseases have become widely known fairly recently, the possibility cannot be ruled out that they were previously underestimated.
In a previous survey [13], we found that VaD was the most common illness causing dementia, followed by AD, posttraumatic syndrome, and then frontotemporal degeneration. The fact that the prevalence of stroke was high in men under the age of 65 years both at the time of onset and the time of the survey is thought to be important as background for the unexpected result that VaD was the most common causative illness. The cause of cerebrovascular disease is also important. In Japan, cerebrovascular disease in old age has been decreasing in recent years. Central to that condition is multiple infarctions and lacunar infarctions, which are to some degree preventable. Incidentally, major cerebral infarction, cerebral hemorrhage, and subdural hemorrhage are common in cerebrovascular disease that is a cause of EOD. There are no reports that these conditions are decreasing in people under the age of 65 years at the time of onset in Japan.
In the 1996 study by Ichinowatari [1] VaD was found to be the most common of the illnesses causing dementia, followed by AD. It is also important that VaD was the leading cause in both of Ichinowatari’s and our surveys. This is not seen in reports from other countries, and it may be the major feature of EOD in Japan. In particular, there were 1.6 times more men than women with dementia caused by VaD in this study and twice as more in the earlier study (Fig. 1.2).

Comparison of the prevalence of AD and VaD between men and women
1.3 LOD
1.3.1 Past Findings in Japan
The epidemiological situation of LOD in Japan in recent years is not well understood for the following reasons: survey methods vary, surveys are small, and there is no history of surveys conducted with the same method at the same time on a national scale.
Figure 1.1 shows the prevalence of dementia in terms of age strata, which has been said to be the greatest common measure. The prevalence of dementia in people aged 65–69 years is 1.5% but is thought to double every 5 years after that, reaching 27% at age of 85. Past estimates of the prevalence of dementia in the elderly population aged 65 years and older put it at around 10% in 2011. Shimokata [14] estimated that the number of dementia patients will increase together with the rapid increase in the elderly population in the future, reaching 3.25 million people in 2020.
1.3.2 The Most Recent National Survey in Japan
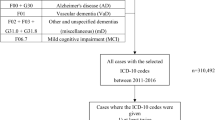
The prevalence of dementia was surveyed with a standardized method in ten areas in all parts of Japan from 2009 to 2012 [15]. The survey was carried out in the following seven regions from October 1, 2009 to September 30, 2010: Kurihara, Miyagi Prefecture; Tone, Ibaraki Prefecture; Joetsu, Niigata Prefecture; Obu, Aichi Prefecture; Ama, Shimane Prefecture; Imari, Saga Prefecture; and Kitsuki, Oita Prefecture. From 2011, it was carried out in Tsukuba, Ibaraki Prefecture; Hisayama, Fukuoka Prefecture; and Omuta, Fukuoka Prefecture for the purpose of understanding the actual situation in urban areas (Fig. 1.3).

Study sites of nationwide survey for dementia prevalence
In stage 1 of the survey, investigators spoke with family members during a home visit and conducted interviews with the patient at the home or interview site. In stage 2, doctors conducted interviews, and in stage 3, MRIs were obtained and blood tests were performed. Tests used in the Alzheimer’s Disease Neuroimaging Initiative, the current global standard, were adopted for assessment of all cases.
In estimating prevalence, data on 7825 subjects and 5386 participants from eight regions were used. From the results, the estimated national prevalence was 15%, with a standard error of 0.0136 and 95% CI of 0.12, 0.17. The number of people with dementia in all of Japan was estimated to be about 4.62 million out of a population of 30.79 million people (definite value) aged 65 years and older as of October 1, 2012 [15]. The number had probably reached 50 million by the end of 2014. The prevalence of dementia gained from the data shown in terms of 5-year age strata is shown in Fig. 1.4.

Prevalence of dementia in terms of 5-year age strata
One may wonder why the prevalence has so clearly exceeded predictions. Crucial to the answer is thought to be the increase in the mean life expectancy in Japan. As has been well known for some time, aging is the largest risk factor for dementia. The risk of dementia is known to double every 5 years after the age of 65. In 1994, the mean life expectancy for Japanese was 77 years for men and 83 for women. After 20 years, it increased to 80 and 87 years, respectively. This is thought to have led to a great increase in the prevalence of dementia.
The number of people with dementia is shown in 5-year age cohorts (Fig. 1.5). This shows that the greatest number of patients is concentrated in the 80s. Here, they account for about half of the number of people with dementia in Japan. By sex, the number of male patients does not increase after the age of 75. Among women, however, the number increases steadily from this age. Carrying this to its logical conclusion, it may not be an overstatement to say that the problem of dementia in Japan is a problem of women in their 80s. Why does such a difference between the sexes exist? The most important thing is thought to be the 7-year age gap in mean life expectancy between men, at 80 years, and women at 87 years. That is because, as mentioned above, the risk of dementia doubles every 5 years after the age of 65. A 7-year age difference is thus equal to about a threefold difference in risk.

Number of demented elderly in terms of 5-year age strata
Regarding illnesses of causing dementia, Alzheimer’s disease (AD) is shown to be the most common form of dementia, followed by vascular dementia (VaD), and DLB or PDD (Fig. 1.6).

Proportion of illnesses causing dementia
The standardized prevalence of mild cognitive impairment is estimated to be about 13% [15]. Thus, the number of elderly people thought to be in a precursor state for dementia is shown to be roughly equal to the number with dementia.
For the immediate future, both the prevalence and the total number of dementia patients are expected to rise steadily with the increase in the mean life expectancy of Japanese. It is truly coming to be that “there is no calling time” for dementia.
References
Ichinowatari N. Health Science Research Grants. Study on the early onset dementia. Annual report for the 8th fiscal year of Heisei, 1997 (in Japanese).
Asada T. Health and Labor Science Research Grants. Comprehensive Research on Aging and Health. Study on the actual condition of the individuals with early onset dementia and providing the infrastructure for them. Annual report for the 20th fiscal year of Heisei, 2009 (in Japanese).
Ikejima C, Ikeda M, Hashimoto M, Ogawa Y, Tanimukai S, Kashibayashi T, Miyanaga K, Yonemura K, Kakuma T, Murotani K, Asada T. Multicenter population-based study on the prevalence of early onset dementia in Japan: vascular dementia as its prominent cause. Psychiatry Clin Neurosci. 2014;68(3):216–24.
Mölsä PK, Marttila RJ, Rinne UK. Epidemiology of dementia in a Finnish population. Acta Neurol Scand. 1982;65:541–52.
Sulkava R, Wikström J, Aromaa A, et al. Prevalence of severe dementia in Finland. Neurology. 1985;35:1025–9.
Schoenberg BS, Anderson DW, Haerer AF. Severe dementia. Prevalence and clinical features in a biracial US population. Arch Neurol. 1985;42:740–3.
Kokmen E, Beard CM, Offord KP, et al. Prevalence of medically diagnosed dementia in a defined United States population: Rochester, Minnesota, January 1, 1975. Neurology. 1989;39(6):773.
Newens AJ, Forster DP, Kay DW, et al. Clinically diagnosed presenile dementia of the Alzheimer type in the Northern Health Region: ascertainment, prevalence, incidence and survival. Psychol Med. 1993;23:631–44.
Ohshiro H, Kurozawa Y, Iwai N, et al. Estimated prevalence of presenile dementia in Tottori prefecture. Nihon Koshu Eisei Zasshi. 1994;41:424–7. (in Japanese)
Ratnavalli E, Brayne C, Dawson K, et al. The prevalence of frontotemporal dementia. Neurology. 2002;58:1615–21.
Harvey RJ, Skelton-Robinson M, Rossor MN. The prevalence and causes of dementia in people under the age of 65 years. J Neurol Neurosurg Psychiatry. 2003;74(9):1206.
Rosso SM, Landweer EJ, Houterman M, et al. Medical and environmental risk factors for sporadic frontotemporal dementia: a retrospective case-control study. J Neurol Neurosurg Psychiatry. 2003;74:1574–6.
Ikejima C, Yasuno F, Mizukami K, et al. Prevalence and causes of early-onset dementia in Japan: a population-based study. Stroke. 2009;40:2709–14.
Shimokata H. Epidemiological statistics of dementia in Japan. Nihon Rinsho. 2004;62(Suppl 4):121–6. (in Japanese)
Asada T. Health and Labor Science Research Grants. Research on Dementia. Prevalence of dementia in the urban areas of Japan and development of treatment of the daily life disability associated with dementia. Report of comprehensive research for the 23rd to 24th fiscal year of Heisei, 2013 (in Japanese).
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2017 Springer Japan
About this chapter
Cite this chapter
Asada, T. (2017). Epidemiology of Dementia in Japan. In: Matsuda, H., Asada, T., Tokumaru, A. (eds) Neuroimaging Diagnosis for Alzheimer's Disease and Other Dementias. Springer, Tokyo. https://doi.org/10.1007/978-4-431-55133-1_1
Download citation
DOI: https://doi.org/10.1007/978-4-431-55133-1_1
Published:
Publisher Name: Springer, Tokyo
Print ISBN: 978-4-431-55132-4
Online ISBN: 978-4-431-55133-1
eBook Packages: MedicineMedicine (R0)