
Abstract
The repertoire of skills needed to provide care to the burn-injured patient includes comprehensive clinical assessment and monitoring, pain management, wound care and psychosocial support. This chapter is focused on providing the nurse with valuable information for the provision of appropriate nursing care.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others



Keywords
These keywords were added by machine and not by the authors. This process is experimental and the keywords may be updated as the learning algorithm improves.
8.1 Introduction
The repertoire of skills needed to provide care to the burn-injured patient includes comprehensive clinical assessment and monitoring, pain management, wound care and psychosocial support. This chapter is focused on providing the nurse with valuable information for the provision of appropriate nursing care.
8.2 Knowledge Base
8.2.1 General Definition and Description
8.2.1.1 Incidence
-
Annually, an estimated 450,000 people seek care for burns in the USA [1, 2].
-
Approximately 45,000 require hospitalisation, greater than half of whom (25,000) receive care in specialised burn units or centres [1, 2].
-
Survival rate, for hospitalised patients, is around 96 %.
-
Children 4 years of age and younger and adults over the age of 55 form the largest group of fatalities.
-
In North America and Europe, 70 % of burn survivors are male and 30 % female.
8.2.1.2 Classification
Burn complexity can range from a relatively minor, uncomplicated injury to a life-threatening, multisystem trauma. The American Burn Association (ABA) has a useful classification system that rates burn injury magnitude from minor to moderate, uncomplicated to major (Table 8.1).
8.3 Aetiology and Risk Factors
The causes of burn injuries are numerous and found in both the home, leisure and workplace settings (Table 8.2).
8.3.1 Pathophysiology
8.3.1.1 Severity Factors
There are five factors that need to be considered when determining the severity of a burn injury (Box 8.1):
-
1.
Extent – There are several methods available to accurately calculate the percentage of body surface area involved:
-
The simplest is the rule of nines (see Chap. 1, Fig. 1.1 and Chap. 2, Fig. 2.2). However, it is only for use with the adult burn population.
-
The Lund and Browder method (see Chap. 1, Fig. 1.1 and Chap. 2, Fig. 2.2) is useful for all age groups, but is more complicated to use.
-
There is a paediatric version of the Lund and Browder method (see Chap. 2, Fig. 2.2).
-
If the burned areas are scattered, small and irregularly shaped, the rule of palm can be used. The palm of the burned person’s hand represents 1 % body surface area.
-
If 10 % or more of the body surface of a child or 15 % or more of that of an adult is burned, the injury is considered serious. The person requires hospitalisation and fluid replacement to prevent shock.
-
-
2.
Depth
-
Two factors determine the depth of a burn wound: temperature of the burning agent and duration of exposure time.
-
Previous terminology to describe burn depth was first, second and third degree. In recent years, these terms have been replaced by those more descriptive in nature: superficial partial-thickness, deep partial-thickness and full-thickness (Table 8.3).
Table 8.3 Classification of burn injury depth -
Superficial burns, such as those produced by sunburn, are not taken into consideration when assessing extent and depth.
-
The skin is divided into three layers, which include the epidermis, dermis and subcutaneous tissue (Fig. 8.1).
Fig. 8.1 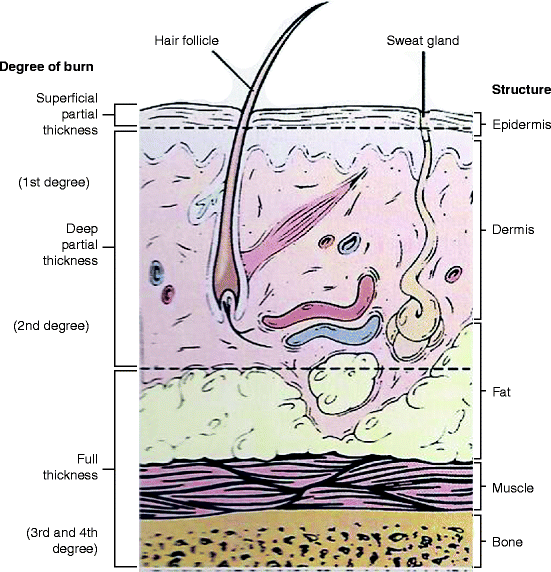
Anatomy of burn tissue depth
-
-
3.
Age
-
For patients less than 2 years of age and greater than 50, there is a higher incidence of morbidity and mortality.
-
Sadly, the infant, toddler and elderly are at increased risk for abuse by burning.
-
-
4.
Part of the body burned
-
Patients with burns to the face, neck, hands, feet or perineum have greater challenges to overcome and require the specialised care offered by a burn centre.
-
-
5.
Past medical history
-
Pre-existing cardiovascular, pulmonary or renal disease will be exacerbated by the burn injury.
-
Persons with diabetes or peripheral vascular disease have a more difficult time with wound healing, especially on the legs and feet.
-

8.3.2 Local Damage
Local damage varies, depending upon:
-
(a)
Temperature of the burning agent
-
(b)
Duration of contact time
-
(c)
Type of tissue involved
Zones of tissue damage:
-
Inner zone of coagulation (full-thickness injury) – irreversible cell death, skin grafting needed for permanent coverage
-
Middle zone of stasis (deep, partial-thickness injury) – some skin-reproducing cells present in the dermal appendages with circulation partially intact, healing generally within 14–21 days
-
Outer zone of hyperaemia (superficial, partial-thickness injury) – minimal cell involvement and spontaneous healing within 7–10 days
8.3.3 Fluid and Electrolyte Shifts
The immediate post-burn period is marked by dramatic circulation changes, producing what is known as “burn shock” (Fig. 8.2).

Burn shock
-
As the capillary walls begin leaking, water, sodium and plasma proteins (primarily albumin) move into the interstitial spaces in a phenomenon known as “second spacing”.
-
When the fluid begins to accumulate in areas where there is normally minimal to no fluid, the term “third spacing” is used. This fluid is found in exudate and blisters.
-
There is also insensible fluid loss through evaporation from large, open body surfaces. A non-burned individual loses about 30–50 mL/h. A severely burned patient may lose anywhere from 200 to 400 mL/h.
-
Circulation is also impaired in the burn patient due to haemolysis of red blood cells.
-
Following successful completion of the fluid resuscitation phase, capillary membrane permeability is restored. Fluids gradually shift back from the interstitial space to the intravascular space, and the patient is no longer grossly oedematous and diuresis is ongoing.
8.4 Cardiovascular, Gastrointestinal and Renal System Manifestations
During the hypovolemic shock phase, only vital areas of circulation are maintained.
-
Cardiac monitoring is essential, particularly if the patient has a pre-burn history of cardiac problems.
-
Electrical burn patients, who arrest at the scene or who experience cardiac arrhythmias post-injury, warrant particular vigilance.
-
Hypovolemic shock and hypoxemia also produce the initial gastrointestinal complications seen post-burn, such as decreased peristalsis and abdominal paralytic ileus.
-
Stress response post-burn releases catecholamines and may produce stress (Curling’s) ulcers in burns >50 % body surface area.
-
Renal complications are predominantly caused by hypovolemia. If perfusion remains poor, high circulating levels of haemoglobin and myoglobin may clog the renal tubules, causing acute tubular necrosis.
8.4.1 Types of Burn Injuries
-
Thermal (Table 8.4)
Table 8.4 Causes of thermal burns -
Dry heat, such as flame and flash
-
Moist heat, such as steam and hot liquids
-
Direct contact, such as hot surfaces and objects
-
Major source of morbidity and mortality across all age groups (Figs. 8.3 and 8.4)
Fig. 8.3 
Third degree/full-thickness flame burn
Fig. 8.4 
Scald burn: looks can be deceiving – burn wound progression over several days
-
-
Chemical (Fig. 8.5)
Fig. 8.5 
Chemical burns: looks can be deceiving – copious flushing for up to several hours
-
More than 25,000 chemicals worldwide
-
Divided into two major groups: acids and alkalis
-
Extent and depth injury: directly proportional to the amount, type and strength of the agent, its concentration, degree of penetration, mechanism of action and length of contact time with the skin
-
-
Electrical (Fig. 8.6)
Fig. 8.6 
Electrical burn
-
Comprise a small portion of the burn population.
-
Outcomes can be devastating due to tissue damage and potential limb loss.
-
Severity of injury difficult to determine as most of the damage may be below skin at level of muscle, fat and bone.
-
Entry and exit points determine probable path of current and potential areas of injury.
-
If person has fallen post-injury, protect head and cervical spine during transport; need to perform spinal x-rays and neurological assessment.
-
May continue to be at risk for cardiac arrhythmias for 24 h post-burn, so ECG needed on admission and at 24 h post-burn.
-
Infuse Lactated Ringer’s solution at a rate that maintains a good urinary output between 75 and 100 mL/h until colour of urine sufficient to suggest adequate dilution of haemoglobin and myoglobin pigments.
-
Administer osmotic diuretic (e.g. mannitol) to establish and maintain acceptable urinary output.
-
-
Smoke and Inhalation Injury (Fig. 8.7)
Fig. 8.7 
Inhalation injury
-
Exposure to smoke and inhalation of hot air, steam or noxious products of combustion.
-
Presence of inhalation injury, with a large burn, can double or triple one’s mortality rate.
-
Signs and symptoms: burns to head and neck, singed nasal hairs, darkened oral and nasal membranes, carbonaceous sputum, stridor, hoarseness, difficulty swallowing, history of being burned in an enclosed space, exposure to flame, including clothing catching fire near the face, indoors and outdoors.
-
Critical period is 24–48 h post-burn.
-
Most fatalities at fire scene caused by carbon monoxide poisoning or asphyxiation (Table 8.5).
Table 8.5 Signs and symptoms of carbon monoxide poisoning -
Treatment is 100 % humidified oxygen until carboxyhemoglobin falls to acceptable levels.
-
-
Radiation
-
Overexposure to sun or radiant heat sources, such as tanning lamps or tanning beds.
-
Nuclear radiation burns require government intervention and specialised treatment.
-





8.4.1.1 Clinical Manifestations
Care Priorities During the Emergent, Acute and Rehabilitative Periods
-
1.
Principles of care for the emergent period: resolution of the immediate problems resulting from the burn injury. The time required for this to occur is usually 1–2 days. The emergent phase ends with the onset of spontaneous diuresis.
-
2.
Principles of care for the acute period: avoidance, detection and treatment of complications and wound care. This second phase of care ends when the majority of burn wounds have healed.
-
3.
Principles of care for the rehabilitative period: eventual return of the burn survivor to an acceptable place in society and completion of functional and cosmetic reconstruction. This phase ends when there is complete resolution of any outstanding clinical problems resulting from the burn injury.
-
Initial assessment of the burn patient is like that of any trauma patient and can best be remembered by the simple acronym “ABCDEF” (Box 8.2). During the emergent period, burn patients exhibit signs and symptoms of hypovolemic shock (Box 8.3). Lack of circulating fluid volumes will also result in minimal urinary output and absence of bowel sounds. The patient may also be shivering due to heat loss, pain and anxiety. With inhalation injury, the airway should be examined visually and then with a laryngoscope/bronchoscope (Box 8.4). The patient may also experience pain, as exhibited by facial grimacing, withdrawing and moaning when touched, particularly if the injuries are partial-thickness in nature. Some areas of full-thickness burn may be anaesthetic to pain and touch if the nerve endings have been destroyed. It is important to examine areas of circumferential full-thickness burn for signs and symptoms of vascular compromise, particularly the extremities (Box 8.5). Areas of partial-thickness burn appear reddened, blistered and oedematous. Full-thickness burns may be dark red, brown, charred black or white in colour. The texture is tough and leathery, and no blisters are present. If the patient is confused, one has to determine if it is the result of hypovolemic shock, inhalation injury, substance abuse, pre-existing history or, more rarely, head injury sustained at the time of the trauma. It is essential to immobilise the c-spines until a full assessment can be performed and the c-spines cleared. At this time, a secondary survey assessment is performed (Box 8.6).
-
In the acute phase, the focus is on wound care and prevention/management of complications. At this point, the burn wounds should have declared themselves as being partial-thickness or full-thickness in nature. Eschar on partial-thickness wounds is thinner, and, with dressing changes, it should be possible to see evidence of eschar separating from the viable wound bed. Healthy, granulation tissue is apparent on the clean wound bed, and re-epithelialising cells are seen to migrate from the wound edges and the dermal bed to slowly close the wound within 10–14 days. Full-thickness wounds have a thicker, more leathery eschar, which does not separate easily from the viable wound bed. Those wounds require surgical excision and grafting. Continuous assessment of the patient’s systemic response to the burn injury is an essential part of an individualised plan of care. Subtle changes quickly identified by the burn team can prevent complications from occurring or worsening over time.
-
During the final, rehabilitative phase, attention turns to scar maturation, contracture development and functional independence issues. The areas of burn, which heal either by primary intention or skin grafting, initially appear red or pink and are flat. Layers of re-epithelialising cells continue to form, and collagen fibres in the lower scar tissue add strength to a fragile wound. Over the next month, the scars may become more red from increased blood supply and more raised from disorganised whorls of collagen and fibroblasts/myofibroblasts. The scars are referred to as hypertrophic in nature. If oppositional forces are not applied through splinting devices, exercises or stretching routines, this new tissue continues to heal by shortening and forming contractures. A certain amount of contracture development is unavoidable, but the impact can be lessened through prompt and aggressive interventions.
-

8.5 Clinical Management
8.5.1 Nonsurgical Care
-
Emergent Phase Priorities: airway management, fluid therapy, initial wound care
-
Emergent Phase Goals of Care: initial assessment, management and stabilisation of the patient during the first 48 h post-burn
-
Emergent Phase Assessment
-
During the rapid, primary survey, airway and breathing assume top priority. A compromised airway requires prompt attention and breath sounds verified in each lung field.
-
If circumferential, full-thickness burns are present on the upper trunk and back, ventilation must be closely monitored as breathing might be impaired and releasing escharotomies necessary (Fig. 8.8).
Fig. 8.8 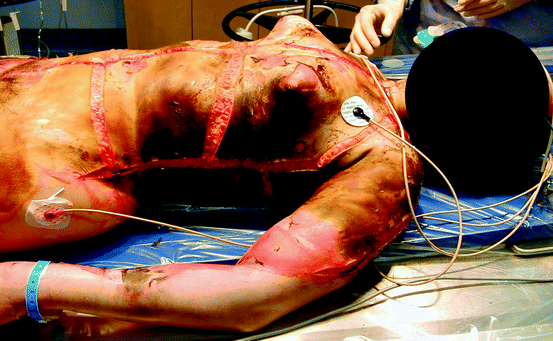
Full-thickness flame burn with releasing escharotomies
-
Spine must be stabilised until c-spines are cleared.
-
Circulation is assessed by examining skin colour, sensation, peripheral pulses and capillary filling. Circumferential, full-thickness burns to the arms or legs must be assessed via palpation or Doppler for evidence of adequate circulation. Escharotomies might be required.
-
Typically, burn patients are alert and oriented the first few hours post-burn. If that is not the case, consideration must be given to associated head injury (including a complete neurological assessment), substance abuse, hypoxia or pre-existing medical conditions.
-
All clothing and jewellery need to be removed in order to visualise the entire body and avoid the “tourniquet-like” effect of constricting items left in place as oedema increases.
-
Adherent clothing needs to be gently soaked off with normal saline to avoid further trauma and unnecessary pain.
-
Prompt fluid resuscitation must be initiated to address hypovolemic shock.
-
Secondary, head-to-toe survey rules out any associated injuries. All medical problems are identified and managed in a timely fashion.
-
Circumstances of the injury must be explored to understand the mechanism, duration and severity of the injury.
-
Patient’s pertinent medical history includes identification of pre-existing disease or associated illness (cardiac or renal disease, diabetes, hypertension), medication/alcohol/drug history, allergies and tetanus immunisation status. A handy mnemonic can be used to remember this information (Box 8.7).
-
-
Emergent Phase Management
-
The top priority of care is to stop the burning process (Box 8.8). During the initial first aid period at the scene, the patient must be removed from the heat source, chemicals should be brushed off and/or flushed from the skin, and the patient wrapped in a clean sheet and blanket ready for transport to the nearest hospital. Careful, local cooling of the burn wound with saline-moistened gauze can continue as long as the patient’s core temperature is maintained and he/she does not become hypothermic.
-
Upon arrival at the hospital, the burned areas can be cooled further with normal saline, followed by a complete assessment of the patient and initiation of emergency treatment (Box 8.9). In a burn centre, the cooling may take place, using a cart shower system, in a hydrotherapy room (Fig. 8.9). The temperature of the water is adjusted to the patient’s comfort level, but tepid is usually best, while the wounds are quickly cleaned and dressings applied.
Fig. 8.9 
Cart shower for hydrotherapy
-
-
Airway management includes administration of 100 % oxygen if burns are 20 % body surface area or greater. Suctioning and ventilatory support may be necessary. If the patient is suspected of having or has an inhalation injury, intubation needs to be performed quickly.
-
Evidence-based procedures for the insertion of central lines and care of ventilated patients have resulted in impressive reductions in central line blood stream infection rates and ventilator-acquired pneumonia (VAP) [3].
-
Circulatory management includes intravenous infusion of fluid to counteract the effects of hypovolemic shock for adult patients with burns >15 % body surface area and children with burns >10 % body surface area. Upon admission, two large bore, intravenous catheters should be inserted, preferably into, but not limited to, unburned tissue.
-
Patients who have large burns where intravenous access will be necessary for a number of days benefit from a central venous access device inserted into either the subclavian, jugular or femoral vein. The overall goal is to establish an access route that will accommodate large volumes of fluid for the first 48 h post-burn.
-
The aim of fluid resuscitation is to maintain vital organ function, while avoiding the complications of inadequate or excessive therapy [4]. The most commonly used regimen is the Parkland (Baxter) formula: 4 ml/kg/% body surface area burn using crystalloid (Lactated Ringer’s) solution (Box 8.10). Fluids are calculated for the first 24 h post-burn with “0” hours being the time of the burn not the time of admission to hospital. One-half of the 24 h total needs to be administered over the first 8 h post-burn, while the remaining half of the estimated resuscitation volume should be administered over the next 16 h.
-
It is important to remember that the formula is only a guideline. The infusion needs to be adjusted based on the patient’s clinical response, which includes vital signs, sensorium and urinary output. For adults, 30–50 mL urine per hour is the goal and 1 mL/kg/h in children weighing less than 30 kg.
-
An indwelling urinary catheter needs to be inserted at the same time as the IV’s are established in order to reliably measure the adequacy of the fluid resuscitation [5].
-
-
Wound care. Wound closure will halt or reverse the various fluid/electrolyte, metabolic and infectious processes associated with an open burn wound. The burns are gently cleansed with normal saline, if the care is being provided on a stretcher or bed. If a hydrotherapy cart shower or immersion tank is used, tepid water cleans the wounds of soot and loose debris (Fig. 8.10). Sterile water is not necessary.
-
Chemical burns should be flushed copiously for at least 20 min, preferably longer.
-
Tar cannot be washed off the wound. It requires numerous applications of an emulsifying agent, such as Tween 80®, Medisol® or Polysporin® ointment.
-
During hydrotherapy, loose, necrotic tissue (eschar) may be gently removed (debrided) using sterile scissors and forceps. Hair-bearing areas that are burned should be carefully shaved, with the exception of the eyebrows. Showering or bathing should be limited to 20 min in order to minimise patient heat loss and physical/emotional exhaustion.
-
More aggressive debridement should be reserved for the operating room, unless the patient receives conscious sedation.
-
After the initial bath or shower, further decisions are made regarding wound care. The frequency of the dressing change depends on the condition of the wound and the properties of the dressing employed. All treatment approaches have certain objectives in common (Table 8.6).
Table 8.6 Objectives of burn wound care -
Wounds are generally treated with a thin layer of topical antimicrobial cream. Topical coverage is selected according to the condition of the wound, desired results and properties of the topical agent (Table 8.7).
Table 8.7 Topical antimicrobial agents used on burn wounds -
Assessment criteria have been established for choosing the most appropriate agent (Box 8.11).
-
The most commonly selected topical antimicrobial agent is silver sulphadiazene, which can be applied directly to saline-moistened gauze, placed on the wound, covered with additional dry gauze or a burn pad and secured with gauze wrap or flexible netting (Fig. 8.11). These dressings are changed once or twice daily.
Fig. 8.11 
Applying silver sulphadiazene cream to saline-moistened gauze
-
Cartilaginous areas, such as the nose and ears, are usually covered with mafenide acetate (Sulfamylon®), which has greater eschar penetration ability.
-
Face care includes the application of warmed, saline-moistened gauze to the face for 20 min, followed by a gentle cleansing and reapplication of a thin layer of ointment, such as polymyxin B sulphate (Polysporin®) (Fig. 8.12).
Fig. 8.12 
Facial burn wound care
-
Silver-impregnated dressings (Acticoat®/Acticoat® Flex, AQUACEL® Ag) are also commonly used in the emergent phase of burn wound care. These dressings are moistened with sterile water, placed on a burn wound and left intact anywhere from 3 to 4 days to as long as 21 days, depending on the patient’s individual clinical status and particular product.
-
The ideal dressing should possess particular criteria (Box 8.12). During the first few days post-burn, wounds are examined to determine actual depth. It usually takes a few days for deep, partial-thickness wounds to “declare” themselves. Scald injuries are almost always deeper than they appear on admission and need to be closely monitored.
Fig. 8.10 
Initial wound care post-admission
-
-
Whatever topical and dressing strategies are chosen, basic aseptic wound management techniques must be followed [6]. Personnel need to wear isolation gowns over scrub suits, masks, head covers and clean, disposable gloves to remove soiled dressings or cleanse wounds. Sterile gloves should be used when applying inner dressings or ointment to the face.
-





-
Acute Phase Priorities: closure of the burn wound, management of any complications
-
Acute Phase Goals of Care: spontaneous diuresis, ongoing fluid management, wound closure, detection and treatment of complications over a period of a week to many months, optimal pain management and nutrition
-
Acute Phase Assessment
-
Fluid therapy is administered in accordance with the patient’s fluid losses and medication administration.
-
Wounds are examined on a daily basis, and adjustments are made to the dressings applied. If a wound is full-thickness, arrangements need to be made to take the patient to the operating room for surgical excision and grafting.
-
Pain and anxiety levels need to be measured and responded to on a daily basis. A variety of pharmacologic strategies are available (Table 8.8) and address both the background discomfort from burn injury itself and the pain inflicted during procedural and rehabilitative activities.
Table 8.8 Sample burn pain management protocol -
Calorie needs are assessed on a daily basis and nutrition adjusted accordingly.
-
-
Acute Phase Management
-
Wound care is performed daily and treatments adjusted according to the changing condition of the wounds (Table 8.9). Selecting the most appropriate method to close the burn wound is by far the most important task in the acute period. During the dressing changes, nurses debride small amounts of loose tissue for a short period of time, ensuring that the patient receives adequate analgesia and sedation. As the devitalized burn tissue (eschar) is removed from the areas of partial-thickness burn, the type of dressing selected is based on its ability to promote moist wound healing. There are biologic, biosynthetic and synthetic dressings and skin substitutes available today (Table 8.10). Areas of full-thickness damage require surgical excision and skin grafting. There are specific dressings appropriate for grafted areas and donor sites.
Table 8.9 Sample burn wound management protocol Table 8.10 Temporary and permanent skin substitutes -
Ongoing rehabilitation, offered through physiotherapy and occupational therapy, is an important part of a patient’s daily plan of care. Depending on the patient’s particular needs and stage of recovery, there are certain range-of-motion exercises, ambulation activities, chest physiotherapy, stretching and splinting routines to follow. The programme is adjusted on a daily/weekly basis as the patient makes progress towards particular goals and as his/her clinical condition improves or worsens.
-
-
Rehabilitative Phase Priorities: maintaining wound closure, scar management, rebuilding strength, transitioning to a rehabilitation facility and/or home
-
Rehabilitative Phase Goal of Care: returning the burn survivor to a state of optimal physical and psychosocial functioning
-
Rehabilitation Phase Assessment
-
The clinical focus in on ensuring all open wounds eventually close, observing and responding to the development of scars and contractures and ensuring that there is a plan for future reconstructive surgical care if the need exists.
-
-
Rehabilitation Phase Management
-
Wound care is generally fairly simple at this time. Dressings should be minimal or non-existent. The healed skin is still quite fragile and can break down with very little provocation. The need to moisturise the skin with water-based creams is emphasised in order to keep the skin supple and to decrease the itchiness that may be present.
-
Visits to outpatient burn clinic provide opportunities for ongoing contact between staff, patients and family post-discharge, wound evaluation and assessment of physical and psychological recovery.
-
Scar maturation begins and contractures may worsen. Scar management techniques, including pressure garments, inserts, massage and stretching exercises, need to be taught to patients, and their importance reinforced with each and every visit.
-
Encouragement is also essential in order to keep patients and families motivated, particularly during the times when progress is slow and there seems to be no end in sight to the months of therapy.
-
The burn surgeon can also plan future reconstructive surgeries for the patient, taking into consideration what improvements the burn patient wishes to see first.
-
8.5.2 Surgical Care
-
Full-thickness burn wounds do not have sufficient numbers of skin-reproducing cells in the dermis to satisfactorily heal on their own. Surgical closure is needed.
-
Common practice in surgical burn management is to begin surgically removing (excising) full-thickness burn wounds within a week of admission. Most patients undergo excision of non-viable tissue (Fig. 8.13) and grafting in the same operative procedure. In some instances, if there is concern the wound bed may not be ready for a graft, the wounds are excised and covered with topical antimicrobials, followed by a temporary biologic or synthetic dressing.
Fig. 8.13 
Surgical excision of full-thickness burn wound
-
Patient preparation preoperatively includes educational and psychological support to ensure an optimal recovery period postoperatively.
-
The donor skin (skin graft), which is harvested in this first O.R., using a dermatome (Fig. 8.14), is then wrapped up in sterile fashion and placed in a skin fridge for later application. Allograft (cadaver skin) may be laid down temporarily.
Fig. 8.14 
Harvesting a split-thickness skin graft. Adrenalin/saline soaks may be applied to donor sites to control bleeding before the donor dressing is applied. Tumescence. Electrocautery may also be used
-
Two days later, the patient returns to the OR to have the excised wounds (recipient bed) examined and the donor skin laid as a skin graft on the clean recipient bed. Dressings remain intact for 5 days postoperatively.
-
Concern over blood loss and lack of sufficient donor sites are the two limiting factors when attempting to excise and graft patients with extensive wounds.
-
Grafts can be split-thickness or full-thickness in depth, meshed or unmeshed in appearance and temporary or permanent in nature (Table 8.11).
Table 8.11 Sources of skin grafts -
Grafts should be left as unmeshed sheets for application to highly visible areas, such as the face, neck or back of the hand (Fig. 8.15).
Fig. 8.15 
Unmeshed split-thickness sheet graft
-
Sheet grafts are generally left open and frequently observed by nursing and medical staff for evidence of serosanguinous exudate under the skin.
-
On other parts of the body, grafts can be meshed using a dermatome mesher (Fig. 8.16). The mesher is set to an expansion ratio chosen by the surgeon. An expansion ratio of 1.5:1 allows for exudate to come through and be wicked into a protective dressing, while at the same time be cosmetically acceptable (Fig. 8.17). Wider expansion ratios (3:1, 6:1) allow for increased coverage when there are limited donor sites.
Fig. 8.16 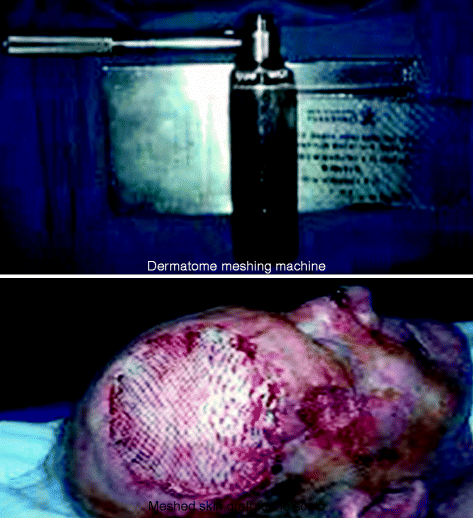
Putting a skin graft through a dermatome mesher. Once harvested, graft is placed on a plastic dermatome carrier and run through a meshing machine. Mesh ratio pattern from 1.5:1 (most common) to 12:1. If donor sites are few and area to cover is large, meshing ratio will increase to 3:1 or 6:1. Exudate can come up through the holes in the mesh pattern to be wicked into the intact dressing. Grafts to the face and hands are not meshed for optimal cosmetic results. These sheet grafts are nursed open
Fig. 8.17 
Meshed split-thickness skin graft
-
Meshed skin grafts are generally covered with one of a number of possible options, including silver-impregnated, vacuum-assisted closure, greasy gauze or cotton gauze dressings. Most are left intact for 5 days to allow for good vascularisation between the recipient bed and the skin graft.
-
Following the initial “take down” at post-op day 5, the dressings are changed every day until the graft has become adherent and stable, usually around day 8.
-
For the next year or so post-burn, the skin grafts mature and their appearance improves (Fig. 8.18). Patients are cautioned that the skin graft appearance will “mature” over the next year and not to be overly concerned about the postoperative appearance.
Fig. 8.18 
(a, b) Mature split-thickness skin graft
-
The donor site can be dressed with either a transparent occlusive, hydrophilic foam or greasy gauze dressing (Fig. 8.19). Donor sites generally heal in 10–14 days and can be reharvested, if necessary, at subsequent operative procedures (Fig. 8.20). Patients are provided with adequate pain management and support as donor sites are very painful.
Fig. 8.19 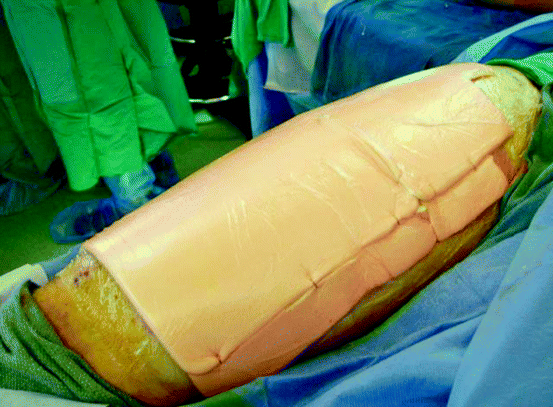
Harvested donor site
Fig. 8.20 
Healed donor site
-
Over the past 10 years, there have been major advancements in the development, manufacture and clinical application of a number of temporary and permanent biologic skin substitutes. Most of these products were initially developed in response to the problems faced when grafting the massive (i.e. >70 %) burn wound where donor sites are limited (Table 8.12). The search for a permanent skin substitute continues.
Table 8.12 Biologic skin replacements








8.5.3 Pharmacological Support
Burn patients are assessed for:
-
Tetanus toxoid, because of the risk of anaerobic burn wound contamination. Tetanus immunoglobulin is given to those patients who have not been actively immunised within the previous 10 years.
-
Pain medication, which should always be administered intravenously during the hypovolemic shock phase as gastrointestinal function is impaired and intramuscular (IM) medications would not be absorbed adequately.
-
The medication of choice for moderate to severe pain management is an opioid, such as morphine or hydromorphone, as they can be given intravenously and orally and are available in fast-acting and slow-release forms (Table 8.8).
-
As the burn wounds close and the patient’s pain level increases, reductions in analgesic therapy should occur by careful taper, rather than abrupt discontinuation, of opioids.
-
-
Sedative agents (Table 8.13).
Table 8.13 Anxiolytics commonly used in burn care -
Non-pharmacologic approaches to pain management (hypnosis, relaxation, imagery).
-
Topical antimicrobial therapy for burn wound care (Table 8.7).
-
The most widely used broad-spectrum antimicrobial agent is silver sulphadiazene. Local application on the burn wound is necessary, as systemic antibiotics would not be able to reach the avascular burn wound.
-
Mafenide acetate is indicated for burned ears and noses as it has a greater ability to penetrate through cartilage.
-
-
Systemic antibiotics when a burn wound infection has been clinically diagnosed or other indicators of sepsis are present, such as pneumonia or uncontrolled fever.
-
Additional medications to manage gastrointestinal complications treat antibiotic-induced superinfections and boost the patient’s metabolic and nutritional status (Table 8.14).
Table 8.14 Medications commonly used in burn care
8.5.4 Psychosocial Support
Psychosocial support to burn survivors and their family members is an essential part of their ongoing care. Concern for family provides them with necessary comfort so they, in turn, can be the patient’s single most important social support.
The social worker in a burn centre can provide ongoing counselling and emotional support to patients and family members. Assistance in coping with difficult or stressful matters, such as financial concerns, finding accommodation, questions about hospital insurance coverage or ongoing problems at work or home, is also available. Chaplains offer spiritual support during times of crisis and at various points along the road to recovery. For some, the burn injury is a tremendous test of spiritual faith and brings forward troubling questions for which there are no easy answers, such as “Why did this happen to me and to my family?” Coming to terms with this traumatic event allows the burn survivor to move forward in a positive way. Some burn patients were troubled psychologically pre-burn. They may have formal psychiatric diagnoses and/or histories of drug and/or alcohol abuse. For others, the psychological trauma begins with the burn injury. Referral to a psychiatrist or psychologist for supportive psychotherapy and/or medication can make a positive difference in those situations. It is important, however, before such referrals are made, to discuss the situation with the patient (if he/she is considered mentally competent). This disclosure provides the team with an opportunity to share their interpretation of the patient’s behaviours and to listen to how the patient views his/her coping abilities and behaviours. The burn patient and his family need to feel supported and not stigmatised by the recommendation to seek psychological support.
In recent years, the role of patient and family support groups has been examined and encouraged by burn team members. The power of the lived experience is profound. The advice and caring that comes from one who truly knows what it is like to survive a burn injury or the family member of one who has been burned is valuable beyond measure [7–9]. Many burn centres are fortunate to have a burn survivor support group affiliated with them. Based in the USA, but with members from around the world, the Phoenix Society has hundreds of area coordinators and volunteers, through the SOAR (Survivors Offering Assistance in Recovery), who meet with burn survivors in their communities and help; however, they can visit http://www.phoenix-society.org or email info@phoenix-society.org or call 1-800-888-2876 (BURN).
School re-entry programmes and burn camps are also widely available through most paediatric burn centres. Additional information can be obtained from the Phoenix Society or from your provincial/state burn unit/centre.
References
Centers for Disease Control and Prevention (2012) Fire deaths and injuries: fact sheet. Available at www.bt.cdc.gov, Accessed on Oct 3, 2012
American Burn Association (2011) Burn incidence and treatment in the U.S. Fact Sheet – 2011. Available at www.ameriburn.org Accessed on Oct 3, 2012
Latenser BA (2009) Critical care of the burn patient: the first 48 hours. Crit Care Med 37:2819
Saffle JR (2007) The phenomenon of “fluid creep” in acute burn resuscitation. J Burn Care Res 28:382
Ahrns KS (2004) Fluid resuscitation in burns. Crit Care Nurs Clin North Am 16:75
Helvig EI (2005) Burn wound care. In: Lynn-McHale Wiegand DJ, Carlson KK (eds) AACN procedure manual for critical care, 5th edn. Elsevier, St. Louis
Kammerer-Quayle BJ (1993) Helping burn survivors face the future. Progressions 5:11
Partridge J (1998) Taking up MacGregor’s challenge. J Burn Care Rehabil 19:174
Blakeney P et al (2008) Psychosocial care of persons with severe burns. Burns 4:433
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2013 Springer-Verlag Wien
About this chapter
Cite this chapter
Knighton, J. (2013). Nursing Management of the Burn-Injured Person. In: Jeschke, M., Kamolz, LP., Shahrokhi, S. (eds) Burn Care and Treatment. Springer, Vienna. https://doi.org/10.1007/978-3-7091-1133-8_8
Download citation
DOI: https://doi.org/10.1007/978-3-7091-1133-8_8
Published:
Publisher Name: Springer, Vienna
Print ISBN: 978-3-7091-1132-1
Online ISBN: 978-3-7091-1133-8
eBook Packages: MedicineMedicine (R0)