
Abstract
Red blood cell (RBC) lysis and iron release contribute to intracerebral hemorrhage (ICH)-induced brain injury. Tissue-type transglutaminase (tTG), which has a role in neurodegeneration, is upregulated after ICH. The current study investigated the effect of RBC lysis and iron release on brain tTG levels and neuronal death in a rat model of ICH. This study had three parts: (1) Male Sprague-Dawley rats received an intrahippocampal injection of 10 μL of either packed RBCs or lysed RBCs; (2) rats had a 10 μL injection of either saline, hemoglobin or FeCl2; (3) rats received a 10 μL injection of hemoglobin and were treated with an iron chelator, deferoxamine or vehicle. All rats were killed 24 h later, and the brains were sectioned for tTG and Fluoro-Jade C staining. Lysed but not packed RBCs caused marked tTG upregulation (p < 0.05) and neuronal death (p < 0.05) in the ipsilateral hippocampus CA-1 region. Both hemoglobin and iron mimicked the effects of lysed RBCs, resulting in tTG expression and neuronal death (p < 0.05). Hemoglobin-induced tTG upreglution and neuronal death were reduced by deferoxamine (p < 0.05). These results indicate that RBC lysis and iron toxicity contribute to neurodegeneration after ICH.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others

Keywords
Introduction
Intracerebral hemorrhage (ICH) is a subtype of stroke with high morbidity and mortality [1]. Community-based studies have indicated a mortality of more than 40%, and many survivors are left with significant neurological deficits [2, 3]. Previous studies have demonstrated that lysed red blood cells (RBC) but not packed RBCs result in marked brain edema at 24 h in a rat ICH model [4]. Both in vivo and in vitro experiments have demonstrated that hemoglobin and its degradation products, especially iron, contribute to brain injury after ICH [5, 6].
Tissue-type transglutaminase (tTG) is abundantly expressed in the brain, and upregulation of tTG may contribute to the pathology of several neurodegenerative conditions, including Alzheimer’s disease, Parkinson’s disease, and Huntington’s disease [7, 8]. Neurodegeneration also occurs after ICH, and evidence indicates that ICH induces perihematomal tTG upregulation and that cystamine, a tTG inhibitor, can reduce ICH-induced brain swelling and neurological deficits [3]. Fluoro-Jade C staining has been used to detect neuronal degeneration [9], and we have developed the intra-hippocampal injection model in rats [10]. In this study, we investigated the effect of iron on the expression of tTG and neuronal death in the hippocampus.
Materials and Methods
Animal Preparation and Intracerebral Infusion
The University of Michigan Committee on the Use and Care of Animals approved the animal protocols. Adult male Sprague-Dawley rats (275–350 g, Charles River Laboratories, Portage, MI) were anesthetized with pentobarbital (45 mg/kg, i.p.). Physiological parameters were recorded immediately before intrahippocampal injections and were in the normal range. Core body temperature was maintained at 37.5°C. Saline, hemoglobin (Hb), FeCl2, packed RBCs and lysed RBCs were infused into the right hippocampus stereotactically (coordinates: 3.8 mm posterior, 3.2 mm ventral, and 3.5 mm lateral to the bregma).
Experiment Groups
This study has three parts: (1) rats (n = 6, each group) received an intrahippocampal injection of 10 μL of either packed RBCs or lysed RBCs; (2) rats (n = 6 each group) had a 10 μL injection of saline, bovine Hb (150 mg/mL) or FeCl2 (1 mM); (3) rats (n = 6 each group) received a 10 μL injection of bovine Hb (150 mg/mL) and were treated with either deferoxamine (100 mg/kg, i.p. given immediately after Hb injection and then every 12 h) or vehicle. All rats were killed 24 h later, and the brains were sectioned for immunohistochemistry and Fluoro-Jade C staining.
Immunohistochemistry
Rats were anesthetized with pentobarbital (60 mg/kg; i.p.) and underwent transcardiac perfusion with 4% paraformaldehyde in 0.1 mol/L (pH 7.4) phosphate-buffered saline. Brains were removed and kept in 4% paraformaldehyde for 6 h, then immersed in 30% sucrose for 3 to 4 days at 4°C. Brains were then placed in optimal cutting temperature embedding compound (Sakura Finetek, Inc., Torrance, CA) and 18-μm sections taken on a cryostat. Sections were examined using the avidin-biotin complex technique. The primary antibody was mouse anti-transglutaminase-2 monoclonal antibody (1:200 dilution, NeoMarkers, Fremont, CA), and the secondary antibody was anti-mouse immunoglobulin G antibody (1:500 dilution, Vector Laboratories, Inc., Burlingame, CA). Normal horse immunoglobulin G (Vector Laboratories, Inc. Burlingame, CA) was used as a negative control. The number of tTG positive cells in the CA1 region was counted.
Fluoro-Jade C Staining
Brain sections were kept in 0.06% potassium permanganate (KMnO4) for 15 min and rinsed in distilled water. Sections were stained by gently shaking for 30 min in a working solution of Fluoro-Jade C (10 mL 0.01% Fluoro-Jade C in distilled water and 90 mL 0.1% acetic acid), then rinsed in distilled water three times. After drying with a blower, slides were quickly dipped into xylol and covered after mounting with DPX. Fluoro-Jade-positive C cells were counted in the CA1 on the pictures taken by a digital camera at high power (×40 magnification) [11].
Statistical Analysis
All the data in this study are presented as mean ± SD. Data were analyzed by Student’s t test. A level of P < 0.05 was considered statistically significant.
Results
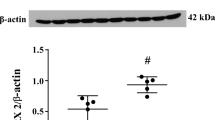
After lysed RBC injection, tTG positive cells were mostly expressed in the ipsilateral hippocampus with very few in the contralateral hippocampus. The number of tTG positive cells was significantly higher in the ipsilateral CA-1 area after injection of lysed RBCs compared to packed RBCs (91 ± 22 vs. 29 ± 13 cells/mm, p < 0.01, Fig. 1a). Lysed RBCs, but not packed RBCs, also induced more Fluoro-Jade C-positive cells in the ipsilateral CA-1 region (81 ± 28 vs. 15 ± 11 cells/mm, n = 6, p < 0.01; Fig. 1b).

tTG (a) and Fluoro-Jade C (b) positive cells in the ipsilateral hippocampus CA-1 area 24 h after an injection of 10 μL lysed RBCs or packed RBCs. Values are expressed as mean ± SD, n = 6, #p < 0.01 vs. packed RBCs
Intrahippocampal injection of Hb and iron mimicked the effects of lysed RBCs on tTG expression and neuronal degeneration. Much higher numbers of tTG positive cells were induced in the ipsilateral hippocampus CA-1 by Hb (125 ± 44 cells/mm) and FeCl2 (127 ± 35 cells/mm) compared to saline (6 ± 6 cell/mm; p < 0.01, Fig. 2a). Also, there were many more Fluoro-Jade-positive cells in the ipsilateral hippocampus after Hb (92 ± 31 cells/mm) and iron injection (110 ± 35 cells/mm) than after saline injection (7 ± 6 cells/mm, p < 0.01, Fig. 2b).

tTG (a) and Fluoro-Jade C (b) positive cells in the ipsilateral hippocampus CA-1 area 24 h after injection of 10 μL saline, Hb (150 mg/mL) or FeCl2 (iron, 1 mM) into the right hippocampus. Values are mean ± SD, n = 6, #p < 0.01 vs. saline
Deferoxamine was used to examine the effect of iron in Hb-induced tTG upregulation and neuronal death. Hb-induced neuronal degeneration was abolished by deferoxamine (tTG positive cells: 29 ± 13 vs. 101 ± 45 cell/mm in vehicle-treated group, p < 0.01, Fig. 3a; Fluoro-Jade C-positive cells: 48 ± 30 vs. 100 ± 26 cells/mm in vehicle-treated group, p < 0.05, Fig. 3b).

tTG (a) and Fluoro-Jade C (b) positive cells in the ipsilateral hippocampus CA-1 area 24 h after an injection of 10 μL hemoglobin (150 mg/mL) in rats treated with either deferoxamine (100 mg/kg) or vehicle. Values are mean ± SD, n = 6, #p < 0.01, *p < 0.05 vs. vehicle-treated group
Discussion
In this study we demonstrate: (1) lysis of RBCs induces brain tTG expression and causes neuronal death in the hippocampus; (2) Hb and iron can mimic the effect of lysed RBCs, causing expression of tTG in hippocampus and resulting in neuronal death; (3) deferoxamine blocks Hb-induced tTG upregulation and neuronal death.
Tissue-type transglutaminase (tTG) has been implicated in various neurodegenerative diseases. tTG has a role in neural development and function [8], but several studies have demonstrated that tTG is present in cells and tissues during apoptotic cell death and is associated with apoptosis [12]. Thus, upregulation of brain tTG has been found in different animal models of CNS diseases, including cerebral ischemia, traumatic brain injury, calcium-induced hippocampal damage and spinal cord injury [13–16]. Our recent study showed that brain tTG levels are increased in the perihematomal area after ICH, and cystamine, a tTG inhibitor, reduces ICH-induced brain edema and neurological deficits [3]. Release of Hb from RBCs and Hb breakdown products cause brain damage after ICH. Iron overload occurs in the brain after ICH, and intracerebral infusion of iron causes brain damage, such as brain edema and oxidative brain injury [17]. The results from our current study suggest that iron can upregulate brain tTG and that such upregulation may contribute to iron-induced brain damage.
To clarify the role of iron in Hb-induced tTG upregulation, an iron chelator, deferoxamine, was used. We found that deferoxamine attenuates Hb-induced upregulation of brain tTG, suggesting that the effects of Hb on tTG are, at least partially, mediated by iron. The mechanisms by which Hb and iron upregulate tTG still need to be fully elucidated. However, it is known that oxidative stress can upregulate tTG in neuronal and astrocyte cultures [18, 19]. This effect may be via both transcriptional regulation [18, 19] and inhibition of proteasomal degradation [20]. In conclusion, iron can increase brain tTG levels and cause brain injury.
References
Qureshi AI, Tuhrim S, Broderick JP, Batjer HH, Hondo H, Hanley DF (2001) Spontaneous intracerebral hemorrhage. N Engl J Med 344:1450–1460
Mendelow AD, Gregson BA, Fernandes HM, Murray GD, Teasdale GM, Hope DT, Karimi A, Shaw MD, Barer DH (2005) Early surgery versus initial conservative treatment in patients with spontaneous supratentorial intracerebral haematomas in the International Surgical Trial in Intracerebral Haemorrhage (STICH): a randomised trial. Lancet 365:387–397
Okauchi M, Xi G, Keep RF, Hua Y (2009) Tissue-type transglutaminase and the effects of cystamine on intracerebral hemorrhage-induced brain edema and neurological deficits. Brain Res 1249:229–236
Xi G, Keep RF, Hoff JT (1998) Erythrocytes and delayed brain edema formation following intracerebral hemorrhage in rats. J Neurosurg 89:991–996
Hua Y, Nakamura T, Keep RF, Wu J, Schallert T, Hoff JT, Xi G (2006) Long-term effects of experimental intracerebral hemorrhage: the role of iron. J Neurosurg 104:305–312
Wagner KR, Sharp FR, Ardizzone TD, Lu A, Clark JF (2003) Heme and iron metabolism: role in cerebral hemorrhage. J Cereb Blood Flow Metab 23:629–652
Citron BA, Suo Z, SantaCruz K, Davies PJ, Qin F, Festoff BW (2002) Protein crosslinking, tissue transglutaminase, alternative splicing and neurodegeneration. Neurochem Int 40:69–78
Lesort M, Tucholski J, Miller ML, Johnson GV (2000) Tissue transglutaminase: a possible role in neurodegenerative diseases. Prog Neurobiol 61:439–463
Gu Y, Hua Y, Keep RF, Morgenstern LB, Xi G (2009) Deferoxamine reduces intracerebral hematoma-induced iron accumulation and neuronal death in piglets. Stroke 40:2241–2243
Song S, Hua Y, Keep RF, Hoff JT, Xi G (2007) A new hippocampal model for examining intracerebral hemorrhage-related neuronal death: effects of deferoxamine on hemoglobin-induced neuronal death. Stroke 38:2861–2863
Schmued LC, Albertson C, Slikker W Jr (1997) Fluoro-Jade: a novel fluorochrome for the sensitive and reliable histochemical localization of neuronal degeneration. Brain Res 751:37–46
Fesus L (1998) Transglutaminase-catalyzed protein cross-linking in the molecular program of apoptosis and its relationship to neuronal processes. Cell Mol Neurobiol 18:683–694
Festoff BW, SantaCruz K, Arnold PM, Sebastian CT, Davies PJ, Citron BA (2002) Injury-induced “switch” from GTP-regulated to novel GTP-independent isoform of tissue transglutaminase in the rat spinal cord. J Neurochem 81:708–718
Tolentino PJ, DeFord SM, Notterpek L, Glenn CC, Pike BR, Wang KK, Hayes RL (2002) Up-regulation of tissue-type transglutaminase after traumatic brain injury. J Neurochem 80:579–588
Tolentino PJ, Waghray A, Wang KK, Hayes RL (2004) Increased expression of tissue-type transglutaminase following middle cerebral artery occlusion in rats. J Neurochem 89:1301–1307
Tucholski J, Roth KA, Johnson GV (2006) Tissue transglutaminase overexpression in the brain potentiates calcium-induced hippocampal damage. J Neurochem 97:582–594
Xi G, Keep RF, Hoff JT (2006) Mechanisms of brain injury after intracerebral haemorrhage. Lancet Neurol 5:53–63
Campisi A, Caccamo D, Li Volti G, Curro M, Parisi G, Avola R, Vanella A, Ientile R (2004) Glutamate-evoked redox state alteration are involved in tissue transglutaminase upregulation in primary astrocyte cultures. FEBS Lett 578:80–84
Curro M, Condello S, Caccamo D, Ferlazzo N, Parisi G, Ientile R (2009) Homocysteine-induced toxicity increases TG2 expression in neuron2a cells. Amino Acids 36:725–730
Luciani A, Villella VR, Vasaturo A, Giardino I, Raia V, Pettoello-Mantovani M, D’Apolito M, Guido S, Leal T, Quaratino S, Maiuri L (2009) SUMOylation of tissue transglutaminase as link between oxidative stress and inflammation. J Immunol 183:2775–2784
Acknowledgements
This study was supported by grants NS-017760, NS-039866 and NS-057539 from the National Institutes of Health (NIH) and 0755717Z and 0840016 N from the American Heart Association (AHA). The content is solely the responsibility of the authors and does not necessarily represent the official views of the NIH and AHA.
Conflict of interest statement We declare that we have no conflict of interest.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2011 Springer-Verlag/Wien
About this chapter
Cite this chapter
Zhao, F., Song, S., Liu, W., Keep, R.F., Xi, G., Hua, Y. (2011). Red Blood Cell Lysis and Brain Tissue-Type Transglutaminase Upregulation in a Hippocampal Model of Intracerebral Hemorrhage. In: Zhang, J., Colohan, A. (eds) Intracerebral Hemorrhage Research. Acta Neurochirurgica Supplementum, vol 111. Springer, Vienna. https://doi.org/10.1007/978-3-7091-0693-8_16
Download citation
DOI: https://doi.org/10.1007/978-3-7091-0693-8_16
Published:
Publisher Name: Springer, Vienna
Print ISBN: 978-3-7091-0692-1
Online ISBN: 978-3-7091-0693-8
eBook Packages: MedicineMedicine (R0)