
Abstract
The first successful kidney transplantation was performed in the 1950s on identical twins in Boston (USA). Nowadays, it is a safe standard therapy for end-stage renal disease (ESRD) with very good success. In 2018, 2191 kidney transplantations were performed in Germany, of which 638 were living donations. The main problem is the severe shortage of post-mortem organs. Alternatives to kidney transplantation are hemodialysis and peritoneal dialysis. In this chapter, organ donation, deceased kidney transplantation and living kidney donation are discussed. The techniques, preoperative preparations, and postoperative management are discussed.
All information concerning law, guidelines and healthcare structure refer to Germany as a member of Eurotransplant and its regulations before 2020.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


10.1 Introduction
-
First successful kidney transplantation (KTx) in 1954 in identical twins in Boston, USA
-
Safe standard procedure with very good success:
-
2018 in Germany: 2191 NTx, thereof 638 living donations
-
-
Problem: Serious organ shortage. Reasons = complex, additional decrease since scandal with organ transplantation
-
Alternative: Therapy of terminal renal failure by replacement procedures:
-
Hemodialysis (HDi)
-
Peritoneal dialysis (CAPD)
-
10.1.1 Legal Framework
-
German Transplantation Act (GTA/TPG) implemented in 1997, last amendment 2012
-
Goal: Promote willingness to donate organs
-
Content German Transplant Act (GTA):
-
Public education
-
Organ donation (post-mortem and living)
-
Organ allocation
-
Organ Transplantation
-
-
Since the introduction of the GTA: Irreversible loss of brain function (formerly: brain death) = recognition as criterion of death
-
Transplantation according to urgency, likelihood of success and equality of chances
10.1.2 Structure in Germany
-
Organization of organ donation: German Foundation for Organ Transplantation (DSO)
-
Organ allocation: Eurotransplant (ET)
-
Organ transplantation: Transplant Centres
Organ donation, allocation and transplantation by independent institutions.
10.1.2.1 German Foundation for Organ Transplantation
-
Structure—7 regions
-
Coordination and implementation of organ donation
10.1.2.2 Eurotransplant
-
Non-profit organisation based in Leiden (The Netherlands)
-
Organ Allocation for:
-
Austria, Belgium, Croatia, Germany, Hungary, Luxembourg, Netherlands, Slovenia
-
-
For Germany: Allocation according to allocation guidelines of the German Medical Association (Bundesärztekammer)
10.1.2.3 Transplant Centers
-
Preparation of the potential recipients
-
Carrying out organ transplantation
-
Follow-up of the recipients after transplantation
10.2 Indication for Transplantation and Preparation of the Recipient
-
Indication for kidney transplantation: Basically in all patients with end-stage renal diseases (ESRD)
-
Prior to registration in the waiting list: Obligatory medical evaluation of the recipient concerning indication of KTx and operability
10.2.1 Indication for Transplantation
10.2.1.1 Indication = ESRD [End-Stage Renal Disease]
-
Liberal indication due to high comorbidity and loss of quality of life due to alternative procedures
-
Waiting time for a post-mortem organ: currently approx. 8–10 years
-
Alternative: Living donation: Also possible preemptively (before the onset of dialysis requirement): sensible starting at approximate glomerular filtration rate (GFR) <15 mL/min
10.2.1.2 Contraindications
-
Severe acute or chronic infections
-
Malignant disease (waiting period between 1 and 5 years)
-
Severe cardiovascular diseases
-
Severe pulmonary diseases
-
Severe psychiatric illnesses
-
Severe extrarenal diseases
-
Alcohol or drug abuse
-
Non-adherence: due to the need for immunosuppression
10.2.1.3 Causes of End-Stage Renal Disease
-
Glomerulonephritis
-
Interstitial nephritis
-
Congenital malformations
-
Bilateral nephrectomy for tumor or trauma
-
Metabolic diseases (e.g. diabetes, oxaluria, etc.)
-
Drug toxicity
-
Hereditary diseases
-
Obstructive diseases
-
Reflux nephropathies
-
Systemic diseases
-
Haemolytic-Uraemic Syndrome (HUS)
-
Irreversible acute renal failure
-
Vasculopathies
Most Common Underlying Condition for New Waiting List Enrollment in 2018 (n = 2348) (Eurotransplant Statistics)
-
Cystic kidney disease: 421
-
Chronic nephritic syndrome: 333
-
Chronic kidney disease: 372
-
Type 1 diabetes: 220
-
Hypertensive kidney disease:206
-
Nephrotic syndrome: 127
-
Chronic tubulointerstitial nephritis: 40
-
Rapid progressive nephritic syndrome: 40
-
Other diagnoses: 589
10.2.2 Recipient Preparation
10.2.2.1 Detailed Information—Medical Aspects
-
Before evaluation of transplantability and qualification for the waiting list
-
About all aspects of kidney transplantation:
-
Registration in the waiting-list
-
Waiting time
-
Transplantation
-
Need for immunosuppression
-
Risks and complications
-
Results
-
10.2.2.2 Medical Evaluation
-
For each organ recipient
-
Objectives/content:
-
Determination of general operability
-
Exclusion of contraindications
-
Compliance review
-
Caution
Due to the permanent immunosuppression required postoperatively, one focus of preoperative diagnosis is the exclusion of possible sources of infection.
10.2.2.3 Diagnostic Procedure
-
Preparation of the recipient = ideally at an early stage before the onset of the dialysis requirement (since a preemptive transplantation can take place in the case of a living donation)
-
Recipient diagnosis in close cooperation with the responsible dialysis center
10.2.2.4 Detailed Anamnesis and Clinical Examination
-
Underlying renal disease
-
Dialysis initiation and procedures
-
Tumor disease
-
Cardiovascular risk factors and pre-existing conditions
-
Pre-existing pulmonary disease
-
Previous operations
-
Infection status
-
Addictive disorders
-
Family medical history
-
Current medication
-
Clinical examination
-
Vascular status
10.2.2.5 Laboratory Tests
-
Blood count, kidney function, electrolytes, liver function, coagulation, inflammatory signs, endocrine diagnosis (HbA1c, parathormone, thyroid levels), PSA (prostate specific antigen, men >45 years)
-
Virology/Bacteriology: Hepatitis B (HBV) and C (HCV); human immunodeficiency virus (HIV), Epstein-Barr virus (EBV), cytomegalovirus (CMV), herpes simplex virus (HSV), varicella-zoster virus (VZV), syphilis (TPHA)
-
Determination of the blood group
-
HLA (“human leucocyte antigen”) typing
-
Donor-specific antibodies
-
Urinalysis
-
Cross-match (living donation)
10.2.2.6 Apparative Examination
-
ECG
-
Chest X-ray
-
Lung function
-
Cardiac echocardiography
-
Exercise ECG, myocardial scintigraphy, coronary angiography if necessary
-
Abdominal sonography
-
Vascular status—if necessary pelvic CT native/angiography
-
CCDS (color-coded Doppler sonography) carotid, if necessary,
-
Urologic evaluation—including cystoscopy
10.2.2.7 Screening
-
Urological screening (men >45 years)
-
Gynaecological screening (women)
-
Colonoscopy (>50 years)
10.2.2.8 Evaluation by Specialist
-
ENT
-
Dentist
-
Dermatologist
-
Urologist
-
Psychological examination, if necessary
10.2.2.9 Vaccinations
-
Influenza
-
Tuberculosis
-
COVID
-
Hepatitis A and B
-
Tetanus
-
Diphtheria
-
Polio
-
Pneumococcus
-
Meningococcus
-
Live vaccines: varicella, measles/mumps/rubella (these are contraindicated under immunosuppression)
Caution
If other diseases are diagnosed, therapy must have been started or completed before registration in the waiting list (e.g. focal treatment for ENT/dental infections, interventional and surgical therapy for CHD, cholecystectomy for symptomatic cholecystolithiasis).
10.2.3 Registration in the Waiting List
10.2.3.1 Indication/Registration
-
Indication is made individually by an interdisciplinary conference (6-eyes-principle)
-
Registration with Eurotransplant as soon as
-
the treating transplant centre has determined indication and
-
all necessary examinations are available
-
Waiting time = time from the first day of dialysis. The time of registration in the waiting list and the registration status have no influence on this.
-
Currently more than 7500 patients in Germany are on the kidney waiting list
10.2.3.2 Urgency Status
-
Distribution (allocation) of organs:
-
Through Eurotransplant
-
According to the urgency status (◘ Table 10.1)
-
-
Causes for immunisation:
-
Previous transplants
-
Blood transfusions
-
Pregnancies
-
-
High-urgency status = extremely rare. Prerequisites:
-
Lack of dialysis access option (vascular surgery report required)
-
Life-threatening situation that can only be resolved by a kidney transplant
-
Severe bladder problems (recurrent cystitis, haematuria) after simultaneous pancreas-kidney transplantation with bladder drainage of exocrine pancreatic secretions. These may occur with loss of graft kidney function and functioning pancreas graft
-
Overview: HU (“high urgency”) status:
-
Application to Eurotransplant
-
Review by expert panel
10.3 Deceased Organ Donation
10.3.1 Organ Donation and Donor Selection
10.3.1.1 Organ Donation
-
Notification of a potential organ donor by the organ retrieval hospital to the DSO
-
Consent to Organ Donation:
-
Existence of written will (e.g. donor card)
-
Oral will (relatives)
-
Presumed will of the patient (relatives)
-
Decision according to the relatives’ own values if the patient’s presumed will is unknown
-
-
Irreversible loss of brain function:
-
Clinical diagnosis by two specialists experienced in the care of severely neurologically ill patients (one of whom is a specialist in neurology/neurosurgery)
-
Apparative diagnosis: e.g. detection of cerebral perfusion arrest, EEG with zero-line
-
Caution
-
Notification to Eurotransplant + further diagnosis: Only permitted after irreversible loss of brain function and if consent to organ donation has been given.
-
Donation in case of cardiocirculatory death: not allowed in Germany
-
Eurotransplant: Deadline of 6 h for the allocation of organs
10.3.1.2 Donor Selection
-
Exclusion of a contraindication to organ donation:
-
Generalized, chronic infection [HIV, HBV, HCV]
-
Malignant disease (waiting period usually = 5 years)
-
Exceptions = non-metastatic brain tumours, skin tumours (excluding malignant melanoma), early-stage prostate tumours
-
Kidney disease
-
-
Carrying out the donation operation in the donor hospital
-
Exact timing depends on the schedule of transplant centers that accept organs with short ischemia time (especially heart, lung)
10.3.1.3 Ischemia Times of Organs
-
Heart: <6 h
-
Lungs: 8 h
-
Liver: 12 h
-
Pancreas: 12 h
-
Kidney: 30 h
10.3.2 Organ Allocation
-
Organ allocation by Eurotransplant
10.3.2.1 Allocation Programs
-
AM (Acceptable Mismatch) Program:
-
All highly immunized patients (PRA >85%)
-
Based on the available HLA typing, organs are selected that are most likely to result in a negative cross-match
-
Patients in the AM program have priority and are allocated before all other patients
-
-
ETKAS program (Eurotransplant Kidney Allocation System, donors <65 years)
-
Allocation within the blood groups
-
Organ allocation (◘ Table 10.2)
-
-
ESP program (Eurotransplant Senior Program, donors ≥65 years)
-
Recipient ≥65 years
-
Regional allocation: short ischemia time
-
Allocation only based on waiting time
-
Waiting time shorter compared to ETKAS
-
No HLA match: immunological risk difficult to assess and usually higher
-
10.3.3 Organ Retrieval
10.3.3.1 Principle
-
All kidneys from donors <2 years of age must be retrieved en bloc
-
Kidneys from donors between 2 and 5 years of age should be retrieved en bloc, but may be divided depending on the recipient profile
-
Kidneys from donors >5 years of age are retrieved as single kidneys as described below
Surgical Procedure
Visceral Organ Perfusion (◘ Fig. 10.1)
-
Insertion of a perfusion cannula in the aortic bifurcation or the common iliac vessel
-
Free preparation of the subdiaphragmatic aorta (above the truncus coeliacus)
-
Ligation of both iliac arteries distal to the catheter as well as the distal vena cava
-
Full heparinisation before the cross clamp
-
Ligation/clamping of the aorta subdiaphragm—cross clamp
-
Immediate start of perfusion, usually with cooled (4 °C) histidine tryptophanetoglutarate (HTK) solution (approx. 8 L)
-
Incision of the distal inferior vena cava as well as the thoracic inferior vena cava, if necessary insertion of a drainage catheter
-
Cooling of the situs with slush ice/Ringer solution

Situs during perfusion
Surgical Procedure
Kidney Retrieval
-
Exposure of the orifice of the left renal vein and dissected at the level of the orifice into the vena cava
-
Transverse transection of the inferior vena cava directly at the upper edge of the confluence of the right renal vein
-
Longitudinal opening of the aorta starting at the aortic bifurcation and extending to the renal arteries
-
Separation of the aorta just above the renal arteries, cutting of the aortic posterior wall, the aorta is left as a patch
-
Transverse transection of the vena cava in the area of the incision
-
After removal of the liver and, if necessary, the pancreas, the kidneys are detached from the retroperitoneum laterocranial.
-
The ureter should be removed as long as possible (clearly beyond the pelvic axis) with surrounding fatty tissue to protect the accompanying vessels
Kidney packing
Caution
Wide variation in renal arterial supply:
-
Often additional superior and/or inferior pole vessels (sometimes several centimeters distant from the main artery)
-
Atypical course of the vessels (e.g. right inferior pole artery often ventral to the vena cava)
-
Ideally, polar arteries should be harvested together with the main artery on a patch
10.4 Living Kidney Donation
10.4.1 Prerequisites
-
Adults at least 18 years of age
-
First and second degree relatives
-
Spouse, partner
-
Persons who have a special personal relationship with the donor
10.4.2 Legal Limits in Germany
-
Altruistic donation
-
Cross-over: Two pairs crossed over in case of AB0 incompatibility, positive cross-match or immunisation
-
Chain transplants: Many pairs crossed over in AB0 incompatibility, positive cross-match or immunisation
10.4.3 Advantages of Living Kidney Donation
-
Short waiting time or preemptive transplantation
-
Better survival of the transplanted kidney
-
Better overall survival of the recipient
-
Mostly direct organ function due to short ischemia time
Absolute priority for living kidney donation = safety of the donor (kidney donor = healthy person with no medical indication for surgery).
10.4.4 Donor Evaluation [Preparation and Diagnosis]
10.4.4.1 Initial Interview with the Potential Donor
-
Verification of the conditions
-
Information about risks for the donor and opportunities for the recipient
-
Exclusion of obvious contraindications by anamnesis
-
Blood group, HLA typing and cross-matching
10.4.4.2 Detailed Medical Examination (Often Inpatient)
-
Anamnesis
-
Medication
-
Clinical examination
-
Lab test
-
Extended virologic examination including e.g. HBV, HCV, HIV, CMV, EBV, etc.
-
24 h collection urine
-
Urine status/sediment
-
Lung function
-
ECG
-
Stress ECG
-
Heart Echography
-
If necessary, long-term blood pressure measurement
-
OGTT (oral glucose tolerance test)
-
Chest X-ray
-
Kidney duplex sonography
-
Abdominal Sonography
-
Psychiatric evaluation if necessary
-
Angio-CT/MRI
-
Renal scintigraphy
-
Screening depending on the age of the donor
10.4.4.3 Presentation to an Ethics Committee
-
Directly in advance detailed explanation by doctor and informed consent
-
Verification of voluntariness
-
Exclusion of organ trafficking
-
Verification of the conditions
10.4.5 Donor Operation
10.4.5.1 OP Procedure
-
Open surgery
-
Laparoscopic
-
Retroperitoneoscopic
10.4.5.2 Open Surgery
-
Advantages:
-
Good overview
-
Good control of the situs
-
-
Disadvantages:
-
Cosmetic (pararectal or lumbar scar)
-
Risk of incisional hernia
-
Risk of abdominal wall relaxation
-
More postoperative pain
-
Longer convalescence
-
Surgical Procedure
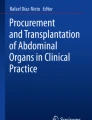
Open Nephrectomy (Minimal Incision; ◘ Fig. 10.2)
-
Positioning: Supine
-
Pararectal section starting from the costal arch (8–10 cm)
-
Severing the lateral abdominal wall
-
Medialisation of the peritoneal sac
-
Exposing the lower pole of the kidney
-
Mobilisation of the entire kidney from laterocaudal
-
Exposure and preparation of the ureter to just below the iliac axis
-
Transection of the ureter (ligation distally, proximally the ureter is not closed)
-
Preparation of the renal vessels from the renal hilus toward central
-
Heparin administration before clamping optional
-
Clamping of the renal vessels centrally and dissection of the vessels
-
Transfer of the kidney for perfusion, cooling and preparation
-
Supply of the vessel stumps with non-absorbable suture material
-
Drainage, wound closure

Open living kidney donation on the left. The V. ovarica/testicularis and V. suprarenalis are already detached and ligated. The renal vein and artery are centrally connected. Caudally the ureter is visible
10.4.5.3 Laparoscopic/Retroperitoneoscopic
-
Advantages:
-
Good overview
-
Cosmetics (Pfannenstiel incision)
-
Less pain
-
Shorter convalescence
-
Lower risk of hernia
-
No relaxation of the abdominal wall
-
-
Disadvantages:
-
Loss of 0.5–1 cm vessel length (can be optimized with narrower staple suture devices)
-
In case of conversion, loss of time due to emergency laparotomy
-
Surgical Procedure
Laparoscopic (Hand-)Assisted Nephrectomy (◘ Fig. 10.3)
-
Positioning: back with slightly raised operating side, on vacuum mattress with pelvic support on opposite side
-
Five trocars (3 × 12 mm, 2 × 5 mm). Placement: 12-mm trocars in the latter Pfannenstiels incision, subumbilical and in the upper abdomen medioclavicular on the contralateral side. 5-mm trocars in the axillary line on the explantation side and epigastric.
-
Entering the retroperitoneum with mobilization of the colon (+duodenum on the right, +pancreas tail and spleen on the left)
-
Right transection of the ovarian vein (technically easier)
-
Exposure and transection of the ureter just below the pelvic axis, the stump is clipped distally
-
Preparation of the ureter up to the hilus
-
Mobilisation of the kidney from laterocaudal and cranial in rendezvous
-
Exposure of the vessels from the hilus to central
-
On the left side, pay attention to the ovaric vein, suprarenal vein and lumbar branches. These must be carefully dissected out and severed between PDS (polydioxanone) clips.
-
Pfannenstiel incision (6–8 cm) and insertion of the port
-
Completing the preparation on the upper pole and vessels
-
Central renal artery and vein disconnection with endo-GIA (vascular)
-
Recovery of the kidney and transfer for perfusion, cooling and dissection
-
Drainage, wound closure

The renal vessels are placed as centrally as possible with an endo-stapler. This results in a loss of approx. 0.5–1 cm of vessel length (width of the stapler)
Surgical Procedure
Perfusion Living Donation
-
Start cooling in 4 °C cold solution (HTK solution, etc.)
-
Irrigation of the kidney with 100 mL heparin solution (50 IU/mL) via the renal artery (in the case of minimally invasive removal, removal of the staple suture line)
-
Flush the kidney with approx. 500 mL perfusion solution until clear reflux via renal vein.
-
Preparation analogous to back-table preparation for postmortem organs
-
Store at 4 °C until transplantation
10.4.6 Risks and Complications
10.4.6.1 Mortality
-
Total mortality = 0.03%
After kidney removal, creatinine levels may be elevated.
10.4.6.2 Morbidity
-
Morbidity: low
-
Bleeding
-
Nausea/vomiting
-
Wound infections
-
Chronic pain
-
Thrombosis
-
Embolism
-
Pneumonia
-
10.4.6.3 Long-Term Risks
-
Proteinuria
-
Arterial hypertension: in about one-third of the cases
-
Risk of needing dialysis: approx. 0.2% (donor) vs. 0.02% (comparable non-donor)
-
Surgical complications
The living kidney donor carries a small residual risk. Therefore, a detailed explanation in the transplant centre (surgeon and nephrologist) is essential before living kidney donation. Perioperative graft loss is particularly stressful.
10.4.7 Donor Aftercare
-
By family doctor or nephrologist
-
3–5 controls during the first year
-
After the first year once a year
-
Recommendation: kidney function, protein excretion and blood pressure control
10.5 Kidney Transplantation
10.5.1 Back-Table Preparation of the Kidney
-
Living kidney donation: Back-table preparation immediately following removal and perfusion
-
Post-mortem kidney removal: back-table preparation is the responsibility of the recipient centre
Surgical Procedure
Back-Table Preparation
-
Tracing of the vessels to the hilus, excess fatty tissue is removed with clamps and ligatures
-
Lateral branches, such as branches to the adrenal gland, are ligated
-
If necessary, vessel reconstruction in case of vessel variations, e.g. polar arteries, accessory vessel supply
-
Exposure of the ureter: The accompanying vessels must be spared at all costs to minimize the risk of ureteral necrosis
-
Caution: Ureter fissus as a norm variant
Checking the seal of the vessels
10.5.2 Surgical Technique of Transplantation
10.5.2.1 Implantation Site
-
Iliac fossa (mostly right), simpler venous vascular access
-
Extraperitoneal position
-
Easy vascular and bladder access
-
Short distance to the bladder
-
Good accessibility for biopsy, ultrasound
-
Surgical Procedure
Kidney Transplantation (◘ Fig. 10.4)
-
Positioning: Supine
-
Preparation: Central venous catheter, sterile insertion of a bladder irrigation catheter, filling of the bladder
-
Hockey stick-shaped cut in the lower abdomen
-
Opening of the lateral abdominal wall: M. obliquus externus, M. obliquus internus and M. transversus
-
Medialization of the peritoneal sac
-
Sparing preparation of the iliac axis in order to ligate as few lymphatic vessels as possible
-
If necessary, shortening of the transplant kidney vein and end-to-side anastomosis to the distal inferior vena cava, common iliac vein or external vena cava, continuous suture with non-absorbable suture material
-
Implantation of the artery mostly on the A. iliaca communis (aorta or A. iliaca externa also possible), continuous suture with non-absorbable suture material
-
The vessels should come to rest without kinking or torsion
-
Reperfusion, if necessary haemostasis in the area of the anastomoses, the hilus and the renal capsule
-
Opening the bladder roof
-
Ureterocystoneostomy and antirefluxplasty according to Lich-Gregoir
-
Ureter must lie free of torsion and tension
-
Implantation of a DJ (double J) catheter optional
-
Drainage, wound closure

Situs after kidney transplantation. The vessels lie stretched. The ureter is then anastomosed with the bladder
10.5.2.2 Immunosuppression
-
Started shortly before reperfusion by steroid bolus
-
250 mg methylprednisolone i.v.
Application of 20% mannitol and Lasix before anastomotic opening = optional and not evidence-based.
-
pAVK in the recipient can significantly complicate implantation; central = create anastomosis proximal to a stenosis; if possible: thrombendarterectomy with vessel reconstruction before actual transplantation
-
In paediatric recipients: anastomosis mostly to aorta and v. cava = compensation of a discrepancy of recipient and donor vessels + possibility of transplantation of kidneys from adult donors to small recipients
Caution
A living donor transplant is technically more challenging due to the lack of an arterial patch.
10.5.3 En Bloc Renal Transplantation
10.5.3.1 Principle
-
Organs from donors <5 years and <10 kg weight
-
Aorta and v. cava of the donor serve as vascular elongation for connection to recipient vessels
10.5.3.2 Advantages
-
Double nephron mass by transplantation of two kidneys
-
Good long-term prognosis
10.5.3.3 Disadvantages
-
Higher complication rate
-
Transplantation must be critically reviewed in young women due to possible pregnancy
-
Difficult biopsy in case of rejection
10.5.4 Surgical Complications
10.5.4.1 Vascular System (Incidence <5%)
10.5.4.1.1 Postoperative Bleeding/Haematoma
-
Localisation: Retroperitoneum, anastomoses, renal parenchyma
-
Occurrence: Immediately postoperative
-
Cause: coagulation disorder, medication (ASS) and infections
-
Therapy: Depending on dynamics and clinical presentation, reoperation if necessary
10.5.4.1.2 Arterial Thrombosis
-
Symptom: Sudden stop of diuresis
-
Occurrence: Early postoperative
-
Diagnosis: Color-coded duplex sonography
-
Therapy: Immediate reoperation and attempt at revascularization
10.5.4.1.3 Graft Vein Thrombosis
-
Symptoms: Sudden stop of diuresis
-
Occurrence: Early postoperative
-
Diagnosis: Color-coded duplex sonography
-
Therapy: Immediate reoperation and attempt at thrombectomy
10.5.4.1.4 Renal Artery Stenosis
-
Symptoms: creatinine increase, arterial hypertension
-
Occurrence: Medium/long term after transplantation
-
Diagnosis: Color-coded duplex sonography
-
Therapy: If possible, interventional therapy with stent, reoperation is likely to cause complications
10.5.4.2 Urological Complications (Incidence 2–10%)
10.5.4.2.1 Urinary Leakage
-
Localization: Laterocranial to the bladder
-
Symptoms: pain, creatinine increase, signs of infection
-
Diagnosis: Sonography, puncture, Mibi (microbiology)/creatinine in the punctate, localization by retrograde pyelography
-
Cause: Frequently high bladder pressure in contracted bladder, ureteral necrosis, injury to urinary drainage system during transplantation
-
Therapy: Depending on location, low-pressure drainage with indwelling bladder catheter (BDK), Splint if necessary, ureteral reimplantation if necessary
10.5.4.2.2 Ureteral Stenosis
-
Localization: Mostly prevesical
-
Symptoms: Urinary retention, pain, creatinine increase, late signs of infection
-
Diagnosis: Sonography, retrograde pyelography
-
Cause: Often swelling in the anastomosis area, scarred stricture of the anastomosis, ureteral necrosis
-
Therapy: Splint, in case of persistence ureteral reimplantation
10.5.4.2.3 Ureteral Necrosis
-
Localization: Prevesical
-
Symptomatology: Clinical presentation of ureteral leakage or ureteral stenosis
-
Diagnosis: Depending on the symptoms
-
Therapy: Reimplantation of the ureter with resection of the necrotic portion
10.5.4.3 Lymphatic Complications (Incidence 2–18%)
10.5.4.3.1 Lymphocele
-
Localization: Mostly mediocaudal to the kidney
-
Symptoms: Urinary retention, pain, increase in retention levels
-
Diagnosis: Sonography, puncture
-
Therapy: Laparoscopic or open fenestration after intraperitoneal
10.6 Postoperative Treatment
10.6.1 Inpatient Stay
-
Length of stay: approx. 14–21 days
10.6.1.1 Content
-
Monitoring of urine production
-
Balanced electrolyte and water balance
-
Early mobilisation
-
Adjusting immunosuppression
-
Prophylaxis: Ulcer (pantoprazole), Candida infections (fluconazole), Pneumocystis jirovecii (cotrimoxazole), CMV (valganciclovir; ◘ Table 10.3)
10.6.1.2 Delayed Graft Function (DGF)/Acute Tubular Necrosis (ATN)
-
Ischemia reperfusion injury
-
Incidence: Up to 30% in postmortem renal transplantation, incidence increases with increase of cold ischemia time
-
No therapy possible, ensure sufficient fluid intake, adequate immunosuppression
-
Problem: Differential diagnosis of other causes of graft failure:
-
Acute rejection: biopsy
-
Circulatory disorder: Color-coded duplex examination
-
Caution
A clinical assessment is not possible in DGF/ATN due to lack of excretion. Therefore, in this situation, a kidney biopsy is always indicated after 7 days.
10.6.2 Immunosuppression
10.6.2.1 Immunosuppressive Therapy
-
Induction phase (transplantation and early postoperative phase)
-
Triple therapy (see below) in higher dosage
-
If necessary, (in case of high immunological risk) additional induction therapy with: Monoclonal (non-depleting) antibodies (e.g. basiliximab) or polyclonal (depleting) antibodies (e.g. antithymocyte globulin)
-
-
Maintenance phase (starting approx. 6 months after transplantation)
-
Triple therapy in low dosage
-
10.6.2.2 Standard Triple Therapy
-
Calcineurin inhibitor (Tacrolimus)
-
Antimetabolite (mycophenolate mofetil, azathioprine)
-
Glucocorticoids (prednisolone)
10.6.2.3 Immunological Risk Factors
-
Long cold ischemia time
-
Low histocompatibility (≥3 HLA mismatches)
-
Donor organ (donor >40 years)
-
Recipients (<50 years)
-
Retransplant
-
Immunized recipient (PRA level elevated)
10.6.2.4 Immunosuppressive Agents
-
Mechanism of action, side effects and application ◘ Table 10.4
-
Dosing according to phase ◘ Table 10.5
Caution
In all immunosuppressed patients:
-
Significantly increased risk of infection
-
Therefore, early anti-infective therapy is obligatory.
-
Opportunistic infections must be included in the differential diagnosis
Individual immunosuppression of each patient weighing the immunological risk versus the risk of infection.
10.6.2.5 ABO-Incompatible Transplantation (Living Donation)
-
Special preparation of the recipient
-
In Europe: 375 mg/m2 BSA (body surface area) rituximab (Mabthera®) 4 weeks before planned transplantation
-
1 week before transplantation start immunoadsorption/plasmapheresis: removal of circulating blood group antibodies against donor blood group
-
IgG titre in target range (IgG <4), then transplantation
-
Triple therapy: Start 1 week preoperative
-
Induction with basiliximab
-
1 week postoperative daily: Titre control and immunadsorption in case of rising titres (in our lab IgG >8)
-
2 weeks postoperative every 2 days: Titre control and immunadsorption in case of rising titres (in our lab IgG >16)
-
Accommodation (exact mechanism unclear): From >2 weeks postoperative: No more titre controls
-
-
Results regarding long-term function of the grafts identical to AB0-compatible living donation
-
Higher risk of developing lymphoceles: Preoperative mycophenolate mofetil administration or immunoadsorption as a cause are discussed
AB0-incompatible living kidney donation for blood group incompatibility = safe standard therapy.
10.6.3 Organ Rejection
10.6.3.1 Hyperacute Rejection
-
Extremely rare since the introduction of the cross-match
-
Aetiology: Circulating antibodies against the donor organ
-
Minutes after reperfusion of the graft
-
Cross-match: Compatibility testing of recipient serum with donor blood, spleen or lymph node cells
10.6.3.2 Acute Rejection
-
Rejection within days to months after transplantation: In approx. 10% of all kidney transplants
-
Clinical presentation: creatinine increase >20%, decrease in excretion, painful, swollen graft
-
Color-coded duplex sonography: increase in intrarenal resistance index
-
Gold standard: kidney biopsy (Banff classification; ◘ Table 10.6)
-
Therapy:
-
T-cell mediated rejection: steroid boli
-
Vascular rejection: antithymocyte globulin
-
Humoral rejection: antithymocyte globulin, plasmapheresis
-
For all forms, increase the dose of maintenance immunosuppression
-
10.6.3.3 Chronic Rejection
-
Rejection within months to years after transplantation
-
Pathomechanism:
-
Formation of donor-specific antibodies (de novo DSA), connection with poor adherence (immunosuppressants) is currently being discussed
-
Recurrent subclinical rejections
-
Presence of memory cells (B lymphocytes) for the formation of donor-specific antibodies, not detected by cross-match and HLA typing (e.g. in the case of living donation from child’s father to mother)
-
-
Clinical presentation: Slow, continuous deterioration of renal function.
-
Therapy:
-
Increasing immunosuppression
-
For donor-specific antibodies mostly frustrating
-
10.6.4 Infections
-
Increased risk due to immunosuppression
10.6.4.1 Bacterial Infections
-
Mostly urinary tract infections or pulmonary infections
-
Atypical germs must be included in differential diagnosis
-
Early resistance-appropriate antibiotic therapy
10.6.4.2 Opportunistic Infections
-
Mostly in the first year after transplantation (higher immunosuppression)
-
Mostly viral infections (CMV, BKV)
-
Common pathogens:
-
CMV
-
Aspergillosis
-
Candida
-
Clostridium difficile
-
10.6.5 Aftercare
-
After discharge from hospital:
-
Initially 2–3 times weekly in cooperation with a nephrologic centre
-
In the course increase of the interval
-
-
One visit per year to the transplant centre
-
Main focus: creatinine progression, immunosuppression
10.7 Results
-
Survival rates ◘ Table 10.7
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2023 The Author(s), under exclusive license to Springer-Verlag GmbH, DE, part of Springer Nature
About this chapter

Cite this chapter
Jänigen, B., Billmann, F., Pisarski, P. (2023). Kidney Transplantation. In: Billmann, F., Keck, T. (eds) Essentials of Visceral Surgery . Springer, Berlin, Heidelberg. https://doi.org/10.1007/978-3-662-66735-4_10
Download citation
DOI: https://doi.org/10.1007/978-3-662-66735-4_10
Published:
Publisher Name: Springer, Berlin, Heidelberg
Print ISBN: 978-3-662-66734-7
Online ISBN: 978-3-662-66735-4
eBook Packages: MedicineMedicine (R0)