
Abstract
Physical activity is an important factor for mental and physical development of children and has benefits for their health especially for their cardiovascular system. The individual development of children and adolescents has to be considered in sport activities. Because of the growing skeleton there is a need for individualized training to prevent overuse injuries. Furthermore, pre-participation screening programs (orthopedic and cardiovascular) are highly recommended to confirm eligibility. Basic knowledge of pediatric medical subjects, e.g., vaccinations, is important in taking care of junior athletes.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
1 Background
Youth sports culture has changed drastically over the past decades. It has become normal that children and adolescents participate in organized sports, specialize in a single sport at younger ages, and play all year round. More children are doing intensive training and have more rigorous competition schedules. Physical activity in children starts at the age of 2–3 years with gymnastics and balance bikes and continues with swimming and kicking until they enter into a club to specialize in their preferred sport at the age of 6–7 years. At the age of 10–11 professionalization, with its specific concomitants, and the selection for elite teams begins. By now, at the latest, a pre-participation screening (orthopedic and cardiovascular) should be performed to confirm eligibility for competitive sports. Playing multiple sports and delaying specialization, is more advantageous if the goal is to succeed athletically. Participating in multiple sports decreases the chance of injuries, stress, and burnout.
2 Physiological Aspects to Consider
Intensive training in young athletes may affect various components of their health, including cardiac, maturation, musculoskeletal. They also have special nutritional requirements—not only for their physical activity—but also for their growth in terms of calories, iron, calcium, and vitamin D. Especially in a pubertal growth spurt, it is important to ensure an adequate iodine intake for proper thyroid gland function as well.
3 Musculoskeletal Aspects to Consider
“Children are not little adults”—and in consequence there are some anatomical and physiological aspects to consider while working with young athletes (Table 1.1). The athlete’s body capacity to withstand stress and in consequence the sportive performance depends on the biomechanics of the growing skeleton. The musculoskeletal system in junior athletes not only consists of muscles, bones, tendons, ligaments, articulation cartilage, but also of apophysis and growth cartilage, which is unique in children. The growth area is divided into several regions: the epiphysis, the growth cartilage, and the metaphysis. The growth takes place in the cartilage area. There the composition of the cellular matrix is different and this leads in consequence to a lower stability. In times of increased growth like in puberty, the mechanical stability of the growth areas decreases and is more susceptible for traumatic and overuse injuries. Locations of typical, age sport-specific injuries in junior athletes, are, for example, the proximal femur epiphysis (Epiphysiolysis capitis femoris), apophysis injuries (e.g., the proximal tibia apophysis: M. Osgood–Schlatter), the apophysis of the vertebral body (M. Scheuermann) or spondylolysis.
Consequently, the training load has to be adapted to the development phases of the athletes. This consideration implicates a precise training regulation regarding intensity because of the heterogeneity of athletes especially in the pubertal phase (girls: 11–13 years, boys: 13–15 years).
Another important aspect to prevent injuries in junior athletes regarding the musculoskeletal system is to perform regular orthopedic screenings to discover early static changes of the normal growth: the leg axis and rotations of the lower limb, hip mobility and spine axis, and finally yet importantly the foot anatomy. In addition, dynamic factors have to be determined regularly like the dynamic knee valgus in one-foot-standing, so that deficits can be detected early and can be approached with specific preventive training programs (mobilization, core stability, jumps and landings, agility) such as FIFA 11+.
4 General Medical Aspects to Consider
4.1 Cardiovascular Aspects
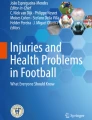
Sudden cardiac death (SCD) in children and adolescents is rare. The reported incidence of SCD for adolescent and young adults ranges from 0.5 to 20 per 100,000 person-years. Several studies have reported a higher risk (2–2.5 times greater) of SCD during athletic competition or exercise. Etiologies included congenital heart disease, hypertrophic cardiomyopathy, primary arrhythmia, mitral valve prolapse, myocarditis, and congenital coronary artery abnormalities (Fig. 1.1). Although SCD is often the initial presenting event, retrospective studies have shown that warning signs or symptoms were noted by 30–50% of affected individuals prior to SCD. The most common symptoms were chest pain and actual or near syncope. Other symptoms included dizziness, palpitations, or dyspnoea. Pre-participation screening has the potential to detect those athletes with higher risk of SCD. We recommend that junior athletes should undergo a standardized cardiovascular screening protocol with medical history taking, a physical examination, 12-lead resting electrocardiogram, and a transthoracic 2D-echocardiography before the start of competitive sport and should be repeated every second year to detect progressive diseases.

Cardiovascular reasons for sudden cardiac death in athletes (modified Maron et al., 2007, Circulation 115:1643–1655). ARVC arrhythmogenic right ventricular cardiomyopathy, HCM hypertrophic cardiomyopathy, LVH left ventricular hypertrophy, MVP mitral valve prolapse
4.2 Respiratory Aspects
In majority of junior athletes, exercise tolerance is limited by cardiovascular and muscular factors. Yet some young athletes do experience respiratory problems with exercise. These problems can be related to underlying acute and chronic respiratory conditions (e.g., infectious disease, asthma, cystic fibrosis, chest wall deformities, neuromuscular disorders, and exercise-induced bronchoconstriction). Although respiratory symptoms can be suggestive of asthma, the diagnosis of asthma should be based on objective measurements. Pharmacologic management of respiratory problems can be difficult and in treatment of athletes with asthma, anti-doping regulations have to be considered (e.g., use of glucocorticosteroids, ß-adrenergic agonists). Exercise-inducible laryngeal obstruction has also been recognized as a relevant respiratory problem in children practicing sports.
4.3 Neurology Aspects
If there is any history of pre-syncope or syncope in a junior athlete, a thorough medical checkup is mandatory. Cardiovascular diseases (e.g., primary arrhythmias, congenital heart defects, systemic hypertension, etc.), metabolic (e.g., hypoglycemia), and neurological reasons (e.g. epileptic seizures) have to be excluded. Even in pharmacological well-controlled epilepsy the decision to compete in water sports (e.g., openwater swimming, rowing, etc.) or disciplines with a potentially higher risk (e.g., climbing, motor sports) should be individualized. There is still an ongoing scientific debate about prophylaxis of concussion in youth sports (e.g., headings in football) to avoid possible irreversible damage of neurological structures. The sports associations are going to develop specific guidelines depending on sport disciplines and age.
4.4 Infectiological Aspects
Prevention of sudden cardiac death due to myocarditis is a key issue in taking care of an athlete with an infectious disease. It is important to note that the clinical presentation of myocarditis with an asymptomatic course complicates both diagnosis and prevention. In myocarditis, the risk for sudden cardiac death does not correlate with the intensity of inflammation. In addition, exercise in patients suffering from myocarditis may worsen cardiomyopathy. The best method of prevention would be a detailed education of young athletes, their families and coaches explaining that suspending exercise during infections can reduce the risk for sudden cardiac death. Furthermore, junior athletes should be immunized by inactivated vaccines against tetanus, diphtheria, pertussis, hepatitis A, hepatitis B, Haemophilus influenzae type b, pneumococci, meningococci C, influenza and by live vaccines against measles, mumps, rubella, and varicella. An appropriate time for vaccination would be at the onset of resting periods. Side effects after inactivated vaccines can be expected within 2 days after vaccination, whereas after live attenuated vaccines they are more likely to occur after 10–14 days.
4.5 Psychological Aspects
There is evidence of burnout and overtraining in children who are specializing in just one sport to early. The concerning statistic is that 70% of kids drop out of organized sports by the age of 13 years. Burnout in children can have very vague symptoms and signs. Often, these children feel depressed or they are irritable. To reduce the likelihood of burnout in youth sports, an emphasis should be placed on skill development over competition and winning. Diversifying and playing multiple sports is actually beneficial, mentally and physically. Multiple sports use different muscles and different bones. Furthermore, making sure that junior athletes take some time off from one particular sport is very important both physically and mentally.
5 Pitfalls in This Population
-
High risk of overuse injuries, especially in elite junior levels, caused by:
-
Insufficient knowledge about specifics of the growing athlete (musculoskeletal) among coaches and health professionals.
-
Specializing in one single sport to early (before puberty).
-
Increased physical load without breaks.
-
-
Risk of sudden cardiac death due to:
-
Congenital cardiovascular disease.
-
Infectious myocarditis.
-
6 Fact Box
-
During athletic competition or exercise there is a higher risk of sudden cardiac death.
-
Pre-participation screening (orthopedic and cardiologic) is recommended to confirm eligibility for competitive sports.
-
“One sport kids” are prone to burnout, overtraining, and overuse injuries.
-
Personalized training will reduce the risk of overuse injuries in the growing athlete.
-
Physical and mental burnout is prevented through “prophylactic” breaks in training.
Recommended References
Drezner JA, Pelliccia A, Corrado D et al (2017) International criteria for electrocardiographic interpretation in athletes: consensus statement. Br J Sports Med 51(9):704–731
DiFiori JP, Benjamin HJ, Brenner JS et al (2014) Overuse injuries and burnout in youth sports: a position statement from the American Medical Society for Sports Medicine. Br J Sports Med 48:287–288
Fritsch P, Oberhoffer R, Petropoulos A et al (2017) Cardiovascular pre-participation screening in young athletes: recommendations of the Association of European Paediatric Cardiology. Cardiol Young 27(9):1655–1660
Gerling S, Loose O, Krutsch W et al (2019) Echocardiographic diagnosis of congenital coronary artery abnormalities in a continuous series of adolescent football players. Eur J Prev Cardiol 26:988–994. https://doi.org/10.1177/2047487319825520
Loose O, Achenbach L, Krutsch W (2018) Injury incidence in semi-professional football claims for increased need of injury prevention in elite junior football. Knee Surg Sports Traumatol Arthrosc 27:978–984. https://doi.org/10.1007/s00167-018-5119-8
Author information
Authors and Affiliations
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2020 ESSKA
About this chapter

Cite this chapter
Loose, O., Gerling, S. (2020). Junior Athletes. In: Krutsch, W., Mayr, H.O., Musahl, V., Della Villa, F., Tscholl, P.M., Jones, H. (eds) Injury and Health Risk Management in Sports. Springer, Berlin, Heidelberg. https://doi.org/10.1007/978-3-662-60752-7_1
Download citation
DOI: https://doi.org/10.1007/978-3-662-60752-7_1
Published:
Publisher Name: Springer, Berlin, Heidelberg
Print ISBN: 978-3-662-60751-0
Online ISBN: 978-3-662-60752-7
eBook Packages: MedicineMedicine (R0)