
Abstract
In 1875, Friedrich Merkel described the cells that bear his name, found within the epidermis and along sweat ducts and hair follicles. These cells are involved in touch reception [1] and are of neuroendocrine lineage, but their origin continues to be an issue of some controversy [2]. Merkel cell carcinomas (MCCs) are tumors that arise from these cells in the dermis; they are usually asymptomatic but may grow significantly over a short period of time. The lesions are red to purple and may appear cystic. They tend to arise in areas of ultraviolet exposure and are often seen in immunocompromised individuals. Most are associated with polyoma virus infection, but the role of polyoma virus in the pathogenesis of MCC is controversial, as antibodies to the virus are seen in up to 50% of the general population. MCC is extremely uncommon in African Americans.
Access provided by CONRICYT-eBooks. Download chapter PDF
Similar content being viewed by others

Keywords
1 Introduction
In 1875, Friedrich Merkel described the cells that bear his name, found within the epidermis and along sweat ducts and hair follicles. These cells are involved in touch reception [1] and are of neuroendocrine lineage, but their origin continues to be an issue of some controversy [2]. Merkel cell carcinomas (MCCs) are tumors that arise from these cells in the dermis; they are usually asymptomatic but may grow significantly over a short period of time. The lesions are red to purple and may appear cystic. They tend to arise in areas of ultraviolet exposure and are often seen in immunocompromised individuals. Most are associated with polyoma virus infection, but the role of polyoma virus in the pathogenesis of MCC is controversial, as antibodies to the virus are seen in up to 50% of the general population. MCC is extremely uncommon in African Americans.
In a large review of the National Cancer Institute’s SEER (Surveillance, Epidemiology, and End Results) database, MCC was found to occur more commonly in males (62%), those of white race (95%), and age greater than 70 years (72%). The most common sites of origin were the head and neck (44%), extremities (37%), and trunk (11%). These tumors were localized in 49% of patients, with regional nodal involvement in 31% and distant metastases in 8% [3]. Like melanomas, MCCs are a challenge to the surgical oncologist because of their high rates of local recurrence and regional or distant metastases, with a poorer prognosis than squamous cell or basal cell carcinomas.
2 Operative Details
2.1 Wide Local Excision
The basic surgical principles for the treatment of MCC are similar to those for melanoma, except for the fact that MCCs are more radiosensitive than melanomas. In general, the primary tumor should be removed with an adequate margin, and in clinically node-negative patients, the regional lymph nodes should be staged by sentinel lymph node biopsy. If the sentinel lymph node is positive, then a regional lymphadenectomy, irradiation of the nodal basin, or both are recommended [4]. In patients with clinically node-positive MCC, sentinel node biopsy is unnecessary. Instead, confirmatory fine-needle aspiration followed by regional lymphadenectomy and/or irradiation of the nodal basin should be performed [5]. Further descriptions of these formal lymph node dissections and of the controversy regarding the optimal surgical versus radiotherapeutic management of regional nodal basins are beyond the scope of this volume.
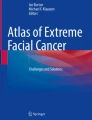
The margins of excision in MCC are a point of controversy, and there are no good, randomized studies to guide the surgeon. Given that intradermal dissemination is common and local recurrence is frequently a problem, wider margins should be considered. Using the treatment of melanoma as a guide, margins of 2 cm are reasonable, where possible. If the lesion is on the trunk, an elliptical incision along Langer’s lines should be carried out, with 2 cm of clearance from the edge of the lesion laterally along the line; the length along the axis should be three times this width to avoid dog ears (6 cm in each direction from the lesion). If the lesion is on an extremity, the long axis should be oriented in a vertical direction along the axis of the limb (Fig. 21.1).
Once the ellipse is marked, incise the skin through the dermis into the subcutaneous fat. Use electrocautery to divide the fat circumferentially down to the underlying muscle (Fig. 21.2a). It is optional as to whether to remove the fascia of the muscle or leave it intact. Pass off the specimen after marking the superior edge with a short stitch and the lateral edge with a long stitch to orient the specimen, in case of positive margins (Fig. 21.2b). Reduce tension by creating flaps, elevating the fat off of the muscle for several centimeters circumferentially. Reapproximate Scarpa’s fascia using simple 2-0 or 3-0 Vicryl sutures, placing 6–8 sutures and tagging them with clamps (Fig. 21.3a). Begin tying the sutures at each end, with an assistant pushing the skin edges together as the sutures are tied. If there is a significant depth between Scarpa’s fascia and the skin, another layer of simple 3-0 Vicryl sutures may be placed to further close the defect and approximate the subcutaneous wound edges. Place 3-0 nylon vertical mattress sutures spaced at 1-cm intervals through the skin edges (Fig. 21.3b), then tag these with clamps. Begin tying from each edge, with an assistant pushing the skin edges together to reduce tension. If the skin can be brought together with these 3-0 sutures, the wound will heal, but the sutures should be left in place for 2 weeks. There is a tendency for wound edges brought together under significant tension to heal with a thick scar and keloid formation, but most patients find this preferable to the even less cosmetic alternative of a skin graft.

Orientation of incisions of the lower extremity (a), upper extremity (b), and trunk (c)

(a) Excision of skin and subcutaneous tissue in an ellipse 2 cm from the lesion in the short axis and 6 cm in the long axis. (b) Marking of the specimen with a long stitch on the lateral edge and a short stitch on the superior edge

(a) Scarpa’s fascia is approximated with interrupted 2-0 Vicryl sutures, then 3-0 nylon vertical mattress sutures are placed but not tied. (b) Closure of the skin after tying nylon sutures
2.2 Local Flaps
If cosmesis is a concern, a simple flap may be considered. A rotational flap can be fashioned by drawing a 90° arc from the apex of the defect, then making an incision of several centimeters at a right angle to the base. The tissue is extensively undermined above the level of the muscle fascia, and then rotated into the defect (Fig. 21.4a). Alternatively, a rhomboid flap can be created by making an incision from the edge of the wound for a distance of about three quarters of the width of the wound. Next, an incision of the same length is made from the end of this line at 60°, so that it runs parallel to the wound edge. The tissue between the incisions is freed up from the underlying muscle, keeping the fascia with the flap for improved blood supply. The point at the edge of the wound and the first incision is sutured to the edge of the wound at the opposite side. The point where the two incisions meet is sutured to the apical area of the wound between the first two points, and then the edge of the bottom incision is rotated to the wound edge (Fig. 21.4b). Interrupted nylon sutures are then used to approximate the edges of the rhombus to the circular defect and to close the lateral incision.

(a) Rotational flap: a 90° arc is made laterally and then rotated into place. (b) Rhomboid flap: an incision is made perpendicular to the edge, slightly smaller than the diameter of the wound; the same length incision is made at 60°. Tissue is extensively undermined, then rotated into the defect as shown. The numbers designate the initial and final positions of the corresponding areas of skin.
2.3 Sentinel Lymph Node Biopsy
Patients are brought to the Nuclear Medicine suite prior to their procedure, and 0.5–2 mCi (18–74 MBq) of filtered 99Tc-sulfur colloid is injected intradermally in four quadrants around the base of the skin lesion. This injection is generally done within a few hours of surgery, but good results can be obtained even when it is done 12–24 h prior to surgery. Lymphoscintigraphy is performed with a gamma camera to determine the nodal basins draining from the lesion. For extremity lesions, these will be in the corresponding axillary or inguinal areas, only rarely involving the epitrochlear or popliteal regions for distal extremity lesions. For truncal lesions, the drainage is less predictable, and could involve either or both axillae and/or inguinal regions, or even cervical nodes. If two to three nodal basins show uptake on lymphoscintigraphy, then that part of the skin can potentially drain to any of these nodes, so sentinel nodes will need to be dissected out for all of these nodal basins.
The patient is transported to the operating room, where we prefer the use of general anesthesia. Using a 25-gauge needle, 0.5–3 mL of isosulfan blue dye (Lymphazurin; US Surgical-Tyco; Norwalk, CT, USA) is injected intradermally in four quadrants around the primary lesion (Fig. 21.5a). If the needle is truly in the intradermal space, the injection will be very difficult, and a blue wheal will develop slowly at the injection site; if the dye goes into the skin easily, then it is probably being injected subcutaneously, which may lead to less reliable mapping. Patient positioning will then depend on the site of the primary tumor and the draining nodes; we try not to have to reposition patients, but sometimes it is necessary, especially if multiple drainage basins are seen. We generally perform the sentinel node biopsy prior to excision of the primary to reduce the risk of contamination of the instruments, which may occur if the primary is resected first. In some cases, however, especially when the lesion is very close to a nodal basin, the primary must be resected first so that background levels can be reduced and will interfere less with the node counts.
Before dissection of a nodal basin, a gamma probe (Navigator, Dilon Diagnostics, Newport News, VA, USA; Neoprobe®, Devicor Medical Productions, Cinncinnati, OH, USA; or C-Trak®, Care Wise Medical Products, Brandon, FL, USA) is passed in vertical lines moving from medially to laterally to determine the site of highest counts, then in horizontal lines inferiorly to superiorly (Fig. 21.5b). The site at which these two areas of highest counts intersect is then marked, and a 10 second count (the pre-excision count) is recorded. Occasionally, lymphoscintigraphy will demonstrate two independent drainage pathways to different nodes (as opposed to one channel traversing a first node and then later appearing in a second node along the same lymphatic channel). When this happens, the two separate nodes should be marked. An incision of 2–3 cm is made over the location of maximal counts (Fig. 21.6a). If this location is in the femoral or inguinal region, the orientation should be vertical or horizontally in a skin crease. These should be oriented so that that if a completion nodal dissection is later carried out, the biopsy site can be encompassed by the lymphadenectomy incision. In the axilla, we generally use an incision that can be encompassed by a future bucket handle incision at the edge of the axillary hairline, when possible.
Once the incision is made, the subcutaneous fat is divided with cautery to a depth of approximately 1 cm. The wound is held open using a self-retaining mastoid retractor; then the gamma probe is placed into the wound. It is aimed in all directions until the area of maximal counts is identified, and a second 10 second count is recorded (in situ count; Fig. 21.6b). Dissection is carried out using a clamp and cautery, dividing the fat in the direction of the node, until a blue node with high counts is seen (Fig. 21.6c). This node is then removed using cautery, and a 10 second count is taken with the node held away from the patient (ex vivo count). Next, the gamma probe is placed back in the wound and aimed in all directions. When the maximal counts are found, then another 10 second count is taken. If this count is 90% less than the pre-excision count or the in situ count, then this nodal basin is finished. If counts remain above this level, it is likely that there is another sentinel node, which should be sought out and removed in similar fashion. After ensuring adequate hemostasis, the subcutaneous layer is reapproximated with one or two 3-0 Vicryl sutures and the skin is closed with a 4-0 Monocryl subcuticular stitch. Surgical glue is applied over the incision.

(a) Intradermal injection of isosulfan blue dye (Lymphazurin) in four quadrants around the primary lesion. (b) Passage of the gamma probe vertically and horizontally to define the area of highest counts

(a) A skin incision 2–3 cm in length is made over the site of maximum counts, oriented along the extremity (or Langer’s lines, if in the head and neck or trunk). (b) In situ counts are taken to determine the direction and depth of dissection. (c) Subcutaneous dissection is carried out until a blue node with high radioactivity is found
3 Results and Follow-Up
Patients return to the clinic for removal of sutures from the primary lesion in 2 weeks. If pathologic examination reveals a close or positive margin, then a re-excision may be necessary. If the sentinel node contains metastatic MCC, then a completion nodal dissection or radiation of the regional nodes is indicated. Depending on the location of the involved node, this procedure would involve an axillary dissection, a superficial and/or deep inguinal node dissection, or potentially a modified neck dissection. It is advisable to perform an 18FDG-PET scan prior to the regional node dissection to rule out distant metastases. The presence of such metastases may argue against further lymphadenectomy, especially in elderly or immunosuppressed patients. If the patient presents with palpably enlarged nodes that are positive on fine-needle aspiration, then a regional nodal dissection, regional irradiation, or both should be performed instead of a sentinel node biopsy. A PET scan would be recommended prior to the procedure to rule out distant disease.
In the SEER database, 10-year survival rates were 71% for patients with localized disease, 48% for those with regional disease, and 20% for those with distant disease [3]. In a series of 251 patients from Memorial Sloan-Kettering Cancer Center, recurrence was seen in 102 (43%) of 237 patients presenting with localized or regional disease, within a median of 9 months. Distant metastases were ultimately seen in 21% of patients presenting with locoregional disease. Factors significantly associated with improved survival were head and neck site, tumor size less than 2 cm, use of chemotherapy, the absence of lymphovascular invasion, and clinical nodal status (which was the only factor significant by multivariate analysis) [6].
Treatment of local recurrence is re-excision, radiotherapy, or both. Distant recurrences are commonly associated with local recurrence, and one should consider performing a PET scan if local recurrence is found. Metastatic disease or troublesome locoregional recurrence can be quite chemosensitive. Various chemotherapy regimens (such as those used for small cell carcinomas) are used, but responses typically last less than a year [2].
References
Maksimovic S, Nakatani M, Baba Y, Nelson AM, Marshall KL, Wellnitz SA, et al. Epidermal Merkel cells are mechanosensory cells that tune mammalian touch receptors. Nature. 2014;509:617–21.
Prieto Munoz I, Pardo Masferrer J, Olivera Vegas J, Medina Montalvo MS, Jover Diaz R, Perez Casas AM. Merkel cell carcinoma from 2008 to 2012: reaching a new level of understanding. Cancer Treat Rev. 2013;39:421–9.
Albores-Saavedra J, Batich K, Chable-Montero F, Sagy N, Schwartz AM, Henson DE. Merkel cell carcinoma demographics, morphology, and survival based on 3870 cases: a population based study. J Cutan Pathol. 2010;37:20–7.
Bichakjian CK, Coit DG, Wong SL. Radiation versus resection for Merkel cell carcinoma. Cancer. 2010;116:1620–2.
Zager JS, Messina JL, Glass FL, Sondak VK. Unanswered questions in the management of stage I-III Merkel cell carcinoma. J Natl Compr Cancer Netw. 2014;12:425–31.
Allen PJ, Bowne WB, Jaques DP, Brennan MF, Busam K, Coit DG. Merkel cell carcinoma: prognosis and treatment of patients from a single institution. J Clin Oncol. 2005;23:2300–9.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2017 Springer-Verlag GmbH Germany
About this chapter
Cite this chapter
Howe, J.R. (2017). Wide Excision and Sentinel Node Mapping for Merkel Cell Carcinoma. In: Howe, J. (eds) Endocrine and Neuroendocrine Surgery. Springer Surgery Atlas Series. Springer, Berlin, Heidelberg. https://doi.org/10.1007/978-3-662-54067-1_21
Download citation
DOI: https://doi.org/10.1007/978-3-662-54067-1_21
Published:
Publisher Name: Springer, Berlin, Heidelberg
Print ISBN: 978-3-662-54065-7
Online ISBN: 978-3-662-54067-1
eBook Packages: MedicineMedicine (R0)