
Abstract
Vascular exclusion techniques in liver surgery include continuous inflow occlusion (first described by J. H. Pringle in 1908), intermittent inflow occlusion (first described by M. Makuuchi in the late 1970s), ischemic preconditioning and (continuous) total vascular exclusion. The use of inflow occlusion varies considerably among centers: some use it routinely, whereas others use it only exceptionally. When using inflow occlusion, a low central venous pressure (CVP) (< 5 mm Hg) needs to be maintained to reduce bleeding caused by backflow from the hepatic veins. The effect of a low CVP associated with a Pringle maneuver can be equivalent to total vascular exclusion. Total vascular exclusion, on the other hand, can lead to cardiovascular instability by reducing cardiac preload. Therefore, adequate volume loading with a high CVP (> 10 mm Hg) must be maintained, or a venovenous bypass is sometimes required in this setting.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
These keywords were added by machine and not by the authors. This process is experimental and the keywords may be updated as the learning algorithm improves.
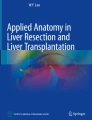
Vascular exclusion techniques in liver surgery include continuous inflow occlusion (Fig. 41.1a) (first described by J. H. Pringle in 1908), intermittent inflow occlusion (Fig. 41.1b) (first described by M. Makuuchi in the late 1970s), ischemic preconditioning (Fig. 41.1c) and (continuous) total vascular exclusion. The use of inflow occlusion varies considerably among centers: some use it routinely, whereas others use it only exceptionally. When using inflow occlusion, a low central venous pressure (CVP) (< 5 mm Hg) needs to be maintained to reduce bleeding caused by backflow from the hepatic veins. The effect of a low CVP associated with a Pringle maneuver can be equivalent to total vascular exclusion. Total vascular exclusion, on the other hand, can lead to cardiovascular instability by reducing cardiac preload. Therefore, adequate volume loading with a high CVP (> 10 mm Hg) must be maintained, or a venovenous bypass is sometimes required in this setting.

Fig. 41.1
Indications and Contraindications
-
Reduction of blood loss during parenchymal dissection
-
Dissection in proximity of major vascular structures
-
Tumor invading vena cava or all hepatic veins, central hepatectomy (for total vascular exclusion)
-
Technical reasons (adhesions, etc.)
-
Cardiac failure (for total vascular exclusion)
Intraoperative Complications
-
Splenic rupture (exceptional): Remove clamps and attempt conservative management of splenic rupture. If not possible, proceed with splenectomy.
-
Cardiovascular instability (in total vascular exclusion): Ensure adequate fluid loading, open clamps, consider venovenous bypass.
Techniques of Vascular Exclusion
Pringle maneuver (inflow occlusion)
A right-angle clamp is passed under the hepatoduodenal ligament to allow a Mersilene band to be placed around it (Fig. 41.2a). A red rubber catheter is passed over the band. It is then pushed downwards as a tourniquet to occlude the ligament, and clamped in place (Fig. 41.2b). The time of inflow occlusion should now be noted. An alternative technique is to place a vessel clamp on the hepatoduodenal ligament (Fig. 41.2c). We prefer the tourniquet because it is mobile and does not get in the way when performing the hepatectomy. Another alternative is to selectively clamp portal venous and arterial branches when a dissection of the structures in the hepatoduodenal ligament has been performed, such as for cholangiocarcinoma.

Fig. 41.2
Total vascular exclusion
Before total vascular exclusion can be performed, the liver needs to be completely mobilized, as for a liver transplantation. ( Chap. 60, “Orthotopic Liver Transplantation”.)
The hepatoduodenal ligament is dissected and the tourniquet is placed around it without closing, as described for inflow occlusion.
The infrahepatic vena cava is prepared on its right and left side for 2 to 3 cm. The right adrenal vein must be identified and transected through ligatures (Fig. 41.3).

Fig. 41.3
A finger is passed under the cava from the right to the left, and the connective tissue is dissected on the finger with electrocautery (Fig. 41.4a). A large right angle is then passed under the infrahepatic vena cava (Fig. 41.4b) and isolated with a Mersilene band (Fig. 41.4c), which is then pulled through a catheter, as when performing inflow occlusion (tourniquet technique as in the Pringle maneuver discussed previously).

Fig. 41.4
Mobilize the retrohepatic and suprahepatic vena cava up to the diaphragm. This is accomplished by passing a finger behind the vena cava and cauterizing the connective tissue (Fig. 41.5). There are no venous branches in this area.

Fig. 41.5
Clamp first the hepatoduodenal ligament to avoid any hypertension in the liver by occluding the outflow. Occlude the infrahepatic cava with the corresponding tourniquet. If this is not tolerated, total vascular exclusion cannot be performed. If it is tolerated, lift up the left hepatic hemiliver and place a large, curved vascular clamp from left to right on the suprahepatic cava, as high as possible. Check whether it can be closed. Clamp the suprahepatic vena cava, including a little bit of diaphragm, if possible (Fig. 41.6a). The liver is now in total vascular exclusion (Fig. 41.6b). We do not routinely use venovenous bypass in this setting. (See the section on venovenous bypass in Chap. 60, “Orthotopic Liver Transplantation”.)

Hepatic vascular exclusion with preservation of the caval flow
Hepatic vascular exclusion with preservation of the caval flow excludes the liver from systemic circulation, thus avoiding caval occlusion. With this method, caval clamping is replaced by hepatic vein clamping. Inflow occlusion is accomplished by clamping of the portal triad, and outflow occlusion by clamping of the hepatic veins (and, if present, clamping of the right inferior hepatic vein) (Fig. 41.7a).
The benefit of this method is a combination of inflow and outflow vascular occlusion without the hemodynamic and biochemical disadvantages of total vascular exclusion or hemorrhage due to venous backflow during the Pringle maneuver alone.
The vascular exclusion can be partial (selective) to the left or the right parts of the liver.
Left partial hepatic vascular occlusion is achieved by selective clamping of the left and middle hepatic veins (outflow occlusion) and complete clamping of the portal triad (inflow occlusion) to avoid middle hepatic vein congestion (Fig. 41.7b). Right partial hepatic vascular occlusion is achieved by selective clamping of the right hepatic vein and right inferior hepatic vein, if present (outflow occlusion), combined with clamping of the right portal pedicle or portal triad (Fig. 41.7c).

Fig. 41.7
Reconstruction of the Vena Cava
This technique is an alternative to associated cava reconstruction. It restores liver perfusion while working on the vena cava.
Open hepatic outflow by releasing the clamp on the suprahepatic vena cava. Clamp the vena cava again below the hepatic veins (Fig. 41.8).

Fig. 41.8
Open hepatic inflow by releasing the tourniquet on the hepatoduodenal ligament. Now the retrohepatic cava is occluded while the liver is perfused.
The retrohepatic vena cava can now be resected. Reconstruction is accomplished with a Gore-Tex interposition graft in an end-to-end fashion. Then release the cava clamp and the tourniquet on the lower cava (Fig. 41.9).

Fig. 41.9
Tricks of the Senior Surgeon
-
Always search for anatomic variants, especially an aberrant left hepatic artery. This artery must be selectively clamped in addition to occlusion of the ligament.
-
Best inflow occlusion is accomplished by pushing down the tourniquet, clamping the band right behind it to hold the tension, and then pushing it down again with some force, before fixing it in position by clamping the tourniquet and the band. This can be repeated several times (“milking down technique”). When inflow occlusion is insufficient, especially in a very large hepatoduodenal ligament, a second tourniquet can be placed and occluded.
-
When bleeding is encountered under total vascular exclusion, the most likely reason is incomplete inflow occlusion. If an obvious reason cannot be identified, open outflow (but keep inflow occlusion and infrahepatic caval occlusion) and ask the anesthesiologist to lower the CVP.
Acknowledgments
We would like to acknowledge Felix Dahm and Pierre-Alain Clavien who were the authors of this chapter in the first edition of the Atlas.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2016 Springer-Verlag Berlin Heidelberg
About this chapter
Cite this chapter
Limani, P., Lesurtel, M. (2016). Techniques of Vascular Clamping, Vascular Exclusion, and Caval Resection in Liver Surgery. In: CLAVIEN, PA., Sarr, M., Fong, Y., Miyazaki, M. (eds) Atlas of Upper Gastrointestinal and Hepato-Pancreato-Biliary Surgery. Springer, Berlin, Heidelberg. https://doi.org/10.1007/978-3-662-46546-2_41
Download citation
DOI: https://doi.org/10.1007/978-3-662-46546-2_41
Published:
Publisher Name: Springer, Berlin, Heidelberg
Print ISBN: 978-3-662-46545-5
Online ISBN: 978-3-662-46546-2
eBook Packages: MedicineMedicine (R0)