
Abstract
Zero-link Hb (OxyVita®, OXYVITA, Inc., New Windsor, New York), a new generation hemoglobin-based-oxygen-carrier (HBOC), is produced using a modified zero-linked polymerization mechanism that employs chemical activators to incorporate inter-dimerically cross-linked bovine hemoglobin tetramers into “super-polymeric” macromolecules (Average M. wt. = 17 MDa) for oxygen delivery when whole blood or packed red cells are not available. This molecular design pathway was developed to address several basic biochemical and physiological concerns associated with earlier generations of HBOCs. Observations made during pre-clinical (various animal models) and clinical studies provided evidence these earlier generation acellular HBOCs gave evidence of reduced retention times within the circulatory system, extravasation across endothelial tissue membranes due to their small molecular size leading to arterial and veinous vasoconstriction that was coupled with rapid increases in mean arterial pressure (MAP) upon infusion. Zero-link Hb’s increased molecular size and structural stability was developed in direct response to these serious concerns that accompanied the evolution of HBOC development within the past several decades. The distinct nature of the zero-linked synthetic route eliminates the need for chemical linkers within the product, eliminates side reaction concerns: such as reversibility and decomposition due to weak and non-specific chemical bonding, changes in temperature and/or pressure within the circulatory system, and residual toxicity. The incorporation of these molecular design characteristics within OxyVita Hb have been responsible for significant findings as determined by the pre-clinical studies that have been carried out by many independent investigators between 2002 to 2012. This chapter will present: (1) a short overview of previous generation HBOCs; (2) the experimental development of OxyVita Hb (liquid and powder forms); (3) the physiochemical properties and functional behavior of OxyVita Hb; and (4) the implications of the molecular design properties for pre-clinical studies that involved issues of extravasation and vasoconstriction, increases in MAP, regulation of oxygen delivery, and effects on coagulatory functions.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others



Keywords
- Mean Arterial Pressure
- Mean Arterial Blood Pressure
- Defense Advanced Research Project Agency
- Defense Advanced Research Project Agency
- Bovine Hemoglobin
These keywords were added by machine and not by the authors. This process is experimental and the keywords may be updated as the learning algorithm improves.
1 Introduction and Background
For several decades extensive research efforts have been directed towards the molecular design of therapeutic oxygen carriers for use when whole blood or packed red blood cells are not available. (Winslow 2008; Alayash et al. 2007; Winslow 2007; Jahr et al. 2012). Most of these efforts have centered upon the development of cell-free (acellular) hemoglobin-based oxygen carriers (HBOC) with the expectation of adequate oxygen delivery as needed.
The rationale for considering the use of an acellular hemoglobin approach goes back many years and has its roots in nature as illustrated in both the terrestrial and marine environments (Hirsch and Harrington 2000; Harrington et al. 2007; Harington et al. 2010). Within natural evolution, the advantage of large polymeric acellular oxygen transport proteins was found to be effective for oxygen transport/delivery for many invertebrate organisms whether living within terrestrial or aquatic conditions (Royer et al. 2006 and 2007). The most obvious characteristic of these functioning natural polymers is the lack of a cellular membrane associated with mammalian red blood cell which normally houses a protective array of enzymes to maintain these hemoglobins in the reduced state necessary for functionality. Given these observations and our understanding of how these acellular oxygen delivery proteins function in vivo, the quest for a safe and efficacious acellular HBOC for clinical application has provided an opportunity to pursue a variety of approaches in molecular design enabling newer HBOCs to address the human physiological conditions(Buehler and Alayash 2008; Estep et al. 2008)
As one examines the efforts to address the development of a functioning HBOC for clinical use, there was the recognition that most of the proposed HBOCs need to function as an acellular molecular species within the human circulatory system. Unfortunately the details of how this was to occur did not receive sufficient attention in the earlier generation of HBOCs, resulting in a series of physiological effects that were recognized to be detrimental in many animal studies and for human clinical applications (Estep 2008).
The evolution of HBOC development at the molecular level has seen important design considerations incorporated into new molecular species with the goal of addressing the many negative characteristics associated with the first generation HBOCs (Stowell et al. 2001; Silverman and Weiskopf 2009; Alayash 2004). These design modifications were initiated with the introduction of an intermolecular cross-linking approach (DCL-Hb/HemAssist®, M.wt. 64 kDa, Baxter Corp., Deerfield. IL.) reducing dimerization of the initial tetrameric hemoglobin. This was followed by several different polymeric approaches involving intermolecular cross-linking polymerization by glutaraldehyde (a non-specific bifunctional cross-linking agent) to cross-link bovine hemoglobin tetramers producing a heterogeneous distribution of larger molecular weight species, (HBOC-201/Hemopure®, human application, and HBOC-200/Oxyglobin®, veterinary applications, M. wt. > 150 kDa, OPK Biotech, Cambridge, MA), raffinose cross-linked human hemoglobin (Hb-Raffinose/Hemolink®, M.wt. > 100 kDa), and pyridoxylated glutaraldehyde cross-linked human hemoglobin (Poly SFH-P PolyHeme®, M.wt. > 120 kDa, Northfield Labs, Evanstone, IL.). Concurrently, several recombinant human hemoglobins were developed that allowed for modification of the oxygen binding properties of these recombinant hemoglobins (rHb1.0 rHb2.0, M.wt. 64 kDa, Somatogen/Baxter Corp.).
Eliminating the dimerization of stroma free hemoglobin (small molecular radii) associated with rapid elimination from the circulatory system and reduced stress within the glomerulus and kidneys was an immediate goal of this approach. Larger molecular weight cross-linked human and bovine hemoglobins were designed with the idea of increasing retention time within the circulation and limiting access to the smaller vascular membrane pores. The rationale here was to limit hemoglobin extravasation and mitigate nitric oxide (NO) binding that is now known to be involved with an increase in vasoconstriction coupled with an elevation in MAP (Olsen et al. 2004).
Pursuing a different direction to alter the molecular size and hydrodynamic properties of an HBOC, pegylated human Hb (MP4, Sangart Inc., San Diego, CA.) the Hemospan product (selected pegylation, M.wt. ~ 90 kDa) was introduced in the 1990s to reduce extravasation thereby mitigating vasoconstriction and maintaining MAP (Vandegriff et al. 2003). This approach was associated with increased water of hydration of this HBOC leading to an increase in the effective hydrodynamic radius of these molecular species, reducing the tendency to extravasate.
Many of these early HBOCs evaluated in phase I−III studies received initial approval for clinical testing because they had demonstrated effectiveness in the delivery of oxygen in specific pre-clinical and specific clinical situations. However, observations of adverse events associated with their use prevented FDA regulatory approval for full clinical use (Winslow 2008; Alayash et al. 2007; Silverman and Weiskopf 2009). Several underlying reasons for this lack of approval by the FDA were due to the inadequacy of the fundamental chemistry employed in the creation of several of these HBOCs and their physiochemical properties. Molecular size and shape, structural integrity (conformational integrity and quaternary structural intactness), redox behavior and stability (ability to be maintained and function in the reduced state) within the human circulatory system are vital to an HBOC functioning as a safe and efficacious therapeutic oxygen delivery system. Several earlier HBOC studies failed to provide this kind of structural information to the scientific community about the molecular integrity, stability, and redox activities of these HBOCs.
This chapter will provide a rationale for the development of a new generation HBOC, OxyVita Hb. Focus will be on its unique molecular design and the physiochemical properties associated with functionality essential for addressing many issues associated with previous attempts to produce an FDA approved therapeutic oxygen delivery acellular hemoglobin. The design and development of OxyVita Hb has resulted from understanding the lessons learned from the data and behavior, or lack thereof, of many previous pre-clinical and clinical studies carried out over the many years of work within this arena. The ultimate goal is to provide the clinical community with a new safe and efficacious therapeutic oxygen carrier as an alternative to blood transfusions when blood or red blood cells are not available. The original effort in the development of this new generation HBOC began in the laboratory of Professor Enrico Bucci and his co-workers (Razynska and Bucci 1998) at the University of Maryland, wherein they utilized a unique zero-linked hemoglobin polymerization technology. Further refinement of OxyVita’s molecular properties has been carried out during a period of scale-up from laboratory preparation to a commercial scale level of production by OxyVita, Inc. It is now recognized that molecular size and the unique chemistry of OxyVita hemoglobin are directly linked to the success of initial pre-clinical studies conducted by many independent investigators throughout the United States (Matheson et al. 2002; Rebel et al. 2003; Mito et al. 2009; Reynolds et al. 2007; Jahr et al. 2008).
1.1 Development: A New Molecular Design Leading to the Production of the Liquid and Powder Forms of OxyVita Hemoglobin
-
(a)
Preparation and synthesis of OxyVita hemoglobin: Although any tetrameric mammalian hemoglobin may be used as the starting material for the preparation of a zero-linked polymeric hemoglobin, bovine blood was chosen as the raw material due to its ubiquitous availability world-wide. Fresh bovine blood is obtained from USDA-approved facilities, providing appropriate documentation of an animal herd. Purification of bovine hemoglobin is carried out through a process of red cell lysis using a hypotonic phosphate buffer, pH 7.4, followed by a series of low-speed and high-speed centrifugation to remove cellular debris. The isolated tetrameric hemoglobins then undergo β-β cross-linking [bis (3,5 dibromosalicyl-adipate)] in preparation for the synthesis of polymeric OxyVita Hb.
The zero-linked polymerization process is governed by the use of a chemical “activator” that initiates the production of intermolecular polymers. In the production of OxyVita Hb, the water soluble carboiimide, EDC [1-ethyl-3-(3-dimethylaminopropyl) carbodiimide], is responsible for the activation of the side chain carboxylate groups on the hemoglobin surface, resulting in a highly reactive and short-lived O-acylisourea derivative. This isourea by-product is very water soluble and is removed directly by dialysis. The complex is formed from the carboxylate groups of C-terminal and side chains of Glu and Asp globin residues of globin. These activated species react with the N-terminal amino groups or amino side chain of the lysyl residues of an adjacent hemoglobin tetrameric molecule to form a stable amide bond (covalent), referred to as a pseudo-peptide bond (Grabarek and Gergely 1990). Some interference can occur during this activation process wherein the activated carboxylic groups may be hydrolyzed by water, limiting their reactivity with available lysyl amino groups. To improve on the efficiency of the polymerization process, a two-step approach to enhance the yield of the amide bond formation was introduced. The introduction of N-hydroxysulfosuccinimide (sulfo-NHS) to the carbodiimide reaction resulted in the formation of an intermediate sulfo-NHS ester, which then reacts with the amino groups (Staros and Wright 1986). One advantage of this approach is the ability to modulate the extent of polymerization by altering the relative amounts of sulfo-NHS and EDC within the reaction mixture. Control of the reaction rate, time and concentration within the polymerization process allows for better regulation of the average molecular weight sizes of an individual preparation.
A more extensive description of this zero-linked polymerization process as applied to the production of the original “zero-linked bovine hemoglobin” (ZL-HbBv) as first described and produced by Professor Enrico Bucci and co-workers can be found in Razynska and Bucci (1998). Earlier pre-clinical studies utilized these initial preparations which typically contained a heterogeneous distribution of high molecular weigh species in the range of 25 MDa (Bucci et al. 2007).
After the initial laboratory development of this bovine zero-linked polymeric hemoglobin, OxyVita, Inc. acquired the license for commercial manufacturing of this HBOC. It introduced some modifications of the preparation procedures in order to produce a more homogeneous molecular weight polymer with an average M. wt. of 17 MDa. Using anion-exchange (DEAE) and size exclusion chromatography (Fractogel 20−40), purification and isolation of discrete molecular weight fractions were achieved. Recent pre-clinical studies (Mito et al. 2009; Jahr et al. 2008; Jia and Alayash 2009) have used the OxyVita Hb preparations within their experimental protocols.
-
(b)
Preparation of OxyVita hemoglobin-powder: The powder from of OxyVita Hb is produced by the lyophilization of the liquid form of this protein. Recent acquisition of a new lyophilization (Virtus, Inc) instrument allows for the production of this product under specific control processing. The new instrument has the capabilities of monitoring (CFR/211 compliant software) the essential steps associated within the freeze-drying process as well as automatically sealing of the product, thus reducing the chances of any endotoxin introduction during the course of the operation. In creating the powder form of OxyVita Hb consideration has been given to a number of different formulations that include the need for proper buffering, essential electrolytes and final osmolarity essential for infusion (IV) applications. Presently, re-constitution time (solubility) is between 10 and 30 s depending upon the compositional constituents.
2 Chemical and Structural Properties of OxyVita Hb
-
(a)
Unique chemistry: The differentiating chemical and structural properties of OxyVita Hb are due fundamentally to the unique chemical and physical methods utilized in its production as described in the methods section. OxyVita Hb is synthesized through a polymerization reaction of purified (ββ)-cross-linked tetrameric bovine hemoglobin using controlled activators which are removed after the initial phase of synthesis. This activation process primarily involves the carboxylic surface residues of the cross-linked tetramers which lead to the formation of the “zero-linked” polymeric molecular species. Selected modulation of these reactions allows for specific lysine residue involvement due to the differential pKs exhibited by these residues at pH 6.7. This approach allows for the absence of any chemical linkers between tetramers remaining within the product, eliminating possible side chain reaction concerns, such as reversibility and decomposition due to weak chemical bonds, dependency on temperature and pressure, and residual toxicity. The pseudopeptide bonds between the globin chains themselves provide a dramatic increase in the structural stability of OxyVita Hb as discussed in the following section (Harrington et al. 2010; Harrington et al. 2011).
The modified production methods allow for enhanced manufacturing and quality control resulting in sustained reproducible batch to batch preparations with a mean molecular weight of 17 MDa as determined by dynamic light scattering. Less than 5 % methemoglobin is present in each preparation. Given the unique chemistry associated with the use of reaction activators, variation of concentration of components involved, time and temperature of polymerization, this flexible polymerization process allows for the production of a range of molecular weight molecules, which may find different clinical applications in the future. Another advantage is this polymerization process allows for the use of any mammalian blood (tetrameric hemoglobin) as the starting raw material for a zero-linked polymeric hemoglobin production.
-
(b)
Implications for the structural-functional relationship of OxyVita Hb: These pseudo-peptide bonds created by the use of activiators, allow the tetrameric hemoglobin molecular linkages within OxyVita Hb to play a crucial role in the overall conformational stability of these large polymeric molecules. Essential structural integrity and biological functionality depend upon the integrity of intramolecular and intermolecular bonds within the tetrameric units and between these multiple tetrameric units (~1000 hemes/polymer) that go to form this “super-polymeric” HBOC. Given the inherent secondary and tertiary structure of bovine hemoglobin (~75 % α-helical) and the fact that within each tetramer cross-linking between the β-82 lysines residues occurs providing inherent tetrameric stability as well, indicates OxyVita Hb will possess increased conformational stability and be very resistant to molecular unfolding. This resistance to conformational unfolding may provide increased protection to the heme-iron moieties responsible for the transport and reversibly binding of molecular oxygen within the circulatory system and oxygen delivery as needed.
Studies on the structural integrity of this “super-polymeric” HBOC carried out by isothermal unfolding studies at 37° C using urea as the perturbant of the secondary and tertiary structure of these large molecules (Harrington et al. 2010; Harrington et al. 2011) are consistent with the presence of strong intermolecular bonding between these tetramers. Figure 15.1 demonstrates the resistance of this HBOC protein to molecular unfolding as compared to several natural acellular polymeric hemoglobins found in the terrestrial and marine environments. The Soret spectral region (350−450 nm) was used to determine the extent of secondary and tertiary conformational changes associated with this HBOC’s unfolding due to its extreme sensitivity to alterations within the heme environment. When tetrameric hemoglobin molecules are in the presence of a conformational perturbant, such as urea, increasing the urea’s concentration leads to the disruption of many intramolecular interactions responsible for the maintenance of the integrity of the native functional structure.
Fig. 15.1 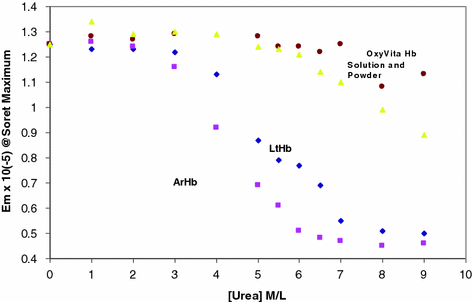
Isothermal unfolding of acellular hemoglobins (arenicola hemoglobin, ArHb; lumbricus hemoglobin, LtHb; and OxyVita Hb, liquid and powder preparations) in the presence of increasing concentrations of urea at T = 37° C. All solutions were equilibrated for 30 min prior to spectral runs (Harrington et al. 2010)
Another advantage of using the Soret spectral region is that it allows for analysis of the redox state of the hemoglobin associated with the unfolding process. In the case of most hemoglobins, spectral wavelength shifts to lower wavelength (blue shift) are associated with an oxidation of the heme-iron as molecular unfolding occurs. Maintenance of the heme-iron complex in the reduced state (heme-Fe+2) is essential for the reversible binding/release of molecular oxygen in vivo. In contrast to LtHb and ArHb, both large acellular natural polymeric hemoglobins, wherein the Soret wavelength maximum blue shifts are 413 → 400 nm and 412→ 398 nm, respectively, OxyVita Hb undergoes little change in the Soret maximum, 410 → 408 nm over the entire range of increasing urea concentrations (Fig. 15.2). This significant blue shift, indicative of methemoglobin formation (heme-Fe+3), is associated with an increase in the extent of heme exposure during subunit dissociation and unfolding within these natural acellular hemoglobins (Harrington et al. 2010). Methemoglobin formation leads to a decrease in oxygen-carrying capacity.
Fig. 15.2 
Changes in wavelength maximum within the Soret region (450−350 nm) for acellular hemoglobins in the presence of increasing concentrations of urea at T = 37° C (Harrington et al. 2010)
Acellular hemoglobins exhibit varying amount of methemoglobin formation via autoxidation with the potential for hemichrome formation and eventual release of the heme–iron which has been associated with cellular and tissue oxidative damage. Interestingly, a study by Jia and Alayash (Jia and Alayash 2009) clearly demonstrated that the zero-linked (OxyVita Hb) polymer gave no additional evidence of heme–iron loss compared to the initial bovine tetramers from which OxyVita Hb is produced. They suggested that its heme stability is related to a well-defined compact conformational structure of this large polymer. This is consistent with the observed resistance to the isothermal urea unfolding studies carried out as describe above which demonstrated the inherent structural stability of OxyVita Hb as well as its reduced tendency to undergo oxidation in the presence of the denaturing pertubant (Harington et al. 2010)).
A related observation on the redox behavior of OxyVita Hb is its ability to be reduced back to the oxyhemoglobin state, albeit slowly, in the presence of ascorbic acid, a known reducing agent often found in the human plasma. This reaction has the potential to offer protection to the OxyVita Hb within the circulatory system without the benefit of the normal protective reducing enzymes that function within the red blood cell. Keeping the acellular OxyVita Hb in the reduced state will improve its functionality as an oxygen binding/release protein. Studies associated with the molecular events that may provide protection via other endogenous reducing agents for this acellular polymeric hemoglobin are on-going.
-
(c)
OxyVita Hb’s molecular size: Impact on other physiological functions: Table 15.1 presents the basic physicochemical properties of OxyVita Hb as determined by a wide range of biophysical and biochemical methods. We have successfully modified this polymeric hemoglobin (originally referred to a ZL-HbBv) through selected chemical steps to produce the “super-polymer” now referred to as OxyVita Hb possessing an average molecular weight of 17 MDa and a hydrodymanic radius of 360 Å. The relative hydrodynamic viscosity for a 6 g % solution of OxyVita Hb is similar to plasma (1.2−1.5 cP) and exhibits a colloidal osmotic pressure of 3 mm Hg (in lactated-Ringer’s, pH 7.4, 23° C) approximately 1/10th that of plasma. It exhibits a P50 = 5−6 mm Hg with an n value (Hill Coefficient) ~1. Less than 5 % methemoglobin is present in the final product.
Table 15.1 Physicochemical properties: OxyVita Hb (6 g %) Further studies using of a wide range of physical and chemical methods over the last several years have clearly shown that the polymeric hemoglobin constituting the OxyVita Hb solution, the OxyVita Hb powder form and the small volume resuscitation fluid (SVRF) are equivalent in all their properties as evident in Table 15.2.
Table 15.2 Physicochemical properties of OxyVita Hb liquid and powder preparations -
(d)
Impact of molecular design properties on pre-clinical studies: The unique chemistry associated with the chemical methods of synthesis of OxyVita Hb and the resultant molecular size and properties of this large polymeric hemoglobin described above have had a profound impact in addressing many fundamental issues within the field of HBOC development. The availability of OxyVita Hb has allowed many independent investigations to address and in several cases help to resolve these issues, which were identified by previous HBOC pre-clinical and clinical studies (Matheson et al. 2002; Rebel et al. 2003; Mito et al. 2009; Reynolds et al. 2007; Jahr et al. 2008). Concerns identified include but are not limited to: (1) loss of retention within the circulatory system; (2) extravasation and its impact on vasoconstriction coupled with increases in mean arterial pressure (MAP) upon HBOC infusion; (3) effect of HBOCs on the cerebral microcirculation and blood flow; (4) treatment of trauma and resuscitation responses; and (5) possible alterations of coagulation behavior. During the last several years (Harrington and Wollocko 2010), each of these concerns has been investigated using OxyVita Hb or the earlier form of this HBOC (ZL-HbBv). These studies, along with the development of several other chemically modified HBOCs, have dramatically improved our understanding of many of the issues involved.


Retention, extravasation, vasocontriction concerns: Early on the question of loss of retention within the circulatory system associated with leakage of tetrameric or cross-linked tetrameric HBOCs was associated with stress on the glomerulus and kidneys. Recently the nature of acellular HBOC extravasation and its impact on vasoconstriction and observed increase in mean arterial blood pressure (MAP) have been linked to complex interactions with nitric oxide (NO). An improved understanding of these critical interactions has lead to a better appreciation of the role of molecular size and its impact on the binding of NO and the concomitant physiological changes (vasoconstriction) associated with any NO binding. The fact that increased molecular size can reduce the extent of acellular extravasation due to the molecules’ inability to cross-over arterial or veinous membranes which exhibit various pore sizes (Matheson et al. 2000; Rippe and Haraldsson 1994) and bind with NO can lead to a reduction in vasoconstriction and help avoid BP elevation. In the case of OxyVita Hb, the larger radius of this molecule allows for greater retention time in the circulatory system with a half-life of 8−12 times longer that smaller radius HBOCs. All earlier animal studies carried out with OxyVita Hb have resulted in no observable vascular extravasation as determined by its absence in the renal hylar lymph after exchange transfusion experiments (Matheson et al. 2002). Furthermore, the recent work of Pittman and co-workers using a top-load rat model clearly showed that no vasoconstriction occurred in rat spinoitrapezius muscle using either form of OxyVita Hb (oxy or CO) and maintained tissue oxygenation (Song et al. 2012).
Cerebral microcirculation and blood flow behavior: The complex nature of the cerebral blood flow has been demonstrated by many investigations over the past decade (Scandinavian Stoke Study Group 1988; The Hemodilution in Stroke Study Group 1989). This complexity is even more apparent when attempts are made to understand and evaluate the role and effectiveness of HBOCs at delivering oxygen and reducing infarct volume during cerebral ischemia. In an detailed study using a mouse model, wherein the transfusion of large polymers of hemoglobin with a wide range on molecular sizes (ZLHb-Bv preparation) was carried out, it was determined that reduction (by 39 %) of the infarct volume was dependent on the concentration (6 g %) of this high-affinity hemoglobin (P50 = 4 mm Hg) and on the range of intermediate size hemoglobin polymers (500−14,000 kDa) transfused (Mito et al. 2009). Little or no reduction in the infract volume was observed under the following conditions: (1) transfusion in 5 % albumin solution; (2) a lower concentration (2−3 g %) of hemoglobin polymers of similar size; (3) hemoglobin polymers without removal of polymers <500 or >14,000 kDa; or (4) cross-linked hemoglobin tetramers with normal oxygen affinity (Mito et al. 2009).
The effective polymeric hemoglobin transfusion solution did not improve the distribution of cerebral blood flow during an ischemic event, nor did it alter blood flow to the brain or other major organs in the mouse model without ischemia. This latter finding also shows that these hemoglobin polymers do not initiate significant vasoconstriction in the brain or in peripheral vascular beds (Mito et al. 2009). Thus, in evaluating the potential of HBOCs for overcoming cerebral ischemia, a number of critical factors including, hemoglobin molecular size, concentration, and oxygen affinity, must be considered. Other HBOCs currently being evaluated may have the potential to address and further improve our understanding of the complex cerebral ischemia transfusion processes and protect the brain from ischemic strokes (Klaus et al. 2010).
Trauma treatment and resuscitation response: For the past several years, the assumption has been that early and rapid fluid resuscitation will restore blood pressure, reduce severe shock, and prevent multiple organ failure for treating uncontrolled hemorrhage. Recently, this approach has been challenged on the basis of new data indicating that aggressive attempts to normalize blood pressure with large fluid boluses produced increased bleeding, hemodynamic decompensation, and mortality (Dubick and Atkins 2003; Stern 2001). A newer procedure for permissive hypotensive resuscitation employing smaller volumes of hypertonic fluids is now favored small volume resuscitation fluid (SVRF). This approach has several advantages: (a) restoration of tissue perfusion accompanied by a modest increase in blood pressure with concomitant lowering of clotting factor dilution and re-bleeding; and (b) alleviation or reversal of lung damage. Within this approach, adequate blood pressure restoration needs to be sufficient without leading to re-bleeding, at the same time enabling adequate oxygen delivery to afford organ perfusion, thus reducing the possibility of multiple organ failure when full resuscitation is achieved.
This approach was recently tested in a Defense advanced research projects agency (DARPA) Reynolds et al. (2007). The specific objective was to determine a resuscitation strategy after 60 % hemorrhage in conscious male long-evans rats, which would lead to improved survival for 3 h in the absence of conventional large-volume crystalloid support. An additional component that was incorporated into this study was the use of OxyVita Hb in conjunction with a hypertonic saline solution and Hextend to enhance survival compared with standard small-volume resuscitation using Hextend only. The direct outcomes for this study included survival up to 3 h and maintenance of a MAP greater than 60 mmHg without additional fluid infusion (Sondeen et al. 2003). Test fluids administered included OxyVita Hb in a pressure-titrated infusion, Hextend titration, OxyVita Hb infused in a bolus method, and a Hextend bolus infusion. Throughout the course of these in vivo experiements, contstant monitoring of cardiovascular data, arterial gases, acid–base data, metabolites, electrolytes, Hb levels, and oxygen saturation were carried out. These occurred: (1) at baseline conditions, (2) at each 20 % hemorrhage increment, and (3) over 1−3 h after the initial hemorrhage. The most important finding from these studies was that a small-volume resuscitation treatment with OxyVita Hb significantly improved survival to 3 h and enhanced adequate MAP support for the duration, independent of the method of administration. These results clearly support the idea that an OxyVita Hb-augmented hypertonic ‘‘cocktail’’ is an encouraging alternative to the standard method for improving the MAP support and survival (Reynolds et al. 2007).
Coagulation acitivity: Use of any HBOC as a transfusion medium whether in the context of an exchange fluid or a replacement fluid must not interfere with the coagulation processes normally found in whole blood. In several earlier studies it was reported that hetastarch solutions resulted in elevated coagulopathy. This effect appeared to be linked to an increase molecular weight via several different mechanisms (DeJonge and Levi 2001; Strauss et al. 2002; Huraux et al. 2001). Given these findings, the risk of coagulopathy in the application and use of high-molecular-weight HBOCs was investigated (Jahr et al. 2008). Using hemodilution during clinical resuscitation after hemorrhagic shock with different amounts of OxyVita Hb (6 g %), hetastarch, and oxyglobin (HBOC-200), coagulopathy behavior in 1:11 to 1:1 dilutions in whole blood was evaluated by a thromboelastographic (TEG) technique in real time. This method allows for direct analysis of clot strength and formation kinetics, and an indirect determination of platelet and coagulation factor functionality and availability (Royston and Von Kier 2001). These ex vivo TEG determinations used blood from healthy donors, eliminating interfering factors such as anticoagulants and other intravenous fluids. This enabled direct evaluation of the effect of the HBOC on the TEG results. Findings from this study (Jahr et al. 2008) indicated that both HBOCs had a hypocoagulative effect on coagulation, and that this was more pronounced than that of 6 % hetastarch at the highest levels of hemodilution. However, minimal coagulopathic effects are expected with the use of OxyVita Hb at the manufacturer’s expected maximum dose of 10 g or 2−3 ml/kg. Thus, some caution should be used when attempting to use OxyVita Hb as a large-volume oxygen plasma expander. Its application is not expected to lead to an increased risk of clinical bleeding when used in relatively small volumes (2−3 ml/kg).
An important related finding regarding the effect of an HBOC on coagulation is the presence of methemoglobin (Moallempour et al. 2009). A dose response study with HBOC-200 (Oxyglobin) was carried out using the thromboelastogram technique. The results from this investigation revealed that high concentrations of methemoglobin in HBOC-200 led to increased coagulation impairment. This negative effect may be because of the effects on platelet function and on other coagulatory proteins of concomitant oxidative species associated with increased methemoglobin levels. Platelets contain functionally important glycoprotein receptors containing thiol groups providing increased sites of interaction for these redox-sensitive structures (Essex and Li 2006). A significant characteristic of OxyVita Hb is the low methemoglobin levels associated with its preparation and its extraordinary resistance to molecular unfolding, which significantly reduces its conversion to methemoglobin in vitro and in vivo (Harrington et al. 2010; Harrington et al. 2011).
3 Summary
The focus of this chapter has been to address the reasons why OxyVita Hb, a new therapeutic oxygen carrier, is fundamentally different from previous generations of HBOCs. As our understanding of the relationship between the structural and functional behavior of the earlier HBOCs evolved, it became apparent that some of the structural characteristics incorporated into the modified HBOCs still resulted in problems of extravasation and vasoconstriction, oxidative degradation, and safety concerns when these HBOCs were evaluated within many pre-clinical and clinical studies. OxyVita Hb was designed to address these concerns. The fundamental aspects of OxyVita Hb’s development and success to date within pre-clinical studies are based upon its unique chemical technology and the recognition that molecular size, hydrodynamic properties, negative surface charge (Harrington et al. 2011) and discrete functional properties all play important physiological roles as an HBOC. As described above, OxyVita Hb is differentiated from all other HBOCs presently being investigated due to: (1) its chemistry: a unique zero-linked polymerization method of synthesis; (2) well characterized physicochemical characteristics associated with its molecular properties and functional behavior; and (3) its potential for long-term storage (Table 15.1), due to these unique physiochemical properties, including extraordinary molecular stability, over a wide range of climatic conditions.
References
Alayash AI (2004) Oxygen therapeutics: can we tame hemoglobin? Nature Rev Drug Discov 3:152–159
Alayash AI, D’Agnillo F, Buehler PW (2007) First-generation blood substitutes: what have we learned? Biochemical and physiological perspectives. Expert Opin Biol Ther 7:665–675
Bucci E, Kwansa H, Koehler RC, Matheson B (2007) Development of zero-linked polymers of hemoglobin, Which do not extravasate and do not induce pressure increases upon infusion. Artif Cells Blood Substit Immobil Biotechnol 35:11–18
Buehler PW, Alayash AI (2008) All hemoglobin-based oxygen carriers are not created equal. Biochim Biophys Acta 1784:1378–11381
DeJonge E, Levi M (2001) Effects of different plasma substitutes on blood coagulation: a comparative review. Crit Care Med 29:1261–1267
Dubick MA, Atkins JL (2003) Small-volume fluid resuscitation for the far-forward combat environment: current concepts. J Trauma Inj Infect Crit Care 54:S43–S45
Essex DW, Li M (2006) Redox modification of platelet glycoproteins. Curr Drug Targets 7:1233–1241
Estep T, Bucci E, Farmer M, Greenberg G, Harrington JP, Kim HW, Klein H, Mitchell P, Nemo G, Olsen K, Palmer A, Valeri R, Winslow R (2008) Basic science focus on blood substitutes: summary of the NHLBI division of blood diseases and resources working group workshop. Transfusion 48:776–782
Grabarek Z, Gergely J (1990) Zero-length crosslinking procedure with the use of active esters. Anal Biochem 185:131–135
Harington JP, Orlig K, Zito SL, Wollocko J, Wollocko H (2010) Structural and redox behavior of OxyVita Hb, a zero-linked polymeric hemoglobin: comparison with natural acellular polymeric hemoglobins. Artif Cells Blood Substit Biotechnol 38:64–68
Harrington JP, Wollocko H (2010) Pre-clinical studies using OxyVita hemoglobin, a zero-linked polymeric hemoglobin: a review. J Artif Organs 13:183–188
Harrington JP, Kobayashi S, Dorman SC, Zito SL, Hirsch RE (2007) Acellular invertebrate hemoglobins as model therapeutic oxygen carriers: unique redox potentials. Artif Cells Blood Substit Biotechnol 35:53–67
Harrington JP, Wollocko J, Kostecki E, Wollocko H (2011) Physicochemical characteristics of OxyVita hemoglobin, a zero-linked polymer: liquid and powder preparations. Artif Cells Blood Substit Biotechnol 39:12–18
Hirsch RE, Harrington JP (2000) Blood substitutes: an overview and perspective. Einstein Q J Biol Med 17:113–123
Huraux C, Ankri A, Eyraud D et al (2001) Hemostatic changes in patients receiving hydroxyethyl starch: the influence of ABO blood group. Anesth Analg 92:1396–1401
Jahr JS, Akha AS, Holtby RJ (2012) Crosslinked, polymerized, and PEG-conjugated hemoglobin-based oxygen carriers: clinical safety and efficacy of recent and current products. Current Drug Discov Technol 9:158−165
Jahr JS, Weeks DL, Desai P, Lim JC, Butch W, Gunther R, Driessen B (2008) Does OxyVita, a new-generation hemoglobin-based oxygen carrier, or oxyglobin acutely interfere with coagulation compared with normal saline or 6 % hetastarch? A ex vivo thromboelastography study. J Cardiothorac Vasc Anesthesiol 22:34–39
Jia Y, Alayash AI (2009) Effects of cross-linking and zero-link polymerization on oxygen transport and redox chemistry of bovine hemoglobin. Biochim Biophys Acta 1794:1234–1242
Klaus JA, Kibler KK, Abuchhowski A, Koehler RC (2010) Early treatment of transient focal cerebral ischemia with bovine PEGylated carboxy hemoglobin transfusion. Artif Cells Blood Substit Biotechnol 38:223–229
Matheson B, Razynska A, Kwansa H, Bucci E (2000) Appearance of dissociable and crosslinked hemoglobins in renal hylar lymph. J Lab Clin Med 135:459–464
Matheson B, Kwansa HE, Bucci E, Rebel A, Koehler RC (2002) Vascular response to infusions of a non-extravasating hemoglobin polymer. J Appl Physiol 93:1479–1486
Mito T, Nemoto M, Kwansa H, Sampei K, Habeeh M, Murphy SJ, Bucci E, Koehler RC (2009) Decreased damage from transient focal cerebral ischemia by transfusion of zero-linked hemoglobin polymers in mouse. Stroke 40:278–284
Moallempour M, Jahr JS, Lim JC, Weeks D, Butch A, Driessen B (2009) Methemoglobin effects on coagulation: a dose-response study with HBOC-2000 (Oxyglobin) in a thrombelastogram model. J Cardiothorac Vasc Anesth 23:41–47
Olsen JS, Foley EW, Rogge C, Tsai AI, Doyle MP, Lemon DD (2004) NO scavenging and the hypertensive effect of hemoglobin-based oxygen carriers. Free Radical Biol Med 36:685–697
Razynska A, Bucci E (1998) Zero-link polymerization: a new class of polymeric hemoglobins blood substitutes present and future perspectives. Elsevier New York pp 265−279
Rebel A, Ulatowski JA, Kwansa H, Bucci E, Koehler RC (2003) Cerebrovascular response to decreased hematocrit: effect of cell free hemoglobin, plasma viscosity, and CO2. Am J Physiol Heart Circ Physiol 285:1600–1608
Reynolds PS, Barbee RW, Skaflen MD, Ward KR (2007) Low-volume resuscitation cocktail extends survival after severe hemorrhagic shock. Shock 28:45–52
Rippe B, Haraldsson B (1994) Transport of macromolecules across microvascular walls: the two pore theory. Physiol Rev 74:163–219
Royer WJ, Sharma H, Strand K, Knapp J (2006) Lumbricus erythrocruorin at 3.5 A resolution: architecture of a megadalton respiratory complex. Structure 14:1167–1177
Royer WJ, Omartian M, Knapp J (2007) Low resolution crystal structure of arenicola erythrocruorin: influence of coiled coils on the architecture of a megadalton respiratory protein. J Mol Biol 365:226–236
Royston D, Von Kier S (2001) Reduced haemostatic factor transfusion using heparinase-modified thromboelastography during cardiopuliminary bypass. Br J Anaesth 86:575–578
Scandinavian Stoke Study Group (1988) Multicenter trial of hemodilution in acute ischemic stroke. Stroke 19:464–471
Silverman TA, Weiskopf RB (2009) Hemoglobin-based oxygen carriers: current status and future directions. Transfusion 49:2495–2515
Sondeen JL, Coppes VG, Holcomb JB (2003) Blood pressure at which rebleedding ocurrs after resuscitation in swine with aortic injury. J Trauma Inj Inf Crit Care 54:S110−S117
Song B, Nugent W, Moon-Massat P, Auker C, McCarron R, Pittman R (2013) Effect of Top-loading a zero-link bovine hemoglobin, OxyVita Hb, on systemic and microcirculatory variables. Mil. Med 178:570–577
Staros JV, Wright RW (1986) Enhancement by N-hydroxysulfosuccinimide of water-soluble carbodiimide-mediated coupling reactions. Anal Biochem 156:220–222
Stern SA (2001) Low-volume fluid resuscitation for presumed hemorrhagic shock: helpful or harmful? Curr Opin Crit Care 7:422–430
Stowell CP, Levin J, Speiss BD (2001) Progress in the development of RBC substitutes. Transfusion 41:287–299
Strauss RG, Pennell BJ, Stump DC (2002) A randomized, blinded trial comparing the hemostatic effects of pentastarch versus hetastarch. Transfusion 42:27–36
The Hemodilution in Stroke Study Group (1989) Hypervolemic hemodilution treatment of acute stroke. Results of a randomized multicenter trial using pentastarch. Stroke 20:317–323
Vandegriff K, Malavalli A, Wooldridge J, Lohman J, Winslow R (2003) MP4, a new nonvasoactive PEG-Hb conjugate. Transfusion 43:509–516
Winslow RM (2007) Red Cell Substitutes. Semin Hematol 44:51–59
Winslow RM (2008) Cell-free oxygen carriers: scientific foundations, clinical development, and new directions. Biochim Biophys Acta 1784:1382–1386
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2013 Springer-Verlag Berlin Heidelberg
About this chapter
Cite this chapter
Harrington, J.P., Wollocko, H. (2013). Zero-Link Hemoglobin (OxyVita®): Impact of Molecular Design Characteristics on Pre-clinical Studies. In: Kim, H., Greenburg, A. (eds) Hemoglobin-Based Oxygen Carriers as Red Cell Substitutes and Oxygen Therapeutics. Springer, Berlin, Heidelberg. https://doi.org/10.1007/978-3-642-40717-8_15
Download citation
DOI: https://doi.org/10.1007/978-3-642-40717-8_15
Published:
Publisher Name: Springer, Berlin, Heidelberg
Print ISBN: 978-3-642-40716-1
Online ISBN: 978-3-642-40717-8
eBook Packages: Chemistry and Materials ScienceChemistry and Material Science (R0)