
Abstract
Dissociative identity disorder (DID) is a disputed psychiatric disorder. Research findings and clinical observations suggest that DID involves an authentic mental disorder related to factors such as traumatisation and disrupted attachment. A competing view indicates that DID is due to fantasy proneness, suggestibility, suggestion and role-playing. Here, we investigate whether dissociative identity state-dependent psychobiological features in DID can be induced in high- or low-fantasy-prone individuals by instructed and motivated role-playing and suggestion. Differences in neural activation patterns were found between the DID patients and both high- and low-fantasy-prone controls. That is, the identity states in DID were not convincingly enacted by DID simulating controls. The findings indicate that DID does not have a sociocultural (e.g. iatrogenic) origin.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
- Dorsal Striatum
- Traumatic Memory
- Brodmann Area
- Multiple Comparison Correction
- Global Cerebral Blood Flow
These keywords were added by machine and not by the authors. This process is experimental and the keywords may be updated as the learning algorithm improves.
1 Introduction
Despite its inclusion in the Diagnostic Manual of Mental Disorders (American Psychiatric Association 2000), the genuineness of dissociative identity disorder (DID) continues to be disputed. Supporters of the diametrically opposed trauma-related and non-trauma-related views have been engaged for decades in a passionate debate regarding its validity as a mental disorder and whether it is related to traumatisation or to fantasy proneness, suggestibility, suggestion, and simulation (Bremner 2010; Coons 2005; Fraser 2005; Giesbrecht et al. 2008, 2010; Piper and Merskey 2004a, b, 2005; Sar 2005).
The non-trauma-related position (Giesbrecht et al. 2008; Merckelbach and Muris 2001; Merckelbach et al. 2002; Piper and Merskey 2004a, b; Pope et al. 2006), also referred to as the sociocognitive model of DID (Lilienfeld et al. 1999; Spanos 1994, 1996), holds that DID is a simulation caused by high suggestibility and/or fantasy proneness (Giesbrecht and Merckelbach 2006; Giesbrecht et al. 2007; Merckelbach et al. 2000, 2001; Rassin et al. 2001), suggestive psychotherapy, and other suggestive sociocultural influences (e.g. the media and/or the church). According to this model, ‘[t]he rules for enacting the [DID] role […] are as follows: (a) Behave as if you are two (or more) separate people who inhabit the same body. (b) Act as if the you I have been addressing thus far is one of those people and as if the you I have been talking to is unaware of the other co-inhabitants. (c) When I provide a signal for contacting another co-inhabitant, act as though you are another person. To the extent that patients behave in terms of these rules, the “classic” symptoms [of DID] follow by implication and do not have to be taught through direct instruction or further suggestion’ Spanos (p.239, (Spanos 1996)). Although fantasy proneness and suggestibility refer to different concepts, they are highly correlated (Braffman and Kirsch 1999; Levin and Spei 2004; Merckelbach et al. 2001; Poulsen and Matthews 2003; Silva and Kirsch 1992), and dissociative symptoms were found to be correlated with fantasy proneness, heightened suggestibility, and susceptibility to pseudomemories (Merckelbach and Muris 2001; Rauschenberger and Lynn 1995). Of note, people who argue against the DID trauma perspective do not solely talk about fantasy proneness but also suggest the possibility of mild cognitive impairment as an alternative explanation (Giesbrecht et al. 2008).
To date, the position that DID is caused by sociocultural factors such as fantasy proneness has not been tested in brain imaging studies involving DID patients, and evidence that the complex phenomenology and psychobiology of DID can be created and sustained over time by these factors is lacking (Brown et al. 1999; Gleaves 1996; Loewenstein 2007; Xiao et al. 2006). Despite this lack of empirical support, the sociocognitive and fantasy-based model of DID is influential in contemporary psychiatry, and there have been proposals to prevent the inclusion of DID in the DSM-V (Gharaibeh and Merskey 2009).
The trauma-related perspective entails that DID is related to a combination of factors that include chronic emotional neglect as well as emotional, physical, and/or sexual abuse from early childhood, insufficient integrative capacity, attachment disorder, and lack of affect regulation by caretakers(Dell and O’Neil 2009; Gleaves 1996; van der Hart et al. 2006; Putnam 1992; Spiegel 2006). In this view DID is thought to be at the far end of the spectrum of trauma-related psychiatric disorders, i.e. being a severe form of post-traumatic stress disorder (PTSD) (van der Hart et al. 2006; Spiegel 1984).
Holders of the trauma-related view acknowledge that some features of dissociative identity states can be influenced by sociocultural factors (van der Hart et al. 2006), that false-positive cases of DID have evolved in a treatment setting and that some psychiatric patients imitate DID (Draijer and Boon 1999). However, they also note that there are differences between authentic and imitated DID and that there is no evidence that DID can (sub-)consciously be created by sociocultural factors (Gleaves 1996). Furthermore, even if DID symptoms can be created iatrogenically or can be enacted, this does not mean that genuine trauma-related DID does not exist (Elzinga et al. 1998).
According to the DSM-IV (American Psychiatric Association, APA, DSM-IV 2000), DID is characterised by, among others, the presence of two or more distinct ‘identities’ or ‘personality states’. Different proposed labels include ‘different emotional states’, ‘alters’, ‘dissociative parts of the personality’ (van der Hart et al. 2006) and ‘dissociative identity states’. Following previously used descriptions and terminology (Reinders et al. 2003, 2006), different types of dissociative identity states are indicated here as the neutral identity state (NIS) and trauma-related identity state (TIS). These indicators are derived from the terms ‘apparently normal part of the personality (ANP)’ and ‘emotional part of the personality (EP)’, respectively, which are used in the theory of structural dissociation (van der Hart et al. 2006; Nijenhuis et al. 2002). This theory defines dissociation as a division of personality into different types of subsystems, each with their own first-person perspective, that is, their own point of view as to who they are, what the world is like, and how they relate to that world (Nijenhuis and Van der Hart 2011). As NIS, DID patients concentrate on functioning in daily life, commonly try to hide their pathology, and have not sufficiently integrated (e.g. have partial or complete amnesia to) traumatic memories. That is, NIS fails to relate the trauma-related nature to its self (Reinders et al. 2003). In contrast, TIS does have conscious access to these memories, recalls them as personal experiences and is bodily and emotionally affected by them. That is, as TIS, the patients are fixated in traumatic memories and engage in defensive actions such as freeze and flight, when they are or feel threatened (Nijenhuis et al. 2002, 2004), thereby activating fast subcortical response routes in the brain (LeDoux 2000; Reinders et al. 2006). Patients, as TIS, either can engage in active kinds of physical defence (e.g. freeze, flight, fight), indicating a dominance of the sympathetic nervous system, or can engage in total submission (i.e. playing dead) which would be primarily mediated by the dorsal vagal branch of the parasympathetic nervous system (Nijenhuis and Den Boer 2009).
1.1 Brain Imaging Studies in DID
Despite the fact that imaging neuroscience has been around for more than 20 years and is by now the predominant technique in behaviour and cognitive neuroscience (Friston 2009), only very few studies have been performed in patients with DID (Dalenberg et al. 2012; Reinders 2008). The first functional brain scan in one patient with DID was a PET scan of the brain resting state (Mathew et al. 1985). This study included three control subjects and revealed blood flow differences in the temporal cortex of the DID patient. Four more studies assessing the resting state of the DID brain have been reported, all four using the low spatial resolution imaging technique of single-photon emission computed tomography (SPECT). Two of these studies were case studies (Saxe et al. 1992; Sheehan et al. 2006) with no control groups. The remaining two SPECT studies were performed by the same research group and include the largest group of 21 DID patients (plus nine healthy controls) ever assessed using brain imaging techniques (Sar et al. 2001, 2007). These two latter studies consistently found bilateral frontal perfusion differences between patients and controls. Enhanced prefrontal cortex functioning was also found during a working-memory task (Elzinga et al. 2007) when comparing 16 DID patients to healthy controls, using functional magnetic resonance imaging (fMRI), a high temporal and spatial resolution imaging technique. Elzinga et al. found that dissociative patients recruited the left anterior prefrontal cortex (BA 10), the left dorsolateral prefrontal cortex (BA 9) and the left parietal cortex (BA 40) more than controls. The prefrontal areas were found to be activated independent of task difficulty, while the parietal cortex activation was task-load dependent.
Two other studies used fMRI but only involved case studies of a DID patient switching between different identity states (Savoy et al. 2012; Tsai et al. 1999). Interestingly, Savoy et al. found the dorsolateral prefrontal cortex (BA9), the anterior prefrontal cortex (BA10) as well as the orbitofrontal cortex (BA 11) to be involved in voluntary switching between identity states. In addition, bilateral activation was found in an area in the striatum, the nucleus accumbens. The study of Tsai et al. did not report the involvement of the prefrontal cortical areas but did report the hippocampal areas to be involved in switching between identity states as well as the parahippocampus, medial temporal structures, substantia nigra, and the global pallidus. The latter structure is part of the dorsal striatum.
The literature review above shows that functional alterations have been reported widespread throughout the brain, i.e. in the temporal (Mathew et al. 1985; Sar et al. 2001; Saxe et al. 1992; Sheehan et al. 2006; Tsai et al. 1999), frontal (Elzinga et al. 2007; Sar et al. 2001, 2007; Savoy et al. 2012), and occipital (Sar et al. 2007) cortices and the nucleus accumbens (Savoy et al. 2012) and the hippocampal and pallidum structures (Tsai et al. 1999). In a multi-subject PET study, Reinders et al. (2006) reported that different dissociative identity states (i.e. NIS and TIS) in DID are associated with different brain activation patterns when confronted with trauma-related cues. They reported the involvement of mainly the cortical multimodal posterior association areas (PAA), the subcortical amygdala, and subparts of the dorsal striatum (i.e. the caudate and putamen) in the psychopathology of DID.
1.2 DID and Fantasy Proneness
Proponents of the sociocognitive view have argued that the different patterns of subjective, psychophysiological, and neural activity for NIS and TIS in response to a trauma-memory script that Reinders et al. (2003, 2006) documented might be due to fantasy proneness, suggestion, and role-playing and that they do not prove a traumagenic origin of DID. Obtaining independent proof of childhood traumatisation in adulthood is most difficult. However, the claim that the previously reported PET results constitute effects of fantasy proneness, suggestion, and role-playing is open to test. Here, we describe a neuroimaging study that involves a psychobiological comparison between NIS and TIS engaging in active kinds of physical defence in DID patients (i.e. the DID identity states from Reinders et al. (2003, 2006)) and simulated NIS and TIS in high- and low-fantasy-prone, mentally healthy women. The women in this control group did not report a trauma history and were instructed and motivated to role-play these different identity states (i.e. simulated identity states).
The a priori hypotheses of the current study are as follows: (i) important previously found neurobiological differences between NIS and TIS in DID patients (Reinders et al. 2003, 2006) are upheld when correcting for the response in the control group, (ii) the upheld neurobiological differences for NIS and TIS in DID patients include higher subcortical activity (e.g. the amygdala and caudate nucleus) for TIS in DID, and (iii) the cortical multimodal posterior association areas (e.g. the intraparietal sulcus and (pre-)cuneus) for NIS in DID patients are hyperactivated when listening to personal trauma scripts.
2 Methods
2.1 Participants
Twenty-nine subjects participated in the PET study: 11 patients with dissociative identity disorder (DID), 10 high-fantasy-prone DID simulating controls (CH), and 8 low-fantasy-prone DID simulating controls (CL). Controls were carefully matched for gender (all female) and age and differences in age were not significant (DID vs. CH: F(1,18) = 0,499 p = 0.489, n.s. and DID vs. CL: F(1,16) = 0.153; p = 0.701, n.s.). The study presented in this chapter has been published elsewhere (Reinders et al. 2012) and a detailed description of the controls and the DID enactment procedure can be found in that paper (Reinders et al. 2012). In sum, the controls were recruited by local newspaper advertisements, did not suffer from potentially traumatising events such as physical abuse and emotional neglect and filled in the Creative Experiences Questionnaire (CEQ) (Merckelbach et al. 2001) which measures fantasy proneness. The controls were divided into two groups based on their CEQ scores resulting in a high-fantasy-prone group (n = 10, age 38.2 (SD 10.9), Traumatic Experience Checklist (TEC; Nijenhuis et al. 2002) 0.7 (SD 1.3), Somatoform Dissociation Questionnaire (SDQ-20; Nijenhuis et al. 1996) 22 (SD 2.4)) with CEQ 13.7 (SD 3.2) and a low-fantasy-prone group (n = 8, age 42.5 (SD 10.1), TEC 0.4 (SD 0.5), SDQ-20 20.9 (SD 1.5)) with CEQ 3.9 (SD 1.6). A CEQ cut-off for high fantasy proneness of ten was used, which the developers of the CEQ recommended for the current sample (Giesbrecht T and Merckelbach H, personal written email communication on the 11th of February, 2008). The controls received written and oral information on dissociative identity states and were instructed to enact the two DID identity states: a neutral identity state (NIS) and a trauma-related identity state (TIS). Controls were asked to provide their most painful memory to serve as an analogue for the patients’ personal trauma memories, as well as a neutral personal episodic memory. Controls were subsequently instructed how to write the autobiographical analogue neutral and ‘trauma’ memory scripts. For the experiment they had to train themselves in being in a neutral state, the NIS who is unresponsive or under-responsive to the painful experience, and in being in a state in which they re-experience the painful memory, the TIS.
A detailed description of the DID patients can be found elsewhere (Reinders et al. 2003, 2006). In short, 11 patients (all female, age 41.0, SD 6.1) participated: (i) whose treatment had progressed to include therapeutic exposure to trauma-related memories; (ii) who met the criteria for DID, as operationalised in the Structured Clinical Interview for DSM-IV Dissociative Disorders (SCID-D(Steinberg 1994)); (iii) who had at least one TIS and one NIS that they could activate on demand; and (iv) with whom the involved TIS had displayed signs of sympathetic nervous system dominance under perceived threat in clinical situations.
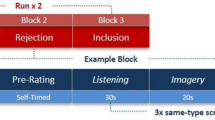
Cerebral blood flow PET (Siemens/CTI ECAT HR+) data and autonomic (systolic and diastolic blood pressure, discrete heart rate and heart rate variability (HRV)) and subjective (controls’ subjective sensorimotor and emotional experiences) reactions were obtained (see for details: (Reinders et al. 2003, 2006, 2012)). DID patients as well as high-fantasy-prone and low-fantasy-prone controls were studied in the two different types of identity states during a memory script (MS)-driven (neutral or trauma-related autobiographical texts) imagery paradigm. Four conditions were obtained twice in patients and three times in controls: NISn, NISt, TISn, TISt, where the last minor character (n or t) denotes the content of the memory script (MS: neutral or trauma related).
2.2 Image Acquisition and Data Processing
Data acquisition, reconstruction, attenuation correction, spatial transformation, spatial smoothing (isotropic Gaussian kernel of 12 mm) and global normalisation were performed as usual (Reinders et al. 2012). The brain imaging data of the three groups was preprocessed and statistically analysed in SPM5 (www.fil.ion.ucl.ac.uk/spm) in a three-by-two-by-two factorial design (see Intermezzo 1 with Fig. 16.1), which allows for the assessment of within- and between-identity state effects within and between the three groups.

The study-specific general linear model as created in SPM
2.3 Statistical Inference and Reporting
Our a priori hypothesis was that earlier findings would still hold after the correction for non-trauma-related factors. Both whole-brain and a priori region of interest (ROI) multiple comparisons correction were performed on the basis of false discovery rate statistics (Genovese et al. 2002). If an a priori hypothesised brain area did not survive whole-brain multiple comparison correction, i.e. only survived an uncorrected threshold of p < 0.001, multiple comparison correction was performed within the a priori region of interest (ROI) (Reinders et al. 2012). Note: In line with previously used statistical thresholds (Reinders et al. 2006), voxels surviving significant levels only uncorrected for multiple testing for the whole brain, i.e. p < 0.001, were reported as well, but for comparison purposes only. Only clusters larger than eight voxels are reported taking into account the spatial resolution of the PET camera. In contrast to the earlier publication (Reinders et al. 2012), here, only the most significant peak voxels in a brain region is reported for simplicity. Brain regions and Brodmann areas (BA) were defined using both the Talairach atlas (Talairach and Tournoux 1988) and Deamon (Lancaster et al. 2000). Activations in sulci were defined using Brain Tutor (www.brainvoyager.com).
3 Results
3.1 Comparing Simulated and Pathological Identity States
The comparison of different conditions in different groups is not always straightforward to understand. It can also be described as a between-group comparison of within-group differences. For clarification this is depicted in Fig. 16.2. The easiest approach is to think of this by starting with the within-group comparisons which can be performed for each group separately, as shown at the top of Fig. 16.2. Figure 16.2 shows a simplified graphical representation of the statistical comparison process and uses the conditions ‘NIS’ and ‘TIS’ as example conditions. These conditions can be replaced by, for example, TISt and NISt to clarify the between-identity state comparisons or by TISt and TISn to understand the within-identity state comparisons. The top row of Fig. 16.2 shows the two conditions in two groups. The middle row shows the result of the simple subtraction analyses between the two conditions within each group. The middle row therefore represents the within-group brain activation maps of the difference between the two conditions. These two differential maps are now compared to each other to obtain the between-group differential brain activation map, which is depicted on the bottom row. It is important to realise that the statistical model must start with a within-group comparison. Thus it is not possible to obtain meaningful results when directly comparing a single condition between groups. For example, we cannot investigate the difference for the NISt condition between the DID and control subjects.

A between-group comparison of within-group differences. This figure depicts two conditions in two groups (DID and Controls) at the top row. The middle row shows the within-group differences of two conditions per group (DID or Controls). The bottom row depicts the between-group differential brain activation patterns. Note that SPM does not calculate each step separately; the figure is for clarification only
3.1.1 Within-Identity State Trauma-Related Memory Script Effects
Trauma-related MS effects within both TIS and NIS are given in Table 16.1. TIS showed significant regionally specific increases and decreases in cerebral blood flow, when processing the trauma-related MS as compared to the neutral MS, between the DID and both the high- and low-fantasy-prone control groups. These findings are depicted in Fig. 16.3.

‘Glass brain’ renderings showing differences in the processing of the trauma-related text (indicated with a small ‘t’) and the neutral text (indicated with a small ‘n’) within the trauma-related identity state (TIS). Differences in regional cerebral blood flow patterns for the dissociative identity disorder (DID) group (left) and the comparison of this group to the high- (middle) and low (right)-fantasy-prone DID simulating controls (CH and CL, respectively) are depicted. See Table 16.1 for the specific areas
3.1.2 Between-Identity State Trauma-Related Memory Script Effects
Trauma-related MS effects between NIS and TIS are given in Table 16.2. Different rCBF patterns were found for NIS and TIS, when processing the trauma-related MS, between the DID and both the high- and low-fantasy-prone control groups. These differential rCBF patterns are shown in Fig. 16.4.

‘Glass brain’ renderings showing differences in the processing of the trauma-related text (indicated with a small ‘t’) between the trauma-related identity state (TIS) and the neutral identity state (NIS). Differences in regional cerebral blood flow patterns for the dissociative identity disorder (DID) group (left) and the comparison of this group to the high- (middle) and low (right)-fantasy-prone DID simulating controls (CH and CL, respectively) are depicted. See Table 16.2 for the specific areas
4 Discussion
The present study was performed to examine whether earlier reported results (Reinders et al. 2003, 2006) for DID hold after correcting for potential iatrogenic effects. To this end, we tested whether these findings can be simulated by motivated role enactment and/or is facilitated by a high level of fantasy proneness (Merckelbach et al. 2001) by reinvestigating the patient population from Reinders et al. (2006). Neither high- nor low-fantasy-prone healthy controls, instructed and motivated to simulate two different types of dissociative identity states in DID (i.e. NIS and TIS), mimicked previously observed psychophysiological and neural reactions that are associated with these identity states in DID (Reinders et al. 2006), which is supportive of our first a priori hypothesis.
From results shown in Figs. 16.3 and 16.4, a first impression of the (dis)similarities between DID patients and controls can be obtained. Figures 16.3 and 16.4 show that most of the original DID rCBF patterns remain present when comparing them to the high- or low-fantasy-prone groups. This clearly demonstrates that neither high- nor low-fantasy-prone controls are able to reliably simulate the DID patients’ rCBF patterns. As patients and controls were scanned in a highly similar experimental setting and because controls were highly motivated to simulate DID, the found commonalities in brain activation between patients and controls were expected. Despite this overlap in brain activation between patients and controls, important previously found psychophysiological and neurobiological differences between NIS and TIS in DID patients were upheld when controlling for fantasy proneness, suggestion, and instructed and motivated role-playing, which is supportive of our first a priori hypothesis. It should be noted that, in addition to not having DID, the control group was non-traumatised as measured with the TEC. Therefore, it could be argued that both groups essentially did not complete the same task, i.e. one group was thinking about a traumatic event and one was thinking about a painful experience, and therefore it might be of less work for the controls than the experimental group. This also could lead to the argument that it is trauma itself that caused the results instead of dissociation, i.e. the results do not indicate compartmentalised autobiographical memory retrieval but instead differential emotional reactivity. However, as the sociocognitive model (Spanos 1994) assumes that DID can easily be simulated, we feel that the current study provides important information to the aetiology discussion concerning DID. Nevertheless, we do recommend that future research include a traumatised group without dissociation, for example, PTSD, and/or the inclusion of additional control condition for patients consisting of a non-autobiographical ‘trauma’ (i.e. negative event).
The activated areas seem to be subdivided in two distinct neural networks, where the NIS activates areas in the cerebral cortex, while the TIS mainly activates subcortical areas (e.g. see Table 16.2 and Fig. 16.4). The tables show a detailed listing of all the brain areas involved. Brain areas that disappear after comparison to a control group are brain areas non-specific to DID, i.e. these areas share commonalities between patients and controls. Other brain areas are specific to DID.
Our findings support the cortico-limbic inhibition model of trauma-related dissociative disorders (Lanius et al. 2010; Nijenhuis et al. 2002). Results of both the NISt-TISt comparison and the main effect of NIS show significant overlap with the activated network of brain regions during emotional memory suppression of unwanted memories in mentally healthy individuals (Anderson et al. 2004), for example, in frontal areas (BA 4/6/8/10/47), cingulate cortex (BA 32), and intraparietal sulcus (BA 7/40). Anderson et al. (2004) did not find all of these brain areas. There is significant overlap between our study and their study, but in our patient population more brain areas were involved in the modulation of access to trauma-related memory. This might be an indication that, when DID patients are functioning as NIS, different cortical processes are involved that modulate conscious and subconscious perception of trauma-related information. These areas, e.g. (pre-)cuneus (BA 7/39, 18/19), fusiform gyrus (BA 18/19/37), lingual gyrus (BA 18), occipital gyrus (BA 18/19/37), and the parahippocampal gyrus (BA 35/36), are located in the posterior association areas (PAA), and there are indications that these areas are involved in multimodal (Driver and Vuilleumier 2001) somatosensory integration (Lanius et al. 2004; Simeon et al. 2000) of information, especially in relation to attention and perceptual awareness. Hyperactivation of cortical multimodal association areas for NIS in DID when listening to personal trauma scripts constituted our third a priori hypothesis. We thus propose that for emotional memory suppression, or NIS’ mental avoidance (Nijenhuis et al. 2002), of unwanted memories in DID the PAA fulfils a pivotal role.
There are notable similarities in the patterns of brain activation for DID patients (see Table 16.1) and mentally healthy individuals unsuppressed memory retrieval (Anderson et al. 2004). Both groups have increased activation of the insula (BA 13) and parietal operculum (BA 40/43). We did not find the hippocampus to play a role in memory retrieval in DID patients, despite the fact that this area has been indicated in memory processing in mentally healthy individuals. Instead we found that the caudate nucleus was activated when DID patients listened to the trauma-memory scripts as TIS. Acute stress can be associated with a shift from hippocampal involvement to caudate nucleus involvement (Schwabe et al. 2008; White 2009). Thus, acute stress is linked with a caudate nucleus-dependent stimulus response at the expense of hippocampal-dependent spatial learning and memory. According to the theory of structural dissociation (van der Hart et al. 2006; Nijenhuis and Den Boer 2009), listening to a description of a personal traumatic memory in an experimental setting constitutes a consciously experienced acute stressor for TIS, because dissociative identity state DID patients do not manage to mentally avoid the relevant memory. An alternative explanation for increased caudate and amygdala activation in DID patients as compared to controls is based on the finding that the dorsal striatum (caudate, putamen, and pallidum) correlates negatively with trait dissociation during stress-induced analgesia (Mickleborough et al. 2011). Thus, we could speculate that the dorsal striatum is involved in dissociation (Mickleborough et al. 2011) and switching between identity states (Tsai et al. 1999) as well as maintaining identity states in DID (Reinders et al. 2006, 2012). In a single subject functional MRI study, Savoy et al. (2012) reported the involvement of the ventral striatum (i.e. the accumbens area) during identity state switching. Furthermore, findings of studies in patients with focal lesions in the dorsal striatum indicate the involvement of this structure in task switching and inhibition of irrelevant information (Yehene et al. 2005, 2008). Taking both the switching and memory hypotheses together, in DID the dorsal striatum is involved in the regulation of memory access by modulating the presence of neutral or trauma-related identity states. This finding is consistent with the TIS as the type of alternate identity that recognises, relates, and emotionally responds to the traumatic past as personal autobiographical information (van der Hart et al. 2006). We could speculate that the caudate plays an important role in DID patients’ ability to recognise trauma-related, emotional information as autobiographical. These findings for TIS are supportive of our second a priori hypothesis.
To date, experimental research of inter-identity amnesia in DID has produced mixed results. One study (Elzinga et al. 2003) demonstrated evidence for inter-identity amnesia, which is in line with the current findings. Other studies (Huntjens et al. 2003, 2005a, b, 2006, 2007) found inter-identity transfer of newly learned non-autobiographical stimuli, even though the ‘amnestic’ identity reported subjective amnesia for these stimuli. Several principles might explain the inconsistent findings: (i) Inter-identity amnesia may only exist for stimuli that have personal relevance for the ‘amnestic’ identity. In the cited studies, it was not assessed if or to what degree the applied stimuli had autobiographical meaning for the tested ‘amnestic’ and ‘mnestic’ dissociative identities. Our study included traumatic memories that were subjectively autobiographical for TIS but not for NIS and found that NIS and TIS had different subjective, psychophysiological, and neural reactions to a description of the involved traumatic memories. We also found that as an NIS, DID patients did not relate these traumatic memories to themselves (Reinders et al. 2003). These results indicate the importance of using autobiographical information when investigating inter-identity amnesia in DID. (ii) Inter-identity amnesia may predominantly exist between different types of dissociative identities, particularly between neural and trauma-related identity states. This has been clinically observed, theoretically proposed (van der Hart et al. 2006) and is in line with our results. Unfortunately, in most studies it was not assessed what types of dissociative identities participated, e.g. NIS or TIS. Therefore, we strongly recommend that in future research in DID the types of dissociative identities are verified and reported and that test material is used that is subjectively autobiographical for one dissociative identity, but not for another.
The sociocognitive view of DID entails the idea that this disorder can be easily and readily created in motivated suggestible individuals and that few suggestions would suffice to generate the symptoms of DID (Spanos 1996). However, this is not supported by our study. Still, one might argue that the short practice period of DID simulation is insufficient to simulate the psychobiological profiles of NIS and TIS. However, even if years of practice could generate these profiles, our findings show that our controls do not activate many brain areas found in DID patients and it seems unlikely that this will change with practice.
For the first time, it is shown using brain imaging that neither high- nor low-fantasy-prone healthy women, who enacted two different types of dissociative identity states, were able to substantially simulate these identity states in psychobiological terms. We feel that our study provides an important contribution to the aetiology discussion for DID as the results do not support the idea of an iatrogenic origin for DID.
References
American Psychiatric Association, (APA), DSM-IV, A.P.A.T.F (2000) Diagnostic and statistical manual of mental disorders: DSM-IV-TR. American Psychiatric Pub, Washington, DC
Anderson MC, Ochsner KN, Kuhl B, Cooper J, Robertson E, Gabrieli SW, Glover GH, Gabrieli JDE (2004) Neural systems underlying the suppression of unwanted memories. Science 303:232–235
Braffman W, Kirsch I (1999) Imaginative suggestibility and hypnotizability: an empirical analysis. J Pers Soc Psychol 77:578–587
Bremner JD (2010) Cognitive processes in dissociation: comment on Giesbrecht et al. (2008). Psychol Bull 136:1–6
Brown D, Frischholz EJ, Scheflin AW (1999) Iatrogenic dissociative identity disorder – an evaluation of the scientific evidence. J Psychiatry Law 27:549
Coons PM (2005) Re: the persistence of folly: a critical examination of dissociative identity disorder. Can J Psychiatry 50:813
Dalenberg CJ, Brand BL, Gleaves DH, Dorahy MJ, Loewenstein RJ, Cardeña E, Frewen PA, Carlson EB, Spiegel D (2012) Evaluation of the evidence for the trauma and fantasy models of dissociation. Psychol Bull 138(3):550–588
Dell PF, O’Neil JA (eds) (2009) Dissociation and the dissociative disorders: DSM-V and beyond. Routledge, New York
Draijer N, Boon S (1999) Imitation of dissociative identity disorder: patients at risk, therapists at risk. J Psychiatry Law 27:423–458
Driver J, Vuilleumier P (2001) Perceptual awareness and its loss in unilateral neglect and extinction. Cognition 79:39–88
Elzinga BM, van Dyck R, Spinhoven P (1998) Three controversies about dissociative identity disorder. Clin Psychol Psychother 5:13–23
Elzinga BM, Phaf RH, Ardon AM, van Dyck R (2003) Directed forgetting between, but not within, dissociative personality states. J Abnorm Psychol 112:237–243
Elzinga BM, Ardon AM, Heijnis MK, De Ruiter MB, Van Dyck R, Veltman DJ (2007) Neural correlates of enhanced working-memory performance in dissociative disorder: a functional MRI study. Psychol Med 37:235–245
Fraser GA (2005) Re: the persistence of folly: a critical examination of dissociative identity disorder. Can J Psychiatry 50:814
Friston KJ (2009) Modalities, modes, and models in functional neuroimaging. Science 326:399–403
Genovese CR, Lazar NA, Nichols T (2002) Thresholding of statistical maps in functional neuroimaging using the false discovery rate. Neuroimage 15:870–878
Gharaibeh N, Merskey H (2009) Removing DID/MPD from DSM-V: an email petition against the inclusion of DID in the DSM-V
Giesbrecht T, Merckelbach H (2006) Dreaming to reduce fantasy? – Fantasy proneness, dissociation, and subjective sleep experiences. Pers Individ Differences 41:697–706
Giesbrecht T, Merckelbach H, Kater M, Sluis AF (2007) Why dissociation and schizotypy overlap: the joint influence of fantasy proneness, cognitive failures, and childhood trauma. J Nerv Ment Dis 195:812–818
Giesbrecht T, Lynn SJ, Lilienfeld SO, Merckelbach H (2008) Cognitive processes in dissociation: an analysis of core theoretical assumptions. Psychol Bull 134:617–647
Giesbrecht T, Lynn SJ, Lilienfeld SO, Merckelbach H (2010) Cognitive processes, trauma, and dissociation–misconceptions and misrepresentations: reply to Bremner (2010). Psychol Bull 136:7–11
Gleaves DH (1996) The sociocognitive model of dissociative identity disorder: a reexamination of the evidence. Psychol Bull 120:42–59
Huntjens RJC, Postma A, Peters ML, Woertman L, van der Hart O (2003) Interidentity amnesia for neutral, episodic information in dissociative identity disorder. J Abnorm Psychol 112:290–297
Huntjens RJC, Peters ML, Postma A, Woertman L, Effting M, van der Hart O (2005a) Transfer of newly acquired stimulus valence between identities in dissociative identity disorder (DID). Behav Res Ther 43:243–255
Huntjens RJC, Postma A, Woertman L, van der Hart O, Peters ML (2005b) Procedural memory in dissociative identity disorder: when can inter-identity amnesia be truly established? Conscious Cogn 14:377–389
Huntjens RJC, Peters ML, Woertman L, Bovenschen LM, Martin RC, Postma A (2006) Inter-identity amnesia in dissociative identity disorder: a simulated memory impairment? Psychol Med 36:857–863
Huntjens RJC, Peters ML, Woertman L, van der Hart O, Postma A (2007) Memory transfer for emotionally valenced words between identities in dissociative identity disorder. Behav Res Ther 45:775–789
Lancaster JL, Woldorff MG, Parsons LM, Liotti M, Freitas CS, Rainey L, Kochunov PV, Nickerson D, Mikiten SA, Fox PT (2000) Automated Talairach atlas labels for functional brain mapping. Hum Brain Mapp 10:120–131
Lanius RA, Williamson PC, Densmore M, Boksman K, Neufeld RW, Gati JS, Menon RS (2004) The nature of traumatic memories: a 4-T FMRI functional connectivity analysis. Am J Psychiatry 161:36–44
Lanius RA, Vermetten E, Loewenstein RJ, Brand B, Schmahl C, Bremner JD, Spiegel D (2010) Emotion modulation in PTSD: clinical and neurobiological evidence for a dissociative subtype. Am J Psychiatry 167:640–647
LeDoux JE (2000) Emotion circuits in the brain. Annu Rev Neurosci 23:155–184
Levin R, Spei E (2004) Relationship of purported measures of pathological and nonpathological dissociation to self-reported psychological distress and fantasy immersion. Assessment 11:160–168
Lilienfeld SO, Lynn SJ, Kirsch I, Chaves JF, Sarbin TR, Ganaway GK, Powell RA (1999) Dissociative identity disorder and the sociocognitive model: recalling the lessons of the past. Psychol Bull 125:507–523
Loewenstein RJ (2007) Dissociative identity disorder: issues in the iatrogenesis controversy. In: Vermetten E, Dorahy M, Spiegel D (eds) Traumatic dissociation: neurobiology and treatment. American Psychiatric Press, Washington, DC, pp 275–299
Mathew RJ, Jack RA, West WS (1985) Regional cerebral blood flow in a patient with multiple personality. Am J Psychiatry 142:504–505
Merckelbach H, Muris P (2001) The causal link between self-reported trauma and dissociation: a critical review. Behav Res Ther 39:245–254
Merckelbach H, Rassin E, Muris P (2000) Dissociation, schizotypy, and fantasy proneness in undergraduate students. J Nerv Ment Dis 188:428–431
Merckelbach H, Horselenberg R, Muris P (2001) The Creative Experiences Questionnaire (CEQ): a brief self-report measure of fantasy proneness. Pers Individ Differences 31:987–995
Merckelbach H, Devilly GJ, Rassin E (2002) Alters in dissociative identity disorder. Metaphors or genuine entities? Clin Psychol Rev 22:481–497
Mickleborough MJS, Daniels JK, Coupland NJ, Kao R, Williamson PC, Lanius UF, Hegadoren K, Schore A, Densmore M, Stevens T, Lanius RA (2011) Effects of trauma-related cues on pain processing in posttraumatic stress disorder: an fMRI investigation. J Psychiatry Neurosci 36:6–14
Nijenhuis ERS, Den Boer JA (2009) Psychobiology of traumatisation and trauma-related structural dissociation of the personality. In: Dell PF, O’Neil JA (eds) Dissociation and the dissociative disorders: DSM-V and beyond. Routledge, New York, pp 337–367
Nijenhuis ERS, van der Hart O (2011) Dissociation in trauma: a new definition and comparison with previous formulations. J Trauma Dissociation 12:416–445
Nijenhuis ER, Spinhoven P, Van Dyck R, Van der Hart O, Vanderlinden J (1996) The development and psychometric characteristics of the Somatoform Dissociation Questionnaire (SDQ-20). J Nerv Ment Dis 184:688–694
Nijenhuis ERS, Van der Hart O, Steele K (2002) The emerging psychobiology of trauma-related dissociation and dissociative disorders. In: D’haenen HAH, Den Boer JA, Willner P (eds) Biological psychiatry. Wiley, West Sussex, pp 1079–1098
Nijenhuis ERS, van der Hart O, Kruger K, Steele K (2004) Somatoform dissociation, reported abuse and animal defence-like reactions. Aust N Z J Psychiatry 38:678–686
Piper A, Merskey H (2004a) The persistence of folly: a critical examination of dissociative identity disorder. Part I. The excesses of an improbable concept. Can J Psychiatry 49:592–600
Piper A, Merskey H (2004b) The persistence of folly: critical examination of dissociative identity disorder. Part II. The defence and decline of multiple personality or dissociative identity disorder. Can J Psychiatry 49:678–683
Piper A, Merskey H (2005) The persistence of folly: a critical examination of dissociative identity disorder. Can J Psychiatry 50:814
Pope HG Jr, Barry S, Bodkin A, Hudson JI (2006) Tracking scientific interest in the dissociative disorders: a study of scientific publication output 1984–2003. Psychother Psychosom 75:19–24
Poulsen BC, Matthews WJ Jr (2003) Correlates of imaginative and hypnotic suggestibility in children. Contemp Hypn 20:198–208
Putnam FW (1992) Multiple personality disorder. Br J Psychiatry 161:415–416
Rassin E, Merckelbach H, Spaan V (2001) When dreams become a royal road to confusion: realistic dreams, dissociation, and fantasy proneness. J Nerv Ment Dis 189:478–481
Rauschenberger SL, Lynn SJ (1995) Fantasy proneness, DSM-III-R axis I psychopathology, and dissociation. J Abnorm Psychol 104:373–380
Reinders AATS (2008) Cross-examining dissociative identity disorder: neuroimaging and etiology on trial. Neurocase 14:44–53
Reinders AATS, Nijenhuis ERS, Paans AMJ, Korf J, Willemsen ATM, den Boer JA (2003) One brain, two selves. Neuroimage 20:2119–2125
Reinders AATS, Nijenhuis ERS, Quak J, Korf J, Haaksma J, Paans AMJ, Willemsen ATM, den Boer JA (2006) Psychobiological characteristics of dissociative identity disorder: a symptom provocation study. Biol Psychiatry 60:730–740
Reinders AATS, Willemsen ATM, Vos HPJ, den Boer JA, Nijenhuis ERS (2012) Fact or factitious? a psychobiological study of authentic and simulated dissociative identity states. PLoS ONE 7:e39279
Sar V (2005) Re: the persistence of folly: a critical examination of dissociative identity disorder. What are Dr Piper and Dr Merskey trying to do? Can J Psychiatry 50:813; author reply 814
Sar V, Unal SN, Kiziltan E, Kundaci T, Ozturk E (2001) HMPAO SPECT study of regional cerebral blood flow in dissociative identity disorder. J Trauma Dissociation 2:5–25
Sar V, Unal SN, Ozturk E (2007) Frontal and occipital perfusion changes in dissociative identity disorder. Psychiatry Res Neuroimaging 156:217–223
Savoy RL, Frederick BB, Keuroghlian AS, Wolk PC (2012) Voluntary switching between identities in dissociative identity disorder: a functional MRI case study. Cogn Neurosci 3:112–119
Saxe GN, Vasile RG, Hill TC, Bloomingdale K, Van der Kolk BA (1992) SPECT imaging and multiple personality disorder. J Nerv Ment Dis 180:662–663
Schwabe L, Dalm S, Schächinger H, Oitzl MS (2008) Chronic stress modulates the use of spatial and stimulus–response learning strategies in mice and man. Neurobiol Learn Mem 90:495–503
Sheehan W, Thurber S, Sewall B (2006) Dissociative identity disorder and temporal lobe involvement: replication and a cautionary note. Aust N Z J Psychiatry 40:374–375
Silva CE, Kirsch I (1992) Interpretive sets, expectancy, fantasy proneness, and dissociation as predictors of hypnotic response. J Pers Soc Psychol 63:847–856
Simeon D, Guralnik O, Hazlett EA, Spiegel-Cohen J, Hollander E, Buchsbaum MS (2000) Feeling unreal: a PET study of depersonalization disorder. Am J Psychiatry 157:1782–1788
Spanos NP (1994) Multiple identity enactments and multiple personality disorder: a sociocognitive perspective. Psychol Bull 116:143–165
Spanos NP (1996) Multiple identities and false memories: a sociocognitive perspective. American Psychological Association (APA), Washington, DC
Spiegel D (1984) Multiple personality as a post-traumatic stress disorder. Psychiatr Clin North Am 7:101–110
Spiegel D (2006) Recognizing traumatic dissociation. Am J Psychiatry 163:566–568
Steinberg M (1994) The structured clinical interview for DSM-IV dissociative disorders-revised (SCID-D-R). American Psychiatric Press, Washington, DC
Talairach J, Tournoux P (1988) Co-planar stereotaxic atlas of the human brain: 3-dimensional proportional system: an approach to cerebral imaging. Thieme, Stuttgart
Tsai GE, Condie D, Wu MT, Chang IW (1999) Functional magnetic resonance imaging of personality switches in a woman with dissociative identity disorder. Harv Rev Psychiatry 7:119–122
van der Hart O, Nijenhuis ERS, Steele K (2006) The haunted self: structural dissociation and the treatment of chronic traumatization, 1st edn. W. W Norton & Company, New York
White NM (2009) Some highlights of research on the effects of caudate nucleus lesions over the past 200 years. Behav Brain Res 199:3–23
Xiao Z, Yan H, Wang Z, Zou Z, Xu Y, Chen J, Zhang H, Ross CA, Keyes BB (2006) Trauma and dissociation in China. Am J Psychiatry 163:1388–1391
Yehene E, Meiran N, Soroker N (2005) Task alternation cost without task alternation: measuring intentionality. Neuropsychologia 43:1858–1869
Yehene E, Meiran N, Soroker N (2008) Basal ganglia play a unique role in task switching within the frontal-subcortical circuits: evidence from patients with focal lesions. J Cogn Neurosci 20:1079–1093
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2014 Springer-Verlag Berlin Heidelberg
About this chapter
Cite this chapter
Reinders, A.A.T.S., Willemsen, A.T.M. (2014). Dissociative Identity Disorder and Fantasy Proneness: A Positron Emission Tomography Study of Authentic and Enacted Dissociative Identity States. In: Dierckx, R., Otte, A., de Vries, E., van Waarde, A., den Boer, J. (eds) PET and SPECT in Psychiatry. Springer, Berlin, Heidelberg. https://doi.org/10.1007/978-3-642-40384-2_16
Download citation
DOI: https://doi.org/10.1007/978-3-642-40384-2_16
Published:
Publisher Name: Springer, Berlin, Heidelberg
Print ISBN: 978-3-642-40383-5
Online ISBN: 978-3-642-40384-2
eBook Packages: MedicineMedicine (R0)