
Abstract
Fractures of the coronoid process of the ulna usually result from a fall on the outstretched hand with the elbow in extension to 20º of flexion with a posterolateral valgus or posteromedial varus stress. These are rare injuries that usually do not occur in isolation. They mostly emerge with elbow dislocations, often combined with radial head and olecranon fractures. According to the current literature, coronoid fractures can be found in 12–39 % of patients with elbow dislocations. Besides concomitant fractures, soft tissue lesions play a major role in the pathophysiology of coronoid fractures. The combination of a coronoid fracture, radial head fracture, and medial collateral ligament (MCL) tear is called the “terrible triad injury” of the elbow, emphasizing the severity of this injury resulting in gross instability if not treated adequately.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
These keywords were added by machine and not by the authors. This process is experimental and the keywords may be updated as the learning algorithm improves.
9.1 Introduction
Fractures of the coronoid process of the ulna usually result from a fall on the outstretched hand with the elbow in extension to 20º of flexion with a posterolateral valgus or posteromedial varus stress. These are rare injuries that usually do not occur in isolation. They mostly emerge with elbow dislocations, often combined with radial head and olecranon fractures. According to the current literature, coronoid fractures can be found in 12–39 % of patients with elbow dislocations. Besides concomitant fractures, soft tissue lesions play a major role in the pathophysiology of coronoid fractures. The combination of a coronoid fracture, radial head fracture, and medial collateral ligament (MCL) tear is called the “terrible triad injury” of the elbow, emphasizing the severity of this injury resulting in gross instability if not treated adequately.
The coronoid process is an important stabilizer of the elbow joint for several reasons: Axial stability is provided by the coronoid functioning as buttress. It is well known that 40 % of the axial forces are conducted through the ulnohumeral joint. The anterior capsule attaches a few millimeters distally to the tip, the brachialis muscle inserts on the base, and the lateral collateral ligament (LCL) to the lateral side of the coronoid. The MCL inserts on the anteromedial facet, the sublime tubercle, and is the primary stabilizer against valgus stress. Fractures of the anteromedial facet are therefore assessed as a distinct entity now and are taken into account by O’Driscoll’s classification of coronoid fractures.
9.2 Diagnosis
Patients present with swelling and pain of the injured elbow. In case of unreduced dislocations, the elbow is deformed. Neurovascular damages must be excluded and stability has to be assessed. Lateral and anteroposterior (a.p.) radiographs form the basis of the diagnostic investigation. Fractures of the anteromedial facet may present as a fracture of the sublime tubercle on the a.p. or as a “double crescent sign” on the lateral radiograph. Sometimes anteromedial facet fractures are misinterpreted as harmless tip fractures, because the oblique fracture component cannot be detected on the standard radiographs. As coronoid fractures can easily be missed or underestimated on plain radiographs, a computed tomography (CT) scan is recommended for the correct classification.
9.3 Classification
Coronoid fractures were first classified by Regan and Morrey in 1989:
Type I | Fracture of the tip |
Type II | Fracture involves less than 50 % |
Type III | Fracture involves more than 50 % of the coronoid |
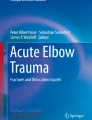
Each type is subclassified according to the absence (A) or presence (B) of a dislocation (Fig. 9.1).

Regan and Morrey classification
In 2003, O’Driscoll et al. [1] introduced a new classification system with special consideration of the anteromedial facet (Table 9.1). Type 1 fractures affect the tip, type 2 the anteromedial facet, and type 3 the base. Each type is divided into subtypes. Treatment options can be derived from this classification.
9.4 Treatment
Most coronoid fractures are small type I fractures of the tip. These can be treated conservatively. The treatment of larger coronoid fragments is usually operative, although the fracture may seem harmless on standard radiographs. As these fractures must be interpreted as fracture-dislocations in most cases, even fractures that appear harmless on standard radiographs may present severe injuries. Correct classification requires a CT scan. Not only the bony structures, but also the soft tissues have to be addressed during surgery.
A medial approach is used for the stabilization of isolated coronoid fractures. The ulnar nerve must be exposed, but not necessarily transposed. Additional lesions may require a different approach or additional approaches. In case of a radial head fracture, the coronoid may be stabilized via Kocher’s approach before stabilization of the radial head. If the elbow is severely unstable, a posterior approach may allow addressing of all lesions with only one skin incision.
9.4.1 Type I
Only isolated small fractures of the coronoid tip type I.1 can be treated conservatively with a short period of immobilization followed by early functional therapy. If a small fragment dislocates into the joint, this loose body should be removed arthroscopically. A CT scan should be performed to ensure that the fracture is not underestimated, as these fractures appear small on the standard radiographs but average 39 % of the coronoid height and therefore include the capsular insertion. Additionally, they may involve the anteromedial facet. These fractures are unstable and should therefore be addressed operatively. If the fragments are large enough, screw fixation may be performed; smaller fragments are reattached with transosseous sutures. Type I fractures are typically part of terrible triad injuries (radial head fracture + coronoid fracture + MCL rupture). Smaller coronoid fragments must not be addressed if maintenance or replacement of the radial head leads to a stable joint. Fractures involving 20–30 % of the coronoid height should be stabilized in this setting. Anatomical reconstruction of all elements is necessary to prevent chronic instability. When stable fixation cannot be achieved, hinged external fixation is recommended to allow early functional therapy.
9.4.2 Type II
As these fractures involve the onset of the anterior bundle of the MCL, they are unstable. Fixation is required. Smaller fragments can be secured with sutures. Larger fragments can be stabilized with screws or a buttress plate through a medial approach.
9.4.3 Type III
Type III fractures represent severe injuries, often concomitant with additional fractures and extensive ligamentous damage. Anatomical reconstruction of the coronoid is the essential point in restoring a stable elbow joint. Screw and plate osteosynthesis is recommended. In case of type III.1 fractures with one or two bigger fragments, stable fixation usually can be achieved. In case of a more complex, comminuted fracture situation, especially coming along with transolecranon fracture dislocations, it may not be possible to obtain stable fixation with osteosynthesis alone. Hinged external fixation should be performed if there is any doubt regarding elbow stability. If the coronoid cannot be repaired, the olecranon tip or a fragment of an irreconstructible radial head can be used to replace it.
9.5 Postoperative Rehabilitation
Active and active-assisted physiotherapy should be initiated as early as possible. Time of splinting should not exceed 2 weeks. However, exercises should begin early postoperatively. Varus and valgus stresses as well as resistive exercises should be omitted for 6 weeks.
9.6 Complications
Complications are numerous with this kind of fracture, especially in case of terrible triad injuries and transolecranon fracture-dislocations. Poor clinical results can be found most notably with severe fracture types. Elbow stiffness and heterotopic ossifications represent the most common complications. Furthermore, ulnar nerve irritation, chronic instability, and joint incongruity can be seen. Elbow stiffness resulting from heterotopic ossifications, ulnar neuropathy, and as instability and incongruity are addressed by early revision surgery. Elbow stiffness resulting from capsular contracture should not be released before 6 months postoperatively. More or less severe osteoarthrosis can be observed in nearly all of the cases, but must not be symptomatic. Anatomic and stable joint restoration marks the best condition to avoid poor results.
9.7 Conclusion
Fractures of the coronoid process of the ulna are rare injuries that usually do not occur in isolation. They mostly emerge with elbow dislocations. Correct diagnosis and classification of these fractures can be challenging. Especially smaller coronoid fragments can easily be underestimated or missed on standard radiographs. Fractures are classified either according to Regan and Morrey’s or, more accurately, to O’Driscoll’s classification with direct consequence to treatment strategies. As the coronoid process is an important stabilizer of the elbow joint, providing axial, varus and rotatory stability, initiation of the correct treatment is essential to restore elbow function and stability. The important role of the coronoid process for elbow stability has been increasingly recognized in recent years. Treatment guidelines have changed to a mainly operative pathway. The current concept is to fix all coronoid fractures that are associated with elbow instability. Only small tip fractures that are not associated with elbow instability may be treated conservatively. But even small coronoid fragments may lead to instability, as these often represent lesions of important soft tissues attachments. Early diagnosis and correct classification of coronoid fractures often require a CT scan. They are essential to restore normal elbow function and stability.
Case 1
Fracture of the anteromedial facet + coronoid tip + sublime tubercle (III.3) (a–c) stabilized with a plate (Acumed, USA), a free screw, and a suture anchor (d and e). (© Klaus Burkhart, Lars Müller, Köln; Pol Rommens, Mainz)

Case 2
Patient with type III.1 fracture (a–c) stabilized with a cannulated screw and a buttress plate (d and e). (© Klaus Burkhart, Lars Müller, Köln; Pol Rommens, Mainz)

Case 3
Conservatively treated patient with I.1–I.2 coronoid fracture. The CT scan and 3D-reconstructions nicely show the tip fracture with an intact sublime tubercle. (© Klaus Burkhart, Lars Müller, Köln; Pol Rommens, Mainz)

Reference
1. O’Driscoll SW, Jupiter JB, Cohen MS, Ring D, McKee MD (2003) Difficult elbow fractures: pearls and pitfalls. Instr Course Lect 52:113–134
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2014 Springer-Verlag Berlin Heidelberg
About this chapter
Cite this chapter
Burkhart, K.J., Rommens, P.M., Müller, L.P. (2014). Coronoid Fractures. In: Oestern, HJ., Trentz, O., Uranues, S. (eds) Bone and Joint Injuries. European Manual of Medicine. Springer, Berlin, Heidelberg. https://doi.org/10.1007/978-3-642-38388-5_9
Download citation
DOI: https://doi.org/10.1007/978-3-642-38388-5_9
Published:
Publisher Name: Springer, Berlin, Heidelberg
Print ISBN: 978-3-642-38387-8
Online ISBN: 978-3-642-38388-5
eBook Packages: MedicineMedicine (R0)