
Abstract
The lifetime incidence of hip trauma is about 23.3 % in males and 11.2 % in females [1, 2]. Major complications of hip traumas include nonunion, malunion, and osteonecrosis. Posttraumatic osteonecrosis, which is reported in a range of 4.8–52.9 %, ultimately leads to arthritis unless diagnosed in the initial stage [3, 4]. Patients with hip injuries should be followed closely for the earlier diagnosis of osteonecrosis. Timely treatment can prevent the progression of osteonecrosis and later arthritic changes. After the diagnosis of necrosis, appropriate treatment must be done in early stages if head preservation seems possible.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
- Femoral Head
- Femoral Neck Fracture
- Extracorporeal Shock Wave Therapy
- Fibular Grafting
- Pinhole Collimator
These keywords were added by machine and not by the authors. This process is experimental and the keywords may be updated as the learning algorithm improves.
1 Introduction
The lifetime incidence of hip trauma is about 23.3 % in males and 11.2 % in females [1, 2]. Major complications of hip traumas include nonunion, malunion, and osteonecrosis. Posttraumatic osteonecrosis, which is reported in a range of 4.8–52.9 %, ultimately leads to arthritis unless diagnosed in the initial stage [3, 4]. Patients with hip injuries should be followed closely for the earlier diagnosis of osteonecrosis. Timely treatment can prevent the progression of osteonecrosis and later arthritic changes. After the diagnosis of necrosis, appropriate treatment must be done in early stages if head preservation seems possible.

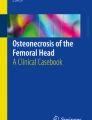
Plain radiographs of a 45-year-old man with right femoral osteonecrosis show linear sclerosis (arrow) in the right femoral neck (a, b). These look like a femoral neck fracture pattern (High signal intensity bandlike lesion, indicated by arrow) on MRI image (c), but bone scan images show the characteristics of avascular necrosis with photon defect and increased uptake of subcapital area (d)

Serial radiographs of anterior rotational trochanteric osteotomy from a 16-year-old man with posttraumatic osteonecrosis of the femoral head are shown

Gluteus medius muscle pedicl bone graft from iliac crest (a, b) and from greater trochanter (c, d)

Serial pinhole bone scintigraphy after vessel-pedicle bone graft for osteonecrosis of the femoral head shows gradually increasing uptake in the femoral head

Three cases of posttraumatic osteonecrosis development are shown
Treatment in both posttraumatic and nontraumatic osteonecrosis is very similar. The choice of treatment will depend on patient age, gender, extent of necrosis, and location of osteonecrosis.
2 Incidence of Posttraumatic Osteonecrosis
Hip trauma is a major risk factor of osteonecrosis together with steroid, alcohol, and connective tissue diseases. The risk increases with the degree of displacement and comminution of fracture and dislocation. The risk of osteonecrosis also increases as the fracture line moves closer to the head, and subcapital fractures have the maximum risk of osteonecrosis [5–10].
The incidence of osteonecrosis after dislocation, which is reported to be in the range of 10–25 %, varies depending on the severity of injury of the associated femoral head or acetabular fractures [11]. Eighty-five to ninety percent of hip dislocations are posterior dislocations with or without other associated femoral head injuries [12]. Hougaahou et al. [4] reported that the incidence of osteonecrosis was 4.8 % when anatomical reduction was performed within 6 h after dislocation, while the percentage rose to 52.9 % when the reduction was performed after 6 h.
The incidence of osteonecrosis after a displaced femoral neck fracture is reported to be 15–20 % [13–16]. The discrepancies in the reported incidence reflect variation with fracture types, accuracy of reduction, and time to reduction.
Osteonecrosis can occur in neck fractures whether the fracture occurs at the intra- and extracapsular level. In general intracapsular fractures are at higher risk compared to extracapsular fractures [17, 18]. The actual incidence may be estimated to be higher considering the possibility of follow-up loss or overlooked reports of osteonecrosis after pertrochanteric fractures in the literature [19].
2.1 Factors Related to the Incidence of Osteonecrosis
2.1.1 Age
Age is a suspected, but unconfirmed, factor related with the incidence of osteonecrosis [13, 20–23]. Some researchers claimed that the incidence of posttraumatic osteonecrosis is positively correlated with age [20, 21], while another study reported that the incidence decreased after 75 years of age [13]. This may reflect the fact that in younger people these injuries often occur after high-energy trauma, with associated damage to soft tissue and vascularity similar to nontraumatic osteonecrosis, in contrast to more elderly individuals in which injuries typically occur after low-energy trauma. These research findings suggest that the estimated incidence of osteonecrosis is high after intracapsular fractures that occur among adults under 50 years of age. It is very important to determine the best treatment, especially in young patients who have a long life expectancy and high activity level.
2.1.2 Degree of Displacement and Reduction
The degree of displacement in the intracapsular fracture is closely related with the development of osteonecrosis. In Garden’s classification, without displacement is classified as Type 1 and 2 and with displacement is classified as Type 3 and 4. This classification helps to predict development of osteonecrosis [14]. Researchers have reported a strong correlation between the development of avascular necrosis and fragment displacement [24]. This suggests that damage in reticular arteries caused by displacement of bone fragments or posterior dislocation plays an important role in the development of posttraumatic osteonecrosis.
The degree of reduction in femur neck fracture is determined based on the Garden’s alignment index, which refers to the angles of the medial cortex line and proximal trabeculae bundle axis on a radiograph of the anterior and posterior segments of hip joints. An acceptable range of 150–185° insures maximum chances of union and minimum chances of osteonecrosis [8, 25, 26]. However, severe comminuted fracture of the femoral neck or malrotation and/or unstable fixation may negatively affect revascularization of the head and may lead to osteonecrosis [14]. Sustained traction or excessive internal/external rotation of the hip, especially if maintained for a long time before surgery, may damage the lateral femoral circumflex artery causing osteonecrosis [27–30].
To decrease risk of damage of the major vessels, it is preferable to avoid excessive extension or internal rotation of the hip joint [28–32]. Several reports recommended that the removal of intracapsular hematoma improves blood flow of the femoral head and decreases the development of osteonecrosis [33–35].
Every reduction after traumatic hip dislocation is also important to prevent osteonecrosis. Sanders et al. [9] found that the incidence of osteonecrosis was 4.8 % when reduced within 6 h and 52.9 % when reduced after 6 h. Similarly, Yeranosian et al. [36] also reported that when the reduction was achieved within 24 h, osteonecrosis progression was four times less as compared to patients in whom reduction was achieved after more than 24 h. These findings emphasize the significance of early reduction in hip joint dislocations.
2.1.3 Timing of Surgical Intervention
It is still controversial whether delay of surgery increases the incidence of osteonecrosis when treating neck fractures [37, 38]. There is a close correlation between delayed treatment and onset of traumatic osteonecrosis of the hip [39, 40]. It was recommended that traction for the neck fracture should be kept in flexion position to decrease intracapsular pressure before surgery [30]. In contrast, another report claimed that early preoperative reduction of the fracture using splinting or traction of a limb did not affect outcome and no correlation was found between the development of osteonecrosis and the time to surgical intervention after trauma. The authors recommended a good preoperative plan and achievement of a stable and anatomical reduction during operation because these aspects are more important than early surgery [38]. More evidence needs to be collected more a definitive conclusion is reached.
2.1.4 Type of Surgery
The type of surgery also affects the development of osteonecrosis. The incidence of posttraumatic osteonecrosis reportedly decreased significantly when less invasive procedure and the accurate reduction was achieved [29]. Garden et al. reported that the results of follow-up of 500 cases of subcapital femoral neck fracture showed a decrease in the incidence of osteonecrosis depending on the skills and experience of the surgeons [14]. The fixation methods affected the incidence of osteonecrosis based on a study of 219 patients with femoral neck fracture in which four different fixation methods were used [37].
The majority of displaced neck fractures require open reduction and internal fixation. However, during the intraoperative femoral head screw fixation, the remaining retinacular vessel can be damaged if the head rotation is not precise. The lateral circumflex artery can be damaged during intramedullary nail insertion in pertrochanteric or subtrochanteric fracture [41]. Thus, at the time of a internal fixation, the surgeon should be careful about malrotation of the femoral head. Attention should be paid to avoid retinacular artery damage when intramedullary nailing is performed.
In older patients with a femoral neck fracture, arthroplasty as a primary treatment has been performed to avoid secondary surgery because of later osteonecrosis or nonunion. Patient’s age is one of the crucial factors for the choice of treatment in femoral neck fracture. Primary arthroplasty rather than internal fixation is preferred in older patients with femoral neck fracture [42]. Bipolar hemiarthroplasty has advantages of shorter surgery time and lesser bleeding compared with total hip arthroplasty. However, since some patients complain of groin pain after bipolar hemiarthroplasty, total hip arthroplasty is increasing [43].
3 Diagnosis of Posttraumatic Osteonecrosis
3.1 Signs and Symptoms
Most patients with osteonecrosis may not present clinically until later stages. Some patients may remain asymptomatic even in the stage of segmental collapse. The pain in osteonecrosis is usually located in the inguinal/gluteal/proximal femoral region. However, it is commonly neglected by patients and wrongly attributed to previous trauma. Therefore it is important that clinician differentiate these symptoms very carefully. Long-term follow-up of these patients is important as segmental collapse can occur as late as 2 years after injury [8, 13]. It is impossible to detect early osteonecrosis in patients with nontraumatic osteonecrosis, while early diagnosis is possible by interval checkup in patients with posttraumatic osteonecrosis. Therefore, compared with patients with nontraumatic osteonecrosis, proper treatment can be provided to patients with posttraumatic osteonecrosis.
3.2 Imaging
3.2.1 X-ray
X-ray diagnosis of posttraumatic osteonecrosis is very similar to nontraumatic osteonecrosis. When a diagnosis of early stage of osteonecrosis is considered using X-ray, the reported sensitivity of radiologic diagnosis in the early stage is around 41 % [44]. It takes 1–5 years for the pathology of osteonecrosis to progress and produce abnormalities that are apparent on X-ray, and posttraumatic osteonecrosis usually does not appear until 1–2 years after injury. Some reports suggested that most patients show radiologic changes of osteonecrosis within 2–3 years after trauma, while others reported the osteonecrosis was detected at 11–24 months after the internal fixation on plain radiography [7, 13, 14, 16, 45]. Considering these dichotomous reports, osteonecrosis should not be ruled out after a simple check of X-ray with normal appearance, and all patients should be followed up for a protracted time.
If osteoclastic resorption overlaps with new bone formation on the revascularized area, it is evident as mottled density on the X-ray. If the femoral head is collapsed, increased density is evident in the compacted area. Subchondral sclerosis or lucency also suggests osteonecrosis. This may be caused by increased density or osteoporosis in bone tissue where blood is not supplied. In cases of associated nonunion, radiologic changes and late femoral head collapse may be further delayed due to the absence of the revascularization process.
The best view for the femoral neck can be obtained by anteroposterior radiographic view with 15° internal rotation of the hip joint in the supine position. For a clearer view of the femoral head, it is necessary to check the femoral head lateral view, because femoral head collapse and crescent sign (subchondral facture sign) in early stages are mainly detected in the anterosuperior segment of the femoral head. The patient is laid in the supine position with the hip in 90° flexion and 45° abduction. The X-ray beam is directed from anterior to posterior. If the metallic implant blocks the necrotic lesion of interest on the X-ray, the patient’s position may be changed to obtain a better view. The radiographic images are only a basic standard for examination. Magnetic resonance imaging (MRI) and bone scan should be added for precise and definite diagnosis.
3.2.2 MRI
MRI is considered to be the most effective diagnostic tool for the diagnosis of nontraumatic osteonecrosis and traumatic osteonecrosis because of its specificity and sensitivity [46, 47]. MRI can detect bone marrow change very early and can predict its progression. MRI has a higher sensitivity than computed tomography (CT) or radionuclide bone scintigraphy [48, 49]. Glickstein et al. [46] reported MRI specificity and sensitivity of 98 and 97 %, respectively. Diagnoses can be made on the T1-weighted axial localizer and T1-weighted or T2-weighted spin-echo coronal images. The necrotic margin is evident as a single line on T1-weighted images and a double line on T2-weighted images. The double-line sign is a specific and pathognomonic sign also in nontraumatic osteonecrosis, and it is seen in concentric low- and high-signal-intensity bands on the T2-weighted image [50].
MRI has a 96.7 % accuracy compared with the pathologic diagnosis of core biopsy [47]. Even though MRI patterns do not exactly match radiographic stages, MRI can provide all the information necessary for diagnosis and clinical staging, while the bone scan offers limited information [51, 52].
Contrary to general beliefs, internal metallic fixation does not cause any problems in MRI imaging because most metallic implants do not have a ferromagnetic property. However, metallic implants have different susceptibility between metallic implants and surrounding tissues which could cause a geometric distortion known as the susceptibility artifact. If an internal metallic fixation is in place after the injury, it leads to image distortion making diagnosis difficult [48, 53]. The cause of the problem is the nonlinearity that characterizes metal elements. Nonlinearity resulting from pixel shift and intensity variation can lead to serious distortions in images [46, 49, 51, 52, 54–57].
This susceptibility artifact is determined by the composition of metallic devices and the different MRI parameters such as the orientation of devices in relation to direction of the main magnetic field, type of pulse sequence, voxel size as determined by the field of view, image matrix, section thickness, and echo train length [47, 50, 57–60]. Titanium implants create fewer artifacts than stainless steel implants [47]. Bagheri et al. [61] reported fewer artifacts with increasing duration after surgery with metallic implants. Artifacts remain a significant problem in MRI. Some artifacts remain, even when the implants are removed [62].
There are few reports about the MRI findings in posttraumatic osteonecrosis. Speer et al. [63] reported that a two-dimensional Fourier transform spin-echo technique detected no changes in the first 48 h after intracapsular neck fracture. Along the same line, another study reported that no significant changes or histological necrosis were detected even after the first 65 days. Kamano et al. [64] reported on the three patterns on the T1 and T2 fat saturation images taken 24.5 h after femur transcervical neck fractures. Type I, which revealed non-enhancement, was related to necrosis in all cases, while type III showing a total enhancement was linked to femoral head viability in all patients. Type II which reveals partial enhancement was related with osteonecrosis in five of 12 cases. In the report of Sugano et al., MRI was done 1, 6, and 12 months after internal fixation in 17 cases of femur neck transcervical fracture [65]. At 1 month after the surgery, a low signal was detected in T1 and high signal in T2 in eight cases. The authors identified three different types of images: small upper lateral infarction was classified as type 1, narrow upper lateral lesion extending to the fovea as type 2, and wide lesion taking up most of femoral head as type 3. All 17 cases were observed to have abnormalities on MRI. None of the cases in type 1, 75 % cases in type 2, and all the cases in type 3 progressed to necrosis. In the report of Kawasaki et al. on femur neck transcervical fracture, T1-weighted MRI and plain radiographic images were taken at 1, 2, 6, and 12 months after internal fixation [45]. On the images taken 2 months after the procedure, eight of 31 cases showed band-like images; on the images taken in 6 months, 12 cases showed band-like images. Among the band-like images classified as B1 (lateral), B2 (superficial), B3 (intermediate), and B4 (extensive), necrosis was related to the B2, B3, and B4 bands. It was also related to Garden types 3 and 4. Specificity and diagnosis accuracy was 100 and 87 %, respectively.
3.2.3 Bone Scan
Planar scintigraphic imaging has a sensitivity ranging from 47.8 to 78.3 %. Despite the fact that sensitivity is low at stages I and II, planar scintigraphic imaging has several strengths. It has no false-positive imaging and is useful in patients with cardiac pacemakers or intracranial clips or who suffer from claustrophobia, for whom MRI is not indicated [66]. Bone scintigraphy can detect early osteonecrosis even when MRI does not detect the necrotic changes [67, 68]. Maillefert et al. [66] reported that bone scintigraphy with a pinhole collimator has a better sensitivity in diagnosing osteonecrosis compared with bone scintigraphy. Turner et al. [69] reported that technetium-99m antimony colloid as a radionuclide does not stop additional osteogenesis by binding with subendothelial dendritic macrophages. According to the authors, uptake of technetium-99 m antimony colloid decreases after bone fracture and devascularization. The uptake increases as the necrosis progresses, and vascularity and bone activity increases. According to Dong et al. [70], nuclide uptake increases 3–4 months after surgery and peaks 6–12 months after surgery.
A pinhole collimator is a type of a conical collimator having a small circular aperture (3–5 mm). A pinhole collimator produces an inverted image as a photographic camera does. This image can be enlarged so that even a small structure can be detected, contributing to diagnosis of scintigraphic abnormality. A pinhole collimator increases the resolution of circumscribed areas, and its acquisition time is just 15 min, while SPECT scanning takes 45 min. Planar scintigraphic imaging using quantitative bone scanning offers physiologic data not possible in MRI and also makes uptake quantification available at perfusion and static phase. Therefore, when the patients with head-preserving surgery were followed for revascularization, planar scintigraphic imaging is most useful than any other diagnostic tools [66].
4 Treatment
4.1 General Considerations for Choosing Treatment
As in the treatment of nontraumatic osteonecrosis, the ultimate goal of treatment for posttraumatic osteonecrosis is to preserve the femoral head, especially in young patients. However, arthroplasty has been widely used with great development of surgical procedures, implants and their materials, high survival rates and patient satisfaction. Clear differentiation of indications between arthroplasty and head salvage procedure is still controversial, and a grey zone still persists. Even though arthroplasty shows good prognosis in most cases, there are some related complications that include joint infection, osteolysis, and aseptic loosening. These compromise the longevity of total hip arthroplasty.
Femoral head-preserving surgery should be considered for young patients, especially adolescent patients, when a surgeon decides on treatment of posttraumatic osteonecrosis considering the remaining life expectancy and high activity of patients.
Osteotomy has been one of the methods preserving the femoral head in osteonecrosis. If the necrotic lesion is anteriorly or posteriorly shifted, rotational trochanteric osteotomy may be one choice. If the lesion is medially or laterally shifted, varus osteotomy or valgus osteotomy can be performed.
After the head-preserving surgery, the healing period until ambulation is around 3 months. On the other hand, total hip arthroplasty is usually shorter in the healing period than that of head-preserving surgery. For this reason, there are some patients who prefer total hip arthroplasty because the patients have to return to work soon. If a patient who has suffered osteonecrosis desires an early return to daily life, even if head-preserving surgery is more appropriate for the patient, total hip arthroplasty may be indicated.
Total hip arthroplasty may be considered inevitable in cases with large necrosis or serious collapse. Regarding the bearing surface for total hip arthroplasty, ceramic-on-ceramic surface is recommended to reduce complications such as aseptic loosening or osteolysis, especially in young patients [71].
In determining the surgery for the osteonecrosis, the age of the patient; severity, extent, and location of necrosis; and socioeconomic needs of the patient should be considered carefully. Surgeon’s ability to perform head-preserving surgery seems one of the factors to be considered in the decision process.
4.2 Head-Preserving Procedures
Electric shock wave shows some effects on the treatment of osteonecrosis but no established conclusion is possible yet. Wang et al. showed that in patients with the ARCO I, II, and III osteonecrosis, treatment with extracorporeal shock wave had better results than treatment with core decompression and nonvascularized fibular grafting. They postulated that shock wave induces hyperstimulation analgesia by increasing threshold of pain and promotes bone healing as a result of microfracture [72]. Further prospective studies with reliable clinical data are required for wide clinical application.
4.2.1 Bisphosphonate
Bisphosphonate can be effective for patients with posttraumatic osteonecrosis if it is used together with other means of treatment [72–76].
The use of bisphosphonate for nontraumatic osteonecrosis both enhances the apoptosis of osteoclasts and reduces the apoptosis of osteoblasts, thus blocking the progression of bone resorption and collapse. Similar effects have been observed among posttraumatic osteonecrosis patients. Agarwala et al. [73] reported that the use of bisphosphonate brought about functional improvement and helped prevent osteonecrosis progression in their study based on 69 cases of hip osteonecrosis including five cases of posttraumatic osteonecrosis. However, the study reported that the result was unsatisfactory for the osteonecrosis where collapse was already in progress. Ramachandran et al. [74] also found in their clinical study of 28 posttraumatic hip cases that bisphosphonate led to a delay in osteonecrosis progression.
In recent years, cocktail therapies that use bisphosphonate together with extracorporeal shock wave therapy, electrical shock wave therapy, hyperoxygen therapy, and nonsteroidal anti-inflammatory drug have been suggested for femoral head necrosis of the hip [72, 75]. Bisphosphonate has been avidly investigated. In treatment of osteonecrosis of the hip, comparison of extracorporeal shock wave with shock wave and alendronate and the proper volume of bisphosphonate and period for using are not established yet [76]. But, research on bisphosphonate suggests that its use for the treatment of patients in a relatively early stage of posttraumatic osteonecrosis could be justified.
4.2.2 Viable Bone Grafting
Viable bone grafting that has been used for nontraumatic osteonecrosis can also be a good method treating traumatic osteonecrosis. Many reports introduced several bone graft methods including autograft or central decompression combined with allogeneic transplantation. Free vascularized fibular grafting for the treatment of osteonecrosis of the femoral head was first described in the 1970s [77]. Later Phemister [78] reported success rate of 70 % using vascularized fibular graft; Zhang et al. [79] reported that free vascularized fibular grafting was worthwhile for teenagers with posttraumatic osteonecrosis, even though collapse of the femoral head had reported that through this method, pain relief and restoration of the sphericity of the femoral head could be expected. Even though the vascularized fibular grafting had good results in atraumatic osteonecrosis in early stages, recently these methods are not used widely due to the unpredictable results and complicated surgical technique.
Since the early 1980s, vessel-pedicle iliac bone has been used for treatment for avascular necrosis. Patients with up to 2 mm collapse of the femoral head can be considered for surgery. Zhang et al. [79] reported a 72 % success rate of free vascularized fibular grafting in teenaged patients. They suggested that free vascularized fibular grafting is a viable procedure in teenagers with posttraumatic osteonecrosis even when the head has already collapsed. Noguchi et al. [80] suggested that success with this method requires surgeons to pay attention to the size of the bone graft, adequate position of insertion, good circulation to the bone graft, and sufficient varus fixation when there is additional transtrochanteric rotational osteotomy of the femoral head. Once the procedure is successful through a microsurgical technique, quicker and definitive healing can be expected. However, some limitations are long operation time and presence of poor lateral femoral circumflex artery in some patients.
Muscle-pedicle iliac bone graft is a method that can be used for patients with the same indications as vessel-pedicle iliac bone graft. Pallazzi et al. [81] first performed tensor fascia lata muscle-pedicle iliac graft in 1973; Baksi reported sartorius muscle-pedicle iliac graft in 1983 and tensor fascia lata muscle-pedicle iliac graft in 1991. All these muscle-pedicle bone grafts have the merit of not requiring microsurgical skill, faster bony union with more cancellous portion, shorter surgical time, and ease of the technique. However, this therapy is limited in preventing head collapse, and some patients may have poor muscle vascularity or weakness of transferred muscle [82, 83]. In our institution, we use the greater trochanter graft instead of iliac graft attached with gluteus medius muscle. This technique is less invasive, with only a small incision, and preserves the strength of the gluteus medius muscle. Furthermore, it shows good results in patients who have undergone muscle-pedicle bone graft with greater trochanter, similar to the results in those who underwent muscle-pedicle bone graft with ilium [84].
4.2.3 Osteotomy
Osteotomy can be used for both nontraumatic or posttraumatic osteonecrosis. The different type are intertrochanteric osteotomy and transtrochanteric rotational osteotomy developed by Sugioka and varus/valgus osteotomy. Intertrochanteric osteotomy rotates the femoral head anteriorly or posteriorly, substituting weight-bearing portion from necrotic lesion to healthy bone and cartilage. This method was first proposed by Wagner and Zeiler in the 1960s [81, 85]. Later, Sugioka et al. [86] tried a new method of transtrochanteric osteotomy; many surgeons subsequently adopted this method. The purpose of the Sugioka transtrochanteric osteotomy is to rotate necrotic lesion of the femoral head from anterosuperior to inferior area, thus removing shearing force transmitted to necrotic lesion, thereby preventing progressive collapse of articular surface in younger patients. This osteotomy is used in lesions that do not proceed to the end stage and which are limited to anterior or posterior of bone head [81]. In their 11-year follow-up, Sugioka et al. reported a success rate of 88 %. Even in stages III and IV where the necrotic area had progressed so as to cause degenerative arthritis, the reported success rates were 73 and 68 %, respectively [86].
The Sugioka osteotomy is done with the patient in the lateral position. An anterolateral approach and capsule incision is used to expose the femoral neck. Two pins are inserted in the basicervical area. Greater trochanteric osteotomy is done perpendicular to the femoral neck long axis, followed by secondary perpendicular osteotomy above the lesser trochanter. By using pin of proximal bone fragment, the femoral head is anteriorly rotated along with necrotic lesion between 70° and 90°, substituting the weight-bearing surface to the non-necrotic portion. Yoon et al. modified the original technique. The quadratus femoris muscle was left attached and the branch of medial circumflex just above the lesser trochanter was identified by Doppler ultrasonography and preserved. After joint capsule incision, osteotomy was then done in the basicervical area perpendicular to the long axis of the neck of femur, without greater trochanteric osteotomy. The femoral neck and head were then rotated using Steinmann pin and fixation accomplished by two or three cannulated cancellous screws. Since Yoon’s modified transtrochanteric rotational osteotomy does not involve greater trochanter osteotomy, fixing the greater trochanter is not needed. The advantage of this osteotomy comparing to Sugioka’s osteotomy is shorter surgery time, less distortion of the proximal femur, and early rehabilitation. Preservation of the greater trochanter makes total hip arthroplasty easier if required later. However, this method is technically demanding, and therefore good results are possible only in the hands of an experienced surgeon [81].
4.3 Hip Joint Arthroplasty
Recently, hip arthroplasty has become the most effective method to treat end-stage osteonecrosis, despite unresolved problems of infection, dislocation, implant failure, osteolysis, and aseptic loosening. Results of total hip arthroplasty for osteonecrosis have varied widely. Ortiguera et al. [87] reported that in the 18-year follow-up of 188 people under the age of 50 who underwent total hip arthroplasty, 79 % of the patients needed revision surgery after primary total hip arthroplasty on osteonecrosis. On the other hand, Kim et al. recently reported no complications, except for one, in a study of 127 cases. They suggested that the cementless metaphyseal-fitting anatomical total hip prosthesis provides outstanding midterm fixation and the alumina-on-alumina ceramic bearing provides a high rate of survivorship without osteolysis. Yoon et al. [88] reported that in a minimum 6-year follow-up of 41 people under the age of 50 who underwent total hip arthroplasty, there were no complications such as osteolysis, femoral stem subsidence, or liner wear at the final follow-up.
When total hip arthroplasty is needed in young patients inevitably, using uncemented stem makes later revision simple [8, 89]. In the past, young and active patients were not recommended for arthroplasty using ceramic-on-ceramic surface because of the problems such as ceramic liner fracture [90]. However, recent development of delta ceramic has provided better longevity by reduced aseptic loosening and osteolysis. Therefore, to reduce incidence of loosening related to osteolysis, the use of ceramic-on-ceramic surface is recommended as the bearing surface choice [91].
5 Summary
Posttraumatic osteonecrosis is one of the most unfortunate complications in patients with hip trauma. The most important thing is early detection and getting the best prevention and treatment. At the postoperative follow-up, accurate and fast diagnosis should be performed. Proper decision should be provided with consideration of age, location of necrotic lesion, extent of necrosis, and socioeconomic demand of the patients. Especially in young patients, total hip arthroplasty should be considered as not the best choice of the treatment but as the last choice of the treatment.
References
Prasad Antapur NM, Gandhi R. Fractures in the elderly: when is hip replacement a necessity? Clin Interv Aging. 2010;6:1–7.
Kanis JA, Johnell O, Oden A, Sembo I, Redlund-Johnell I, Dawson A, De Laet C, Jonsson B. Long-term risk of osteoporotic fracture in Malmo. Osteoporos Int. 2000;11:669–74.
Sen RK, Tripathy SK, Gill SS, Verma N, Singh P, Radotra BD. Prediction of posttraumatic femoral head osteonecrosis by quantitative intraosseous aspirate and core biopsy analysis: a prospective study. Acta Orthop Belg. 2010;76:486–92.
Hougaard K, Thomsen PB. Traumatic posterior dislocation of the hip–prognostic factors influencing the incidence of avascular necrosis of the femoral head. Arch Orthop Trauma Surg. 1986;106:32–5.
McCutchen JW, Carnesale PG. Comparison of fixation in the treatment of femoral neck fractures. Clin Orthop Relat Res. 1982;171:44–50.
Hungerford DS. Early diagnosis of ischemic necrosis of the femoral head. Johns Hopkins Med J. 1975;137(6):270–5.
Jacobs B. Epidemiology of traumatic and nontraumatic osteonecrosis. Clin Orthop Relat Res. 1978;130:51–67.
Bachiller FG, Caballer AP, Portal LF. Avascular necrosis of the femoral head after femoral neck fracture. Clin Orthop Relat Res. 2002;399:87–109.
Sanders S, Tejwani N, Egol KA. Traumatic hip dislocation–a review. Bull NYU Hosp Jt Dis. 2010;68:91–6.
Aaron RK, Stulberg BN, Lennox DW. Clinical and radiographic outcomes in untreated symptomatic osteonocrosis of the femoral head. Tech Orthop. 2001;16:1–5.
Callaghan JJ, Aaron G, Rubash HE. The adult hip. 2nd ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2007.
Kain MS, Tornetta lllP. Hip dislocations and fractures of the femoral head. Bucholz RW, Heckman JD, Court-Brown CM, Tornetta P, editors. Rockwood and Green’s Fractures in Adults, 7th ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2010.
Barnes R, Brown JT, Garden RS, Nicoll EA. Subcapital fractures of the femur. A prospective review. J Bone Joint Surg Br. 1976;58:2–24.
Garden RS. Malreduction and avascular necrosis in subcapital fractures of the femur. J Bone Joint Surg Br. 1971;53:183–97.
James J, Steijn-Myagkaya GL. Death of osteocytes. Electron microscopy after in vitro ischaemia. J Bone Joint Surg Br. 1986;68:620–4.
Sevitt S. Avascular necrosis and revascularisation of the femoral head after intracapsular fractures: a combined arteriographic and histological necropsy study. J Bone Joint Surg Br. 1964;46:270–96.
Shin AY, Morin WD, Gorman JD, Jones SB, Lapinsky AS. The superiority of magnetic resonance imaging in differentiating the cause of hip pain in endurance athletes. Am J Sports Med. 1996;24:168–76.
Chen CM, Chiu FY, Lo WH. Avascular necrosis of femoral head after gamma-nailing for unstable intertrochanteric fractures. Arch Orthop Trauma Surg. 2001;121:505–7.
Bartonicek J, Fric V, Skala-Rosenbaum J, Dousa P. Avascular necrosis of the femoral head in pertrochanteric fractures: a report of 8 cases and a review of the literature. J Orthop Trauma. 2007;21:229–36.
Brown JT, Abrami G. Transcervical femoral fracture. A review of 195 patients treated by sliding nail-plate fixation. J Bone Joint Surg Br. 1964;46:648–63.
Graham J. Early or delayed weight-bearing after internal fixation of transcervical fracture of the femur. A clinical trial. J Bone Joint Surg Br. 1968;50:562–9.
Protzman RR, Burkhalter WE. Femoral-neck fractures in young adults. J Bone Joint Surg Am. 1976;58:689–95.
Stromqvist B, Hansson LI, Nilsson LT, Thorngren KG. Hook-pin fixation in femoral neck fractures. A two-year follow-up study of 300 cases. Clin Orthop Relat Res. 1987;218:58–62.
Lu-Yao GL, Keller RB, Littenberg B, Wennberg JE. Outcomes after displaced fractures of the femoral neck. A meta-analysis of one hundred and six published reports. J Bone Joint Surg Am. 1994;76:15–25.
Kofoed H. Femoral neck fractures in young adults. Injury. 1982;14:146–50.
Lindequist S, Tornkvist H. Quality of reduction and cortical screw support in femoral neck fractures. An analysis of 72 fractures with a new computerized measuring method. J Orthop Trauma. 1995;9:215–21.
Arnoldi CC, Lemperg RK. Fracture of the femoral neck. II. Relative importance of primary vascular damage and surgical procedure for the development of necrosis of the femoral head. Clin Orthop Relat Res. 1977;129:217–22.
Crawfurd EJ, Emery RJ, Hansell DM, Phelan M, Andrews BG. Capsular distension and intracapsular pressure in subcapital fractures of the femur. J Bone Joint Surg Br. 1988;70:195–8.
Gómez-Castresana FB. Fracturas de la extremidad superior del fémur: Estudio de la presión intramedular de la cabeza del fémur y análisis estadístico y valor diagnóstuco de la necrosis avascular. Estudio comparativo con la venografía intraósea [dissertation]. Madrid: Editorial de la Universidad Complutense; 1981.
Maruenda JI, Barrios C, Gomar-Sancho F. Intracapsular hip pressure after femoral neck fracture. Clin Orthop Relat Res. 1997;340:172–80.
Soto-Hall R, Johnson LH, Johnson RA. Variations in the intra-articular pressure of the hip joint in injury and disease. A probable factor in avascular necrosis. J Bone Joint Surg Am. 1964;46:509–16.
Woodhouse CF. Dynamic influences of vascular occlusion affecting the development of avascular necrosis of the femoral head. Clin Orthop Relat Res. 1964;32:119–29.
Bonnaire F, Schaefer DJ, Kuner EH. Hemarthrosis and hip joint pressure in femoral neck fractures. Clin Orthop Relat Res. 1998;353:148–55.
Harper WM, Barnes MR, Gregg PJ. Femoral head blood flow in femoral neck fractures. An analysis using intra-osseous pressure measurement. J Bone Joint Surg Br. 1991;73:73–5.
Laing PG, Ferguson Jr AB. Radiosodium clearance rates as indicators of femoral-head vascularity. J Bone Joint Surg Am. 1959;41-A:1409–22.
Yeranosian M, Horneff JG, Baldwin K, Hosalkar HS. Factors affecting the outcome of fractures of the femoral neck in children and adolescents: a systematic review. Bone Joint J. 2013;95-B:135–42.
Holmberg S, Kalen R, Thorngren KG. Treatment and outcome of femoral neck fractures. An analysis of 2418 patients admitted from their own homes. Clin Orthop Relat Res. 1987;218:42–52.
Gao YS, Ai ZS, Zhu ZH, Yu XW, Zhang CQ. Injury-to-surgery interval does not affect postfracture osteonecrosis of the femoral head in young adults: a systematic review. Eur J Orthop Surg Traumatol. 2013;23:203–9.
Parker MJ, Pryor GA, Myles JW. The value of a special surgical team in preventing complications in the treatment of hip fractures. Int Orthop. 1994;18:184–8.
Zuckerman JD, Skovron ML, Koval KJ, Aharonoff G, Frankel VH. Postoperative complications and mortality associated with operative delay in older patients who have a fracture of the hip. J Bone Joint Surg Am. 1995;77:1551–6.
Orler R, Hersche O, Helfet DL, Mayo KA, Ward T, Ganz R. Avascular femur head necrosis as severe complication after femoral intramedullary nailing in children and adolescents. Unfallchirurg. 1998;101:495–9.
Bhandari M, Devereaux PJ, Tornetta 3rd P, Swiontkowski MF, Berry DJ, Haidukewych G, Schemitsch EH, Hanson BP, Koval K, Dirschl D, Leece P, Keel M, Petrisor B, Heetveld M, Guyatt GH. Operative management of displaced femoral neck fractures in elderly patients. An international survey. J Bone Joint Surg Am. 2005;87:2122–30.
Diwanji SR, Kim SK, Seon JK, Park SJ, Yoon TR. Clinical results of conversion total hip arthroplasty after failed bipolar hemiarthroplasty. J Arthroplasty. 2008;23:1009–15.
Resnick D, Niwayama G. Osteonecrosis: diagnostic techniques, special situations and complications. Philadelphia: WB Saunders; 1995.
Kawasaki M, Hasegawa Y, Sakano S, Sugiyama H, Tajima T, Iwasada S, Iwata H. Prediction of osteonecrosis by magnetic resonance imaging after femoral neck fractures. Clin Orthop Relat Res. 2001;385:157–64.
Glickstein MF, Lawrence BD, Scheibler ML, et al. Avascular necrosis versus other diseases of the hip. Radiology. 1988;169:213–215.
Sofka CM. Optimizing techniques for musculoskeletal imaging of the postoperative patient. Radiol Clin North Am. 2006;44:323–9.
Hendrick RE. The AAPM/RSNA physics tutorial for residents. Basic physics of MR imaging: an introduction. Radiographics. 1994;14:829–46; Quiz 47–8.
Bui FM, Li J, Bott K, Mintchev MP. Volterra series modelling and compensation of non-linear distortions caused by susceptibility difference artefacts related to the presence of ferromagnetic implants in magnetic resonance imaging. Med Eng Phys. 2001;23:207–15.
Laakman RW, Kaufman B, Han JS, Nelson AD, Clampitt M, O’Block AM, Haaga JR, Alfidi RJ. MR imaging in patients with metallic implants. Radiology. 1985;157:711–4.
Baldwin LN, Wachowicz K, Thomas SD, Rivest R, Fallone BG. Characterization, prediction, and correction of geometric distortion in 3 T MR images. Med Phys. 2007;34:388–99.
Schenck JF. The role of magnetic susceptibility in magnetic resonance imaging: MRI magnetic compatibility of the first and second kinds. Med Phys. 1996;23:815–50.
Taber KH, Herrick RC, Weathers SW, Kumar AJ, Schomer DF, Hayman LA. Pitfalls and artifacts encountered in clinical MR imaging of the spine. Radiographics. 1998;18:1499–521.
Pauchard Y, Smith M, Mintchev M. Modeling susceptibility difference artifacts produced by metallic implants in magnetic resonance imaging with point-based thin-plate spline image registration. Conf Proc IEEE Eng Med Biol Soc. 2004;3:1766–9.
Beuf O, Briguet A, Lissac M, Davis R. Magnetic resonance imaging for the determination of magnetic susceptibility of materials. J Magn Reson B. 1996;112:111–8.
Posse S. Direct imaging of magnetic field gradients by group spin-echo selection. Magn Reson Med. 1992;25:12–29.
Lee MJ, Kim S, Lee SA, Song HT, Huh YM, Kim DH, Han SH, Suh JS. Overcoming artifacts from metallic orthopedic implants at high-field-strength MR imaging and multi-detector CT. Radiographics. 2007;27:791–803.
Harris CA, White LM. Metal artifact reduction in musculoskeletal magnetic resonance imaging. Orthop Clin North Am. 2006;37:349–59, vi.
Suh JS, Jeong EK, Shin KH, Cho JH, Na JB, Kim DH, Han CD. Minimizing artifacts caused by metallic implants at MR imaging: experimental and clinical studies. AJR Am J Roentgenol. 1998;171:1207–13.
Port JD, Pomper MG. Quantification and minimization of magnetic susceptibility artifacts on GRE images. J Comput Assist Tomogr. 2000;24:958–64.
Bagheri MH, Hosseini MM, Emami MJ, Foroughi AA. Metallic artifact in MRI after removal of orthopedic implants. Eur J Radiol. 2012;81:584–90.
Buckwalter KA. Optimizing imaging techniques in the postoperative patient. Semin Musculoskelet Radiol. 2007;11:261–72.
Speer KP, Spritzer CE, Harrelson JM, Nunley JA. Magnetic resonance imaging of the femoral head after acute intracapsular fracture of the femoral neck. J Bone Joint Surg Am. 1990;72:98–103.
Kamano M, Narita S, Honda Y, Fukushima K, Yamano Y. Contrast enhanced magnetic resonance imaging for femoral neck fracture. Clin Orthop Relat Res. 1998;350:179–86.
Sugano N, Masuhara K, Nakamura N, Ochi T, Hirooka A, Hayami Y. MRI of early osteonecrosis of the femoral head after transcervical fracture. J Bone Joint Surg Br. 1996;78:253–7.
Maillefert JF, Toubeau M, Piroth C, Piroth L, Brunotte F, Tavernier C. Bone scintigraphy equipped with a pinhole collimator for diagnosis of avascular necrosis of the femoral head. Clin Rheumatol. 1997;16:372–7.
Yoon TR, Rowe SM, Song EK, Mulyadi D. Unusual osteonecrosis of the femoral head misdiagnosed as a stress fracture. J Orthop Trauma. 2004;18:43–7.
Yamagata M, Chao EY, Ilstrup DM, Melton 3rd LJ, Coventry MB, Stauffer RN. Fixed-head and bipolar hip endoprostheses. A retrospective clinical and roentgenographic study. J Arthroplasty. 1987;2:327–41.
Turner JH. Post-traumatic avascular necrosis of the femoral head predicted by preoperative technetium-99 m antimony-colloid scan. An experimental and clinical study. J Bone Joint Surg Am. 1983;65:786–96.
Dong QR, Wang JX, Dong TH. Early diagnosis by scintigraphy of segmental collapse of the femur head following femur neck fracture. J Radiol. 1994;75:423–5.
Hungerford DS. Treatment of osteonecrosis of the femoral head: everything’s new. J Arthroplasty. 2007;22:91–4.
Wang CJ, Wang FS, Huang CC, Yang KD, Weng LH, Huang HY. Treatment for osteonecrosis of the femoral head: comparison of extracorporeal shock waves with core decompression and bone-grafting. J Bone Joint Surg Am. 2005;87:2380–7.
Agarwala S, Jain D, Joshi VR, Sule A. Efficacy of alendronate, a bisphosphonate, in the treatment of AVN of the hip. A prospective open-label study. Rheumatology (Oxford). 2005;44:352–9.
Ramachandran M, Ward K, Brown RR, Munns CF, Cowell CT, Little DG. Intravenous bisphosphonate therapy for traumatic osteonecrosis of the femoral head in adolescents. J Bone Joint Surg Am. 2007;89:1727–34.
Hsu SL, Wang CJ, Lee MS, Chan YS, Huang CC, Yang KD. Cocktail therapy for femoral head necrosis of the hip. Arch Orthop Trauma Surg. 2010;130:23–9.
Lai KA, Shen WJ, Yang CY, Shao CJ, Hsu JT, Lin RM. The use of alendronate to prevent early collapse of the femoral head in patients with nontraumatic osteonecrosis. A randomized clinical study. J Bone Joint Surg Am. 2005;87:2155–9.
Aldridge 3rd JM, Urbaniak JR. Vascularized fibular grafting for osteonecrosis of the femoral head with unusual indications. Clin Orthop Relat Res. 2008;466:1117–24.
Phemister DB. Treatment of the necrotic head of the femur in adults. J Bone Joint Surg Am. 1949;31A:55–66.
Zhang CQ, Sun Y, Chen SB, Jin DX, Sheng JG, Cheng XG, Xu J, Zeng BF. Free vascularised fibular graft for post-traumatic osteonecrosis of the femoral head in teenage patients. J Bone Joint Surg Br. 2011;93:1314–9.
Noguchi M, Kawakami T, Yamamoto H. Use of vascularized pedicle iliac bone graft in the treatment of avascular necrosis of the femoral head. Arch Orthop Trauma Surg. 2001;121:437–42.
Yoon TR. How do I treat ONFH with medium and large lesion in young patients. In: The 57th Spring Congress of the Korean Orthopaedic Association. Hotel inter-burgo DAEGU. 2013.
Baksi DP, Pal AK, Baksi DD. Long-term results of decompression and muscle-pedicle bone grafting for osteonecrosis of the femoral head. Int Orthop. 2009;33:41–7.
Baksi DP. Treatment of osteonecrosis of the femoral head by drilling and muscle-pedicle bone grafting. J Bone Joint Surg Br. 1991;73:241–5.
Baksi DP. Treatment of post-traumatic avascular necrosis of the femoral head by multiple drilling and muscle-pedicle bone grafting. Preliminary report. J Bone Joint Surg Br. 1983;65:268–73.
Wagner H, Zeiler G. Idiopathic avascular necrosis of the femoral head. Results of intertrochanteric osteotomy and resurfacing (author’s translation). Orthopade. 1980;9:290–310.
Sugioka Y. Transtrochanteric anterior rotational osteotomy of the femoral head in the treatment of osteonecrosis affecting the hip: a new osteotomy operation. Clin Orthop Relat Res. 1978;130:191–201.
Ortiguera CJ, Pulliam IT, Cabanela ME. Total hip arthroplasty for osteonecrosis: matched-pair analysis of 188 hips with long-term follow-up. J Arthroplasty. 1999;14:21–8.
Byun JW, Yoon TR, Park KS, Seon JK. Third-generation ceramic-on-ceramic total hip arthroplasty in patients younger than 30 years with osteonecrosis of femoral head. J Arthroplasty. 2012;27:1337–43.
Phillips FM, Pottenger LA, Finn HA, Vandermolen J. Cementless total hip arthroplasty in patients with steroid-induced avascular necrosis of the hip. A 62-month follow-up study. Clin Orthop Relat Res. 1994;303:147–54.
Hannouche D, Nich C, Bizot P, Meunier A, Nizard R, Sedel L. Fractures of ceramic bearings: history and present status. Clin Orthop Relat Res. 2003;417:19–26.
Hamilton WG, McAuley JP, Dennis DA, Murphy JA, Blumenfeld TJ, Politi J. THA with Delta ceramic on ceramic: results of a multicenter investigational device exemption trial. Clin Orthop Relat Res. 2010;468:358–66.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2014 Springer-Verlag Berlin Heidelberg
About this chapter
Cite this chapter
Yoon, T.R., Kim, H.S. (2014). Posttraumatic Osteonecrosis of the Femoral Head. In: Koo, KH., Mont, M., Jones, L. (eds) Osteonecrosis. Springer, Berlin, Heidelberg. https://doi.org/10.1007/978-3-642-35767-1_15
Download citation
DOI: https://doi.org/10.1007/978-3-642-35767-1_15
Published:
Publisher Name: Springer, Berlin, Heidelberg
Print ISBN: 978-3-642-35766-4
Online ISBN: 978-3-642-35767-1
eBook Packages: MedicineMedicine (R0)