
Abstract
Extending labour marked participation of older people (aged 55+) is an important target of European social policy (“Lisbon Strategy”). In addition to reducing economic incentives of early retirement, investments into “good” work, in terms of a favourable psychosocial work environment, are proposed as promising measures towards this end. Distinct national social policies may enhance such efforts.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
These keywords were added by machine and not by the authors. This process is experimental and the keywords may be updated as the learning algorithm improves.
1 Relations of Quality of Work and Retirement
Extending labour marked participation of older people (aged 55+) is an important target of European social policy (“Lisbon Strategy”). In addition to reducing economic incentives of early retirement, investments into “good” work, in terms of a favourable psychosocial work environment, are proposed as promising measures towards this end. Distinct national social policies may enhance such efforts.
In this contribution, we investigate whether important aspects of a “good” quality of work (in terms of a favourable psychosocial work environment) experienced during a relevant stage of people’s employment trajectories are associated with a reduced probability of early retirement. Preliminary findings based on SHARE data indicate that the intention to leave work and employment prematurely is strongly associated with a poor work environment, in particular with a health-adverse psychosocial work environment (Siegrist and Wahrendorf 2009; Siegrist et al. 2007). However, it is not known whether factual retirement decisions follow the same pattern. Because health is an important determinant of early retirement we are also interested in exploring associations of quality of work with health, at least, given the restrictions of our study design, with health status after labour market exit.
Given the fact that SHARE offers opportunities of studying country variations we additionally analyse associations of distinct indicators of national labour and welfare policies with quality of work as well as with early retirement. This analysis is based on evidence indicating differential effects of labour and welfare policies on quality of work and its association with health (Dragano et al. 2010). More specifically the following two complementary hypotheses are tested: First, we assume a relationship between the degree of active labour and social policy and aggregate measures of quality of work across the European countries under study. Second, we assume a relationship between the degree of active labour and social policies and the extent of early retirement across countries.
How is quality of work defined and measured in this analysis? To measure quality of work theoretical models are needed that identify specific stressful job characteristics. Several such models were developed (Antoniou and Cooper 2005), but two models received special attention in occupational research, the demand-control-support model (Karasek et al. 1998) and the effort-reward imbalance model (Siegrist et al. 2004). The first model identifies stressful work by job task profiles characterised by high demand, low control (decision latitude) and low social support at work. The second model claims that an imbalance between high efforts spent and low reward received in turn (money, esteem, career opportunities, job security) adversely affects health. In SHARELIFE all core dimensions of these two work stress models were assessed using 12 Likert-scaled items from the original questionnaires (see Measurement).
Against this background, we provide preliminary answers to the following three questions:
-
1.
Is poor quality of work experienced during a significant period of participants’ employment trajectory associated with reduced health after labour market exit?
-
2.
Is poor quality of work experienced during a significant period of participants’ employment trajectory associated with a higher probability of early retirement?
-
3.
Does quality of work vary according to specific indicators of national labour market and social policies? Does the same hold true for the probability of early retirement?
2 Measuring Quality of Work in SHARELIFE
In addition to retrospective data from the SHARELIFE project, we use data derived from the second wave of SHARE with information on respondents’ health status. For the analyses, we included all people aged 50 or older who reported to be employed at least once during their life course. Furthermore, since we were interested in the influence of quality of work on health during retirement, we restricted the sample to people who already left the labour market in wave 2. Finally, respondents who had difficulties to respond to the retrospective questionnaire (4%) were not included either. This results in a sample of 6,619 men and 7,688 women (N = 14,307) from 13 European countries.
SHARELIFE contains an extensive module on work history collecting information on each job a respondent had during his or her working career (the mean number of jobs is 2.7; see also Chap. 11). In addition to general information (e.g. occupational status, working time), this module includes an assessment of the psychosocial work environment of the last main job of the working career (lasting longer than 5 years). As a result, quality of work during working life (assessed retrospectively) can be related to health and well-being during retirement. Furthermore, quality of work can be related to information on the participants’ retirement behaviour. For the respective analyses, we created five binary indicators of poor quality of work, all based on 12 questionnaire items (4-point Likert scaled) taken from established work stress measures. Each indicator corresponds to a core dimension of existing work stress models (Karasek et al. 1998; Siegrist et al. 2004): physical demands (two items), psychosocial demands (three items), social support at work (three items), control at work (two items), and reward (two items). The respective dimensions were replicated in factor analyses. Here we calculate a simple sum-score for each dimension with higher scores indicating poorer quality of work (threshold: scoring in the upper tertile of the respective measure). The items are displayed in Table 15.1.
Our first research question points to the association of poor quality of work with health status after labour market exit. To this end, we used five different binary indicators of health, taken from the second wave of SHARE and widely used in recent publications (e.g. Avendano et al. 2009): Poor self-perceived health (less than good), scoring high on depressive symptoms (more than three symptoms on the EURO-D-scale), diagnosed chronic diseases (two or more), self-reported symptoms (two or more), and a measure of functional limitation (at least one ADL or IADL limitation). To study associations between quality of work and early retirement (our second research question), we created a binary indicator measuring whether or not respondents were employed at the age of 60 (for all respondents aged 60 or older).
We choose specific macro indicators related to labour market policies within the European countries under study, in particular measures of active labour market policies (ALMP). In general, six different categories of ALMP are distinguished (cf.: European Commission 2009), of which two are used in the context of our analyses: (a) measures related to training programs for the working population, and (b) measures related to rehabilitative services of a country. Training programs refer to programs aiming at increasing working skills, such as workplace training or further education. They improve the level of qualification and strengthen older people’s position within the labour market. To represent this category, we use two indicators in our analyses, one indicator referring to the factual participation in such activities, and one indicator referring to the extent of a country’s labour market expenditures invested into training programs. Specifically, the first indicator is measured as percentage of persons aged 25–64 who stated that they received education or training in the last month. The extent of expenditures is measured as percentage of GDP. The second category of ALMP concerns rehabilitative services in a country, and more specifically supported employment and rehabilitation services for people with limited working capacity. Such measures are thought to increase rates of return to work of people with chronic illness and to reduce time intervals from treatment to re-uptake of work. Our proposed indicator is the amount of a country’s expenditures in such programs, expressed as percentage of GDP. For each macro-variable, we collected information available from 1985 to 2005 from the OECD database, and we computed a respective country mean score for each indicator.
Additional variables are gender, age (divided into age categories), and occupational status (based on ISCO-codes) of the main job of the working career. Respective categories are “legislators and professionals”, “associated professionals and clerks”, “skilled workers”, and “elementary occupations”.
We performed two sets of analyses. First, we present bivariate and multivariate associations between poor quality of work on the one hand and health and early retirement on the other hand. All multivariate analyses are based on logistic multilevel models for binary outcome variables, with individuals (level 1) nested within countries (level 2). This allows for an accurate adjustment for country affiliation. In a second set of analyses, we investigate associations between the three macro indicators on the one hand and the two main measures of quality of work (low control, low reward) and early retirement on the other hand. Weights were considered within the analyses.
3 Effects of Quality of Work on Health and Early Retirement
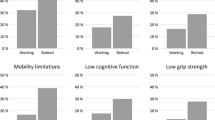
Is the experience of poor quality of work during a prolonged period of one’s working associated with poor health after labour market exit? Table 15.2 gives an initial answer to this question – our first research question. Results indicate that people who experienced poor quality of work in their main job are more likely to report reduced health. This holds true for all five indicators of poor health. As exemplified in Fig. 15.1 by the health indicator of depressive symptoms, this association holds true for all single countries under study, using low control and low reward at work as two main indicators of poor quality of work. The associations reported in Table 15.2 remain significant in multilevel models, where age, gender, occupational status, and country affiliation are considered as potential confounders (see Table 15.2). These findings suggest that the experience of an adverse psychosocial environment is related to poor health during retirement – even after taking into account workers’ occupational status and country affiliation.

Quality of work and depressive symptoms after labour market exit
To investigate our second research question, – the association between quality of work and probability of early retirement – we again consider Table 15.1 where the proportion of people still employed at the age of 60 is presented according to the five indicators of poor quality of work. As can be seen, this proportion of retired people who indicated to have been still employed by the age of 60 is always higher in the group reporting good quality of work as compared to the group reporting poor quality of work. However, once the multivariate model adjusts for the effects of occupational status and country affiliation these differences are no longer statistically significant, with the exception of low control at work. This observation may indicate that occupational status accounts for some part of the association between poor quality of work and early retirement. Similarly, the country seems to be an important confounder, affecting both the level of quality of work and the probability of being still employed at the age of 60. This latter aspect is explored more rigorously in the following section.
How are the three macro indicators related to the two main indicators of poor quality of work (low control and low reward), and to early retirement? Answers are given in Figs. 15.2 and 15.3. First, we observe a pronounced association between a country’s amount of activities related to lifelong learning and its aggregate measure of quality of work (on the left hand side of Fig. 15.2): Higher participation rates in lifelong learning go along with better mean quality of work (higher amount of control and reward at work). However, when comparing this ALMP indicator with the second indicator, the proportion of expenditures in such activities as part of the GDP, respective associations with quality of work are less pronounced (see the middle of Fig. 15.2). This finding may indicate that the first variable is better suited to capture a respective macro-level effect on quality of work (Table 15.3).

Macro indicators and poor quality of work

Macro indicators and still employed at age 60
Second, with regard to expenditures in rehabilitative services, associations with quality of work are again observed in the expected direction: higher investments at country level go along with better mean quality of work (see right hand side of Fig. 15.2).
Third, in Fig. 15.3 we analyse respective associations of the three macro-indicators with the probability of staying at work beyond age 60. Again, the strongest associations are found in case of rates of participation in lifelong learning, where continued employment at older age is more prevalent among people working in countries with high rates of participation, such as Sweden, Denmark or the Netherlands.
4 Summary
In this chapter, retrospective data from SHARELIFE were used to measure poor quality of work in working life and to study its association with five indicators of poor health after labour market exit (question 1), and with continued employment in late mid-life (question 2). Furthermore, we studied whether poor quality of work and continued employment vary according to specific macro indicators of labour market policies (question 3).
Our main results are as follows:
-
First, we found strong evidence that people who experienced poor working conditions during a significant period of their employment trajectory are more likely to report poor health during retirement. Associations were consistent across different health indicators and were observed for all five indicators of poor quality of work (high physical demands, high psychosocial demands, low control, low reward, and low social support at work). Associations remain significant after considering occupational status and country-affiliation in multivariate analyses. Apparently, poor quality of work remains associated with people’s health status after retirement, independent of occupational status and country affiliation.
-
Second, continued employment at older age (60 or older) was found to be more prevalent among people who experienced “good” quality of work, in particular high control at work. However, these associations weakened considerably when occupational status and country affiliation were considered in multivariate analyses. This suggests that occupational status and country affiliation both affect the level of quality of work and the probability of being still employed at the age of 60.
-
Third, quality of work was generally higher in countries with a pronounced active labour market policy. This association was most pronounced in case of high participation rates in training programs for adults (lifelong learning). Similarly, continued employment into old age was more prevalent in countries with high expenditures in rehabilitation services.
In conclusion, these results show that an active labour policy for older workers and the investment into continued education during working life (life long learning) have beneficial effects on working conditions, in terms a favourable psychosocial work environment. Given the strong associations of good quality of work on mental and physical health, long-term effects on employees’ health are considerable. Therefore, promoting quality of work by strengthening these more distant determinants may have beneficial medium- and long-term effects on the workability of an ageing workforce in Europe.
References
Antoniou, A. S., & Cooper, C. (2005). Research companion to organizational health psychology. Chelterham: Edward Elgar Publishers.
Avendano, M., Jürges, H., & Mackenbach, J. P. (2009). Educational level and changes in health across Europe: Longitudinal results from SHARE. Journal of European Social Policy, 19, 301–316.
Dragano, N., Siegrist, J., & Wahrendorf, M. (2010). Welfare regimes, labour policies and workers’ health: A comparative study with 9917 older employees from 12 European countries. JECH, in press.
European Communities. (2009). Labour market policy – Expenditures and participants. Luxembourg: European Union.
Karasek, R., Brisson, C., Kawakami, N., Houtman, I., Bongers, P., & Amick, B. (1998). The Job Content Questionnaire (JCQ): An instrument for internationally comparative assessments of psychosocial job characteristics. Journal of Occupational Health Psychology, 3, 322–355.
Siegrist, J., & Wahrendorf, M. (2009). Quality of work, health, and retirement. The Lancet, 374, 1872–1873.
Siegrist, J., Wahrendorf, M., von dem Knesebeck, O., Jürges, H., & Börsch-Supan, A. (2007). Quality of work, well-being, and intended early retirement of older employees – Baseline results from the SHARE Study. The European Journal of Public Health, 17, 62–68.
Siegrist, J., Starke, D., Chandola, T., Godin, I., Marmot, M., Niedhammer, I., et al. (2004). The measurement of effort-reward imbalance at work: European comparisons. Social Science & Medicine, 58, 1483–1499.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2011 Springer-Verlag Berlin Heidelberg
About this chapter
Cite this chapter
Siegrist, J., Wahrendorf, M. (2011). Quality of Work, Health and Early Retirement: European Comparisons. In: Börsch-Supan, A., Brandt, M., Hank, K., Schröder, M. (eds) The Individual and the Welfare State. Springer, Berlin, Heidelberg. https://doi.org/10.1007/978-3-642-17472-8_15
Download citation
DOI: https://doi.org/10.1007/978-3-642-17472-8_15
Published:
Publisher Name: Springer, Berlin, Heidelberg
Print ISBN: 978-3-642-17471-1
Online ISBN: 978-3-642-17472-8
eBook Packages: Humanities, Social Sciences and LawSocial Sciences (R0)