
Abstract
The drug treatment of Parkinson’s disease (PD) is accompanied by a loss of drug efficacy, the onset of motor complications, lack of effect on non-motor symptoms, and a failure to modify disease progression. As a consequence, novel approaches to therapy are sought, and adenosine A2A receptors (A2AARs) provide a viable target. A2AARs are highly localized to the basal ganglia and specifically to the indirect output pathway, which is highly important in the control of voluntary movement. A2AAR antagonists can modulate γ-aminobutyric acid (GABA) and glutamate release in basal ganglia and other key neurotransmitters that modulate motor activity. In both rodent and primate models of PD, A2AAR antagonists produce alterations in motor behavior, either alone or in combination with dopaminergic drugs, which suggest that they will be effective in the symptomatic treatment of PD. In clinical trials, the A2AAR antagonist istradefylline reduces “off” time in patients with PD receiving optimal dopaminergic therapy. However, these effects have proven difficult to demonstrate on a consistent basis, and further clinical trials are required to establish the clinical utility of this drug class. Based on preclinical studies, A2AAR antagonists may also be neuroprotective and have utility in the treatment of neuropsychiatric disorders. We are only now starting to explore the range of potential uses of A2AAR antagonists in central nervous system disorders, and their full utility is still to be uncovered.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others

Keywords
1 Introduction
Increasing life expectancy will inevitably lead to an increase in the incidence of neurodegenerative illnesses, such as Parkinson’s disease (PD), constituting an increasing social and economic burden (Dorsey et al. 2007). At the same time, the dopaminergic therapies currently used to treat the motor symptoms of PD, while effective in the initial stages of the illness, become inadequate as the disease progresses, do not reverse non-motor symptomatology, and become associated with adverse effects that prove difficult to manage (Fahn and Janlovic 2007; Jankovic 2006). In this situation, drug treatments that act beyond the damaged dopaminergic system, for example adenosine A2A receptor (A2AAR) antagonists, are becoming important targets for the treatment of PD since they may be effective in both the early and late stages of PD and avoid the unwanted side effects currently associated with chronic dopaminergic treatment.
2 Parkinson’s Disease
PD affects 1 in 500 of the general population and 1 in 100 of those individuals aged 60 or over. The incidence of the illness is age related and this remains the only clearly established predisposing factor (Weintraub et al. 2008a). It is characterized by akinesia, rigidity, tremor and postural abnormalities, but increasingly there is awareness that it is a much broader illness that induces a range of non-motor symptoms such as sweating, falling, speech and swallowing difficulties, and neuropsychiatric components such as depression, anxiety and cognitive decline (Chaudhuri et al. 2005). Many of these features can precede the onset of motor symptoms and they, and others, are being actively investigated as early diagnostic features of those individuals that are likely to go on to develop clinical PD (Berg 2006; Siderowf and Stern 2006). The motor symptoms of PD are due primarily to the degeneration of the dopaminergic nigrostriatal pathway, with the mesolimbic/mesocortical dopaminergic pathways remaining relatively intact. However, pathology is widespread, with cell loss also occurring in many other brain areas, such as the locus coeruleus, raphe nuclei, dorsal motor nucleus of the vagus and the ventral forebrain, leading to changes in a range of neurotransmitters, including noradrenaline, 5-hydroxytryptamine (5-HT) and acetylcholine (Agid 1991; Jellinger 2002). Precisely how these contribute to the symptomatology of PD is not known, but they may be the origin of the non-motor features of the illness. Recently, the suggestion was made that PD is a progressive pathological disorder that starts in the periphery and then affects the brain, sweeping from the brainstem through to the cortex and only leading to a diagnosis of PD when the pathological process starts to affect the basal ganglia (BG) (Braak et al. 2006a, b; Braak and Del 2008). Although this is controversial, it implies that treatment strategies should be more broadly based and that pathological change in the BG may be a later feature of PD than previously thought.
PD can be induced by gene defects in rare familial cases, but the bulk of the PD population is considered to have idiopathic disease (Gasser 2007; Hardy et al. 2006). In all probability, it is not a single disorder but a syndrome with multiple causes and with clear differences between, for example, young-onset PD and late-onset illness, and between tremor-dominant and akinetic manifestations. The usual description of PD is that it is due to a combination of genetic and environmental factors that can interact to varying degrees and at different levels (McCulloch et al. 2008). The pathogenic process responsible for neuronal loss in PD remains unknown, but contributing factors are oxidative and nitrative stress, mitochondrial dysfunction, excitotoxicity and altered proteolysis (Jenner and Olanow 2006; Litvan et al. 2007a, b). Cells are presumed to die by apoptosis, but this has not been conclusively demonstrated. There are, however, two key features of PD that probably provide the major clues to the underlying mechanisms. First, pathological change is always accompanied by the appearance of cytoplasmic inclusions, termed Lewy bodies, in surviving neurons (Wakabayashi et al. 2007), and second, there is a reactive microgliosis and to some extent astrocytosis that leads to inflammatory change and that may contribute to the progression of pathology in PD (McGeer and McGeer 2008).
The primary effect of dopaminergic loss in the striatum in PD leads to a disruption of the parallel processing loops between the motor cortex, basal ganglia, thalamus and back to pre-motor and motor cortex that are responsible for the integration of motor, sensory and cognitive information that controls voluntary movement (Obeso et al. 2000, 2004). Dopamine plays three important roles in the striatum that are lost in PD. It controls the activity of the corticostriatal glutamatergic input, it determines the activity of the GABAergic medium spiny neurons that make up the major striatal output pathways—the direct and indirect pathways (see below), and it plays a key role in motor programming through the maintenance of long-term potentiation or long-term depression (LTP/LDP)-type processes (Calabresi et al. 2006, 2007). All of these are key to how dopaminergic therapy reverses the motor symptoms of PD and to how non-dopaminergic drugs, such as adenosine antagonists, can also alter basal ganglia function in PD.
3 Treatment of PD and Limitations of Therapy
The current therapy for PD is based on dopaminergic replacement therapy using 3,4-dihydroxy-l-phenylalanine (l-DOPA) and dopamine agonists, notably ropinirole and pramipexole (Horstink et al. 2006a, b; Weintraub et al. 2008b). These lead to almost complete reversal of motor symptoms in the early stages of the disease, but the dopamine agonists do not possess as great an efficacy as l-DOPA. This may be related to their more selective effects on dopamine receptor subtypes, largely D2∕D3 receptors, and to the fact that l-DOPA stimulates all dopamine receptor populations and also enhances noradrenergic and serotoninergic transmission and can alter glutamate release among a range of actions. Adjuncts to dopaminergic therapy are the other major drug types used in PD. These are the catechol-O-methyl transferase (COMT) inhibitors entacapone and tolcapone, which prevent the metabolism of l-DOPA to 3-O-methyl-DOPA, as well as the monoamine oxidase B (MAO B) inhibitors selegiline and rasagiline, which prevent the breakdown of endogenous dopamine and dopamine derived from l-DOPA. Otherwise, the only other drugs routinely used to treat PD are anticholinergics, which are particularly effective against tremor, or the weak NMDA antagonist amantadine, which has some mild symptomatic actions but is usually employed to suppress dyskinesia (see below).
However, the symptomatic treatment of PD becomes more complex with disease progression and with chronic drug treatment (Fabbrini et al. 2007; Jankovic 2005; Jankovic and Stacy 2007; Stacy and Galbreath 2008; Stocchi 2003). Dopaminergic drugs show a shortening of duration of effect (wearing-off), and the clinical response becomes unpredictable and subject to rapid oscillations, with patients switching rapidly between mobility and immobility (on–off). This can be treated by using a longer-acting dopamine agonist drug or by adding a COMT inhibitor or MAO B inhibitor to therapy, but this is only a short-term measure. A significant proportion of PD patients develop involuntary movements or dyskinesia (chorea, dystonia, athetosis), particularly when treated with l-DOPA. Once established, these are evoked by every dose of dopaminergic medication that is administered. Treatment is usually by dose reduction, but this worsens PD; or by the addition of amantadine, but this is poorly tolerated by many patients; or by the use of continuous drug infusions (subcutaneous apomorphine or intraduodenal l-DOPA); or by referral for deep brain stimulation, employing electrode placement in the subthalamic nucleus (Guridi et al. 2008).
Dopaminergic medications induce a range of acute side effects that further complicate current treatment. These include acute effects such as nausea and vomiting and more prolonged changes in cardiovascular function and in hormonal status. Probably most worrying, however, are the neuropsychiatric complications of dopaminergic treatment usually seen after longer periods of treatment in more advanced patients with PD. Psychosis induced by dopaminergic medication, particularly in elderly patients showing cognitive decline, can become treatment limiting. More recently, dopaminergic dysregulation syndromes, such as compulsive gambling and hypersexuality, have been identified as affecting significant numbers of individuals (Stamey and Jankovic 2008; Stocchi 2005) and leading to legal action that may limit the use of this drug class. All of this leads to the conclusion that new approaches to treatment are required. While dopaminergic medication is highly effective against the motor symptoms of PD, it has little effect on the non-motor components of PD, which are largely non-dopaminergic in origin. Cognitive decline in PD and the high incidence of anxiety and depression require particular attention (Weintraub et al. 2008c). These have become a major problem in treating PD, and novel therapeutic approaches are required.
All current treatment of PD is orientated towards symptomatic therapy. There are no proven treatments that alter the rate of progression of PD. A key objective is to find disease-modifying treatments that stop or slow disease progression. However, neuroprotection is proving a difficult issue, with drugs that look highly effective in preclinical models of PD turning out to be ineffective in clinical trials (Ahlskog 2007; Hung and Schwarzschild 2007; Kieburtz and Ravina 2007; LeWitt 2006; Schapira 2008; Stocchi and Olanow 2003). This has occurred with MAO B inhibitors, glutamate antagonists, inhibitors of apoptotic mechanisms, enhancers of mitochondrial function, trophic factors, and dopamine agonists, amongst others. The reasons for this are not entirely clear, but it may relate to the inappropriateness of the animal models or to the multiple causes of PD and the use of patient populations with different pathogenic mechanisms underlying the origin of their disease.
New approaches to neuroprotection are needed, and clues may be gained by looking at factors that are thought to reduce the risk of developing PD in the human population. Some of the more robust, although still controversial, include cigarette smoking, the use of nonsteroidal anti-inflammatory drugs, antihypertensive agents (notably calcium channel blockers), and caffeine (Becker et al. 2008; Bornebroek et al. 2007; Esposito et al. 2007; Hu et al. 2007; Powers et al. 2008; Ritz et al. 2007). The ability of caffeine to reduce risk may be highly relevant to the potential therapeutic effects of A2AAR antagonists in the treatment of PD.
4 Basal Ganglia Organization
4.1 Localization of A2A ARs in Basal Ganglia
The BG comprise a group of tightly interconnected forebrain nuclei, intercalated among the cerebral cortex, thalamus and brainstem, and mainly involved in motor control and sensorimotor integration. Within the last decade, a number of dedicated studies have extensively shown how dopamine and adenosine interact to modulate motor function at this level (Fuxe et al. 2007; Schwarzschild et al. 2006; Schiffmann et al. 2007).
Adenosine binds at least four different G-protein-coupled receptors, namely A1, A2A, A2B, A3 (Fredholm et al. 1994). In contrast to the widespread distribution of A1, A2B and A3 adenosine receptors in the brain, A2AARs are more selectively distributed, being abundantly expressed in the BG, and reaching the highest levels of expression in the caudate-putamen (CPu) (Rosin et al. 1998; Schiffmann et al. 1991). This selective distribution of A2AARs, involving a potentially low incidence of side effects, first led to the consideration of A2AAR antagonists among the most promising non-dopaminergic agents for the treatment of PD motor symptoms.
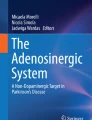
The CPu is mainly composed of medium spiny GABAergic neurons, which are equally divided into two neuronal populations: striatonigral neurons, which connect the CPu with the substantia nigra pars reticulata (SNr) or globus pallidus (GP) internal segment (GPi), otherwise called the entopeduncular nucleus in rodents, and striatopallidal neurons, which connect the CPu with the GP or GPe (globus pallidus external segment) in primates (Fig. 1). Within this system, A2AARs are restricted to GABAergic neurons projecting to the GP which also selectively express the D2 dopamine receptor and the peptide enkephalin (ENK) (Fink et al. 1992; Schiffmann et al. 1991). Conversely, striatonigral neurons, which selectively express the D1 dopamine receptor and the peptide dynorphin (DYN), do not contain appreciable levels of A2AAR. At the molecular level, Gs-coupled A2AARs activate adenylate cyclase, resulting in stimulation of neuronal activity, and opposing the dopamine-mediated inactivation of adenylate cyclase through the Gi-coupled D2 receptor (Fredholm 1995). Recent studies have demonstrated that in striatopallidal neurons the A2AAR can form heteromers with the D2 receptor to attenuate coupling to the signaling pathway of the latter, offering a molecular mechanism of interaction which has compelling implications for PD treatment (Fuxe et al. 2005; Hillion et al. 2002).

Proposed mechanisms of adenosine A2A receptor (A2AAR) antagonist activity in Parkinson’s disease (PD). Mechanisms of symptomatic effects are drawn in black, whereas mechanisms of neuroprotection are drawn in gray. In PD, lack of dopamine (DA) induces hypoactivity of striatonigral D1-containing neurons and hyperactivity of striatopallidal D2-containing neurons, resulting in subthalamus (STN) and substantia nigra pars reticulata (SNr) hyperactivity. Acetylcholine (Ach) interneurons in the caudate-putamen (CPu) are also hyperactive. The final outcome is depressed activity of thalamocortical (Th) projections, which produces characteristic symptoms of akinesia. A2AAR blockade in striatopallidal neurons, and likely in the globus pallidus (GP), relieves their hyperactivity, restoring balance between the output pathways. As a consequence, SNr and Th-cortical neurons become normoactive, relieving the akinesia. Moreover, A2AAR blockade in Ach interneurons restores Ach tone, which may contribute to counteracting tremor. In the parkinsonian state, glial proliferation is present in both the CPu and the substantia nigra pars compacta (SNc). As neuroprotective agents, A2AAR antagonists attenuate dopaminergic cell degeneration through a mechanism that may involve A2AARs located presynaptically or alternatively A2AARs in glial cells
The second most abundant neuronal population within the CPu are the large cholinergic aspiny interneurons, which represent about 5% of the entire population (Gerfen 1992). Striatal cholinergic nerve terminals express A2AARs, which, by modulating the release of acethylcholine in the rat CPu (Fig. 1), represent a novel interesting target for tremor control in PD models (see later).
4.2 Function of A2A ARs in Basal Ganglia
In an intact CPu, adenosine via A2AARs excites striatopallidal neurons, opposing the inhibitory effect exerted by dopamine (Fig. 1). In PD, lack of dopamine generates an imbalance in the activity of striatal output pathways. Striatonigral neurons become hypoactive, whereas striatopallidal neurons, losing the inhibitory effect of dopamine while undergoing the stimulatory influence of adenosine, become hyperactive, boosting their inhibitory influence on GP neurons. Such imbalanced activity leads to a markedly increased inhibitory output from SNr/GPi to thalamocortical neurons, which produces hypokinetic symptoms in PD. Many authors have suggested that the positive effects of A2AAR antagonists in PD rely on the blockade of A2AARs on striatopallidal neurons, which should dampen their excessive activity and restore some balance between striatonigral and striatopallidal neurons, consequently relieving thalamocortical activity. This mechanism offers a rationale for the use of A2AR antagonists as a monotherapy in PD, as well as for the synergistic effect observed upon the concurrent administration of A2AAR antagonists with l-DOPA or dopaminergic agonists, which restore dopamine receptor stimulation (Jenner 2003; Morelli 2003).
Of great interest is the neuronal colocalization and synergistic interaction observed between striatal A2A receptor and metabotropic glutamate subtype 5 (mGlu5), glutamate receptor, which itself represents one of the most promising targets for treatment of PD symptoms (Ferré et al. 2002; Rodrigues et al. 2005). A potentiation of motor activity has been reported upon combined administration of A2A and mGlu5 receptor antagonists, together with a synergistic interaction at the level of signal transduction pathways (Coccurello et al. 2004; Ferré et al.(2002); Kachroo et al. 2005; Nishi et al. 2003). The recent discovery of A2A–mGlu5 heteromers in CPu has further strengthened the rational for studying antiparkinsonian strategies that simultaneously block A2AARs and mGlu5 receptors (Ferré et al. 2002).
4.3 Role of Globus Pallidus A2A Adenosine Receptors
An important function of A2AARs located outside the CPu, particularly in the GP, has been evidenced by the positive effects displayed by A2AAR antagonists when administered in association with dopaminergic therapies. In recent years, several works have led to a reconsideration of the role played by the GP in BG circuits, with this nucleus now placed at a critical functional position to modulate the excitability of afferent (CPu and STN) and efferent (SNr) nuclei (Obeso et al. 2006). The infusion of GABA agonists directly into the GP has been found to severely hamper motor function, whereas the antagonism of pallidal GABAergic transmission results in beneficial motor effects (Hauber 1998). The GP receives a direct dopaminergic innervation, being enriched in D2 dopamine receptors. In the parkinsonian state, in which the GP discharge rate and oscillatory activity are altered, intrapallidal dopaminergic antagonists produce akinesia, whereas dopamine stops this symptom (Galvan et al. 2001; Hauber and Lutz 1999), suggesting that dopamine depletion either directly or indirectly disrupts the modulatory function of GP within the BG. A2AARs are highly expressed in the GP, mainly in the neuropil, where they can regulate pallidal extracellular GABA concentration and, thereafter, GP activity (Rosin et al. 1998; 2003). While stimulation of pallidal A2AARs enhances striatopallidal GABA outflow, their blockade reduces it (Ochi et al. 2004; Shindou et al. 2003). Recently, it was reported that while intrapallidal infusion of A2AAR antagonists in 6-hydroxydopamine (6-OHDA)-lesioned rats does not elicit any motor response per se, it does potentiate motor activity induced by l-DOPA or dopaminergic agonists, suggesting that the beneficial effect exerted by these compounds in PD might also rely on the blockade of pallidal A2AARs (Simola et al. 2006; 2008). It might be hypothesized that in PD, the blockade of pallidal A2AARs, by reducing extracellular GABA, may contribute to restoring GP activity and in turn subthalamic nucleus activity, leading to a more balanced activation of direct and indirect pathways and, when associated with dopaminergic agonists, an enhancement of their motor-stimulating effects.
5 Motor-Behavioral Effects of A2AAR Antagonists in Animal Models of Parkinson’s Disease
5.1 Effects of Acute A2A AR Antagonism on Motor Deficits
The highly enriched distribution of adenosine A2AARs in striatopallidal neurons, and their ability to form functional heteromeric complexes with dopamine D2 and metabotropic glutamate mGlu5 receptors, mean that A2AAR antagonists are of particular interest for the modulation of motor behavior, whilst at the same time they display a low predisposition to induce non-motor side effects.
Research performed to evaluate the effects produced by AR ligands on motor behavior in experimental rodents has provided the first evidence that adenosine is implicated in the modulation of movement. The critical role of A2AAR in the regulation of motor behavior was first highlighted by data showing inhibition of motor behavior by the A2AAR agonist 2-p-[(2-carboxyethyl)-phenethylamino]-5′-N-ethylcarboxamidoadenosine (CGS-21680), while the A2AAR antagonist 7-(2-phenylethyl)-5-amino-2-(2-furyl)-pyrazolo -[4,3-e] -1,2,4-triazolo[1,5-c]pyrimidine (SCH-58261) was found to stimulate motor activity (Morelli et al. 1994; Pollack and Fink 1996; Pinna et al. 1996).
A large number of A2AAR antagonists have been demonstrated to affect motor behavior by reversing catalepsy in rodents (reducing its duration and severity), hence accounting for an improvement in parkinsonian motor deficit by these drugs. Moreover, combined administration of the A2AAR antagonists with l-DOPA has been shown to potentiate the l-DOPA-induced anticataleptic effect, indicating the existence of a synergistic interaction between l-DOPA and A2AAR antagonists (Kanda et al. 1994; Shiozaki et al. 1999; Wardas et al. 2001).
In line with results obtained in the catalepsy protocol, A2AAR antagonists showed motor-facilitatory activity in animals rendered parkinsonian by the administration of dopaminergic neurotoxins, such as 6-OHDA and 1-methyl-4-phenyl-1,2,3,6-tetrahydropyridine (MPTP), which induce the degeneration of nigrostriatal dopaminergic neurons, resulting in models of parkinsonian-like disabilities (akinesia, bradykinesia, etc.) in the animals treated.
Acute administration of the A2AAR agonist CGS 21680 to unilaterally 6-OHDA-lesioned rats has been shown to significantly reduce the turning behavior induced by l-DOPA and either D1 or D2 dopamine receptor agonists (Morelli et al. 1994). Conversely, the A2A receptor antagonist SCH 58261, when administered acutely to 6-OHDA-lesioned rats, has been demonstrated to significantly potentiate turning behavior induced by l-DOPA and either D1 or D2 dopamine receptor agonists (Pinna et al. 1996). An increase in the turning behavior stimulated by l-DOPA or apomorphine was observed following acute A2AAR blockade by 1,3-dipropyl-7-methyl-8-(3,4-dimethoxystyryl)xanthine (KF-17837), 2-butyl-9-methyl-8-(2H-1,2,3-triazol-2-yl)-9H-purin-6-ylamine (ST-1535) or (E)-1,3-diethyl-8-(3,4-dimethoxystyryl)-7-methyl-3,7-dihydro-1H-purine-2,6-dione (KW-6002) (Koga et al. 2000; Rose et al. 2007; Tronci et al. 2007).
Besides turning behavior, subtle aspects of PD symptomatology develop in rats as a consequence of dopamine neuron degeneration, such as forelimb akinesia, gait impairment and sensory-motor integration deficits that are considered analogous to the PD symptoms seen in humans. Acute administration of the A2AAR antagonists SCH-58261 and ST-1535, in a similar manner to l-DOPA although with a lower intensity, counteracted the lesion-induced impairments to the initiation time of the stepping test, to adjusting steps, and to vibrissae-evoked forelimb placing (Pinna et al. 2007). These results suggest that A2AAR antagonists might ameliorate parkinsonian symptoms in PD patients, even when used as a monotherapy.
Most importantly, the efficacy of A2AAR antagonists in MPTP-treated nonhuman primates, provided the impetus for experimentating with these compounds in clinical trials. Acute administration of the A2AAR antagonist KW-6002 counteracted motor impairments and increased locomotor activity in primates previously treated with MPTP (Kanda et al. 1998a, b). Furthermore, a synergistic interaction between A2AAR antagonists and l-DOPA, as well as dopaminergic agonists, in decreasing motor impairment has been observed in MPTP-treated common marmosets (Kanda et al. 2000; Rose et al. 2007).
The crucial role of CPu in the effects of A2AAR antagonists has been confirmed by data indicating that the intrastriatal infusion of the A2AAR antagonist MSX-3 significantly counteracted catalepsy produced by D1 or D2 receptor antagonists (Hauber et al. 2001). However, further to the well-documented role of CPu in mediating motor facilitation produced by A2AAR antagonists, extrastriatal circuits may also be involved in this effect (see Sects. 4.3 and 5.5).
5.2 Efficacy of A2A AR Antagonists in Relieving Parkinsonian Tremor and Muscular Rigidity
To date, tremor and rigidity are devoid of adequate pharmacological treatments, and so preclinical evidence showing that A2AAR antagonists may be effective in relieving rigidity as well as resting tremor, one of the first symptoms manifested in individuals affected by PD, has greatly increased the attention directed towards A2AAR antagonist compounds.
Promising effects of A2AAR antagonists have been observed in rat models of parkinsonian-like muscular rigidity. Haloperidol and reserpine induce a muscular stiffness that displays electromyographic and mechanographic features that partly overlap with those of parkinsonian muscular rigidity. Both effects are attenuated by the administration of the A2AAR antagonist SCH-58261, suggesting the existence of a potential beneficial effect of A2AAR blockade on parkinsonian-like muscular rigidity (Wardas et al. 2001).
Blockade of A2AARs effectively counteracts tremulous jaw movements (TJM), a valuable model for the screening of new antitremorigenic agents in rats. Administration of either the A2AAR antagonist SCH-58261 or ST-1535 has been demonstrated to significantly suppress tacrine-induced TJM and, in line with this finding, antagonism of A2AAR by KF-17837 has been reported to relieve TJM elicited by haloperidol, suggesting a beneficial use of these drugs as specific agents against this parkinsonian symptom (Correa et al. 2004; Mally and Stone 1996; Simola et al. 2004). In addition, intracranial infusion of A2AAR antagonists revealed a critical role of the ventrolateral portion of the CPu in counteracting TJM (Simola et al. 2004). Interestingly, a specific increase in A2AAR mRNA expression in this striatal portion was detected following dopamine denervation in the 6-OHDA model of PD (Pinna et al. 2002).
In order to explain the antitremorigenic effect, it should be noted that striatal cholinergic nerve terminals express A2AARs, and A2AAR antagonists can reduce the evoked release of acethylcoline in rat CPu (Kurokawa et al. 1996), whereas increased acetylcholine transmission, particularly in the ventrolateral portion of CPu, is believed to play an important role in the genesis of TJM in rats (Salamone et al. 1998).
5.3 Effects of Chronic A2A AR Antagonism on Motor Complications and Dyskinesia
In line with data obtained following acute administration, long-term treatment with A2AAR antagonists has been shown to significantly counteract motor disabilities in rodent and nonhuman primate PD models (kanda et al. 1998b; Pinna et al. 2001). Moreover, chronic A2AAR antagonism has been shown not to induce tolerance to motor-stimulant effects in both rats and primates (Halldner et al. 2000; Jenner 2003; Pinna et al. 2001). Lack of tolerance to motor-stimulant effects of A2AAR antagonists is of particular significance in PD, in which the motor-improving properties of therapeutic agents are required to persist during the chronic regimen.
A major finding emerging from studies on chronic A2AAR antagonists is represented by the results reported on motor fluctuations (“wearing off”) and dyskinesia in experimental animals treated with A2AAR antagonists and l-DOPA (Koga et al. 2000). The wearing off of l-DOPA that is observed in humans is mimicked in 6-OHDA-lesioned rats, where the duration of rotational behavior elicited by l-DOPA is progressively reduced during chronic administration. Combined administration of the A2AAR antagonist KW-6002 prevented the shortening of rotational behavior, reflecting a potential beneficial influence of A2AAR blockade on l-DOPA wearing off (Koga et al. 2000). At the same time, sensitization of rotational behavior and development of abnormal involuntary movements (AIMs) is thought to mimic dyskinetic effects elicited by l-DOPA. In this paradigm, interesting results concerning the modulation of dyskinesia by A2AAR blockade have been obtained by comparing the rotational behavior elicited by long-term administration of a higher dose of l-DOPA to an equipotent combination of a lower dose of l-DOPA plus the A2AAR antagonist ST-1535 (Rose et al. 2007; Tronci et al. 2007). Although both l-DOPA (high dose) and l-DOPA (lower dose) plus ST-1535 produced a comparable degree of rotations on the first administration, sensitization of rotational behavior and AIMs were observed only in response to chronic l-DOPA alone, not to chronic l-DOPA plus ST-1535, suggesting that the association between the two drugs represents a treatment with low dyskinetic potential (Tronci et al. 2007). These results have been strengthened by studies showing that genetic deletion of the A2AAR prevents the sensitization of rotational behavior stimulated by l-DOPA in 6-OHDA-lesioned A2AAR knockout (KO) mice (Fredduzzi et al. 2002).
Results obtained in MPTP-treated primates confirm and further extend those deriving from 6-OHDA-lesioned rats. First, A2AAR antagonists do not induce dyskinesia per se, since administration of KW-6002 to parkinsonian primates relieved motor disability without stimulating abnormal movements (Grondin et al. 1999; kanda et al. 1998, 2000). Second, in MPTP-treated marmosets previously exposed to chronic l-DOPA in order to develop dyskinesia, motor stimulation induced by KW-6002 was not associated with an exacerbation of dyskinetic movements (kanda et al. 1998). Furthermore, no sign of apomorphine-induced dyskinesia was observed in parkinsonian cynomolgus monkeys chronically treated with a combination of apomorphine and KW-6002 (Bibbiani et al. 2003). Interestingly, when KW-6002 (but not apomorphine) administration was interrupted, primates previously treated with KW-6002 displayed apomorphine-induced dyskinesia only 10–12 days after KW-6002 discontinuation, thus accounting for a potential preventive effect of A2AAR blockade on the development of dyskinesia (Bibbiani et al. 2003; Morelli 2003). It should be noted, however, that while A2AAR antagonists associated with a low nondyskinetic dosage of l-DOPA may achieve satisfactory results in motor stimulation, whilst at the same time limiting the severity of l-DOPA-induced dyskinesia, no study has yet demonstrated the ability of A2AAR antagonists to revert an already established dyskinesia in animal models.
In this regard, in MPTP-treated common marmosets previously rendered dyskinetic by chronic l-DOPA, it has been shown that the relief of motor impairment produced by an optimal dose of l-DOPA presenting a high dyskinetic potential was adequately mimicked by a combination of KW-6002 plus a suboptimal dose of l-DOPA, which, in contrast, was associated with weak induction of dyskinesia (Bibbiani et al. 2003).
Taken together, data obtained from several preclinical studies indicate the existence of beneficial effects of chronic A2AAR antagonists on PD motor disability and on motor complications produced by long-term l-DOPA. These effects are of considerable interest in light of the fact that motor complications are one of the intrinsic limitations of l-DOPA therapy, and are often insensitive to pharmacological manipulation.
5.4 Effects of Acute and Chronic A2A AR Antagonismon Biochemical Parameters
The study of the effects of A2AAR antagonists on behavioral parameters in both rat and primate models has been paralleled by the analysis of the influence of A2AAR blockade on the biochemical modifications induced by chronic l-DOPA in 6-OHDA lesioned rats in the basal ganglia. Prolonged administration of l-DOPA, according to a regimen capable of inducing a sensitized (dyskinetic-like) rotational response and AIMs, has been shown to modify the expression of the neuropeptides ENK and DYN as well as of the enzyme glutamic acid decarboxylase (GAD67) in the basal ganglia of 6-OHDA-lesioned rats (Carta et al. 2002; Cenci et al. 1998). Although a direct relationship between these biochemical changes and l-DOPA-induced dyskinesia onset has not been unequivocally demonstrated, they have nevertheless been postulated to reflect a more general aberrant functionality of BG produced by long-term l-DOPA, which is thought to underlie the dyskinesia elicited by this drug.
Interestingly, combined administration of low doses of l-DOPA with the A2AAR antagonists SCH-58261 or ST-1535, which (as reported above) induce the same degree of contralateral rotation upon the first administration, did not induce the modifications in the striatal levels of ENK, DYN and GAD67 mRNAs produced by chronic higher doses of l-DOPA in 6-OHDA-lesioned rats (Carta et al. 2002; Tronci et al. 2007).
Moreover, beneficial effects of A2AAR blockade on the regulation of the phosphorylation state of the α-amino-3-hydroxy-5-methyl-4-isoxazolepropionic acid (AMPA) type of glutamate receptor by l-DOPA have been described. Hyperphosphorylation of the striatal AMPA receptor consequent to chronic administration of l-DOPA to 6-OHDA-lesioned rats is in fact prevented by combined administration with KW-6002 (Chase et al. 2003).
In addition to the postulated A2AAR regulatory effects on neuronal responsiveness following prolonged dopaminergic stimuli, it should be considered that A2AAR antagonists, by potentiating the motor effects of l-DOPA or dopamine agonist drugs, allow the use of dopaminomimetic compounds at low nondyskinetic doses. Therefore, the sparing of these agents produced by combined administration with A2AAR antagonists might contribute towards reducing, or at least delaying, the onset of neuroplastic modifications in BG.
5.5 Biochemical Changes in Extrastriatal Basal Ganglia Areas
In the context described above, the increase in GAD67 mRNA in the GP of 6-OHDA-lesioned rats treated subchronically with l-DOPA (full effective dose) but not with SCH-58261 plus l-DOPA (threshold dose) is particularly important, indicating that chronic l-DOPA—but not an equally effective combination of SCH-58261 plus l-DOPA—elicits abnormal modifications of GP neuronal activity (Carta et al. 2003).
Moreover, subchronic studies have shown that, while a fully effective dose of l-DOPA reduces the 6-OHDA lesion-induced increase in GAD67 mRNA in SNr, it simultaneously reduces GAD67 mRNA values to below the levels present on the intact side, producing an excessive inhibition of SNr efferent neurons (Carta et al. 2003). In contrast, the combined subchronic administration of SCH-58261 plus l-DOPA reduces GAD67 mRNA to a lesser extent, decreasing GAD67 mRNA to levels similar to those present on the intact nonlesioned side (Carta et al. 2003). Excessive inhibition of SNr in rodents and GP internal segment in primates, together with an altered firing pattern, is correlated with the onset of dyskinetic movements after l-DOPA (Boraud et al. 2001; Papa et al. 1999). Thus, the ability of subchronic SCH-58261 plus l-DOPA to produce a decrease in GAD67 mRNA values to levels similar to those present in nonlesioned SNr may correlate with the presence of contralateral turning (index of therapeutic response) and to the failure to produce sensitization in contralateral turning (index of dyskinetic movements).
The results of those studies underline the importance of the role played by the indirect CPu-GP-STN-SNr pathway in eliciting the therapeutic response of A2AAR receptor antagonists, and its involvement in abnormal motor responses produced by subchronic l-DOPA.
6 Clinical Actions of Adenosine A2AAR Antagonists
The anatomic localization of A2AARs and their biochemical and pharmacological properties suggest that modulation of striatal GABAergic output will modify motor function in PD, and that this should occur with no risk of the development or expression of dyskinesia (Kase et al. 2003). The activity of A2AARs in functional models of PD also points to actions of the A2AAR antagonists as monotherapy and as adjuncts to l-DOPA and dopamine agonists. Only one A2AAR antagonist has undergone detailed clinical evaluation so far: istradefylline (KW-6002).
In healthy subjects, istradefylline (40, 60, 80 and 160 mg per day for 14 days) showed dose-proportional increases in the area under the curve (AUC) and a C max with a half-life (t 1 ∕ 2) of 67–95 h, suggesting that once-daily dosing should be effective (Rao et al. 2005a). Similar studies in patients with PD showed that istradefylline (60 and 80 mg per day for 14 days) also exhibits a dose-proportional pharmacokinetic profile (Rao et al. 2005b). The occupation of striatal A2AARs by istradefylline was shown using 11C-istradefylline as a ligand for PET investigations in healthy subjects (Brooks et al. 2008). These studies showed > 90% occupation of A2AARs at doses of istradefylline exceeding 5 mg, while this decreased proportionally at lower doses. From these studies, it was concluded that 20 or 40 mg per day istradefylline would provide consistent A2AAR occupation, and that this would be an appropriate dosage for subsequent clinical investigations.
Some early clinical efficacy studies to establish proof of concept in patients with PD took place prior to the completion of the PET A2AAR imaging investigations, and so these studies utilized higher doses. These involved studies of the effects of istradefylline (40 or 80 mg per day over four weeks) alone or in combination with subsequent steady-state intravenous infusions of l-DOPA using an optimal or low infusion rate (Bara-Jimenez et al. 2003). Perhaps surprisingly, istradefylline alone had no effect on motor disability. This finding contrasts with the mild symptomatic effects of istradephylline seen in MPTP-treated primates, but is more consistent with the absence of significant rotation in 6-OHDA-lesioned rats. The data suggest that the drug would not be effective as monotherapy in the treatment of PD, but there is only one recent report on the efficacy of istradefylline as sustained monotherapy, which was inconclusive (Fernandez et al. 2008).
The results of the effects of istradefylline in conjunction with l-DOPA infusions gave the first indication of the clinical actions of the effect of A2AAR receptor occupation. Istradefylline in conjunction with an optimal l-DOPA infusion had no effect on the severity of motor deficits (Bara-Jimenez et al. 2003). However, when combined with a low dose of l-DOPA, istradefylline (80 mg per day) potentiated the improvement in motor function by 36% while dyskinesia was unchanged. All primary motor symptoms of PD were improved by the addition of istradefylline. Istradefylline also increased the duration of efficacy of l-DOPA by 76%, as judged by the length of time patients remained mobile (“on” time) following cessation of l-DOPA infusion.
These findings are interesting, as they strongly support the results of the preclinical investigations in 6-OHDA-lesioned rats and in MPTP-treated primates, which showed that istradefylline potentiated the effects of low-threshold doses of l-DOPA but that little effect was seen when combined with high effective doses of the drug. The implication is that the optimal clinical effects would therefore be observed under similar conditions, but, as will be seen, the major clinical trials were undertaken in patients receiving optimal administration of dopaminergic therapy for regulatory reasons related to the need to demonstrate efficacy as a decrease in the length of time patients were immobile during the waking day (“off” time) in a group not adequately controlled by currently available medication.
In a 12-week exploratory study of safety and efficacy in advanced PD patients receiving l-DOPA therapy and other dopaminergic agents with both motor fluctuations and peak dose dyskinesia, istradefylline (up to 20 or 40 mg per day) reduced off time by 1.2 h during the waking day in the later stages of the study, as assessed using a home diary, although no change in the unified Parkinson’s disease rating scale (UPDRS) scores for motor function or clinical global impression (CGI) of improvement in parkinsonian symptoms was found (Hauser et al. 2003; Hauser and Schwarzschild 2005). This is similar to the reductions produced by the COMT inhibitor entacapone when added to l-DOPA therapy. No overall increase in dyskinesia was observed, but perhaps surprisingly based on the preclinical findings, there was an increase in the amount of on time during which dyskinesia occurred. The overall success of this study then paved the way for a series of longer-term clinical investigations in larger patient populations.
These studies have largely confirmed the effects seen in the initial investigations with istradefylline. In a double-blind multicenter study, in PD patients with prominent end-of-dose wearing off, istradefylline (40 mg per day) reduced off time during the waking day by 1.2 h compared to placebo (LeWitt et al. 2004, 2008; Stacy et al. 2004). There was no increase in dyskinesia that was disabling to the patient, but on time with dyskinesia was increased as a result of an increase in mild dyskinesia that was not troublesome to the patient and did not impair mobility. This was not unexpected on the basis of the earlier clinical studies, but it does conflict with the preclinical data on dyskinesia in MPTP-treated primates, although these studies were largely carried out using low doses of l-DOPA. In another study of istradefylline in PD patients with motor complications using 20 or 60 mg per day istradefylline versus placebo, almost identical findings were obtained except that the decreases in off time were 0.64 and 0.72 h, respectively, for the 20 and 60 mg per day doses, respectively (LeWitt et al. 2004; Stacy et al. 2004, 2008). A long-term open-label efficacy study lasting 52 weeks in advanced-stage PD patients who had previously completed a double-blind placebo-controlled investigation showed that the efficacy of the drug in reducing off time in doses of between 20 and 60 mg per day was maintained in patients who were already taking the drug at the start of the study (Mark et al. 2005). In those patients from the placebo arm of the previous double-blind study who started istradefylline, or those who had been off the drug for more than two weeks and were restarted on the drug, off time was reduced after two weeks and then maintained. The findings of these studies have more or less set the scene for the clinical effects of this A2AAR antagonist in advanced PD patient populations.
However, problems have recently been encountered relating to the efficacy of istradefylline in other Phase III clinical studies, which are probably due to the problem of large and maintained placebo effects in PD and the modest duration of the decrease in off time seen throughout the clinical development. In patients with advanced PD exhibiting motor fluctuations, as defined by an average of at least 3 h off time, 20 mg per day istradefylline reduced the off times at two and four weeks but not at eight or twelve weeks (Hauser et al. 2006, 2008; Shulman et al. 2006; Trugman et al. 2006), although the effect was significant at the end-point (determined by the last observation carried forward, LOCF), with a 0.73 h reduction in off time. An analysis of secondary end-points showed a reduction in UPDRS Part 3 for motor symptoms at four weeks, a trend at two and eight weeks, and no effect at twelve weeks. Similarly, in patients with PD showing motor complications that were not adequately controlled by l-DOPA, istradefylline (10, 20 or 40 mg per day) did not decrease off time compared to a larger than expected placebo effect, although a trend for the improvement in response to increase with increasing istradefylline dosage (a dose-ordered response) was observed between the istradefylline-treated groups (Guttman et al. 2006; Pourcher et al. 2006). The results from these studies have led the FDA to issue a nonapprovable letter for the use of istradefylline in late-stage PD.
Since istradefylline is the only A2AAR antagonist with results from clinical trials for PD reported to date, it is difficult to know whether the profile seen with this drug is typical of this class of drugs, or whether the design of the clinical trials in line with regulatory end-points will provide further insights into the efficacy of this class of drugs for PD. A number of other A2AAR antagonists are in clinical trials at this time, such as V2006 and SCH-58261, and the results of these studies are eagerly awaited. Based on its preclinical profile, istradefylline would have been expected to have some modest symptomatic effects as a monotherapy, but this needs further investigation. Moreover, based on preclinical investigations, istradefylline should produce an additive effect with l-DOPA, but perhaps the necessity of undertaking the clinical studies in patients on optimal dopaminergic medication has masked its ability to potentiate the effects of low-threshold doses of l-DOPA, an effect that was clearly demonstrated in preclinical studies. Thus, the design of clinical trials for istradefylline with this in mind may have provided a different outcome.
7 Future Directions
7.1 Effects on Cognition
Clinical evidence demonstrates the occurrence of cognitive impairments irrespective of motor disability in parkinsonian patients, including both overt dementia during later stages of the disease and less marked deficits displayed by the majority of subjects during the early stages. PD-associated cognitive symptoms involve abnormalities in visuospatial performance and memory deficits, with both short- and long-term memory being affected. Alterations in organization, planning, regulation of goal-directed behaviors and information retrieval and attention are widely observed in PD patients and are key events triggering the manifestations of PD-associated cognitive decline (Apollonio et al. 1994).
l-DOPA has been found to exert contradictory effects, if any, on cognitive deficits in PD, improving several symptoms whilst worsening others. Thus, the development of new therapeutic options currently constitutes an important requirement in the treatment of cognitive decline observed in PD, and A2AAR antagonists may represent a valid option. Several data obtained in experimental animals have evidenced how counteracting A2AAR-mediated signaling by drugs or genetic deletion of the gene encoding for the A2AAR may significantly improve cognitive functions, whereas working memory deficits have been demonstrated in rats overexpressing the A2AAR (Giménez-Llort et al. 2007; Wang et al. 2006). Moreover, studies employing the A2AAR antagonists KW-6002 and SCH-412348 have revealed how A2AAR blockade exerts beneficial effects on cognition-related functions other than memory, enhancing both motivation and attention, facilitating reward-related behaviors, increasing motor readiness, and speeding up motor-preparatory responses (O’Neill and Brown 2006; Takahashi et al. 2008).
Several authors have hypothesized how a defective functionality of the frontostriatal dopaminergic circuit connecting the CPu to the frontal cortex contributes towards cognitive deficits associated with PD (Gao and Goldman-Rakic 2003; Kulisevsky et al. 2000). A2AARs are particularly abundant in the CPu, and are also (although to a lesser extent) expressed in the frontal cortex (Rosin et al. 2003). Hence, by facilitating dopamine receptor-mediated effects, A2AAR antagonists may boost neurotransmission at the level of the frontostriatal circuit, eventually exerting a positive influence on parkinsonian cognitive deficits. Moreover, in addition to the modulation of dopaminergic transmission by A2AARs, cholinergic system functioning may also be affected. Interestingly, the A2AAR antagonist SCH-58261 has been found to increase acetylcholine release in rat frontal cortex (Acquas et al. 2002). The latter finding may be potentially relevant to the treatment of cognitive deficits in PD, suggesting the potential ability of A2AAR antagonism to modify hypofunctionality of the frontal cortex cholinergic system, implicated to some extent in cognitive decline in PD, an effect which may contribute towards improving this specific symptom of PD. These results do not exclude a potential role of adenosine A1 receptor in contrasting cognitive decline in PD (Mihara et al. 2007).
7.2 Neuroprotective Potential
One of the major limitations of the current pharmacological treatment of PD is represented by its substantial ineffectiveness in counteracting the degeneration of dopaminergic neurons, which underlies this condition. In this regard, it has recently been emphasized that the blockade of adenosine A2AARs may potentially represent a valuable approach in counteracting neuronal death in PD (Chen et al. 2007).
Neuroprotective effects have been obtained in different PD animal models by drug administration or in A2AAR KO mice. In the MPTP mouse model, blockade of A2AARs by either SCH-58261 or KW-6002 or deletion of the gene encoding for the A2AAR has been shown to substantially reduce both the demise of dopaminergic nigral neurons and the fall in striatal dopamine concentration elicited by MPTP administration (Chen et al. 2001; Ikeda et al. 2002; Pierri et al. 2005).
Despite the fact that neuroprotection elicited by A2AAR antagonists in PD animal models is clearly manifested, the neuronal mechanisms underlying this effect have not yet been ascertained, although they would seem to differ from those mediating the motor-stimulating effects of these agents.
An abnormal increase in glutamate outflow may be implicated in triggering the demise of dopaminergic neurons observed in PD, and so an involvement of glutamate in A2AAR blockade-mediated neuroprotection has been suggested, since A2AARs located presynaptically on glutamatergic terminals control glutamate release in a negative way (Cunha 2001; Popoli et al. 2002). It should nevertheless be taken into account that mechanisms other than that regulating glutamate release may be involved in the neuroprotection mediated by A2AAR blockade, in view of the modulation by A2AARs of a large number of brain functions. The ability of A2AARs to modulate the activity of non-neuronal cell types (e.g., microglia or astroglia) is of particular interest to this regard, in view of the crucial role played by glia-mediated neuroinflammation in PD. Therefore, interference with glial-released neurotoxic factors might confer protective properties on these agents as well, leading to the compelling possibility that a unique broad mechanism might subserve A2AAR-mediated neuroprotection in diverse neurodegenerative pathologies (Kust et al. 1999; Nishizaki et al. 2002).
To date no clinical studies have been carried out to investigate potential neuroprotective effects on the dopaminergic system following the administration of A2AAR antagonists. However, epidemiological studies have demonstrated how the incidence of idiopathic PD negatively correlates with caffeine intake, being significantly lower in individuals that regularly consume caffeine throughout their lifetime (Ascherio et al. 2001).
Therefore, direct evidence of neuroprotection mediated by A2AAR antagonists in experimental animals, as well as data from epidemiological studies, provide new insights into the study of the antiparkinsonian potential of these drugs. It can therefore be postulated that A2AAR antagonists may not only relieve motor deficits in established PD but may also potentially prevent the the pathology from progressing by arresting the degeneration of dopaminergic mesencephalic neurons.
8 Conclusions
Although the neuroprotective and symptomatic effects of A2AAR antagonists on parkinsonian neuronal demise appear to be most promising, it should be noted that (i) by acting on A2A ARs to produce vasodilation, adenosine affects oxygen supply:demand, (ii) by acting on A2AARs on inflammatory cells, adenosine produces anti-inflammatory responses, and (iii) by acting on A2AARs on endothelial cells, adenosine decreases endothelial permeability. Therefore, blockade of A2AARs may produce adverse effects in regions other than the brain, such as the heart, kidney, lung and inflammatory responses in general. For more information on A2AARs in other organs, please refer to other chapters in this volume, such as those focusing on adenosine receptors and the kidney (Chap. 15), heart (Chaps. 6 and 7), asthma (Chap. 11), and inflammation (Chap. 8). As a consequence, more detailed studies should be undertaken in the future in both experimental animals and humans to clarify whether (and under which specific conditions) A2AAR antagonists may be used as safe and effective agents in the treatment of PD.
Abbreviations
- AIMs:
-
Abnormal involuntary movements
- A2AAR:
-
Adenosine A2A receptor
- AUC:
-
Area under the curve
- AMPA:
-
Alpha-amino-3-hydroxy-5-methyl-4-isoxazolepropionic acid
- BG:
-
Basal ganglia
- COMT:
-
Catechol-O-methyl transferase
- CPu:
-
Caudate-putamen
- CGI:
-
Clinical global impression
- DA:
-
Dopamine
- DYN:
-
Dynorphin
- ENK:
-
Enkephalin
- GABA:
-
γ-Aminobutyric acid
- GAD67:
-
Glutamic acid decarboxylase
- GP:
-
Globus pallidus
- GPe:
-
Globus pallidus, external segment
- GPi:
-
Globus pallidus, internal segment
- 5-HT:
-
5-Hydroxytryptamine
- LOCF:
-
Last observation carried forward
- KO:
-
Knockout
- l-DOPA:
-
3,4-Dihydroxy-l-phenylalanine
- LTP/LDP:
-
Long-term potentiation/long-term depression
- mGlu5:
-
Metabotropic glutamate subtype 5
- MAO B:
-
Monoamine oxidase B
- 6-OHDA:
-
6-Hydroxydopamine
- MPTP:
-
1-Methyl-4-phenyl-1,2,3,6-tetrahydropyridine
- PD:
-
Parkinson’s disease
- STN:
-
Subthalamus
- SNr:
-
Substantia nigra pars reticulata
- TJM:
-
Tremulous jaw movement
- UPDRS:
-
Unified Parkinson’s disease rating scale
References
Acquas E, Tanda G, Di Chiara G (2002) Differential effects of caffeine on dopamine and acetylcholine transmission in brain areas of drug-naive and caffeine-pretreated rats. Neuropsychopharmacology 27:182–193
Agid Y (1991) Parkinson’s disease: pathophysiology. Lancet 337:1321–1324
Ahlskog JE (2007) I can’t get no satisfaction: still no neuroprotection for Parkinson disease. Neurology 69:1476–1477
Appollonio I, Grafman J, Clark K, Nichelli P, Zeffiro T, Hallett M (1994) Implicit and explicit memory in patients with Parkinson’s disease with and without dementia. Arch Neurol 51:359–367
Ascherio A, Zhang SM, Hernán MA, Kawachi I, Colditz GA, Speizer FE, Willett WC (2001) Prospective study of caffeine consumption and risk of Parkinson’s disease in men and women. Ann Neurol 50:56–63
Bara-Jimenez W, Sherzai A, Dimitrova T, Favit A, Bibbiani F, Gillespie M, Morris MJ, Mouradian MM, Chase TN (2003) Adenosine A(2A) receptor antagonist treatment of Parkinson’s disease. Neurology 61:293–296
Becker C, Jick SS, Meier CR (2008) Use of antihypertensives and the risk of Parkinson disease. Neurology 70:1438–1444
Berg D (2006) Marker for a preclinical diagnosis of Parkinson’s disease as a basis for neuroprotection. J Neural Transm Suppl:123–132
Bibbiani F, Oh JD, Petzer JP, Castagnoli N Jr, Chen JF, Schwarzschild MA (2003) A2A antagonist prevents dopamine agonist-induced motor complications in animal models of Parkinson’s disease. Exp Neurol 184:285–294
Boraud T, Bezard E, Bioulac B, Gross CE (2001) Dopamine agonist-induced dyskinesias are correlated to both firing pattern and frequency alterations of pallidal neurones in the MPTP-treated monkey. Brain 124:546–557
Bornebroek M, de Lau LM, Haag MD, Koudstaal PJ, Hofman A, Stricker BH, Breteler MM (2007) Nonsteroidal anti-inflammatory drugs and the risk of Parkinson disease. Neuroepidemiology 28:193–196
Braak H, Bohl JR, Muller CM, Rub U, de Vos RA, Del TK (2006a) Stanley Fahn Lecture 2005: the staging procedure for the inclusion body pathology associated with sporadic Parkinson’s disease reconsidered. Mov Disord 21:2042–2051
Braak H, Muller CM, Rub U, Ackermann H, Bratzke H, de Vos RA, Del TK (2006b) Pathology associated with sporadic Parkinson’s disease: where does it end? J Neural Transm Suppl 89–97
Braak H, Del TK (2008) Invited article: Nervous system pathology in sporadic Parkinson disease. Neurology 70:1916–1925
Brooks DJ, Doder M, Osman S, Luthra SK, Gunn R, Hirani E, Hume S, Kase H, Kilborn J, Martindill S, Mori A (2008) Positron emission tomography analysis of [11C]KW-6002 binding to human and rat adenosine A2A receptors in the brain. Synapse 62:671–681
Calabresi P, Picconi B, Parnetti L, Di FM (2006) A convergent model for cognitive dysfunctions in Parkinson’s disease: the critical dopamine–acetylcholine synaptic balance. Lancet Neurol 5:974–983
Calabresi P, Picconi B, Tozzi A, Di FM (2007) Dopamine-mediated regulation of corticostriatal synaptic plasticity. Trends Neurosci 30:211–219
Carta AR, Pinna A, Cauli O, Morelli M (2002) Differential regulation of GAD67, enkephalin and dynorphin mRNAs by chronic-intermittent L-dopa and A2A receptor blockade plus L-dopa in dopamine-denervated rats. Synapse 44:166–174
Carta AR, Tabrizi MA, Baraldi PG, Pinna A, Pala P, Morelli M (2003) Blockade of A2A receptors plus L-DOPA after nigrostriatal lesion results in GAD67 mRNA changes different from L-DOPA alone in the rat globus pallidus and substantia nigra reticulata. Exp Neurol 184:679–87
Cenci MA, Lee CS, Bjorklund A (1998) L-DOPA-induced dyskinesia in the rat is associated with striatal overexpression of prodynorphin- and glutamic acid decarboxylase mRNA. Eur J Neurosci 10:2694–706
Chase TN, Bibbiani F, Bara-Jimenez W, Dimitrova T, Oh-Lee JD (2003) Translating A2A antagonist KW6002 from animal models to parkinsonian patients. Neurology 61:S107–11
Chaudhuri KR, Yates L, Martinez-Martin P (2005) The non-motor symptom complex of Parkinson’s disease: a comprehensive assessment is essential. Curr Neurol Neurosci Rep 5:275–283
Chen JF, Xu K, Petzer JP, Staal R, Xu YH, Beilstein M, Sonsalla PK, Castagnoli K, Castagnoli N Jr, Schwarzschild MA (2001) Neuroprotection by caffeine and A(2A) adenosine receptor inactivation in a model of Parkinson’s disease. J Neurosci 21:RC143
Chen JF, Sonsalla PK, Pedata F, Melani A, Domenici MR, Popoli P, Geiger J, Lopes LV, de Mendonça A (2007) Adenosine A2A receptors and brain injury: broad spectrum of neuroprotection, multifaceted actions and fine tuning modulation. Prog Neurobiol 83:310–331
Coccurello R, Breysse N, Amalric M (2004) Simultaneous blockade of adenosine A2A and metabotropic glutamate mGlu5 receptors increase their efficacy in reversing Parkinsonian deficits in rats. Neuropsychopharmacology 29:1451–61
Correa M, Wisniecki A, Betz A, Dobson DR, O’Neil MF, O’Neil MJ, Salamone JD (2004) The adenosine A2A antagonist KF17837 reverses the locomotor suppression and tremulous jaw movements induced by haloperidol in rats: possible relevance to parkinsonism. Behav Brain Res 148:47–54
Cunha RA (2001) Adenosine as a neuromodulator and as a homeostatic regulator in the nervous system: different roles, different sources and different receptors. Neurochem Int 38:107–125
Dorsey ER, Constantinescu R, Thompson JP, Biglan KM, Holloway RG, Kieburtz K, Marshall FJ, Ravina BM, Schifitto G, Siderowf A, Tanner CM (2007) Projected number of people with Parkinson disease in the most populous nations, 2005 through 2030. Neurology 68:384–386
Esposito E, Di MV, Benigno A, Pierucci M, Crescimanno G, Di GG (2007) Non-steroidal anti-inflammatory drugs in Parkinson’s disease. Exp Neurol 205:295–312
Fabbrini G, Brotchie JM, Grandas F, Nomoto M, Goetz CG (2007) Levodopa-induced dyskinesias. Mov Disord 22:1379–1389
Fahn S, Jankovic J (2007) Principles and practice of movement disorders. Elsevier, Philadelphia, pp 1–652
Fernandez HH, 6002-US-051 Clinical Investigator Group (2008) The safety and efficacy of istradephylline, an adenosine A2A antagonist, as monotherapy in Parkinson’s Disease: results of the KW-6002-US-051 trial. Presented at the 12th International Congress of Parkinson’s Disease and Movement Disorders, Chicago. Mov Disord 23(Suppl 1):S87
Ferré S, Karcz-Kubicha M, Hope BT, Popoli P, Burgueño J, Gutiérrez MA, Casadó V, Fuxe K, Goldberg SR, Lluis C, Franco R, Ciruela F (2002) Synergistic interaction between adenosine A2A and glutamate mGlu5 receptors: implications for striatal neuronal function. Proc Natl Acad Sci USA 99:11940–11945
Fink JS, Weaver DR, Rivkees SA, Peterfreund RA, Pollack AE, Adler EM, Reppert SM (1992) Molecular cloning of the rat A2 adenosine receptor: selective co-expression with D2 dopamine receptors in rat striatum. Brain Res Mol Brain Res 14:186–195
Fredduzzi S, Moratalla R, Monopoli A, Cuellar B, Xu K, Ongini E (2002) Persistent behavioral sensitization to chronic L-DOPA requires A2A adenosine receptors. J Neurosci 22:1054–1062
Fredholm BB (1995) Purinoceptors in the nervous system. Pharmacol Toxicol 76:228–239
Fredholm BB, Abbracchio MP, Burnstock G, Daly JW, Harden TK, Jacobson KA, Leff P, Williams M (1994) Nomenclature and classification of purinoceptors. Pharmacol Rev 46:143–156
Fuxe K, Ferré S, Canals M, Torvinen M, Terasmaa A, Marcellino D, Goldberg SR, Staines W, Jacobsen KX, Lluis C, Woods AS, Agnati LF, Franco R (2005) Adenosine A2A and dopamine D2 heteromeric receptor complexes and their function. J Mol Neurosci 26:209–220
Fuxe K, Marcellino D, Genedani S, Agnati L (2007) Adenosine A(2A) receptors, dopamine D(2) receptors and their interactions in Parkinson’s disease. Mov Disord 22:1990–1917
Galvan A, Floran B, Erlij D, Aceves J (2001) Intrapallidal dopamine restores motor deficits induced by 6-hydroxydopamine in the rat. J Neural Transm 108:153–166
Gao WJ, Goldman-Rakic PS (2003) Selective modulation of excitatory and inhibitory microcircuits by dopamine. Proc Natl Acad Sci USA 100:2836–2841
Gasser T (2007) Update on the genetics of Parkinson’s disease. Mov Disord 22(Suppl 17):S343–S350
Gerfen CR (1992) The neostriatal mosaic: multiple levels of compartmental organization. Trends Neurosci 15:133–139
Giménez-Llort L, Schiffmann SN, Shmidt T, Canela L, Camón L, Wassholm M, Canals M, Terasmaa A, Fernández-Teruel A, Tobeña A, Popova E, Ferré S, Agnati L, Ciruela F, Martínez E, Scheel-Kruger J, Lluis C, Franco R, Fuxe K, Bader M (2007) Working memory deficits in transgenic rats overexpressing human adenosine A2A receptors in the brain. Neurobiol Learn Mem 87:42–56
Grondin R, Bedard PJ, Hadj Tahar A, Gregoire L, Mori A, Kase H (1999) Antiparkinsonian effect of a new selective adenosine A2A receptor antagonist in MPTP-treated monkeys. Neurology 52:1673–1677
Guridi J, Obeso JA, Rodriguez-Oroz MC, Lozano AA, Manrique M (2008) L-Dopa-induced dyskinesia and stereotactic surgery for Parkinson’s disease. Neurosurgery 62:311–23
Guttman M, 6002-US-018 Clinical Investigator Group (2006) Efficacy of istradephylline in Parkinson’s disease patients treated with levodopa with motor response complications: results of the KW-6002-US-018 study. Presented at the 10th International Congress of Parkinson’s Disease and Movement Disorders, Kyoto. Mov Disord 21(Suppl. 15):S585
Halldner L, Lozza G, Lindström K, Fredholm BB (2000) Lack of tolerance to motor stimulant effects of a selective adenosine A(2A) receptor antagonist. Eur J Pharmacol 406:345–354
Hardy J, Cai H, Cookson MR, Gwinn-Hardy K, Singleton A (2006) Genetics of Parkinson’s disease and parkinsonism. Ann Neurol 60:389–398
Hauber W (1998) Involvement of basal ganglia transmitter systems in movement initiation. Prog Neurobiol 56:507–540
Hauber W, Lutz S (1999) Dopamine D1 or D2 receptor blockade in the globus pallidus produces akinesia in the rat. Behav Brain Res 106:143–150
Hauber W, Neuscheler P, Nagel J, Muller CE (2001) Catalepsy induced by a blockade of dopamine D1 or D2 receptors was reversed by a concomitant blockade of adenosine A(2A) receptors in the caudate-putamen of rats. Eur J Neurosci 14:1287–93
Hauser RA, Hubble JP, Truong DD (2003) Randomized trial of the adenosine A(2A) receptor antagonist istradefylline in advanced PD. Neurology 61:297–303
Hauser RA, Schwarzschild MA (2005). Adenosine A2A receptor antagonists for Parkinson’s disease: rationale, therapeutic potential and clinical experience. Drugs Aging 22:471–482
Hauser R, 6002-US-013 Clinical Investigator Group (2006) Effects of istradephylline (KW-6002) in levodopa treated Parkinson’s disease patients with motor response complications: secondary efficacy results of the KW-6002-US-013 study. Presented at the 10th International Congress of Parkinson’s Disease and Movement Disorders, Kyoto. Mov Disord 21(Suppl 15):S510
Hauser RA, Shulman LM, Trugman JM, Roberts J, Mori A, Ballerini R, Sussman NM (2008) Study of istradefylline in patients with Parkinson’s disease on levodopa with motor fluctuations. Mov Disord 23:2177–2185
Hillion J, Canals M, Torvinen M, Casado V, Scott R, Terasmaa A, Hansson A, Watson S, Olah ME, Mallol J, Canela EI, Zoli M, Agnati LF, Ibanez CF, Lluis C, Franco R, Ferre S, Fuxe K (2002) Coaggregation, cointernalization, and codesensitization of adenosine A2A receptors and dopamine D2 receptors. J Biol Chem 277:18091–18097
Horstink M, Tolosa E, Bonuccelli U, Deuschl G, Friedman A, Kanovsky P, Larsen JP, Lees A, Oertel W, Poewe W, Rascol O, Sampaio C (2006a) Review of the therapeutic management of Parkinson’s disease. Report of a joint task force of the European Federation of Neurological Societies and the Movement Disorder Society–European Section. Part I: early (uncomplicated) Parkinson’s disease. Eur J Neurol 13:1170–1185
Horstink M, Tolosa E, Bonuccelli U, Deuschl G, Friedman A, Kanovsky P, Larsen JP, Lees A, Oertel W, Poewe W, Rascol O, Sampaio C (2006b) Review of the therapeutic management of Parkinson’s disease. Report of a joint task force of the European Federation of Neurological Societies (EFNS) and the Movement Disorder Society–European Section (MDS-ES). Part II: late (complicated) Parkinson’s disease. Eur J Neurol 13:1186–1202
Hu G, Bidel S, Jousilahti P, Antikainen R, Tuomilehto J (2007) Coffee and tea consumption and the risk of Parkinson’s disease. Mov Disord 22:2242–2248
Hung AY, Schwarzschild MA (2007) Clinical trials for neuroprotection in Parkinson’s disease: overcoming angst and futility? Curr Opin Neurol 20:477–483
Ikeda K, Kurokawa M, Aoyama S, Kuwana Y (2002) Neuroprotection by adenosine A2A receptor blockade in experimental models of Parkinson’s disease. J Neurochem 80:262–270
Jankovic J (2005) Motor fluctuations and dyskinesias in Parkinson’s disease: clinical manifestations. Mov Disord 20(Suppl 11):S11–S16
Jankovic J (2006) An update on the treatment of Parkinson’s disease. Mt Sinai J Med 73:682–689
Jankovic J, Stacy M (2007) Medical management of levodopa-associated motor complications in patients with Parkinson’s disease. CNS Drugs 21:677–692
Jellinger KA (2002) Recent developments in the pathology of Parkinson’s disease. J Neural Transm Suppl 347–376
Jenner P (2003) A2A antagonists as novel non-dopaminergic therapy for motor dysfunction in PD. Neurology 61:S32–S38
Jenner P, Olanow CW (2006) The pathogenesis of cell death in Parkinson’s disease. Neurology 66:S24–S36
Kachroo A, Orlando LR, Grandy DK, Chen JF, Young AB, Schwarzschild MA (2005) Interactions between metabotropic glutamate 5 and adenosine A2A receptors in normal and parkinsonian mice. J Neurosci 25:10414–19
Kanda T, Shiozaki S, Shimada J, Suzuki F, Nakamura J (1994) KF17837: a novel selective adenosine A2A receptor antagonist with anticataleptic activity. Eur J Pharmacol 256:263–268
Kanda T, Tashiro T, Kuwana Y, Jenner P. (1998a) Adenosine A2A receptors modify motor function in MPTP-treated common marmosets. Neuroreport 9:2857–2860
Kanda T, Jackson MJ, Smith LA, Pearce RK, Nakamura J, Kase H, Kuwana Y, Jenner P (1998b) Adenosine A2A antagonist: a novel antiparkinsonian agent that does not provoke dyskinesia in parkinsonian monkeys. Ann Neurol 43:507–513
Kanda T, Jackson MJ, Smith LA, Pearce RK, Nakamura J, Kase H (2000) Combined use of the adenosine A(2A) antagonist KW-6002 with L-DOPA or with selective D1 or D2 dopamine agonists increases antiparkinsonian activity but not dyskinesia in MPTP-treated monkeys. Exp Neurol 162:321–327
Kase H, Aoyama S, Ichimura M, Ikeda K, Ishii A, Kanda T, Koga K, Koike N, Kurokawa M, Kuwana Y, Mori A, Nakamura J, Nonaka H, Ochi M, Saki M, Shimada J, Shindou T, Shiozaki S, Suzuki F, Takeda M, Yanagawa K, Richardson PJ, Jenner P, Bedard P, Borrelli E, Hauser RA, Chase TN (2003) Progress in pursuit of therapeutic A2A antagonists: the adenosine A2A receptor selective antagonist KW6002: research and development toward a novel nondopaminergic therapy for Parkinson’s disease. Neurology 61:S97–S100
Kieburtz K, Ravina B (2007) Why hasn’t neuroprotection worked in Parkinson’s disease? Nat Clin Pract Neurol 3:240–241
Koga K, Kurokawa M, Ochi M, Nakamura J, Kuwana Y (2000) Adenosine A(2A) receptor antagonists KF17837 and KW-6002 potentiate rotation induced by dopaminergic drugs in hemi-Parkinsonian rats. Eur J Pharmacol 408:249–255
Kulisevsky J, García-Sánchez C, Berthier ML, Barbanoj M, Pascual-Sedano B, Gironell A, Estévez-González A (2000) Chronic effects of dopaminergic replacement on cognitive function in Parkinson’s disease: a two-year follow-up study of previously untreated patients. Mov Disord 15(4):613–626
Kurokawa M, Koga K, Kase H, Nakamura J, Kuwana Y (1996) Adenosine A2A receptor-mediated modulation of striatal acetylcholine release in vivo. J Neurochem 66:1882–1888
Küst BM, Biber K, van Calker D, Gebicke-Haerter PJ (1999) Regulation of K + channel mRNA expression by stimulation of adenosine A2A-receptors in cultured rat microglia. Glia 25:120–130
LeWitt PA (2006) Neuroprotection for Parkinson’s disease. J Neural Transm Suppl:113–122
LeWitt PA, 6002-US-005/6002-US-006 Clinical Investigator Group (2004) OFF time reduction from adjunctive use of istradephylline (KW-6002) in levodopa-treated patients with advanced Parkinson’s disease. Presented at 8th International Congress of Parkinson’s Disease and Movement Disorders, Rome. Mov Disord 19(Suppl 9):S222
LeWitt PA, Guttman M, Tetrud JW, Tuite PJ, Mori A, Chaikin P, Sussman NM (2008) Adenosine A2A receptor antagonist istradefylline (KW-6002) reduces OFF time in Parkinson’s disease: a double-blind, randomized, multicenter clinical trial (6002-US-005). Ann Neurol 63:295–302
Litvan I, Chesselet MF, Gasser T, Di Monte DA, Parker D Jr, Hagg T, Hardy J, Jenner P, Myers RH, Price D, Hallett M, Langston WJ, Lang AE, Halliday G, Rocca W, Duyckaerts C, Dickson DW, Ben-Shlomo Y, Goetz CG, Melamed E (2007a) The etiopathogenesis of Parkinson disease and suggestions for future research. Part I. J Neuropathol Exp Neurol 66:251–257
Litvan I, Halliday G, Hallett M, Goetz CG, Rocca W, Duyckaerts C, Ben-Shlomo Y, Dickson DW, Lang AE, Chesselet MF, Langston WJ, Di Monte DA, Gasser T, Hagg T, Hardy J, Jenner P, Melamed E, Myers RH, Parker D Jr, Price DL (2007b) The etiopathogenesis of Parkinson disease and suggestions for future research. Part II. J Neuropathol Exp Neurol 66:329–336
Mally J, Stone TW (1996) Potential role of adenosine antagonist therapy in pathological tremor disorders. Pharmacol Ther 72:243–250
Mark MH, 6002-US-007 Clinical Investigator Group (2005) Long-term efficacy of istradephylline in patients with advanced Parkinson’s disease. Presented at 9th International Congress of Parkinson’s disease and Movement Disorders, New Orleans. Mov Disord 20(Suppl 10):S93
McCulloch CC, Kay DM, Factor SA, Samii A, Nutt JG, Higgins DS, Griffith A, Roberts JW, Leis BC, Montimurro JS, Zabetian CP, Payami H (2008) Exploring gene–environment interactions in Parkinson’s disease. Hum Genet 123:257–265
McGeer PL, McGeer EG (2008) Glial reactions in Parkinson’s disease. Mov Disord 23:474–483
Mihara T, Mihara K, Yarimizu J, Mitani Y, Matsuda R, Yamamoto H, Aoki S, Akahane A, Iwashita A, Matsuoka N (2007) Pharmacological characterization of a novel, potent adenosine A1 and A2A receptor dual antagonist, 5-[5-amino-3-(4-fluorophenyl)pyrazin-2-yl]-1-isopropylpyridine-2(1H)-one (ASP5854), in models of Parkinson’s disease and cognition.J Pharmacol Exp Ther 323:708–719
Morelli M (2003) Adenosine A2A antagonists: potential preventive and palliative treatment for Parkinson’s disease. Exp Neurol 184:20–23
Morelli M, Fenu S, Pinna A, Di Chiara G (1994) Adenosine A2 receptors interact negatively with dopamine D1 and D2 receptors in unilaterally 6-hydroxydopamine-lesioned rats. Eur J Pharmacol 251:21–25
Nishi A, Liu F, Matsuyama S, Hamada M, Higashi H, Nairn AC, Greengard P (2003) Metabotropic mGlu5 receptors regulate adenosine A2A receptor signaling. Proc Natl Acad Sci USA 100:1322–1327
Nishizaki T, Nagai K, Nomura T, Tada H, Kanno T, Tozaki H, Li XX, Kondoh T, Kodama N, Takahashi E, Sakai N, Tanaka K, Saito N (2002) A new neuromodulatory pathway with a glial contribution mediated via A(2a) adenosine receptors. Glia 39:133–147
Obeso JA, Rodriguez-Oroz MC, Rodriguez M, Lanciego JL, Artieda J, Gonzalo N, Olanow CW (2000) Pathophysiology of the basal ganglia in Parkinson’s disease. Trends Neurosci 23:S8–S19
Obeso JA, Rodriguez-Oroz M, Marin C, Alonso F, Zamarbide I, Lanciego JL, Rodriguez-Diaz M (2004) The origin of motor fluctuations in Parkinson’s disease: importance of dopaminergic innervation and basal ganglia circuits. Neurology 62:S17–S30
Obeso JA, Rodriguez-Oroz MC, Javier Blesa F, Guridi J (2006) The globus pallidus pars externa and Parkinson’s disease. Ready for prime time? Exp Neurol 202:1–7
Ochi M, Shiozaki S, Kase H (2004) Adenosine A(2A) receptor-mediated modulation of GABA and glutamate release in the output regions of the basal ganglia in a rodent model of Parkinson’s disease. Neuroscience 127:223–231
O’Neill M, Brown VJ (2006) The effect of the adenosine A(2A) antagonist KW-6002 on motor and motivational processes in the rat. Psychopharmacology 184:46–55
Papa SM, Desimone R, Fiorani M, Oldfield EH (1999) Internal globus pallidus discharge is nearly suppressed during levodopa-induced dyskinesias. Ann Neurol 46:732–738
Pierri M, Vaudano E, Sager T, Englund U (2005) KW-6002 protects from MPTP induced dopaminergic toxicity in the mouse. Neuropharmacology 48:517–524
Pinna A, di Chiara G, Wardas J, Morelli M (1996) Blockade of A2A adenosine receptors positively modulates turning behaviour and c-Fos expression induced by D1 agonists in dopamine-denervated rats. Eur J Neurosci 8:1176–1181
Pinna A, Fenu S, Morelli M (2001) Motor stimulants effects of the adenosine A2A receptor antagonist SCH 58261 do not develop tolerance after repeated treatments in 6-hydroxydopamine lesioned rats. Synapse 39:233–239
Pinna A, Corsi C, Carta AR, Valentini V, Pedata F, Morelli M (2002) Modification of adenosine extracellular levels and adenosine A2A receptor mRNA by dopamine denervation. Eur J Pharmacol 446:75–82
Pinna A, Pontis S, Morelli M (2007) Adenosine A2A receptor antagonists improve deficits in initiation of movement and sensory motor integration in the unilateral 6-hydroxydopamine rat model of Parkinson’s disease. Synapse 61:606–614
Pollack AE, Fink JS (1996) Synergistic interaction between an adenosine antagonist and a D1 dopamine agonist on rotational behavior and striatal c-Fos induction in 6-hydroxydopamine-lesioned rats. Brain Res 743:124–130
Popoli P, Pintor A, Domenici MR, Frank C, Tebano MT, Pèzzola A, Scarchilli L, Quarta D, Reggio R, Malchiodi-Albedi F, Falchi M, Massotti M (2002) Blockade of striatal adenosine A2A receptor reduces, through a presynaptic mechanism, quinolinic acid-induced excitotoxicity: possible relevance to neuroprotective interventions in neurodegenerative diseases of the striatum. J Neurosci 22:1967–1975
Pourcher E, 6002-US-018 Clinical Investigator Group (2006) Safety and tolerability of istradephylline (KW-6002) in Parkinson’s disease with motor response complications: results of the KW-6002-US-018 study. Presented at the 10th International Congress of Parkinson’s Disease and Movement Disorders, Kyoto. Mov Disord 21(Suppl 15):S508
Powers KM, Kay DM, Factor SA, Zabetian CP, Higgins DS, Samii A, Nutt JG, Griffith A, Leis B, Roberts JW, Martinez ED, Montimurro JS, Checkoway H, Payami H (2008) Combined effects of smoking, coffee, and NSAIDs on Parkinson’s disease risk. Mov Disord 23:88–95
Rao N, Uchimura T, Mori A (2005a) Evaluation of safety, tolerability, and multiple dose pharmacokinetics of istradephylline in healthy subjects. Clin Pharmacol Ther 83(Suppl):PIII-89
Rao N, Uchimura T, Mori A (2005b) Evaluation of safety, tolerability, and multiple dose pharmacokinetics of istradephylline in Parkinson’s disease patients. Clin Pharmacol Ther 83(Suppl):PIII-88
Ritz B, Ascherio A, Checkoway H, Marder KS, Nelson LM, Rocca WA, Ross GW, Strickland D, Van Den Eeden SK, Gorell J (2007) Pooled analysis of tobacco use and risk of Parkinson disease. Arch Neurol 64:990–997
Rodrigues RJ, Alfaro TM, Rebola N, Oliveira CR, Cunha RA (2005) Co-localization and functional interaction between adenosine A(2A) and metabotropic group 5 receptors in glutamatergic nerve terminals of the rat striatum. J Neurochem 92:433–441
Rose S, Ramsay Croft N, Jenner P. The novel adenosine A2A antagonist (2007) ST1535 potentiates the effects of a threshold dose of L-dopa in unilaterally 6-OHDA-lesioned rats. Brain Res 1133:110–114
Rosin DL, Robeva A, Woodard RL, Guyenet PG, Linden J (1998) Immunohistochemical localization of adenosine A2A receptors in the rat central nervous system. J Comp Neurol 401:163–186
Rosin DL, Hettinger BD, Lee A, Linden J (2003) Anatomy of adenosine A2A receptors in brain: morphological substrates for integration of striatal function. Neurology 61:S12–S18
Salamone JD, Mayorga AJ, Trevitt JT, Cousins MS, Conlan A, Nawab A (1998) Tremulous jaw movements in rats: a model of parkinsonian tremor. Prog Neurobiol 56:591–611
Schapira AH (2008) Progress in neuroprotection in Parkinson’s disease. Eur J Neurol 15(Suppl 1):5–13
Schiffmann SN, Jacobs O, Vanderhaeghen JJ (1991) Striatal restricted adenosine A2 receptor (RDC8) is expressed by enkephalin but not by substance P neurons: an in situ hybridization histochemistry study. J Neurochem 57:1062–1067
Schiffmann SN, Fisone G, Moresco R, Cunha RA, Ferré S (2007) Adenosine A2A receptors and basal ganglia physiology. Prog Neurobiol 83:277–292
Schwarzschild MA, Agnati L, Fuxe K, Chen JF, Morelli M (2006) Targeting adenosine A2A receptors in Parkinson’s disease. Trends Neurosci 29:647–654
Shindou T, Richardson PJ, Mori A, Kase H, Ichimura M (2003) Adenosine modulates the striatal GABAergic inputs to the globus pallidus via adenosine A2A receptors in rats. Neurosci Lett 352:167–170
Shiozaki S, Ichikawa S, Nakamura J, Kitamura S, Yamada K, Kuwana Y (1999) Actions of adenosine A2A receptor antagonist KW-6002 on drug-induced catalepsy and hypokinesia caused by reserpine or MPTP. Psychopharmacology 147:90–95
Shulman LM, 6002-US-013 Clinical Investigator Group (2006) The safety profile of istradephylline (KW-6002) in Parkinson’s disease with motor response complications on levodopa/carbidopa: results of KW-6002-US-013 study. Presented at 10th International Congress of Parkinson’s Disease and Movement Disorders, Kyoto. Mov Disord 21(Suppl 15):S488
Siderowf A, Stern MB (2006) Preclinical diagnosis of Parkinson’s disease: are we there yet? Curr Neurol Neurosci Rep 6:295–301
Simola N, Fenu S, Baraldi PG, Tabrizi MA, Morelli M (2004) Blockade of adenosine A2A receptors antagonizes parkinsonian tremor in the rat tacrine model by an action on specific striatal regions. Exp Neurol 189:182–188
Simola N, Fenu S, Baraldi PG, Tabrizi MA, Morelli M (2006) Involvement of globus pallidus in the antiparkinsonian effects of adenosine A(2A) receptor antagonists. Exp Neurol 202:255–257
Simola N, Fenu S, Baraldi PG, Tabrizi MA, Morelli M (2008) Blockade of globus pallidus adenosine A(2A) receptors displays antiparkinsonian activity in 6-hydroxydopamine-lesioned rats treated with D(1) or D(2) dopamine receptor agonists. Synapse 62:345–351
Stacy M, Galbreath A (2008) Optimizing long-term therapy for Parkinson disease: levodopa, dopamine agonists, and treatment-associated dyskinesia. Clin Neuropharmacol 31:51–56
Stacy M, 6002-US-005/6002-US-006 Clinical Investigator Group (2004) Istradephylline (KW-6002) as adjunctive therapy in patients with advanced Parkinson’s disease: a positive safety profile with supporting efficacy. Presented at 8th International Congress on Parkinson’s Disease and Movement Disorders, Rome. Mov Disord 19(Suppl 9):S215
Stacy M, Silver D, Mendis T, Sutton J, Mori A, Chaikin P, Sussman NM (2008) A 12-week, placebo-controlled study (6002-US-006) of istradefylline in Parkinson disease. Neurology 70:2233–2240
Stamey W, Jankovic J (2008) Impulse control disorders and pathological gambling in patients with Parkinson disease. Neurologist 14:89–99
Stocchi F (2003) Prevention and treatment of motor fluctuations. Parkinsonism Relat Disord 9(Suppl 2):S73–S81
Stocchi F (2005) Pathological gambling in Parkinson’s disease. Lancet Neurol 4:590–592
Stocchi F, Olanow CW (2003) Neuroprotection in Parkinson’s disease: clinical trials. Ann Neurol 53(Suppl 3):S87–S97
Takahashi RN, Pamplona FA, Prediger RD (2008) Adenosine receptor antagonists for cognitive dysfunction: a review of animal studies. Front Biosci 13:2614–2632
Tronci E, Simola N, Borsini F, Schintu N, Frau L, Carminati P, Morelli M (2007) Characterization of the antiparkinsonian effects of the new adenosine A2A receptor antagonist ST1535: acute and subchronic studies in rats. Eur J Pharmacol 566:94–102
Trugman JM, 6002-US-013 Clinical Investigator Group (2006) Efficacy of istradephylline (KW-6002) in levodopa-treated Parkinson’s disease patients with motor response complications: primary efficacy results of the KW-6002-US-013 study. Presented at 10th International Congress of Parkinson’s Disease and Movement Disorders, Kyoto. Mov Disord 21(Suppl 15):S513
Wakabayashi K, Tanji K, Mori F, Takahashi H (2007) The Lewy body in Parkinson’s disease: molecules implicated in the formation and degradation of alpha-synuclein aggregates. Neuropathology 27:494–506
Wang JH, Ma YY, van den Buuse M (2006) Improved spatial recognition memory in mice lacking adenosine A2A receptors. Exp Neurol 199:438–445
Wardas J, Konieczny J, Lorenc-Koci E (2001) SCH 58261, an A(2A) adenosine receptor antagonist, counteracts parkinsonian-like muscle rigidity in rats. Synapse 41:160–171
Weintraub D, Comella CL, Horn S (2008a) Parkinson’s disease—Part 1: Pathophysiology, symptoms, burden, diagnosis, and assessment. Am J Manag Care 14:S40–S48
Weintraub D, Comella CL, Horn S (2008b) Parkinson’s disease—Part 2: Treatment of motor symptoms. Am J Manag Care 14:S49–S58
Weintraub D, Comella CL, Horn S (2008c) Parkinson’s disease—Part 3: Neuropsychiatric symptoms. Am J Manag Care 14:S59–S69
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2009 Springer-Verlag Berlin Heidelberg
About this chapter
Cite this chapter
Morelli, M., Carta, A.R., Jenner, P. (2009). Adenosine A2A Receptors and Parkinson’s Disease. In: Wilson, C., Mustafa, S. (eds) Adenosine Receptors in Health and Disease. Handbook of Experimental Pharmacology, vol 193. Springer, Berlin, Heidelberg. https://doi.org/10.1007/978-3-540-89615-9_18
Download citation
DOI: https://doi.org/10.1007/978-3-540-89615-9_18
Published:
Publisher Name: Springer, Berlin, Heidelberg
Print ISBN: 978-3-540-89614-2
Online ISBN: 978-3-540-89615-9
eBook Packages: Biomedical and Life SciencesBiomedical and Life Sciences (R0)