
Abstract
Thin, small webs mostly cause nothing or only mild dysphonia. If the web is big and thick, dysphonia and dyspnea may be present. The final diagnosis can be established by direct microlaryngoscopy combined with 0°-25°-45°-70° telescopes to determine the exact thickness of the membrane below the anterior commissure. Only very thin anterior commissure webs can be cured by simple endoscopic dissection of the membrane using laser or a microscalpel with a disposable sharp blade. In other cases, it is necessary, after dissection and division of the web, to fix a silicone sheet or keel between the deepithelialized parts of the dissected membrane. After dissecting the web, the wound surface is painted with mitomycin C to decrease fibroblast activity and the risk of recurrence. The keel is established using the endoextralaryngeal needle carrier of Lichtenberger. To achieve a good result, it is important that the keel appropriately covers the deepithelialized parts. After surgery the patient must be given broad-band antibiotics at least for 5 days. Administration of steroids during the first 3 days has proved advantageous. It is recommended that the position of the keel be checked after surgery. The keel is removed 3 weeks later by microlaryngoscopy after cutting the ends of the thread on the neck. The operation may be performed on small children.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
These keywords were added by machine and not by the authors. This process is experimental and the keywords may be updated as the learning algorithm improves.
12.2 Diagnosis
Indirect laryngoscopy or magnifying indirect laryngoscopy are usually enough to establish the diagnosis in adults. Direct microlaryngoscopy may be necessary in children and newborns because of a lack of collaboration by other means. The final diagnosis can be established by direct microlaryngoscopy combined with 0°-25°-45°-70° telescopes to determine the exact thickness of the membrane below the anterior commissure.
12.3 Preoperative Workup
The preoperative workup may include blood oxygen saturation monitoring and pulmonary function tests. In acquired cases, there may be an investigation for gastroesophageal reflux disease.
12.4 Therapy
12.4.1 Conservative Approach
In acute acquired cases, right after the damage is revealed, there is a chance to cover the rough deepithelialized surface with fibrin glue in an attempt to prevent adhesions. Mitomycin C may also be administered.
12.4.2 Surgical Approach
Only very thin anterior commissure webs can be cured by simple endoscopic dissection of the membrane using laser or a microscalpel with a disposable sharp blade. In other cases, it is necessary, after dissection and division of the web, to fix a silicone sheet, or keel, between the deepithelialized parts of the dissected membrane.
Surgical techniques with outer exposure of the larynx, mostly after preliminary tracheostomy, are seldom used nowadays. The most frequently used procedure with outer exposure was described by Montgomery and Gamble [3]. The procedure is done mostly after preliminary tracheostomy. The larynx is opened by means of thyreotomy. The cartilage incision is made exactly in the midline, and the web is dissected. Afterward, an umbrella-like T-shaped silicone keel is placed in the anterior commissure between the vocal cords (Fig. 12b.1). When the keel is in the appropriate place, the soft tissues and skin are closed above the larynx. Six weeks later the keel is removed after the wound surfaces are healed.


Surgical technique with outer exposure of the larynx according to Montgomery and Gamble. A T-shaped silicone keel is placed in the anterior commissure betwwen the vocal cords
Endoscopic-microlaryngoscopic techniques with fixation of a keel or sheet in the anterior commissure by Nessel for 2-3 weeks without tracheostomy can be done using extraendolaryngeal sutures. The anterior commissure web is dissected by performing direct microlaryngoscopy. Two thick serum needles are pushed through the larynx from outside to inside. One needle is pushed through the cricothyroid and the other through the thyreohyoid membrane. Afterward, one thread is pushed through the first needle and then the other thread through the second needle. The ends of the threads are grasped with microforceps, which is not always easy owing to bleeding from the stitching canal making it difficult to find the ends of the threads. After grasping the ends of the threads, they are pulled out and are tightened and knotted outside the laryngoscope. A silicone sheet is then fixed on the thread. The ends of the thread are pulled back, and the sheet is placed between the two parts of the dissected web in the anterior commissure. Having positioned the sheet in the appropriate place, the ends of the threads are tightened and knotted on a piece of silicone tube placed on the skin of the neck [4] (Fig. 12b.2).


Endoscopic-microlaryngoscopic technique with fixation of a keel or sheet in the anterior commissure by Nessel
Endoscopic-microlaryngoscopic technique with fixation of a keel or sheet in the anterior commissure for 2-3 weeks without tracheostomy using endoextralaryngeal sutures by Lichtenberger [1, [2] is also available. here, the anterior commissure web is dissected by performing direct microlaryngoscopy. The web may be dissected using laser or a microscalpel holder with a safety lock by Lichtenberger with disposable sharp blades (Fig. 12b.3).


Microscalpel holder with safety lock and disposable blades by Lichtenberger
Both dissection options have advantages and disadvantages. With laser there is less bleeding, but tissue loss and delayed wound healing are present. When performing the same intervention with a disposable sharp blade, there is more bleeding but there is no tissue loss and more rapid healing occurs. It seems that the laser technique is indicated if there is a thick web causing not only dysphonia but also dyspnea. In such cases, the most important factor is the patient’s breathing, with the voice being of only secondary importance. In contrast, when there is a thin web that cannot be managed without interposition (keel or sheet) and the patient suffers only dysphonia, use of a sharp blade may be better because it does not cause tissue loss, which is important if the aim is to improve the voice of the patient.
After dissecting the web, the wound surface is painted with mitomycin C (0.2-0.6 mg/ml), a step that is repeated two more times. The introduction of mitomycin C after dissection of the web may further improve the results.
A homemade silicon keel is used (Fig. 12b.4). This keel is chosen from the series of keels made from a medical grade silicone block. Before fixing the keel on the thread, the chosen keel is placed in the anterior commissure without fixation. if the size and shape of the keel are appropriate, the thread is then placed through the keel.


Silicone keel for endoscopic management of an anterior commissure web
Placing the thread through the keel is important for two reasons: The first is the safety factor—to prevent the thread cutting through the silicone keel. The other reason is that when the thread is placed appropriately it covers the deepithelialized areas in a craniocaudal direction. Afterward, the operation is continued with the endoextralaryngeal needle carrier (Fig. 12b.5).


Needle carrier instrument by Lichtenberger
One end of the fixing thread is led through a specially designed curved needle. Then the needle is placed in the distal, curved end of the device, and the needle carrier is pushed through the laryngoscope. (The use of the Weerda or Steiner laryngoscope can be recommended for this purpose.)
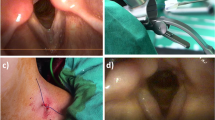
The distal bent, blunt end of the needle carrier is placed below the anterior commissure, and the special needle is pushed through the larynx with one end of the thread (Fig. 12b.6a). It is important that the thread goes through the thyroid cartilage, ensuring a stable position, not through the membranes (as in other techniques), to avoid an unstable position and dislocation of the keel with the consequence of re-scarring.


a-c Endoextralaryngeal keel fixation technique by Lichtenberger
Then the silicone keel is fixed on the thread and the same procedure is repeated, but now the stitching occurs with the other end of the thread above the anterior commissure (Fig. 12b.6b). The ends of the thread are pulled after the keel is placed in the appropriate place; the thread ends are pulled and tightened on a bent silicone tube on the skin of the neck (Fig. 12b.6c). Three weeks later, the keel is removed by microlaryngoscopy after cutting the ends of the thread on the neck.
The operation may be performed on small children (Fig. 12b.7) and newborns. However, in infants < 1 year of age, it must be ensured that the anterior edge of the keel is not sharp. Otherwise, the keel may cut through the soft thyroid cartilage, as happened in one of our first cases.


Small child after dissection of the web and fixing a keel with the endoextralaryngeal suture technique
To achieve a good result, it is important that the keel appropriately covers the deepithelialized parts of the larynx. This can be verified by endoscopy (Fig. 12b.8).


Endoscopic picture about the keel fixed in the anterior commissure
It is necessary to have a series of keels from which to choose the most suitable one. A silicone sheet can also be introduced in some adults. However, in these cases it must be taken into consideration that crustation may develop around the sheet, narrowing the lumen of the larynx temporary. The use of a thin sheet is not recommended in children because it cannot be fixed appropriately and it may move through the stitched canal, threatening the results of the surgery.
12.5 Tips and Pearls
-
The whole procedure should be done under totally sterile conditions.
-
It means that not only the devices are sterile as with a simple microlaryngoscopy.
-
The skin is disinfected, and the patient is covered with drapes before the operation.
-
The keel of appropriate size is chosen from the series of homemade, medical grade silicone keels.
-
An atraumatic, thin, specially curved needle is used.
-
The keel should cover the deepithelialized areas in every direction.
-
The silicone tube placed on the neck should have a bent shape to prevent decubitation of the skin at the two ends of the tube.
-
The keel and the thread must be removed after 20-21 days in adults and after 14 days in children.
References
Lichtenberger G, Toohill RJ (1991) The endo-extralaryngeal needle carrier. Otolaryngol Head Neck Surg 105(5):755-756
Lichtenberger G, Toohill RJ (1994) New keel fixing technique for endoscopic repair of anterior commissure webs. Laryngoscope 104(6 Pt 1):771-774
Montgomery WW, Gamble JE (1970) Anterior glottic stenosis. Experimental and clinical management. Arch Otolaryngol 92(6):560-567
Nessel E (1968) A suggestion for a simplified management of the vocal fold synechia. HNO 16(9):284-287
Author information
Authors and Affiliations
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2009 Springer-Verlag Berlin Heidelberg
About this chapter
Cite this chapter
Lichtenberger, G. (2009). Synechia of the Anterior Commissure. In: Remacle, M., Eckel, H. (eds) Surgery of Larynx and Trachea. Springer, Berlin, Heidelberg. https://doi.org/10.1007/978-3-540-79136-2_15
Download citation
DOI: https://doi.org/10.1007/978-3-540-79136-2_15
Published:
Publisher Name: Springer, Berlin, Heidelberg
Print ISBN: 978-3-540-79135-5
Online ISBN: 978-3-540-79136-2
eBook Packages: MedicineMedicine (R0)