
Abstract
This chapter provides a clinical perspective on how the kidney can be used as a sentinel for cardiovascular disease (CVD) burden and, perhaps, as a means of measuring therapeutic success for the treatment of cardiovascular disease. To accomplish these goals, we will first provide some background about the relationship between chronic kidney disease and CVD. Next, we will discuss the value of estimating glomerular filtration rate (GFR) as a better measure of overall kidney function as opposed to simply using a serum creatinine. In addition, we will also focus on the importance of residual albuminuria or proteinuria and its implications for predicting CVD. These observations will set the stage for assessing appropriate blood pressure, cholesterol and glucose goals for patients, and the pharmacologic means of attaining these goals. Finally, we will describe non-traditional CVD risk factors unique to the CKD population and recommend some therapeutic strategies whenever possible.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
- Chronic kidney disease
- Cardiovascular disease
- Microalbuminuria
- Estimated glomerular filtration rate
- Creatinine clearance
- Nephropathy
- Proteinuria
- Albuminuria
- End-stage renal disease
1 Introduction
Several epidemiological studies have identified chronic kidney disease (CKD) as a risk factor for cardiovascular disease (CVD) and vice versa. However, whether such a complex relationship is a causal relationship or a mere epiphenomenon remains to be established. On the one hand, kidney disease and cardiovascular disease share a cluster of traditional modifiable and non-modifiable risk factors, such as tobacco use, obesity, diabetes mellitus (DM), systemic arterial hypertension (HTN) and dyslipidemia. On the other hand, the onset of CKD is often associated with findings which have been identified as non-traditional cardiovascular risk factors, unique to this patient population, such as reduction in estimated glomerular filtration rate (eGFR), micro- or macro-albuminuria, anemia in CKD, CKD-Mineral and Bone Disorder (CKD-MBD) with vascular calcifications, chronic inflammation and protein-energy wasting (PEW), acid-base and electrolyte disturbances, and volume overload. Thus, eGFR and albuminuria, both of which are independent risk factors of CVD, ought to be incorporated into any reliable clinical prediction model aimed at quantifying CVD risk. Although CVD is the leading cause of death in all CKD groups (dialysis, non-dialysis, transplant recipients), most major clinical trials aimed at managing CVD or its risk factors exclude patients with advanced CKD, making an evidence-based approach to CVD risk reduction and management quite challenging. Finally, formulating a roadmap that combines non-pharmacological as well as pharmacological therapeutic strategies to slow down the progression of CKD and minimize CVD risk is essential to promote survival.
2 Epidemiology: The Burden of CKD and CVD Traditional Risk Factors
2.1 Systemic Arterial Hypertension
In 2013, the World Health Organization (WHO) published “A Global Brief on Hypertension”, in which it identifies CVD as the most common cause of death among humans, claiming about one third of the total mortality burden in our species, and resulting in around 17 million deaths annually, of which 9.4 million deaths are due to complications of HTN. Among patients who died of heart disease, HTN was the leading cause of death in at least 45%, and in 51% amongst those who died of stroke. Hypertension affects 40% of all adults aged 25 years or higher worldwide with the highest prevalence being among Africans and in low-income countries [1].
In the United States (US), the National Health and Nutrition Examination Survey (NHANES) 2011–2012 reports that 29.1% of adults older than 18 years have HTN, 17.2% of whom have not been diagnosed and 75.7% were on blood-pressure (BP) lowering medications, and a mere 51.9% had controlled HTN [2].
In patients with stage 1–5 CKD, the prevalence of systemic arterial hypertension exceeds 70% [3,4,5] and varies proportionately with the degree of kidney disease [6]; the 2015 USRDS-ADR estimates that 74% of NHANES 2007–2012 participants with stage 1–4 CKD have HTN and as many as 84.1% of patients with stages 4–5 CKD having systemic arterial hypertension [7].
2.2 Diabetes Mellitus
Similarly, in 2016, the WHO published a “Global Report on Diabetes”, in which it reports that DM affects 8.5% of adults as of 2014, almost double the 1980 rate and totaling 422 millions adults worldwide. This rise mirrors the epidemic of overweight and obesity, and it is not confined by geographical location or income. In 2012, dys-glycemia directly resulted in 3.7 million deaths: DM was directly responsible for 1.5 million deaths and pre-DM was responsible for the remaining 2.2 million deaths, with 43% of all these deaths occurring at an age less than 70 years [8].
In the US, the 2014 National Diabetes Statistics Report estimates that DM affects 12.3% of the adult population (28.9 million) of whom around 27.8% have not been diagnosed, and a further 36.6% (86 millions) have pre-DM of whom around 90% are not aware of their diagnosis and without lifestyle modifications 15–30% will progress to DM within 5 years [7, 9].
The 2015 USRDS-ADR estimates that 39.2% of NHANES 2007–2012 adult participants with stage 1–4 CKD have DM [7]. Inversely, DM is the major cause of CKD and ESKD worldwide. Kidney disease complicates diabetes in 25–40% after a course of 20–25 years and around one third of those patients develop ESKD requiring renal replacement therapy but the majority will die of cardiovascular causes before progression to ESKD [10]. The 2015 USRDS-ADR lists DM as the primary cause in 43.9% of incident ESKD patients. In a cohort of 2097 diabetic participants in the NHANES 2009–2014, aged 20 years and over, diabetic nephropathy was present in 26.2% with 15.9% having Stage A2 or A3 albuminuria and 14.1% having an abnormal eGFR; this data projects that as of 2014, 8.2 million Americans have diabetic CKD [11].
2.3 Dyslipidemia
In its 2015 “Heart Disease and Stroke Statistics” report, the American Heart Association (AHA) estimated that 31.7% of American adults have a high cholesterol or a high low-density lipoprotein, of whom 48.1% are receiving pharmacological therapy and only 29.5% have achieved optimal control [12, 13].
In patients with CKD, dyslipidemia is common and is dependent on severity of CKD stage, degree of urine protein excretion, and DM status [14].
2.4 Tobacco Use
Data from the 2014 NHANES survey reveals that 16.8% of adults age 18 years and over are active tobacco users [15] and tobacco use ranks second amongst all causes of deaths and disability and third for death from coronary heart disease [13]. Great progress has been made in the fight against tobacco use and rates have steadily declined over the past decades; however, such advances may be threatened by e-tobacco use and e-cigarettes, potential risks and benefits of which are being actively researched.
2.5 Obesity
In the aforementioned 2016 WHO “Global Report on Diabetes”, the report also highlighted that more than 1 in 3 adults worldwide were overweight and more than one in ten were obese in 2014 [8]; with a calculated rise in the age- standardized global mean body mass index (BMI) by 0.4 kg/m2 in men and by 0.5 kg/m2 in women per decade between 1980 and 2008 [16].
In the US, DM affects 9.3% of the population (29.1million as of 2012) of whom 27.8% have not been diagnosed [9]; 70.7% of adults age 20 years and higher are overweight or obese: 32.8% overweight and 37.9% obese (2013–2014 data) [17].
2.6 Exercise
The 2014 NHANES survey show that 49.2% of Americans adults (≥18 years) met the 2008 Federal Physical Activity Guidelines for leisure-time aerobic physical activity (but only 20.8% met the guidelines for both aerobic physical and muscle-strengthening activity. For aerobic physical activity, the weekly recommendation is for 150 min of moderate-intensity exercise, or 75 min of high-intensity, or some combination, and most favorably spread over many week-days. For muscle-strengthening, the weekly recommendation is to exercise all muscle groups in a moderate- to high-intensity workout at least twice a week [18].
2.7 CKD
CKD affects about 10% of adults worldwide. In the US, 10% of adults have CKD (more than 20 million people), with the rising incidence and prevalence being almost all concentrated in individuals aged 60 years or more; approximately one third of diabetic patients have CKD and about one fifth of hypertensive patients have CKD [19]. Worldwide, there are huge disparities in the access to CKD care, in fact, care is limited in its majority to the developed world; 80% of patients with end stage kidney disease (ESKD, Stage 5D CKD) who are receiving renal replacement therapy (RRT) live in the developed world where the cost of RRT is most likely to be subsidized [20].
3 CKD: Definition, Stages and Causes
CKD refers to an abnormality in kidney function or structure that persists beyond a period of 3 months. Such abnormalities manifest in one or more of the following clinical biomarkers: (1) a relative rise in serum creatinine with a resultant reduction in the eGFR (2) micro- or macro-albuminuria (3) microscopic or macroscopic/gross hematuria (4) abnormal urine sediment (e.g. cellular elements, casts or crystals) (5) urinary system structural abnormalities detected by imaging studies (e.g. congenital anomalies, cysts, stones) (6) acid-base or electrolyte imbalances reflecting renal tubular disease (7) abnormal results confirmed by a kidney biopsy [21].
3.1 KDIGO eGFR and Albuminuria Categories
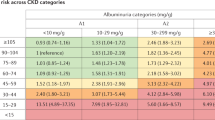
In 2012, the Kidney Disease: Improving Global Outcomes (KDIGO) CKD Work Group recommended a CKD prognostic classification that adds the level of urine albumin excretion rate to the 2002 National Kidney Foundation (NKF) Kidney Disease Outcomes Quality Initiative (K/DOQI) definition and staging of CKD based on the eGFR. Six categories of eGFR (mL/min/1.73 m2 BSA) (G1 ≥ 90, G2 60–89, G3a 45–59, G3b 30–44, G4 15–29, G5 < 15) and three categories of albuminuria based on the urinary albumin-to-creatinine ratio (ACR, mg Albumin/g Creatinine) (A1 < 30, A2 30–300 also known elsewhere in the literature as micro-albuminuria, A3 > 300 also known as macro-albuminuria) are described. This system incorporates mounting evidence of the deleterious effects of a higher urine albumin excretion rate and helps predict and classify the patient’s risk of CKD progression into the following categories: low risk, moderately increased risk, high risk and very high risk (Fig. 8.1) [21]; an example of such evidence comes from the Multiple Risk Factor Intervention Trial (MRFIT) team, who identified a 41-fold increased risk of progression to ESKD amongst individuals with an eGFR <60 mL/min per 1.73 m2 and ≥2+ dipstick proteinuria, amongst 12,886 men with high CVD risk and followed for a period of 25 years [22]. For example, a patient with an estimated GFR of 58 mL/min/1.73 m2 BSA and a urine albumin excretion rate of 358 mg albumin/ g creatinine would be classified as having stage 3 (G3a A3) CKD and has a “very high risk” of CKD progression.

(a) Cardiovascular disease mortality by age, race, and gender in the general population and in dialysis patients. Cardiovascular mortality is defined as death due to arrhythmias, cardiomyopathy, cardiac arrest, myocardial infarction, atherosclerotic heart disease, and pulmonary edema. Data from the general population are from the National Center for Health Statistics multiple cause of mortality files 1993. Data from dialysis patients include hemodialysis and peritoneal dialysis combined from USRDS 1994–1996. (Reprinted with permission from National Kidney Foundation Task Force on Cardiovascular Disease [252])
3.2 Prevalence of CKD by eGFR and Albuminuria Category
The 2015 USRDS-ADR estimates the prevalence of CKD in the 2007–2012 NHANES samples at 13.65% amongst adults aged 20 years and over with the 4.18% having category G1 CKD, 2.95% having category G2 CKD, the biggest cluster of 5.90% having category G3 CKD, 0.48% having category G4 CKD and only 0.14% having category G5 CKD [7]. Among all 1988–2012 NHANES participants, 90.8% had category A1 albuminuria (70.7% < 10 mg albumin/g creatinine and 20.1% 10–29 mg/g), 7.8% had category A2 albuminuria, and 1.4% had category A3 albuminuria. Adopting the 2012 KDIGO prognostic classification, 86.2% of the 2007–2012 NHANES participants were classified as low risk CKD, 9.8% as moderately increased risk CKD, 2.3% as high risk CKD, and 1.7% as very high risk CKD. As mentioned earlier, CKD affects the elderly much more than it does the young; for example, in an Italian cohort of 4574 patients, <1% of individuals aged 18–24 had Stage 3–5 CKD compared to an excess of 30% for individuals aged 75 years or older [23].
3.3 Most Common Causes of CKD
Amongst incident ESKD patients, DM was the primary cause in 43.9%, HTN in 28.7%, glomerulonephritis in 7.5%, cystic kidney diseases in 2.1%, and other or unknown in 17.8% [7]. Among 2007–2012 NHANES participants with ND-CKD, DM was present in 39.2% of patients and HTN in 31% [7].
3.4 CKD Awareness and CKD Lifetime Risk
CKD awareness remains a problem just as is seen with HTN and type 2 diabetes (DMT2). Only 44.2% of 2001–2012 NHANES participants were aware of their stage 4 CKD, 8.4% of their stage 3 CKD, 5.0% of their stage 2 CKD and 3% of their stage 1 CKD. It is also important to note that epidemiological studies have shown that African Americans have three times the risk of progression to ESKD when compared to whites, and Hispanics 1.5 times the risk when compared to non-Hispanics; both male and female African-Americans have a significantly higher lifetime risk of stage 4 CKD and stage 5 CKD than Caucasians, and they develop ESKD around 15 years earlier than Caucasians [24]. It is no surprise then that the highest adjusted incidence and prevalence of ESKD is present amongst Black/African Americans; Hispanics had a higher incidence at 1.4 when compared to non-Hispanics. African Americans, Asians, Pacific Islanders, and Native Americans all had a higher incidence and prevalence of EKSD than Caucasians [7].
3.5 Therapeutic Options for ESKD
As CKD progresses, patients with stage 5 CKD are started on renal replacement therapy (RRT) when a clinical indication arises; usually this occurs when the eGFR is below 10 mL/min/1.73 m2 BSA and occasionally when below 15 mL/min/1.73 m2 BSA, and it is at this point that a patient is said to have ESKD. The most superior form of RRT is kidney transplantation, which offers the best survival rates and quality of life especially with pre-emptive kidney transplantation; however, with the shortage of organ supply in the face of increasing demand, dialysis (in-center or home hemodialysis HD, peritoneal dialysis PD) remains a valuable life-saving form of therapy albeit an inferior one. Short of a clinical indication, there is no known benefit for early versus late start of RRT with dialysis in patients with stage 5 CKD [25]. The 2015 USRDS-ADR reports that as of 2013, there were 116,990 incident patients with ESKD who received RRT (88.4% initiated HD, 9.0% initiated PD, 2.6% received pre-emptive kidney transplantation) and a total of 659,869 prevalent Americans with ESKD (63.9% on HD, 6.9% on PD, 29.3% with a functioning kidney transplant) [7].
3.6 Referral to Nephrology
Unfortunately, up to 38% of incident ESKD patients in 2013 received minimal or no nephrology care at all prior to initiation of RRT [7].
4 CKD Biomarkers: Estimating GFR and Quantifying Urinary Protein Excretion
Screening for CKD must be aimed at patients with a high pretest probability, namely individuals with DM, HTN, aged over 55 years or a relevant positive family history [26]. A timely nephrology referral is strongly recommended for any patient with stage 3–5 CKD or stage 2–3 albuminuria, in other words any patient who has a risk of progression other than low as per the 2012 KDIGO risk classification (Fig. 8.2). For such a timely referral, it is essential to use the eGFR rather than the serum creatinine, since the latter seems to lead to an underestimation of the severity of CKD [27].

2012 KDIGO risk classification
The 2002 National Kidney Foundation Kidney Disease Outcomes Quality (NKF K/DOQI) definition and the 2012 KDIGO prognostic classification of CKD created a shift in clinical practice in the new millennium, which made eGFR mathematical models the point of focus for quantifying CKD. Many major laboratories in the US currently report an eGFR, marking a decline in the use of reciprocal serum creatinine and the timed (classically 24-h) urine Creatinine clearance (UV/P).
4.1 Estimated Glomerular Filtration Rate eGFR
Creatinine (Cr) remains the major measured serum biomarker used by many such models (eGFRcr models) but it has its limitations; for example, Cr is dependent on muscle mass and dietary protein intake, and while Cr is freely filtered at the glomerular level, it is also secreted by the proximal tubular cells and estimating the secretion rate is not uniformly reliable. Cystatin C (Cys-C) provides an alternative measured serum biomarker, which is not affected by muscle mass or dietary protein intake, giving it an advantageous edge over Cr in certain populations, such as the elderly or those afflicted with neuromuscular disease. Cys-C has also been used by mathematical models to estimate GFR (eGFRcys models), while a third set of mathematical models combines both serum biomarkers (eGFRcr-cys).
The best mathematical model to calculate the eGFR, currently based on measured serum biomarkers Cr or Cys-C or both, must minimize bias (difference between the population mean of a set of calculated eGFRs and the true GFR) while maximizing precision (measures random error or degree of variability amongst calculated eGFRs) and accuracy (measures systematic errors and the overall difference between calculated eGFRs and the true GFR); usually, the true GFR is measured by urinary clearance of 125I-iothalamate which remains the gold standard. At this time, there does not seem to be one model where “one size fits all”. The most commonly used mathematical models which have been validated in clinical practice and research are: (1) the Modification of Diet in Renal Disease (MDRD) Study equation, (2) the Chronic Kidney Disease Epidemiology Collaboration (CKD-EPI) equation and (3) maybe to a lesser extent the Cockcroft-Gault equation.
The CKD-EPI equation performs better than the MDRD equation, and provides an eGFR which is more accurate and reflective of the true GFR, in patients with normal kidney function or Stage 1–2 CKD [28]. Thus, it should be adopted as the equation of choice in the general population; using the MDRD equation in the general population would result in a falsely high prevalence of CKD and misclassification of patients by CKD stage [29]. Both formulae are comparable in stages 4–5 CKD. Both these eGFRcr models are limited in subjects with altered body habitus (such as the obese, muscular bodybuilders, amputees and the pregnant), in individuals on a special diet such as vegetarian or vegan diets or those who consume large amounts of meat, in patients with a chronic illness such as malnutrition or neuromuscular diseases and in patients who are on prescription medications that compete with tubular creatinine secretion such as trimethoprim [30]. In such individuals, it is recommended to estimate the creatinine clearance by two separate 24-h urine collections or to use eGFRcys models.
4.2 Spot or Random Albumin to Creatinine Ratio (ACR)
An ACR, or a random protein to creatinine ratio (PCR), have become the most commonly used methods to quantitate urinary protein excretion and both have been validated against the gold-standard timed or 24-h urine collection for protein. The ACR or PCR urine sample is much more conveniently and quickly collected and cheaper than a timed sample; however, the latter has the advantage of more reproducible results with less variability in time, less concern for the timing of sample collection, providing additional clinical pearls such as quantitation of daily fluid and sodium and urea/protein and intake. A 24 h urine collection remains the most reliable clinical tool in pregnant women, morbidly or extremely obese, or when making major clinical decisions [31, 32].
4.3 Other Biomarkers
Numerous other biomarkers have been evaluated over the years such as urinary kidney injury molecule 1 (KIM-1), urinary liver–type fatty acid–binding protein (L-FABP), and neutrophil gelatin-associated lipocalin (NGAL), but they have a very limited current evidence-based established role in the wider clinical practice arena.
5 Relationship Between CKD and CVD: The CKD-CVD Connection
Cardiovascular disease (CVD) is the leading cause of death in patients with non-dialysis CKD, dialysis CKD as well as in kidney transplant recipients. CKD and CVD are intricately related; the overlap in risk factors makes the task of separating these two disease clusters rather difficult, if not impossible. Furthermore, the number of CVD risk factors increases proportionately with the severity of CKD; in fact, all patients with Stage 4–5 CKD have at least two or more CVD risk factors [33]. Not all facets of the CKD-CVD connection are well-understood.
5.1 CKD as a Sentinel for CVD Risk
Both biomarkers of CKD, reduced eGFR and abnormal urinary albumin excretion, are risk factors for ESKD as well as CVD morbidity and mortality [26, 34].
Albuminuria has been validated as a surrogate end point for the progression of CKD and it is estimated that a 30% reduction in the urinary albumin excretion results in a 23.7% reduction in the risk of progression to ESKD [35]. Similarly, Albuminuria has also been validated as an independent risk factor for cardiovascular and all-cause mortality [36,37,38]; it is a predictor of CVD and all-cause mortality in patients with DM or HTN, and even in non-diabetic normotensive individuals [39, 40]. For example, in a cohort of patients who had elective percutaneous coronary angiogram and revascularization, 11% of patients with macro-albuminuria (stage A3) met the primary endpoint of cardiac death or myocardial infarction after a median follow-up period of 1564 days, compared to 8% in the micro-albuminuria group (stage A2) and 3% in the normal-albuminuria group (stage A1) (p-value 0.004) [41]. Furthermore, a reduction in the rate of urine albumin excretion decreases the risk of CVD [42].
Reduced eGFR, especially at levels less than 60 mL/min/1.73 m2, has also been validated as an independent cardiovascular and all-cause mortality risk factor [36, 37, 43,44,45] and a patient with CKD is 16–40 times more likely to die than to reach ESKD, with the risk of CVD and death increasing proportionately with worsening stage of CKD [19, 46, 47]. For example, CKD is associated with a higher risk of mortality, estimated at 51%, 1 year after a myocardial infarction (MI), when compared to a 36% mortality risk in non-CKD patients [48]; the two-year mortality rate is 43% for non-CKD patients, 54% for CKD Stage 1–2 patients and 70% for Stage 4–5 patients [7]. Amongst patients who have their first acute myocardial infarction (AMI), there was a graded and proportionate association between eGFR decline/CKD stage, even when the CKD was mild/Stage 2, and risk of all-cause mortality, cardiovascular mortality, myocardial re-infarction, HF, cardiac arrest, or stroke [49]. Thus, CKD with a reduced eGFR, is a coronary heart disease risk equivalent, which means that a stage 3–5 CKD patient has a 10-year risk of coronary death or MI equivalent to that of patient who has already had an MI (>20%) [50]. Many guidelines currently incorporate risk stratification and risk calculators to guide initiation of a certain pharmacological therapy; thus, eGFR and albuminuria ought to be incorporated into any novel clinical prediction model aimed at quantitating and treating CVD risk in any patient with CKD [51]. Hardly any risk calculators have incorporated eGFR or urine albumin excretion rate at this time in their prediction models; for example, the only calculator that does so is the Joint British Societies (JBS3) risk calculator, which uses the presence or absence of CKD as a prediction variable in their model, but does not account for the stage/severity of CKD or albuminuria [52].
5.2 CVD Phenotypes in CKD
CVD in the CKD population can manifest as one of several phenotypes such as left ventricular hypertrophy (LVH), acute MI or atherosclerotic heart disease (AHD), heart failure (HF), valvular disease, atrial fibrillation, pulmonary hypertension, sudden cardiac death due to a cardiac arrest or an arrhythmia, or cerebrovascular accident (CVA). There are several pathophysiologic pathways that may explain the CKD-CVD connection, and fortunately, kidney transplantation not only stops but also reverses many of these processes.
-
1.
There is accelerated obstructive AHD with a staggering 5–20 fold increased risk compared to non-CKD individuals, 38–62.5% of incident ESKD patients starting dialysis have established coronary artery disease (CAD) and 36% have HF [53,54,55]. In a prospective cohort of 24 incident HD patients, a surveillance coronary angiogram after 1 month of initiating HD showed that 62.50% (15/24) had AHD/CAD and 45.8% had multi-vessel disease (4/24 or 16.7% had single vessel disease, 5/24 or 20.8% had two-vessel disease, and 6/24 or 25.0% had three-vessel disease) with 46.9% of the lesions detected being complex and 29.0% being diffuse [56].
Furthermore, coronary yellow plaques in patients with CKD seem to occur more frequently [57] and to be different in composition from non-CKD patients and have thin-cap fibroatheromas with more calcium and cholesterol crystals with a higher risk of thrombogenicity, plaque rupture [58] and intra-plaque hemorrhage and neo-angiogenesis [59].
When DM and CKD coexist, the cumulative risk for CVD mortality is additive, with CKD being the major contributor for the risk accrued. In NHANES III participants, CKD with eGFR category G3-G5 or stage 2–3 albuminuria was present in 9.4% of those with no DM and in 42.3% of those with DMT2; the 10-year cumulative all-cause mortality was 7.7% in participants without either condition, 11.5% in participants with DMT2 but no CKD, and a staggering 31.1% in patients with both DMT2 and CKD, with similar trends whether the mortality is cardiovascular or not [60].
-
2.
CKD patients are at risk of development of systolic and diastolic dysfunction and secondary complications such as HF. CKD is associated with structural and functional myocardial changes such as LVH and cardiac fibrosis with a secondary decline in left ventricular (LV) function and in myocardial tolerance to ischemia.
Many risk factors, such as anemia, elevated BP and volume overload, conglomerate to result in LVH in patients with CKD. Importantly, LVH (or an increased left ventricular mass index, LVMI) is an independent predictor of all-cause mortality, cardiovascular-mortality and cardiovascular events such as HF, ischemic heart disease, cardiac arrhythmias and sudden cardiac death [61, 62] and it is the most common phenotypical abnormality in ESKD [63].
The CRIC study investigators evaluated serial echocardiograms in a total of 190 patients with stage 4–5 non-dialysis CKD initially upon enrollment, and later after progression to ESKD requiring RRT (HD or PD) (mean time between 2 echocardiograms 2 years), and detected an increase in systolic dysfunction reflected by a significant decline in LVEF but no significant change in LVH or LVMI [64]. In a cohort of 254 asymptomatic patients with ESKD on dialysis therapy, 26–48% had evidence of systolic dysfunction assessed by abnormal myocardial contractility on echocardiography (e.g. LVEF) [65].
Finally, the increased risk of diastolic dysfunction measured by an E/A ratio on echocardiography in CKD patients predicts HF risk in the is population; HF risk increases by two-fold when E/A ratio is less or equal to 0.75 compared to a ratio of 0.75–1.5 [62].
-
3.
CKD patients have enhanced vascular calcification and stiffness due to arterial medial smooth muscle cell calcifications; they also develop atherosclerotic, plaque, neo-intimal calcification, a finding also proportional to the severity of CKD [55]. These abnormalities may manifest with a wide pulse pressure, treatment-resistant HTN or isolated systolic HTN. The finding of calcified atherosclerotic lesions in large-conduit arteries and the increased stiffness of large capacitive arteries gain significant clinical relevance as contributors to CVD and predictors of mortality in CKD patients [63].
For example, in a cohort of patients aged 30–65 years with non-dialysis CKD, increased coronary-artery calcification (CAC) risk was detected in patients with stage 3–5 CKD but not stage 1–2 CKD; the CAC risk was most pronounced, a substantial nine-fold higher, among diabetics with stage 3–5 CKD when compared to diabetics with no CKD [66]. Total CAC score predicted the number of affected coronaries, and single-vessel CAC score predicted the degree of stenosis [67]. As to ESKD requiring dialysis (HD or PD), a cohort of young patients (age 7–30 years) detected a high CAC score by electron-beam computed tomography (EBCT) in patients who were older than 20 years or who had a higher dialysis vintage (p < 0.001) when compared to healthy controls; for example, 87.5% (14 out of 16) of patients aged 20–30 years had CAC which was progressive, but none of those younger than 20 years had CAC [68]. CAC score is an independent predictor of mortality amongst patient with ESKD on dialysis [69, 70], but not in patients with mild to moderate CKD [71].
Based on the current evidence, using an EBCT CAC score as a sole diagnostic tool to predict or diagnose AHD may have a role in the general population or non-dialysis patients, but has no current role in patients with ESKD on dialysis due to a low accuracy, a significant variability in sensitivity/specificity depending on the CAC score cutoff chosen, and failure to correlate with the severity of coronary stenosis [72,73,74].
-
4.
Acute or chronic inflammation, increased oxidative stress, and protein energy wasting are prevalent in patients with CKD and are associated with a sequence of undesirable events such as endothelial dysfunction and protein-calorie malnutrition; biomarkers of inflammation and malnutrition have been shown to correlate with CVD risk or mortality risk [75,76,77].
For example, in a cohort of 840 patients with stage 3–5 CKD (eGFR 12–55, 96% non-diabetic) followed over a median duration of 125 months, a C-reactive protein (CRP) level at 3 mg/L or more was an independent risk factor for cardiovascular mortality and independently predicted a 56% increase in all-cause mortality; while serum albumin was not an independent risk factor for cardiovascular mortality, each 0.1 g/dL increment independently predicted a 6% decline in for all-cause mortality [76]. Similarly, patients with ESKD on hemodialysis have CRP levels that are 5–10 times higher than non-CKD controls [78], and a CRP level exceeding 10 mg/L at three or 6 months or on both occasions after initiation of hemodialysis was associated with a higher cardiovascular as well as non-cardiovascular mortality when compared to patients with a normal CRP over a five-year followup, the risk was highest in patients who had an elevated CRP on both occasions [79].
Many inflammatory biomarkers have been evaluated in CKD patients over the years, such as homocysteine, fibrinogen, ceruloplasmin, pro- and counter-inflammatory cytokines, CRP, and ESR, but their role in clinical practice remains very limited.
-
5.
In patients with stage 3–5 CKD, there is an increased risk of sudden cardiac death that is proportional to the severity of CKD [80].
5.3 CVD in ESKD + RRT
The most striking association between CKD and CVD can be illustrated in patients with EKSD on RRT with dialysis, where CVD accounts for 53.1% of mortality and is attributed to sudden cardiac death (cardiac arrest, arrhythmia) in 37%, acute MI and AHD in 6.7%, HF in 5.8%, CVA in 3.1% and other cardiac causes in 0.5% [7]. Furthermore, the risk of pulmonary hypertension increases proportionately with dialysis vintage [53, 54].
ESKD and dialysis seem to be associated with an additional flurry of increased CVD risks such as the aforementioned AHD, LV changes, repeated cardiac stress and ischemia in patients receiving HD, autonomic dysfunction, steep electrolyte and volume shifts, uremic ambience, all of which may contribute to this significantly increased risk of sudden cardiac death and cardiovascular mortality [81, 82]. For instance, ESKD patients with no evidence of any significant coronary occlusive disease, experience repetitive myocardial ischemia during hemodialysis, evidenced by sharp global as well as segmental reductions in myocardial blood flow, and some of these reductions are associated with regional wall motion abnormalities [83]. Finally, a patient with ESKD on dialysis who develops a first AMI, has an all-cause mortality risk of 59.3% at 1 year, 73.0% at 2 years, and 89.9% at 5 years, and a cardiac mortality risk of 40.8% at 1 year, 51.8% at 2 years and 70.2% at 5 years [84].
Based on this evidence, it is worth noting that a unique and atypical cardiovascular risk profile (e.g. intermittent and/or chronic volume overload, aberrant mineral metabolism, cardiovascular including valvular and coronary calcifications, chronic inflammation and malnutrition) in patients with ESKD on RRT with dialysis outcompetes the traditional cardiovascular risk factors responsible for CVD in non-dialysis CKD and non-CKD patients, and likely accounts for the excessive mortality in this patient group. This may also offer an explanation as to why standard pharmacological agents used for CVD secondary prevention, such as HMG-CoA reductase inhibitors, have a very limited benefit, if any, in patients with ESKD.
6 Diagnostic Challenges of CVD in CKD Patients
6.1 Atypical Clinical Manifestation of CVD
A major challenge in the CKD population is that the clinical manifestations of CVD are different and atypical, they may be subtle or not apparent at all, and this often leads to missed or delayed diagnosis.
For example, patients with Stage 3b-5 CKD are 3.82 times more likely to manifest their AHD suddenly with an AMI rather than with any typical warning symptoms of angina (e.g chest or arm or shoulder or neck pain) when compared to patients with a normal eGFR [85], and were more likely to experience shortness of breath than non-CKD patients [86].
Similarly, in a retrospective analysis comparing 3049 patients with ESKD on HD to 534,395 matching non-dialysis patients, all of whom were hospitalized and diagnosed with an AMI during their hospital stay, an admission diagnosis of AMI was missed in 44.8% of dialysis patients compared to 21.2% of the non-dialysis group, the typical symptom of chest pain was a presenting symptom in 44.4% of dialysis patients and 68.3% of the non-dialysis group, and finally the typical electrocardiographic abnormality of ST segment elevation was present in 19.1% of dialysis patients and 35.9% of the non-dialysis group [87]. In one cohort of 24 patients with incident EKSD starting HD, the presence of significant occlusive AHD was confirmed by coronary angiogram in 53.8% of patients without any symptoms (and in 72.7% of those with symptoms) [56].
6.2 Cardiac Biomarkers and Diagnostic Tools
Another challenge is that some standard non-invasive cardiac diagnostic tools have been validated in the general population to detect a CVD rooted in traditional risk factors, but may not offer any adjustments for the non-traditional risk factors and thus may be of limited utility in this population.
Cardiac biomarkers, routinely used to assist in the diagnosis of AMI or HF may be elevated in asymptomatic patients with CKD due to reduced eGFR and clearance or structural heart disease rather than true myocardial damage or fluid overload, thus reducing their diagnostic specificity. Despite such observations, numerous studies have validated high-sensitivity cardiac troponin T and natriuretic peptides as biomarkers that enhance CVD prediction in CKD patients [88].
-
In a cohort of 18 asymptomatic hemodialysis patients, 72% had at least one high creatinine kinase (CK) and 88–100% had at least one elevated MB isoenzyme (CK-MB) levels when serial testing was done over a 36-month period [89].
-
A rising level of cardiac troponin followed by a later decline, along with a suggestive clinical picture is highly suggestive of an acute coronary syndrome in patients with CKD; in contradistinction, a persistent and stable high level of cardiac troponin is more consistent with a “troponin leak” due to volume overload, or structural heart disease due to poorly controlled HTN or systolic/diastolic dysfunction or LVH [90]. It must be noted, however, that a steady troponin T elevation is associated with an increased risk of cardiovascular as well as all-cause mortality in asymptomatic dialysis-CKD patients; said mortality risk is incremental and starts at levels equal to or exceeding 0.01 ng/mL and patients with a level exceeding 0.10 ng/mL have double the mortality rate of patients with a lower level. Troponin I is less reliable in the CKD patient population due to variable cut-off values in clinical trials and lack of unified assay standardization [74].
In a systematic review of the role of troponin in patients with non-dialysis CKD (ND-CKD) and suspected ACS, the sensitivity and specificity were 71–100% and 31–86% respectively for troponin T, and 43–94% and 48–100% for troponin I. Elevated levels of either isozyme predicted higher risk for cardiac events and short-term mortality; only elevated troponin I predicted long term mortality, it also carried a worse prognosis in patients with advanced CKD [91].
A similar review in patients with CKD but without suspected ACS reported that an elevated troponin level in dialysis patients carried an increased risk for cardiovascular as well as all-cause mortality. An elevated troponin T was associated with an adjusted hazards ratio of 3.0 for all-cause mortality and 3.3 for cardiovascular mortality, an elevated troponin I was associated with an adjusted hazards ratio of 2.7 for all-cause mortality and and 4.2 for cardiovascular mortality. Similar findings were reported in ND-CKD patients [92].
-
As far as stress testing, stressing the myocardium with exercise may not be possible in some patients, and use of electrocardiogram (ECG) may be hindered by baseline abnormalities in others. For example, in a cohort of 30 patients with Stage 5 CKD about to start RRT, who were asymptomatic and had no cardiac or anginal symptoms or prior MI, subclinical and occult significant AHD (more than 50% narrowing in 1 or more coronary arteries) was detected by coronary angiography in 53.3% (16/30, 10/16 had single-vessel disease, 4/16 had two-vessel disease, 2/16 had three-vessel disease) of the patients; five patients had >90% luminal narrowing and underwent dipyridamole stress cardiac scintigraphy with a sensitivity of 40% (two patients had a positive test and three had a negative test) [93].
Similarly, amongst 45 kidney-transplant candidates with ESKD who had screening for AHD with dipyridamole single photon emission computed tomography (SPECT) thallium imaging and with a coronary angiogram, the latter diagnosed significant AHD (more than 50% narrowing in 1 or more coronary arteries) in 42% of the patients; thallium imaging had a lower sensitivity (37%) than in the control non-ESKD population, falsely diagnosed seven patients with AHD (negative coronary angiogram for any stenosis >50%), and most significantly missed diagnosing AHD (detected by coronary angiogram) that resulted in five out of the six cardiac deaths during the study followup duration of 25 months [94].
In 66 asymptomatic hemodialysis patients who had simultaneous high-dose dipyridamole and symptom-limited exercise stress echocardiography and stress myoview , combined pharmacological and exercise echocardiography had a 92% accuracy (sensitivity 86%, specificity 94%) at detecting myoview cardiac ischemia, and both tests were accurate (echocardiography 84%, myoview 91%) at detecting CAD confirmed by an angiogram [95].
A meta-analysis confirmed that among kidney transplant candidates, with diabetic or non-diabetic ESKD, a positive myocardial perfusion study, either dobutamine stress echocardiography (DSE) or a nuclear myoview with thallium scintigraphy, predicted an increased risk of AMI (RR 2.73) and of cardiovascular mortality (RR 2.92) [96].
Finally, a 2012 “American College of Cardiology Foundation (ACCF)/American Heart Association (AHA)” scientific statement for “Cardiac Disease Evaluation and Management Among Kidney and Liver Transplantation Candidates” pooled data from clinical trials which compared results of cardiac stress testing (DSE or MPS) to coronary angiography findings in patients with stage 5 CKD (GFR < 15 mL/min/1.73 m2 or dialysis) and calculated that DSE had a sensitivity of 44–89% and a specificity of 71–94%, MPS had a sensitivity of 29–92% and a specificity of 67–89% for identifying at least one coronary occlusion of 70% or more. The statement concludes that DSE may be “somewhat superior” [74].
As mentioned earlier, the use of EBCT CAC score has no established role at this time as a stand-alone diagnostic tool in assessing cardiovascular risk in patients with CKD [74].
6.3 Underutilization of Evidence-Based Therapeutic Interventions
A further challenge is that CKD patients with CVD tend to be historically under-treated; for example, patients with Stage 3b-5 CKD who had an AMI were less likely to receive pharmacological therapy with anti-platelet agents, beta-blockers or HMG CoA-reductase inhibitors or coronary re-vascularization than others [49]. Although a more recent analysis of trends in providing evidence-based care for CVD shows an improvement in all CKD stages, underuse of evidence-based pharmacological therapy remains a significant problem [97].
Similarly, patients with ESKD on dialysis who are diagnosed with an AMI are less likely have coronary reperfusion interventions due to eligibility exclusions based on parameters such as contraindications to thrombolytic therapy, kidney failure or a poor quality of life. They were also less likely to have coronary bypass graft surgery or to receive standard pharmacological therapy than non-dialysis patients [87].
6.4 Therapeutic Interventions Have a Lower Success Rate
Yet another challenge is that patients with CKD have less successful outcomes and higher mortality than non-CKD patients, and this may discourage healthcare providers from pursuing invasive cardiac diagnostic and therapeutic interventions.
For example, in a cohort of 5244 patients with ST-elevation acute MI (STEMI) who underwent primary percutaneous coronary intervention (PCI) found that patients with lower eGFR had a higher mortality rate and were less likely to achieve desired angiographic outcomes such as post-intervention TIMI flow grade or ST-segment elevation resolution [98].
Similarly, studying temporal trends shows that among 12,087 patients diagnosed with acute MI between 1985 and 2008, although patients with stage 4–5 CKD had a decline in 30-day mortality over the two decades studied reflecting improved MI care, the outcomes for these patients remained quite poor: median survival was only 1.8 years for patients with stage 4–5 CKD, compared with 8 years for stage 3 CKD, 15 years for stage 2 CKD, and 20 years for normal kidney function [97].
6.5 Delaying Diagnostic and Therapeutic Interventions Over Concerns of Contrast Nephropathy
A final challenge is the timing of a coronary angiogram, when indicated for diagnostic or therapeutic purposes in patients with CKD ; many a time, the angiogram is put off over concerns of AKI and worsening CKD.
The European Renal Best Practice (ERBP) guidelines for managing patients with diabetic stage 1-3a CKD recommend that a clinically indicated coronary angiogram should not be delayed for concerns over contrast induced nephropathy (CIN) .
CIN is the end result of contrast induced tubular toxicity, intense vasoconstriction and tubular as well as medullary ischemia, and oxidative stress [99]. Risk factors for CIN include pre-existing CKD, DM, effective arterial volume depletion especially in patients on diuretics, HF and reduced LVEF, hypotension and age. Prevention of contrast nephropathy after a coronary angiogram is a constant cause for nephrology consultations. Thus, several prediction models have been devised and validated but none reported their impact on clinical decision-making or patient outcomes [100]. Strategies to prevent contrast induced nephropathy include isotonic fluid resuscitation with sodium bicarbonate or normal saline to maintain optimal effective arterial volume and avoid volume depletion, using iso-osmolal contrast agents, minimizing the volume of contrast used and avoiding repetitive administration over a short time-frame, oral N-acetylcysteine, and an oral statin [101]. Furthermore, it may be advisable to stop RAAS inhibition 1–3 days before the administration of the contrast; a pilot study Cerebrolysin Asian Pacific trial in acute brain injury and neuro recovery (CAPTAIN trial) in patients with moderate CKD (serum creatinine ≥1.7 mg/dL within 3 months or creatinine ≥1.5 mg/dL within 1 week prior to angiogram) demonstrated a non-significant reduction in CIN and a significantly lower rise in serum creatinine after the angiogram [102].
6.6 Guidelines
The 2012 American College of Cardiology Foundation (ACCF)/American Heart Association (AHA) scientific statement for “Cardiac Disease Evaluation and Management Among Kidney and Liver Transplantation Candidates” recommends that asymptomatic advanced-CKD patients who are enlisting for a kidney transplant be risk stratified and considered for non-invasive cardiac stress testing accordingly, even if they have a functional status equal to or exceeding 4 metabolic equivalent tasks (METS); with a recommendation to proceed with such testing if the patient has three or more of the following risk factors: age over 60 years, dialysis vintage exceeding 1 year, prior history of CVD, LVH, DM, HTN, dyslipidemia, and active tobacco use.
This guideline echoes prior recommendations from the 2007 report of the Lisbon conference, the 2005 NKF/KDOQI Guidelines, 2001 American Society of Transplantation (AST) Guidelines , and the 2000 ERBP, with one difference that the NKF/KDOQI and the AST recommend periodic stress testing in all diabetic patients irrespective of lack of any symptoms.
The scientific statement did not find adequate evidence to make a recommendation for repeated and periodic testing for myocardial ischemia while on the kidney transplant waiting list.
The statement found it reasonable to perform an echocardiogram to evaluate for pulmonary hypertension, and if present, to investigate for secondary causes; if right ventricular systolic pressure exceeds 45 mmHg then a right heart catheterization is warranted and if pulmonary HTN is confirmed than referral for advanced vasodilator therapy ought to be initiated [74].
7 Management of Traditional CVD Risk Factors in CKD
7.1 Blockade of the Renin Angiotensin Aldosterone System
Aberrations in the systemic or local renin-angiotensin-aldosterone system (RAAS) accelerate AHD, HTN, inflammation, promote the development of metabolic syndrome at the center of which are insulin resistance and obesity [103] while at the same time accelerating eGFR decline and urinary albumin excretion rates. Angiotensin II (Ang II) and aldosterone play an important role in the genesis and progression of both CKD and CVD.
Pharmacological therapy with RAAS blockade in the CKD patient population reduces the rate of albumin excretion, decelerates the progression of CKD, and thus the development of ESKD; while observational studies also report a resultant reduction in all-cause and cardiovascular mortality rate, a systematic review detected such a trend but the benefits did not meet statistical significance [104].
Most best practice guidelines recommend an angiotensin converting enzyme inhibitor (ACEi) or an angiotensin II receptor blocker (ARB) as first line antihypertensive therapy for systemic arterial hypertension, including patients with non-dialysis CKD, micro- or macro-albuminuria, and secondary prevention of cardiovascular disease such as HF and CAD.
7.1.1 RAAS Inhibition in ESKD
In patients with dialysis-CKD receiving RRT, therapy with an ACEi or an ARB, results in a progressive regression in LVH, as assessed by left ventricular mass index (LVMI) [105, 106]; long term use of ARB (>365 days) significantly reduces the incidence of major cardiovascular events (including AMI, CAD requiring coronary stenting or percutaneous transluminal coronary angioplasty (PTCA), peripheral artery disease (PAD) requiring PTCA, and acute CVA among dialysis-CKD patients with no prior history of a major cardiovascular event and protective effect was directly proportional to the cumulative prescription days of ARB.
ACEi or ARB therapy in patients receiving RRT with continuous ambulatory peritoneal dialysis (CAPD) provides a significant and similar benefit on preserving residual kidney function with long-term therapy (≥12 months) with wither class; however, one randomized controlled trial (RCT) pooled in this meta-analysis evaluated the effect of ACEi therapy on cardiovascular events and mortality when compared with other anti-hypertensive agents and reported no significant differences [107]. The results of this meta-analysis are concordant with prior published literature [108].
In conclusion, we recommend the initiation of RAAS inhibition with an ACEi or an ARB in patients with ESKD receiving HD or PD for antihypertensive therapy, prevention of major cardiovascular events, and preservation of residual kidney function. Aldosterone receptor antagonism (ARA) may be added for patients with treatment resistant hypertension (TRH) or with reduced LVEF (<35%).
7.1.2 RAAS Inhibition in Kidney Transplant Recipients
In kidney transplant recipients, the use of RAAS inhibition is usually preserved for the intermediate (1–4 months) and late (≥4 months) post-transplant period and avoided in the early post-transplant period (first month) due to the increased risk of hyperkalemia and worsening kidney allograft function [109, 110].
Therapy with an ACEi (captopril) or an ARB over a period of 27 months was associated with significant reductions in GFR, hematocrit and urinary protein excretion [110], but there was a paucity of evidence evaluating the long-term effect of RAAS inhibition on allograft survival, cardiovascular events or all-cause mortality.
Finally, therapy with ARB in patients with Interstitial fibrosis/tubular atrophy (IF/TA), a major cause of kidney transplant allograft loss, resulted in a significant decrease in the volume of the cortical interstitium when compared to placebo, but this pathological benefit failed to translate into any clinical endpoints on secondary analysis, namely time to a composite endpoint of doubling of serum creatinine, ESKD or death. However, there was a trend towards decreased incidence of all-cause ESKD with AIIT1RA therapy [111].
In conclusion, we suggest the use of RAAS inhibition with an ACEi or an ARB in kidney transplant recipients in the late post-transplant period, and in the intermediate post-transplant period if a compelling indication arises, for antihypertensive therapy, prevention of major cardiovascular events, slowing down progression of CKD, and proteinuria. ARA may be added for patients with treatment resistant hypertension (TRH) of with reduced LVEF (<35%).
7.1.3 CKD and Acute MI or HF
The use of an ACEi (Captopril) within 3–16 days after an acute myocardial infarction MI in patients whose LVEF was ≤40% and whose serum creatinine was <2.5 mg/dL reduced risk of future cardiovascular events [112].
In patients with HF due to decreased LVEF or valvular disease, there is a state of chronic renal hypoperfusion in the setting of an increased overall extracellular fluid volume; counter-regulatory adaptive mechanisms to restore perfusion result in neurohormonal activation of the RAAS, sympathetic nervous system and anti-diuretic hormone, the end result being more sodium and water retention and further volume expansion.
In patients with HF, kidney dysfunction portends a worse long-term prognosis with higher hospitalization rate [113] and a higher cardiovascular as well as all-cause mortality and the risk rises with the severity of the kidney disease [114, 115] with a 7% increase in mortality for every eGFR decrement of 10 mL/min per 1.73 m2 of body-surface area [116]. The renal impairment is a more powerful predictor of mortality in patients with advanced HF than the LVEF or New York Heart Association (NYHA) class [117] and its validity as a prognosticator does not change whether the HF is due to systolic or diastolic dysfunction [118]. Similarly, renal impairment predicts a higher all-cause mortality and cardiovascular mortality as well as recurrent myocardial infarction in patients who had an acute myocardial infarction especially with an eGFR <45 per 1.73 m2 of body-surface area [112, 119].
In patients with clinically diagnosed HF and angiographic evidence of coronary artery disease (CAD), ACEi reduces mortality at 12-months in patients with stage 1–2 CKD but not in those with more advanced CKD stage [120]. However, other trials have shown a survival benefit with ACEi in patients with HF across all strata of creatinine clearance and CKD stage [118].
In summary, ACEi are essential for secondary cardiovascular prevention in patients with HF and/or reduced LVEF; they help optimize cardiac function, decrease mortality as well as hospitalization rate. Furthermore, evidence from the Randomized Aldactone Evaluation Study (RALES) trials supports adjunctive aldosterone receptor antagonist therapy with spironolactone to decrease mortality and morbidity in patients with severe HF and a LVEF <35% [121]; similarly, the EMPHASIS-HF Study Group reported that adjunctive eplrenone therapy decreased mortality and morbidity in patients with NYHA class II HF and LVEF<35% [122].
7.1.4 Dual RAAS Blockade
While dual or multi-level RAAS blockade offers further lowering of BP as well as further reductions in urine albumin excretion rate, it may be associated with symptomatic hypotension and a higher risk of hyperkalemia and/or AKI [123].
-
1.
The Cardiorenal end points in a trial of aliskiren for type 2 diabetes (ALTITUDE) investigators evaluated the impact of adjunctive aliskiren therapy added to ACEi or ARB on cardiovascular and renal outcomes in patients with systemic arterial hypertension, DMT2 and with diabetic nephropathy (micro- or macro-albuminuria) or cardiovascular disease or both, stage 3 CKD, aged 35 years or older, and reported that addition of aliskiren resulted in a (statistically non-significant) trend with an increase in adverse primary composite outcome of cardiorenal events, secondary composite outcome of cardiovascular and renal events, and all-cause mortality; more patients in the treatment group experienced an adverse event and subsequently discontinued the direct renin inhibition (DRI) (p < 0.001) with he most encountered complications being hyperkalemia, acute kidney injury and hypotension. Dual therapy was associated with lower BP and urinary protein excretion rate [124].
-
2.
The Renal outcomes with telmisartan, ramipril, or both, in people at high vascular risk (ONTARGET) investigators showed a significant increase in the primary renal outcome (dialysis, doubling of serum creatinine, death) and secondary renal outcomes (dialysis, doubling of serum creatinine) and a significant decline in GFR (−6.11 mL/min, p < 0.0001) amongst patients with CAD, PAD, cerebrovascular disease or DM with target-organ damage who received dual therapy [125, 126].
-
3.
A meta-analysis of thirty-three RCTs evaluated the impact of long-term (> 1 year) dual RAAS blockade with an ACE-i and an ARB versus monotherapy on all-cause as well as cardiovascular mortality, and concluded that there was no benefit of dual blockade over monotherapy for either endpoint. Dual therapy resulted in a significant decrease in HF hospitalization rate (18% reduction), but there was a significantly higher risk of hyperkalemia (55% increase), hypotension (66% increase), AKI (41%) and adverse events leading to withdrawal of therapy (27% increase). Subgroup analysis showed a significantly higher risk of AKI with dual therapy in patients with HF as compared to those without HF, and a higher all-cause mortality in patients without HF when compared to those with HF [127].
-
4.
The risk-benefit of dual versus single RAAS blockade in patients with albuminuria or stage 3–5 CKD was evaluated in a meta-analysis of fifty-nine RCTs, and reported a statistically significant reduction in urinary albumin excretion rate with dual blockade, as well as a higher success rate at achievement of blood pressure goal; however, dual blockade was associated with a statistically significant reduction in GFR and a higher rate of hypotension and hyperkalemia and had no effect on mortality rates [128].
-
5.
The addition of spironolactone to an ACEi or an ARB, in patients with proteinuric stage 1–3 CKD, over a period of 2–20 months, reduced the degree of proteinuria and SBP but had no effect on cardiovascular outcomes or on the rate of progression to ESKD; it had a less well defined effect on eGFR but it increased the risk of hyperkalemia and gynecomastia. Individual trials report similar results with eplerenone; addition of eplerenone, too, increased risk of hyperkalemia but there was no risk of gynecomastia [129].
-
6.
The addition of a DRI or an ARB or and ARA to ACEi-based conventional therapy in patients with HF and its impact on mortality and cardiovascular event rate was evaluated in a meta-analyses of 16 RCTs (31,429 patients) over a period of 3 months. Only additional aldosterone receptor antagonists, and not DRI or an ARB, significantly reduced the risk of all-cause mortality, cardiovascular mortality, HF hospitalization but there was an increase in the rate of hyperkalemia. The addition of an ARB increased the rate of hyperkalemia, AKI and hypotension; additional DRI increased risk of hypotension [130].
In summary, while most trials report reduction in BP and urinary excretion rates, and in view of the increased risks of AKI, hyperkalemia, and symptomatic hypotension associated with dual or multilevel RAAS blockade, dual RAAS blockade should be preserved for clinical use where evidence rather than theory exists. Its major use is in patents with HF and reduced LVEF where aldosterone receptor antagonists offer a survival benefit [131].
7.2 Blood Pressure Control, Goals and Choice of Pharmacological Agents
HTN is a major CVD risk factor and is the second most common cause of ESKD; on the other hand, it is also a complication of CKD. Achieving BP goals is one of the cornerstones of any therapeutic plan aimed at primary and secondary prevention of CVD risk as well as slowing down the progression of CKD. One cannot over-emphasize that achieving goal BP, in itself, is a more important and reno-protective end-point than the choice of the BP lowering class or agent. However, the main challenge lies in the nuances of determining the ideal BP goal for different patient groups, such as patients with CKD of different stages, stage A2-A3 albuminuria, DM status, patients with AHD, elderly patients, ethnicity, etc…
7.2.1 Exclude Secondary Causes
As mentioned earlier, CKD is a cause as well as a complication of HTN. An evaluation for secondary causes of HTN, when warranted, must be pursued. For example, obstructive sleep apnea (OSA) is an under-diagnosed contributor to hypertension which may need to be evaluated when a clinical index of suspicion arises or if the patient has treatment-resistant hypertension.
7.2.2 What Is the Optimal BP Goal?
Non-pharmacological lifestyle modifications and pharmacological interventions should target a BP less than 140/90 mm Hg in all patients (regardless of age) with stage 1–5 CKD or DM according to Joint National Committee 2014 evidence-based guideline for the management of high blood pressure (JNC8) [132], and to levels less than 130/80 mm Hg in the presence of micro- or macro-albuminuria as per the 2012 KDIGO Clinical Practice Guideline for the Management of Blood Pressure in Chronic Kidney Disease [133]. A 2014 ERBP position statement endorsed the KDIGO guidelines for the management of BP in CKD patients [134].
While, the optimal level of blood pressure control in different patient populations continues to evolve, it is widely acceptable that controlling blood pressure (BP) to levels <140/90 mmHg has kidney as well as cardiovascular protective effects; as mentioned earlier, lower target BP levels have been recommended for patients with CKD, proteinuria >1 g per day, and cardiovascular disease. For example, the SPRINT research group evaluated the impact of two different systolic BP (SBP) goals on 9361 high cardiovascular-risk non-diabetic patients over a period of 3.26 years and reported that the group with more intensive SBP control (121.4 mm Hg versus 136.2 mm Hg) had a significantly lower all-cause mortality and a lower rate of the primary composite end point of AMI, other acute coronary syndromes, CVA, HF and death from cardiovascular disease. However, there was a significantly higher rate of hypotension, syncope, AKI, electrolyte abnormalities in the intensive treatment group [135].
7.2.3 Home BP Logs
All patients with HTN must be empowered and encouraged to keep a daily home BP log , which will assist the health care provider in evaluating the patient for white-coat hypertension as well as masked hypertension, and thus avoid a lot of potential complications of missing either diagnosis. This useful tool may also keep the patient engaged and involved in their care plan and may assist in achieving desired BP goals.
Home BP logs will also assist in the diagnosis of white coat hypertension as well as masked hypertension. A persistent discordance between home BP logs and office BP measurements should trigger a referral for 24 h ambulatory BP monitoring (ABPM).
7.2.4 Non-pharmacological Therapeutic Strategies
Non-pharmacological therapy consists of lifestyle modifications aimed at [132]:
-
1.
Adopting the Dietary Approaches to Stop Hypertension (DASH) diet which combines low-sodium, fruits and vegetables and low fat dairy products,
-
2.
Weekly aerobic physical activity for 150 min of moderate-intensity exercise every week or 75 min of high-intensity, or some combination, and most favorably spread over many week-days,
-
3.
Muscle-strengthening aiming to exercise all muscle groups in a moderate- to high-intensity workout at least twice a week,
-
4.
Moderate alcohol use (not to exceed one standard drink for women and two for men per day),
-
5.
Weight regulation (goal BMI 20–25 kg/m2) and
-
6.
Tobacco cessation.
7.2.5 Pharmacological Therapy
The ideal pharmacological agent to be used ought to help achieve BP goal, offer cardiovascular protection, reduce urine albumin/protein excretion rate, and slow down the progression of CKD all at the same time while being maximally tolerated by patients and having minimal adverse reactions.
Both ACEis and ARBs are recommended by many best-practice guidelines, as first line antihypertensive therapy for systemic arterial hypertension in patients with CKD (with the strongest evidence for benefit being in those with micro- or macro-albuminuria) and secondary prevention of cardiovascular disease such as HF and CAD, regardless of race, age, or diabetes status. Recommendations for use as first line therapy were made by the JNC 8 [132], KDIGO [133], National Kidney Foundation K/DOQI [136], American College of Physicians (ACP) [137], and ERBP [134] guidelines for treatment of systemic arterial hypertension in CKD. Such inhibition reduces albuminuria and slows down progression of CKD, with a BP-independent effect which offers more protection than can be accounted for by BP lowering alone. However, the bulk of clinical evidence at the core of these guidelines applies to patients with stages 1–3 CKD or with micro- or macro-albuminuria; evidence is scarce regarding its role in stages 4–5 CKD or patients with normal urinary albumin excretion rate [138].
In the kidney, AngII is a potent vasoconstrictor with preferential vasoconstrictive effects on the glomerular efferent arteriole; this effect plays a physiologic role in maintaining normal hydrostatic and glomerular filtration pressures. RAAS inhibition with an ACEi or an ARB, results in a more marked glomerular efferent arteriolar dilatation, which in turn, reversibly reduces the hydrostatic and glomerular filtration pressures. Thus, it is quite expected, as well as desirable, that such RAAS inhibition may result in a reversible rise in the serum creatinine and subsequently a decline in the eGFR; it is widely acceptable that such a change is not to exceed 30% from baseline within the first 2–4 weeks after initiation of therapy, especially when optimal BP goals are achieved. The magnitude of such a change in GFR and serum creatinine becomes more prominent clinically in patients with (1) decreased effective arterial blood volume due to conditions such as excessive diuresis, or low forward cardiac output due reduced left ventricular ejection fraction (LVEF), valvular disease, or heart failure (HF), and (2) adaptive glomerular hyper-filtration due to CKD or diabetic nephropathy where this compensatory effect is blunted by glomerular afferent arteriolar vasodilatation [139].
Diuretics should be prescribed for the majority of patients with CKD and HTN; they are second line therapy to ACE-i or ARBs in patients with stage A2-A3 albuminuria. In patients with stage 1–3 CKD, especially in the presence of increased extracellular fluid volume (ECF volume), (e.g. peripheral edema), a thiazide diuretic is indicated along with dietary sodium restriction to 1.5–2.0 grams daily and is thought to promote the effect of RAAS blockers on reducing urinary protein excretion; in more advanced stage 4–5 CKD, thiazides become less effective and thus a loop diuretic is preferred. When a diuretic is used, it is strongly recommended to evaluate patients for continued volume overload, volume depletion or hypotension or AKI, electrolyte disturbances especially hypomagnesemia and hypokalemia [140].
If goal BP is not achieved with the ACE-i or ARB and the diuretic, the addition of a non-dihydropyridine calcium channel blockers (non DHP-CCB), namely diltiazem or verapamil, offers further blood pressure lowering and an additional inherent anti-proteinuric effect [141]; either agent may be used in addition to ACE-i or ARBs or as first-line when a patient with albuminuria is intolerant to both RAAS blockers. Dihydropyridine calcium channel blocker (DHP-CCB) also offer further BP lowering effects but do not have any inherent anti-proteinuric effects, and thus, DHP-CCB should not be used as sole agents or first-line agents in patients with CKD and stage A2-A3 albuminuria [142, 143].
In patients with ESKD on HD, HTN and LVH, atenolol-based antihypertensive therapy was associated with a lower rate of serious cardiovascular events (AMI, stroke, hospitalization for HF, cardiovascular death) and all-cause hospitalization when compared to lisinopril-based antihypertensive therapy [144]; this may promote the use of beta-blocker therapy in this patient population but further studies reproducing similar results are needed.
Finally, in 2013, the KDIGO Blood Pressure Work Group published a “Clinical Practice Guideline for the Management of Blood Pressure in Non-Dialysis CKD” [133], the major recommendations are hereby listed:
-
1.
Customize goal BP and pharmacological therapy based on patient’s age, CKD risk, CVD risk, presence of retinopathy in patients with DM and monitor for any adverse reactions such as orthostatic dizziness and evaluate for orthostatic hypotension each clinical visit. Adopt lifestyle modifications as detailed earlier.
-
2.
Hypertensive patients (regardless of DM status) with no micro- or macroalbuminuria (stage A1) should target a goal BP is ≤140/90 mmHg.
-
3.
Hypertensive patients (regardless of DM status) with micro- (stage A2) or macro-albuminuria (stage A3) should target a goal BP is ≤130/80 mmHg with a regimen to include an ACE-i or an ARB.
-
4.
Hypertensive kidney transplant recipients should target a goal BP is ≤130/80 mmHg.
-
5.
In elderly patients, start pharmacological therapy, when needed, at the lowest dose possible, and increase dose slowly while always evaluating for safety and adverse reactions such as orthostatic hypotension, AKI, electrolyte imbalances.
Needless to say, many CKD patients have a higher than average daily pill burden; thus, to maximize compliance, it its essential to simplify the regimen as much as possible by minimizing the frequency of administration as well as number of pills (e.g. by using dose combinations) and ensuring that the medication is affordable.
7.3 Diabetes Mellitus and Optimal Glycemic Control
DM is the major cause of CKD worldwide. Kidney disease complicates diabetes in 25–40% after a course of 20–25 years and around one third of those patients develop ESKD requiring renal replacement therapy but the majority will die of cardiovascular causes before progression to ESKD [10]. Microalbuminuria in diabetic patients is a predictor of early cardiovascular mortality [145] with a two to four-fold increase in such risk with microalbuminuria, and an even higher risk in patients who have systemic arterial hypertension and macro-albuminuria [146]. In a cohort of 2097 diabetic participants in the NHANES 2009–2014, aged 20 years and over, diabetic nephropathy was present in 26.2% with 15.9% having stage A2 or A3 albuminuria and 14.1% having an abnormal eGFR; this data projects that as of 2014, 8.2 million Americans have diabetic CKD [11].
7.3.1 Blood Pressure Control and Drugs of Choice
Achieving BP goal in patients with DM and CKD is essential to reduce risks of CVD and progression to ESKD. Goal BP is determined by presence of micro- or macro-albuminuria where the goal BP is <130/80 mmHg; otherwise, goal BP is <140/90 mmHg.
In patients with DMT2 and diabetic nephropathy with stage A3 albuminuria, the Reduction of Endpoints in NIDDM with the Angiotensin II Antagonist Losartan Study (RENAAL) team, among many others, demonstrated that the ARB losartan significantly decreases the urine albumin excretion rate and slows down the progression of diabetic nephropathy after a mean follow-up of 3.4 years, albeit without a survival benefit and without a reduction cardiovascular morbidity and mortality, and with a beneficial effect independent and more than can be accounted for by the BP lowering effect alone [147]. Similar results were demonstrated by the Irbesartan Diabetic Nephropathy Trial (IDNT) team with he ARB irbesartan [143].
A Cochrane Database Systemic review of fifty RCTs highlighted the important concept that neither ACEi nor ARB had a significant effect on all-cause mortality in patients with diabetic CKD unless full-dose or maximum-tolerable dose was used with ACEi; both classes seem to be equally effective, three RCTs compared ACEi to ARB and found no difference in all-cause mortality between the two forms of therapy in diabetic kidney disease. Both forms of therapy resulted in a statistically significant reduction in the risk of ESKD and of progression from micro- to macroalbuminuria with a significant increase in regression from micro- to normaalbuminuria [146].
7.3.2 Glycemic Control
Glycemic control plays an essential role in preventing diabetic microvascular (retinopathy, neuropathy and nephropathy), and has a less clear role in preventing macrovascular (CAD, PAD, CVA) complications.
In DMT1, The Diabetes Control and Complications Trial (DCCT) group randomized 1441 patients to intensive therapy versus conventional therapy and reported, after a mean duration of 6.5 years, a significant reduction in the incidence (by 76%) or progression (by 54%) of retinopathy, as well as a significant reduction in the onset of microalbuminuria (by 39%) and macro-albuminuria (by 54%), and a decrease in the incidence of clinical neuropathy (by 60%) [148]. The DCCT/Epidemiology of Diabetes Interventions and Complications (DCCT/EDIC) Study Research Group followed 93% of the original DCCT cohort for an additional mean 17 years, and reported a 42% reduction of any CVD events (macrovascular), as well as reductions in fatal and non-fatal MI and mortality in the intensive therapy group [149, 150].
In DMT2, several major trials have confirmed that tight glycemic controls reduces microvascular complications; for example, the UK Prospective Diabetes Study (UKPDS) Group evaluated 3867 incident DMT2 patients over a 10 year period and found that a more intensive glycemic control (HbA1c 7.0%) reduced the risk of microvascular complications, mainly retinopathy, by 25% when compared to conventional glycemic control (HbA1c 7.9%), but there was no statistically significant reduction in macrovascular complications [151].
Similarly, the Action in Diabetes and Vascular Disease: Preterax and Diamicron Modified Release Controlled Evaluation (ADVANCE) Collaborative Group evaluated 11,140 patients with DMT2 over a median follow-up period of 5 years and reported that intensive glycemic control (mean HbA1c 6.5%) reduced the rate of microvascular complications, namely incidence of nephropathy (HR 0.79) when compared to standard glycemic control (mean HbA1c 7.3%), but had no effect on the rate of retinopathy and offered no benefit as far as macrovascular complications [152]; among 8494 patients who had continued post-trial followup for an additional median of 5.4 years and for whom HbA1c differences between the two groups have dissipated by the first post-trial visit after a median of 2.9 years, there remained a benefit of reduced ESKD in the intensive control group albeit relatively few events were reported [153].
Finally, the ACCORD trial group randomized 10,251 patients with DMT2 to intensive glycemic control (median HbA1c 6.4%) versus standard control (median HbA1c 7.5%) and had to transition all patients in the intensive-control arm of the trial to standard control after a median followup of 3.4 years due to increased cardiovascular as well as all-cause mortality rates in the intensive-control group, followup was continued for 5 years and there was a significant delay in the onset of albuminuria in the intensive-control group at the time of the transition as well as at the time of the trial completion [154].
It’s worth noting that all the above trials showed a higher risk of hypoglycemia with more intensive protocols.
7.3.3 American Diabetes Association (ADA) Standard of Medical Care in Diabetes
The American Diabetes Association (ADA) issued a periodic revision of the “Standard of Medical Care in Diabetes” and its most recent recommendations are summarized in Table 8.1 [155].
7.3.4 European Renal Best Practice (ERBP) Guidelines for Managing Patients with DM and Stage 1-3a CKD
The European Renal Best Practice (ERBP) guidelines for managing patients with DM and stage 1-3a CKD (GFR > 45 mL/min per 1.73 m2 BSA) provide the following recommendations for primary and secondary prevention and treatment of cardiovascular disease [156]:
-
1.
A clinically indicated coronary angiogram should not be delayed for concerns over contrast induced nephroapthy.
-
2.
Medical therapy for stable CAD should be optimized and is the preferred choice of therapy unless there is significant myocardial ischemia, proximal left anterior descending (LAD) or left main coronary disease is present.
-
3.
In patients with multi-vessel CAD or complex lesions, coronary artery bypass graft is preferred over percutaneous coronary interventions for revasularization.
-
4.
Neither the presence of DM nor that of CKD should impact the therapy of acute coronary syndrome.
-
5.
Maximal dose ACEi, and not an ARB, is the treatment of choice for secondary prevention of cardiovascular disease in patients with HF or CAD; combination RAAS inhibition should be avoided.
-
6.
Goal BP is <140/90 mmHg and in the absence of micro-albuminuria all anti-hypertensive agents are equal to lower BP.
7.3.5 European Renal Best Practice (ERBP) Guidelines for Managing Patients with DM and Stage 3b-5 CKD
Similarly, the ERBP issued guidelines for managing patients with DM and stage 3b-5 CKD (GFR < 45 mL/min per 1.73 m2 BSA) provide the following recommendations [156]:
-
1.
HbA1c remains the recommended diagnostic tool to monitor long-term glycemic control in patients with stage 3b-5 CKD, although its accuracy may be diminished by the effect or uremic toxins (higher than expected HbA1c), decreased RBC survival in more advanced CKD or increased erythropoiesis when an erythropoiesis stimulating agent (ESA) or iron is used (lower than expected HbA1c).
-
2.
Setting a goal HbA1c must be customized to each individual patient and weighed against their risk of hypoglycemia, a risk which increases with severity of CKD.
-
2a.
The risk of severe hypoglycemia (i.e. patient requires assistance for management) is high in patients with stage 5 CKD or hepatic failure or gastroparesis, or in patients receiving insulin or long-acting sulfonylurea with active metabolites.
-
2b.
Moderate risk for hypoglycemia is seen in patients prescribed short acting sulfonylureas or sulfonylureas with inactive metabolites or meglitinides.
-
2c.
Low risk for hypoglycemia is seen in patients taking the biguanide metformin, alpha glucosidase inhibitors, dipeptidyl peptidase IV (DPP-4) inhibitors, incretin mimetics such as glucagon-like peptide-1 (GLP-1) receptor agonists, thiazolidinediones, and Sodium-glucose co-transporter-2 (SGLT2) inhibitors.
-
2d.
Hypoglycemia risk must be avoided, and if risk is high, this may necessitate adopting more liberal goals for glycemic control with a HbA1c ≤ 8.5%; such a liberal goal may also be suitable for patients with a reduced life expectancy, established cardiovascular (macrovascular) disease or micro-vascular complications, poor motivation; yet, continued vigilant efforts must be made to achieve such a goal if the HbA1c is higher. If a patient is high risk for hypoglycemia, then more frequent self-monitoring is required.
-
2e.
In patients who are on non-pharmacological lifestyle modifications or on pharmacological therapy with low risk for hypoglycemia, a goal HbA1c of ≤7.0% is recommended.
-
2f.
In patients with a DM vintage exceeding 10 years and who are on pharmacological therapy with moderate risk for hypoglycemia, a goal HbA1c of ≤8.0% is recommended.
-
2g.
For patients who do not fit into any of the previous categories, a goal HbA1c of ≤7.5% is recommended.
-
2a.
-
3.
Metformin continues to be first line therapy in DM, after life style modifications, and dose must be reduced as CKD progresses and should be used with extreme caution in stage 4 CKD and must be stopped in stage 5 CKD; empower patient and provide printed educational reminders to hold metformin if any AKI risk develops such as with volume depletion (e.g. recurrent vomiting or diarrhea) or administration of IV contrast, and continue to hold until a time when the risk disappears. If additional pharmacological therapy is needed, then additional medications which are low-risk for hypoglycemia may be added.
-
4.
When a coronary angiogram is indicated, it should not be omitted for the sole concern of contrast-induced nephropathy.
-
4a.
In patients with stable AHD/CAD, maximal medical therapy is preferred, unless there is significant left main coronary or significant proximal LAD disease for which an elective CABG is the treatment of choice.
-
4b.
In patients with mutlivessel or complex disease, CABG is favored over PCI.
-
4c.
In patients with an acute MI, treatment strategies should not be any different from those offered to patients with DM/no-CKD or stage 1-3a CKD/no-DM. In patients with STEMI, primary PCI, whenever available in a timely fashion, is preferred over thrombolytic therapy. In patients with non-STEMI and left main disease or multi-vessel disease, CABG is associated with better outcomes and lower mortality rate when compared with PCI.
-
4d.
Dose of thrombolytic therapy must be adjusted by severity of CKD and eGFR level.
-
4a.
-
5.
Treat patients with HF or ischemic heart disease with ACE-i at maximal dose tolerated; evidence to use ARB in these patients is lacking and combining ACE-i, ARB or DRI must be avoided.
-
6.
Treat patients with lipophilic (rather than hydrophilic) selective-beta blockers as these agents may decrease the risk of sudden cardiac death.
-
7.
Avoid lower BP goals than in the general population (<140/90 mmHg) as some patients may have autonomic dysfunction and orthostasis. In the absence of albuminuria, all BP lowering meds may be used equally.
-
8.
Recommend start a statin in patients with stage 3b-4 CKD and consider doing so in stage 5 CKD; use a fibrate if patient is intolerant to statin.
-
9.
Advise patients to adopt an individualized and regular exercise program to achieve goal body mass index (BMI), build muscle mass and reduce body fat and improve quality of life.
-
10.
Start an aspirin for primary as well as secondary prevention in the absence of major bleeding risk or contraindication; if intolerant, consider clopidogrel as alternative therapy.
-
11.
In patients with ACS or high-risk coronary intervention, do not add glycoprotein IIb/IIIa inhibitors to standard care due to potential increase in bleeding risk.
-
12.
In patients with ACS or high-risk coronary intervention, avoid adding thienopyridine or ticagrelor to standard care unless it is certain bleeding risk is not increased.
-
13.
When providing education for RRT (usually GFR < 30 mL/min/m2 BSA), kidney transplantation is by far the most superior therapeutic option available, but there is no evidence that any dialysis modality of RRT (CAPD, continuous cycling peritoneal dialysis (CCPD), home HD, in-center HD, nocturnal HD) is superior to the others, and thus dialysis modality-education should be unbiased and help the patient choose the modality which suits them best.
-
14.
There is no benefit for early versus late initiation of RRT with dialysis and thus dialysis should be initiated when a clinical indication arises while simultaneously accounting for dialysis access best-choice and readiness of use.
-
15.
When HD is chosen, vein-preservation strategies would be adopted and a native arteriovenous (AV) fistula would be the best choice for access, followed by an AV graft; catheters must be avoided if at all possible due to increased risk of mortality, infections and secondary vascular complications.
-
16.
For patients with DMT1, live-kidney transplantation or simultaneous pancreas-kidney (SPK) transplantation or pancreas after kidney (PAK) transplantation be sought with a complete understanding of risks involved with each procedure, but islet transplantation is not recommended. For patients with DMT2, kidney transplantation is recommended for suitable candidates after evaluation, but not SPK or PAK or pancreas transplantation.
7.3.6 Safety of Oral Hypoglycemics in DMT2 and CKD
In patients with CKD and DMT2, metformin must be used with extreme caution when eGFR declines below 30 mL/min/1.73 m2 BSA, due to concerns over severe life-threatening type B lactic acidosis. It may be used in patients with stage 1–3 CKD with dosage adjustments to eGFR and close monitoring of kidney function [157, 158].
Sodium-glucose cotransporter type 2 (SGLT2) inhibitors prevent renal proximal tubular glucose reabsorption and have been associated with urinary tract infections, increased risk of ketoacidosis [159], and some reports to the FDA cite concerns of acute kidney injury. Thus, these agents must be used with caution in patients with stage 3–5 CKD until their safety is clarified. Health care providers and patients must aggressively mitigate any risk factors for AKI such as hypovolemia (e.g. diuretics, HF) and avoid concurrent use of agents resulting in hemodynamic renal hypoperfusion (e.g. non-steroidal anti-inflammatory drugs (NSAIDs) or ACE-i or ARBs) [160].
In patients in whom sulfonylurea therapy is planned, short-acting agents with no active metabolites, such as glipizide are preferred to longer-acting agents or those with active metabolites in order to avoid increased risk of hypoglycemia.
7.4 Lipid Management
Dyslipidemia is an established modifiable major risk factor for CVD in patients with ND-CKD.
The Study of Heart and Renal Protection (SHARP) Investigators followed 6247 ND-CKD patients and 3023 ESKD patients on dialysis, with no prior history of MI or coronary revascularization, for a median duration of 4.9 years after they were randomized to either receive simvastatin plus ezetimibe or placebo and found that the LDL reduction in the active treatment group was associated with a significant 17% risk reduction of a first major atherosclerotic event (coronary death or non-fatal MI, any arterial revascularization procedure or any non-hemorrhagic CVA), and significant protection against non-hemorrhagic CVA and arterial revascularization [161].
However, the power of high LDL-cholesterol to predict AHD risk seems to grow weaker with the severity of CKD and may dissipate entirely in dialysis patients where a more accelerated CVD pathway and a higher mortality rate are driven by other non-traditional risk factors. Clinical trials in hemodialysis patients, such as the Die Deutsche Diabetes Dialyse Studie trial [162] and the A Study to Evaluate the Use of Rosuvastatin in Subjects on Regimen Hemodialysis: An assessment of survival and cardiovascular events (AURORA) trial [163], failed to show any significant beneficial effects of LDL reductions with statin therapy on cardiovascular mortality or all-cause mortality.
7.4.1 KDIGO Guidelines for Lipid Management in CKD
In 2013, the KDIGO Lipid Work Group published a “Clinical Practice Guideline for Lipid Management in CKD” [164]:
-
1.
Check a lipid panel only in patients with newly diagnosed non-dialysis CKD, ESKD, or kidney transplant recipient (total cholesterol, LDL cholesterol, HDL cholesterol, triglycerides). Followup lipid panels are not required in the majority of patients with non-dialysis CKD, ESKD on dialysis, or kidney transplant recipients.
-
2.
In patients aged 50 years or over and with non-dialysis non-transplant Stage 1–5 CKD, initiate pharmacological therapy with a statin or statin/ezetimibe combination.
-
3.
In patients aged 18–49 years with non-dialysis non-transplant Stage 1–5 CKD, pharmacological therapy with a statin is suggested if any of the following co-morbidities exist: (3a). known coronary disease (myocardial infarction or coronary revascularization) (3b). diabetes mellitus (3c). prior ischemic stroke (3d). estimated 10-year incidence of coronary death or non-fatal myocardial infarction >10%.
-
4.
In patients with dialysis-dependent CKD, initiation of pharmacological therapy was not recommended; continuation of any previously prescribed said therapy is suggested.
-
5.
In kidney transplant recipients, initiate pharmacological therapy with a statin.
-
6.
In patients with non-dialysis CKD, ESKD on dialysis, or kidney transplant recipients who are diagnosed with hypertriglyceridemia, therapeutic lifestyle changes are advised.
In summary, it seems that the recommendations for established non-dialysis stage 1–5 CKD patients age 50 years and over, adopt a strategy of “test no one and treat everyone”. This establishes a major shift in clinical practice, where the focus on LDL-cholesterol levels and targets is abandoned in this patient population.
7.5 Obesity and the Metabolic Syndrome
The epidemic of obesity seems to have no geographic, ethnic /racial, gender or age boundaries; obesity carries an increased risk of morbidity and mortality and is the second leading cause of preventable disease in the US.
Epidemiological studies have identified obesity or a higher body mass index (BMI) as an independent risk factor for the development and progression of CKD [165,166,167] and for CVD [168]. Obesity at a younger age (18–34 years) carries an increased risk for future ESKD; compared to a normal BMI, the adjusted RR for future ESKD was 1.87 for a BMI of 25.0–29.9, 3.57 for a BMI of 30.0–34.9, 6.12 for a BMI of 35.0–39.9 and 7.07 for a BMI at or exceeding 40 kg/m2 [169].
Obesity may also cause obesity-related glomerulomegaly and glomerulopathy, with glomerular hyperfiltration and pathological features of secondary adaptive focal segmental glomerulosclerosis with sub-nephrotic proteinuria [170]. Furthermore, obesity has been associated with increased risk of metabolic syndrome, sleep apnea, obesity-associated HTN, insulin resistance and DMT2, dyslipidemia, and various cancers.
The obese population is not a homogenous one; up to one third of obese patients have a “metabolically benign” profile with no apparent increase in CVD risk [171]. The mechanisms by which obesity alters CVD and CKD risk are not fully elucidated, the obesity-CKD association is especially complex. For example, when compared with individuals who have a normal weight and no metabolic syndrome, overweight and obese patients with the metabolic syndrome had a higher risk of ESKD (hazards ratio 2.03), but overweight and obese patients without the metabolic syndrome had a lower risk of ESKD (hazards ratio 0.47) [167]. In patients with established prevalent ND-CKD, some have suggested a U-shaped association between obesity and clinical outcomes of CKD progression and all-cause mortality with the best clinical outcomes at a BMI of 25–35 kg/m2; a BMI < 25 predicted worse outcomes in all patients regardless of CKD stage while a BMI > 35 predicted worse outcomes in patients with stage 1–3 CKD with said risk growing weaker in advanced CKD [172].
In dialysis patients, use of BMI to diagnose obesity and overweight should be done with extreme caution; this is due to protein-energy wasting and loss of muscle mass seen in patients with ESKD on dialysis. Thus in such patients, excessive central or total body adiposity may be masked by a balancing loss of muscle mass, keeping the BMI apparently “normal” [173]. In fact, a higher BMI, when it reflects weight gain resulting from increased muscle mass, was associated with a better and incremental survival rate in a cohort of 121,762 patients on maintenance hemodialysis followed over 5 years [174]. A measure of abdominal and visceral adiposity, such as weight circumference, in a cohort of 537 patients with ESKD, was found to be a reliable and direct predictor of cardiovascular as well as all-cause mortality whereas BMI was not, cardiovascular mortality was highest amongst participants with a waist circumference at or exceeding the median and a BMI below the median, and it was lowest in patients with a waist circumference below the median and a BMI at or above the median; similarly waist/hip ratio also predicted cardiovascular as well as all-cause mortality [175].
Lifestyle modifications focused on caloric restriction, weight loss, regular daily exercise, and when needed surgical interventions, to achieve a BMI of 20–25 kg/m2 are recommended for patients with ND-CKD to reduce risk of CVD and prevent incident or new-onset CKD; however, the ideal target BMI in patients with established-prevalent CKD may be more complex and more clinical studies are needed, some studies have suggested a U-shaped association with best clinical outcomes achieved at a BMI of 25–35. In morbidly obese patients, who fail to achieve or sustain weight loss, surgical interventions such as bariatric surgery ought to be pursued. In ESKD patients on maintenance dialysis, health care providers need to focus on strategies to increase muscle weight.
7.6 Tobacco Cessation
Tobacco use is the leading cause of preventable disease in the US, and ranks only second to HTN as the health risk factor responsible for the highest number of deaths worldwide [176].
Tobacco use is a known risk factor for CVD as well as cardiovascular and all-cause mortality, and it has been associated with nephrosclerosis [177], idiopathic nodular glomerulosclerosis [178,179,180] and worsening progression of CKD and albuminuria in many primary and secondary kidney diseases such as DM, IgA nephropathy, lupus nephritis and polycystic kidney disease [181,182,183,184,185].
However, the evidence for the tobacco-CKD association has not been always reproducible or uniform. For example, in a cohort of 23,534 participants followed over a period of 20 years, tobacco use carried a significant increase in risk of CKD (identified by ESKD or CKD on death certificate verified by a chart review) with a hazard ratio of 2.9 in women and 2.4 in men, with a 31% proportion of the increased risk of CKD attributed to smoking [186]. On the other hand, the SHARP Collaborative Group evaluated the effects of tobacco use in a cohort 9270 CKD patients (13% current smokers, 35% former smokers and 51% never smokers) over a mean duration of 4.9 years and found increased risk in current-smokers for atherosclerotic and non-atherosclerotic vascular events (RR 1.36), lung cancer (RR 9.31) and upper aerodigestive tract cancers (RR 4.87), as well as all-cause mortality (RR 1.48) when compared to never-smokers, but there was no association with rate of change in eGFR or incidence of ESKD [187].
Tobacco use remains a strong risk factor for CVD in patients with CKD of any stage [188]; it is also hypothesized that toxic metabolites of tobacco may accumulate in patients with more advanced CKD, thus enhancing CVD risk. Tobacco cessation reduces CVD risk in patients with CKD [189] and may also be beneficial in slowing down CKD progression in some kidney diseases. Finally, most transplant centers in the US do not accept active tobacco users with advanced CKD or ESKD as candidates for kidney transplant waitlisting.
The most recent update of the US Preventive Services Task Force (USPSTF) guidelines for interventions for tobacco smoking cessation in adults that all healthcare providers inquire about tobacco use, advise active users to stop, evaluate willingness to quit, offer interventions to help the patient quit and arrange for followups; the guidelines advise interventions with evidence-based effectiveness be pursued and to steer away from electronic smoking due to lack of adequate evidence to risks and benefits [190]. Offering behavioral and pharmacological interventions with nictoine-replacement therapy or partial nicotine agonists enhances successful quit rate and must be tailored to patient’s safety and eGFR.
7.7 Exercise
“Exercise is medicine”. A sedentary lifestyle, with a lack of regular exercise, is a risk factor for CVD and has been associated with progression of CKD in some observational studies.
CKD itself and its complications may limit exercise tolerance via factors such as anemia and vascular disease [191]; walking seems to be the most popular form of exercise in patients with stage 3–5 CKD and has been associated with improved survival and decreased risk of RRT [192].
All able CKD patients must be encouraged regularly to follow the 2008 Federal Physical Activity Guidelines for:
-
1.
Leisure-time aerobic physical activity, a weekly recommendation for 150 min of moderate-intensity exercise, or 75 min of high-intensity, or some combination, and most favorably spread over many week-days, and
-
2.
Muscle-strengthening, a weekly recommendation to exercise all muscle groups in a moderate- to high-intensity workout at least twice a week [18, 193].
In a cohort of 256 individuals with stage 3–4 CKD from the Seattle Kidney Study, those who had more than 150 min of weekly physical activity had a slower CKD progression over a median 3.7 years of follow-up [194].
Additionally, exercise is encouraged in patients with ESKD on HD. Use of intra-dialytic exercise during HD time has been shown to be beneficial and safe in many small studies and is implemented in some dialysis centers in Europe and Australia [195] but has not made it to North America.
In summary, many studies have shown the benefits of aerobic physical activity and muscle strengthening in patients with stages 2–5 CKD, including those on RRT, and thus exercise is medicine in this patient population and should be prescribed to all who are able and who have no restricting clinically-active CAD, either in a home-based program, or in-center during dialysis, or in another setting [196].
8 Management of Non-traditional CVD Risk Factors in CKD
8.1 Preventing or Slowing Down Progression of CKD
Strategies to slowing down the progression of CKD must focus on achieving optimal blood pressure control, optimal glycemic control, optimal lipemic control, tobacco cessation, achieving ideal BMI and waist/hip ratio for CKD stage, anemia management, correction of acid-base and electrolyte abnormalities, management of mineral and bone disorder, dietary protein restriction, treatment with an ACEi or an ARB especially in patients with stage A2-A3 albuminuria.
8.1.1 Depression and Cognitive Dysfunction in CKD
Furthermore, CKD, whether lower eGFR or albuminuria, is associated with cognitive dysfunction, and around 26.5% of CKD patients are clinically depressed [197]; both conditions result in a decreased quality of life. Thus, it is important to evaluate every CKD patient thoroughly for either problem as either may interfere with compliance, motivation, and the success of preventive and therapeutic strategies.
8.1.2 Genetic Predisposition
The role of genetic predisposition in CKD and CVD is not yet well established, but clinical research continues to make slow and steady strides in this futuristic field. For example, black individuals with variants of apolipoprotein L1 (APOL1) are more susceptible to develop certain forms of CKD and progress to ESKD; two APOL1 alleles incur a 1.49 higher risk for CKD and a 1.88 higher risk for ESKD when compared to zero or one allele [198].
8.2 Reduction of Urine Albumin Excretion Rate
Urine Albumin excretion rate (UAER) is an independent CVD risk factor; it is also an excellent prognosticator of CKD progression as well as a strong biomarker of response to therapy. Pharmacological therapies that have been shown to decrease (UAER) include RAAS inhibitors (ACEis, ARBs, DRIs and ARAs), and when not tolerated non-dihydropyridine CCBs (Diltiazem).
8.3 Treatment of Anemia in CKD
Anemia in CKD may represent different pathophysiological pathways such as erythropoietin deficiency, erythropoietin resistance due to a multitude of causes such as chronic inflammation or secondary hyperparathyroidism (SHPT), chronic blood loss (may be more significant in dialysis patients), iron deficiency, vitamin B12 or folate deficiency, or a shortened erythrocyte life span [199, 200]. Furthermore, angiotensin II may play a minor physiological role in stimulating erythropoietin production in humans [201,202,203]; ACEi may theoretically reduce the response to ESAs and contribute to ESA hypo-responsiveness or resistance [204, 205].
Anemia usually occurs once eGFR declines below 60 and hemoglobin (Hb) levels usually correlate with severity of CKD. The best marker in CKD patients is the Hb, rather than the hematocrit, which may vary with ECF volume, measuring methods, and sample storage time. Workup for anemia in patients with CKD should reinforce:
-
1.
age-appropriate screening for occult blood loss,
-
2.
evaluate a peripheral smear and a reticulocyte count,
-
3.
check an iron panel with ferritin keeping in mind that ferritin is an acute phase reactant that is often increased in patients with chronic inflammation [206]. CKD patients also have increased plasma hepcidin levels, thus inhibiting duodenal iron absorption and further contributing to iron deficiency [207].
-
4.
check a vitamin B12 and RBC-folate levels, but
-
5.
should not include erythropoietin levels, which rarely add anything to the evaluation and management plan.
Anemia has been associated with increased mortality, more frequent hospitalizations, impaired cognitive function, reduced functional status and exercise tolerance, a higher left ventricular mass index (LVMI) and left ventricular hypertrophy (LVH, an independent predictor of increased mortality risk) [61], and increased cardiovascular disease.
Treatment of anemia decreases the need for RBC transfusions [208], may cause partial regression of LVH [209], reverses most clinical manifestations, may improve functional status, and some even report improved survival. The benefits of treatment of anemia remains a topic of debate; for example, a systematic review of the effect of ESA therapy on affects health-related quality of life (HRQOL) in CKD patients did not reveal any significant improvement [210].
Currently approved ESAs by the FDA in the USA include recombinant human erythropoietin, darbepoetin alpha, and methoxy polyethylene glycol-epoetin beta. One of the adverse effects of erythropoietic stimulating agents (ESAs) is a higher BP. Oral iron must be taken between meals and should not be combined with calcium-based binders as they bind each other.
In summary, for the majority of patients, ESA therapy is initiated when Hb levels decline below 9 g/dL and therapy should target a goal Hb of 10–11 g/dL and levels higher than 12 g/dL must be avoided. Higher goals have been associated with poorer BP control and increased risk of stroke and mortality [208, 211].
8.3.1 KDIGO Clinical Practice Guideline for Anemia in CKD
In 2012, the KDIGO Anemia Work Group published a “Clinical Practice Guideline for Anemia in CKD” [212].
-
1.
Diagnosis and Evaluation:
-
1a.
Diagnose anemia in CKD when the hemoglobin (Hb) concentration is <13 g/dL in men and < 12 g/dL in women.
-
1b.
In patients with CKD but no anemia, measure Hb when a clinical indications arises and at least once every 12 months in patients with stage 3 CKD, at least once every 6 months in patients with stage 4–5 non-dialysis CKD, and at least every 3 months in patients on hemodialysis or peritoneal dialysis.
-
1c.
In patients with CKD and anemia receiving pharmacological therapy with ESA, measure Hb when a clinical indications arises and at least once every 3 months in patients with stage 3–5 non-dialysis CKD or who are on peritoneal dialysis, and at least every 1 month in patients on hemodialysis.
-
1d.
In any patient with CKD diagnosed with anemia, initial workup must include a complete blood count (CBC), absolute reticulocyte count, serum ferritin level and a serum transferrin saturation (TSAT), serum vitamin B12 and folate levels.
-
1a.
-
2.
Iron Therapy. When prescribing intravenous (IV) iron therapy for patients with CKD, anemia and iron deficiency:
-
2a.
Weigh the advantages (alleviation of clinical symptoms, minimization of blood transfusions, optimal utilization of ESA therapy) against the short-term and long-term potential risks (anaphylactoid and other acute reactions, unknown long-term risks).
-
2b.
Exclude any active infection, especially systemic.
-
2c.
Confirm pre-requisite laboratory data: transferrin saturation (TSAT) ≤ 30% and a ferritin ≤ 500 ng/ml.
-
2d.
For patients not receiving any ESA therapy, a trial of IV iron may be initiated when a higher Hb concentration is desired without ignition any ESA.
-
2e.
For patients receiving ESA therapy who are not receiving iron supplementation, a trial of IV iron may be initiated after exclusion other causes of ESA hypo-responsiveness, and when a higher Hb concentration or a lower ESA dose is desired.
-
2f.
For patients with non-dialysis CKD, a trial of oral iron therapy for 1–3 months may be initiated as an alternative to IV iron depending on “the severity of iron deficiency, availability of venous access, response to prior oral iron therapy, side effects with prior oral or IV iron therapy, patient compliance, and cost”.
-
2g.
Evaluate clinical picture, past and present responses to iron therapy, iron parameters, blood loss, Hb trends, ESA dose and responsiveness to judge the utility of future iron use.
-
2h.
Measure TSH and Ferritin at least every 3 months when starting or maintaining iron therapy, or more often when monitoring response to IV iron or when starting, maintaining or changing ESA therapy, or when a clinical indication arises.
-
2i.
Study the safety of the IV iron formulation used and ensure a safe environment for administration, adequate monitoring and resuscitation if an adverse event occurs.
-
2a.
-
3.
ESA Therapy: When prescribing ESA therapy for patients with CKD and anemia:
-
3a.
Exclude, and treat, reversible causes such as iron deficiency of inflammatory diseases.
-
3b.
Weigh the advantages (alleviation of clinical symptoms, minimization of blood transfusions, optimal utilization of ESA therapy) against the potential risks (higher BP, increased thrombotic complications such as clotting of arteriovenous access or stroke).
-
3c.
In patients with active malignancy with a favorable prognosis, history of malignancy or history of CVA, uses ESA with extreme caution.
-
3d.
For patients with ND-CKD and a Hb ≥ 10 g/dL, ESA therapy should not be initiated; if Hgb < 10 g/dL then clinical risk-benefit analysis should be done to reach an individualized decision whether to initiate ESA therapy.
-
3e.
In patients with stage 5D-CKD, avoid Hb decline to a level below 9.0 g/dL and initiate ESA when Hb is 9.0–10.0 g/dL.
-
3f.
ESA may be started at higher Hb in select patients who may have a better quality of life.
-
3g.
Maintenance ESA therapy should be used to maintain a Hgb level at 10–11.5 g/dL in most patients and never to intentionally target a Hgb above 13 g/dL.
-
3h.
Initial ESA dose is weight based, and considers severity of anemia and clinical manifestations. Dose adjustments are tailored to ESA responsiveness, rate of Hb increments, clinical picture, patient safety and freedom from adverse events. When a Hb drop is desired, decreasing ESA dose is preferred to withholding dose whenever possible.
-
3i.
For patients with ND-CKD or stage 5D-CKD on PD, subcutaneous administration of ESA is suggested; for patients on hemodialysis either intravenous or subcutaneous is suggested.
-
3j.
Frequency of ESA administration must be customized based on CKD stage, ESA type and half-life, administration setting, responsiveness, and patient preference.
-
3a.
-
4.
Difficulty Achieving Goal Hb:
-
4a.
When initiating ESA therapy, check Hb at least once a month. For patient on maintenance therapy, measure Hb at least monthly in stage 5D-CKD patients and at least every 3 months in ND-CKD patients.
-
4b.
Identify initial ESA hypo-responsiveness in new patients receiving the proper weight-based ESA dose and whose Hb fails to respond; titrating ESA dose should not exceed double the initiation dose.
-
4c.
Identify subsequent acquired ESA hypo-responsiveness in patients who had a stable Hb on a maintenance ESA therapy, and who then require two dose increases of 50% or more of the original maintenance ESA dose for a declining Hb; titrating ESA dose should not exceed double the original maintenance ESA dose.
-
4d.
Evaluate hypo-responsive patients for specific causes such as inadequate iron stores, infection or inflammation, SHPT, etc… and if correcting any secondary causes fails to achieve goal Hb, then individualize therapy with ESA and or blood transfusions to achieve minimum safe Hb.
-
4a.
-
5.
Red Blood Count (RBC) Transfusion:
-
5a.
Avoid RBC transfusions, whenever possible, for treatment of anemia due to inherent transfusion risks; especially in kidney transplant candidates to minimize risk of allosensitization.
-
5b.
Consider RBC transfusion in select patients, where benefits outweigh risk, such as patients with ESA hyporesonsiveness or bone marrow failure or hemoglobinopathies where ESA therapy is ineffective, or in patients with an active or past malignancy or a history of a CVA.
-
5c.
RBC transfusion should be guided by occurrence of symptoms and not be any Hb threshold.
-
5a.
8.4 Managing CKD-MBD
Patients with CKD develop a series of abnormalities relating to mineral (calcium and phosphorus) and bone metabolism. The earliest biomarker abnormality to herald this complex disorder is a rise in parathyroid hormone (PTH) reflective of parathyroid tissue hyperplasia, usually seen when the eGFR declines below 60, and other biomarkers include an elevated fibroblast growth factor 23 (FGF-23), elevated bone alkaline phosphatase, a low 1,25-dihydroxy-vitamin D3 (calcitriol) level, hyperphosphatemia, and hypocalcemia [213]. Such biochemical abnormalities usually indicate defective bone metabolism (with increased fracture risk) with one or other of two major phenotypes: high bone turnover as is seen in osteitis fibrosa cystica, or low bone turnover as is seen in adynamic bone disease or osteomalacia. Furthermore, this chain of events is believed to trigger the transformation of vascular medial smooth muscle stem cells into osteoblast progenitor cells, which promote vascular calcification.
8.4.1 Hyperphospahtemia
In patients with ND-CKD, hyperphosphatemia or a serum phosphorus in the upper normal range is a risk factor for CVD, arterial and valvular calcification and all-cause mortality, and for every rise in serum phosphorus by 1 mg/dL, there was a statistically significant rise in prevalence of CAC by 21%, thoracic aortic calcification by 33% and mitral valve calcification by 25% [214]. Similarly, high FGF-23 levels independently predicted increased LVMI and risk of LVH [215].
With reduced renal phosphorus clearance, hyperphosphatemia is usually treated with dietary modifications to restrict daily phosphorus intake to one gram and with phosphate binders. Phosphorus is an intracellular ion, and while most dialysis patients develop hypo-phosphatemia during a dialysis session, rebound hyperphosphatemia may still ensue post-dialysis.
Currently, FDA approved phosphate binders available in the US include:
-
1.
Calcium-based phosphate binders such as calcium acetate and calcium carbonate,
-
2.
Non-calcium-based binders:
-
2a.
sevelamer hydrochloride and sevelamer bicarbonate. Sevelamer has the added benefit of producing reductions in LDL-cholesterol.
-
2b.
lanthanum carbonate,
-
2c.
iron-based phosphate binders such as sucroferric oxyhydroxide, and ferric citrate,
-
2d.
aluminum hydroxide. Regular use of aluminum hydroxide has been abandoned due to bone toxicity (osteomalacia and cysts) and neurotoxicity (encephalopathy or dementia).
-
2a.
There is conflicting evidence whether calcium-based binders are inferior to non-calcium based binders in patients with non-dialysis CKD or ESKD on dialysis, as far as all-cause mortality or cardiovascular mortality, due to concerns that calcium-based binders may enhance CAC and other arterial calcifications [216].
A recent meta-analysis, including 77 clinical trials and 12,562 patients, mostly dialysis patients, compared the effects of calcium-based phosphate binders or non-calcium-based phosphate binders on cardiovascular events and all-cause mortality and found no difference when compared to placebo; in subgroup analysis, sevelamer had a lower overall mortality rate (OR 0.39) when compared to calcium-based phosphate binders [217]. Similar major systematic reviews failed to show a similar survival benefit with Sevelamer [218, 219].
8.4.2 Vitamin D Insufficiency or Deficiency
Traditionally, the role of Vitamin D replacement in CKD patients has been to treat secondary hyperparathyroidism (SHPT) with the activated hormonal vitamin D form, calcitriol (1,25-dihydroxycholecalciferol), or with a synthetic vitamin D analog (e.g. calcifediol, doxercalciferol, paricalcitol). However, 25-hydroxy vitamin D insufficiency or deficiency has been increasingly diagnosed in CKD patients and it is believed it accelerates SHPT, and thus when diagnosed in this setting, it is recommended to replace this deficiency with vitamin D2 (ergocalciferol) or vitamin D3 (cholecalciferol).
One of the reasons that pharmacological therapy, rather, than augmented dietary intake is favored, is that vitamin D, a fat-soluble vitamin, would dictate a high-fat food items, a diet not generally encouraged in this patient population.
With vitamin D receptors being discovered in many tissues (e.g. heart, prostate), the scope of vitamin D therapy may be expanded beyond SHPT, for example, some observational data have linked activated vitamin D intake in patients with EKSD on dialysis to improved cardiovascular outcomes and survival [220, 221].
8.4.3 SHPT
Current therapies for SHPT include pharmacological therapy with a vitamin D analog or a calcimimetic, or surgical parathyroidectomy.
There is no current evidence that either form of pharmacological therapy is superior to the other in SHPT, and many patients may receive a combination of both forms of therapy. When monotherapy is suitable, the choice is usually guided by the patient’s biochemical profile, i.e. serum calcium and phosphorus levels: vitamin D analogs tend to promote hyperclacemia and hyperphosphatemia whereas calcimimetics may cause hypocalcemia [222]. There is no clinical evidence at this time that vitamin D analogs enhance vascular calcifications via promoting a higher serum calcium level.
Cinacalcet, an oral calcimimetic, used to treat SHPT in patients with ESKD on dialysis, failed to show any survival benefit in patients with moderate to severe SHPT and receiving standard therapy when compared to placebo; furthermore, the EVOLVE trial investigators did not detect and decrease in cardiovascular events with cinacalcet [223].
While SHPT and hyperphosphatemia are risk factors for increased mortality, no pharmacological intervention to this date have been shown to offer any survival benefit. For example, a recent metanalysis of 28 clinical trials with 6999 participants reported “weak and imprecise” associations between different pharmacological agents, surrogate biomarkers and mortality and added that many trials were plagued with risk of bias [224].
8.4.4 KDIGO Clinical Practice Guideline for the Diagnosis, Evaluation, and Treatment of CKD–Mineral and Bone Disorder
The “2009 KDIGO Clinical Practice Guideline for the Diagnosis, Evaluation, and Treatment of CKD–Mineral and Bone Disorder (CKD-MBD)” recommends the following for patients with stage 3–5D CKD [225]:
-
1.
Biochemical:
-
1a.
Start checking calcium, phosphorus, iPTH, and alkaline phosphatase regularly in any patient with stage 3–5D CKD and monitor calcium and phosphorus every 6–12 months in stage 3 CKD, every 3–6 months in patients with stage 4 CKD and every 1–3 months in stage 5 CKD; monitor alkaline phosphatase and iPTH less frequently depending on baseline levels and rate of CKD progression. Monitoring frequency may be increased when abnormalities are identified or when therapeutic interventions are initiated.
-
1b.
Check 25-hydroxy-vitamin D (calcidiol) and correct any insufficiency or deficiency and order follow-up levels based on baseline levels and whether therapeutic interventions have been initiated.
-
1c.
It is best to base therapeutic decision making on trends of biomarkers rather than single laboratory values.
-
1d.
Its is suggested that calcium and phosphorus levels be used to guide clinical decisions rather than the CaxP product.
-
1e.
All labs must be interpreted in lieu of the sample source and handling, and assay methods used at the laboratory.
-
1a.
-
2.
Bone:
-
2a.
A bone biopsy may be performed if a clinical indication arises, such as persistent bone pain, unexplained fractures or hyperclacemia or hypophosphatemia, suspected aluminum toxicity, prior use of bisphosphonates.
-
2b.
In patients with clinical evidence of CKD-MBD, routine bone mineral density testing is not recommended because it fails to predict fracture risk or type of renal osteodystrophy.
-
2c.
Bone disease can be evaluated with iPTH or bone-specific alkaline phosphatase, both of which may provide clues to state of bone turnover.
-
2a.
-
3.
Vascular calcifications:
-
3a.
When indicated, a lateral abdominal radiograph to detect vascular calcifications and an echocardiogram to detect valvular calcifications be used rather than an EBCT.
-
3b.
Patients with vascular or valvular calcifications should be classified as highest cardiovascular risk.
-
3a.
-
4.
Treatment of Mineral Disorders:
-
4a.
Keep serum phosphorus in normal range for ND-CKD patients and lower phosphorus toward normal range in dialysis patients.
-
4b.
Keep serum calcium in normal range.
-
4c.
(4c) In stage 5D-CKD a dialysate calcium between 2.5 and 3.0 mEq/L is suggested.
-
4d.
Restrict dietary phosphorus intake in patients with hyperphosphatemia.
-
4e.
Use phosphate binders to treat hyperphosphatemia, and restrict calcium-based binders and vitamin D analogs in patients with persistent or recurrent hypercalcemia or arterial calcifications or dynamic bone disease or a persistently low iPTH.
-
4f.
Avoid long-term use of aluminum-based phosphate binders.
-
4a.
-
5.
Treatment of SHPT:
-
5a.
In patients with stage 3–5 ND-CKD, optimal ipTH level is not clear and patients with SHPT should be checked and treated if reversible causes are detected such as hyperphsophatemia, hypoclacemia, and low 25-hydroxy vitamin D insufficiency or deficiency.
-
5b.
In patients with stage 3–5 ND-CKD with persistent SHPT despite treating all potential causes, initiate calcitriol or vitamin D analog therapy.
-
5c.
Look for trends in iPTH levels to guide therapy, rather than single values, and maintain levels between 2–9 upper normal limit of the assay.
-
5d.
In patients with stage 5D-CKD and SHPT, therapy with calcitriol or vitamin D analog therapy or a calcimimetic or a combination should be started and choice should be guided by serum calcium and phosphorus levels. Vitamin D therapy should be reduced or stopped when hypercalcemia or hyperphosphatemia ensue; similarly calcimimetic therapy should be adjusted or stopped if hypocalcemia develops and based on clinical manifestations. Stop any therapy if iPTH goes below two times the upper normal level of the iPTH assay.
-
5e.
In patients with stage 5D-CKD and SHPT, who fail to respond to therapy, surgical parathyroidectomy is suggested.
-
5a.
-
6.
Other pharmacological therapies:
-
6a.
In patients with stage 1–2 CKD with osteoporosis or high fracture risk, manage as non-CKD patients.
-
6b.
In patients with stage 3 CKD and normal PTH with osteoporosis or high fracture risk, manage as non-CKD patients.
-
6c.
In patients with stage 3 CKD and CKD-MBD with low bone mineral density or fragility fractures, consider a bone biopsy and customize therapy based on magnitude and reversibility of CKD-MBD.
-
6d.
In patients with stage 4–5D CKD and CKD-MBD with low bone mineral density or fragility fractures, a bone biopsy is suggested prior to initiating therapy.
-
6a.
8.5 Managing Acid-Base and Electrolyte Disturbances
Metabolic acidosis, mostly normal anion-gap and occasionally high-anion-gap in more advanced stage 4–5 CKD or uremic ESKD, complicate CKD in its more advanced stages (usually at an eGFR<25).
Metabolic Acidosis is due to:
-
1.
A decreased nephron mass and thus an impaired ability to excrete a net daily dietary intake of an acid load estimated at 1 mEq per kg,
-
2.
Decreased total ammoniagenesis and ammonia excretion (required as one of the buffers of the excreted acid load) despite an adaptive increase in ammonia production by each of functional renal tubules, and
-
3.
Decreased phosphorus excretion which limits the extent of tubular intra-luminal acid titration.
Adaptive mechanisms also result in the upregulation of aldosterone dependent proton excretion via type-A intercalated cells in the collecting duct. The resultant adaptive mechanisms enhancing ammonia production and aldosterone activity, among others, (a) enhance CKD progression; furthermore, metabolic acidosis is thought to (b) enhance protein catabolism in muscles as well as inhibit albumin synthesis and thus promoting muscle wasting and protein energy wasting and malnutrition, (c) worsen bone disease, (d) promote inflammation (the increased ammoniagenesis in remaining nephrons activates complement system), and (e) increase mortality.
Current recommendations for management of metabolic acidosis in ND-CKD are to initiate oral alkali therapy (e.g oral sodium bicarbonate) to correct the metabolic acidosis to a serum bicarbonate level of 22–24 mEq/L and to endeavor not to overcorrect due to potential adverse CV outcomes. In patients on dialysis, the dialysate bicarbonate is adjusted by the primary nephrologist to correct the metabolic acidosis [226]; and similarly overcorrection and ensuing metabolic alkalosis must be avoided as it accentuates the arrhythmogenic effects of hypokalemia.
8.6 Management of Protein Energy Wasting (PEW)/Protein Energy Malnutrition (PEM)
PEW/PEM is a risk factor for mortality and morbidity in stage 3–5D CKD patients.
The K/DOQI recommends assessment of protein and caloric intake in all patients with stage 3–5D CKD. There is no one biochemical marker to quantitate PEW/PEM; surrogates for nutritional status include albumin or prealbumin which serve as biomarkers of visceral protein, whereas anthropometric measurements (e.g. edema-free weight and BMI, waist circumference, waist/hip ratio, % body fat, skin fold thickness) and creatinine production rates serve as biomarkers of somatic/muscle proteins. Other methods to evaluate protein intake include normalized protein nitrogen appearance (nPNA), a subjective global assessment (SGA includes appetite, GI symptoms, food intake, physician’s assessment) or food diaries.
PEW is the end of result of multiple pathophysiological processes:
-
1.
Decreased daily caloric intake and dietary protein intake due to CKD clinical manifestations such as poor appetite, nausea or vomiting,
-
2.
Increased branched amino acid catabolism in muscles and inhibition of albumin synthesis due to metabolic acidosis,
-
3.
Diminished visceral protein anabolism due to acute or chronic inflammation.
Dietary protein restriction in patients with ND-CKD is hypothesized to slow down the progression of CKD, but the evidence in the literature is controversial, not always reproducible or uniform. However, protein restriction to 0.8 g/kg per day of healthy body weight (not safe to go below 0.6 g/kg per day) with the addition of daily urinary protein losses is a reasonable and safe recommendation as it would serve not to counter the effects of anti-proteinuric therapy as well as reduce risks of hyperphosphatemia, metabolic acidosis, and azotemia [227,228,229]. Other goals to minimize PEW/PEM include maintaining serum bicarbonate level of 22–24 mEq/L and targeting an albumin goal above 4 g/dL.
In dialysis patients, protein energy wasting is a risk factor of mortality and a high-protein diet of 1.4 g/kg per day is recommended and often patients may be prescribed oral protein supplements.
8.7 Chronic Inflammation
CKD , irrespective of the specific underlying etiology, is invariably associated with a reduction in functional renal mass and secondary adaptive glomerular hyperfiltration; persistent hyperfiltration and increased intraglomerular capillary pressure promote immune-activation and an inflammatory state, eventually leading to injury and damage in all the kidney compartments, namely, glomerular, vascular endothelial, and tubulointerstitial. Similarly, glomerular podocyte injury and the resultant micro- or macro-albuminuria results in a pro-inflammatory state and tubulointerstitial disease [230, 231].
Chronic inflammation is a risk factor for cardiovascular mortality in patients with CKD. Inflammation is multifactorial:
-
1.
CKD patients have altered gut microbiota (intestinal dysbiosis) and intestinal inflammation with significant disruptions in the functional integrity of the intestinal epithelial barrier, resulting in a “leaky gut” and translocation of bacterial DNA and endotoxins into the systemic circulation. Blood endotoxin levels correlate with severity of CKD and in stage 5D-CKD, said levels predict the severity of inflammation and correlate with atherosclerosis risk. To compound this problem further, dietary restrictions imposed on CKD patients, especially low potassium and low phosphorus, dictate a low plant fiber diet which also result in a secondary change in the gut microbiome. Epidemiological studies suggest that a high-fiber diet promotes the growth of endosymbiotic bacteria, thus preventing gram-negative bacterial overgrowth and the production of endotoxins and gut-derived uremic toxins, and thereby minimizing these triggers of systemic inflammation. Similarly, some observational studies suggest a beneficial role of prebiotics (ingested non-digestible compounds which enhance bacterial growth and activity, e.g. chicory), and probiotics (ingested live organisms, e.g. treated yogurts) [232,233,234].
-
2.
CKD patients with DM must have regular foot exams to detect any diabetic foot ulcers, which are a significant source of inflammation.
-
3.
Patients with ESKD on RRT have multiple potential sources of inflammation such as presence of dialysis catheters, exposure of blood to dialysis membranes and tubings in HD, exposure of peritoneal cavity to peritoneal dialysate in PD.
There are currently no evidence-based interventions from large clinical trials to stop, decrease or reverse inflammation and CVD risk in patients with CKD. However, it is recommended that a high plant-fiber diet (Dietary Reference Intakes advises 14 g dietary fiber per 1000 kcal per day) be used to restore a more favorable gut microbiota. Furthermore, the use of biocompatible dialysis membranes and PD solutions may also decrease the burden of inflammation.
8.8 Dietary Modifications
Patients with CKD are advised to follow the following dietary restrictions, which may also help minimize risk of CVD:
-
1.
Restrict daily sodium intake to 2 grams (or 5 grams of sodium chloride) daily. Unfortunately, this may be a challenge for some in the present time especially that most pre-packaged processed foods are usually high in salt. High salt intake is associated with increased oxidative, which may contribute to CKD and CVD, and a more expanded ECF volume and higher BP thus interfering with effectiveness of BP lowering medications.
-
2.
A protein restriction to 0.6–0.8 g/kg per day of healthy body weight (plus daily urinary protein losses) may help slow down progression of CKD especially in patients with DM, reducing eGFR decline by 0.53 mL/min per annum [235], while preventing PEW/PEM. A high animal-protein diet has been associated with glomerular hyperfiltration [236] as well as worsening metabolic acidosis and is thus not recommended in patients with CKD. In contrast, increasing plant-protein intake does not increase glomerular filtration, does not increase daily acid load, increases daily fiber intake which in turn may decrease inflammation [234].
-
3.
A high fiber diet is recommended for patient with CKD with special attention to potassium and phosphorus imbalances, examples include fruits and vegetables, whole grains and legumes. A high-fiber diet (16–17 grams daily) in elderly Swedish subjects was associated with slower CKD progression assessed by eGFR (cystatin C), less inflammation reflected by CRP and IL6 levels, lower cancer-mortality, and better overall survival in patients with stage 3–5D CKD after a median followup of 10 years [237].
8.9 Constant Monitoring for Prescription and Non-Prescription Medications
Patients with CKD and or CVD frequently have a significant pill burden; in fact, patients with ESKD on HD have a median daily pill burden of 19 with 25% of the patients taking more than 25 pills a day [238]. This triggers concerns over medication or dosing errors (e.g. not adjusting dose to eGFR), use of contraindicated agents, drug-drug interactions, risk of adverse reactions, and overall safety. Thus it is essential that PCPs, nephrologists and other specialists work closely together to simplify dosing regimens (avoid more than twice daily dosing whenever possible) and to ensure safety of medication choice, dosing as well as the whole prescription regimen.
For example, in a cohort of 267 patients with stage 3–5 CKD from the “Safe Kidney Care study”, 69.3% of participants had an adverse event, with hypoglycemia being the highest patient-reported adverse event followed by severe dizziness or falls, and hyperkalemia being the highest laboratory-confirmed adverse event [239]. Thus, special care must be offered to choosing and dosing oral hypoglycemics in CKD patients.
Slowing down the progression of CKD and thus avoiding an additional CVD burden risk, requires constant diligence to monitor the intake of potential nephrotoxic medications or herbs. Analgesics, especially non-steroidal anti-inflammatory drugs top the list of the undesirables; high-dose acetaminophen should also be avoided. Alternative medicines and supplements, to this date, are not FDA regulated, and as many as one third been shown to be contaminated with heavy metals at the production site [240]; in addition, the safety of many has not been studied in clinical trials and some are known to be harmful or nephrotoxic. The NKF published a list of 37 harmful herbs that must be avoided in patients with CKD, this list can be accessed at the NKF website [241].
Illicit drug use has been associated with increased CKD as well as CVD risk [242]. For example, cocaine and meth-amphetamines have been associated with hypertensive and ischemic damage resulting in ESKD as well as cardiomyopathy; adulterated cocaine has also been associated with ANCA-vasculitis.
8.10 Evidence for Specific CV Conditions
8.10.1 Sudden Cardiac Death
As mentioned earlier, sudden cardiac death accounts for 37% of mortality seen in patients with ESKD on HD. A meta-analysis of seven RCTs (2867 patients) evaluated the benefits of primary prevention implantable cardioverter-defibrillator (ICD) in CKD and found that the survival benefit attributed to ICDs is GFR dependent and retained its statistical significance for a GFR ≥60 mL/min/1.73 m2 but not lower [243].
8.10.2 Percutaneous Coronary Interventions
In patients with an eGFR <60 and when indicated, a meta-analysis of 26 clinical trials with 66,840 patients has shown a survival benefit and lower complication rate (repeat revascularization, myocardial infarction) when using drug-eluting stents when compared to bare-metal stents [244]. The lower restenosis rate with drug-eluting stents was reproduced by another randomized clinical trials in CKD patients [245].
8.10.3 Atrial Fibrillation
Atrial fibrillation is associated with an increased risk for all-cause mortality, cardiovascular mortality, stroke namely thromboembolic stroke (but not hemorrhagic stroke), ischemic heart disease, HF, PAD, sudden cardiac death, and CKD [246].
In turn, CKD is associated with a higher risk of non-valvular AF and stroke as well as a higher risk of bleeding.
In patients with ND-CKD, anticoagulation for high risk (CHADS1) non-valvular AF decreases risk of ischemic strokes and all-cause as well as cardiovascular mortality without a significant rise in major bleeding [247,248,249].
However, the debate of the risk-benefit ratio with the use of anticoagulation for the treatment of high-risk ESKD dialysis patients with non-valvular AF is ongoing. For example, a 2016 meta-analyses reported a significant rise in the risk of major bleeding and no benefit in stroke prevention with warfarin therapy in this patient population [247], while other studies report a benefit with lower thromboembolic risk. Thus, the decision for or against anticoagulation therapy in dialysis patients must be customized to each patient based on a thorough risk-benefit analysis.
8.10.4 Cardiorenal Syndromes
The 2013 “American College of Cardiology Foundation (ACCF)/American Heart Association (AHA) Guideline for the Management of HF” recommends that all patients with HF have an initial as well as serial monitoring of kidney function [250]; this reflects the fact that neither CKD nor worsening kidney function are uncommon in HF, and both carry a poorer prognosis. However, whereas albuminuria and eGFR are both useful at quantitating risk in HD, eGFR alone should be used to guide HF therapy at this time and until such evidence emerges for the role of other CKD biomarkers as far as therapy and prognosis [251].
The main challenge in types 1 and 2 cardiorenal syndromes is to achieve the optimal balance between successive diuresis and the maximal benefit of RAAS inhibition to avoid the fluctuation from one extreme and another, namely between acuter decompensated heart failure on the one hand and AKI due to excessive diuresis and effective arterial volume depletion on the other. Furthermore, worsening kidney function may predispose to hyperkalemia and deprive patients with symptomatic HF and reduced LVEF from the survival benefits associated with dual aldosterone receptor antagonist therapy and ACEi therapy.
A meta-analysis evaluated the impact of worsening kidney function (WRF) after initiation of RAAS inhibition in patients with HF and left ventricular systolic dysfunction, and included five clinical trials (SOLVD – Studies of Left Ventricular Dysfunction, SAVE Survival and Ventricular Enlargement Trial, RALES – the Randomized Aldactone Evaluation Study, Val-HeFT – Valsartan Heart Failure Trial, and EPHESUS – Eplerenone Post-Acute Myocardial Infarction Heart Failure Efficacy and Survival Study) and showed a survival benefit with RAAS inhibition irrespective of whether the patients experienced WRF (Relative Risk RR 0.72, P < 0.001) or not (RR 0.91, P = 0.04). More patients in the RAAS treatment group developed WRF and WRF was a predictor of increased mortality (RR 1.22, P = 0.0003) when compared to the RAAS treatment group with no WRF. However, when the mortality rates in the RAAS treatment group with WRF were compared to the placebo group with WRF, RAAS inhibition was associated with a reduction in mortality; the magnitude of this protective effect was greatest in patients in the treatment subgroup with WRF [119].
9 Summary and Conclusions
CKD is associated with increased risk for CVD. Patients with CKD require a specialized focus on multiple clinical parameters that may lead to the progression of CKD, but also need global cardiovascular risk reduction efforts. Estimation of GFR provides a better measure of renal function compared to the serum creatinine, and better informs clinicians of the need for needed intervention and appropriate targets for therapy. Earlier treatment of CKD may slow progression and optimize treatment for renal replacement therapy.
References
World Health Organization. A global brief on hypertension: silent killer, global public health crisis. World Health Day 2013. [Internet]. Geneva, Switzerland: World Health Organization; 2013. p. 1–39. Available from: http://apps.who.int/iris/bitstream/10665/79059/1/WHO_DCO_WHD_2013.2_eng.pdf?ua=1.
Nwankwo T, Yoon SS, Burt V, Gu Q. Hypertension among adults in the United States: National Health and nutrition examination survey, 2011-2012. NCHS Data Brief. 2013;133:1–8.
Parikh NI, Hwang S-J, Larson MG, Meigs JB, Levy D, Fox CS. Cardiovascular disease risk factors in chronic kidney disease: overall burden and rates of treatment and control. Arch Intern Med. 2006;166(17):1884–91.
Coresh J, Wei GL, McQuillan G, Brancati FL, Levey AS, Jones C, et al. Prevalence of high blood pressure and elevated serum creatinine level in the United States: findings from the third National Health and nutrition examination survey (1988-1994). Arch Intern Med. 2001;161(9):1207–16.
Muntner P, Anderson A, Charleston J, Chen Z, Ford V, Makos G, et al. Hypertension awareness, treatment, and control in adults with CKD: results from the Chronic Renal Insufficiency Cohort (CRIC) study. Am J Kidney Dis Off J Natl Kidney Found. 2010;55(3):441–51.
National Kidney Foundation. K/DOQI clinical practice guidelines for chronic kidney disease: evaluation, classification and stratification. Am J Kidney Dis. 2002;39(9suppl 1):S1–S266.
Saran R, Li Y, Robinson B, Abbott KC, Agodoa LY, Ayanian J, Bragg-Gresham J, Balkrishnan R, Chen JL, Cope E, Eggers PW, Gillen D, Gipson D, Hailpern SM, Hall YN, He K, Herman W, Heung M, Hirth RA, Hutton D, Jacobsen SJ, Kalantar-Zadeh K, Kovesdy CP, Lu Y, Molnar MZ, Morgenstern H, Nallamothu B, Nguyen DV, O'Hare AM, Plattner B, Pisoni R, Port FK, Rao P, Rhee CM, Sakhuja A, Schaubel DE, Selewski DT, Shahinian V, Sim JJ, Song P, Streja E, Kurella Tamura M, Tentori F, White S, Woodside K, Hirth RA. US Renal data system 2015 annual data report: epidemiology of kidney disease in the United States. Am J Kidney Dis. 2016;67(3 Supplement 1):S1–434.
World Health Organization. Global report on diabetes. Wolrd Health Day 2016. Geneva; 2016 p. 1–86.
Centers for Disease Control and Prevention. National diabetes statistics report: estimates of diabetes and its burden in the United States, 2014. Atlanta: US Department of Health and Human Services; 2014.
Ritz E, Orth SR. Nephropathy in patients with type 2 diabetes mellitus. N Engl J Med. 1999;341(15):1127–33.
Afkarian M, Zelnick LR, Hall YN, Heagerty PJ, Tuttle K, Weiss NS, et al. Clinical manifestations of kidney disease among US adults with diabetes, 1988-2014. JAMA. 2016;316(6):602–10.
Carroll MD, Kit BK, Lacher DA, Yoon SS. Total and high-density lipoprotein cholesterol in adults: National Health and nutrition examination survey, 2011-2012. NCHS Data Brief. 2013;132:1–8.
Mozaffarian D, Benjamin EJ, Go AS, Arnett DK, Blaha MJ, Cushman M, et al. Heart disease and stroke statistics--2015 update: a report from the American Heart Association. Circulation. 2015;131(4):e29–322.
Kasiske BL. Hyperlipidemia in patients with chronic renal disease. Am J Kidney Dis Off J Natl Kidney Found. 1998;32(5 Suppl 3):S142–56.
Centers for Disease Control and Prevention. Smoking: early release of selected estimates based on data from the national health interview survey, 2014. Atlanta: Centers for Disease Control and Prevention; June 2015.
Global Burden of Metabolic Risk Factors for Chronic Diseases Collaboration. Cardiovascular disease, chronic kidney disease, and diabetes mortality burden of cardiometabolic risk factors from 1980 to 2010: a comparative risk assessment. Lancet Diabetes Endocrinol. 2014 Aug;2(8):634–47.
National Center for Health Statistics. Health, United States, 2015: with special feature on racial and ethnic health disparities. Hyattsville: National Center for Health Statistics; 2016.
Centers for Disease Control and Prevention. Leisure-time physical activity: early release of selected estimates based on data from the national health interview survey, 2014. Atlanta: Centers for Disease Control and Prevention; June 2015.
Centers for Disease Control and Prevention (CDC). National chronic kidney disease fact sheet: general information and national estimates on chronic kidney disease in the United States, 2014. Atlanta: US Department of Health and Human Services, Centers for Disease Control and Prevention; 2014.
Chronic Kidney Disease [Internet]. World Kidney Day. [cited 2016 Sep 30]. Available from: http://www.worldkidneyday.org/faqs/chronic-kidney-disease/
Chapter 1: definition and classification of CKD. Kidney Int Suppl (2011). 2013;3(1):19–62. PMID: 25018975 PMCID: PMC4089693. https://doi.org/10.1038/kisup.2012.64.
Ishani A, Grandits GA, Grimm RH, Svendsen KH, Collins AJ, Prineas RJ, et al. Association of single measurements of dipstick proteinuria, estimated glomerular filtration rate, and hematocrit with 25-year incidence of end-stage renal disease in the multiple risk factor intervention trial. J Am Soc Nephrol. 2006;17(5):1444–52.
Cirillo M, Laurenzi M, Mancini M, Zanchetti A, Lombardi C, De Santo NG. Low glomerular filtration in the population: prevalence, associated disorders, and awareness. Kidney Int. 2006;70(4):800–6.
Grams ME, Chow EKH, Segev DL, Coresh J. Lifetime incidence of CKD stages 3-5 in the United States. Am J Kidney Dis Off J Natl Kidney Found. 2013;62(2):245–52.
Cooper BA, Branley P, Bulfone L, Collins JF, Craig JC, Fraenkel MB, et al. A randomized, controlled trial of early versus late initiation of dialysis. N Engl J Med. 2010;363(7):609–19.
Hallan SI, Coresh J, Astor BC, Asberg A, Powe NR, Romundstad S, et al. International comparison of the relationship of chronic kidney disease prevalence and ESRD risk. J Am Soc Nephrol. 2006;17(8):2275–84.
Patel UD, Young EW, Ojo AO, Hayward RA. CKD progression and mortality among older patients with diabetes. Am J Kidney Dis Off J Natl Kidney Found. 2005;46(3):406–14.
Levey AS, Stevens LA, Schmid CH, Zhang YL, Castro AF, Feldman HI, et al. A new equation to estimate glomerular filtration rate. Ann Intern Med. 2009;150(9):604–12.
Matsushita K, Mahmoodi BK, Woodward M, Emberson JR, Jafar TH, Jee SH, et al. Comparison of risk prediction using the CKD-EPI equation and the MDRD study equation for estimated glomerular filtration rate. JAMA. 2012;307(18):1941–51.
Stevens LA, Levey AS. Measured GFR as a confirmatory test for estimated GFR. J Am Soc Nephrol. 2009;20(11):2305–13.
Fashuyi SA. The pattern of human intestinal helminth infections in farming communities in different parts of Ondo state, Nigeria. West Afr J Med. 1992;11(1):13–7.
Shidham G, Hebert LA. Timed urine collections are not needed to measure urine protein excretion in clinical practice. Am J Kidney Dis Off J Natl Kidney Found. 2006;47(1):8–14.
Foley RN, Wang C, Collins AJ. Cardiovascular risk factor profiles and kidney function stage in the US general population: the NHANES III study. Mayo Clin Proc. 2005;80(10):1270–7.
Fox CS, Matsushita K, Woodward M, Bilo HJG, Chalmers J, Heerspink HJL, et al. Associations of kidney disease measures with mortality and end-stage renal disease in individuals with and without diabetes: a meta-analysis. Lancet Lond Engl. 2012;380(9854):1662–73.
Heerspink HJL, Kröpelin TF, Hoekman J, de Zeeuw D. Reducing albuminuria as surrogate endpoint (REASSURE) consortium. Drug-induced reduction in albuminuria is associated with subsequent Renoprotection: a meta-analysis. J Am Soc Nephrol. 2015;26(8):2055–64.
Hallan S, Astor B, Romundstad S, Aasarød K, Kvenild K, Coresh J. Association of kidney function and albuminuria with cardiovascular mortality in older vs younger individuals: the HUNT II study. Arch Intern Med. 2007;167(22):2490–6.
Chronic Kidney Disease Prognosis Consortium, Matsushita K, van der Velde M, Astor BC, Woodward M, Levey AS, et al. Association of estimated glomerular filtration rate and albuminuria with all-cause and cardiovascular mortality in general population cohorts: a collaborative meta-analysis. Lancet. 2010;375(9731):2073–81.
Hillege HL, Fidler V, Diercks GFH, van Gilst WH, de Zeeuw D, van Veldhuisen DJ, et al. Urinary albumin excretion predicts cardiovascular and noncardiovascular mortality in general population. Circulation. 2002;106(14):1777–82.
Arnlöv J, Evans JC, Meigs JB, Wang TJ, Fox CS, Levy D, et al. Low-grade albuminuria and incidence of cardiovascular disease events in nonhypertensive and nondiabetic individuals: the Framingham heart study. Circulation. 2005;112(7):969–75.
Tanaka F, Komi R, Makita S, Onoda T, Tanno K, Ohsawa M, et al. Low-grade albuminuria and incidence of cardiovascular disease and all-cause mortality in nondiabetic and normotensive individuals. J Hypertens. 2016;34(3):506–12. discussion 512
Kunimura A, Ishii H, Uetani T, Harada K, Kataoka T, Takeshita M, et al. Prognostic value of albuminuria on cardiovascular outcomes after elective percutaneous coronary intervention. Am J Cardiol. 2016;117(5):714–9.
Ibsen H, Olsen MH, Wachtell K, Borch-Johnsen K, Lindholm LH, Mogensen CE, et al. Reduction in albuminuria translates to reduction in cardiovascular events in hypertensive patients: losartan intervention for endpoint reduction in hypertension study. Hypertens Dallas Tex 1979. 2005;45(2):198–202.
Go AS, Chertow GM, Fan D, McCulloch CE, Hsu C. Chronic kidney disease and the risks of death, cardiovascular events, and hospitalization. N Engl J Med. 2004;351(13):1296–305.
Sarnak MJ, Levey AS, Schoolwerth AC, Coresh J, Culleton B, Hamm LL, et al. Kidney disease as a risk factor for development of cardiovascular disease: a statement from the American Heart Association councils on kidney in cardiovascular disease, high blood pressure research, clinical cardiology, and epidemiology and prevention. Circulation. 2003;108(17):2154–69.
Tonelli M, Wiebe N, Culleton B, House A, Rabbat C, Fok M, et al. Chronic kidney disease and mortality risk: a systematic review. J Am Soc Nephrol. 2006;17(7):2034–47.
Collins AJ, Li S, Gilbertson DT, Liu J, Chen S-C, Herzog CA. Chronic kidney disease and cardiovascular disease in the Medicare population. Kidney Int Suppl. 2003;87:S24–31.
Foley RN, Murray AM, Li S, Herzog CA, McBean AM, Eggers PW, et al. Chronic kidney disease and the risk for cardiovascular disease, renal replacement, and death in the United States Medicare population, 1998 to 1999. J Am Soc Nephrol. 2005;16(2):489–95.
Meisinger C, Döring A, Löwel H, KORA Study Group. Chronic kidney disease and risk of incident myocardial infarction and all-cause and cardiovascular disease mortality in middle-aged men and women from the general population. Eur Heart J. 2006;27(10):1245–50.
Anavekar NS, McMurray JJV, Velazquez EJ, Solomon SD, Kober L, Rouleau J-L, et al. Relation between renal dysfunction and cardiovascular outcomes after myocardial infarction. N Engl J Med. 2004;351(13):1285–95.
Tonelli M, Muntner P, Lloyd A, Manns BJ, Klarenbach S, Pannu N, et al. Risk of coronary events in people with chronic kidney disease compared with those with diabetes: a population-level cohort study. Lancet Lond Engl. 2012;380(9844):807–14.
Matsushita K, Coresh J, Sang Y, Chalmers J, Fox C, Guallar E, et al. Estimated glomerular filtration rate and albuminuria for prediction of cardiovascular outcomes: a collaborative meta-analysis of individual participant data. Lancet Diabetes Endocrinol. 2015;3(7):514–25.
Joint British Societies for the prevention of cardiovascular disease: the JBS3 risk calculator. http://www.jbs3risk.com/pages/risk_calculator.htm.
Bhatti NK, Karimi Galougahi K, Paz Y, Nazif T, Moses JW, Leon MB, et al. Diagnosis and Management of Cardiovascular Disease in Advanced and End-Stage Renal Disease. J Am Heart Assoc. 2016;5(8):e003648.
Stack AG, Bloembergen WE. A cross-sectional study of the prevalence and clinical correlates of congestive heart failure among incident US dialysis patients. Am J Kidney Dis Off J Natl Kidney Found. 2001;38(5):992–1000.
Nakano T, Ninomiya T, Sumiyoshi S, Fujii H, Doi Y, Hirakata H, et al. Association of kidney function with coronary atherosclerosis and calcification in autopsy samples from Japanese elders: the Hisayama study. Am J Kidney Dis Off J Natl Kidney Found. 2010;55(1):21–30.
Joki N, Hase H, Nakamura R, Yamaguchi T. Onset of coronary artery disease prior to initiation of haemodialysis in patients with end-stage renal disease. Nephrol Dial Transplant Off Publ Eur Dial Transpl Assoc – Eur Ren Assoc. 1997;12(4):718–23.
Wada M, Ueda Y, Higo T, Matsuo K, Nishio M, Hirata A, et al. Chronic kidney disease and coronary artery vulnerable plaques. Clin J Am Soc Nephrol. 2011;6(12):2792–8.
Kato K, Yonetsu T, Jia H, Abtahian F, Vergallo R, Hu S, et al. Nonculprit coronary plaque characteristics of chronic kidney disease. Circ Cardiovasc Imaging. 2013;6(3):448–56.
Nakano T, Ninomiya T, Sumiyoshi S, Onimaru M, Fujii H, Itabe H, et al. Chronic kidney disease is associated with neovascularization and intraplaque hemorrhage in coronary atherosclerosis in elders: results from the Hisayama study. Kidney Int. 2013;84(2):373–80.
Afkarian M, Sachs MC, Kestenbaum B, Hirsch IB, Tuttle KR, Himmelfarb J, et al. Kidney disease and increased mortality risk in type 2 diabetes. J Am Soc Nephrol. 2013;24(2):302–8.
Levin A, Thompson CR, Ethier J, Carlisle EJ, Tobe S, Mendelssohn D, et al. Left ventricular mass index increase in early renal disease: impact of decline in hemoglobin. Am J Kidney Dis Off J Natl Kidney Found. 1999;34(1):125–34.
Peterson GE, de Backer T, Contreras G, Wang X, Kendrick C, Greene T, et al. Relationship of left ventricular hypertrophy and diastolic function with cardiovascular and renal outcomes in African Americans with hypertensive chronic kidney disease. Hypertens Dallas Tex 1979. 2013;62(3):518–25.
London GM. Cardiovascular disease in chronic renal failure: pathophysiologic aspects. Semin Dial. 2003;16(2):85–94.
Bansal N, Keane M, Delafontaine P, Dries D, Foster E, Gadegbeku CA, et al. A longitudinal study of left ventricular function and structure from CKD to ESRD: the CRIC study. Clin J Am Soc Nephrol. 2013;8(3):355–62.
Zoccali C, Benedetto FA, Mallamaci F, Tripepi G, Giacone G, Cataliotti A, et al. Prognostic value of echocardiographic indicators of left ventricular systolic function in asymptomatic dialysis patients. J Am Soc Nephrol. 2004;15(4):1029–37.
Kramer H, Toto R, Peshock R, Cooper R, Victor R. Association between chronic kidney disease and coronary artery calcification: the Dallas heart study. J Am Soc Nephrol. 2005;16(2):507–13.
Haydar AA, Hujairi NMA, Covic AA, Pereira D, Rubens M, Goldsmith DJA. Coronary artery calcification is related to coronary atherosclerosis in chronic renal disease patients: a study comparing EBCT-generated coronary artery calcium scores and coronary angiography. Nephrol Dial Transplant Off Publ Eur Dial Transpl Assoc – Eur Ren Assoc. 2004;19(9):2307–12.
Goodman WG, Goldin J, Kuizon BD, Yoon C, Gales B, Sider D, et al. Coronary-artery calcification in young adults with end-stage renal disease who are undergoing dialysis. N Engl J Med. 2000;342(20):1478–83.
Matsuoka M, Iseki K, Tamashiro M, Fujimoto N, Higa N, Touma T, et al. Impact of high coronary artery calcification score (CACS) on survival in patients on chronic hemodialysis. Clin Exp Nephrol. 2004;8(1):54–8.
Block GA, Raggi P, Bellasi A, Kooienga L, Spiegel DM. Mortality effect of coronary calcification and phosphate binder choice in incident hemodialysis patients. Kidney Int. 2007;71(5):438–41.
Ix JH, Katz R, Kestenbaum B, Fried LF, Kramer H, Stehman-Breen C, et al. Association of mild to moderate kidney dysfunction and coronary calcification. J Am Soc Nephrol. 2008 Mar;19(3):579–85.
Fujimoto N, Iseki K, Tokuyama K, Tamashiro M, Takishita S. Significance of coronary artery calcification score (CACS) for the detection of coronary artery disease (CAD) in chronic dialysis patients. Clin Chim Acta Int J Clin Chem. 2006;367(1–2):98–102.
Sharples EJ, Pereira D, Summers S, Cunningham J, Rubens M, Goldsmith D, et al. Coronary artery calcification measured with electron-beam computerized tomography correlates poorly with coronary artery angiography in dialysis patients. Am J Kidney Dis Off J Natl Kidney Found. 2004;43(2):313–9.
Lentine KL, Costa SP, Weir MR, Robb JF, Fleisher LA, Kasiske BL, et al. Cardiac disease evaluation and management among kidney and liver transplantation candidates: a scientific statement from the American Heart Association and the American College of Cardiology Foundation. J Am Coll Cardiol. 2012;60(5):434–80.
Oberg BP, McMenamin E, Lucas FL, McMonagle E, Morrow J, Ikizler TA, et al. Increased prevalence of oxidant stress and inflammation in patients with moderate to severe chronic kidney disease. Kidney Int. 2004;65(3):1009–16.
Menon V, Greene T, Wang X, Pereira AA, Marcovina SM, Beck GJ, et al. C-reactive protein and albumin as predictors of all-cause and cardiovascular mortality in chronic kidney disease. Kidney Int. 2005;68(2):766–72.
Li W-J, Chen X-M, Nie X-Y, Zhang J, Cheng Y-J, Lin X-X, et al. Cardiac troponin and C-reactive protein for predicting all-cause and cardiovascular mortality in patients with chronic kidney disease: a meta-analysis. Clin São Paulo Braz. 2015;70(4):301–11.
Wanner C, Metzger T. C-reactive protein a marker for all-cause and cardiovascular mortality in haemodialysis patients. Nephrol Dial Transplant Off Publ Eur Dial Transpl Assoc – Eur Ren Assoc. 2002;17(Suppl 8):29–32.
den Elzen WPJ, van Manen JG, Boeschoten EW, Krediet RT, Dekker FW. The effect of single and repeatedly high concentrations of C-reactive protein on cardiovascular and non-cardiovascular mortality in patients starting with dialysis. Nephrol Dial Transplant Off Publ Eur Dial Transpl Assoc – Eur Ren Assoc. 2006;21(6):1588–95.
Pun PH, Smarz TR, Honeycutt EF, Shaw LK, Al-Khatib SM, Middleton JP. Chronic kidney disease is associated with increased risk of sudden cardiac death among patients with coronary artery disease. Kidney Int. 2009;76(6):652–8.
Herzog CA, Mangrum JM, Passman R. Sudden cardiac death and dialysis patients. Semin Dial. 2008;21(4):300–7.
Selby NM, Burton JO, Chesterton LJ, McIntyre CW. Dialysis-induced regional left ventricular dysfunction is ameliorated by cooling the dialysate. Clin J Am Soc Nephrol. 2006;1(6):1216–25.
McIntyre CW, Burton JO, Selby NM, Leccisotti L, Korsheed S, Baker CSR, et al. Hemodialysis-induced cardiac dysfunction is associated with an acute reduction in global and segmental myocardial blood flow. Clin J Am Soc Nephrol. 2008;3(1):19–26.
Herzog CA, Ma JZ, Collins AJ. Poor long-term survival after acute myocardial infarction among patients on long-term dialysis. N Engl J Med. 1998;339(12):799–805.
Go AS, Bansal N, Chandra M, Lathon PV, Fortmann SP, Iribarren C, et al. Chronic kidney disease and risk for presenting with acute myocardial infarction versus stable exertional angina in adults with coronary heart disease. J Am Coll Cardiol. 2011;58(15):1600–7.
Sosnov J, Lessard D, Goldberg RJ, Yarzebski J, Gore JM. Differential symptoms of acute myocardial infarction in patients with kidney disease: a community-wide perspective. Am J Kidney Dis Off J Natl Kidney Found. 2006;47(3):378–84.
Herzog CA, Littrell K, Arko C, Frederick PD, Blaney M. Clinical characteristics of dialysis patients with acute myocardial infarction in the United States: a collaborative project of the United States renal data system and the National Registry of myocardial infarction. Circulation. 2007;116(13):1465–72.
Matsushita K, Ballew SH, Coresh J. Cardiovascular risk prediction in people with chronic kidney disease. Curr Opin Nephrol Hypertens. 2016;25(6):518–23.
Green TR, Golper TA, Swenson RD, Pulliam JP, Morris CD. Diagnostic value of creatine kinase and creatine kinase MB isoenzyme in chronic hemodialysis patients: a longitudinal study. Clin Nephrol. 1986;25(1):22–7.
Mishra RK, Li Y, DeFilippi C, Fischer MJ, Yang W, Keane M, et al. Association of cardiac troponin T with left ventricular structure and function in CKD. Am J Kidney Dis Off J Natl Kidney Found. 2013;61(5):701–9.
Stacy SR, Suarez-Cuervo C, Berger Z, Wilson LM, Yeh H-C, Bass EB, et al. Role of troponin in patients with chronic kidney disease and suspected acute coronary syndrome: a systematic review. Ann Intern Med. 2014;161(7):502–12.
Michos ED, Wilson LM, Yeh H-C, Berger Z, Suarez-Cuervo C, Stacy SR, et al. Prognostic value of cardiac troponin in patients with chronic kidney disease without suspected acute coronary syndrome: a systematic review and meta-analysis. Ann Intern Med. 2014;161(7):491–501.
Ohtake T, Kobayashi S, Moriya H, Negishi K, Okamoto K, Maesato K, et al. High prevalence of occult coronary artery stenosis in patients with chronic kidney disease at the initiation of renal replacement therapy: an angiographic examination. J Am Soc Nephrol. 2005;16(4):1141–8.
Marwick TH, Steinmuller DR, Underwood DA, Hobbs RE, Go RT, Swift C, et al. Ineffectiveness of dipyridamole SPECT thallium imaging as a screening technique for coronary artery disease in patients with end-stage renal failure. Transplantation. 1990;49(1):100–3.
Dahan M, Viron BM, Poiseau E, Kolta AM, Aubry N, Paillole C, et al. Combined dipyridamole-exercise stress echocardiography for detection of myocardial ischemia in hemodialysis patients: an alternative to stress nuclear imaging. Am J Kidney Dis Off J Natl Kidney Found. 2002;40(4):737–44.
Rabbat CG, Treleaven DJ, Russell JD, Ludwin D, Cook DJ. Prognostic value of myocardial perfusion studies in patients with end-stage renal disease assessed for kidney or kidney-pancreas transplantation: a meta-analysis. J Am Soc Nephrol. 2003;14(2):431–9.
Nauta ST, van Domburg RT, Nuis R-J, Akkerhuis M, Deckers JW. Decline in 20-year mortality after myocardial infarction in patients with chronic kidney disease: evolution from the prethrombolysis to the percutaneous coronary intervention era. Kidney Int. 2013;84(2):353–8.
Vavalle JP, van Diepen S, Clare RM, Hochman JS, Weaver WD, Mehta RH, et al. Renal failure in patients with ST-segment elevation acute myocardial infarction treated with primary percutaneous coronary intervention: predictors, clinical and angiographic features, and outcomes. Am Heart J. 2016;173:57–66.
Azzalini L, Spagnoli V, Ly HQ. Contrast-induced nephropathy: from pathophysiology to preventive strategies. Can J Cardiol. 2016;32(2):247–55.
Silver SA, Shah PM, Chertow GM, Harel S, Wald R, Harel Z. Risk prediction models for contrast induced nephropathy: systematic review. BMJ. 2015;351:h4395.
Zhang B, Liang L, Chen W, Liang C, Zhang S. The efficacy of sodium bicarbonate in preventing contrast-induced nephropathy in patients with pre-existing renal insufficiency: a meta-analysis. BMJ Open. 2015;5(3):e006989.
Bainey KR, Rahim S, Etherington K, Rokoss ML, Natarajan MK, Velianou JL, et al. Effects of withdrawing vs continuing renin-angiotensin blockers on incidence of acute kidney injury in patients with renal insufficiency undergoing cardiac catheterization: results from the angiotensin converting enzyme inhibitor/angiotensin receptor blocker and contrast induced nephropathy in patients receiving cardiac catheterization (CAPTAIN) trial. Am Heart J. 2015;170(1):110–6.
Favre GA, Esnault VLM, Van Obberghen E. Modulation of glucose metabolism by the renin-angiotensin-aldosterone system. Am J Physiol Endocrinol Metab. 2015;308(6):E435–49.
Khan UA, Garg AX, Parikh CR, Coca SG. Prevention of chronic kidney disease and subsequent effect on mortality: a systematic review and meta-analysis. PLoS One. 2013;8(8):e71784.
Kanno Y, Kaneko K, Kaneko M, Kotaki S, Mimura T, Takane H, et al. Angiotensin receptor antagonist regresses left ventricular hypertrophy associated with diabetic nephropathy in dialysis patients. J Cardiovasc Pharmacol. 2004;43(3):380–6.
Yang L-Y, Ge X, Wang Y-L, Ma K-L, Liu H, Zhang X-L, et al. Angiotensin receptor blockers reduce left ventricular hypertrophy in dialysis patients: a meta-analysis. Am J Med Sci. 2013;345(1):1–9.
Zhang L, Zeng X, Fu P, Wu HM. Angiotensin-converting enzyme inhibitors and angiotensin receptor blockers for preserving residual kidney function in peritoneal dialysis patients. Cochrane Database Syst Rev. 2014;6:CD009120.
Akbari A, Knoll G, Ferguson D, McCormick B, Davis A, Biyani M. Angiotensin-converting enzyme inhibitors and angiotensin receptor blockers in peritoneal dialysis: systematic review and meta-analysis of randomized controlled trials. Perit Dial Int J Int Soc Perit Dial. 2009;29(5):554–61.
Curtis JJ, Laskow DA, Jones PA, Julian BA, Gaston RS, Luke RG. Captopril-induced fall in glomerular filtration rate in cyclosporine-treated hypertensive patients. J Am Soc Nephrol. 1993;3(9):1570–4.
Hiremath S, Fergusson D, Doucette S, Mulay AV, Knoll GA. Renin angiotensin system blockade in kidney transplantation: a systematic review of the evidence. Am J Transplant Off J Am Soc Transplant Am Soc Transplant Surg. 2007;7(10):2350–60.
Ibrahim HN, Jackson S, Connaire J, Matas A, Ney A, Najafian B, et al. Angiotensin II blockade in kidney transplant recipients. J Am Soc Nephrol. 2013 Feb;24(2):320–7.
Tokmakova MP, Skali H, Kenchaiah S, Braunwald E, Rouleau JL, Packer M, et al. Chronic kidney disease, cardiovascular risk, and response to angiotensin-converting enzyme inhibition after myocardial infarction: the survival and ventricular enlargement (SAVE) study. Circulation. 2004;110(24):3667–73.
Hillege HL, Nitsch D, Pfeffer MA, Swedberg K, McMurray JJV, Yusuf S, et al. Renal function as a predictor of outcome in a broad spectrum of patients with heart failure. Circulation. 2006;113(5):671–8.
Damman K, Navis G, Voors AA, Asselbergs FW, Smilde TDJ, Cleland JGF, et al. Worsening renal function and prognosis in heart failure: systematic review and meta-analysis. J Card Fail. 2007;13(8):599–608.
Shlipak MG, Smith GL, Rathore SS, Massie BM, Krumholz HM. Renal function, digoxin therapy, and heart failure outcomes: evidence from the digoxin intervention group trial. J Am Soc Nephrol. 2004;15(8):2195–203.
Smith GL, Lichtman JH, Bracken MB, Shlipak MG, Phillips CO, DiCapua P, et al. Renal impairment and outcomes in heart failure: systematic review and meta-analysis. J Am Coll Cardiol. 2006;47(10):1987–96.
Hillege HL, Girbes AR, de Kam PJ, Boomsma F, de Zeeuw D, Charlesworth A, et al. Renal function, neurohormonal activation, and survival in patients with chronic heart failure. Circulation. 2000;102(2):203–10.
McAlister FA, Ezekowitz J, Tonelli M, Armstrong PW. Renal insufficiency and heart failure: prognostic and therapeutic implications from a prospective cohort study. Circulation. 2004;109(8):1004–9.
Clark H, Krum H, Hopper I. Worsening renal function during renin-angiotensin-aldosterone system inhibitor initiation and long-term outcomes in patients with left ventricular systolic dysfunction. Eur J Heart Fail. 2014;16(1):41–8.
Ezekowitz J, McAlister FA, Humphries KH, Norris CM, Tonelli M, Ghali WA, et al. The association among renal insufficiency, pharmacotherapy, and outcomes in 6,427 patients with heart failure and coronary artery disease. J Am Coll Cardiol. 2004;44(8):1587–92.
Pitt B, Zannad F, Remme WJ, Cody R, Castaigne A, Perez A, et al. The effect of spironolactone on morbidity and mortality in patients with severe heart failure. Randomized Aldactone evaluation study investigators. N Engl J Med. 1999;341(10):709–17.
Zannad F, McMurray JJV, Krum H, van Veldhuisen DJ, Swedberg K, Shi H, et al. Eplerenone in patients with systolic heart failure and mild symptoms. N Engl J Med. 2011;364(1):11–21.
Harel Z, Gilbert C, Wald R, Bell C, Perl J, Juurlink D, et al. The effect of combination treatment with aliskiren and blockers of the renin-angiotensin system on hyperkalaemia and acute kidney injury: systematic review and meta-analysis. BMJ. 2012;344:e42.
Parving H-H, Brenner BM, McMurray JJV, de Zeeuw D, Haffner SM, Solomon SD, et al. Cardiorenal end points in a trial of aliskiren for type 2 diabetes. N Engl J Med. 2012;367(23):2204–13.
Mann JFE, Schmieder RE, McQueen M, Dyal L, Schumacher H, Pogue J, et al. Renal outcomes with telmisartan, ramipril, or both, in people at high vascular risk (the ONTARGET study): a multicentre, randomised, double-blind, controlled trial. Lancet Lond Engl. 2008;372(9638):547–53.
ONTARGET Investigators, Yusuf S, Teo KK, Pogue J, Dyal L, Copland I, et al. Telmisartan, ramipril, or both in patients at high risk for vascular events. N Engl J Med. 2008;358(15):1547–59.
Makani H, Bangalore S, Desouza KA, Shah A, Messerli FH. Efficacy and safety of dual blockade of the renin-angiotensin system: meta-analysis of randomised trials. BMJ. 2013;346:f360.
Susantitaphong P, Sewaralthahab K, Balk EM, Eiam-ong S, Madias NE, Jaber BL. Efficacy and safety of combined vs. single renin-angiotensin-aldosterone system blockade in chronic kidney disease: a meta-analysis. Am J Hypertens. 2013 Mar;26(3):424–41.
Bolignano D, Palmer SC, Navaneethan SD, Strippoli GFM. Aldosterone antagonists for preventing the progression of chronic kidney disease. Cochrane Database Syst Rev. 2014;4:CD007004.
Bangalore S, Kumar S, Messerli FH. When conventional heart failure therapy is not enough: angiotensin receptor blocker, direct renin inhibitor, or aldosterone antagonist? Congest Heart Fail Greenwich Conn. 2013;19(3):107–15.
Arici M, Erdem Y. Dual blockade of the renin-angiotensin system for cardiorenal protection: an update. Am J Kidney Dis Off J Natl Kidney Found. 2009;53(2):332–45.
James PA, Oparil S, Carter BL, Cushman WC, Dennison-Himmelfarb C, Handler J, et al. 2014 evidence-based guideline for the management of high blood pressure in adults: report from the panel members appointed to the eighth joint National Committee (JNC 8). JAMA. 2014;311(5):507–20.
Becker GJ, Wheeler DC, De Zeeuw D, Fujita T, Furth SL, Holdaas H, Mendis S, Oparil S, Perkovic V, Rodrigues CI, Sarnak MJ. Kidney Disease: Improving Global Outcomes (KDIGO) Blood Pressure Work Group: KDIGO clinical practice guideline for the management of blood pressure in chronic kidney disease. Kidney Int Suppl. 2012;2(5):337–414.
Verbeke F, Lindley E, Van Bortel L, Vanholder R, London G, Cochat P, et al. A European renal best practice (ERBP) position statement on the kidney disease: improving global outcomes (KDIGO) clinical practice guideline for the management of blood pressure in non-dialysis-dependent chronic kidney disease: an endorsement with some caveats for real-life application. Nephrol Dial Transplant Off Publ Eur Dial Transpl Assoc – Eur Ren Assoc. 2014;29(3):490–6.
SPRINT Research Group, Wright JT, Williamson JD, Whelton PK, Snyder JK, Sink KM, et al. A randomized trial of intensive versus standard blood-pressure control. N Engl J Med. 2015;373(22):2103–16.
National Kidney Foundation. KDOQI clinical practice guideline for diabetes and CKD: 2012 update. Am J Kidney Dis Off J Natl Kidney Found. 2012;60(5):850–86.
Qaseem A, Hopkins RH, Sweet DE, Starkey M, Shekelle P. Clinical Guidelines Committee of the American college of physicians. Screening, monitoring, and treatment of stage 1 to 3 chronic kidney disease: a clinical practice guideline from the American College of physicians. Ann Intern Med. 2013;159(12):835–47.
Taler SJ, Agarwal R, Bakris GL, Flynn JT, Nilsson PM, Rahman M, et al. KDOQI US commentary on the 2012 KDIGO clinical practice guideline for management of blood pressure in CKD. Am J Kidney Dis Off J Natl Kidney Found. 2013;62(2):201–13.
Bakris GL, Weir MR. Angiotensin-converting enzyme inhibitor-associated elevations in serum creatinine: is this a cause for concern? Arch Intern Med. 2000;160(5):685–93.
Kidney Disease Outcomes Quality Initiative (K/DOQI). K/DOQI clinical practice guidelines on hypertension and antihypertensive agents in chronic kidney disease. Am J Kidney Dis Off J Natl Kidney Found. 2004;43(5 Suppl 1):S1–290.
Bakris GL, Weir MR, Secic M, Campbell B, Weis-McNulty A. Differential effects of calcium antagonist subclasses on markers of nephropathy progression. Kidney Int. 2004;65(6):1991–2002.
Agodoa LY, Appel L, Bakris GL, Beck G, Bourgoignie J, Briggs JP, et al. Effect of ramipril vs amlodipine on renal outcomes in hypertensive nephrosclerosis: a randomized controlled trial. JAMA. 2001;285(21):2719–28.
Lewis EJ, Hunsicker LG, Clarke WR, Berl T, Pohl MA, Lewis JB, et al. Renoprotective effect of the angiotensin-receptor antagonist irbesartan in patients with nephropathy due to type 2 diabetes. N Engl J Med. 2001;345(12):851–60.
Agarwal R, Sinha AD, Pappas MK, Abraham TN, Tegegne GG. Hypertension in hemodialysis patients treated with atenolol or lisinopril: a randomized controlled trial. Nephrol Dial Transplant Off Publ Eur Dial Transpl Assoc – Eur Ren Assoc. 2014;29(3):672–81.
Dinneen SF, Gerstein HC. The association of microalbuminuria and mortality in non-insulin-dependent diabetes mellitus. A systematic overview of the literature. Arch Intern Med. 1997;157(13):1413–8.
Strippoli GFM, Bonifati C, Craig M, Navaneethan SD, Craig JC. Angiotensin converting enzyme inhibitors and angiotensin II receptor antagonists for preventing the progression of diabetic kidney disease. Cochrane Database Syst Rev. 2006;4:CD006257.
Brenner BM, Cooper ME, de Zeeuw D, Keane WF, Mitch WE, Parving HH, et al. Effects of losartan on renal and cardiovascular outcomes in patients with type 2 diabetes and nephropathy. N Engl J Med. 2001 Sep 20;345(12):861–9.
The Diabetes Control and Complications Trial Research Group. The effect of intensive treatment of diabetes on the development and progression of long-term complications in insulin-dependent diabetes mellitus. N Engl J Med. 1993;329(14):977–86.
Nathan DM, Cleary PA, Backlund J-YC, Genuth SM, Lachin JM, Orchard TJ, et al. Intensive diabetes treatment and cardiovascular disease in patients with type 1 diabetes. N Engl J Med. 2005;353(25):2643–53.
Nathan DM, Bayless M, Cleary P, Genuth S, Gubitosi-Klug R, Lachin JM, et al. Diabetes control and complications trial/epidemiology of diabetes interventions and complications study at 30 years: advances and contributions. Diabetes. 2013;62(12):3976–86.
UK Prospective Diabetes Study (UKPDS) Group. Intensive blood-glucose control with sulphonylureas or insulin compared with conventional treatment and risk of complications in patients with type 2 diabetes (UKPDS 33). Lancet Lond Engl. 1998;352(9131):837–53.
ADVANCE Collaborative Group, Patel A, MacMahon S, Chalmers J, Neal B, Billot L, et al. Intensive blood glucose control and vascular outcomes in patients with type 2 diabetes. N Engl J Med. 2008;358(24):2560–72.
Zoungas S, Chalmers J, Neal B, Billot L, Li Q, Hirakawa Y, et al. Follow-up of blood-pressure lowering and glucose control in type 2 diabetes. N Engl J Med. 2014;371(15):1392–406.
Ismail-Beigi F, Craven T, Banerji MA, Basile J, Calles J, Cohen RM, et al. Effect of intensive treatment of hyperglycaemia on microvascular outcomes in type 2 diabetes: an analysis of the ACCORD randomised trial. Lancet Lond Engl. 2010;376(9739):419–30.
Standards of medical care in diabetes—2016: summary of revisions. Diabetes Care. 2016;39(Supplement 1):S4–5.
Guideline Development Group. Clinical Practice Guideline on management of patients with diabetes and chronic kidney disease stage 3b or higher (eGFR <45 mL/min). Nephrol Dial Transplant Off Publ Eur Dial Transpl Assoc – Eur Ren Assoc. 2015;30(Suppl 2):ii1–142.
Inzucchi SE, Lipska KJ, Mayo H, Bailey CJ, McGuire DK. Metformin in patients with type 2 diabetes and kidney disease: a systematic review. JAMA. 2014;312(24):2668–75.
Lalau J-D, Arnouts P, Sharif A, De Broe ME. Metformin and other antidiabetic agents in renal failure patients. Kidney Int. 2015;87(2):308–22.
Palmer BF, Clegg DJ, Taylor SI, Weir MR. Diabetic ketoacidosis, sodium glucose transporter-2 inhibitors and the kidney. J Diabetes Complicat. 2016;30(6):1162–6.
Research C for DE and Drug Safety and Availability – FDA Drug Safety Communication: FDA strengthens kidney warnings for diabetes medicines canagliflozin (Invokana, Invokamet) and dapagliflozin (Farxiga, Xigduo XR) [Internet]. [cited 2016 Oct 1]. Available from: http://www.fda.gov/Drugs/DrugSafety/ucm505860.htm.
Baigent C, Landray MJ, Reith C, Emberson J, Wheeler DC, Tomson C, et al. The effects of lowering LDL cholesterol with simvastatin plus ezetimibe in patients with chronic kidney disease (study of heart and renal protection): a randomised placebo-controlled trial. Lancet Lond Engl. 2011;377(9784):2181–92.
Wanner C, Krane V, März W, Olschewski M, Mann JFE, Ruf G, et al. Atorvastatin in patients with type 2 diabetes mellitus undergoing hemodialysis. N Engl J Med. 2005;353(3):238–48.
Fellström BC, Jardine AG, Schmieder RE, Holdaas H, Bannister K, Beutler J, et al. Rosuvastatin and cardiovascular events in patients undergoing hemodialysis. N Engl J Med. 2009;360(14):1395–407.
Kidney Disease: Improving Global Outcomes (KDIGO) Lipid Work Group. KDIGO clinical practice guidelinefor lip management in chronic kidney disease. Kidney Int. Suppl. 2013;(3):259–305.
Domrongkitchaiporn S, Sritara P, Kitiyakara C, Stitchantrakul W, Krittaphol V, Lolekha P, et al. Risk factors for development of decreased kidney function in a southeast Asian population: a 12-year cohort study. J Am Soc Nephrol. 2005;16(3):791–9.
Iseki K, Ikemiya Y, Kinjo K, Inoue T, Iseki C, Takishita S. Body mass index and the risk of development of end-stage renal disease in a screened cohort. Kidney Int. 2004;65(5):1870–6.
Panwar B, Hanks LJ, Tanner RM, Muntner P, Kramer H, McClellan WM, et al. Obesity, metabolic health, and the risk of end-stage renal disease. Kidney Int. 2015;87(6):1216–22.
Poirier P, Giles TD, Bray GA, Hong Y, Stern JS, Pi-Sunyer FX, et al. Obesity and cardiovascular disease: pathophysiology, evaluation, and effect of weight loss: an update of the 1997 American Heart Association scientific statement on obesity and heart disease from the obesity Committee of the Council on nutrition, physical activity, and metabolism. Circulation. 2006;113(6):898–918.
Hsu C, McCulloch CE, Iribarren C, Darbinian J, Go AS. Body mass index and risk for end-stage renal disease. Ann Intern Med. 2006;144(1):21–8.
Praga M, Morales E. The fatty kidney: obesity and renal diease. Nephron. 2017;136:273–6.
Ogorodnikova AD, Kim M, McGinn AP, Muntner P, Khan U, Wildman RP. Incident cardiovascular disease events in metabolically benign obese individuals. Obes Silver Spring Md. 2012;20(3):651–9.
Lu JL, Kalantar-Zadeh K, Ma JZ, Quarles LD, Kovesdy CP. Association of body mass index with outcomes in patients with CKD. J Am Soc Nephrol. 2014;25(9):2088–96.
Abramowitz MK, Sharma D, Folkert VW. Hidden obesity in Dialysis patients: clinical implications. Semin Dial. 2016;29(5):391–5.
Kalantar-Zadeh K, Streja E, Kovesdy CP, Oreopoulos A, Noori N, Jing J, et al. The obesity paradox and mortality associated with surrogates of body size and muscle mass in patients receiving hemodialysis. Mayo Clin Proc. 2010;85(11):991–1001.
Postorino M, Marino C, Tripepi G, Zoccali C. CREDIT (Calabria registry of Dialysis and transplantation) working group. Abdominal obesity and all-cause and cardiovascular mortality in end-stage renal disease. J Am Coll Cardiol. 2009;53(15):1265–72.
Ezzati M, Lopez AD, Rodgers A, Vander Hoorn S, Murray CJL. Comparative risk assessment collaborating group. Selected major risk factors and global and regional burden of disease. Lancet Lond Engl. 2002;360(9343):1347–60.
Ejerblad E, Fored CM, Lindblad P, Fryzek J, Dickman PW, Elinder C-G, et al. Association between smoking and chronic renal failure in a nationwide population-based case-control study. J Am Soc Nephrol. 2004;15(8):2178–85.
Liang KV, Greene EL, Oei LS, Lewin M, Lager D, Sethi S. Nodular glomerulosclerosis: renal lesions in chronic smokers mimic chronic thrombotic microangiopathy and hypertensive lesions. Am J Kidney Dis Off J Natl Kidney Found. 2007;49(4):552–9.
Nasr SH, D’Agati VD. Nodular glomerulosclerosis in the nondiabetic smoker. J Am Soc Nephrol. 2007;18(7):2032–6.
Kusaba T, Hatta T, Sonomura K, Mori Y, Tokoro T, Nagata T, et al. Idiopathic nodular glomerulosclerosis: three Japanese cases and review of the literature. Clin Nephrol. 2007;67(1):32–7.
Remuzzi G. Cigarette smoking and renal function impairment. Am J Kidney Dis Off J Natl Kidney Found. 1999;33(4):807–13.
Orth SR, Ogata H, Ritz E. Smoking and the kidney. Nephrol Dial Transplant Off Publ Eur Dial Transpl Assoc – Eur Ren Assoc. 2000;15(10):1509–11.
Pinto-Sietsma SJ, Mulder J, Janssen WM, Hillege HL, de Zeeuw D, de Jong PE. Smoking is related to albuminuria and abnormal renal function in nondiabetic persons. Ann Intern Med. 2000;133(8):585–91.
De Cosmo S, Lamacchia O, Rauseo A, Viti R, Gesualdo L, Pilotti A, et al. Cigarette smoking is associated with low glomerular filtration rate in male patients with type 2 diabetes. Diabetes Care. 2006;29(11):2467–70.
Orth SR, Schroeder T, Ritz E, Ferrari P. Effects of smoking on renal function in patients with type 1 and type 2 diabetes mellitus. Nephrol Dial Transplant Off Publ Eur Dial Transpl Assoc – Eur Ren Assoc. 2005;20(11):2414–9.
Haroun MK, Jaar BG, Hoffman SC, Comstock GW, Klag MJ, Coresh J. Risk factors for chronic kidney disease: a prospective study of 23,534 men and women in Washington County, Maryland. J Am Soc Nephrol. 2003;14(11):2934–41.
Staplin N, Haynes R, Herrington WG, Reith C, Cass A, Fellström B, et al. Smoking and adverse outcomes in patients with CKD: the study of heart and renal protection (SHARP). Am J Kidney Dis Off J Natl Kidney Found. 2016;68(3):371–80.
Cheung AK, Sarnak MJ, Yan G, Dwyer JT, Heyka RJ, Rocco MV, et al. Atherosclerotic cardiovascular disease risks in chronic hemodialysis patients. Kidney Int. 2000;58(1):353–62.
Foley RN, Herzog CA, Collins AJ. Smoking and cardiovascular outcomes in dialysis patients: the United States renal data system wave 2 study. Kidney Int. 2003;63(4):1462–7.
Siu AL, U.S. Preventive services task force. Behavioral and pharmacotherapy interventions for tobacco smoking cessation in adults, including pregnant women: U.S. preventive services task force recommendation statement. Ann Intern Med. 2015;163(8):622–34.
Van Craenenbroeck AH, Van Craenenbroeck EM, Van Ackeren K, Hoymans VY, Verpooten GA, Vrints CJ, et al. Impaired vascular function contributes to exercise intolerance in chronic kidney disease. Nephrol Dial Transplant Off Publ Eur Dial Transpl Assoc – Eur Ren Assoc. 2016.
Chen I-R, Wang S-M, Liang C-C, Kuo H-L, Chang C-T, Liu J-H, et al. Association of walking with survival and RRT among patients with CKD stages 3-5. Clin J Am Soc Nephrol. 2014;9(7):1183–9.
Wilkinson TJ, Shur NF, Smith AC. “Exercise as medicine” in chronic kidney disease. Scand J Med Sci Sports. 2016;26(8):985–8.
Robinson-Cohen C, Littman AJ, Duncan GE, Weiss NS, Sachs MC, Ruzinski J, et al. Physical activity and change in estimated GFR among persons with CKD. J Am Soc Nephrol. 2014;25(2):399–406.
Parker K. Intradialytic exercise is medicine for hemodialysis patients. Curr Sports Med Rep. 2016;15(4):269–75.
Heiwe S, Jacobson SH. Exercise training in adults with CKD: a systematic review and meta-analysis. Am J Kidney Dis Off J Natl Kidney Found. 2014;64(3):383–93.
Palmer S, Vecchio M, Craig JC, Tonelli M, Johnson DW, Nicolucci A, et al. Prevalence of depression in chronic kidney disease: systematic review and meta-analysis of observational studies. Kidney Int. 2013;84(1):179–91.
Foster MC, Coresh J, Fornage M, Astor BC, Grams M, Franceschini N, et al. APOL1 variants associate with increased risk of CKD among African Americans. J Am Soc Nephrol. 2013;24(9):1484–91.
Coronado Daza J, Martí-Carvajal AJ, Ariza García A, Rodelo Ceballos J, Yomayusa González N, Páez-Canro C, et al. Early versus delayed erythropoietin for the anaemia of end-stage kidney disease. Cochrane Database Syst Rev. 2015;12:CD011122.
Palmer SC, Saglimbene V, Mavridis D, Salanti G, Craig JC, Tonelli M, et al. Erythropoiesis-stimulating agents for anaemia in adults with chronic kidney disease: a network meta-analysis. Cochrane Database Syst Rev. 2014;12:CD010590.
Gossmann J, Burkhardt R, Harder S, Lenz T, Sedlmeyer A, Klinkhardt U, et al. Angiotensin II infusion increases plasma erythropoietin levels via an angiotensin II type 1 receptor-dependent pathway. Kidney Int. 2001;60(1):83–6.
Freudenthaler SM, Schenck T, Lucht I, Gleiter CH. Fenoterol stimulates human erythropoietin production via activation of the renin angiotensin system. Br J Clin Pharmacol. 1999;48(4):631–4.
Freudenthaler S, Benöhr P, Grenz A, Selzer T, Schmidt T, Mörike K, et al. Do alterations of endogenous angiotensin II levels regulate erythropoietin production in humans? Br J Clin Pharmacol. 2003;56(4):378–87.
Matsumura M, Nomura H, Koni I, Mabuchi H. Angiotensin-converting enzyme inhibitors are associated with the need for increased recombinant human erythropoietin maintenance doses in hemodialysis patients. Risks of cardiac disease in Dialysis patients study group. Nephron. 1997;77(2):164–8.
Navarro JF, Mora C, Rivero A. Effect of angiotensin-converting enzyme inhibitors on hematological parameters and recombinant human erythropoietin doses in peritoneal dialysis patients. Nephron. 1998;80(2):239.
Panwar B, Gutiérrez OM. Disorders of Iron metabolism and Anemia in chronic kidney disease. Semin Nephrol. 2016;36(4):252–61.
Ganz T, Nemeth E. Iron balance and the role of Hepcidin in chronic kidney disease. Semin Nephrol. 2016;36(2):87–93.
Pfeffer MA, Burdmann EA, Chen C-Y, Cooper ME, de Zeeuw D, Eckardt K-U, et al. A trial of darbepoetin alfa in type 2 diabetes and chronic kidney disease. N Engl J Med. 2009;361(21):2019–32.
Glassock RJ, Pecoits-Filho R, Barberato SH. Left ventricular mass in chronic kidney disease and ESRD. Clin J Am Soc Nephrol. 2009;4(Suppl 1):S79–91.
Collister D, Komenda P, Hiebert B, Gunasekara R, Xu Y, Eng F, et al. The effect of erythropoietin-stimulating agents on health-related quality of life in Anemia of chronic kidney disease: a systematic review and meta-analysis. Ann Intern Med. 2016;164(7):472–8.
Phrommintikul A, Haas SJ, Elsik M, Krum H. Mortality and target haemoglobin concentrations in anaemic patients with chronic kidney disease treated with erythropoietin: a meta-analysis. Lancet Lond Engl. 2007;369(9559):381–8.
The Global Outcomes (KDIGO) Anemia Work Group. 2012 Kidney Disease: Improving Global Outcomes (KDIGO). KDIGO clinical practice guideline for anemia in chronic kidney disease. Kidney Int Suppl. 2012; 2: 279–335. 282.
Ishimura E, Nishizawa Y, Inaba M, Matsumoto N, Emoto M, Kawagishi T, et al. Serum levels of 1,25-dihydroxyvitamin D, 24,25-dihydroxyvitamin D, and 25-hydroxyvitamin D in nondialyzed patients with chronic renal failure. Kidney Int. 1999;55(3):1019–27.
Adeney KL, Siscovick DS, Ix JH, Seliger SL, Shlipak MG, Jenny NS, et al. Association of serum phosphate with vascular and valvular calcification in moderate CKD. J Am Soc Nephrol. 2009;20(2):381–7.
Gutiérrez OM, Januzzi JL, Isakova T, Laliberte K, Smith K, Collerone G, et al. Fibroblast growth factor 23 and left ventricular hypertrophy in chronic kidney disease. Circulation. 2009;119(19):2545–52.
Suki WN, Zabaneh R, Cangiano JL, Reed J, Fischer D, Garrett L, et al. Effects of sevelamer and calcium-based phosphate binders on mortality in hemodialysis patients. Kidney Int. 2007;72(9):1130–7.
Palmer SC, Gardner S, Tonelli M, Mavridis D, Johnson DW, Craig JC, French R, Ruospo M, Strippoli GF. Phosphate-binding agents in adults with CKD: a network meta-analysis of randomized trials. Am J Kidney Dis. 2016;68(5):691–702. https://doi.org/10.1053/j.ajkd.2016.05.015. Epub 2016 Jul 22.
Navaneethan SD, Palmer SC, Craig JC, Elder GJ, Strippoli GFM. Benefits and harms of phosphate binders in CKD: a systematic review of randomized controlled trials. Am J Kidney Dis Off J Natl Kidney Found. 2009;54(4):619–37.
Navaneethan SD, Palmer SC, Vecchio M, Craig JC, Elder GJ, Strippoli GF. Phosphate binders for preventing and treating bone disease in chronic kidney disease patients. Cochrane Database Syst Rev. 2011;(2):CD006023.
Tentori F, Hunt WC, Stidley CA, Rohrscheib MR, Bedrick EJ, Meyer KB, et al. Mortality risk among hemodialysis patients receiving different vitamin D analogs. Kidney Int. 2006;70(10):1858–65.
Kalantar-Zadeh K, Kuwae N, Regidor DL, Kovesdy CP, Kilpatrick RD, Shinaberger CS, et al. Survival predictability of time-varying indicators of bone disease in maintenance hemodialysis patients. Kidney Int. 2006;70(4):771–80.
Wetmore JB, Gurevich K, Sprague S, Da Roza G, Buerkert J, Reiner M, et al. A randomized trial of Cinacalcet versus vitamin D analogs as Monotherapy in secondary hyperparathyroidism (PARADIGM). Clin J Am Soc Nephrol. 2015;10(6):1031–40.
Trial Investigators EVOLVE, Chertow GM, Block GA, Correa-Rotter R, Drüeke TB, Floege J, et al. Effect of cinacalcet on cardiovascular disease in patients undergoing dialysis. N Engl J Med. 2012;367(26):2482–94.
Palmer SC, Teixeira-Pinto A, Saglimbene V, Craig JC, Macaskill P, Tonelli M, et al. Association of Drug Effects on serum parathyroid hormone, phosphorus, and calcium levels with mortality in CKD: a meta-analysis. Am J Kidney Dis Off J Natl Kidney Found. 2015;66(6):962–71.
Kidney Disease: Improving Global Outcomes (KDIGO). KDIGO clinical practice guideline for the diagnosis, evaluation, and treatment of CKD–Mineral and Bone Disorder (CKD-MBD). Kidney Int Suppl. 2009;76(Supplement 113):Sv–S121.
Kraut JA, Madias NE. Metabolic acidosis of CKD: an update. Am J Kidney Dis Off J Natl Kidney Found. 2016;67(2):307–17.
Locatelli F, Alberti D, Graziani G, Buccianti G, Redaelli B, Giangrande A. Prospective, randomised, multicentre trial of effect of protein restriction on progression of chronic renal insufficiency. Northern Italian cooperative study group. Lancet Lond Engl. 1991;337(8753):1299–304.
Klahr S, Levey AS, Beck GJ, Caggiula AW, Hunsicker L, Kusek JW, et al. The effects of dietary protein restriction and blood-pressure control on the progression of chronic renal disease. Modification of diet in renal disease study group. N Engl J Med. 1994;330(13):877–84.
Mitch WE, Remuzzi G. Diets for patients with chronic kidney disease, still worth prescribing. J Am Soc Nephrol. 2004;15(1):234–7.
Remuzzi G, Bertani T. Pathophysiology of progressive nephropathies. N Engl J Med. 1998;339(20):1448–56.
Remuzzi G, Ruggenenti P, Perico N. Chronic renal diseases: renoprotective benefits of renin-angiotensin system inhibition. Ann Intern Med. 2002;136(8):604–15.
Slavin JL. Position of the American dietetic association: health implications of dietary fiber. J Am Diet Assoc. 2008;108(10):1716–31.
Ramezani A, Raj DS. The gut microbiome, kidney disease, and targeted interventions. J Am Soc Nephrol. 2014;25(4):657–70.
Lau WL, Kalantar-Zadeh K, Vaziri ND. The gut as a source of inflammation in chronic kidney disease. Nephron. 2015;130(2):92–8.
Kasiske BL, Lakatua JD, Ma JZ, Louis TA. A meta-analysis of the effects of dietary protein restriction on the rate of decline in renal function. Am J Kidney Dis Off J Natl Kidney Found. 1998;31(6):954–61.
Friedman AN, Yu Z, Juliar BE, Nguyen JT, Strother M, Quinney SK, et al. Independent influence of dietary protein on markers of kidney function and disease in obesity. Kidney Int. 2010;78(7):693–7.
Xu H, Huang X, Risérus U, Krishnamurthy VM, Cederholm T, Arnlöv J, et al. Dietary fiber, kidney function, inflammation, and mortality risk. Clin J Am Soc Nephrol. 2014;9(12):2104–10.
Chiu Y-W, Teitelbaum I, Misra M, de Leon EM, Adzize T, Mehrotra R. Pill burden, adherence, hyperphosphatemia, and quality of life in maintenance dialysis patients. Clin J Am Soc Nephrol. 2009;4(6):1089–96.
Ginsberg JS, Zhan M, Diamantidis CJ, Woods C, Chen J, Fink JC. Patient-reported and actionable safety events in CKD. J Am Soc Nephrol. 2014;25(7):1564–73.
Newmaster SG, Grguric M, Shanmughanandhan D, Ramalingam S, Ragupathy S. DNA barcoding detects contamination and substitution in north American herbal products. BMC Med. 2013;11:222.
Herbal Supplements and Kidney Disease [Internet]. The National Kidney Foundation. 2015 [cited 2016 Oct 2]. Available from: https://www.kidney.org/atoz/content/herbalsupp.
Buettner M, Toennes SW, Buettner S, Bickel M, Allwinn R, Geiger H, et al. Nephropathy in illicit drug abusers: a postmortem analysis. Am J Kidney Dis Off J Natl Kidney Found. 2014;63(6):945–53.
Pun PH, Al-Khatib SM, Han JY, Edwards R, Bardy GH, Bigger JT, et al. Implantable cardioverter-defibrillators for primary prevention of sudden cardiac death in CKD: a meta-analysis of patient-level data from 3 randomized trials. Am J Kidney Dis Off J Natl Kidney Found. 2014;64(1):32–9.
Wang ZJ, Harjai KJ, Shenoy C, Gao F, Shi DM, Liu YY, et al. Drug-eluting stents versus bare-metal stents in patients with decreased GFR: a meta-analysis. Am J Kidney Dis Off J Natl Kidney Found. 2013;62(4):711–21.
Tomai F, Ribichini F, De Luca L, Petrolini A, Ghini AS, Weltert L, et al. Randomized comparison of Xience V and multi-link vision coronary stents in the same multivessel patient with chronic kidney disease (RENAL-DES) study. Circulation. 2014;129(10):1104–12.
Odutayo A, Wong CX, Hsiao AJ, Hopewell S, Altman DG, Emdin CA. Atrial fibrillation and risks of cardiovascular disease, renal disease, and death: systematic review and meta-analysis. BMJ. 2016;354:i4482.
Dahal K, Kunwar S, Rijal J, Schulman P, Lee J. Stroke, major bleeding, and mortality outcomes in warfarin users with atrial fibrillation and chronic kidney disease: a meta-analysis of observational studies. Chest. 2016;149(4):951–9.
Bonde AN, Lip GYH, Kamper A-L, Hansen PR, Lamberts M, Hommel K, et al. Net clinical benefit of antithrombotic therapy in patients with atrial fibrillation and chronic kidney disease: a nationwide observational cohort study. J Am Coll Cardiol. 2014;64(23):2471–82.
Carrero JJ, Evans M, Szummer K, Spaak J, Lindhagen L, Edfors R, et al. Warfarin, kidney dysfunction, and outcomes following acute myocardial infarction in patients with atrial fibrillation. JAMA. 2014;311(9):919–28.
WRITING COMMITTEE MEMBERS, Yancy CW, Jessup M, Bozkurt B, Butler J, Casey DE, et al. 2013 ACCF/AHA guideline for the management of heart failure: a report of the American College of Cardiology Foundation/American Heart Association task force on practice guidelines. Circulation. 2013;128(16):e240–327.
van Veldhuisen DJ, Ruilope LM, Maisel AS, Damman K. Biomarkers of renal injury and function: diagnostic, prognostic and therapeutic implications in heart failure. Eur Heart J. 2016;37(33):2577–85.
National Kidney Foundation Task Force on Cardiovascular Disease. Controlling the epidemic of cardiovascular disease in chronic renal disease. Am J Kidney Dis. 1998;32(Suppl 3):S115.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2019 Springer Nature Switzerland AG
About this chapter

Cite this chapter
Lakkis, J.I., Weir, M. (2019). Chronic Kidney Disease in the Primary Care Setting: Cardiovascular Disease Risk and Management. In: Toth, P., Cannon, C. (eds) Comprehensive Cardiovascular Medicine in the Primary Care Setting. Contemporary Cardiology. Humana Press, Cham. https://doi.org/10.1007/978-3-319-97622-8_8
Download citation
DOI: https://doi.org/10.1007/978-3-319-97622-8_8
Published:
Publisher Name: Humana Press, Cham
Print ISBN: 978-3-319-97621-1
Online ISBN: 978-3-319-97622-8
eBook Packages: MedicineMedicine (R0)