
Abstract
Epileptic seizures are caused by an electrical disturbance of brain activity that results in abnormal and excessive synchronization of neurons. Adenosine is a long-known anticonvulsant endogenous substance, exerting its actions through diverse mechanisms of action at different cellular targets. In this review we discuss the main actions of adenosine during acute and chronic phases of epileptic seizure progression and the mechanisms involved. There should be considered three main levels of adenosine actions: (1) neuronal level, where adenosine, mostly through its receptors A1, A2A and A3, alters intrinsic neuronal properties and excitatory/inhibitory network balance; (2) non-neuronal level, by affecting astrocytic function; and (3) homeostatic control level, through epigenetic regulatory mechanisms. Together, these actions make adenosine as a sort of “universal modulator or maestro” of desynchronization of epileptic focus, with great therapeutic potential in the treatment of resistant forms of epileptic seizures. Indeed, adenosine augmentation therapies are being considered to tackle epilepsy, which include gene therapy strategies and dietary interventions. Further research on new drugs that specifically target the mechanisms of actions involved in the pathological process of the disease are needed to take full advantage of adenosine anticonvulsant actions in the control of epileptic seizures.
Access provided by CONRICYT-eBooks. Download chapter PDF
Similar content being viewed by others

Keywords
- Epilepsy
- Seizure models
- Neuroprotection
- Adenosine-control mechanisms
- Adenosine-based therapies
- GABAergic transmission.
13.1 Introduction
This chapter aims to provide an overview on how adenosine, through its receptors, acts as an anticonvulsant substance to control seizure activity. We will focus our attention on the main modulatory targets of adenosine which include the control of intrinsic neuronal properties, excitatory and inhibitory network balance and the homeostatic and epigenetic regulation. The mechanisms involved in these actions will be addressed, and its impact on in vitro and in vivo models of epilepsy will be analysed. Lastly, we will highlight the most recent and innovative adenosine-based strategies developed for therapeutic intervention in the control of epileptic seizures.
13.2 Epilepsy and Epileptic Seizures
Epilepsy is a brain disease with an heterogenous prevalence among different countries but estimated to be of around 1% worldwide (Sander and Shorvon 1996; Beghi and Hesdorffer 2014; Bell et al. 2014). The disease is predominantly characterized by the recurrent and unpredictable interruption of normal brain function by epileptic seizures, and it comprises all the neurobiological, cognitive, psychological and social consequences that this condition may have on people’s lives (Fisher et al. 2005). For practical and clinical purposes, it was recently included in the definition of epilepsy the requirement of having at least two epileptic seizures occurring >24h apart or one epileptic seizure and a very high risk of recurrence over the next 10 years (Fisher et al. 2014). This definition, elaborated by the International League Against Epilepsy (ILAE), points out two important aspects that should be emphasized: first, that epilepsy exists when recurrent epileptic seizures occur, but epileptic seizures may occur without implying the diagnose of epilepsy; second, that epilepsy is not only characterized by its clinical neurological manifestations but also by all the repercussions that the disease may have on the patient and its family (including social implication).
Adenosine has been coined as a putative endogenous anticonvulsant a long time ago (Dunwiddie 1980; Dragunow et al. 1985). Since then, there was a great increase in our knowledge of the mechanisms of action of adenosine receptors that mediate its action and metabolic pathways involved in the homeostatic control of its intra- and extracellular concentration. The understanding of seizures also increased. In this chapter we will mostly focus our attention on adenosine actions that are related with seizure events. These include adenosine action on the mechanism underlying epileptic seizures per se, on the sequence of events that convert a normal neuronal network into a hyperexcitable network (epileptogenesis) and on the control of seizure activity in in vitro and in vivo experimental models of epilepsy. Although some of the epilepsy-associated comorbidities will be briefly addressed, we will leave all the other elements that define this disease out of our discussion.
It is important also to clarify the definition of epileptic seizures (or simply referred as seizures), which are described as a transient occurrence of signs and/or symptoms due to abnormal excessive or synchronous neuronal activity in the brain (Fisher et al. 2005). Clinically, when an epileptic seizure is identified, it is crucial that the clinician classifies the seizure according to its type and aetiology. This is helpful not only for diagnostic purposes but also for the use and development of antiepileptic therapies, investigation of seizure mechanisms and facilitation of worldwide communication among pairs. Seizures are thus classified according to its type in (1) focal, when originated within a network limited to one hemisphere; (2) generalized, when originated in bilaterally distributed networks; or (3) unclassified, when the local of onset is unknown (Berg and Millichap 2013). Each category can be further classified according to the level of awareness (retained awareness seizure or impaired awareness seizure), motor behaviour (atonic, tonic, clonic, myoclonic, epileptic spasms or a combination of these) and nonmotor behaviour (e.g. absence seizures) (Fisher et al. 2017). A focal seizure can eventually generalize, being classified as focal to bilateral tonic-clonic seizure (Fisher et al. 2017).
The etiologic classification recognizes six groups that have also implications for treatment. These include structural, genetic, infectious, immune, metabolic or unknown aetiology (Scheffer et al. 2017). A structural aetiology implies the presence of neuroimaging abnormalities as the most likely cause of seizure. Such changes may be acquired by stroke, trauma or even infection or developmental malformations. Genetic aetiology is when the epileptic seizures directly result from a known or presumed genetic disorder. Infection is one of the most common aetiologies of epileptic seizures worldwide (Vezzani et al. 2016) and includes viral, bacterial, fungal and parasitic infections of the central nervous system that result in seizures. An immune-mediated seizure is mostly associated with auto-immune diseases affecting the central nervous system (such as anti-NMDA receptor encephalitis) and deserves an isolated category given its specific treatment implications (Lancaster and Dalmau 2012). Metabolic causes refer to well-stablished metabolic defects where seizures are the core symptom (examples include porphyria or pyridoxine-dependent seizure). Unknown cause is defined when the aetiology is not possible to stablish. Unknown aetiology accounts for about one-third of all seizures worldwide, but this number varies depending on the healthcare provider and country (Banerjee et al. 2009). In this classification, of course, the categories are not hierarchical nor mutually exclusive, and a seizure event can have more than one aetiology (e.g. tuberous sclerosis complex, which results from mutations in genes TSC1 and TSC2 causing central nervous system tumours, is considered to have a genetic and a structural cause).
Given the diversity of types and aetiologies of seizures, we cannot consider only one form of epilepsy but rather a group of epilepsy syndromes, each of which characterized by the occurrence of specific seizure properties. Such differences need to be considered when planning and carrying experimental research on epilepsy, namely, in the devise of animal models in vitro and in vivo. These models serve a variety of purposes that include the screening of new antiepileptic compounds for their anticonvulsant or antiepileptogenic properties (in acute or chronic models of epilepsy), their efficacy against different types of epilepsy and the study of the mechanisms involved in drug resistance in epilepsy or associated comorbid features, such as cognitive and psychiatric comorbidities (Löscher 2011). Animal models are usually grouped in “acute seizure models” and “chronic epilepsy models”. The term “acute” refers to models in which seizures are induced by electrical or chemical stimulation in otherwise naïve and healthy (non-epileptic) animals; the term “chronic” is used to refer to models in which animals have been made epileptic by electrical, chemical or genetic means (Löscher 2011) (Table 13.1). Other mechanisms can be used to induce acute or chronic seizures, depending on the epilepsy aetiology to be studied (e.g. traumatic brain injury, hyperthermia, hypoxia, systemic/focal infection, among others).
The in vitro seizure models include neuronal cultures, brain slice cultures (organotypic) or acute slice models (Raimondo et al. 2017). These are particularly important for the study of basic physiology, pharmacology and molecular biology of seizures and epileptogenesis. Acute slices can be obtained from “normal” animals, in which in vitro manipulations are used to generate epileptiform activity or obtained from chronically epileptic animals or even human patients. To induce epileptiform activity in otherwise naïve slices, many different strategies can be used depending on what type of seizure activity is intended to be measured. These include high-frequency electrical stimulation, GABAergic inhibition, glutamatergic (kainic acid) or muscarinic (pilocarpine) activation, potassium channel blockers (4-aminopyridine), low extracellular calcium, low extracellular magnesium or high extracellular potassium models (Ivanov and Bernard 2017).
A plethora of >20 antiepileptic drugs (AEDs) are currently available to use in clinical practice. In fact, up to 70% of newly diagnosed people with epilepsy can be successfully treated with the drugs currently available (Kwan and Brodie 2001). The mechanism of action of most drugs reflects what we know about the underlying abnormalities occurring in seizure generation and propagation. These include targeting hyper-excitation or hypo-inhibition by preventing activation of depolarizing sodium or calcium channels, enhancing the inactivation of sodium channels, facilitating hyperpolarizing potassium channels or affecting neurotransmission by blocking glutamate-mediated actions or promoting GABA-induced inhibition (Bialer and White 2010; Rogawski et al. 2016) (Fig. 13.1). Nonetheless, one-third of patients with epilepsy cannot be controlled with these tools (Granata et al. 2009). Resistance to pharmacotherapy may be already present when the treatment is initiated, as occurs in some infant seizure syndromes (e.g. include Ohtahara syndrome, Dravet syndrome and others), or it may evolve during the course of chronic epilepsy or status epilepticus, after a positive initial response to the drug (Heinemann et al. 2006). When medication fails to control seizures, other options are considered and may include neurosurgical treatment (Engel 1996a), vagus nerve stimulation (Uthman 2000) or dietary therapy (e.g. ketogenic diet) (Bough and Rho 2007). Apart from surgery, where the rational is to isolate or resect the epileptogenic tissue (i.e., the focus of the disease), vagus nerve stimulation and ketogenic diet are alternative neuromodulatory approaches aimed to influence several neuronal targets simultaneously and achieve a greater control of the disease. Identical reasoning can be applied to the use of adenosine-based strategies in the control of seizures and epilepsy. In fact, most of the targets of AEDs mentioned above are, indeed, also targets of adenosine modulation (Sebastião and Ribeiro 2009). Ketogenic diet also involves adenosine-dependent mechanism (Masino and Geiger 2008). Thus, it is not surprising that, apart from all difficulties with the implementation of adenosine in clinical practice (mostly due to the well-known peripheral side effects), adenosine is still highly and enthusiastically studied as an important and promising approach to fight drug-resistant epilepsies.

Mechanisms of action of antiepileptic drugs at inhibitory and excitatory synapses and astrocytes. The targets include block activation of sodium channels (phenytoin, carbamazepine, oxcarbazepine, eslicarbazepine acetate, lamotrigine, topiramate, rufinamide, felbamate, zonisamide, valproate) or enhance inactivation of sodium channels (lacosamide, rufinamide), block calcium channels (gabapentin, pregabalin, lamotrigine, ethosuximide, valproate) and open potassium channels (retigabine); enhance GABAAR actions (benzodiazepines, felbamate, valproate, topiramate, zonisamide, barbiturates) or extrasynaptic GABAARs (stiripentol); increase GABA turnover by increasing its synthesis – via GAD – and/or release (valproate), inhibiting GABA reuptake through GABA transporters type 1 (GAT1) (tiagabine) or inhibiting GABA transaminase (GABA-T) (vigabatrin); block AMPA and kainate receptors (topiramate, perampanel) or NMDA receptors (felbamate); and inhibit synaptic vesicle glycoprotein 2 (SV2A) (levetiracetam)
13.3 Grounds for Anticonvulsant Actions of Adenosine
Since Phillis’ first observations that adenosine has a depressive action in the central nervous system (Phillis et al. 1974), many studies have followed showing that adenosine is capable of influencing not only neuronal firing (Kostopoulos et al. 1975; Phillis and Kostopoulos 1975) but also to directly alter excitatory synaptic responses (Kuroda and Kobayashi 1975; Scholfield 1978; Schubert and Mitzdorf 1979; Dunwiddie and Hoffer 1980). The first evidence relating adenosine and epileptic seizures came from studies showing that right after seizure initiation there was a rapid and dramatic increase in adenosine levels (Pull and McIlwain 1972; Schultz and Lowenstein 1978; Schrader et al. 1980; Winn et al. 1980). Later, adenosine was shown to act as an endogenous anticonvulsant in vitro, in a rat hippocampal preparation of epileptiform discharges (Dunwiddie 1980), and also in vivo, in a rat drug-induced seizure model (Dunwiddie and Worth 1982). These and other findings (Albertson et al. 1983; Barraco et al. 1984; Dragunow et al. 1985; Chin 1989) paved the way for comprehensive studies about the use of adenosine and adenosine-related compounds as putative therapeutic strategies in epilepsy. Today, it is largely accepted that adenosine indeed has a role as an anticonvulsant substance. There are, however, several aspects that should be considered when discussing the influence of adenosine on seizures and epilepsy.
First is that the capacity of adenosine to shape neuronal excitability and arrest seizures depends on the stage of disease progress. This is of particular interest since the adenosinergic system not only influences neuronal excitability during a seizure event but is also dramatically affected by the epileptogenic process per se. This means that adenosine-mediated actions may vary depending on whether they are directed to neuronal circuits that are experiencing a seizure event for the first time (i.e. acute seizures) or circuits suffering from neurobiological modifications after a first neuronal insult (that may also affect the adenosinergic system) as occurs during epileptogenesis and stablished epilepsy (i.e. chronic seizures). This has also important clinical and therapeutic implications. Acute actions of endogenous adenosine in an inaugural seizure event may have significant neuroprotective value but little application for clinical intervention. On the other hand, subsequent adaptive changes that contribute to the development of recurrent seizure events and the establishment of epilepsy, as well as the emergence of resistance to classical EADs, may potentially benefit from adenosine-based therapies.
Another aspect to consider is the targets of adenosine actions. Indeed, adenosine is known to affect excitability far beyond its synaptic effects (Cunha 2001). Thus, in a tentative dissection of the mechanism by which adenosine exerts its anticonvulsant actions, it is relevant to separate the actions occurring at the (1) neuronal level, which include changes in neuronal excitability and synaptic transmission; (2) non-neuronal level, mostly related to regulation of glial function; and (3) homeostatic control level, corresponding to variations in adenosine metabolism and epigenetic control . Nevertheless, all mechanisms are mutually dependent and operate together to generate an orchestrated action to influence network activity and seizures. It is noteworthy to mention that this chapter does not intend exhaustively describe all mechanisms by which adenosine exerts its actions upon excitability. We will only focus on studies where there is direct evidence for the interference of adenosine or adenosine receptors on seizure activity.
13.4 Adenosine as a Seizure Control Substance
13.4.1 A1Rs in Acute Models of Seizure
As mentioned above, the capacity of adenosine to control seizure events has been proposed a long time ago (Dunwiddie 1980; Dunwiddie and Worth 1982). Studies that followed have confirmed and broaden the actions of adenosine on many different seizure models in vitro and in vivo . We should start by looking to adenosine action on acute seizure models of epilepsy. As first observed by Dunwiddie and Worth, adenosine actions in these models are mostly associated with A1 receptors (A1Rs) (Dunwiddie and Worth 1982). When adenosine analogues or selective A1R agonists were systemically injected in electrical- or chemical-induced seizure models, an anticonvulsant action and arrest of epileptic seizures were observed (Dragunow and Goddard 1984; Turski et al. 1985; Morrisett et al. 1987; Whitcomb et al. 1990; Von Lubitz et al. 1993; Young and Dragunow 1994; Adami et al. 1995; Pourgholami et al. 1997a; Malhotra and Gupta 1997; Sarro et al. 1999; Zgodziński et al. 2001; Huber et al. 2002; Girardi et al. 2007; Li et al. 2013). These actions were observed also in immature animals, suggesting that the A1R-mediated anticonvulsant effects also occur early in the developing brain (Mareš 2010; Pometlová et al. 2010). Repeated activation of A1Rs, however, tends to develop tolerance and a gradual loss of their anticonvulsant capacities (Adami et al. 1995). Importantly, there is an endogenous role of adenosine in the suppression of seizures since blocking A1R activation aggravates epileptic activity (Dragunow and Goddard 1984; Dragunow and Robertson 1987; Morrisett et al. 1987; Whitcomb et al. 1990; Zhang et al. 1993; Von Lubitz et al. 1993; Fukuda et al. 2010) and converts recurrent seizure patterns into status epilepticus (Young and Dragunow 1994). Significant seizure suppression can also be achieved by increasing adenosine levels through inhibitors of adenosine kinase, adenosine deaminase or adenosine transporters blockers (Eldridge et al. 1989; Zhang et al. 1993). Together, these studies highlight three main aspects: first, that adenosine is not only capable of preventing seizure occurrence when administered before the trigger insult but also stop an already stablished seizure event (working as a true anticonvulsant substance); second, adenosine-mediated endogenous mechanisms are crucial to restrain ongoing seizure events, but further anticonvulsant effect is still possible through exogenous activation of A1R; and, finally, adenosine actions occur in different acute models of epileptic seizures, regardless the mechanism of induction is electrical stimulation (Dragunow and Robertson 1987; Whitcomb et al. 1990; Young and Dragunow 1994; Pometlová et al. 2010) or by manipulation of GABAergic system (Zhang et al. 1993; Adami et al. 1995; Malhotra and Gupta 1997; Girardi et al. 2007; Mareš 2010; Li et al. 2013), of the glutamatergic system (Von Lubitz et al. 1993; Li et al. 2013), or by other chemical manipulation (Turski et al. 1985; Eldridge et al. 1989; Li et al. 2013).
All mentioned studies have in common the control by A1R via intraperitoneal injections of selective drugs. However, their low permeability through the blood-brain barrier (Brodie et al. 1987) and peripheral actions, mostly related to cardiovascular side effects (Stella et al. 1993; Schindler et al. 2005), has hampered the use of A1R agonists for the treatment of central nervous system (CNS) diseases. To minimize these effects and potentiate adenosine actions in the brain, other approaches include intracranial activation of A1R in specific brain regions known to be responsible for the epileptic seizure initiation and/or spreading. In fact, intracranial perfusion of A1R agonists conferred protection against 3-nitropropionic acid (a mitochondrial toxin) (Zuchora et al. 2001), bicuculline-induced (Franklin et al. 1989) and pilocarpine-induced seizures through changes in glutamate, GABA and dopamine levels at the epileptic focus (Khan et al. 2000, 2001). An alternative, non-invasive possibility is the development of tissue selective adenosine receptor agonists. An A1R agonist with anticonvulsant activity without causing motor behaviour alterations usually occurring as a consequence of sedation and bradycardia has been identified (Tosh et al. 2012), but the mechanisms subserving such tissue selectivity remain to be identified.
13.4.2 A1Rs in Chronic Models of Epilepsy
Regarding actions of A1Rs in chronic models of epilepsy, they are described for the kindling model of limbic seizure propagation, which mostly involves connections between piriform cortex, amygdala, hippocampus and entorhinal cortex (Lopes da Silva et al. 1990). The kindling model is one of the most commonly used chronic models of epilepsy, particularly for the study of temporal lobe (limbic) epilepsy (TLE) (Goddard 1967; Goddard et al. 1969). In kindling animals, seizures initiate and are confined to the focal area of stimulation and progressively propagate through other brain structures that serve as pathways for generalization of subsequent seizures (Sato et al. 1990). Thus, seizure progression may be hypothetically interrupted not only in the original focus of the seizure but also in parts of the brain, other than the epileptic focus, that are responsible for its propagation. This is, indeed, what happens with adenosinergic control of limbic seizures. Intra-hippocampal and intra-amygdala injections of A1R agonists have, as expected, inhibitory actions on hippocampal- and amygdala-kindling parameters, respectively (Rosen and Berman 1987; Pourgholami et al. 1997b). Importantly, however, activation of A1Rs in the hippocampus (Pourgholami et al. 1997a; Alasvand Zarasvand et al. 2001), entorhinal cortex (Mohammad-Zadeh et al. 2005), piriform cortex (Rezvani et al. 2007a, b) or perirhinal cortex (Mirnajafi-Zadeh et al. 1999) reduced seizure duration and afterdischarges specifically in amygdala. These effects are pathway dependent, since intra-amygdala A1R activity had no significant anticonvulsant action neither on hippocampal-kindled seizures (except for secondary afterdischarges) (Mirnajafi-Zadeh et al. 2000), entorhinal cortex-kindled seizures (Mohammad-Zadeh et al. 2005) nor piriform cortex-kindling animals (Shahabi et al. 2006), despite the influence of amygdala in its propagation (Sato et al. 1990). Hippocampal and entorhinal cortex A1Rs are also involved in supressing entorhinal cortex- and piriform cortex-kindling, respectively (Heidarianpour et al. 2006; Zeraati et al. 2006; Hosseinmardi et al. 2007). Importantly, blockade of A1R actions in these models aggravates seizure activity and generalization, pointing to an endogenous action of adenosine, through A1Rs, in restraining limbic epilepsy. Together, these results indicate that the anticonvulsant actions of A1Rs (1) are not only relevant in acute seizure control but also in chronic models of epilepsy, (2) are region and pathway specific and (3) are capable of restraining seizure exacerbation not only in the brain region where seizure emerges but also in the surrounding areas responsible for propagation and consequent generalization of seizures.
The translational potential of invasive approaches as intracranial injections of A1R agonists can only be envisaged for very serious disease conditions. Another potential approach for intracranial activation of A1Rs is to provide a local and sustained source of adenosine. This was first achieved by intraventricular implantation of an adenosine-releasing synthetic polymer, which led to a reduction of seizure activity in the rat kindling model of partial epilepsy (Boison et al. 1999). Also, ex vivo gene therapy approaches in kindled rats showed profound but transient reduction in seizure activity (Huber et al. 2001; Boison et al. 2002; Güttinger et al. 2005a). Long-term anticonvulsive effects were obtained with local release of adenosine through encapsulated myoblasts implanted in the vicinity of the epileptic focus (Güttinger et al. 2005b). Protection from convulsive seizures lasted for 3 to 8 weeks and caused no desensitization of A1Rs and no side effects as sedation or changes in locomotor behaviour (Güttinger et al. 2005b).
The capacity of adenosine to keep the epileptic focus localized was also demonstrated in a status epilepticus model using A1R-knock out (A1R-KO) mice (Fedele et al. 2006). In fact, A1R-KO animals submitted to unilateral intra-hippocampal kainic acid injections not only showed severe convulsions and increased mortality when compared to control animals but also displayed greater extend of neuronal loss both in the ipsi- and contralateral hippocampus. Similar results were obtained with A1R-KO mice subjected to traumatic brain injury-induced seizures (Kochanek et al. 2006).
Despite the neuroprotective and anticonvulsant actions of adenosine A1Rs in acute and chronic stages of epilepsy, adenosine release and A1R (but also A2AR) activation during seizures have been associated with sudden unexpected death in epilepsy (SUDEP) (Shen et al. 2010; Faingold et al. 2016). Postictal hypoventilation is considered as a major contributor to the cause of death in SUDEP, particularly during the sleeping period (Massey et al. 2014; Richerson et al. 2016). Thus, given the known depressant actions of adenosine on brainstem respiratory network (Vandam et al. 2008; Zwicker et al. 2011) and its sedative effects (Porkka-Heiskanen et al. 1997), seizure-induced elevation of adenosine levels may further contribute to respiratory distress associated with SUDEP. Importantly, caffeine treatment after seizure onset might be beneficial (Shen et al. 2010).
Altogether, data from chronic models of epilepsy reveal that even after the establishment of recurrent seizure events, and besides all the consequent neuronal adaptations that may occur in neuronal circuitry, adenosine A1Rs are still able to restrain and cease further progression of the disease in a tentative action to re-establish normal network communication. Risk of SUDEP may however be increased.
13.4.3 Adenosine A2ARs and A3Rs in Seizure Control
Although the major interest about adenosine control of epileptic activity has been the inhibitory A1R system, an increasing number of studies are now focusing on facilitatory adenosine A2A receptors (A2ARs).
The majority of results point to a pro-excitatory role of A2ARs, although some data is still conflicting. Some studies have shown that A2R or A2ARs are not involved in convulsions (Rosen and Berman 1987; Janusz and Berman 1992; Young and Dragunow 1994; Malhotra and Gupta 1997; Uzbay et al. 2007; Rezvani et al. 2007a; Akula and Kulkarni 2014). Surprisingly, studies using acute models of chemical-induced seizures and audiogenic-susceptible seizures show that activation of A2R or even A2ARs agonists contribute to seizure suppression (Adami et al. 1995; Jones et al. 1998a, b; Sarro et al. 1999; Boison et al. 2002) and that its blockade has proconvulsant actions (Vianna et al. 2005). In a kindling model of chronic epilepsy, the effects of NECA (an agonist with slightly more potency to A2R than A1R) was compared with that of a prototype A1R agonist, and data obtained allowed to suggest an A2R-mediated seizure suppression in the caudate nucleus (Rosen and Berman 1987), but not in the amygdala (Janusz and Berman 1992). Focal injection of CGS21680 (an adenosine A2AR agonist) leads to a reduction in the severity of bicuculline-induced seizures, but these actions were attributed to A1Rs (Zhang et al. 1994), which highlights the need of careful pharmacological controls before concluding on the action of adenosine receptors, in particular of those expressed at low levels in relevant brain areas, in seizures.
Apart from these initial studies, some of them performed before development of selective adenosine receptor ligands, more recent studies have consistently been showing proconvulsive effects of A2ARs in chronic models of amygdala (Li et al. 2012b) and piriform cortex (Zeraati et al. 2006; Hosseinmardi et al. 2007) kindling. Genetic ablation of A2ARs confirms these proconvulsant actions since A2AR-KO animals show attenuated intensity of pentylenetetrazol-induced (El Yacoubi et al. 2008) or ethanol withdrawal-induced (El Yacoubi et al. 2001) seizures. Protection is not only evident during the acute convulsive period but also in preventing proconvulsive epileptogenic changes during evolution of kindling (El Yacoubi et al. 2009). An A2AR antagonist was also shown to reduce synchronous pyramidal cell firing in acute hippocampal slices under hyperexcitable conditions (Rombo et al. 2015).
In a genetic model of absence epilepsy (WAG/Rij), in vivo A2AR activation increases spontaneous discharges and aggravates epileptiform activity of hippocampal slices recorded 1–5 h post-injections (D’Alimonte et al. 2009). It was recently shown that a genetic variation in human adenosine A2AR gene (ADORA2A) associated with increased expression of A2AR and higher levels of cAMP production is a predisposing factor for childhood encephalopathy following severe febrile seizures (Shinohara et al. 2013), a finding that also favours the idea of a proconvulsant action of A2ARs.
Progressive development of stress-induced seizures and deficits in learning and memory have been reported to occur in mice with genetic deletion of adenosine kinase (ADK-KO) in the brain (Sandau et al. 2016). This somehow mimics a rare disease in humans, ADK deficiency, which have psychomotor delay and convulsive seizures commencing between the first and third year of life (Bjursell et al. 2011). Intracellular ADK is known to regulate extracellular levels of adenosine, with low ADK activity being associated with protection against seizures (Gouder 2004). Thus, the finding that ADK-KO leads to progressive seizure development was unexpected. A study designed to find out possible mechanisms underlying these findings allowed to conclude that chronically enhanced levels of extracellular adenosine, caused by absence of adenosine kinase in the forebrain, favour A2AR activity, which thus enhances the action of brain-derived neurotrophic factor (BDNF) upon synaptic plasticity (Sandau et al. 2016), which most probably leads to maladaptative circuitry formation. Indeed, blocking A2AR activity in ADK-KO mice, as well as blocking BDNF receptors, attenuated seizure risk and restored cognitive performance. Interestingly, A1R blockade exacerbates seizure phenotype in this mice model, thus indicating that extracellular adenosine, through A1R, maintains its anticonvulsant activity (Sandau et al. 2016). This study, together with other studies showing the proconvulsant action of A2AR, highlights the need to attenuate the overactivation of A2AR while testing the action of adenosine augmentation therapies against pharmacoresistant forms of epilepsy.
In conclusion, the presently available evidence points towards a proconvulsant action of A2AR. Some discrepancies that have been reported may be ascribed to several reasons including pharmacological tools to identify the receptors, the mode of administration and concentrations used (receptor selectivity vs access of drugs to the epileptic tissue), differences in the seizure model used (that underlie different mechanisms of seizure induction) and the brain region and the neuronal circuits involved in seizure initiation and propagation (brain region and pathway specificity of A2AR actions). Maladaptive changes of A2ARs levels in acute and chronic models of epilepsy may also explain part of the inconsistencies (see Chapter 13.5 below).
Regarding A3Rs , much less information is known, and again, some discrepancies are reported. In an audiogenic seizure model of epilepsy, A3Rs were ineffective in controlling seizures (Sarro et al. 1999). However, the A3R-selective agonists , Cl-IB-MECA, were reported to facilitate epileptiform discharges in the CA3 area of the immature hippocampus (Laudadio and Psarropoulou 2004), whereas A3R antagonists increased the GABAergic current stability in different epileptic tissues (Roseti et al. 2008), in line with the possibility of a proconvulsant action of A3Rs. In contrast, in acute chemical-induced seizure models, activation of A3R seemed to be anticonvulsant (Von Lubitz et al. 1995a), and its blockade was proconvulsant (Vianna et al. 2005). In an electroshock seizure model, A3Rs raised the threshold for electro-convulsions and reduced the severity of seizures, in line with the idea of the anticonvulsant actions of this receptor (Borowicz et al. 2004). The relatively low affinity of adenosine to A3R (Von Lubitz et al. 1994a; Dunwiddie et al. 1997) makes their activation possible only when relatively high concentrations of extracellular adenosine are reached, as occurs during high-frequency neuronal discharge. Furthermore, the expression of A3R is much more restricted to some tissues and brain areas than that of A1R. These two characteristics of A3R can turn into an advantage and raise the interest to develop A3R-selective ligands, which may have less side effects than A1R agonists to control pharmacoresistant seizures. However, it becomes clear that further steps in this direction require further studies to clarify the role of A3R in epilepsy.
Overall, it becomes evident that the actions of adenosine in acute and chronic phases of the epileptogenic process are valuable to hamper the progression of epileptic seizures. The long-known strategy of activating A1Rs as therapeutic approach to suppress seizures may profit from concomitant modulation of A2ARs and A3Rs to further promote the anticonvulsant effects of adenosine.
13.4.4 Adenosine and AEDs
Since the early findings that adenosine acts as an anticonvulsant substance, there is interest in the study of its interaction with conventional AED . In fact, there is evidence that some AEDs influence the purinergic transmission and that purine ligands affect AED actions. Early reports suggested that alterations in extracellular levels of adenosine or in the degree of activation of adenosine receptors may be an important component of the anticonvulsant actions of carbamazepine (Lewin and Bleck 1977; Skeritt et al. 1982). The interaction seems much stronger at A1Rs then A2ARs (Marangos et al. 1983; Skerritt et al. 1983; Weir et al. 1984; Dodd et al. 1986; Fujiwara et al. 1986). Prolonged treatment with carbamazepine, however, causes a marked upregulation of adenosine receptors in the brain (Marangos et al. 1985). Benzodiazepines such as diazepam and midazolam, as well as diphenylhydantoin, act as potent adenosine uptake inhibitors at therapeutic doses (Hammond et al. 1981; Phillis and Wu 1982; Phillis 1984; Bender and Hertz 1986; Narimatsu and Aoki 1999) causing an accumulation of extracellular endogenously released adenosine and potentiating their anticonvulsant actions (Kaplan et al. 1992; Narimatsu and Aoki 1999).
Conversely, adenosine receptor ligands also interfere with AED actions. Aminophylline and theophylline (non-selective A1R/A2AR antagonists) have been shown to diminish the efficacy of diazepam and valproate against electrical- and chemical-induced seizures (Czuczwar et al. 1985; Kulkarni et al. 1991; Malhotra et al. 1996; Zuchora et al. 2005), in line with the possibility that some of the anticonvulsant actions of those AEDs are due to enhanced extracellular adenosine levels. This may also apply to the sedative actions of benzodiazepines, since both aminophylline and theophylline showed to reverse the sedative effects of diazepam in postoperative animal models (Arvidsson et al. 1982; Niemand et al. 1984, 1986; Malhotra et al. 1996). Also, adenosine receptor activation potentiated the anticonvulsant actions of diazepam and valproate via A1Rs (Czuczwar et al. 1990) and phenobarbital, diphenylhydantoin, valproate and carbamazepine via both A1Rs and A3Rs (Borowicz et al. 1997, 2000, 2002) in electrical models of epilepsy. Together, these studies show a close interaction between AEDs and adenosine receptors in the control of seizures and highlight the potential concomitant use of conventional and adenosine-based strategies to potentiate their anticonvulsant actions.
13.5 Adenosine Control Mechanisms in Epileptic Seizures
Before discussing the specific mechanisms by which adenosine acts as an anticonvulsant and antiepileptogenic substance, a discussion about how the adenosinergic system per se is affected by acute and chronic seizures should be made (Table 13.2).
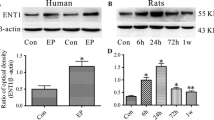
Anticonvulsant actions of adenosine result from a rapid increase in its extracellular concentration after seizures initiation, both in animal models (Schrader et al. 1980; Winn et al. 1980; Lewin and Bleck 1981; Berman et al. 2000; Kaku et al. 2001) and humans (During and Spencer 1992; Van Gompel et al. 2014). Adenosine levels increase 6- to 31-folds its basal levels, reaching ~2–3 μM concentration few seconds after the onset of epileptic activity (During and Spencer 1992) and remain high up to seizure termination (Van Gompel et al. 2014). Released adenosine is generated in the cytosol of spiking neurons as a consequence of metabolic exhaustion, reaching extracellular space directly through equilibrate nucleoside transporters (ENTs) (Lovatt et al. 2012). Extracellular levels are controlled by the activity of intracellular adenosine kinase (ADK) , an enzyme that in the hippocampus, from P14 onwards, is mostly expressed in astrocytes (Studer et al. 2006; Etherington et al. 2009; Kiese et al. 2016). During a seizure event induced by chemical agents, the density of A1R, or their G-protein coupling, increases after the first minutes to hours after the convulsion (Daval and Sarfati 1987; Angelatou et al. 1990, 1991; Daval and Werck 1991; Pagonopoulou et al. 1993; Psarropoulou et al. 1994; Vanore et al. 2001). An exception to this overall increase seems to be the striatum where no change or a slight decrease in A1R density was detected, as compared with other brain areas where the expected increase was found (Angelatou et al. 1990, 1991). In electrically evoked seizure models induced with single electroconvulsive shock, no changes were observed in expression of A1Rs (Newman et al. 1984; Gleiter et al. 1989). However, this may be related with the intensity of stimulus used to induce seizures, since stronger multi-shock stimulation does lead to an increase in A1R density (Gleiter et al. 1989). It is clear from this set of data that the first adaptation of the adenosinergic system after initiation of seizures is to restrain the abnormal convulsive activity and try to re-establish normal network function. This is mostly achieved by potentiating the neuroprotective actions of adenosine through increase of its extracellular levels and A1R expression.
On the other hand, long-term adaptations of adenosine and adenosine receptors to recurrent seizures differ from those observed in acute models (Table 13.2). When evaluating adenosine levels and adenosine receptor density in chronic models of seizures, several aspects can be pointed out: (1) the rising concentrations of adenosine during a recurrent convulsion in chronic models do not reach the same values as in an inaugural seizure event (Rebola et al. 2003); (2) outside the convulsive periods, the extracellular concentration of adenosine drops to levels lower then basal concentrations observed in non-epileptic tissue (Rebola et al. 2003); and (3) A1R density decreases progressively along the epileptogenesis process (Ekonomou et al. 1998, 2000) and remains low several weeks after the first convulsion (Ochiishi et al. 1999; Rebola et al. 2003, 2005). These observations are also supported by a loss of hippocampal A1Rs in patients suffering from temporal lobe epilepsy (Glass et al. 1996) and are in agreement with the requirement of higher doses of A1R agonists necessary to produce anticonvulsant effects along status epilepticus progression (Young and Dragunow 1994; Adami et al. 1995). However, part of the reduction in A1R density may be influenced by significant neuronal loss observed after recurrent seizures events (Engel 1996b). This may explain some of the contrasting results showing increased A1R protein and mRNA levels in chronic models of seizure (Adén et al. 2004; Tchekalarova et al. 2005; Hargus et al. 2012). Also, in tissue from human temporal lobe epilepsy (Angelatou et al. 1993) and human Rasmussen encephalitis (Luan et al. 2017), it was found an increase in the density of A1R. The exact reason for discrepancies compared to Glass observations (Glass et al. 1996) is unclear, but one possible explanation may be the differences in control tissue (biopsy vs autopsy of non-epileptic brain controls).
Regarding A2ARs, most studies report long-term changes in receptor protein levels . In opposite to A1Rs, A2ARs protein levels are increased several weeks after the establishment of epilepsy (Rebola et al. 2005). Upregulation of A2ARs does not only occur in neurons but also in glia (Saura et al. 2005; Orr et al. 2015). One study, though, describes a decrease in A2AR protein and mRNA levels using a kindled seizure model of epilepsy (Adén et al. 2004). Curiously, using a genetic model of absence epilepsy , where it is thus possible to evaluate receptor levels before and after seizures onset, it was shown that A2AR levels are only high after the first symptoms appear and not during the presymptomatic period, where A2AR density is even lower than in control animals (D’Alimonte et al. 2009). This increase may thus be a consequence, and not a direct cause, of recurrent seizure activity, although it may contribute to the progression and aggravation of convulsions. Alternatively, one may think that the increase in A2AR levels is itself a gate of the disease, coinciding with the very first event. Pharmacological treatment of these animals with an A2AR antagonist before disease onset would help to clarify this issue.
In parallel with changes in receptor levels, other long-term changes in the adenosinergic system also occur. These include decrease in ATP levels (Rebola et al. 2003) and suppression of recurrent epileptiform discharges through activation of A1Rs (Avsar and Empson 2004; Klaft et al. 2012; Muzzi et al. 2013); increase in ecto-5´-nucleotidase activity (Schoen et al. 1999; Lie et al. 1999; Rebola et al. 2003), the enzyme responsible for hydrolysing AMP into adenosine (Zimmermann et al. 2012); decrease in ecto-ATPase activity (Nagy et al. 1990; Bonan et al. 2000a, b); decrease in density and efficiency of equilibrative nucleoside transporter (ENT) (Pagonopoulou and Angelatou 1998; Rebola et al. 2003); and upregulation of ADK in rodents and human epileptic tissue (Aronica et al. 2011). Together, these long-term changes will contribute to low, but mostly ATP-derived, extracellular levels of adenosine that will lead to activation of A2ARs (Cunha et al. 1996) and contribute to propagation of seizure activity (for a resume of the changes, see Table 13.2).
13.5.1 Neuronal Mechanisms of A1Rs
The in vivo models of seizure are extremely useful to address the consequences of adenosine manipulation for the control of seizures and epileptogenesis, as discussed in the previous section. Nonetheless, when trying to further explore and detail the specific mechanisms by which adenosine and adenosine receptors exert its effects, the use of in vitro models of seizures may prove extremely helpful. Indeed, how A1Rs exert its anticonvulsant effects was first advanced by Lee and co-workers in vitro by demonstrating that A1R-mediated suppression of epileptiform activity was chemical synapse independent (Lee et al. 1984). The authors proposed that a hyperpolarizing effect of A1Rs, through blockage of outward K+ currents, might be involved in the process. Indeed, some years later, adenosine A1Rs were shown to change K+ channels not by inhibiting outward K+ currents but instead by facilitating G-proteins coupled inwardly rectifying K+ channels (GIRKs) (Trussell and Jackson 1987), ATP-sensitive K+ channels (KATP) (Li and Henry 1992) and small conductance Ca2+-activate K+ channels (SK) (Clark et al. 2009) and in this way regulate local depolarization of neurons through hyperpolarization (Ehrengruber et al. 1997). This is still considered one of the main mechanisms that contribute to A1R-dependent suppression of seizures.
Many other alternatives and complementary mechanisms have been proposed to explain adenosine actions on the different forms of epileptic seizures (Fig. 13.2). As discussed before, seizures have traditionally been viewed as caused by an imbalance between excitation (too much) and inhibition (too little) that compromise normal network functioning. Hyper-excitation may be caused by ionic (inward sodium or calcium current) changes or excitatory neurotransmission dysfunction (mostly glutamate); hypo-inhibition may result from dysregulation of potassium or chloride currents or disturbances in GABA-mediated neurotransmission. Most of these systems are also targets of adenosine receptors. In fact, in parallel with the postsynaptic hyperpolarizing effect already mentioned, A1Rs also control epileptiform activity by altering glutamatergic and GABAergic transmission.

Actions of adenosine during epileptic seizures. The mechanism by which adenosinergic system exerts its anticonvulsant actions is shown. These can be separated in neuronal mechanisms, which include A1R and A2AR presynaptic actions (on glutamate and GABA release) and postsynaptic actions (through potassium channels, AMPAR, NMDAR and GABAARs); non-neuronal mechanisms, involving astrocytes and regulation of adenosine levels (through changes in density and activity of ADK, E5NT, GAT or ENT); and homeostatic and epigenetic control, by modulating DNA methylation status and epileptogenesis. See text for further details and references. A1R, A1 receptor; A2AR, A2A receptor; Ado, adenosine; ADK, adenosine kinase; AMP, adenosine 5’-monophosphate; AMPAR, α-amino-3-hydroxy-5-methyl-4-isoxazolepropionic acid receptor; ATP, adenosine 5’-triphosphate; E5NT, ecto-5’-nucleotidase; ENT, equilibrative nucleoside transporter, GABA, gamma-aminobutyric acid; GABAAR, GABA type A receptor; GAT, GABA transporter; NMDAR , N-methyl-D-aspartate receptor
Considering glutamatergic transmission, we can distinguish pre- and postsynaptic actions of adenosine. Presynaptically, A1Rs reduce the release probability of glutamate through inhibition of voltage-dependent Ca2+ channels (VDCCs) (MacDonald et al. 1986; Schubert et al. 1986; Wu and Saggau 1994) or reduction of Ca2+-independent spontaneous release (Scholz and Miller 1992; Scanziani et al. 1992), with demonstrated anticonvulsant consequences in kainic acid-induced and picrotoxin-induced models of seizures (Arvin et al. 1989; Wang et al. 2013). Postsynaptically, actions are mostly related with interactions with AMPARs and NMDARs . Increased neuronal excitability during seizures leads to increased glutamate release and activation of glutamate receptors. Both AMPARs and NMDARs have been implicated in the initiation and establishment of epileptic seizures (Rice and Delorenzo 1998; Kharazia and Prince 2001; Kohl and Dannhardt 2001; Zhang et al. 2003). Suppression of A1R tonus in vitro causes a sustained synaptic-mediated epileptiform activity that has an AMPAR-dependent (Alzheimer et al. 1993; Moschovos et al. 2012) and NMDAR-dependent component (Thümmler and Dunwiddie 2000). Antiepileptogenic actions through AMPARs may be explained by a recent finding showing that A1Rs mediate a persistent synaptic depression of glutamatergic transmission through AMPAR endocytosis (Chen et al. 2014). Through NMDARs, A1R modulation involves the control of synaptic transmission and synaptic plasticity phenomena (de Mendonça et al. 1995; De Mendonça and Ribeiro 2000) that have implications during intense neuronal activity. For example, hampering A1R activation during burst activity will result in overactivation of NMDARs and consequent induction of maladaptive NMDAR-dependent plasticity phenomena responsible for maintaining and exacerbating disruptive circuits and seizures (Thümmler and Dunwiddie 2000). In a Mg2+-free in vitro model of seizures, the epileptiform activity gated by NMDAR activation (Nowak et al. 1984) is reduced after activation of A1R (O’Shaughnessy et al. 1988). Also, in a 3-MP model of seizures, A1Rs prevent the adaptive changes of NMDAR system (decrease in NR2B subunit expression) that occur as a consequence of seizures (Giraldez and Girardi 1998; Girardi et al. 2010). Together, these studies support the idea of a protective role of endogenous adenosine A1R activation through NMDARs by keeping excessive excitability, thus checking and preventing epileptogenesis, which has been observed both ex vivo (Alzheimer et al. 1989; Hamil et al. 2012) and in vivo (Hamil et al. 2012). Reciprocal modulation has also been observed between A1Rs and NMDARs. In fact, NMDAR activation during synchronized neuronal activity is another mechanism that explains the rising levels of adenosine during seizures (Hoehn and White 1990a, b; Manzoni et al. 1994). Also, chronic activation of NMDARs (in doses insufficient to cause behaviourally effects) promote a shift in A1R function towards a high-affinity state (Von Lubitz et al. 1995b) that results in increased potency of protective effects of A1Rs following a new and intensive insult (Von Lubitz et al. 1994b). The interplay between A1R and NMDAR contributes in this way to explain part of the neuroprotective actions of A1Rs during stablished epileptic activity.
In the case of inhibitory transmission, adenosine A1Rs have proven to directly influence GABA function in several brain areas (Sebastião et al. 2015). At the hippocampus, however, strong evidence exists about the lack of A1R effects on phasic GABAergic transmission (Yoon and Rothman 1991; Lambert and Teyler 1991; Prince and Stevens 1992). Alternative mechanisms (Rombo et al. 2016b) include direct influence on GABA type A receptor (GABAAR) , the ionotropic receptor for GABA (Petersen 1991; Concas et al. 1993) and control of tonic inhibition (Rombo et al. 2016a). While evaluating control of GABAergic function at the hippocampus, it is important to distinguish between control of GABAergic inputs to inhibitory neurons and control of GABAergic inputs to excitatory neurons. A1R-mediated decrease in tonic inhibition seems to be less relevant in pyramidal neurons than in interneurons (Rombo et al. 2016a), thus most probably contributing to an overall decrease in pyramidal neuron excitability. Whether the A1R-mediated inhibition of GABAAR function reported by Concas et al. (1993) also predominates in interneurons rather than in pyramidal neurons is not known.
A complex interaction seems to exist between adenosine and GABAAR recognition sites, including sites for allosteric ligands (such as benzodiazepine). There is nevertheless evidence that A1R-mediated influence over GABA-dependent transmission contributes to the anticonvulsant actions of adenosine (Klitgaard et al. 1993). Some authors document an interference of adenosine analogues on GABAAR number (Skolnick et al. 1980; Davies 1985) and binding properties (Davies 1985). Others show no effects of adenosine and adenosine receptors on GABAAR affinity (Williams et al. 1981). Another mechanistic explanation for these actions is that A1R activation would exert a shunting effect over GABAAR-mediated chloride conductance through facilitation of K+ channels (Ilie et al. 2012). This effect is particularly relevant during intense neuronal activity, when GABAAR responses transiently switch from hyperpolarizing to depolarizing and excitatory (Thompson and Gähwiler 1989; Staley et al. 1995; Kaila et al. 1997). In such conditions of increased GABA and adenosine concentrations, inhibition of tonic GABA responses in principal neurons would further suppress network excitability (Ortiz and Gutiérrez 2015; Rombo et al. 2016a). Control of GABA levels by regulating GABA transporter (GAT) function in nerve terminals and astrocytes, in an activity-dependent manner, may also contribute to these actions (Cristóvão-Ferreira et al. 2009, 2013). To our knowledge, besides A1R-GABA interplay to refrain epileptiform activity during ongoing seizures, there are no studies relating these two systems in the prevention of epileptogenesis and control of mechanisms that lead to stablished epilepsy.
Together, the above-mentioned studies provide experimental evidence to support the general consensus that neuronal anticonvulsant and antiepileptogenic mechanisms of adenosine A1Rs are mostly mediated by changes in excitatory transmission and hyperpolarization of principal neurons. Other complementary mechanisms affecting GABA-mediated transmission may interfere to further potentiate endogenous A1R-mediated antiseizure actions and reestablishment of normal network functioning.
13.5.2 Neuronal Mechanisms of A2ARs and A3Rs
In opposition to A1R actions , both A2ARs and A3Rs are mostly considered excitatory and proconvulsant . This is supported by in vitro studies where these receptors contribute to the progression of seizures (Fig. 13.2).
Ex vivo, antagonists of A2ARs restrain epileptiform activity (Etherington and Frenguelli 2004; Rombo et al. 2015), and A2AR agonists show a proconvulsant action (Klitgaard et al. 1993; Longo et al. 1995). The exact mechanisms by which A2AR blockade confers neuroprotection in epilepsy are not completely understood, since most of what is known is from models of brain damage after ischemia (Cunha 2005). It is, however, reasonable to think that similar mechanisms may also be present during excessive neuronal activation generated from seizure events. This would include control of glutamate release, where A2AR blockade protects neurons from excitotoxic glutamate outflow induced by ischemic stimuli (Popoli et al. 2002; Melani et al. 2003; Marcoli et al. 2003). Other possible mechanisms include prevention of neurotoxicity induced by AMPARs (Dias et al. 2012, 2013) and NMDARs (Robledo et al. 1999; Wirkner et al. 2004). However, ex vivo models of seizures show complex modulatory actions of A2ARs, since while facilitating NMDAR -independent induction of persistent epileptiform activity, A2ARs also suppress NMDAR-dependent progression of neuronal discharges (Moschovos et al. 2012). A novel mechanism by which brain-wide ADK deficiency (with significantly increased brain adenosine levels) leads to epileptic phenotype includes increased activation of A2ARs and disruption of synaptic plasticity phenomena, through a mechanism that involves A2AR-mediated exacerbation of BDNF functioning (Sandau et al. 2016). Despite the evidence of direct effect of A2AR activation on excitatory glutamatergic synapses, this may not completely explain the proconvulsive actions of these receptors. In fact, facilitation of epileptiform activity through A2ARs can also be explained by synergistic disinhibition of pyramidal cells through GABAergic communication between interneurons (Rombo et al. 2015). Direct actions of A2ARs on GABA function are also observed in human epileptic tissue, where endogenous A2AR activity was shown to increase GABAAR instability and consequent rundown of GABAergic responses (Roseti et al. 2008, 2009). Precluding these actions by preventing A2AR activation during epileptiform activity has significant anticonvulsant effects (Roseti et al. 2008; Rombo et al. 2015).
Much less is known about A3Rs, and as discussed above there is evidence for anti- as well as proconvulsive actions of A3R agonists. Their endogenous contribution to the promotion of epileptiform activity is limited, although its blockade is still capable of attenuating seizure intensity (Etherington and Frenguelli 2004). The effects may be direct or indirect, through A1Rs, influencing presynaptically glutamatergic transmission or postsynaptically K+ channels function (Dunwiddie et al. 1997) and desensitization of GABAARs (Roseti et al. 2009).
Despite scarce information about the operating mechanisms exerted by A2ARs and A3Rs during epileptiform activity, it is evident that blockade of A2AR , and most probably also of A3R, would prevent their synaptic neurotoxic effects responsible for aggravating neuronal excitability and epileptiform activity.
13.5.3 Non-neuronal Mechanisms of Adenosine
Astrocytes play a pivotal role in the generation and propagation of epileptic seizures by controlling synchronization of neuronal firing, ion homeostasis, reuptake of neurotransmitters and neuromodulators and release of gliotransmitters (Seifert et al. 2010). In what concerns adenosine metabolism, astrocytes have been implicated in regulating the levels of endogenous extracellular adenosine by directly participating in the adenosine cycle (Fig. 13.2). This involves (1) neuronal and astrocyte release of ATP (Pascual et al. 2005; Fields and Burnstock 2006), (2) extracellular formation of adenosine via a cascade of ecto-nucleotidases (Zimmermann 2000) and (3) uptake of adenosine back to neurons and astrocytes through ENT (King et al. 2006). The extracellular levels of adenosine are primarily controlled by actions of the astroglial enzyme ADK (Boison 2006). Perturbation of astrocyte homeostasis can affect the adenosinergic system and disrupt its neuroprotective effects. In fact, astrogliosis occurring in the epileptic brain is associated with increased expression of ADK and consequent depletion of adenosine levels, further exacerbating seizures (Gouder 2004; Li et al. 2008; de Groot et al. 2012). This evidence led to the proposal of an “ADK hypothesis of epileptogenesis” (Boison 2008, 2016a) based on biphasic changes in adenosine homeostasis during disease progression. A dysregulation of the normal brain functioning (due to structural, genetic, infectious, immune or metabolic causes) may result in an imbalance between excitatory and inhibitory mechanisms, thus leading to a seizure event. The immediate response to the insult consists of an acute surge in adenosine levels that is potentiated by acute downregulation of ADK (Gouder 2004), resulting in the termination of seizure. However, these seizure control actions may come with a price. Besides neuroprotective A1R activation, seizure event and adenosine rise will also contribute to adaptive changes that occur in the adenosinergic system including (1) downregulation of inhibitory A1Rs; (2) upregulation and overactivation of excitatory A2ARs; (3) switch in ADK expression, from decreased levels to sustained ADK overexpression (Gouder 2004); and (4) exacerbation of astrogliosis (Fiebich et al. 1996; Gebicke-Haerter et al. 1996; Bouilleret et al. 1999). All these adaptive changes contribute for the progression of the epileptogenic process (Li et al. 2007a). In fact, once astrogliosis and ADK overexpression are stablished, recurrent seizure onset is more likely (Li et al. 2007a, 2008, 2012a). Therefore, dysregulation of astrocyte and ADK functioning plays a significant role in the process that turns a normal brain into an epileptic brain (Boison 2016a).
13.5.4 Homeostatic and Epigenetic Mechanisms
One of the main actions of adenosine in mammalian cells is to control cell metabolism. Adenosine is in a privileged position to do this since minor changes in intracellular ATP concentrations as a result of metabolic challenges will result in disproportional larger changes in extracellular concentrations of adenosine (Cunha 2001). Besides the adenosine receptor-dependent actions discussed in the previous sections, adenosine exerts a more global biochemical regulation of cell function by means of epigenetic control, through DNA methylation (Williams-Karnesky et al. 2013) (Fig. 13.2). The classical source of adenosine is from a hydrolysing cascade reaction from ATP to ADP and to AMP by ectonucleotidases . However, another important source of adenosine is the hydrolysis of S-adenosyl-L-homocysteine (SAH) by SAH hydrolase (SAHH) (Schrader et al. 1981). SAH is involved in the transmethylation pathway responsible for methylation of DNA (James et al. 2002). Alterations in adenosine levels will thus influence SAH levels and DNA methylation. These epigenetic modifications are responsible for altering gene transcription without modifying the underlying DNA sequence. Methylation of the DNA has already been described in cells from the CNS (Ma et al. 2009), and it is responsible for some of the pathological changes observed during epileptogenic process (Henshall and Kobow 2015). When adenosine levels rise (e.g. during a seizure event), there is a shift in the equilibrium of the SAHH reaction towards the formation of SAH . Rises in SAH levels block DNA methyltransferase activity and decrease global DNA methylation levels (Williams-Karnesky et al. 2013). In this phase, adenosine-induced epigenetic mechanisms may be responsible for transcription and expression of epileptogenesis initiating genes (Boison 2016a). In later stages of epileptogenesis, increased ADK expression leads to a decrease in adenosine levels and consequent establishment of an hypermethylated DNA status that will further aggravate the epileptogenic condition (Miller-Delaney et al. 2015; Boison 2016b). These studies highlight a novel modulatory mechanism of adenosine in the control of epileptogenesis involving DNA methylation and epigenetic control.
13.6 Adenosine-Based Therapies
The experimental evidence discussed above about the anticonvulsant, neuroprotective and antiepileptogenic properties of adenosine provides the rational for the use of adenosine augmentation therapies in the treatment of epileptic seizures and epilepsy. This section intends to briefly discuss the most prominent approaches to increase adenosine levels in brain and holt synchronized neuronal activity and seizure progression.
13.6.1 Focal Adenosine Augmentation
One of the main reasons to prefer focal adenosine delivery approaches instead of systemic drug use is to avoid the considerable peripheral side effects of adenosine (mostly cardiovascular). Focal approaches are considered safe and feasible alternatives given the focal nature of many forms of epilepsy (Nilsen and Cock 2004). Tools for focal delivery include polymeric brain implant (Wilz et al. 2008), cell-based therapy and gene therapy (Löscher et al. 2008). To increase the concentrations of adenosine in the epileptic focus and supress seizure, the most effective strategy is by disrupting metabolic adenosine clearance through manipulation of ADK activity.
Starting with gene therapy approaches, two strategies have been used to augment adenosine levels: (1) antisense cDNA to disrupt the endogenous Adk gene (Theofilas et al. 2011) and (2) RNA interference (RNAi) to knock down ADK expression (Ren et al. 2007; Boison 2010). Both strategies can effectively be used to engineer focal release of adenosine, but additional studies are needed to evaluate its effectiveness in clinically relevant models of epilepsy (Boison 2016a).
Cell therapy approaches consist of injecting into the brain cell-derived implants that will exert its anticonvulsant actions via paracrine release of adenosine (Nilsen and Cock 2004). This method proved to be extremely efficient in supressing seizures and epileptogenesis (Huber et al. 2001; Li et al. 2007b, 2008, 2009).
Silk-based adenosine delivery strategies have unique therapeutic properties that bring them closer to clinical implementation. These properties include high biocompatibility and slow degradation kinetics (Horan et al. 2005). As occurred with cell-based therapies, polymeric brain implants were effective either when implanted before seizure induction (Wilz et al. 2008) or after full establishment of epilepsy (Szybala et al. 2009).
Together, data briefly discussed above suggests that focal adenosine augmentation therapies are promising strategies for preventing seizure occurrence and hamper epileptogenesis progression.
13.6.2 Dietary Therapies
Dietary therapies are effective, safe, non-pharmacologic treatments for intractable epilepsy, especially in children (Payne et al. 2011). The most used type of diet is the ketogenic diet (KD). This is a high-fat, low-carbohydrate, adequate-protein diet that has been used since the 1920s but resurged in popularity over the past 15 years (Wheless 2008). Despite its long clinical use, the mechanism by which KD suppresses seizure is not completely clarified (Rogawski et al. 2016). The hallmark of KD is the production of ketone bodies by the liver and its use as primary energy source. The anticonvulsant mechanisms include (1) ketone body-mediated inhibition of glutamate release and activation of KATP; (2) increased GABA synthesis; (3) increased mitochondrial function and biogenesis (with consequent rise in ATP production); (4) decreased production of reactive oxygen species; and (5) increased adenosine concentration, among others. The adenosine and adenosine receptor-mediated actions are indeed one of the key mechanisms underlying the anticonvulsant actions of KD (Masino et al. 2014). It was shown that reduction of seizure with KD is caused by increased adenosine signalling in the brain (Masino and Geiger 2008, 2009, Masino et al. 2011, 2012), mostly through activation of A1Rs (Masino et al. 2011). It is now clear the beneficial effects of the KD in the treatment of several forms of epilepsy (Neal et al. 2008; Lambrechts et al. 2017). The success of this strategy probably relies on its strong multifactorial mechanisms , and adenosine A1R-mediated anticonvulsant actions significantly contribute for this.
13.7 Conclusions and Future Perspectives
Accumulated evidence from the past 50 years of research on adenosine actions to control the initiation and progression of seizure events and epilepsy were briefly reviewed in this chapter. There are three main conclusions we can take from this data:
-
1.
Endogenous adenosine has a true anticonvulsant capacity and antiepileptogenic potential, mostly through A1R activation. However, recent data have been demonstrating the benefits of concomitantly modulating A2AR and even A3R to further potentiate its actions. The therapeutic use of adenosine depends on the stage of disease progression (acute vs chronic) and the targeting receptor and should always take into consideration its peripheral side effects (mostly cardiovascular-related).
-
2.
There are considerable adaptations of the adenosinergic system during the epileptogenic process that influences the mechanisms of action and disease progression. The anticonvulsant actions are exerted (I) at the synaptic level, mostly through A1R activation of potassium channels but also by A1R and A2AR control of glutamate and GABA function at pre-, post- and peri-synaptic compartments; (II) at non-neuronal level, by changing adenosine concentration through ADK expression in astrocytes; and (III) at homeostatic control level, by affecting DNA methylation status and consequently, the epileptogenic process.
-
3.
Several strategies are being developed to take advantage of all the potential of adenosinergic manipulation in the control and treatment of seizure events and prevent epileptogenesis. These include therapeutic adenosine augmentation strategies ranging from gene therapy to dietary intervention (such as ketogenic diet). The concomitant use of adenosine strategies together with conventional AED therapies currently available may potentiate and expand the efficacy of the intervention.
The diversity of adenosine effects and mechanisms of action are, indeed, an advantage for its use in epilepsy. However, this capacity of adenosine to act as a “universal modulator or maestro” of network functioning may come with a price. In fact, attention should be given to clearly differentiate the anti- and proconvulsant actions of adenosine that result from activation of different receptors at different neuronal and non-neuronal compartments. The mechanisms by which adenosine exerts its influence to regulate excitability in physiological, but mostly during pathophysiological situations, should thus be further understood. The challenge will be to take advantage of the homeostatic role of adenosine without never losing sight on the highly selective and sometimes opposing effects that are exerted by adenosine through its different receptors. Attention should thus be given not only to further develop strategies for increasing adenosine levels in the brain with the least peripheral side effects possible but also in the development of innovative adenosine ligands specifically directed to affect relevant neuronal targets, leaving untouched the ones not involved in the pathology.
As a final remark, and considering epileptogenesis itself, where too little is known on the influence of adenosine, inflammatory pathways have been highlighted as crucial in the underlying molecular mechanisms of epilepsy (van Vliet et al. 2018). Adenosine receptors, in particular A2AR (Chen and Pedata 2008; Dai and Zhou 2011) and A3R (Jacobson et al. 2017), interfere with the inflammatory cascade in a multiplicity of ways. There is thus time to also explore this avenue to better predict the influence of adenosine-based therapies in epilepsy.
References
Adami M, Bertorelli R, Ferri N et al (1995) Effects of repeated administration of selective adenosine A1 and A2A receptor agonists on pentylenetetrazole-induced convulsions in the rat. Eur J Pharmacol 294:383–389. https://doi.org/10.1016/0014-2999(95)00557-9
Adén U, O’Connor WT, Berman RF (2004) Changes in purine levels and adenosine receptors in kindled seizures in the rat. Neuroreport 15:1585–1589. https://doi.org/10.1097/01.wnr.0000133227
Akula KK, Kulkarni SK (2014) Effect of Curcumin Against Pentylenetetrazol- Induced Seizure Threshold in Mice : Possible Involvement of Adenosine A 1 Receptors. Phytother Res 721:714–721
Alasvand Zarasvand M, Mirnajafi-Zadeh J, Fathollahi Y, Palizvan MR (2001) Anticonvulsant effect of bilateral injection of N6-cyclohexyladenosine into the CA1 region of the hippocampus in amygdala-kindled rats. Epilepsy Res 47:141–149. https://doi.org/10.1016/S0920-1211(01)00300-X
Albertson TE, Stark LG, Joy RM, Bowyer JF (1983) Aminophylline and kindled seizures. Exp Neurol 81:703–713
Alzheimer C, Sutor B, ten Bruggencate G (1989) Transient and selective blockade of adenosine A1-receptors by 8-cyclopentyl-1,3-dipropylxanthine (DPCPX) causes sustained epileptiform activity in hippocampal CA3 neurons of guinea pigs. Neurosci Lett 99:107–112. https://doi.org/10.1016/0304-3940(89)90273-90275
Alzheimer C, Sutor B, Ten Bruggencate G (1993) Disinhibition of hippocampal CA3 neurons induced by suppression of an adenosine A1 receptor-mediated inhibitory tonus: Pre- and postsynaptic components. Neuroscience 57:565–575. https://doi.org/10.1016/0306-4522(93)90006-2
Angelatou F, Pagonopoulou O, Kostopoulos G (1990) Alterations of A1 adenosine receptors in different mouse brain areas after pentylenetetrazol-induced seizures, but not in the epileptic mutant mouse “tottering”. Brain Res 534:251–256. https://doi.org/10.1016/0006-8993(90)90136-Y
Angelatou F, Pagonopoulou O, Kostopoulos G (1991) Changes in seizure latency correlate with alterations in A1 adenosine receptor binding during daily repeated pentylenetetrazol-induced convulsions in different mouse brain areas. Neurosci Lett 132:203–206. https://doi.org/10.1016/0304-3940(91)90302-A
Angelatou F, Pagonopoulou O, Maraziotis T et al (1993) Upregulation of A1 adenosine receptors in human temporal lobe epilepsy: a quantitative autoradiographic study. NeurosciLett 163:11–14
Aronica E, Zurolo E, Iyer A et al (2011) Upregulation of adenosine kinase in astrocytes in experimental and human temporal lobe epilepsy. Epilepsia 52:1645–1655. https://doi.org/10.1111/j.1528-1167.2011.03115.x
Arvidsson SB, Ekström-Jodal B, Martinell SA, Niemand D (1982) Aminophylline antagonises diazepam sedation. Lancet (London, England) 2:1467
Arvin B, Neville LF, Pan J, Roberts PJ (1989) 2-chloroadenosine attenuates kainic acid-induced toxicity within the rat straitum: relationship to release of glutamate and Ca2+ influx. Br J Pharmacol 98:225–235
Avsar E, Empson RM (2004) Adenosine acting via A1 receptors, controls the transition to status epilepticus-like behaviour in an in vitro model of epilepsy. Neuropharmacology 47:427–437. https://doi.org/10.1016/j.neuropharm.2004.04.015
Banerjee PN, Filippi D, Allen Hauser W (2009) The descriptive epidemiology of epilepsy-A review. Epilepsy Res 85:31–45. https://doi.org/10.1016/j.eplepsyres.2009.03.003
Barraco RA, Swanson TH, Phillis JW, Berman RF (1984) Anticonvulsant effects of adenosine analogues on amygdaloid- kindled seizures in rats. Neurosci Lett 46:317–322
Beghi E, Hesdorffer D (2014) Prevalence of epilepsy-An unknown quantity. Epilepsia 55:963–967. https://doi.org/10.1111/epi.12579
Bell GS, Neligan A, Sander JW (2014) An unknown quantity - The worldwide prevalence of epilepsy. Epilepsia 55:958–962. https://doi.org/10.1111/epi.12605
Bender AS, Hertz L (1986) Similarities of adenosine uptake systems in astrocytes and neurons in primary cultures. Neurochem Res 11:1507–1524
Berg AT, Millichap JJ (2013) The 2010 revised classification of seizures and epilepsy. Continuum (Minneap Minn) 19:571–597. https://doi.org/10.1212/01.CON.0000431377.44312.9e
Berman RF, Fredholm BB, Aden U, Connor WTO (2000) Evidence for increased dorsal hippocampal adenosine release and metabolism during pharmacologically induced seizures in rats. Brain Res 872:44–53
Bialer M, White HS (2010) Key factors in the discovery and development of new antiepileptic drugs. Nat Rev Drug Discov 9:68–82. https://doi.org/10.1038/nrd2997
Bjursell MK, Blom HJ, Cayuela JA et al (2011) Adenosine kinase deficiency disrupts the methionine cycle and causes hypermethioninemia, encephalopathy, and abnormal liver function. Am J Hum Genet 89:507–515. https://doi.org/10.1016/j.ajhg.2011.09.004
Boison D (2006) Adenosine kinase, epilepsy and stroke: mechanisms and therapies. Trends Pharmacol Sci 27:652–658. https://doi.org/10.1016/j.tips.2006.10.008
Boison D (2008) The adenosine kinase hypothesis of epileptogenesis. Prog Neurobiol 84:249–262. https://doi.org/10.1016/j.pneurobio.2007.12.002
Boison D (2010) Inhibitory RNA in epilepsy: Research tools and therapeutic perspectives. Epilepsia 51:1659–1668. https://doi.org/10.1111/j.1528-1167.2010.02672.x
Boison D (2016a) Adenosinergic signaling in epilepsy. Neuropharmacology 104:131–139. https://doi.org/10.1016/j.neuropharm.2015.08.046
Boison D (2016b) The Biochemistry and Epigenetics of Epilepsy: Focus on Adenosine and Glycine. Front Mol Neurosci 9:26. https://doi.org/10.3389/fnmol.2016.00026
Boison D, Scheurer L, Tseng JL et al (1999) Seizure suppression in kindled rats by intraventricular grafting of an adenosine releasing synthetic polymer. Exp Neurol 160:164–174. https://doi.org/10.1006/exnr.1999.7209
Boison D, Huber A, Padrun V et al (2002) Seizure suppression by adenosine-releasing cells is independent of seizure frequency. Epilepsia 43:788–796. https://doi.org/10.1046/j.1528-1157.2002.33001.x
Bonan CD, Amaral OB, Rockenbach IC et al (2000a) Altered ATP hydrolysis induced by pentylenetetrazol kindling in rat brain synaptosomes. Neurochem Res 25:775–779. https://doi.org/10.1023/A:1007557205523
Bonan CD, Walz R, Pereira GS et al (2000b) Changes in synaptosomal ectonucleotidase activities in two rat models of temporal lobe epilepsy. Epilepsy Res 39:229–238. https://doi.org/10.1016/S0920-1211(00)00095-4
Borowicz KK, Kleinrok Z, Czuczwar SJ (1997) N6-2-(4-aminophenyl) ethyl-adenosine enhances the anticonvulsive activity of antiepileptic drug. Eur J Pharmacol 327:125–133. https://doi.org/10.1016/S0014-2999(97)89651-3
Borowicz KK, Kleinrok Z, Czuczwar SJ (2000) N6-2-(4-Aminophenyl)ethyl-adenosine enhances the anticonvulsive action of conventional antiepileptic drugs in the kindling model of epilepsy in rats. Eur Neuropsychopharmacol 10:237–243. https://doi.org/10.1016/S0924-977X(00)00081-X
Borowicz KK, Luszczki J, Czuczwar SJ (2002) 2-Chloroadenosine, a preferential agonist of adenosine A1 receptors, enhances the anticonvulsant activity of carbamazepine and clonazepam in mice. Eur Neuropsychopharmacol 12:173–179. https://doi.org/10.1016/S0924-977X(02)00009-3
Borowicz KK, Swiader M, Wielosz M, Czuczwar SJ (2004) Influence of the combined treatment of LY 300164 (an AMPA/kainate receptor antagonist) with adenosine receptor agonists on the electroconvulsive threshold in mice. Eur Neuropsychopharmacol 14:407–412. https://doi.org/10.1016/j.euroneuro.2003.12.003
Bough KJ, Rho JM (2007) Anticonvulsant mechanisms of the ketogenic diet. Epilepsia 48:43–58. https://doi.org/10.1111/j.1528-1167.2007.00915.x
Bouilleret V, Ridoux V, Depaulis A et al (1999) Recurrent seizures and hippocampal sclerosis following intrahippocampal kainate injection in adult mice: Electroencephalography, histopathology and synaptic reorganization similar to mesial temporal lobe epilepsy. Neuroscience 89:717–729. https://doi.org/10.1016/S0306-4522(98)00401-1
Brodie MS, Lee K, Fredholm BB et al (1987) Central versus peripheral mediation of responses to adenosine receptor agonists: Evidence against a central mode of action. Brain Res 415:323–330. https://doi.org/10.1016/0006-8993(87)90214-9
Chen J-F, Pedata F (2008) Modulation of ischemic brain injury and neuroinflammation by adenosine A2A receptors. Curr Pharm Des 14:1490–1499
Chen Z, Xiong C, Pancyr C et al (2014) Prolonged Adenosine A1 Receptor Activation in Hypoxia and Pial Vessel Disruption Focal Cortical Ischemia Facilitates Clathrin-Mediated AMPA Receptor Endocytosis and Long-Lasting Synaptic Inhibition in Rat Hippocampal CA3-CA1 Synapses: Differential Regulat. J Neurosci 34:9621–9643. https://doi.org/10.1523/JNEUROSCI.3991-13.2014
Chin JH (1989) Adenosine receptors in brain: neuromodulation and role in epilepsy. Ann Neurol 26:695–698. https://doi.org/10.1002/ana.410260602
Clark BD, Kurth-Nelson ZL, Newman EA (2009) Adenosine-evoked hyperpolarization of retinal ganglion cells is mediated by G-protein-coupled inwardly rectifying K+ and small conductance Ca2+-activated K+ channel activation. J Neurosci 29:11237–11245. https://doi.org/10.1523/JNEUROSCI.2836-09.2009
Concas A, Santoro G, Mascia MP et al (1993) Anticonvulsant doses of 2-chloro-N6-cyclopentyladenosine, an adenosine A1 receptor agonist, reduce GABAergic transmission in different areas of the mouse brain. J Pharmacol Exp Ther 267:844–851
Cristóvão-Ferreira S, Vaz SH, Ribeiro JA, Sebastião AM (2009) Adenosine A2A receptors enhance GABA transport into nerve terminals by restraining PKC inhibition of GAT-1. J Neurochem 109:336–347. https://doi.org/10.1111/j.1471-4159.2009.05963.x
Cristóvão-Ferreira S, Navarro G, Brugarolas M et al (2013) A1R-A2AR heteromers coupled to Gs and G i/0 proteins modulate GABA transport into astrocytes. Purinergic Signal 9:433–449. https://doi.org/10.1007/s11302-013-9364-5
Cunha RA (2001) Adenosine as a neuromodulator and as a homeostatic regulator in the nervous system: different roles, different sources and different receptors. Neurochem Int 38:107–125
Cunha RA (2005) Neuroprotection by adenosine in the brain: From A(1) receptor activation to A (2A) receptor blockade. Purinergic Signal 1:111–134. https://doi.org/10.1007/s11302-005-0649-1
Cunha RA, Correia-de-Sá P, Sebastião AM, Ribeiro JA (1996) Preferential activation of excitatory adenosine receptors at rat hippocampal and neuromuscular synapses by adenosine formed from released adenine nucleotides. Br J Pharmacol 119:253–260
Czuczwar SJ, Turski WA, Ikonomidou C, Turski L (1985) Aminophylline and CGS 8216 Reverse the Protective Action of Diazepam Against Electroconvulsions in Mice. Epilepsia 26:693–696. https://doi.org/10.1111/j.1528-1157.1985.tb05713.x
Czuczwar SJ, Szczepanik B, Wamil A et al (1990) Differential effects of agents enhancing purinergic transmission upon the antielectroshock efficacy of carbamazepine, diphenylhydantoin, diazepam, phenobarbital, and valproate in mice. J Neural Transm 81:153–166. https://doi.org/10.1007/BF01245835
D’Alimonte I, D’Auro M, Citraro R et al (2009) Altered distribution and function of A2A adenosine receptors in the brain of WAG/Rij rats with genetic absence epilepsy, before and after appearance of the disease. Eur J Neurosci 30:1023–1035. https://doi.org/10.1111/j.1460-9568.2009.06897.x
Dai S-S, Zhou Y-G (2011) Adenosine 2A receptor: a crucial neuromodulator with bidirectional effect in neuroinflammation and brain injury. Rev Neurosci 22:231–239. https://doi.org/10.1515/RNS.2011.020
Daval JL, Sarfati A (1987) Effects of bicuculline-induced seizures on benzodiazepine and adenosine receptors in developing rat brain. Life Sci 41:1685–1693. https://doi.org/10.1016/0024-3205(87)90595-9
Daval J, Werck M (1991) Autoradiographic changes in brain adenosine A1 receptors and their coupling to G proteins following seizures in the developing rat. Brain Res Dev Brain Res 59:237–247
Davies LP (1985) Pharmacological studies on adenosine analogues isolated from marine organisms. Trends Pharmacol Sci 6:143–146. https://doi.org/10.1016/0165-6147(85)90066-5
de Groot M, Iyer A, Zurolo E et al (2012) Overexpression of ADK in human astrocytic tumors and peritumoral tissue is related to tumor-associated epilepsy. Epilepsia 53:58–66. https://doi.org/10.1111/j.1528-1167.2011.03306.x
De Mendonça A, Ribeiro JA (2000) Long-term potentiation observed upon blockade of adenosine A1 receptors in rat hippocampus is N-methyl-D-aspartate receptor-dependent. Neurosci Lett 291:81–84. https://doi.org/10.1016/S0304-3940(00)01391-4
De Mendonça A, Sebastião AM, Ribeiro JA (1995) Inhibition of NMDA receptor-mediated currents in isolated rat hippocampal neurones by adenosine A1 receptor activation. Neuroreport 6:1097–1100
De Sarro G, De Sarro A, Donato E et al (1999) Effects of adenosine receptor agonists and antagonists on audiogenic seizure-sensible DBAr2 mice. Eur J Pharmacol 371:137–145
Dias RB, Ribeiro JA, Sebastião AM (2012) Enhancement of AMPA currents and GluR1 membrane expression through PKA-coupled adenosine A(2A) receptors. Hippocampus 22:276–291. https://doi.org/10.1002/hipo.20894
Dias RB, Rombo DM, Ribeiro JA, Sebastião AM (2013) Ischemia-induced synaptic plasticity drives sustained expression of calcium-permeable AMPA receptors in the hippocampus. Neuropharmacology 65:114–122. https://doi.org/10.1016/j.neuropharm.2012.09.016
Dodd PR, Watson WE, Johnston GA (1986) Adenosine receptors in post-mortem human cerebral cortex and the effect of carbamazepine. Clin Exp Pharmacol Physiol 13:711–722
Dragunow M, Goddard GV (1984) Adenosine modulation of amygdala kindling. Exp Neurol 84:654–665. https://doi.org/10.1016/0014-4886(84)90212-7
Dragunow M, Robertson HA (1987) 8-Cyclopentyl 1,3-dimethylxanthine prolongs epileptic seizures in rats. Brain Res 417:377–379. https://doi.org/10.1016/0006-8993(87)90468-9
Dragunow M, Goddard GV, Laverty R (1985) Is adenosine an endogenous anticonvulsant? Epilepsia 26:480–487
Dunwiddie TV (1980) Endogenously released adenosine regulates excitability in the in vitro hippocampus. Epilepsia 21:541–548. https://doi.org/10.1111/j.1528-1157.1980.tb04305.x
Dunwiddie TV, Hoffer BJ (1980) Adenine nucleotides and synaptic transmission in the in vitro rat hippocampus. Br J Pharmacol 69:59–68
Dunwiddie TV, Worth T (1982) Sedative and anticonvulsant effects of adenosine analogs in mouse and rat. J Pharmacol Exp Ther 220:70–76
Dunwiddie TV, Diao L, Kim HO et al (1997) Activation of hippocampal adenosine A3 receptors produces a desensitization of A1 receptor-mediated responses in rat hippocampus. J Neurosci 17:607–614
During MJ, Spencer DD (1992) Adenosine: A potential mediator of seizure arrest and postictal refractoriness. Ann Neurol 32:618–624. https://doi.org/10.1002/ana.410320504
Ehrengruber MU, Doupnik CA, Xu Y et al (1997) Activation of heteromeric G protein-gated inward rectifier K+ channels overexpressed by adenovirus gene transfer inhibits the excitability of hippocampal neurons. Proc Natl Acad Sci U S A 94:7070–7075
Ekonomou A, Vergnes M, Kostopoulos G (1998) Lower density of A1 adenosine receptors in nucleus reticularis thalami in rats with genetic absence epilepsy. Neuroreport 9:2135–2140
Ekonomou A, Sperk G, Kostopoulos G, Angelatou F (2000) Reduction of A1 adenosine receptors in rat hippocampus after kainic acid-induced limbic seizures. NeurosciLett 284:49–52
El Yacoubi M, Ledent C, Parmentier M et al (2001) Absence of the adenosine A2A receptor or its chronic blockade decrease ethanol withdrawal-induced seizures in mice. Neuropharmacology 40:424–432. https://doi.org/10.1016/S0028-3908(00)00173-8
El Yacoubi M, Ledent C, Parmentier M et al (2008) Evidence for the involvement of the adenosine A2A receptor in the lowered susceptibility to pentylenetetrazol-induced seizures produced in mice by long-term treatment with caffeine. Neuropharmacology 55:35–40. https://doi.org/10.1016/j.neuropharm.2008.04.007
El Yacoubi M, Ledent C, Parmentier M et al (2009) Adenosine A2A receptor deficient mice are partially resistant to limbic seizures. Naunyn Schmiedebergs Arch Pharmacol 380:223–232. https://doi.org/10.1007/s00210-009-0426-8
Eldridge FL, Paydarfar D, Scott SC, Dowell RT (1989) Role of endogenous adenosine in recurrent generalized seizures. Exp Neurol 103:179–185. https://doi.org/10.1016/0014-4886(89)90080-0
Engel J (1996a) Surgery for Seizures. N Engl J Med 334:647–653. https://doi.org/10.1056/NEJM199603073341008
Engel J (1996b) Introduction to temporal lobe epilepsy. Epilepsy Res 26:141–150. https://doi.org/10.1016/S0920-1211(96)00043-5
Etherington LV, Frenguelli BG (2004) Endogenous adenosine modulates epileptiform activity in rat hippocampus in a receptor subtype-dependent manner. Eur J Neurosci 19:2539–2550. https://doi.org/10.1111/j.0953-816X.2004.03355.x
Etherington LA, Patterson GE, Meechan L et al (2009) Astrocytic adenosine kinase regulates basal synaptic adenosine levels and seizure activity but not activity-dependent adenosine release in the hippocampus. Neuropharmacology 56:429–437. https://doi.org/10.1016/j.neuropharm.2008.09.016
Faingold CL, Randall M, Kommajosyula SP (2016) Susceptibility to seizure-induced sudden death in DBA/2 mice is altered by adenosine. Epilepsy Res 124:49–54. https://doi.org/10.1016/j.eplepsyres.2016.05.007
Fedele DE, Li T, Lan JQ et al (2006) Adenosine A1 receptors are crucial in keeping an epileptic focus localized. Exp Neurol 200:184–190. https://doi.org/10.1016/j.expneurol.2006.02.133
Fiebich BL, Biber K, Lieb K et al (1996) Cyclooxygenase-2 expression in rat microglia is induced by adenosine A2a-receptors. Glia 18:152–160 doi: 10.1002/(SICI)1098-1136(199610)18:2<152::AID-GLIA7>3.0.CO;2-2
Fields RD, Burnstock G (2006) Purinergic signalling in neuron-glia interactions. Nat Rev Neurosci 7:423–436. https://doi.org/10.1038/nrn1928
Fisher RS, Van Emde BW, Blume W et al (2005) Epileptic seizures and epilepsy: Definitions proposed by the International League Against Epilepsy (ILAE) and the International Bureau for Epilepsy (IBE). Epilepsia 46:470–472. https://doi.org/10.1111/j.0013-9580.2005.66104.x
Fisher RS, Acevedo C, Arzimanoglou A et al (2014) ILAE Official Report: A practical clinical definition of epilepsy. Epilepsia 55:475–482. https://doi.org/10.1111/epi.12550
Fisher RS, Cross JH, D’Souza C et al (2017) Instruction manual for the ILAE 2017 operational classification of seizure types. Epilepsia 58:531–542. https://doi.org/10.1111/epi.13671
Franklin PH, Zhang G, Tripp ED, Murray TF (1989) Adenosine A1 receptor activation mediates suppression of (-) bicuculline methiodide-induced seizures in rat prepiriform cortex. J Pharmacol Exp Ther 251:1229–1236
Fujiwara Y, Sato M, Otsuki S (1986) Interaction of carbamazepine and other drugs with adenosine (A1and A2) receptors. Psychopharmacology (Berl) 90:332–335. https://doi.org/10.1007/BF00179186
Fukuda M, Suzuki Y, Hino H et al (2010) Adenosine A1 receptor blockage mediates theophylline-associated seizures. Epilepsia 51:483–487. https://doi.org/10.1111/j.1528-1167.2009.02382.x
Gebicke-Haerter PJ, Christoffel F, Timmer J et al (1996) Both adenosine A1- and A2-receptors are required to stimulate microglial proliferation. Neurochem Int 29:37–42. https://doi.org/10.1016/0197-0186(95)00137-9
Giraldez L, Girardi E (1998) Modification of [3H]MK801 binding to rat brain NMDA receptors after the administration of a convulsant drug and an adenosine analogue: A quantitative autoradiographic study. Neurochem Res 23:1327–1336. https://doi.org/10.1023/A:1020708603495
Girardi ES, Canitrot J, Antonelli M et al (2007) Differential expression of cerebellar metabotropic glutamate receptors mGLUR2/3 and mGLUR4a after the administration of a convulsant drug and the adenosine analogue cyclopentyladenosine. Neurochem Res 32:1120–1128. https://doi.org/10.1007/s11064-006-9275-8
Girardi E, Auzmendi J, Charó N et al (2010) 3-mercaptopropionic acid-induced seizures decrease NR2B expression in Purkinje cells: Cyclopentyladenosine effect. Cell Mol Neurobiol 30:985–990. https://doi.org/10.1007/s10571-010-9546-4
Glass M, Faull RL, Bullock JY et al (1996) Loss of A1 adenosine receptors in human temporal lobe epilepsy. Brain Res 710:56–68
Gleiter CH, Deckert J, Nutt DJ, Marangos PJ (1989) Electroconvulsive Shock (ECS) and the Adenosine Neuromodulatory System: Effect of Single and Repeated ECS on the Adenosine A1 and A2 Receptors, Adenylate Cyclase, and the Adenosine Uptake Site. J Neurochem 52:641–646. https://doi.org/10.1111/j.1471-4159.1989.tb09168.x
Goddard GV (1967) Development of epileptic seizures through brain stimulation at low intensity. Nature 214:1020–1021. https://doi.org/10.1038/2141020a0
Goddard GV, McIntyre DC, Leech CK (1969) A permanent change in brain function resulting from daily electrical stimulation. Exp Neurol 25:295–330. https://doi.org/10.1016/0014-4886(69)90128-9
Gouder N (2004) Overexpression of Adenosine Kinase in Epileptic Hippocampus Contributes to Epileptogenesis. J Neurosci 24:692–701. https://doi.org/10.1523/JNEUROSCI.4781-03.2004
Granata T, Marchi N, Carlton E et al (2009) Management of the patient with medically refractory epilepsy. Expert Rev Neurother 9:1791–1802. https://doi.org/10.1586/ern.09.114
Güttinger M, Fedele D, Koch P et al (2005a) Suppression of kindled seizures by paracrine adenosine release from stem cell-derived brain implants. Epilepsia 46:1162–1169. https://doi.org/10.1111/j.1528-1167.2005.61804.x
Güttinger M, Padrun V, Pralong WF, Boison D (2005b) Seizure suppression and lack of adenosine A1receptor desensitization after focal long-term delivery of adenosine by encapsulated myoblasts. Exp Neurol 193:53–64. https://doi.org/10.1016/j.expneurol.2004.12.012
Hamil NE, Cock HR, Walker MC (2012) Acute down-regulation of adenosine A(1) receptor activity in status epilepticus. Epilepsia 53:177–188. https://doi.org/10.1111/j.1528-1167.2011.03340.x
Hammond JR, Paterson AR, Clanachan AS (1981) Benzodiazepine inhibition of site-specific binding of nitrobenzylthioinosine, an inhibitor of adenosine transport. Life Sci 29:2207–2214
Hargus NJ, Jennings C, Perez-Reyes E et al (2012) Enhanced actions of adenosine in medial entorhinal cortex layer II stellate neurons in temporal lobe epilepsy are mediated via A(1)-receptor activation. Epilepsia 53:168–176. https://doi.org/10.1111/j.1528-1167.2011.03337.x
Heidarianpour A, Sadeghian E, Mirnajafi-Zadeh J et al (2006) Anticonvulsant effects of N6-cyclohexyladenosine microinjected into the CA1 region of the hippocampus on entorhinal cortex-kindled seizures in rats. Epileptic Disord 8:259–266. https://doi.org/10.1684/epd.2006.0037
Heinemann U, Kann O, Remy S, Beck H (2006) Novel mechanisms underlying drug resistance in temporal lobe epilepsy. Adv Neurol 97:85–95
Henshall DC, Kobow K (2015) Epigenetics and Epilepsy. Cold Spring Harb Perspect Med 5:715–736. https://doi.org/10.1101/cshperspect.a022731
Hoehn K, White TD (1990a) Role of excitatory amino acid receptors in K+- and glutamate-evoked release of endogenous adenosine from rat cortical slices. J Neurochem 54:256–265
Hoehn K, White TD (1990b) N-methyl-D-aspartate, kainate and quisqualate release endogenous adenosine from rat cortical slices. Neuroscience 39:441–450
Horan RL, Antle K, Collette AL et al (2005) In vitro degradation of silk fibroin. Biomaterials 26:3385–3393. https://doi.org/10.1016/j.biomaterials.2004.09.020
Hosseinmardi N, Mirnajafi-Zadeh J, Fathollahi Y, Shahabi P (2007) The role of adenosine A1 and A2A receptors of entorhinal cortex on piriform cortex kindled seizures in rats. Pharmacol Res 56:110–117. https://doi.org/10.1016/j.phrs.2007.04.011
Huber A, Padrun V, Déglon N et al (2001) Grafts of adenosine-releasing cells suppress seizures in kindling epilepsy. Proc Natl Acad Sci U S A 98:7611–7616. https://doi.org/10.1073/pnas.131102898
Huber A, Güttinger M, Möhler H, Boison D (2002) Seizure suppression by adenosine A(2A) receptor activation in a rat model of audiogenic brainstem epilepsy. Neurosci Lett 329:289–292
Ilie A, Raimondo JV, Akerman CJ (2012) Adenosine release during seizures attenuates GABAA receptor-mediated depolarization. J Neurosci 32:5321–5332. https://doi.org/10.1523/JNEUROSCI.5412-11.2012
Ivanov AI, Bernard C (2017) Hippocampus in vitro. In: Models of seizures and epilepsy, 2nd edn. Elsevier Inc., United Kingdom, pp 261–272
Jacobson KA, Merighi S, Varani K, et al (2017) A3adenosine receptors as modulators of inflammation: from medicinal chemistry to therapy. Med Res Rev 1–42. doi: https://doi.org/10.1002/med.21456
James SJ, Melnyk S, Pogribna M et al (2002) Elevation in S-adenosylhomocysteine and DNA hypomethylation: potential epigenetic mechanism for homocysteine-related pathology. J Nutr 132:2361S–2366S
Janusz CA, Berman RF (1992) The A2-selective adenosine analog, CGS 21680, depresses locomotor activity but does not block amygdala kindled seizures in rats. Neurosci Lett 141:247–250. https://doi.org/10.1016/0304-3940(92)90905-M
Jones P, Smith R, Stone T (1998a) Protection against kainate-induced excitotoxicity by adenosine A2A receptor agonists and antagonists. Neuroscience 85:229–237. https://doi.org/10.1016/S0306-4522(97)00613-1
Jones PA, Smith RA, Stone TW (1998b) Protection against hippocampal kainate excitotoxicity by intracerebral administration of an adenosine A2A receptor antagonist. Brain Res 800:328–335
Kaila K, Lamsa K, Smirnov S et al (1997) Long-lasting GABA-mediated depolarization evoked by high-frequency stimulation in pyramidal neurons of rat hippocampal slice is attributable to a network-driven, bicarbonate-dependent K+ transient. J Neurosci 17:7662–7672
Kaku T, Jiang MH, Hada J et al (2001) Sodium nitroprusside-induced seizures and adenosine release in rat hippocampus. Eur J Pharmacol 413:199–205. https://doi.org/10.1016/S0014-2999(01)00763-4
Kaplan GB, Cotreau MM, Greenblatt DJ (1992) Effects of benzodiazepine administration on A1 adenosine receptor binding in-vivo and ex-vivo. J Pharm Pharmacol 44:700–703
Khan GM, Smolders I, Ebinger G, Michotte Y (2000) Anticonvulsant effect and neurotransmitter modulation of focal and systemic 2-chloroadenosine against the development of pilocarpine-induced seizures. Neuropharmacology 39:2418–2432
Khan GM, Smolders I, Ebinger G, Michotte Y (2001) 2-chloro-N(6)-cyclopentyladenosine-elicited attenuation of evoked glutamate release is not sufficient to give complete protection against pilocarpine-induced seizures in rats. Neuropharmacology 40:657–667
Kharazia VN, Prince DA (2001) Changes of alpha-amino-3-hydroxy-5-methyl-4-isoxazole-propionate receptors in layer V of epileptogenic, chronically isolated rat neocortex. Neuroscience 102:23–34 doi: S0306-4522(00)00467-X [pii]
Kiese K, Jablonski J, Boison D, Kobow K (2016) Dynamic regulation of the adenosine kinase gene during early postnatal brain development and maturation. Front Mol Neurosci 9. https://doi.org/10.3389/fnmol.2016.00099
King AE, Ackley MA, Cass CE et al (2006) Nucleoside transporters: from scavengers to novel therapeutic targets. Trends Pharmacol Sci 27:416–425. https://doi.org/10.1016/j.tips.2006.06.004
Klaft ZJ, Schulz SB, Maslarova A et al (2012) Extracellular ATP differentially affects epileptiform activity via purinergic P2X7 and adenosine A1 receptors in naive and chronic epileptic rats. Epilepsia 53:1978–1986. https://doi.org/10.1111/j.1528-1167.2012.03724.x
Klitgaard H, Knutsen LJ, Thomsen C (1993) Contrasting effects of adenosine A1 and A2 receptor ligands in different chemoconvulsive rodent models. Eur J Pharmacol 242:221–228
Kochanek PM, Vagni VA, Janesko KL et al (2006) Adenosine A1 receptor knockout mice develop lethal status epilepticus after experimental traumatic brain injury. J Cereb Blood Flow Metab 26:565–575. https://doi.org/10.1038/sj.jcbfm.9600218
Kohl BK, Dannhardt G (2001) The NMDA receptor complex: a promising target for novel antiepileptic strategies. Curr Med Chem 8:1275–1289. https://doi.org/10.2174/0929867013372328
Kostopoulos GK, Limacher JJ, Phillis JW (1975) Action of various adenine derivatives on cerebellar Purkinje cells. Brain Res 88:162–165
Kulkarni C, Joseph T, David J (1991) Influence of adenosine receptor antagonists, aminophylline and caffeine, on seizure protective ability of antiepileptic drugs in rats. Indian J Exp Biol 29:751–754
Kuroda Y, Kobayashi K (1975) Effects of Adenosine and Adenine Nucleotides on the Posts ynaptic Potential and on the Formation of Cyclic Adenosine 3 ’, 5 ’. Monophosphate from Radioactive Adenosine Triphosphate in Guinea Pig Olfactory Cortex Slices. Proc Jpn Acad 51:495–500
Kwan P, Brodie MJ (2001) Effectiveness of first antiepileptic drug. Epilepsia 42:1255–1260. https://doi.org/10.1046/j.1528-1157.2001.04501.x
Lambert NA, Teyler TJ (1991) Adenosine depresses excitatory but not fast inhibitory synaptic transmission in area CA1 of the rat hippocampus. Neurosci Lett 122:50–52. https://doi.org/10.1016/0304-3940(91)90190-90195
Lambrechts DAJE, de Kinderen RJA, Vles JSH et al (2017) A randomized controlled trial of the ketogenic diet in refractory childhood epilepsy. Acta Neurol Scand 135:231–239. https://doi.org/10.1111/ane.12592
Lancaster E, Dalmau J (2012) Neuronal autoantigens—pathogenesis, associated disorders and antibody testing. Nat Rev Neurol 8:380–390. https://doi.org/10.1038/nrneurol.2012.99
Laudadio MA, Psarropoulou C (2004) The A3 adenosine receptor agonist 2-Cl-IB-MECA facilitates epileptiform discharges in the CA3 area of immature rat hippocampal slices. Epilepsy Res 59:83–94. https://doi.org/10.1016/j.eplepsyres.2004.03.005
Lee KS, Schubert P, Heinemann U (1984) The anticonvulsive action of adenosine: a postsynaptic, dendritic action by a possible endogenous anticonvulsant. Brain Res 321:160–164. https://doi.org/10.1016/0006-8993(84)90694-2
Lewin E, Bleck V (1977) Cyclic AMP Accumulation in Cerebral Cortical Slices: Effect of Carbamazepine, Phenobarbital, and Phenytoin. Epilepsia 18:237–242. https://doi.org/10.1111/j.1528-1157.1977.tb04472.x
Lewin E, Bleck V (1981) Electroshock Seizures in Mice: Effect on Brain Adenosine and Its Metabolites. Epilepsia 22:577–581. https://doi.org/10.1111/j.1528-1157.1981.tb04129.x
Li H, Henry JL (1992) Adenosine-induced hyperpolarization is depressed by glibenclamide in rat CA1 neurones. Neuroreport 3:1113–1116
Li T, Quan Lan J, Fredholm BB et al (2007a) Adenosine dysfunction in astrogliosis: cause for seizure generation? Neuron Glia Biol 3:353–366. https://doi.org/10.1017/S1740925X0800015X
Li T, Steinbeck JA, Lusardi T et al (2007b) Suppression of kindling epileptogenesis by adenosine releasing stem cell-derived brain implants. Brain 130:1276–1288. https://doi.org/10.1093/brain/awm057
Li T, Ren G, Lusardi T et al (2008) Adenosine kinase is a target for the prediction and prevention of epileptogenesis in mice. J Clin Invest 118:571–582. https://doi.org/10.1172/JCI33737
Li T, Ren G, Kaplan DL, Boison D (2009) Human mesenchymal stem cell grafts engineered to release adenosine reduce chronic seizures in a mouse model of CA3-selective epileptogenesis. Epilepsy Res 84:238–241. https://doi.org/10.1016/j.eplepsyres.2009.01.002
Li T, Lytle N, Lan JQ et al (2012a) Local disruption of glial adenosine homeostasis in mice associates with focal electrographic seizures: A first step in epileptogenesis? Glia 60:83–95. https://doi.org/10.1002/glia.21250
Li X, Kang H, Liu X et al (2012b) Effect of adenosine A2A receptor antagonist ZM241385 on amygdala-kindled seizures and progression of amygdala kindling. J Huazhong Univ Sci Technolog Med Sci 32:257–264. https://doi.org/10.1007/s11596-012-0046-2
Li M, Kang R, Shi J et al (2013) Anticonvulsant Activity of B2, an Adenosine Analog, on Chemical Convulsant-Induced Seizures. PLoS One 8:1–10. https://doi.org/10.1371/journal.pone.0067060
Lie AA, Blümcke I, Beck H et al (1999) 5’-Nucleotidase activity indicates sites of synaptic plasticity and reactive synaptogenesis in the human brain. J Neuropathol Exp Neurol 58:451–458
Longo R, Zeng YC, Sagratella S (1995) Opposite modulation of 4-aminopyridine and hypoxic hyperexcitability by A1 and A2 adenosine receptor ligands in rat hippocampal slices. Neurosci Lett 200:21–24. https://doi.org/10.1016/0304-3940(95)12064-B
Lopes da Silva FH, Witter MP, Boeijinga PH, Lohman AH (1990) Anatomic organization and physiology of the limbic cortex. Physiol Rev 70:453–511
Löscher W (2011) Critical review of current animal models of seizures and epilepsy used in the discovery and development of new antiepileptic drugs. Seizure 20:359–368. https://doi.org/10.1016/j.seizure.2011.01.003
Löscher W, Gernert M, Heinemann U (2008) Cell and gene therapies in epilepsy - promising avenues or blind alleys? Trends Neurosci 31:62–73. https://doi.org/10.1016/j.tins.2007.11.012
Lovatt D, Xu Q, Liu W et al (2012) Neuronal adenosine release, and not astrocytic ATP release, mediates feedback inhibition of excitatory activity. Proc Natl Acad Sci 109:6265–6270. https://doi.org/10.1073/pnas.1120997109
Luan G, Wang X, Gao Q et al (2017) Upregulation of neuronal adenosine A1receptor in human Rasmussen encephalitis. J Neuropathol Exp Neurol 76:720–731. https://doi.org/10.1093/jnen/nlx053
Ma DK, Jang M-H, Guo J et al (2009) Neuronal activity-induced Gadd45b promotes epigentic DNA and adult neurogenesis. Science (80- ) 323:1070–1074
MacDonald RL, Skerritt JH, Werz MA (1986) Adenosine agonists reduce voltage-dependent calcium conductance of mouse sensory neurones in cell culture. J Physiol 370:75–90
Malhotra J, Gupta YK (1997) Effect of adenosine receptor modulation on pentylenetetrazole-induced seizures in rats. Br J Pharmacol 120:282–288. https://doi.org/10.1038/sj.bjp.0700869
Malhotra J, Seth SD, Gupta SK, Gupta YK (1996) Adenosinergic mechanisms in anticonvulsant action of diazepam and sodium valproate. Environ Toxicol Pharmacol 1:269–277. https://doi.org/10.1016/1382-6689(96)00020-8
Manzoni OJ, Manabe T, Nicoll RA (1994) Release of adenosine by activation of NMDA receptors in the hippocampus. Science 265:2098–2101
Marangos PJ, Post RM, Patel J et al (1983) Specific and potent interactions of carbamazepine with brain adenosine receptors. Eur J Pharmacol 93:175–182. https://doi.org/10.1016/0014-2999(83)90135-8
Marangos PJ, Weiss SRB, Montgomery P et al (1985) Chronic Carbamazepine Treatment Increases Brain Adenosine Receptors. Epilepsia 26:493–498. https://doi.org/10.1111/j.1528-1157.1985.tb05686.x
Marcoli M, Raiteri L, Bonfanti A et al (2003) Sensitivity to selective adenosine A1 and A2A receptor antagonists of the release of glutamate induced by ischemia in rat cerebrocortical slices. Neuropharmacology 45:201–210. https://doi.org/10.1016/S0028-3908(03)00156-4
Mareš P (2010) Anticonvulsant action of 2-chloroadenosine against pentetrazol-induced seizures in immature rats is due to activation of A1 adenosine receptors. J Neural Transm 117:1269–1277. https://doi.org/10.1007/s00702-010-0465-9
Masino SA, Geiger JD (2008) Are purines mediators of the anticonvulsant/neuroprotective effects of ketogenic diets? Trends Neurosci 31:273–278. https://doi.org/10.1016/j.tins.2008.02.009
Masino SA, Geiger JD (2009) The ketogenic diet and epilepsy: Is adenosine the missing link? Epilepsia 50:332–333. https://doi.org/10.1111/j.1528-1167.2008.01771.x
Masino SA, Li T, Theofilas P et al (2011) A ketogenic diet suppresses seizures in mice through adenosine A3 receptors. J Clin Invest 121:2679–2683. https://doi.org/10.1172/JCI57813
Masino SA, Kawamura M, Ruskin DN et al (2012) Purines and neuronal excitability: Links to the ketogenic diet. Epilepsy Res 100:229–238. https://doi.org/10.1016/j.eplepsyres.2011.07.014
Masino SA, Kawamura M, Ruskin DN (2014) Adenosine receptors and epilepsy. Current evidence and future potential. In: Adenosine Receptors in Neurology and Psychiatry, 1st edn. Elsevier Inc., United Kindom, p 233–255
Massey CA, Sowers LP, Dlouhy BJ, Richerson GB (2014) Mechanisms of sudden unexpected death in epilepsy: The pathway to prevention. Nat Rev Neurol 10:271–282. https://doi.org/10.1038/nrneurol.2014.64
Melani A, Pantoni L, Bordoni F et al (2003) The selective A2A receptor antagonist SCH 58261 reduces striatal transmitter outflow, turning behavior and ischemic brain damage induced by permanent focal ischemia in the rat. Brain Res 959:243–250. https://doi.org/10.1016/S0006-8993(02)03753-8
Miller-Delaney SFC, Bryan K, Das S et al (2015) Differential DNA methylation profiles of coding and non-coding genes define hippocampal sclerosis in human temporal lobe epilepsy. Brain 138:616–631. https://doi.org/10.1093/brain/awu373
Mirnajafi-Zadeh J, Pourgholami MH, Palizvan MR et al (1999) Anticonvulsant action of 2-chloroadenosine injected focally into the perirhinal cortex in amygdaloid kindled rats. Epilepsy Res 37:37–43. https://doi.org/10.1016/S0920-1211(99)00025-X
Mirnajafi-Zadeh J, Fathollahi Y, Pourgholami MH (2000) Intraperitoneal and intraamygdala N6-cyclohexyladenosine suppress hippocampal kindled seizures in rats. Brain Res 858:48–54. https://doi.org/10.1016/S0006-8993(99)02425-7
Mohammad-Zadeh M, Amini A, Mirnajafi-Zadeh J, Fathollahi Y (2005) The role of adenosine A1 receptors in the interaction between amygdala and entorhinal cortex of kindled rats. Epilepsy Res 65:1–9. https://doi.org/10.1016/j.eplepsyres.2005.03.012
Morrisett RA, Jope RS, Snead OC (1987) Effects of drugs on the initiation and maintenance of status epilepticus induced by administration of pilocarpine to lithium-pretreated rats. Exp Neurol 97:193–200. https://doi.org/10.1016/0014-4886(87)90293-7
Moschovos C, Kostopoulos G, Papatheodoropoulos C (2012) Endogenous adenosine induces NMDA receptor-independent persistent epileptiform discharges in dorsal and ventral hippocampus via activation of A2 receptors. Epilepsy Res 100:157–167. https://doi.org/10.1016/j.eplepsyres.2012.02.012
Muzzi M, Coppi E, Pugliese AM, Chiarugi A (2013) Anticonvulsant effect of AMP by direct activation of adenosine A1 receptor. Exp Neurol 250:189–193. https://doi.org/10.1016/j.expneurol.2013.09.010
Nagy AK, Houser CR, Delgado-Escueta AV (1990) Synaptosomal ATPase activities in temporal cortex and hippocampal formation of humans with focal epilepsy. Brain Res 529:192–201
Narimatsu E, Aoki M (1999) Involvement of the adenosine neuromodulatory system in the benzodiazepine-induced depression of excitatory synaptic transmissions in rat hippocampal neurons in vitro. Neurosci Res 33:57–64. https://doi.org/10.1016/S0168-0102(98)00110-2
Neal EG, Chaffe H, Schwartz RH et al (2008) The ketogenic diet for the treatment of childhood epilepsy: a randomised controlled trial. Lancet Neurol 7:500–506. https://doi.org/10.1016/S1474-4422(08)70092-9
Newman M, Zohar J, Kalian M, Belmaker RH (1984) The effects of chronic lithium and ECT on A1 and A2 adenosine receptor systems in rat brain. Brain Res 291:188–192. https://doi.org/10.1016/0006-8993(84)90670-X
Niemand D, Martinell S, Arvidsson S et al (1984) Aminophylline inhibition of diazepam sedation: is adenosine blockade of GABA-receptors the mechanism? Lancet (London, England) 1:463–464
Niemand D, Martinell S, Arvidsson S et al (1986) Adenosine in the inhibition of diazepam sedation by aminophylline. Acta Anaesthesiol Scand 30:493–495
Nilsen KE, Cock HR (2004) Focal treatment for refractory epilepsy: Hope for the future? Brain Res Rev 44:141–153. https://doi.org/10.1016/j.brainresrev.2003.11.003
Nowak L, Bregestovski P, Ascher P et al (1984) Magnesium gates glutamate-activated channels in mouse central neurones. Nature 307:462–465. https://doi.org/10.1038/307462a0
O’Shaughnessy CT, Aram JA, Lodge D (1988) A1 adenosine receptor-mediated block of epileptiform activity induced in zero magnesium in rat neocortex in vitro. Epilepsy Res 2:294–301. https://doi.org/10.1016/0920-1211(88)90037-X
Ochiishi T, Takita M, Ikemoto M et al (1999) Immunohistochemical analysis on the role of adenosine A1 receptors in epilepsy. Neuroreport 10:3535–3541
Orr AG, Hsiao EC, Wang MM et al (2015) Astrocytic adenosine receptor A2A and Gs-coupled signaling regulate memory. Nat Neurosci 18:1–17. https://doi.org/10.1038/nn.3930
Ortiz F, Gutiérrez R (2015) Entorhinal cortex lesions result in adenosine-sensitive high frequency oscillations in the hippocampus. Exp Neurol 271:319–328. https://doi.org/10.1016/j.expneurol.2015.06.009
Pagonopoulou O, Angelatou F (1998) Time development and regional distribution of [3H]nitrobenzylthioinosine adenosine uptake site binding in the mouse brain after acute pentylenetetrazol-induced seizures. J Neurosci Res 53:433–442. https://doi.org/10.1002/(SICI)1097-4547(19980815)53:4<433::AID-JNR5>3.0.CO;2-7
Pagonopoulou O, Angelatou F, Kostopoulos G (1993) Effect of pentylenetetrazol-induced seizures on A1 adenosine receptor regional density in the mouse brain: a quantitative autoradiographic study. Neuroscience 56:711–716
Pascual O, Casper KB, Kubera C et al (2005) Astrocytic purinergic signaling coordinates synaptic networks. Science 310:113–116. https://doi.org/10.1126/science.1116916
Payne NE, Cross JH, Sander JW, Sisodiya SM (2011) The ketogenic and related diets in adolescents and adults--a review. Epilepsia 52:1941–1948. https://doi.org/10.1111/j.1528-1167.2011.03287.x
Petersen EN (1991) Selective protection by adenosine receptor agonists against DMCM-induced seizures. Eur J Pharmacol 195:261–265
Phillis JW (1984) Interactions of the anticonvulsants diphenylhydantoin and carbamazepine with adenosine on cerebral cortical neurons. Epilepsia 25:765–772
Phillis JW, Kostopoulos GK (1975) Adenosine as a putative transmitter in the cerebral cortex. Studies with potentiators and antagonists. Life Sci 17:1085–1094
Phillis JW, Wu PH (1982) The effect of various centrally active drugs on adenosine uptake by the central nervous system. Comp Biochem Physiol Part C, Comp 72:179–187. https://doi.org/10.1016/0306-4492(82)90082-X
Phillis JW, Kostopoulos GK, Limacher JJ (1974) Depression of corticospinal cells by various purines and pyrimidines. Can J Physiol Pharmacol 52:1226–1229
Pometlová M, Kubová H, Mareš P (2010) Effects of 2-chloroadenosine on cortical epileptic afterdischarges in immature rats. Pharmacol Reports 62:62–67. https://doi.org/10.1016/S1734-1140(10)70243-7
Popoli P, Pintor A, Domenici MR et al (2002) Blockade of striatal adenosine A2A receptor reduces, through a presynaptic mechanism, quinolinic acid-induced excitotoxicity: possible relevance to neuroprotective interventions in neurodegenerative diseases of the striatum. J Neurosci 22:1967–1975 doi: 22/5/1967 [pii]
Porkka-Heiskanen T, Strecker RE, Thakkar M et al (1997) Adenosine: a mediator of the sleep-inducing effects of prolonged wakefulness. Science 276:1265–1268
Pourgholami MH, Mirnajafi-Zadeh J, Behzadi J (1997a) Effect of intraperitoneal and intrahippocampal (CA1) 2-chloroadenosine in amygdaloid kindled rats. Brain Res 751:259–264. https://doi.org/10.1016/S0006-8993(96)01406-0
Pourgholami MH, Rostampour M, Mirnajafi-Zadeh J, Palizvan MR (1997b) Intra-amygdala infusion of 2-chloroadenosine suppresses amygdala-kindled seizures. Brain Res 775:37–42
Prince DA, Stevens CF (1992) Adenosine decreases neurotransmitter release at central synapses. Proc Natl Acad Sci U S A 89:8586–8590. https://doi.org/10.1073/pnas.89.18.8586
Psarropoulou C, Matsokis N, Angelatou F, Kostopoulos G (1994) Pentylenetetrazol-induced seizures decrease gamma-aminobutyric acid-mediated recurrent inhibition and enhance adenosine- mediated depression. Epilepsia 35:12–19
Pull I, McIlwain H (1972) Metabolism of ( 14 C)adenine and derivatives by cerebral tissues, superfused and electrically stimulated. Biochem J 126:965–973
Raimondo JV, Heinemann U, de Curtis M et al (2017) Methodological standards for in vitro models of epilepsy and epileptic seizures. A TASK1-WG4 report of the AES/ILAE Translational Task Force of the ILAE. Epilepsia 58:40–52. https://doi.org/10.1111/epi.13901
Rebola N, Coelho JE, Costenla AR et al (2003) Decrease of adenosine A1 receptor density and of adenosine neuromodulation the hippocampus of kindled rats. Eur J Neurosci 18:820–828. https://doi.org/10.1046/j.1460-9568.2003.02815.x
Rebola N, Porciúncula LO, Lopes LV et al (2005) Long-term effect of convulsive behavior on the density of adenosine A1 and A 2A receptors in the rat cerebral cortex. Epilepsia 46(Suppl 5):159–165. https://doi.org/10.1111/j.1528-1167.2005.01026.x
Ren G, Li T, Lan JQ et al (2007) Lentiviral RNAi-induced downregulation of adenosine kinase in human mesenchymal stem cell grafts: A novel perspective for seizure control. Exp Neurol 208:26–37. https://doi.org/10.1016/j.expneurol.2007.07.016
Rezvani ME, Mirnajafi-Zadeh J, Fathollahi Y, Palizvan MR (2007a) Anticonvulsant effect of A1 but not A2A adenosine receptors of piriform cortex in amygdala-kindled rats. Can J Physiol Pharmacol 85:606–612. https://doi.org/10.1139/y07-046
Rezvani ME, Mirnajafi-Zadeh J, Fathollahi Y, Palizvan MR (2007b) Changes in neuromodulatory effect of adenosine A1 receptors on piriform cortex field potentials in amygdala kindled rats. Eur J Pharmacol 565:60–67. https://doi.org/10.1016/j.ejphar.2007.02.010
Rice AC, Delorenzo RJ (1998) NMDA receptor activation during status epilepticus is required for the development of epilepsy. Brain Res 782:240–247. https://doi.org/10.1016/S0006-8993(97)01285-7
Richerson GB, Boison D, Faingold CL, Ryvlin P (2016) From unwitnessed fatality to witnessed rescue: Pharmacologic intervention in sudden unexpected death in epilepsy. Epilepsia 57:35–45. https://doi.org/10.1111/epi.13236
Robledo P, Ursu G, Mahy N (1999) Effects of adenosine and gamma-aminobutyric acid A receptor antagonists on N-methyl-D-aspartate induced neurotoxicity in the rat hippocampus. Hippocampus 9:527–533. https://doi.org/10.1002/(SICI)1098-1063(1999)9:5<527::AID-HIPO6>3.0.CO;2-U
Rogawski MA, Löscher W, Rho JM (2016) Mechanisms of action of Antiseizure Drugs and the Ketogenic diet. Cold Spring Harb Perspect Med 6:28. https://doi.org/10.1101/cshperspect.a022780
Rombo DM, Newton K, Nissen W et al (2015) Synaptic mechanisms of adenosine A2A receptor-mediated hyperexcitability in the hippocampus. Hippocampus 25:566–580. https://doi.org/10.1002/hipo.22392
Rombo DM, Dias RB, Duarte ST et al (2016a) Adenosine A1 Receptor Suppresses Tonic GABAA Receptor Currents in Hippocampal Pyramidal Cells and in a Defined Subpopulation of Interneurons. Cereb Cortex 26:1081–1095. https://doi.org/10.1093/cercor/bhu288
Rombo DM, Ribeiro JA, Sebastião AM (2016b) Hippocampal GABAergic transmission: a new target for adenosine control of excitability. J Neurochem 139:1056–1070. https://doi.org/10.1111/jnc.13872
Rosen JB, Berman RF (1987) Differential Effects of Adenosine Analogs on Amygdala, Hippocampus, and Caudate Nucleus Kindled Seizures. Epilepsia 28:658–666. https://doi.org/10.1111/j.1528-1157.1987.tb03697.x
Roseti C, Martinello K, Fucile S et al (2008) Adenosine receptor antagonists alter the stability of human epileptic GABAA receptors. Proc Natl Acad Sci U S A 105:15118–15123. https://doi.org/10.1073/pnas.0807277105
Roseti C, Palma E, Martinello K et al (2009) Blockage of A2A and A3 adenosine receptors decreases the desensitization of human GABA(A) receptors microtransplanted to Xenopus oocytes. Proc Natl Acad Sci U S A 106:15927–15931. https://doi.org/10.1073/pnas.0907324106
Sandau US, Colino-Oliveira M, Jones A et al (2016) Adenosine Kinase Deficiency in the Brain Results in Maladaptive Synaptic Plasticity. J Neurosci 36:12117–12128. https://doi.org/10.1523/JNEUROSCI.2146-16.2016
Sander JW, Shorvon SD (1996) Epidemiology of the epilepsies. J Neurol Neurosurg Psychiatry 61:433–443. https://doi.org/10.1136/jnnp.61.5.433
Sato M, Racine RJ, McIntyre DC (1990) Kindling: basic mechanisms and clinical validity. Electroencephalogr Clin Neurophysiol 76:459–472. https://doi.org/10.1016/0013-4694(90)90099-6
Saura J, Angulo E, Ejarque A et al (2005) Adenosine A2A receptor stimulation potentiates nitric oxide release by activated microglia. J Neurochem 95:919–929. https://doi.org/10.1111/j.1471-4159.2005.03395.x
Scanziani M, Capogna M, Gähwiler BH, Thompson SM (1992) Presynaptic inhibition of miniature excitatory synaptic currents by baclofen and adenosine in the hippocampus. Neuron 9:919–927
Scheffer IE, Berkovic S, Capovilla G et al (2017) ILAE classification of the epilepsies: Position paper of the ILAE Commission for Classification and Terminology. Epilepsia 58:512–521. https://doi.org/10.1111/epi.13709
Schindler CW, Karcz-Kubicha M, Thorndike EB et al (2005) Role of central and peripheral adenosine receptors in the cardiovascular responses to intraperitoneal injections of adenosine A 1 and A 2A subtype receptor agonists. Br J Pharmacol 144:642–650. https://doi.org/10.1038/sj.bjp.0706043
Schoen SW, Ebert U, Löscher W (1999) 5’-Nucleotidase activity of mossy fibers in the dentate gyrus of normal and epileptic rats. Neuroscience 93:519–526. https://doi.org/10.1016/S0306-4522(99)00135-9
Scholfield CN (1978) Depression of evoked potentials in brain slices by adenosine compounds. Br J Pharmacol 63:239–244. https://doi.org/10.1111/j.1476-5381.1978.tb09752.x
Scholz KP, Miller RJ (1992) Inhibition of quantal transmitter release in the absence of calcium influx by a G protein-linked adenosine receptor at hippocampal synapses. Neuron 8:1139–1150
Schrader J, Wahl M, Kuschinsky W, Kreutzberg GN (1980) Increase of adenosine content in cerebral cortex of the rat during bicuculline-induced seizures. Pfluegers Arch 387:245–251
Schrader J, Schütz W, Bardenheuer H (1981) Role of S-adenosylhomocysteine hydrolase in adenosine metabolism in mammalian heart. Biochem J 196:65–70
Schubert P, Mitzdorf U (1979) Analysis and quantitative evaluation of the depressive effect of adenosine on evoked potentials in hippocampal slices. Brain Res 172:186–190
Schubert P, Heinemann U, Kolb R (1986) Differential effect of adenosine on pre- and postsynaptic calcium fluxes. Brain Res 376:382–386
Schultz V, Lowenstein JM (1978) The purine nucleotide cycle. Studies of ammonia production and interconversions of adenine and hypoxanthine nucleotides and nucleosides by rat brain in situ. J Biol Chem 253:1938–1943
Sebastião AM, Ribeiro JA (2009) Adenosine receptors in health and disease. Springer Berlin Heidelberg, Berlin/Heidelberg
Sebastião AM, Rombo DM, Ribeiro JA (2015) Adenosinergic receptor modulation of GABAergic transmission. In: Adenosine Signaling Mechanisms: Pharmacology, Functions and Therapeutic Aspects. Ramkunmar V, Paes de Carvalho R (editors). Nova Science Publishers, United States.
Seifert G, Carmignoto G, Steinhäuser C (2010) Astrocyte dysfunction in epilepsy. Brain Res Rev 63:212–221. https://doi.org/10.1016/j.brainresrev.2009.10.004
Shahabi P, Mirnajafi-Zadeh J, Fathollahi Y et al (2006) Amygdala adenosine A1 receptors have no anticonvulsant effect on piriform cortex-kindled seizures in rat. Can J Physiol Pharmacol 84. https://doi.org/10.1139/Y06-041
Shen HY, Li T, Boison D (2010) A novel mouse model for sudden unexpected death in epilepsy (SUDEP): Role of impaired adenosine clearance. Epilepsia 51:465–468. https://doi.org/10.1111/j.1528-1167.2009.02248.x
Shinohara M, Saitoh M, Nishizawa D et al (2013) ADORA2A polymorphism predisposes children to encephalopathy with febrile status epilepticus. Neurology 80:1571–1576. https://doi.org/10.1212/WNL.0b013e31828f18d8
Skeritt JH, Davies LP, Johnston GA (1982) A purinergic component in the anticonvulsant action of carbamazepine? Eur J Pharmacol 82:195–197
Skerritt JH, Davies LP, Johnston GAR (1983) Interactions of the anticonvulsant carbamazepine with adenosine receptors. 1. Neurochemical studies. Epilepsia 24:634–642. https://doi.org/10.1111/j.1528-1157.1983.tb03429.x
Skolnick P, Lock KL, Paul SM et al (1980) Increased benzodiazepine receptor number elicited in vitro by a novel purine, EMD 28422. Eur J Pharmacol 67:179–186
Staley KJ, Soldo BL, Proctor WR (1995) Ionic mechanisms of neuronal excitation by inhibitory GABAA receptors. Science 269:977–981. https://doi.org/10.1126/science.7638623
Stella L, Berrino L, Maione S et al (1993) Cardiovascular effects of adenosine and its analogs in anaesthetized rats. Life Sci 53:755–763. https://doi.org/10.1016/0024-3205(93)90497-Q
Studer FE, Fedele DE, Marowsky A et al (2006) Shift of adenosine kinase expression from neurons to astrocytes during postnatal development suggests dual functionality of the enzyme. Neuroscience 142:125–137. https://doi.org/10.1016/j.neuroscience.2006.06.016
Szybala C, Pritchard EM, Lusardi T et al (2009) Antiepileptic effects of silk-polymer based adenosine release in kindled rats. Exp Neurol 219:126–135. https://doi.org/10.1016/j.expneurol.2009.05.018
Tchekalarova J, Sotiriou E, Georgiev V et al (2005) Up-regulation of adenosine A1 receptor binding in pentylenetetrazol kindling in mice: Effects of angiotensin IV. Brain Res 1032:94–103. https://doi.org/10.1016/j.brainres.2004.11.004
Theofilas P, Brar S, Stewart KA et al (2011) Adenosine kinase as a target for therapeutic antisense strategies in epilepsy. Epilepsia 52:589–601. https://doi.org/10.1111/j.1528-1167.2010.02947.x
Thompson SM, Gähwiler BH (1989) Activity-dependent disinhibition. I. Repetitive stimulation reduces IPSP driving force and conductance in the hippocampus in vitro. J Neurophysiol 61:501–511
Thümmler S, Dunwiddie TV (2000) Adenosine receptor antagonists induce persistent bursting in the rat hippocampal CA3 region via an NMDA receptor-dependent mechanism. J Neurophysiol 83:1787–1795
Tosh DK, Paoletta S, Deflorian F et al (2012) Structural sweet spot for A1 adenosine receptor activation by truncated (N)-methanocarba nucleosides: receptor docking and potent anticonvulsant activity. J Med Chem 55:8075–8090. https://doi.org/10.1021/jm300965a
Trussell LO, Jackson MB (1987) Dependence of an adenosine-activated potassium current on a GTP-binding protein in mammalian central neurons. J Neurosci 7:3306–3316
Turski WA, Cavalheiro EA, Ikonomidou C et al (1985) Effects of aminophylline and 2-chloroadenosine on seizures produced by pilocarpine in rats: Morphological and electroencephalographic correlates. Brain Res 361:309–323. https://doi.org/10.1016/0006-8993(85)91302-2
Uthman BM (2000) Vagus nerve stimulation therapy for seizures. Arch Med Res 31:300–303. https://doi.org/10.1097/ANA.0b013e31815b7df1
Uzbay TI, Kayir H, Ceyhan M (2007) Effects of tianeptine on onset time of pentylenetetrazole-induced seizures in mice: Possible role of adenosine A1 receptors. Neuropsychopharmacology 32:412–416. https://doi.org/10.1038/sj.npp.1301143
Van Gompel JJ, Bower MR, Worrell GA et al (2014) Increased cortical extracellular adenosine correlates with seizure termination. Epilepsia 55:233–244. https://doi.org/10.1111/epi.12511
van Vliet EA, Aronica E, Vezzani A, Ravizza T (2018) Review: Neuroinflammatory pathways as treatment targets and biomarker candidates in epilepsy: emerging evidence from preclinical and clinical studies. Neuropathol Appl Neurobiol 44:91–111. https://doi.org/10.1111/nan.12444
Vandam RJ, Shields EJ, Kelty JD (2008) Rhythm generation by the pre-Bötzinger complex in medullary slice and island preparations: effects of adenosine A(1) receptor activation. BMC Neurosci 9:95. https://doi.org/10.1186/1471-2202-9-95
Vanore G, Giraldez L, Rodríguez de Lores Arnaiz G, Girardi E (2001) Seizure activity produces differential changes in adenosine A1 receptors within rat hippocampus. Neurochem Res 26:225–230. https://doi.org/10.1023/A:1010912516299
Vezzani A, Fujinami RS, White HS et al (2016) Infections, inflammation and epilepsy. Acta Neuropathol 131:211–234. https://doi.org/10.1007/s00401-015-1481-1485
Vianna EPM, Ferreira AT, Doná F et al (2005) Modulation of seizures and synaptic plasticity by adenosinergic receptors in an experimental model of temporal lobe epilepsy induced by pilocarpine in rats. Epilepsia 46(Suppl 5):166–173. https://doi.org/10.1111/j.1528-1167.2005.01027.x
Von Lubitz DK, Paul IA, Carter M, Jacobson KA (1993) Effects of N6-cyclopentyl adenosine and 8-cyclopentyl-1,3-dipropylxanthine on N-methyl-D-aspartate induced seizures in mice. Eur J Pharmacol 249:265–270
Von Lubitz DK, Lin RC, Popik P et al (1994a) Adenosine A3 receptor stimulation and cerebral ischemia. Eur J Pharmacol 263:59–67. https://doi.org/10.1016/0014-2999(94)90523-1
Von Lubitz DK, Paul IA, Ji XD et al (1994b) Chronic adenosine A1 receptor agonist and antagonist: effect on receptor density and N-methyl-D-aspartate induced seizures in mice. EurJPharmacol 253:95–99. https://doi.org/10.1016/j.surg.2006.10.010.Use
Von Lubitz DK, Carter MF, Deutsch SI et al (1995a) The effects of adenosine A3 receptor stimulation on seizures in mice. Eur J Pharmacol 275:23–29. https://doi.org/10.1016/0014-2999(94)00734-O
Von Lubitz DKJE, Kim J, Beenhakker M et al (1995b) Chronic NMDA receptor stimulation: Therapeutic implications of its effect on adenosine A1 receptors. EurJPharmacol 283:185–192
Wang S, Kurada L, Cilz NI et al (2013) Adenosinergic Depression of Glutamatergic Transmission in the Entorhinal Cortex of Juvenile Rats via Reduction of Glutamate Release Probability and the Number of Releasable Vesicles. PLoS One 8:1–10. https://doi.org/10.1371/journal.pone.0062185
Weir RL, Padgett W, Daly JW, Anderson SM (1984) Interaction of anticonvulsant drugs with adenosine receptors in the central nervous system. Epilepsia 25:492–498
Wheless JW (2008) History of the ketogenic diet. Epilepsia 49:3–5. https://doi.org/10.1111/j.1528-1167.2008.01821.x
Whitcomb K, Lupica CR, Rosen JB, Berman RF (1990) Adenosine involvement in postictal events in amygdala-kindled rats. Epilepsy Res 6:171–179. https://doi.org/10.1016/0920-1211(90)90070-C
Wieraszko A, Seyfried TN (1989) Increased amount of extracellular ATP in stimulated hippocampal slices of seizure prone mice. Neurosci Lett 106:287–293. https://doi.org/10.1016/0304-3940(89)90178-X
Williams M, Risley EA, Huff JR (1981) Interaction of putative anxiolytic agents with central adenosine receptors. Can J Physiol Pharmacol 59:897–900. https://doi.org/10.1139/y81-136
Williams-Karnesky RL, Sandau US, Lusardi TA et al (2013) Epigenetic changes induced by adenosine augmentation therapy prevent epileptogenesis. J Clin Invest 123:3552–3563. https://doi.org/10.1172/JCI65636
Wilz A, Pritchard EM, Li T et al (2008) Silk polymer-based adenosine release: therapeutic potential for epilepsy. Biomaterials 29:3609–3616. https://doi.org/10.1016/j.biomaterials.2008.05.010
Winn HR, Welsh JE, Rubio R, Berne RM (1980) Changes in brain adenosine during bicuculline-induced seizures in rats. Effects of hypoxia and altered systemic blood pressure. Circ Res 47:568–577. https://doi.org/10.1161/01.RES.47.4.568
Wirkner K, Gerevich Z, Krause T et al (2004) Adenosine A2A receptor-induced inhibition of NMDA and GABAA receptor-mediated synaptic currents in a subpopulation of rat striatal neurons. Neuropharmacology 46:994–1007. https://doi.org/10.1016/j.neuropharm.2004.01.008
Wu LG, Saggau P (1994) Adenosine inhibits evoked synaptic transmission primarily by reducing presynaptic calcium influx in area CA1 of hippocampus. Neuron 12:1139–1148. https://doi.org/10.1016/0896-6273(94)90321-2
Yoon KW, Rothman SM (1991) Adenosine inhibits excitatory but not inhibitory synaptic transmission in the hippocampus. J Neurosci 11:1375–1380. https://doi.org/10.4161/cib.3.5.12287
Young D, Dragunow M (1994) Status epilepticus may be caused by loss of adenosine anticonvulsant mechanisms. Neuroscience 58:245–261. https://doi.org/10.1016/0306-4522(94)90032-9
Zeraati M, Mirnajafi-Zadeh J, Fathollahi Y et al (2006) Adenosine A1 and A2A receptors of hippocampal CA1 region have opposite effects on piriform cortex kindled seizures in rats. Seizure 15:41–48. https://doi.org/10.1016/j.seizure.2005.10.006
Zgodziński W, Rubaj A, Kleinrok Z, Sieklucka-Dziuba M (2001) Effect of adenosine A1 and A2 receptor stimulation on hypoxia-induced convulsions in adult mice. Pol J Pharmacol 53:83–92
Zhang G, Franklin PH, Murray TF (1993) Manipulation of endogenous adenosine in the rat prepiriform cortex modulates seizure susceptibility. J Pharmacol Exp Ther 264:1415–1424
Zhang G, Franklin PH, Murray TF (1994) Activation of adenosine A1 receptors underlies anticonvulsant effect of CGS21680. Eur J Pharmacol 255:239–243. https://doi.org/10.1016/0014-2999(94)90104-X
Zhang G, Raol YSH, Hsu F-C, Brooks-Kayal AR (2003) Long-term alterations in glutamate receptor and transporter expression following early-life seizures are associated with increased seizure susceptibility. J Neurochem 88:91–101. https://doi.org/10.1046/j.1471-4159.2003.02124.x
Zimmermann H (2000) Extracellular metabolism of ATP and other nucleotides. Naunyn Schmiedebergs Arch Pharmacol 362:299–309. https://doi.org/10.1007/s002100000309
Zimmermann H, Zebisch M, Sträter N (2012) Cellular function and molecular structure of ecto-nucleotidases. Purinergic Signal 8:437–502. https://doi.org/10.1007/s11302-012-9309-4
Zuchora B, Turski WA, Wielosz M, Urbanska EM (2001) Protective effect of adenosine receptor agonists in a new model of epilepsy--seizures evoked by mitochondrial toxin, 3-nitropropionic acid, in mice. NeurosciLett 305:91–94
Zuchora B, Wielosz M, Urbańska EM (2005) Adenosine A1 receptors and the anticonvulsant potential of drugs effective in the model of 3-nitropropionic acid-induced seizures in mice. Eur Neuropsychopharmacol 15:85–93. https://doi.org/10.1016/j.euroneuro.2004.05.006
Zwicker JD, Rajani V, Hahn LB, Funk GD (2011) Purinergic modulation of preBötzinger complex inspiratory rhythm in rodents: the interaction between ATP and adenosine. J Physiol 589:4583–4600. https://doi.org/10.1113/jphysiol.2011.210930
Acknowledgements
The research carried out by the authors of this work have been supported by LISBOA-01-0145-FEDER-007391, project co-funded by FEDER through POR Lisboa 2020 (Programa Operacional Regional de Lisboa) from PORTUGAL 2020 and Fundação para a Ciência e Tecnologia (FCT), by an FCT project (PTDC/DTP-FTO/3346/2014) and by Twinning action (SynaNet) from the EU H2020 programme (project number: 692340).
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2018 Springer Nature Switzerland AG
About this chapter

Cite this chapter
Rombo, D.M., Ribeiro, J.A., Sebastião, A.M. (2018). Role of Adenosine Receptors in Epileptic Seizures. In: Borea, P., Varani, K., Gessi, S., Merighi, S., Vincenzi, F. (eds) The Adenosine Receptors. The Receptors, vol 34. Humana Press, Cham. https://doi.org/10.1007/978-3-319-90808-3_13
Download citation
DOI: https://doi.org/10.1007/978-3-319-90808-3_13
Published:
Publisher Name: Humana Press, Cham
Print ISBN: 978-3-319-90807-6
Online ISBN: 978-3-319-90808-3
eBook Packages: Biomedical and Life SciencesBiomedical and Life Sciences (R0)