
Abstract
Radiolabeled anti-CD20 monoclonal antibody, 90Y-ibritumomab tiuxetan became available for the treatment of refractory or relapsed low-grade B-cell non-Hodgkin’s lymphoma (NHL). Although FDG-PET is widely used for monitoring the response to chemotherapy and radiotherapy, there are limited data for monitoring the response of NHL to radioimmunotherapy (RIT) with FDG-PET.
Experience in our institute We retrospectively evaluated our experience using FDG-PET/CT for monitoring the response of NHL to RIT. Methods A total of 34 patients received 90Y-ibritumomab tiuxetan and underwent FDG-PET/CT scans before and at 3 months after RIT. Subsequent scans were performed at 7–12 months and at 12–24 months after RIT. PET/CT scans after additional treatment with clinical evidence of relapse after RIT was excluded from analysis; all patients did not receive additional treatment during the evaluating period. Tumor metabolic activity was assessed before and after RIT visually on PET/CT images and compared with the treatment effect and clinical course. Results According to the revised IWC criteria, the maximal response was CR in 22 patients, PR in 5 patients, and PD in 1 patient (1 patient not evaluable). FDG-PET was positive in 10 patients before RIT, 5 patients at 3 months, 5 patients at 7–12 months, and 1 patient at 13 months after RIT. Among 18 patients with negative PET results at 3 months after RIT, only one patient relapsed later. In 2 patients, although PET was positive at 3 months after RIT, abnormal accumulation diminished at 7–9 months after RIT without further treatment.
Conclusions FDG-PET/CT is a useful noninvasive imaging modality for monitoring the response of NHL to RIT. Negative PET finding at 3 months after RIT predicts the treatment effects with high probability. However, positive PET results at 3 months after RIT does not warrant immediate additional therapy because the metabolic response to RIT can be gradual, with continued declines of FDG uptake occurring between 7 and 9 months after RIT without additional therapy.
Access provided by CONRICYT-eBooks. Download chapter PDF
Similar content being viewed by others


Keywords
- B-cell non-Hodgkin’s lymphoma
- Follicular lymphoma
- Mantle cell lymphoma
- 90Y-ibritumomab tiuxetan
- 111In-ibritumomab tiuxetan
- Revised IWC criteria
- FDG
- PET
- Metabolic response
- Expected biodistribution
- Altered biodistribution
1 Introduction
Many therapeutic regimens for B-cell lymphomas include the chimeric anti-CD20 monoclonal antibody rituximab, in combination with chemotherapy or alone. Radiolabeled anti-CD20 monoclonal antibody, 90Y-ibritumomab tiuxetan, as well as 131I-tositumomab, became available for the treatment of refractory or relapsed low-grade B-cell non-Hodgkin’s lymphoma (NHL) as shown in the previous chapters.
FDG-PET is known as a noninvasive imaging modality for disease staging, restaging, and monitoring response of lymphoma to chemotherapy and radiotherapy. Multiple studies have shown that FDG-PET is superior to anatomic imaging for detecting active disease after therapy [1,2,3].
Although FDG-PET is widely used for monitoring the response to chemotherapy and radiotherapy , there are limited data for monitoring the response of NHL to radioimmunotherapy (RIT) with FDG-PET.
2 Evaluation of FDG-PET/CT for Monitoring the Response to RIT
Here we present our experience (in Kurashiki Central Hospital, Kurashiki, Japan) of the evaluation of FDG-PET/CT for monitoring the response of NHL to RIT retrospectively.
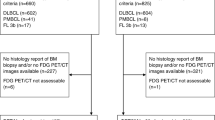
A total of 34 clinical patients with relapsed or refractory low-grade B-cell lymphoma who underwent RIT using Y-90-labeled antibody were enrolled in our study (Figs. 1 and 2).

(Relapsed case). A 72-year-old female patient with history of follicular lymphoma (grade 3a). She underwent chemotherapy of eight courses of R-THP-COP prior to RIT. FDG-PET images before chemotherapy (a) showed multiple FDG-avid nodules in the neck, axilla, spleen, and abdomen before chemotherapy. After chemotherapy (b), most of FDG-avid lesions disappeared, while some uptake was still seen in the neck and in the abdomen. At 3 months after RIT (c), increased FDG uptake was seen in the neck. At 5 months after RIT, the lymph nodes enlarged and biopsy showed relapse of lymphoma. Afterward she received additional chemotherapy


(Late responder). A 63-year-old male patient with follicular lymphoma (grade 3). He underwent chemotherapy of R-CHOPx5, DeVICx5, and THP-COPx1 prior to RIT. FDG-PET images before RIT (a) (d) showed weak FDG accumulation in the mesenteric lymph nodes suggestive of residual lymphoma. At 3 months after RIT (b) (e), FDG uptake in the abdominal lesion increased. However, the uptake disappeared without additional treatment at 9 months after RIT (c) (f). The patient achieved CR and did not relapse during the follow-up period, suggestive of transient increase of FDG uptake at 3 months after RIT
The patient characteristics are shown in Table 1. Twenty-four patients had follicular lymphoma , while four patients had MALT lymphoma and mantle cell lymphoma . One patient had marginal zone B-cell lymphoma and low-grade B-cell lymphoma not otherwise specified.
All patients received three regimens of chemotherapy before RIT on average (range 1–6).
The dose of yttrium-90-labeled antibody for RIT was defined based on the platelet count as follows:
Plt ≧ 150,000/μl: | 14.8(MBq/kg) | 22 patients |
Plt 100,000–150,000/μl: | 11.1(MBq/kg) | 12 patients |
Whole-body imaging using indium-labeled antibody was routinely performed 1 week before therapy in all patients to exclude patients with improper distribution of antibody from RIT. However, no patient was excluded from RIT based on the imaging findings.
Yttrium-90-labeled antibody was injected shortly (approx. 1 h) after rituximab pretreatment.
2.1 FDG-PET/CT Imaging
A dedicated PET/CT scanner (Aquiduo, Toshiba Medical Systems, Otawara, Japan) was used. After fasting for at least 5 h, each patient received an IV injection of FDG (FDGscan inj., Nihon-Mediphysics, Tokyo Japan). A whole-body PET emission scan was performed 60 min after administration of FDG with our routine protocol. CT images were acquired immediately before the PET scan without the use of contrast media.
Tumor metabolic activity was assessed before and after RIT visually on PET/CT images as positive, negative, or inconclusive. PET/CT findings were compared with the treatment effect and clinical course. The maximal treatment response was assessed based on the revised IWC criteria and classified as complete response (CR), partial response (PR), stable disease (SD), and progressive disease (PD) [4].
PET/CT scans after additional treatment with clinical evidence of relapse after RIT were excluded from analysis ; all patients did not receive additional treatment during the evaluating period.
3 Summary of the Results
The maximal response in all 34 patients during the follow-up period of 91–796 days (median, 420 days) was shown in Table 2. No assessment was available in 1 patient. Four patients relapsed in the study group during the follow-up period.
The overall PET findings before and after RIT are summarized in Table 3. Before RIT, 11 patients were PET positive, while 17 patients were PET negative. After RIT, the number of PET-positive patients decreased by time.
The results of patient subgroups based on PET findings are shown in Tables 4, 5, 6, and 7.
Table 4 shows PET-positive results in 11 patients before RIT. After RIT, FDG-PET became negative in three patients, while the other patients became inconclusive or remained PET positive. Although the response rate was high, three patients relapsed during the follow-up period.
Table 5 shows PET-negative results in 17 patients before RIT. Although almost all patients had PET-positive disease initially, these patients became PET-negative after chemotherapy before RIT. After RIT, FDG-PET remained negative in the majority of patients. Sixteen patients achieved CR and no patient relapsed.
Table 6 shows the results of the 6 patients with PET-positive findings at 3 months after RIT. FDG-PET became negative in some patients at subsequent PET scans after 6 months, while some other patients remained PET positive, including 3 relapsed patients.
Table 7 shows PET-negative results in 20 patients at 3 months after RIT. All patients achieved CR and no patient relapsed in this subgroup. In the follow-up PET scans, FDG-PET remained negative in the majority of patients.
4 Discussion
FDG-PET/CT is a useful noninvasive imaging technique for monitoring the response of lymphoma to therapy. The response of a tumor to treatment was conventionally evaluated by measuring the tumor size using morphological imaging modalities such as CT and MRI. The determination of treatment response in patients with non-Hodgkin’s lymphoma is complicated, and criteria proposed by a National Cancer Institute–sponsored international workshop have been used as a standard system of classification [5]. This system defines categories of complete response, complete response–unconfirmed, partial response, stable disease, and progressive disease. Complete response requires disappearance of all disease at physical examination, normalization of lactate dehydrogenase levels, and CT findings that show that all lymph nodes and nodal masses have regressed to normal size. Partial response requires a greater than 50% decrease in mass size.
However, distinguishing viable residual tumors from fibrotic scars after irradiation is difficult. It is known that FDG-PET can distinguish viable lymphoma from fibrotic change after treatment because most non-Hodgkin’s lymphomas are FDG-avid [6,7,8,9,10], and FDG-PET is superior to CT for the assessment of recurrent lymphoma after chemotherapy [11]. Recently, revised criteria for the assessment of lymphoma treatment response were published [4, 12]. We used these criteria for assessment of treatment response of RIT in the present study.
After radioimmunotherapy, Jacene et al. reported FDG uptake in tumors typically dropped significantly and a continued decline in tumor SUVlean max between 12 and 24 weeks without additional therapy can occur, suggesting a need for delayed-response assessment. The information provided by combined 18F-FDG-PET/CT is informative for monitoring the response of lymphoma to radioimmunotherapy [13].
Ulaner et al. reported on 10 patients with refractory or relapsed NHL who underwent 18F-FDG-PET/CT for restaging 4–6 months after 90Y-ibritumomab tiuxetan, and the results were similar [10]. The use of combined FDG-PET/CT may enable superior assessment of response to 90Y-ibritumomab tiuxetan treatment than the use of CT alone, at which one may underestimate 90Y-ibritumomab tiuxetan response by considering inactive residual CT masses to be residual disease.
In another previous report, early assessment of response to RIT by using PET/CT (at 2 months after RIT) might be useful in the identification of patients needing additional therapeutic strategies [14].
Hanaoka et al. reported that a significant difference in pretherapeutic FDG SUVmax was observed between responders and nonresponders and pretherapeutic FDG accumulation was predictive of the tumor response in 90Y-ibritumomab tiuxetan therapy. The results were consistent with our experience [15].
Quantitative analyses with SUV are not considered necessary to determine PET positivity. We applied IWC-PET criteria in our study to assess response to therapy, although prospective validation of quantitative criteria for determining response may prove helpful in the future, particularly in the setting of residual masses on CT.
The optimal timing to obtain a PET scan after radioimmunotherapy has not been defined. The initial studies evaluating 18F-FDG-PET for monitoring the response of lymphoma were primarily obtained after cytotoxic chemotherapy or radiotherapy. The optimal time to obtain a posttherapy PET is not completely resolved, but a minimum of 10 days after chemotherapy has been recommended, to avoid false-negative and false-positive scan findings due to early treatment effects of stunning and inflammation. Longer and more variable times after external-beam radiation have been suggested. According to our results and literatures, a longer delay to initial response assessment might allow more accurate assessment of a slow responder. Although long delay might not be acceptable in nonresponding patients, the potential benefit from earlier detection of disease and further treatment might not always be critical because the progression of most indolent lymphoma for RIT indication is gradual.
The mechanism of transient increase of FDG accumulation after RIT in our study is not clarified. FDG is not a cancer-specific agent and is known to accumulate in cases of acute inflammation, in granulomatous diseases , and in autoimmune diseases. Under such conditions, the suggestion is that 18F-FDG is taken up by infiltrating cells such as macrophages, lymphocytes, and granulocytes [16]. In a report of lung cancer patients, FDG is accumulated in the inflammatory tissue of radiation induced pneumonitis and a temporal increase in FDG uptake at 1–2 weeks after stereotactic radiotherapy appeared to reflect the acute reaction of the tumor [17]. The exact mechanism of death of lymphoma cells after RIT is unknown, but it is possible that a combination of a mitotic lymphoma cell death and delayed immunologic effects may contribute to the observed temporal changes of FDG accumulation.
Prior to 90Y-ibritumomab tiuxetan therapy , imaging with 111In-ibritumomab tiuxetan may be performed to verify the expected biodistribution and exclude patients who show an altered biodistribution , such as the rapid clearance of 111In-ibritumomab tiuxetan from the blood pool, with prominent liver, spleen, or marrow uptakes [15]. However, a high rate of a complete response after 90Y-ibritumomab tiuxetan therapy has often been observed in patients with negative 111In-ibritumomab tiuxetan accumulation in lesions, and accumulation of 111In-ibritumomab tiuxetan does not predict treatment effect.
5 Conclusions
In conclusion, FDG-PET/CT is a useful noninvasive imaging modality for monitoring the response of NHL to RIT. In our experience, negative PET findings before and at 3 months after RIT predict the treatment effects with high probability. However, positive PET results at 3 months after RIT do not warrant immediate additional therapy because metabolic response to RIT can be gradual, with continued declines of FDG uptake occurring between 7 and 9 months after RIT without additional therapy. The optimal condition of imaging, especially the time interval between the therapy and the FDG-PET/CT scan, is to be established by further prospective studies with a large number of patients.
Abbreviations
- 111In:
-
Indium-111
- FDG:
-
18F-fluorodeoxyglucose
- MALT:
-
Mucosa-associated lymphoid tissue
- PET:
-
Positron emission tomography
- RIT:
-
Radioimmunotherapy
References
Jerusalem G, Beguin Y, Fassotte MF, et al. Whole-body positron emission tomography using 18F-fluorodeoxyglucose for posttreatment evaluation in Hodgkin’s disease and non-Hodgkin’s lymphoma has higher diagnostic and prognostic value than classical computed tomography scan imaging. Blood. 1999;94:429–33.
Naumann R, Vaic A, Beuthien-Baumann B, et al. Prognostic value of positron emission tomography in the evaluation of post-treatment residual mass in patients with Hodgkin’s disease and non-Hodgkin’s lymphoma. Br J Haematol. 2001;115:793–800.
Spaepen K, Stroobants S, Dupont P, et al. Prognostic value of positron emission tomography (PET) with fluorine-18 fluorodeoxyglucose ([18F]FDG) after first line chemotherapy in non-Hodgkin’s lymphoma: is [18F]FDG-PET a valid alternative to conventional diagnostic methods? J Clin Oncol. 2001;19:414–9.
Cheson BD, Pfistner B, Juweid ME, et al. Revised response criteria for malignant lymphoma. J Clin Oncol. 2007;25:579–86.
Cheson BD, Horning SJ, Coiffier B, et al. Report of an international workshop to standardize response criteria for non-Hodgkin’s lymphomas. NCI sponsored international working group. J Clin Oncol. 1999;17:1244.
Conti PS, Lilien DL, Hawley K, Keppler J, Grafton ST, Bading JR. PET and [18F]-FDG in oncology: a clinical update. Nucl Med Biol. 1996;23:717–35.
Gambhir SS, Czernin J, Schwimmer J, Silverman DH, Coleman RE, Phelps ME. A tabulated summary of the FDG PET literature. J Nucl Med. 2001;42(5 Suppl):1S–93S.
Joyce JM, Degirmenci B, Jacobs S, McCook B, Avril N. FDG PET CT assessment of treatment response after yttrium-90 ibritumomab tiuxetan radioimmunotherapy. Clin Nucl Med. 2005;30:564–8.
Torizuka T, Zasadny KR, Kison PV, Rommelfanger SG, Kaminski MS, Wahl RL. Metabolic response of non-Hodgkin’s lymphoma to 131I-anti-B1 radioimmunotherapy: evaluation with FDG PET. J Nucl Med. 2000;41:999–1005.
Ulaner GA, Colletti PM, Conti PS. B-cell non-Hodgkin’s lymphoma: PET/CT evaluation after 90Y-ibritumomab tiuxetan radioimmunotherapy: initial experience. Radiology. 2008;246:895–902.
Hoekstra OS, Ossenkoppele GJ, Golding R, et al. Early treatment response in malignant lymphoma, as determined by planar fluorine-18-fluorodeoxyglucose scintigraphy. J Nucl Med. 1993;34:1706–10.
Juweid ME, Stroobants S, Hoekstra OS, et al. Use of positron emission tomography for response assessment of lymphoma: consensus of the Imaging Subcommittee of International Harmonization Project in Lymphoma. J Clin Oncol. 2007;25:571–8.
Jacene HA, et al. FDG PET/CT for monitoring the response of lymphoma to radioimmunotherapy. J Nucl Med. 2009;50:8–17.
Storto G, et al. Assessment of metabolic response to radioimmunotherapy with 90Y-ibritumomab tiuxetan in patients with relapsed or refractory B-cell non-Hodgkin lymphoma. Radiology. 2010;254(1):245–52.
Hanaoka K, Hosono M. Et aI. Heterogeneity of intratumoral (111)in-ibritumomab tiuxetan and (18)F-FDG distribution in association with therapeutic response in radioimmunotherapy for B-cell non-Hodgkin's lymphoma. EJNMMI Res. 2015;5:10. https://doi.org/10.1186/s13550-015-0093-3. eCollection 2015.
Ishimori T, Saga T, Mamede M, et al. Increased 18F-FDG uptake in a model of inflammation: concanavalin A–mediated lymphocyte activation. J Nucl Med. 2002;43:658–63.
Ishimori T, Saga T, Nagata Y, et al. 18F-FDG and 11C-methionine PET for evaluation of treatment response of lung cancer after stereotactic radiotherapy. Ann Nuc Med. 2004;18:669–74.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2018 Springer International Publishing AG, part of Springer Nature
About this chapter

Cite this chapter
Ishimori, T., Nakatani, K. (2018). Radiological Evaluation of Response and Resistance of Ibritumomab. In: Hosono, M., Chatal, JF. (eds) Resistance to Ibritumomab in Lymphoma. Resistance to Targeted Anti-Cancer Therapeutics, vol 18. Springer, Cham. https://doi.org/10.1007/978-3-319-78238-6_5
Download citation
DOI: https://doi.org/10.1007/978-3-319-78238-6_5
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-319-78237-9
Online ISBN: 978-3-319-78238-6
eBook Packages: Biomedical and Life SciencesBiomedical and Life Sciences (R0)