
Abstract
Objective Identification of best practices constitutes an important strategy for organizational improvement. We compared different criteria (different measurement thresholds, different comparators, and performance consistency over time) on identification of high-performing facilities, especially positive deviants.
Methods The design was serial cross-sectional, using yearly VHA administrative data (2009–2013). Our primary outcome measure was facility-level rate of HbA1c overtreatment of diabetes in patients at risk for hypoglycemia. Outlier status was assessed by three methods.
Results From 2009 to 2013, the rate of overtreatment overall based on a threshold of 6.5% decreased from 28.6% in 2009 to 22.7% in 2013; the rate of undertreatment increased from 7 to 10.3%. Fourteen facilities were identified in the lowest decile of overtreatment. Undertreatment rates among these facilities were compared to the mean overall undertreatment rate; several facilities identified as positive deviants based on overtreatment rates had exceptionally high rates of undertreatment.
Conclusion Because two facilities may arrive at the same results via very different pathways, it is important to consider that a best practice may actually reflect a separate worst practice.
Access provided by CONRICYT-eBooks. Download chapter PDF
Similar content being viewed by others


1 Introduction
The adoption of “best practices” constitutes an important strategy for organizational improvement [1,2,3,4]. Best practices can be sought from high-performing outliers [5,6,7]. This is the first step in using the positive deviance process, a strategy that is gaining popularity in healthcare improvement [8,9,10,11,12,13,14,15,16].
The “positive deviance approach” to social/behavior change began in the area of childhood nutrition when it was noted that within communities with high levels of childhood malnutrition, some families had well-nourished children [17, 18]. These families, referred to as positive deviants, evidenced uncommon but successful behaviors or strategies that enabled them to find better solutions to a problem than their peers, despite facing similar challenges and having no apparent extra resources or knowledge. A similar approach, termed bright spotting, has been applied in primary care to the identification of patients with diabetes at high risk of complications who have managed to maintain their health [19].
The term positive deviance has been used in different ways in management improvement and research. The concept of positive deviance has also been used to describe behavior of individuals within organizations [20,21,22,23,24]. More recently, this concept has been applied to organizations themselves, especially in healthcare. For example in systematic review, Baxter et al. identified four key themes of positive deviance:
-
1.
Positive deviants were defined as high performers
-
2.
Positive deviants demonstrated different or uncommon behaviors
-
3.
Positive deviance is a bottom-up approach
-
4.
Positive deviant solutions are sustainable within current resource [8]
Although definitions of positive deviance vary widely, the phenomenon of positive deviance is often mentioned in the context of complexity, whether complexity science , complexity theory , or complexity thinking . For example, Lindberg and Clancy identified complexity science concepts and related then to the positive deviance process in reducing the occurrence of intravenous line infections in the intensive care unit [25]. These concepts included:
-
The number and nature of relationships
-
Difference and diversity in perspective and action
-
The extent to which power is centralized or shared
-
The degree to which variability and order exist
In being attuned to the number and nature of relationships, the positive deviance process seeks to involve all whose behavior affects the problem and relies on facilitators who are skilled at nurturing open conversation and encouraging participation in small group conversation [25]. Similarly, Spindler and Wagenheim described positive deviance dynamics as “typically a ‘grassroots’ self-organising unit, within teams, organisations, networks or society yet often outside the formal structure, that has a different, even contrarian, perspective of the social system. Such deviants can be considered holons that contain all the characteristics of the whole system to which they belong yet operate with an entrepreneurial independence. This autonomy and unique perspective allows them to observe the system’s blindness and realise different solutions (p. 647)” [26]. Thus, the positive deviance approach implies the necessity of thinking that the process unfolds in the context of a complex adaptive system, in short, complexity thinking. Further exploration of the philosophical (ontological and epistemological) underpinnings of complexity thinking is beyond the scope of this paper. Readers are referred to the work of Richardson and others [27, 28].
A structured approach to employing the positive deviance process includes the definition of the problem, the identification of positive deviant individuals or teams, and the discovery of the uncommon practices or behaviors that allow the positive deviants to be successful [29]. Addressing mortality in intensive care units following myocardial infarction provides an exemplar of this approach.
Bradley et al. noted that there was marked hospital variation in ICU mortality for myocardial infarction [9, 11]. Their first step involved identification of organizations that demonstrated exceptionally high performance in this area of interest—positive deviants. In this case, there was a well-established metric for the outcome. In addition, a criterion of consistent high performance was used. This was operationalized by analyzing data from two consecutive years. They then selected hospitals that ranked in the top and bottom 5% of performance during both years. In the original work on positive deviance in public health, the comparators were required to be those with similar access to resources. In contrast, Bradley et al. selected hospitals that were diverse in areas such as the volume of patients with acute myocardial infarction, teaching status, and socioeconomic status of patients. They were seeing to identify “information rich” participants that have certain characteristics, detailed knowledge, or direct experience relevant to the phenomenon of interest. Later studies examined what the positive deviants were doing that was different from other intensive care units, and those actions were shared with others.
Many hospitals have since adopted those practices with resulting improvement in outcomes. However, despite their good results, several questions are raised about extrapolating that approach to other issues. First, in this case there was a very well-established and uniform metric, something often lacking. In addition to there being a wide range of performance metrics , how the definition is operationalized can vary greatly. Both the length of time deemed necessary to demonstrate consistency and the procedures to identify high performance vary. In contrast to Bradley et al., others have examined performance during a single 1-year period based on 99 percentile confidence limits [30]. In addition, in the latter study, the comparator was limited to other hospitals in the same, albeit very large, organizational unit. In the original work on positive deviance in childhood nutrition, performance was assessed by simple observation rather than statistical analysis [18, 29]. The difference between malnourished and well-nourished children was obvious. This may or may not be the case with organizational positive deviance. There are no agreed upon methods to determine the criteria for high performance or to define an appropriate comparator. The identification of an outlier depends on the measures and statistical methods chosen, and different methods often do not agree [7, 31,32,33,34].
Diabetes , a common chronic condition, lends itself to this type of assessment because there are well-established performance measures [35]. Many of these measures have been based on assessment of glycemic control using hemoglobin A1c (HbA1c) levels and have focused primarily on rates of inadequate or undertreatment. Recently, more attention has been paid to the increasing problem of hypoglycemia which may be an unintended consequence of overly intensive glycemic control [36,37,38,39]. Overtreatment can result from setting HbA1c targets that are inappropriately low based on patients’ life expectancy, comorbid conditions, and other factors [40,41,42,43,44]. We previously developed a measure of overtreatment [30]. The objective of our study was to determine the effect of different factors on identification of high-performing outliers—positive deviants, especially consistency of performance over time, and use of different comparators. In addition, we included a reciprocal measure, one of undertreatment . Such undertreatment could be a consequence of efforts to reduce overtreatment or the combination of high rates of undertreatment and low rates of overtreatment could reflect lack of attention to diabetes care in general.
2 Methods
2.1 Research Design and Healthcare System Under Study
The design was serial cross-sectional, using yearly Veterans Health Administration (VHA) administrative data (2009–2013) [30]. VHA provides healthcare to eligible veterans of the Armed Services in >100 hospitals and their related clinics. During the period 2009–2013, VHA was organized into 21 regional networks (Veterans Integrated Service Networks or VISNs), each consisting of 3–10 facilities. The facilities vary by size, range of services offered locally, and other factors from which is calculated a complexity level. There are 18–32 facilities in each of the 5 complexity levels.
2.2 Outcome Measures
We used our previously developed measure for overtreatment and used an HbA1c threshold of 6.5%. Overtreatment rates were calculated at the facility level as the proportion of patients in the chosen population with HbA1c<6.5%. In brief, the population at high risk for hypoglycemia (hence overtreatment) included patients taking a diabetes drug known to have a relatively high frequency of hypoglycemia (insulin and/or sulfonylurea agents) plus having at least one of the following additional criteria: age 75 years or older, chronic kidney disease (defined as last serum creatinine measurement in a year greater than 2.0 mg/dL/176.8 mmol/L, or an ICD-9-CM diagnosis of cognitive impairment or dementia in ambulatory care) [30]. Undertreatment rates were calculated in the same patient population as the proportion of patients with an HbA1c greater than 9%. Rates were calculated for each year.
2.3 Outlier Status
Outlier status was assessed by a facility outlier value measure standardized within a year and for each of three comparator groups:
-
1.
All VA hospitals
-
2.
Hospitals within the same VISN
-
3.
Hospitals within the same complexity level
The facility outlier value was calculated as:
3 Analyses
We calculated yearly rates of over- and undertretment as well as outlier status.
3.1 Results
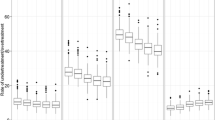
Outlier values for our primary measure ranged from approximately − 1.5 to + 3.5 (Fig. 14.1). There was little effect of facility complexity and VISN on outlier identification. Use of different HbA1c thresholds results in different sets of outliers with only modest overlap (data not shown). Of the 14 facilities identified in the highest-performing decile for overtreatment in 2009, only 7 were consistent high performers in all the years from 2009 to 2013. While undertreatment in this population at high risk for hypoglycemia rose over time from a mean of 7.1% to 10.3%, consistent high-performing outliers for overtreatment had higher rates of undertreatment (HbA1c > 9%) in general. However, three of the high performers had overtreatment rates similar to VHA facilities as a whole; the remainder had higher rates at baseline that rose even more than facilities in general (Fig. 14.2).

Overtreatment outlier values over time by 2009 deciles using 6.5% threshold and all VA facilities as comparator. Asterisk, top performing decile; filled circle, remaining 90%

Undertreatment rates in the population at high risk for hypoglycemia. Undertreatment rates in the population at high risk for hypoglycemia over time among facilities with lowest rates of overtreatment (dashed lines) and the average rate +95% Confidence interval among all VA facilities (solid line within shaded area). Seven facilities were identified as high performers using overtreatment metrics; high rates of undertreatment were observed in many and looking at the undertreatment rates over time and comparing them to the undertreatment rates of all VA facilities, several high performers with regard to overtreatment have consistently high rates of undertreatment
4 Discussion
Statistical identification of positive deviants for diabetes overtreatment was dependent not only upon the specific measure used but also on time, i.e., high performance was consistent in only half of the facilities identified in the baseline year. Most importantly, our findings indicate the importance of including a balancing measure or countermeasure to identify unintended negative consequences. Thus, facilities which appeared to be similar based on one measure (equifinality) could be differentiated based on a balancing measure.
Equifinality and multifinality are each characteristic of open systems and represent opposite sides of the same coin. The principle of equifinality states that a given end state can be achieved by different paths or trajectories. In short, “all roads (may) lead to Rome,” though the routes vary. In contrast, the principle of multifinality states that different end states can be reached starting from the same initial conditions. In short, every journey, regardless of where it ends, begins with the (same) first step. These principles make process improvement possible. Open systems exhibit change, but their end states are not ordained in a linear fashion from their initial states [45]. Different healthcare systems starting from different initial conditions reach a similar state of quality care. Moreover, different configurations of factors (and their interactions) may result in similar end states, a phenomenon that provides the basis for the methodology of qualitative comparative analysis [46].
The limitations of our study notwithstanding (e.g., single condition which is multidimensional and involves patients, providers, and organizations; single healthcare system; our focus on identification of high-performing sites rather than the best practices themselves) our findings have implications for the positive deviance approach because they illustrate the danger of taking a very narrow approach to what constitutes equifinality. Although there are numerous methods for outlier detection and differences in both criteria and comparator, our study suggests that considerable thought needs to be given to this issue at the outset, before attempts are made to identify performance outliers. Specifically, the end state of low rates of overtreatment may be observed under both desirable and undesirable conditions. Ideally, low rates of overtreatment occur as a result of specific attention to patients at risk for hypoglycemia. Less ideally, a low rate of overtreatment may occur as an artifact of widespread undertreatment and a facility-wide tendency toward higher HbA1c levels. We term this phenomenon pseudo-equifinality. In other words, two roads may lead to Rome, but one may lead to the Pantheon and the other to the Cloaca Maxima (greatest sewer).
References
Bretschneider S, Marc-Aurele Jr F, Wu J. “Best practices” research: a methodological guide for the perplexed. J Public Adm Res Theory 2005;15:307–23.
Guzman G, Fitzgerald JA, Fulop L, et al. How best practices are copied, transferred, or translated between health care facilities: a conceptual framework. Health Care Manag Rev. 2015;40:193–202.
Maggs-Rapport F. ‘Best research practice’: in pursuit of methodological rigour. J Adv Nurs. 2001;35:373–83.
Mold J, Gregory M. Best practices research. Fam Med. 2003;35:131–4.
A systematic review of outliers detection techniques in medical data: preliminary study. 11 Jan 26; Rome, Italy: HEALTHINF 2011, 2011.
Hodge V, Austin J. A survey of outlier detection methodologies. Artif Intell Rev. 2004;22:85–126.
Shahian DM, Normand SL. What is a performance outlier? BMJ Qual Saf. 2015;24:95–9.
Baxter R, Kellar I, Taylor N, Lawton R. How is the positive deviance approach applied within healthcare organizations? A systematic review of methods used. BMC Health Serv Res. 2014;14 Suppl 2:7.
Bradley EH, Curry LA, Ramanadhan S, Rowe L, Nembhard IM, Krumholz HM. Research in action: using positive deviance to improve quality of health care. Implement Sci. 2009;4:25.
Gabbay RA, Friedberg MW, Miller-Day M, Cronholm PF, Adelman A, Schneider EC. A positive deviance approach to understanding key features to improving diabetes care in the medical home. Ann Fam Med. 2013;11 Suppl 1:S99–107.
Krumholz HM, Curry LA, Bradley EH. Survival after acute myocardial infarction (SAMI) study: the design and implementation of a positive deviance study. Am Heart J. 2011;162:981–7.
Lawton R, Taylor N, Clay-Williams R, Braithwaite J. Positive deviance: a different approach to achieving patient safety. BMJ Qual Saf. 2014;23:880–3.
Luft HS. Data and methods to facilitate delivery system reform: harnessing collective intelligence to learn from positive deviance. Health Serv Res. 2010;45:1570–80.
Setiawan M, Sadiq S. A methodology for improving business process performance through positive deviance. Int J Inf Syst Model Des. 2013;4:1–22.
Singhal A, Greiner K. Using the Positive Deviance approach to reduce hospital-acquired infections at the Veterans Administration Healthcare System in Pittsburgh. In: Suchman A, Sluyter D, Williamson P, editors. Leading change in healthcare: transforming organizations using complexity, positive psychology, and relationship-centered care. New York: Radcliffe Publishing; 2011. p. 177–209.
Marsh G. Are follow-up consultations at medical outpatient departments futile? BMJ 1982;284:1176–7.
Sternin J. Practice positive deviance for extraordinary social and organizational change. In: The change champion’s field guide: strategies and tools for leading change in your organization. Hoboken, NJ: Wiley; 2013. p. 20–37.
Zeitlin M, Ghassemi H, Mansour M. Positive deviance in child nutrition - with emphasis on psychosocial and behavioural aspects and implications for development. New York: United Nations University Press; 1991.
Selby L. Public health project taps into superstar patients’ expertise. http://thedo.osteopathic.org/2015/04/public-health-project-taps-into-superstar-patients-expertise/ (2017). Accessed 5 Jan 2017.
Mainemelis C. Stealing fire: creative deviance in the evolution of new ideas. Acad Manag Rev. 2010;35:558–78.
Spreitzer G, Sonenshein S. Positive deviance and extraordinary organizing. In: Cameron K, Dutton J, editors. Positive organizational scholarship: foundations of a new discipline. Oakland, CA: Berrett-Koehler Publishers; 2003. p. 207–24.
Spreitzer G, Sonenshein S. Toward the construct definition of positive deviance. Am Behav Sci. 2004;47:828–47.
Vadera A, Pratt M, Mishra P. Constructive deviance in organizations: integrating and moving forward. J Manag. 2013;39:1221–76.
Warren D. Constructive and destructive deviance in organizations. Acad Manag Rev. 2003;28:622–32.
Lindberg C, Clancy TR. Positive deviance: an elegant solution to a complex problem. J Nurs Adm. 2010;40:150–3.
Spindler M, Wagenheim G. Positive deviance: sparks that ignite systems change. Chall Organ Soc. 2015;4:647–9.
Richardson KA, Mathieson G, Cilliers P. The theory and practice of complexity science: epistemological considerations for military operational analysis. SysteMexico 2000;1:25–66.
Richardson KA. Complex systems thinking and its implications for policy analysis. In: Handbook of decision making. Boca Raton, FL: CRC Press; 2007. p. 189–122.
Pascale R, Sternin J, Sternin M. The power of positive deviance: how unlikely innovators solve the world’s toughest problems. Boston, MA: Harvard Business Press; 2010.
Tseng CL, Soroka O, Maney M, Aron DC, Pogach LM. Assessing potential glycemic overtreatment in persons at hypoglycemic risk. JAMA Intern Med. 2013;174:259–68.
Bilimoria KY, Cohen ME, Merkow RP, et al. Comparison of outlier identification methods in hospital surgical quality improvement programs. J Gastrointest Surg. 2010;14:1600–7.
Mull HJ, Chen Q, O’Brien WJ, et al. Comparing 2 methods of assessing 30-day readmissions: what is the impact on hospital profiling in the veterans health administration? Med Care 2013;51:589–96.
Rothberg MB, Morsi E, Benjamin EM, Pekow PS, Lindenauer PK. Choosing the best hospital: the limitations of public quality reporting. Health Aff. (Millwood) 2008;27:1680–7.
Paddock SM, Adams JL, Hoces dlG. Better-than-average and worse-than-average hospitals may not significantly differ from average hospitals: an analysis of Medicare Hospital Compare ratings. BMJ Qual Saf. 2015;24:128–34.
Aron DC. Quality indicators and performance measures in diabetes care. Curr Diab Rep. 2014;14:472.
National action plan for adverse drug event prevention. Washington, DC: U.S. Department of Health and Human Services, Office of Disease Prevention and Health Promotion; 2014. https://health.gov/hcq/pdfs/ade-action-plan-508c.pdf. Accessed 5 Jan 2017.
Trucil D. AGS unveils revised list of topics to talk about with older adults as part of choosing wisely®campaign. http://www.choosingwisely.org/ags-unveils-revised-list-of-topics-to-talk-about-with-older-adults-as-part-of-choosing-wisely-campaign/. Accessed 5 Jan 2017.
Duckworth W, Abraira C, Moritz T, Reda D, Emanuele N, et al. Glucose control and vascular complications in veterans with type 2 diabetes. N Engl J Med. 2009;360:129–39.
Miller ME, Bonds DE, Gerstein HC, et al. The effects of baseline characteristics, glycaemia treatment approach, and glycated haemoglobin concentration on the risk of severe hypoglycaemia: post hoc epidemiological analysis of the ACCORD study. BMJ 2010;340:b5444.
Inzucchi SE, Bergenstal RM, Buse JB, et al. Management of hyperglycaemia in type 2 diabetes: a patient-centered approach. Position statement of the American Diabetes Association (ADA) and the European Association for the Study of Diabetes (EASD). Diabetologia 2012;55:1577–96.
Ismail-Beigi F, Moghissi ES, Tiktin M, Hirsch IB, Inzucchi SE, Genuth S. Individualizing glycemic targets in type 2 diabetes mellitus: implications of recent clinical trials. Ann Intern Med 2011;154:554–9.
Montori V, Fernandez-Balsells M. Glycemic control in type 2 diabetes: time for an evidence-based about-face? Ann Intern Med. 2009;150:803–8.
Pogach L, Aron D. Balancing hypoglycemia and glycemic control: a public health approach for insulin safety. JAMA 2010;303:2076–7.
Pogach LM, Tiwari A, Maney M, Rajan M, Miller DR, Aron D. Should mitigating comorbidities be considered in assessing healthcare plan performance in achieving optimal glycemic control? Am J Manag Care 2007;13:133–40.
Kapsali M. Equifinality in project management exploring causal complexity in projects. Syst Res Behav Sci. 2013;30:2–14.
Ragin CC, Shulman D, Weinberg A, Gran B. Complexity, generality, and qualitative comparative analysis. Field Methods 2003;15:323–40.
Acknowledgements
Funding. The work was supported by grants from the Veterans Health Administration (VHA) Health Services Research & Development Service and its Quality Enhancement Research Initiative (QUERI) to Dr. Aron (SCE 12-181), to Dr. Pogach (RRP-12-492), and to Dr. Tseng (IIR 11-077).
Disclaimer. The opinions expressed are solely those of the authors and do not represent the views of the Department of Veterans Affairs.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2018 Springer International Publishing AG, part of Springer Nature
About this chapter

Cite this chapter
Aron, D.C., Wilson, B., Tseng, CL., Soroka, O., Pogach, L.M. (2018). Positive Deviance in Health Care: Beware of Pseudo-Equifinality. In: Sturmberg, J. (eds) Putting Systems and Complexity Sciences Into Practice. Springer, Cham. https://doi.org/10.1007/978-3-319-73636-5_14
Download citation
DOI: https://doi.org/10.1007/978-3-319-73636-5_14
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-319-73635-8
Online ISBN: 978-3-319-73636-5
eBook Packages: MedicineMedicine (R0)