
Abstract
Non-Neoplastic conditions of the salivary glands range from various forms of inflammation to sialadenosis to reactive lymph nodes. Sialadenitis is the most common non-neoplastic condition, and includes acute or chronic sialadenitis as well as granulomatous disease. Depending upon the study, the risk of malignancy for aspirates of non-neoplastic salivary gland lesions is approximately 10%. While non-neoplastic conditions of salivary glands can on occasion mimic a neoplasm leading to a false positive diagnosis, the most problematic aspect is the possibility of a false negative diagnosis due to inadequate sampling.
Access provided by CONRICYT-eBooks. Download chapter PDF
Similar content being viewed by others



Keywords
General Background
The non-neoplastic lesions of the salivary glands are relatively common, and can clinically mimic a neoplasm due to the presence of a distinct mass [1,2,3,4,5]. Acute and chronic sialadenitis that also include granulomatous disease are the most common non-neoplastic lesions [6] (Table 3.1). Acute sialadenitis typically results from bacterial infection and is rarely sampled by fine-needle aspiration (FNA) due to its typical clinical presentation. Chronic sialadenitis can result from causes that lead to salivary duct obstruction, most often sialolithiasis, but in some cases can be related to systemic causes such as IgG4-related autoimmune disease. Granulomatous inflammation of the salivary gland is uncommon; the causes include mucoceles, infections, and sarcoidosis [7,8,9,10,11,12].
The average risk of malignancy (ROM) for aspirates of salivary gland lesions classified as “Non-Neoplastic” is approximately 10% with study ranges from 0 to 20% [8,9,10,11,12,13]. It is crucial that the ROM should be interpreted within the context of the patient population selected to undergo a salivary gland FNA since there is often a suspicion of malignancy. Many of the non-neoplastic salivary gland conditions can also be secondary to synchronous neoplastic processes. One of the goals of the Milan System is to improve test performance. A careful clinical and radiologic correlation is necessary to avoid the pitfall of a false negative FNA result when reporting a salivary gland FNA as “Non-Neoplastic.”
General Definition
The designation “Non-Neoplastic” is used for specimens that show benign non-neoplastic changes, including those associated with acute or chronic reactive responses to inflammation, structural alterations, and infection. The designation “Non-Neoplastic” is intended to be used in conjunction with available clinical and radiologic information.
Sialolithiasis
Sialolithiasis, the formation of ductal calculi , is often associated with salivary gland enlargement and pain, and clinical symptoms can mimic a neoplasm [6]. The stones are usually composed of calcium phosphate and calcium carbonate admixed with other minor components. Sialolithiasis occurs primarily in the submandibular gland (up to 80% in Wharton’s duct), less often in the parotid gland (approximately 20% in Stensen’s duct), and very rarely in sublingual glands. Imaging studies such as computed tomography (CT) are very accurate in detecting ductal calculi and corresponding duct dilatation.
Cytologic Criteria
-
Hypocellular aspirate
-
Scant or absent acinar cells
-
Groups of benign ductal cells and/or metaplastic squamous, ciliated, or mucinous cells
-
Inflammatory background ± mucin
-
Calcifications (stone fragments)
Explanatory Note
In the very early stages of disease, aspirates of a salivary gland mass due to sialolithiasis may yield only normal-appearing salivary gland tissue. In such situations, the major diagnostic consideration is a sampling error. In long-standing cases, the gland is involved by chronic inflammation (i.e., chronic sialadenitis), squamous metaplastic changes in the ductal epithelium, and parenchymal atrophy (Fig. 3.1). The diagnosis of sialolithiasis is usually straightforward when clinical and radiological findings are available. Fragments of stone or crystalline debris are present in the FNA specimen in approximately 50% of cases (Fig. 3.2). However, when stone fragments are absent, epithelial changes (especially metaplastic squamous and mucinous cells) and a mucoid background can be difficult to distinguish from a low-grade mucoepidermoid carcinoma (LGMEC ) (see Chap. 7, Malignant). Squamous metaplastic cells with atypia can also raise the possibility of metastatic squamous cell carcinoma, although the degree of cytologic atypia usually is mild in cases of sialolithiasis (Fig. 3.3). In some instances, a diagnosis of “Atypia of Undetermined Significance (AUS) ” with an explanatory note may be necessary (see Chap. 4, Atypia of Undetermined Significance).

Non-Neoplastic. This aspirate of sialolithiasis contains a cluster of metaplastic ductal cells with background acute and chronic inflammation (smear, Papanicolaou stain)

Non-Neoplastic. This aspirate of sialolithiasis shows stone fragments and a multinucleated giant cell (smear, Papanicolaou stain)

Non-Neoplastic. This smear shows metaplastic ductal cells from an aspirate of sialolithiasis (smear, Papanicolaou stain)
Acute Sialadenitis
Acute sialadenitis most frequently involves the parotid gland followed by the submandibular gland [6, 14]. It is rarely evaluated by FNA since it is usually diagnosed based upon typical clinical symptoms and is treated with antibiotics. It can occur as suppurative or nonsuppurative forms. Acute suppurative sialadenitis is most often caused by oral cavity bacteria such as Staphylococcus aureus or Streptococcus sp. It is more common in older patients with dehydration, poor oral hygiene, malnutrition, oral neoplasms, liver cirrhosis, and diabetes mellitus. Acute nonsuppurative sialadenitis is more common in children, and is often associated with viral infections including those caused by paramyxovirus (mumps), cytomegalovirus (CMV) , and Epstein–Barr virus (EBV) (mononucleosis). In addition, acute sialadenitis secondary to obstruction of the submandibular (Wharton’s) duct by stones or strictures has been reported.
Cytologic Criteria
-
Abundant neutrophils ± bacteria (Fig. 3.4)
Fig. 3.4 
Non-Neoplastic. These aspirates of acute sialadenitis (a) (smear, Romanowsky stain) and (b) (Papanicolaou stain) show abundant acute inflammation with occasional histiocytes and background debris, but no evidence of a neoplastic process. Clinical follow-up and radiologic correlation are needed to ensure that the aspirate is representative
-
Histiocytes
-
Necroinflammatory debris (suppurative)
-
Granulation tissue (later stages)

Explanatory Notes
Although infrequently aspirated, FNA of acute sialadenitis, which is usually painful, is used to exclude an underlying neoplastic condition. Aspiration of any residual mass should be performed after resolution of the inflammatory process since tumor diathesis in high-grade cancers can mimic acute sialadenitis. In contrast, caution should be exercised not to overinterptet the reactive atypia and degenerative changes in ductal cells (Fig. 3.5) due to acute inflammation as a neoplastic process. Special stains for bacteria as well as material for microbiologic culture and sensitivity testing can be useful.

Non-Neoplastic. This smear shows focal ductal cells (upper right) with reactive atypia in a background of marked acute sialadenitis (smear, Papanicolaou stain)
Chronic Sialadenitis Including IgG4-Related Disease
Chronic sialadenitis is primarily a condition involving the submandibular glands [15]. It is most common in middle-aged adults with a slightly increased incidence in males. The clinical history and physical examination will often suggest the diagnosis; however, some cases will present as a firm mass simulating a neoplasm. It has a strong association with obstruction of a major duct secondary to sialolithiasis. Other potential causes of duct obstruction and chronic sialadenitis include radiation, surgery, trauma, autoimmune disorders, and bulimia. Chronic obstructive sialadenitis, chronic recurrent sialadenitis, and chronic sclerosing sialadenitis are the three main forms of the disease. Chronic sclerosing sialadenitis is also known as Küttner tumor , and some cases represent a form of IGg4-related disease, which can be either localized or occasionally systemic. Chronic sclerosing sialadentitis is often bilateral and causes a generalized firmness of the gland. The presence of IgG4-positive plasma cells and elevated serum levels of IgG4 would suggest IgG-4-related disease whose diagnosis is made based upon specific clinical features and histopathologic criteria.
Cytologic Criteria
-
Hypocellular
-
Small groups of ductal cells, may be basaloid or metaplastic
-
Absent or scant acinar cells
-
Chronic inflammation (including lymphocytes and plasma cells)
-
Fibrotic stromal fragments
Explanatory Notes
The combination of a hypocellular aspirate with absent acinar cells, small cohesive ductal groups, and mild chronic inflammation is characteristic of chronic sialadenitis (Fig. 3.6), but clinical and radiologic correlations are needed to exclude a non-representative FNA sample. The most common pitfall for chronic sialadenitis is misinterpretation of the metaplastic or atrophic ductal cells (Fig. 3.7) as a basaloid neoplasm (see Chap. 4). In contrast, chronic sialadentitis generally lacks the degree of cellularity and larger three-dimensional epithelial groups found in aspirates of a basaloid neoplasm.

Non-Neoplastic. (a) This aspirate of chronic sialadenitis shows a sheet of cytologically bland ductal cells. (b) This aspirate of chronic sialadenitis demonstrates reactive ductal atypia (smear, Papanicolaou stain)

Non-Neoplastic. This smear of chronic sialadenitis demonstrates a smaller atrophic ductal group with basaloid qualities and background chronic inflammation; avoid misinterpreting this as a basaloid neoplasm (smear, Papanicolaou stain)
In addition to stone fragments and inflammatory cells, a subset of chronic sialadenitis cases and benign inflamed cysts can have amylase crystalloids (Fig. 3.8), which are non-birefringent crystalline structures with rectangular, needlelike, and rhomboid geometric shapes [16, 17]. Amylase crystalloids are primarily associated with benign, non-neoplastic conditions, although they have occasionally been reported in Warthin tumor and pleomorphic adenoma (PA) . It is important that inflamed cases with amylase crystalloids include a comment in the diagnosis that clinical and radiologic correlations are needed to help exclude a neoplastic condition. Other crystalloids that can be seen in salivary gland aspirates include floret-shaped tyrosine crystalloids as well as collagenous crystalloids, and calcium oxalate crystals. Unlike amylase crystalloids, tyrosine crystalloids are more commonly associated with neoplastic conditions, most often with PA, but with some malignant neoplasms as well [17].

Non-Neoplastic. Amylase crystalloids (a, b) are non-birefringent crystalline structures with rectangular, needle-shaped, rhomboid, and platelike shapes. They are most commonly associated with non-neoplastic inflammatory conditions as in this case (smear, Papanicolaou stain)
Granulomatous Sialadenitis
Granulomatous inflammation can involve the salivary gland parenchyma or associated lymph nodes. Patients usually present with a slow-growing mass [14]. It is commonly a response to extravasated ductal contents, particularly mucin, secondary to obstructive sialadenopathy, which can result from a variety of causes including specific infections (e.g., mycobacterial, actinomycosis, cat-scratch disease, toxoplasmosis, tularemia) or less commonly a systemic granulomatous disease such as sarcoidosis. In very rare cases, granulomatous inflammation can be due to certain neoplastic conditions such as Hodgkin lymphoma, T-cell lymphoma, and a subset of metastatic carcinomas (e.g., nasopharyngeal carcinoma).
Cytologic Criteria
-
Hypocellular (scant acinar and ductal cells)
-
Groups of epithelioid histiocytes
-
Variable amounts of acute and chronic inflammatory cells
-
± Multinucleated giant cells
-
± Necrotic background debris
Explanatory Notes
The diagnosis of granulomatous sialadenitis relies on identifying groups of epithelioid histiocytes (Fig. 3.9a). Obstructive sialadenopathy with extravasation of ductal contents is the most common cause of a granulomatous reaction, which can result from calculi or less often tumors. In cases with more marked granulomas, care should be taken to avoid misinterpreting the epithelioid histiocytes with their moderate amounts of eosinophilic cytoplasm and curved nuclei as an epithelial neoplasm. Mycobacterial infection (tuberculous or nontuberculous) is the most common etiology for infectious granulomatous sialadenitis, although special stains (AFB) infrequently reveal diagnostic acid fast bacteria. Other granulomatous infections of the salivary glands are rare. Cat-scratch fever and tularemia can be associated with suppurative granulomatous inflammation, including peripherally palisading epithelioid histiocytes, centrally located neutrophils, and an associated mixed chronic inflammation. When infectious etiologies are suspected, special stains can be performed using cell block material or using liquid based slides. In addition, the cytopathologist should consider submitting material for microbiology cultures and/or polymerase chain reaction (PCR) testing; otherwise, the patient might be subjected to a repeat FNA to obtain additional material.

Non-Neoplastic. (a) This aspirate of granulomatous sialadenitis shows a large group of epithelioid histiocytes; an infectious agent should be excluded. (b) Aspirates of sarcoidosis yield loose collections of epithelioid histiocytes, and usually lack background necrosis (noncaseating) (smear, Papanicolaou stain)
Sarcoidosis (Fig. 3.9b) is among the most common systemic causes of granulomatous sialadenitis. Aspirates yield loose collections of epithelioid histiocytes, and usually lack background necrosis (noncaseating). Sarcoidosis is a diagnosis of exclusion, and requires clinical and microbiologic correlation as well as special stains to exclude an infectious cause.
Reactive Lymph Node Hyperplasia
Enlarged intra- and peri-parotid lymph nodes are a common non-neoplastic cause of a salivary gland mass (Table 3.2). They are frequently sampled by FNA to confirm benign disease, to diagnose infection, or to rule-out either metastatic disease or lymphoma [18]. The etiology of parotid gland lymph node hyperplasia can be nonspecific, or it can be a response to clinical or subclinical bacterial or viral infection often involving the skin of the face or scalp. Mononucleosis, tuberculosis, and cat-scratch disease, among others, can also result in such a reaction.
Cytologic Criteria
Aspirates of reactive lymph node hyperplasia are usually cellular and contain (Figs. 3.10 and 3.11):
-
Mixed population of lymphocytes with predominance of small mature forms
-
Tingible body macrophages
-
Lymphohistiocytic aggregates representing the cytologic correlate of germinal centers
-
Background lymphoglandular bodies

Non-Neoplastic. These aspirates of reactive lymph node hyperplasia (a) (smear, Romanowsky stain) (Courtesy of William Geddie, MD, Laboratory Medicine & Pathobiology, University of Toronto, Toronto, Canada) and (b) (smear, Papanicolaou stain) show a mixed population of mostly small and intermediate-size lymphocytes admixed with follicular dendritic cells. Flow cytometry can be used to confirm a polyclonal population

Non-Neoplastic. These aspirates of reactive lymph node hyperplasia show (a) a cohesive group of lymphocytes and follicular dendritic cells representing a germinal center fragment. (b, c) Tingible body macrophages are present in a background of predominantly small mature lymphocytes and occasional follicular dendritic cells (smear, Papanicolaou stain)
Explanatory Notes
The presence of a heterogeneous population of lymphocytes, tingible body macrophages, and dendritic cells suggests the diagnosis of reactive lymphoid hyperplasia. In most cases, the predominant cell population will consist of a mixture of small mature B- and T-lymphocytes. Clinical correlation is needed along with demonstration of polyclonality by flow cytometry or immunohistochemical studies. Caution is recommended, particularly when evaluating aspirates of lymph nodes in the elderly, lymph nodes larger than 3 cm, and multiple enlarged or matted lymph nodes. In addition, patients with autoimmune disease such as Sjögren’s syndrome are at increased risk of developing primary parotid gland lymphomas. Occasionally, reactive lymphoid hyperplasia can contain an increased proportion of larger cells, either lymphoid or histiocytic (Fig. 3.12), which can lead to a diagnosis of AUS. Infectious mononucleosis due to EBV can produce markedly atypical cells. It is also important to note that a subset of lymphomas can yield an aspirate with a heterogeneous appearance mimicking reactive lymphoid hyperplasia, namely extranodal marginal zone lymphoma as well as others such as Hodgkin lymphoma, some T-cell lymphomas, and T-cell rich B-cell lymphoma. For any case of a salivary gland lymph node aspirate where lymphoma is in the differential diagnosis, flow cytometry using an aliquot of unfixed material is highly recommended.

Atypia of Undetermined Significance (AUS). This lymph node aspirate shows an increased proportion of larger lymphocytes. In the absence of flow cytometry to exclude lymphoma, such aspirates should be classified as AUS (smear, Romanowsky stain)
Clinical correlation and follow-up are important in patients with lymphadenopathy, and a note suggesting additional evaluation for patients with persistent lymphadenopathy can be useful. This is particularly true in cases where immunophenotyping is not performed, as well as for certain unsuspected lymphomas such as Hodgkin lymphoma where flow cytometry can be negative.
Benign Lymphoepithelial Lesion/Lymphoepithelial Sialadenitis (LESA)
Lymphoepithelial sialadenitis (LESA) is a benign condition characterized by a lymphocytic infiltrate associated with parenchymal atrophy and foci of ductal hyperplasia with intraepithelial lymphocytes (Fig. 3.13). It is an autoimmune lesion and is often related to Sjögren’s syndrome; it is more common in women, and affects the parotid glands in about 90% of cases [19]. Bilateral disease is typical, although one gland may be more severely affected than the other. Patients experience recurrent, often progressive, parotid gland enlargement with varying degrees of discomfort or pain. Patients with Sjögren’s syndrome have an increased risk of developing lymphoma, particularly extranodal marginal zone lymphoma.

Non-Neoplastic. This aspirate demonstrates the lymphoepithelial lesion of lymphoepithelial sialadenitis, which consists of a bland sheet of ductal epithelial cells with admixed small lymphocytes (smear, Papanicolaou stain)
Cytologic Criteria
The hallmark cytologic features of LESA are:
-
Cellular aspirate
-
Lymphoepithelial lesions consisting of cohesive sheets of ductal cells, often with squamous metaplastic changes, and with small mature lymphocytes percolating through the epithelial sheets (Fig. 3.14).
Fig. 3.14 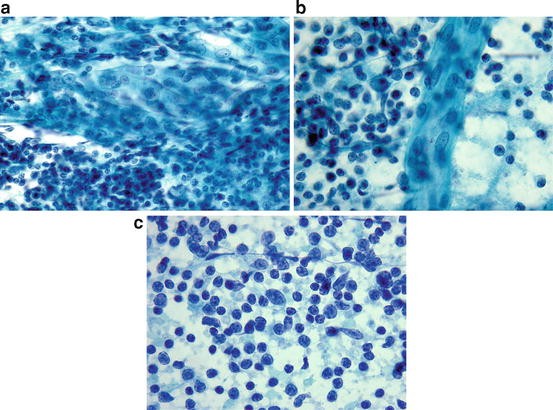
Non-Neoplastic. (a, b) The lymphoepithelial lesions of lymphoepithelial sialadenitis (LESA) are sheets of ductal cells that can exhibit squamous metaplastic features. (c) The associated lymphoid population in LESA is a mixed pattern with a predominance of small mature lymphocytes (smear, Papanicolaou stain)
-
Mixed population of lymphocytes, dendritic cells, and tingible body macrophages with predominance of small mature lymphocytes
-
Lymphohistiocytic aggregates
-
Acinar cells are usually absent

Explanatory Notes
The lymphoepithelial lesions in aspirates of LESA will often have squamous metaplastic features. The ductal epithelial cells will exhibit a uniform atypia, including enlarged nuclei with variably distinct nucleoli that overall resembles reparative changes. In some cases, the lymphoepithelial lesions can raise a differential diagnosis of metastatic carcinoma to a lymph node, particularly when reviewed outside of the clinical context of LESA. In contrast to metastatic carcinoma, the epithelial cells in aspirates of LESA lack significant nuclear pleomorphism, mitotic activity, hyperchromasia, and background necrosis. Given the increased risk of primary lymphoma in patients with LESA, care should be taken to assess the aspirate for polyclonality using flow cytometry, and for a population of lymphocytes with atypical features.
In contrast to LESA, which is usually solid, aspirates of lymphoepithelial cysts (including those associated with HIV) will lack the large sheetlike lymphoepithelial lesions of LESA, and consist of proteinaceous cyst contents with admixed degenerating squamous cells, keratin debris, as well lymphocytes and lymphohistiocytic aggregates (Fig. 3.15). In some cases, a glandular cyst lining component, which can be ciliated, may also be encountered. In middle-aged and older patients, care should be taken to exclude the possibility of metastatic squamous cell carcinoma, which will usually exhibit more marked squamous atypia than in a lymphoepithelial cyst.

Non-Neoplastic. (a) Aspirates of lymphoepithelial cysts consist of a mixed population of lymphocytes and variable numbers of dendritic cells. (b) Some cases may show only cyst contents with abundant bland nucleate and anucleate squamous cells. Clinical context is important to exclude a squamous cell carcinoma (smear, Papanicolaou stain)
Entities Sometimes Classified as “Non-Neoplastic”
Sialadenosis
Sialadenosis or sialosis is an uncommon persistent, non-inflammatory, non-neoplastic enlargement of salivary glands [7]. Sialadenosis primarily affects the parotid glands, often bilaterally, although it can occasionally occur in the submandibular glands. Sialadenosis is almost always associated with an underlying systemic disorder such as diabetes, hypothyroidism, malnutrition, obesity, pregnancy, alcohol abuse, cirrhosis, HIV infection, or with several medications (especially antihypertensives). Clinically, the salivary gland swelling develops gradually, without a defined mass, and is usually painless.
Cytologic Criteria (Fig. 3.16)
-
Cellular aspirate
-
Clusters of enlarged (hypertrophic) acinar cells
-
Normal cytoarchitectural arrangement of acini is maintained
-
Background of stripped acinar cell nuclei
-
Fibroadipose tissue
-
Features suggestive of neoplasm, cyst, or inflammatory lesion are absent

Non-Neoplastic. This aspirate of sialadenosis shows a cluster of large vacuolated acinar cells. Clinical correlation is needed to interpret this aspirate (smear, Romanowsky stain)
Explanatory Notes
The enlarged acinar size in sialadenosis may be difficult to appreciate by FNA, but the condition is suspected clinically. Clinical and radiologic correlations are essential in diagnosing sialadenosis, since the major differential diagnosis is a sampling error (i.e., “Non-Diagnostic,” see Chap. 2, Non-Diagnostic). Therefore, for aspirates containing only non-neoplastic salivary gland elements, the cytopathologist should usually classify the aspirate as “Non-Diagnostic” when a discrete mass is present (i.e., suggesting a possible sampling error), or as “Non-Neoplastic” in the absence of a discrete mass and with appropriate clinicoradiological information. In either case, a comment describing the possibility of a sampling error is strongly recommended (see sample report).
Because numerous acinar cells are present in sialadenosis, care must be taken not to confuse this entity with a well-differentiated acinic cell carcinoma (see Chap. 7). Most importantly, the cells of sialadenosis maintain a normal cytologic and histologic cytoarchitectural arrangement, including a normal ductal component, while the neoplastic cells of acinic cell carcinoma do not. Other entities in the differential diagnosis of sialadenosis include accessory parotid gland, hamartoma, lipoma/lipomatosis, and sialolithiasis. Accessory parotid gland tissue may present clinically as a mass, and can occur anywhere along the parotid (Stensen’s) duct overlying the masseter muscle.
Oncocytosis
Oncocytosis is primarily encountered in older adults. It is considered a hyperplastic change in which there are variable degrees of oncocytic metaplasia of acinar and ductal cells (Fig. 3.17). Depending upon the extent of oncocytosis, distinction from oncocytoma (a true neoplasm) is often not possible since the two entities overlap clinically and histologically [20]. Because of this, most FNA cases of oncocytosis will be placed into the “Neoplasm: Salivary Gland Neoplasm of Uncertain Malignant Potential (SUMP)” category (See Chap. 5, Neoplasm).

Non-Neoplastic. This aspirate of oncocytosis from a multinodular gland shows a sheetlike collection of oncocytes merging with a small fragment of ductal epithelium (smear, Papanicolaou stain)
Cytologic Criteria
-
Acinar and ductal cells with abundant, granular, eosinophilic cytoplasm
-
Normal cytoarchitectural arrangement of acini and ductal cells is maintained
-
Variable amounts of benign ductal cells and fibroadipose tissue
-
Features suggestive of neoplasm, cyst, or inflammatory lesion are absent
Explanatory Notes
Oncocytosis in the salivary gland is more common with increasing age. The differential diagnosis includes oncocytoma as well as oncocytic changes that can occur in several primary salivary gland neoplasms, including pleomorphic adenoma and mucoepidermoid carcinoma. Recognizing the admixture of oncocytic acinar and ductal cells in a “normal” architectural pattern is the key to avoid misdiagnosing oncocytosis as an oncocytic neoplasm.
Clinical Management
Salivary gland lesions diagnosed as “Non-Neoplastic” by FNA should be followed clinically by repeat physical examination, cross-sectional imaging, or a combination of both depending upon the nature of the lesion. Any change in either the clinical or radiologic features should prompt repeat sampling, especially given the risk of sampling error in this subset of salivary gland lesions.
Sample Reports
Example 1:
Satisfactory for evaluation
NON-NEOPLASTIC
Abundant acute inflammation and reactive changes consistent with acute sialadenitis. See note.
Note: Correlation with microbiologic studies is suggested.
Example 2:
Evaluation limited by scant cellularity
NON-NEOPLASTIC
Consistent with chronic sialadenitis. See note.
Note: Clinical and radiological correlations are recommended to ensure that the aspirate is representative of the lesion.
Example 3:
Satisfactory for evaluation
NON-NEOPLASTIC
Granulomatous inflammation. See note.
Note: Non-necrotizing granulomas are present admixed with acute and chronic inflammation. Diagnostic considerations include a non-specific reaction secondary to obstructive sialadenopathy, infection, and sarcoidosis. Correlation with microbiologic studies is suggested.
Example 4:
Satisfactory for evaluation
NON-NEOPLASTIC
Consistent with reactive lymphoid hyperplasia. See note.
Note: Corresponding flow cytometry is benign, supporting the diagnosis. Clinical follow-up is recommended, and if lymphadenopathy persists, additional evaluation may be indicated.
Example 5:
Satisfactory for evaluation
NON-NEOPLASTIC
Consistent with lymphoepithelial sialadenitis. See note.
Note: Corresponding flow cytometry is benign, supporting the diagnosis.
Example 6:
Satisfactory for Evaluation.
NON-NEOPLASTIC
Benign salivary gland tissue suggestive of sialadenosis. See Note.
Note: Based on the clinical presentation of bilateral salivary gland enlargement without a discrete mass and with enlarged acinar cells microscopically, the findings are suggestive of sialadenosis. Clinical and radiologic correlations are needed to ensure that the FNA sample is representative of the lesion.
References
DeMay RM. Salivary gland. In: The art & science of cytopathology. vol. 2. 2nd ed. Chicago: ASCP Press; 2012. p. 775–838.
Droese M. Cytological diagnosis of sialadenosis, sialadenitis, and parotid cysts by fine-needle aspiration biopsy. Adv Otorhinolaryngol. 1981;26:49–96.
Eveson JW, Nagao T. Diseases of the salivary glands. In: Barnes L, editor. Surgical pathology of the head and neck, vol. 1. 3rd ed. New York: Informa Healthcare; 2009. p. 475–648.
Faquin WC, Powers CN. Salivary gland cytopathology. Essentials in cytopathology, vol. 5. Rosenthal DL, series editor. New York: Springer; 2008. p. 41–80.
Gupta S, Sodhani P. Sialadenosis of parotid gland: a cytomorphologic and morphometric study of four cases. Anal Quant Cytol Histol. 1998;20(3):225–8.
Stanley MW, Bardales RH, Beneke J, Korourian S, Stern SJ. Sialolithiasis. Differential diagnostic problems in fine-needle aspiration cytology. Am J Clin Pathol. 1996;106(2):229–33.
Ascoli V, Albedi FM, De Blasiis R, Nardi F. Sialadenosis of the parotid gland: report of four cases diagnosed by fine-needle aspiration cytology. Diagn Cytopathol. 1993;9(2):151–5.
Stewart CJR, MacKenzie K, McGarry GW, Mowat A. Fine-needle aspiration cytology of salivary gland: a review of 341 cases. Diagn Cytopathol. 2000;22(3):139–46.
Jain E, Gupta R, Kudesia M, Singh S. Fine needle aspiration cytology in diagnois of salivary gland lesions: a study with histological comparison. Cytojournal. 2013;10:5.
Pastore A, Borin M, Malagutti N, Di Laora A, Becati D, Delazer AL, et al. Preoperative assessment of salivary gland neoplasm with fine needle aspiration cytology and echography: a retrospective analysis of 357 cases. Int J Immunopathol Pharmacol. 2013;26(4):965–71.
Layfield LJ, Glasgow BJ. Diagnosis of salivary gland tumors by fine needle aspiration cytology: A review of clinical utility and pitfalls. Diagn Cytopathol. 1991;7(3):267–72.
Rossi ED, Wong LQ, Bizzarro T, Petrone G, Mule A, Fadda G, Baloch ZW. The impact of FNAC in the management of salivary gland lesions: institutional experiences leading to a risk-based classification scheme. Cancer Cytopathol. 2016;124(6):388–96.
Wei S, Layfield LJ, LiVolsi VA, Montone KT, Baloch ZW. Reporting of fine needle aspiration (FNA) specimens of salivary gland lesions: a comprehensive review. Diagn Cytopathol. 2017;45(9):820–7.
Tyagi R, Dey P. Diagnostic problems of salivary gland tumors. Diagn Cytopathol. 2015;43(6):495–509.
Bhatti RM, Stelow EB. IgG4-related disease of the head and neck. Adv Anat Pathol. 2013;20(1):10–6.
Nasuti JF, Gupta PK, Fleisher SR, LiVolsi VA. Nontyrosine crystalloids in salivery gland lesions: report of seven cases with fine-needle aspiration cytology and follow-up surgical pathology. Diagn Cytopathol. 2000;22(3):167–71.
Pantanowitz LP, Goulart RA, Cao QJ. Salivary gland crystalloids. Diagn Cytopathol. 2006;34(11):749–50.
Wakely PE Jr., Cibas ES. Lymph nodes. In: Cibas ES, Ducatmnan BS, editors. Cytology: diagnostic principles and clinical correlates, 3rd ed. (Expert Consult). Philadelphia: Elsevier Saunders; 2009. p. 319–58.
Michelow P, Dezube BJ, Pantanowitz L. Fine needle aspiration of salivary gland masses in HIV-infected patients. Diagn Cytopathol. 2012;40(8):684–90.
Rooper L, Onenerk M, Siddiqui MT, Faquin WC, Bishop JA, Ali S. Multinodular oncocytic hyperplasia: can cytomorphology allow preoperative diagnosis of a non-neoplastic salivary disease? Cancer Cytopathol. 2017;125(8):627–34.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2018 Springer International Publishing AG
About this chapter

Cite this chapter
Faquin, W.C. et al. (2018). Non-Neoplastic. In: Faquin, W., et al. The Milan System for Reporting Salivary Gland Cytopathology . Springer, Cham. https://doi.org/10.1007/978-3-319-71285-7_3
Download citation
DOI: https://doi.org/10.1007/978-3-319-71285-7_3
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-319-71284-0
Online ISBN: 978-3-319-71285-7
eBook Packages: MedicineMedicine (R0)