
Abstract
This chapter makes use of the theory of planned behavior to identify factors that motivate intention toward Waqf giving. The chapter examines the relationship between intention and actual support toward the construction of modern Waqf-based hospital in Uganda. The study adopted factor analysis, principal component analysis, and Structural Equation Modeling (SEM) to analyze data from 300 valid questionnaires. The findings reveal that three motivating factors, namely attitude, moral duties, and religious duties significantly and positively influence Muslim community’s intentions to provide actual financial and non-financial support for the construction of modern Waqf-based hospital in Uganda. Accordingly, Muslim religious authorities and relevant parties should use these three motivating factors to influence Muslim community decision to support Waqf-based projects for their socioeconomic development.
The paper was presented at the 10th International Conference on Islamic Economics and Finance (ICIEF), March 23–24, 2015, Doha, Qatar.
Access provided by CONRICYT-eBooks. Download chapter PDF
Similar content being viewed by others


Keywords
1 Introduction
Good health is one of the main determinants of economic growth and a component of well-being of the population (ILO 2008; Scheil-Adlung et al. 2006). Accessibility to healthcare services makes society healthier and raises their earning capacities. In addition, good health has positive impacts on school attendance, employment , and human capital development (Lamiraud et al. 2005). Better health means much higher survival rates for infants and children, which raise GDP per capita by increasing the ratio of workers to dependents. Better health among adults increases labor force participation and improves the productivity of those who are at work (ILO 2008). These together have significant positive impact on sustainable economic growth and social development, which in turn improves social welfare (Victor 2004).
However, not all countries enjoy good health care services and its benefits. For instance, Uganda ’s health care performance is still ranked among the worst in the world by the World Health Organization (WHO 2009). Uganda is a landlocked country in East Africa with estimated population of 34 million, and its population growth rate is 3.4% (WHO 2013). Uganda is still a low-income developing country ranking 161 on the Global Human Development Index in 2012 (HDI 2013). In Uganda, total health expenditure is US$52 per capita while household expenditure on health as a percentage of total health expenditure is 42%. The resources available for health are less than required to deliver the Uganda National Minimum Health Care Package. Indeed, household continues to carry a heavy burden with a high out-of-pocket expenditure on health care services (WHO 2014). This is because government investment on health is still low, and according to health ministry report (2013), financial investment in health by government shows a further decline over the years from 9.6% in 2009/2010 to 7.4% in 2012/2013.
With low government investments on health coupled with unaffordable private health care services, societies resort to other viable alternatives to meet their needs. For example, according to Sen (2000), nations adopt two pathways to increase the provision and accessibility of health care services to their citizens. The first route is through rapid economic development, where high-income nations can afford to provide high-quality health care services for all their citizens likewise citizens can afford to pay for high-quality health care services. The second pathway is a “support-led,” where individuals, corporations, charitable organizations, and religious and non-religious affiliated NGOs provide health care services to the poor and the needy section of society through donations. Today, the second pathway is increasingly contributing significantly toward providing health care services to the poor and the needy in both developed and developing countries.
For instance, in the USA, social services are regarded as the responsibilities of active citizen. In 1989, contribution of nonprofit institutions to the health care services was 56% of the total health care services in the country. They financed 3427 hospitals compared to public sector, which financed 1142 hospitals during the same period (Salamon 1999). In 1996, the sector spent US$262.5 billion on health care services, and the largest part of these incomes came from donations. By 2000, the nonprofit sector accounts for half of the USA’s health care services (Salamon et al. 2000). Weisbrod (1998) reported that 212 of the UK’s top 500 charities are health care service providers. In Pakistan, Imran Khan (former national cricket team captain) built Shaukat Khanum Memorial Cancer Hospital and Research Centre (SKMCH&RC) as Trust. The hospital opened to patients on December 29, 1994, upon completion of the first of its three phases at the cost of US$22 million. Sixty-seven percent of this fund was raised in the form of donation (SKMCH&RC annual report 2010). In Malaysia , Waqaf An-Nur Corporation Berhad (WANCorp) was established as part of Johor corporation social responsibilities. JCorp via WANCorp in cooperation with State Islamic Councils and support from KPJ Healthcare Berhad built and managed 20 Waqaf An-Nur Clinics (KWAN). This is in addition to one Waqaf An-Nur Hospital (HWAN) and two mobile clinics, both also being financed through Waqf . Today, WANCorp provides good health care services at affordable price of RM5 Malaysian Ringgit (inclusive of medication) to more than 1 million patients across states in Malaysia (Jcorp Annual Report 2013).
In Uganda , while the role of NGOs toward health care services is increasingly becoming prominent, the role of trusts, foundations, and endowments, particularly Waqf, is very appalling. Apart from few Waqf assets such as mosques , schools, and the Islamic Universities in Uganda built by the Organization of Islamic Cooperation (OIC) as Awqaf (Basar 1987), unfortunately, most of Waqf assets in the country are scattered, mismanaged , expropriated, underdeveloped, and in some instances sold privately by the trustees. The revival of Waqf to meet the socioeconomic needs of Muslim communities in Uganda, particularly a health care project such as hospital , is imperative. Reviving Waqf in Uganda will primarily depend on the extent to which the donors are motivated, and how these motivations influence their intention to support a Waqf-based health care project in the country. To the best knowledge of the authors, hardly any empirical study has examined the relationship between intention to donate and actual support of Muslim communities toward Waqf-based health care projects.
This chapter attempts to fill the gaps by examining the relationship between four antecedents (attitude, moral duties , perceived behavioral control, and religious duties), intentions, and actual financial and non-financial support by Muslim community for the construction of modern Waqf-based hospital in Uganda . Against this backdrop, this chapter attempts to answer the following research questions:
-
1.
What is the relationship between Muslim community attitude, intention, and the actual support for the construction of modern Waqf-based hospital in Uganda ?
-
2.
What is the relationship between moral duties , intention, and the actual support for the construction of modern Waqf-based hospital in Uganda ?
-
3.
What is the relationship between perceived behavioral control, intention, and the actual support for the construction of modern Waqf-based hospital in Uganda ?
-
4.
What is the relationship between religious duties, intention, and the actual support for the construction of modern Waqf-based hospital in Uganda ?
2 Theory of Planned Behavior (TPB)
This study is based on the theory of planned behavior (TPB) coined by Azjen (1991). TPB is one of the most influential and well-supported social psychological theories for predicting human behavior. The theory is an extension introduced to overcome the limitations of TRA—Theory of Reasoned Action.
The Theory of Reasoned Action (TRA) studies attitude–behavior relationship by connecting attitudes, subjective norms, behavioral intentions, and actual behavior (Ajzen and Fishbein 1975; Fishbein and Ajzen 1980). According to the theory, behavior is a consequence of behavioral intention, which is in turn a consequence of combination of people’s attitude toward performing the behavior in question and their perceptions of the pressure put upon them by referents to perform or not to perform that behavior (Ajzen and Fishbein 1980). The TRA is based on two main antecedents (attitude and subjective norm), which predict intention. Attitude refers to the evaluative effect of individuals’ positive or negative feelings in order to perform a particular behavior (Fishbein and Ajzen 1975). A subjective norm, on the other hand, refers to an individual’s perception of other people’s opinions on whether he or she should perform or not a particular behavior (Ajzen 1991). In other words, subjective norm is an individual perception of the likelihood that potential referent groups or individuals would approve or disapprove performing a given behavior (Ryan and Bonfield 1980).
Despite the fact that a high correlation of attitudes and subjective norms to behavioral intention and subsequently to behavior has been confirmed in many studies, the theory was found to be limited in explaining behaviors over which an individual has no volitional control. In order to overcome these limitations, Ajzen (1991) extended TRA by introducing Theory of Planned Behavior (TPB) where he added a new component, i.e., “perceived behavioral control.” The extension of the theory was necessitated to accommodate the correlates of behavior that are covered by the TRA and the correlates behavior that are not totally under a person’s control (Ajzen 1991). He asserts that behavioral decisions are not made all of a sudden, but are the consequences of attitudes, subject norms, and perceived behavioral control over the behavior. Ajzen further supported the integration of additional variables into the model. Figure 9.1 below shows Ajzen’s TPB theoretical framework.

Source http://www.healthcommcapacity.org/ retrieved on December 30, 2014
TPB Theoretical framework.
TRA and TPB are widely applied in psycho-social studies including, Islamic banking and finance (Echchabi and Olaniyi 2012; Yousafzai et al. 2010; Syed et al. 2011), study of health behaviors such as healthy eating (Astrom and Rise 2001; Corner et al. 2002), alcohol , and tobacco use (Mcmillan and Corner 2003), and exercise behavior (Bozionelos and Bennett 1999), blood donation (Giles and Cairns 1995), and volunteering behavior (Warburton and Terry 2000). There are a number of studies that have focused on altruistic and helping behavior (Konkoly and Perloff 1990; Becker 1974; Arrow 1975; Andreoni 1989, 1990; Rose-Ackerman 1997). Similarly, several studies have been conducted on charitable giving behavior (Linden 2011; Smith and Mcsweeney 2007; Osman et al. 2014). For instance, Linden (2011) used the theory of planned behavior as the underpinning theory in determining charitable giving behavior.
This study has modified TPB model to examine the extent to which the intention of Muslim community in Uganda to support the construction of Waqf-based hospital can be translated into actual financial and non-financial support. In addition to attitude, moral duties , and perceived behavioral control, the study adds religious duties as the fourth variable.
3 The Variables
The present study aspires to examine the relationship between four antecedents (attitude, moral duties , perceived behavioral control, and religious duties), intentions, and actual financial and non-financial support by Muslim community for the construction of modern Waqf-based hospital in Uganda .
3.1 Attitude
Attitude is said to arise from a combination of people’s belief about behavioral outcomes and their evaluation of those outcomes (Ajzen and Fishbein 1977; Sparks and Shepherd 1992). Hence, attitude toward behavior is determined by a person’s evaluation of the outcomes associated with the behavior and by the strength of these associations. Generally, a person who believes that performing a given behavior will lead to mostly positive outcomes will hold a favorable attitude toward performing the behavior, whereas a person who believes that performing the behavior will lead to mostly negative outcomes will hold an unfavorable attitude.
In the context of support for the construction of modern Waqf-based hospital in Uganda , the donor’s response might be used to understand attitude toward the support behavior. For example, belief that Waqf contributes to the socioeconomic development of the Muslim community in Uganda, belief that Waqf support could reduce government and individual expenditure, and belief that Waqf is a source of fund that can support health care projects might be taken as evidence of positive attitude toward the actual support. By way of contrast, an unfavorable attitude would be implied by expression of beliefs suggesting that Waqf support is difficult to perform. Numerous studies have documented the significant relationship between attitude and intention (Shih and Fang 2004; Lada et al. 2009; Amin and Chong 2011). Therefore, it is expected that there would be a positive relationship between Muslims attitude, intention, and the actual support for the construction of modern Waqf-based hospital in Uganda.
3.2 Moral Duties
Linden (2011) hypothesized that moral norms rather than social norms are likely to play a significant role in the formation of charitable intentions. In addition to moral norms, “attitude,” “perceived behavioral control,” and “past behavior” were also identified as significant predictors. Similarly, Smith and McSweeney (2007) findings from study on charitable giving behavior using a theory of planned behavior (TPB) reveal that attitudes, perceived behavioral control, injunctive norms, moral norms, and past behavioral control influence charitable giving intention. Hence, moral duties are expected to have positive relationship with attitude, intention, and the actual support for the construction of modern Waqf-based hospital in Uganda .
3.3 Perceived Behavioral Control
Perceived behavioral control is defined as people’s perceptions of their ability to carry out a given behavior (Ajzen 1991; 2011). It measures the degree to which a person has mental and physical control over his behavior and how confident he feels about being able to perform the behavior. This includes access to money, time, and other resources needed to perform a given behavior (Ajzen 2011).
In the support for the construction of Waqf-based hospital , such information like campaign or promotion about the project could enhance the awareness and knowledge of donor and eventually increase his or her support. Besides, financial commitment and income level will also determine his or her ability for contributing.
Smith and McSweeney (2007) conducted a study on charitable giving behavior using a theory of planned behavior (TPB) as a baseline theory to determine the influence of attitudes, norms, perceived behavior control, and past behavior on intention to donate money to charitable organizations. Their findings reveal that attitudes, perceived behavioral control, injunctive norms, moral norms , and past behavioral control influence charitable giving intention. Perceived behavioral control is expected to have positive relationship with attitude, intention, and the actual support for the construction of modern Waqf-based hospital in Uganda .
3.4 Religious Duties
Kamri (2010) mentioned that the practice of Waqf giving behavior is a form of ibadah that brings oneself closer to God (Allah ) by entrusting the Waqf for the benefit of the public. Several verses of the Quran and Prophetic tradition or hadith stipulate that the Waqf founder (Waqif) is promised a continuous reward from the Waqf he/she made. For example, Allah says in the Quran (al-Hadid, 57:11):
Who is he that will loan on God a beautiful loan for (God) will increase it manifold to his credit, and he will have (beside) a noble reward.
Kotler and Keller (2012) argued that religion is part of culture, and culture influences and shapes one’s intention and behavior. Religion is one of the most important cultural institutions which has significant influence on people’s attitudes, values, and behaviors at both micro—and macro-societal levels (Echchabi and Aziz 2012).
Several researches (Amin 2012; Amin et al. 2011; Sun et al. 2012) have focused directly on examining the relationship of religious obligation with behavioral intention. For example, the study by Alam et al. (2012) found that religiosity is a significant factor on the intention to undertake Islamic home financing among Muslims in Klang Valley. Similarly, Sun et al. (2012) examine religious and commitment and perceived attributes of Islamic mobile banking service adoption among 135 Southeast Asian young adults, and findings from the multiple regression analysis reveal that Islamic mobile phone banking is moderated by religious affiliations and commitment. Ong and Moschis (2006) and Mokhlis (2006) have documented the importance of religiosity in determining one’s consumption behavior.
In the context of this study, religious duties refer to the degree to which a person believes that participating in Waqf giving would be of religious influence, as it is strongly encouraged in Islam in order to earn mardhatillah (Allah ’s blessings ). It is therefore expected that religious duties would have positive relationship with attitude, intention, and the actual support for the construction of modern Waqf-based hospital in Uganda.
3.5 Intention
Intentions are assumed to capture the motivational factors that influence behavior; they are indications of how hard people are willing to try, of how much of an effort they are planning to exert, in order to perform the behavior. The stronger the intention to engage in a behavior, the more likely is the performance. These intentions remain behavioral characters until, at the appropriate time and opportunity, an attempt is made to translate them into action.
Empirical studies on Waqf giving behavior intention have yet to be documented although such acts have been strongly emphasized in Islamic heritage. For example, the beloved Prophet Muhamad (pbuh) mentioned in his hadith pertaining to intention and action:
Verily actions are by intentions, and for every person is what he intended, so the one whose hijrah was to Allah and His messenger, then his hijrah was to Allah and His messenger, and the one whose hijrah was for the world to gain from, or for a woman to marry, then his hijrah was to what he made hijrah for (Al-Bukhari).
The hadith mentions that every action or behavior is determined by the individual’s intention, which is the basic criteria for every act in all spheres of the individual’s life such as religious , social, economic, and political. Ajzen (1985) theories about intention support what had been said by the Prophet Muhamad (pbuh) several centuries ago. Fishbein and Ajzen (1975) define intention as a person’s readiness to do or perform a particular behavior as a result of two influential factors, namely attitude and subjective norm. Therefore, intention is expected to have positive relationship with the actual support for the construction of modern Waqf-based hospital in Uganda .
3.6 Financial and Non-Financial Support (Charity)
As discussed earlier, this chapter examines the extent to which attitude, moral duties , religious duties, and perceived behavioral control can translate the intention of donors into actual financial and non-financial support (in this case charity) toward the establishment of Waqf-based hospital in Uganda . Charity is a universal value although the motive toward giving behavior can ideologically vary.
Islam views charity not only as a means of wealth transfer to the poor but also as a mechanism for self-development and an avenue for seeking Allah ’s pleasure and His reward in the Hereafter. Thus, the motive for giving alms is solely to seek Allah’s pleasure. Allah says in the Quran: “It is neither their meat nor their blood that reaches Allah, but it is piety from you that reaches Him” (22:37).
In the Western worldview , the motives for giving charity include social desirability, career advancement, religious , expectations of respect and recognition, positive attitudes toward community as well as altruism or humanitarian (Olson 1965; Becker 1974; Arrow 1975; Andreoni 1989, 1990; Rose-Ackerman 1997). According to Laffont (1975), individuals choose action they would mostly prefer everyone would choose when donating to charities or supplying public goods. He analyzes the case where individuals believe that others will act as they do, then maximize their utility given this belief. Under these beliefs, he shows that individuals voluntarily contribute certain amount toward public goods and social welfare, with the hope that others will do the same. While Andreoni (1989) argues that individuals may be motivated by altruism, this depends on the extent to which they care about the level of public goods produced, warm glow, and their own responsibility for the production of these public goods.
Andreoni (1990) added that when people donate to privately provided public goods, they may not only gain utility from increasing its total supply, but they may also gain pleasure from the act of giving (warm glow). Rose-Ackerman (1997) argues that some people give to charity because of the result of feelings of commitment; some results from sympathy; some arises from belief in the moral value of reciprocity; and some is motivated by private benefits of the donor such as prestige, pride, and attendance at elite parties. Motivations for giving are inextricably linked. One can obtain prestige from making a gift only if others view one’s action as worthy. If the narrow private benefits of giving gifts are too obvious and large, gift givers will not be praised for their self-sacrifice (Rose-Ackerman 1997). Johnson (1968) opines that an individual will donate to charity only to avoid “societal costs” in the form of social pressure and religious belief. The height of societal costs depends on the folkways and custom of the society, the type, and the quantity of the public good as well as the social position and wealth of the individuals in question.
4 Conceptual Framework
Based on the literature survey, we develop a conceptual framework to investigate the extent to which attitude, moral duties , perceived behavioral control, and religious duties translate the intention of Muslim community in Uganda into actual financial and non-financial support for the construction of Waqf-based hospital . Figure 9.2 shows the conceptual framework of the study adapted from the TPB.

Source author’s own illustration based on TPB
Conceptual framework.
4.1 Hypotheses
Based on the literature review and the adapted TPB, the following hypotheses were developed to test the relationships between the dependent and independent variables:
- H1:
-
There is a significant and positive relationship between Muslims attitude, intention, and the actual support for the construction of modern Waqf-based hospital in Uganda .
- H2:
-
There is a significant and positive relationship between Muslims commitment to fulfill their moral duties , intention, and the actual support for the construction of modern Waqf-based hospital in Uganda .
- H3:
-
There is a significant and positive relationship between perceived behavioral control (such as abilities and willingness to donate), intention, and the actual support for the construction of modern Waqf-based hospital in Uganda .
- H4:
-
There is a significant and positive relationship between Muslims commitment to fulfill their religious duties, intention, and the actual support for the construction of modern Waqf-based hospital in Uganda .
4.2 Research Methodology
This study has used quantitative research method for data collection (self-administered survey) and analysis. According to Burns and Bush (2000), a survey is a suitable method for collecting data about attitudes and opinions. It also allows quantitative analysis to be conducted in the testing of inferences and permits generalization of findings. The process of developing the questionnaire began with an extensive survey of the related literature. The literature survey provided bases for identifying the relevant variables and related instruments that were used in past studies. The questionnaire was designed based on the Likert scale that consisted of statements that express agreement and disagreement of the respondents toward the object of interest (Cooper and Schindler 2006). The Likert scale is easy to develop, easy for the respondents to answer questions, and is reliable (Emory 1985). Therefore, this study used four-point Likert scale, and the responses ranges from “agree to strongly agree” to “disagree and strongly disagree” for all the questions in the questionnaire. Cronbach’s Alpha test was conducted to measure reliability of the instrument. A total of 330 questionnaires were distributed to the Muslim population across the central, southern, and northern Uganda . Respondents were classified by gender, age, marital status, and education level. The study used SPSS for descriptive analysis and reliability test and later adopted AMOS software for Confirmatory Factor Analysis (CFA), Measurement Model, and Structural Equation Modeling (SEM), which is considered a superior method of analysis for multivariate behavioral research that involves a complex structural relationship among variables (Buhi et al. 2007).
5 Results and Discussion
This section presents the findings from the quantitative survey. The section comprises the profiles of the respondents , analysis of the SEM results, and results of the hypotheses testing.
5.1 Profile of the Respondents
The majority of the respondents are: male (68%), young—aged between 20–30 years (42%) and 31–40 age group (33%), educated class comprising degree holders (47%), middle-income earners (31%) and work as professionals (24%) , academicians (11%), and business community (22%) . Twenty-four percent (24%) had more than 10 years work experience, and 37% worked between 5–10 years. Hence, the respondents represent young male Muslims who are professionals, educated, well-informed, and of middle-income section of the society. This reflects positively on the quality of the data collected.
5.2 Reliability Statistics, Fitness of SEM, and Results of Hypotheses Testing
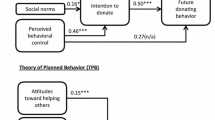
The Cronbach’s alpha obtained a value of 0.791, which indicates a satisfactory level of internal consistency, and the scale can be considered reliable with our sample (Tabachnick and Fidell 2001). A total of 300 questionnaires, representing 83% of the responses were collected as valid and complete. The SEM results show that the model is acceptable as it obtained the required values for each of the indices such as CFI = 0.990 and RMSEA = 0.046. Figure 9.3 shows Structural Model of the overall model fit. The figure shows the intention–behavior relationships, which connect religious obligations, moral norms , behavioral intention, and actual behavior.

Source authors’ own computation
Relationship between intention to support the construction of Waqf-based hospital and actual behavior.
Accordingly, the model supports the four hypotheses, i.e., there are significant and positive relationships between the four antecedents (attitudes, moral duties , perceived behavioral control, and religious duties), intentions, and the actual support for the construction of modern Waqf-based hospital in Uganda . In other words, the model predicts that positive attitude, positive perceived behavioral control, and commitments to fulfill both the religious and moral duties will positively influence the decision of Muslim community to provide actual financial and non-financial support for the construction of modern Waqf-based hospital in Uganda.
Meanwhile, the regression’s weights that substantiate the findings given by AMOS 5.0 are reported in Table 9.1. Overall, regression model reveals significant and positive relationship among the variables at p-value greater than 0.05, and the path coefficients of the causal structure are statistically significant at C.R above 5.00.
The results in Table 9.1 reveal that there are positive and significant relationships between three antecedents (attitude, moral duties , and religious duties), intentions, and actual financial and non-financial support for the construction of modern Waqf-based hospital in Uganda , β = 0.54, C.R = 6.42. In addition, desire to assist others for a noble cause (β = 0.62), for humanity (β = 0.78), for seeking the pleasure of Allah (β = 0.61), and His rewards in the Hereafter (β = 0.75) positively and significantly influence the decision of Muslim community to support the construction of modern Waqf-based hospital in Uganda financially (β = 0.784) and non-financially (β = 0.736). In other words, Muslim community in Uganda in reality will support (financially and non-financially) the constructions of modern Waqf-based hospital because of humanity, a belief that it is a social responsibility to help the poor and the needy to get decent and affordable health care services (moral duties), it is an avenue to seek Allah’s pleasure and His rewards in the Hereafter (religious duties), and also due to the belief that it is a virtue or noble cause to assist in the construction of Waqf-based hospital so that every individual will have equal access to affordable good health care services irrespective of their income status (attitude). These findings are consistent with many studies on altruism and donors giving behavior.
6 Conclusion
In nutshell, this study has predicted that intentions to endow for the construction of modern Waqf-based hospital can be materialized in the form of financial and non-financial support. Commitment to fulfill both moral and religious obligations and believe in noble cause will positively and significantly influence Muslim community’s intentions to actually provide financial and non-financial support for the construction of modern Waqf-based hospital in Uganda . It is, therefore, imperative for Islamic religious institutions in Uganda including Uganda Muslim Supreme Council (UMSC), which is the highest body managing the affairs of Muslim community in the country, to emphasize on these three motivating factors when they want to raise fund for the construction of Waqf-based hospital and other projects. These factors will influence Muslims decision to donate for socioeconomic development. This in turn will improve on the social welfare of Muslim community in Uganda.
References
Ajzen, I. (1985). From intentions to actions: A theory of planned behavior. Germany: Springer-Verlag.
Ajzen, I. (1991). The theory of planned behavior. Organizational Behavior and Human Decision Processes, 50(2), 179–211.
Ajzen, I. (2011). The theory of planned behaviour: Reactions and reflections. Psychology & Health, 26, 1113–1127.
Ajzen, I., & Fishbein, M. (1975). Belief, attitude, intention, and behavior: An introduction to theory and research (1st ed.). Reading, Mass: Addison-Wesley Pub. Co.
Ajzen, I., & Fishbein, M. (1977). Attitude-behavior relations: A theoretical analysis and review of empirical research. Psychological Bulletin, 84(5), 888–918.
Ajzen, I., & Fishbein, M. (1980). Understanding attitudes and predicting social behavior. Upper Saddle River, NJ: Prentice-Hall Inc.
Alam, S. S., Janor, H., Zanariah, Che-Wel, C. A., & Ahsan, M. N. (2012). Is religiosity an important factor in influencing the intention to undertake Islamic home financing in Klang Valley? World Applied Sciences Journal, 19(7): 1030–1041.
Amin, H. (2012). Patronage factors of Malaysian local customers toward Islamic credit cards. Management Research Review, 35(6), 512–530. https://doi.org/10.1108/01409171211238271.
Amin, H., & Chong, R. (2011). Is the theory of reasoned action valid for Ar-Rahnu? An empirical investigation. Australian Journal of Basic and Applied Sciences, 5(10), 716–726.
Amin, H., Abdul-Rahman, A. R., Chooi Hwa, A. M., & Sondoh, S. L., Jr. (2011). Determinants of customers’ intention to use Islamic personal financing: The case of Malaysian Islamic banks. Journal of Islamic Accounting and Business Research, 2(1), 22–42.
Andreoni, J. (1989). Giving with impure altruism: Applications to charity and Ricardian equivalence. Journal of Political Econom, 97(6), 1447–1458.
Andreoni, J. (1990). Impure altruism and donations to public goods: A theory of warm—glow giving. Economic Journal, 100(401), 464–477.
Arrow, K. J. (1975). Gifts and exchanges. In E. S. Phelps (Ed.), Altruism, morality and economic theory. New York: Russell Sage Foundation.
Astrom, A. N., & Rise, J. (2001). Young adult’s intentions to eat healthy food: Extending the theory of planned behavior. Psychology and Health, 16(2), 223–237.
Basar, H. (1987). Management and development of Awqaf properties. Jeddah: Islamic Research and Training Institute, Islamic Development Bank.
Becker, G. S. (1974). A theory of social interactions. Joumal of Political Economy, 82(2), 1063–1093.
Bozionelos, G., & Bennet, P. (1999). The theory of planned behavior as predictor of exercise: The moderating influence of beliefs and personality variables. Journal of Health Psychology, 15, 383–405.
Buhi, E., Goodson, P., & Neilands, T. (2007). Structural equation modeling: A primer for health behavior researchers. American Journal of Health Behaviors, 31(1), 74–85.
Burns, A. C., & Bush, R. F. (2000). Marketing research. London: Prentice Hall.
Conner, M., Norman, P., & Bell, R. (2002). The theory of planned behaviour and healthy eating. Health Psychology, 21(2), 195–201.
Cooper, D. R., & Schindler, P. S. (2006). Business research methods (9th ed.). USA: McGraw-Hill.
Echchabi, A., & Aziz, H. A. (2012). The relationship between religiosity and customers’ adoption of Islamic banking services in Morocco. Arabian Journal of Business and Management review (OMAN Chapter), 1(10), 89–94.
Echchabi, A., & Olaniyi, O. N. (2012). Using theory of reasoned action to model the patronisation behaviour of islamic banks’ customers in malaysia. Research Journal of Business Management, 6, 70–82.
Emory, W. C. (1985). Business research methods (3rd ed.). Homewood, Ill: Irwin. ISBN: 9780256030099.
Giles, M., & Cairns, E. (1995). Blood donation and Ajzen’s theory of planned behavior: An examination of perceived behavioural control. British Journal of Social Psychology, 34(2), 173–188.
Human Development Report. (2013). Key to HDI countries and ranks, 2012. New York: United Nations development Programme. Online Source at: http://hdr.undp.org/en/2013-report.
ILO. (2008). Social health protection: An ILO strategy towards universal access to health care, Social Security Policy Briefings, Paper No 1, Social Security Department, Geneva: International Labour Organisation.
Johnson, D. (1968). The fundamental economics of the charity market. PhD Dissertation, University of Virginia.
Johor Corporation. (2013). Annual report. Online source, available at: http://www.jcorp.com.my/waqaf-an-nur-hospital-clinics-35.aspx.
Kamri, N. (2010). The roles of ethics in waqf management: Case of jawhar. Shariah Journal, 18(3), 659–680.
Konkoloy, T. H., & Perloff, R. M. (1990). Applying the theory reason action to charitable intent. Psychological Report, 67(1), 91–94.
Kotler, P., & Keller, K. L. (2012). Marketing management (Vol. 14). New Jersey: Pearson-Prentice Hall.
Lada, S., Harvey Tanakinjal, G., & Amin, H. (2009). Predicting intention to choose halal products using theory of reasoned action. International Journal of Islamic and Middle Eastern Finance and Management, 2(1), 66–76.
Laffont, J. J. (1975). Macroeconomic constraints, economic efficiency and ethics: An introduction to kantian economics. Economica, 42, 430–437.
Lamiraud, K., Boysen, F., & Scheil-Adlung, X. (2005). The impact of social health protection on access to health care, health expenditure and impoverishment: A case study of South Africa, Extension of Social Security Paper Series 23, Geneva: International Labour Organisation.
Linden, S. (2011). Charitable intent: a moral or social construct? A revised theory of planned behavior model. Current Psychology, 30(4), 355–374.
McMillan, B., & Conner, M. (2003). Using the theory of planned behavior to understand alcohol and tobacco use in students. Psychology, Health and Medicine, 8, 317–328.
Mokhlis, S. (2006). The effect of Religiosity on shopping orientation: An exploratory study in Malaysia. Journal of American Academy of Business, 9(1), 64–74.
Olson, M. (1965). The logic of collective action. Harvard University Press.
Ong, F. S., & Moschis, G. P. (2006). Religiosity and consumer behaviour: A cross cultural study. Paper presented at the BAI Conference Proceedings. Singapore, July 12–14.
Osman, A. F., Muhammed, M. O., & Amin, H. (2014). An analysis of cash waqf participation among young intellectual. Paper published in Book Article. Waqf Iqlimi. Universiti Sains Islam Malaysia.
Rose-Ackerman, S. (1997). Altruism, nonprofits, and economic theory. Journal of Economic Literature, 34(2), 701–728.
Ryan, M. J., & Bonfield, E. H. (1980). Fishbein’s intentions model: A test of external and pragmatic validity. Journal of Marketing, 44(2) (Spring, 1980), 82–95.
Salamon, L. M. (1999). America’s nonprofit sector: A primer (2nd ed.). New York: Foundation Center.
Salamon, L. M., Sokolowski, S. W., & Anheier, H. K. (2000). Social origins of civil society: An overview. Baltimore, MD: The Johns Hopkins University Center for Civil Society Studies.
Scheil‐Adlung, X, Guy, C., Johannes, J., & Ke, X. (2006). What is the impact of social health protection on access to health care, health expenditure and impoverishment? A comparative analysis of three African countries, Extension of Social Security Paper Series 24, Geneva: International Labour Organisation.
Sen, A. K. (2000). Development as freedom. New York: Anchor Books.
Shih, Y. Y., & Fang, K. (2004). The use of a decomposed theory of planned behaviour to study internet banking in Taiwan. Internet Research, 14(3), 213–223.
Smith, R., & Mcsweeney, J. (2007). Charitable giving : The effectiveness of a revised theory of planned behaviour model in predicting donating intentions and behaviour. Journal of Community and Applied Social Psychology, 17(5), 363–386.
Sparks, P., & Shepherd, R. (1992). Self-identity and the theory of planned behavior: Assessing the role of identification with green consumerism. Social Psychology Quarterly, 55, 388–399.
Sun, S., Goh, T., Fam, K. S., & Xue, Y. (2012). The influence of religion on Islamic mobile phone banking services adoption. Journal of Islamic Marketing, 3(1), 81–98.
Tabachnick, B. G., & Fidell, L. S. (2001). Using multivariate statistics (4th ed.). Allyn and Bacon. [2007].
Victor, R. F. (2004). Reflections on the socio-economic correlates of health. Journal of Health Economics, 23(6), 1083–1099.
Warburton, J., & Terry, D. J. (2000). Volunteer decision making by older people: A test of a revised theory of planned behavior. Basic and Applied Social Psychology, 22(3), 245–257.
Weisbrod, B. (1998). To profit or not to profit: The commercial transformation of the nonprofit sector. New York: Cambridge University Press.
WHO. (2008 & 2009). Uganda cooperation strategy 2009–2014. Geneva: World Health Organisation. Online Source at http://www.who.int/nha/en.
WHO. (2013 & 2014). Health expenditure. Geneva: World Health Organisation. Online Source at http://apps.who.int/gho/data/view.main.HEALTHEXPRATIOUGA?lang=en.
Yousafzai, S. Y., Foxall, G. R., & Pallister, J. G. (2010). Explaining internet banking behaviour: Theory of reasoned action, theory of planned behavior, or technology acceptance model. Journal of Applied Social Psycholology, 40, 1172–1202.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2017 The Author(s)
About this chapter

Cite this chapter
Mohammed, M.O., Ahmed, U. (2017). Relationship Between Intention and Actual Support Toward the Construction of Modern Waqf-Based Hospital in Uganda. In: Zulkhibri, M., Ismail, A. (eds) Financial Inclusion and Poverty Alleviation. Palgrave Studies in Islamic Banking, Finance, and Economics. Palgrave Macmillan, Cham. https://doi.org/10.1007/978-3-319-69799-4_9
Download citation
DOI: https://doi.org/10.1007/978-3-319-69799-4_9
Published:
Publisher Name: Palgrave Macmillan, Cham
Print ISBN: 978-3-319-69798-7
Online ISBN: 978-3-319-69799-4
eBook Packages: Economics and FinanceEconomics and Finance (R0)