
Abstract
Subtrochanteric femur fractures are significant injuries that despite surgery can lead to relatively high rates of nonunion, malunion, and subsequent poor clinical outcomes.
Access provided by CONRICYT-eBooks. Download chapter PDF
Similar content being viewed by others

Introduction and Epidemiology
Subtrochanteric femur fractures are significant injuries that despite surgery can lead to relatively high rates of nonunion, malunion, and subsequent poor clinical outcomes.
Overall, subtrochanteric femur fractures comprise 10–34% of all hip fractures [1]. Several retrospective studies report a bimodal distribution among patients [2,3,4,5]. Velasco and Comfort reported that 63% of subtrochanteric fractures occurred in patients 51 years and older and 24% in patients between the ages of 17 and 50 years [4]. Younger patients sustain the fractures via high-energy mechanisms, while older individuals via lower-energy mechanisms as well as bisphosphonate-associated insufficiency fractures [2, 6,7,8]. A review of subtrochanteric fractures at a Level I trauma center, by Bergman et al., noted an average age of 40 years in the high-energy trauma group and 76 years in the low-energy trauma group [2].
An understanding of the relevant anatomy and biomechanics of the proximal femur has helped define operative management for subtrochanteric fractures. Advances in engineering and manufacturing of new implants [9,10,11] have provided hardware with greater strength and overall fatigue life. In addition to managing the deforming anatomical forces, the surgeon must chose an implant design that is able to withstand the large biomechanical forces subjected to the subtrochanteric region [12]. The use of cephalomedullary locked nails and open indirect reduction techniques that preserve the soft tissue envelope and vasculature has resulted in a reduction of postoperative nonunions [13,14,15,16,17,18,19]. With an understanding of each patient and their fracture patterns, the surgeon can strategically choose the appropriate treatment to improve their patient’s clinical outcomes.
Relevant Anatomy and Biomechanics
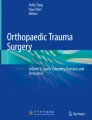
The subtrochanteric region of the femur is defined from the lesser trochanter to 5 cm distal to the lesser trochanter. These fractures can often extend into the intertrochanteric region and are called “pertrochanteric” fractures or intertrochanteric fractures with subtrochanteric extension. Proximal femoral anatomy causes powerful deforming forces that create characteristic, complex fracture pattern. The typical radiographic appearance consists of a proximal fragment that is in varus, abduction, and external rotation, while the distal fragment is adducted (Fig. 9.1). The pull of specific muscle groups in the proximal femur results in this characteristic deformity. The gluteal muscles, the iliopsoas, and the short external rotators are responsible for the proximal segment external rotation, while the gracilis, adductor brevis, adductor longus, and adductor magnus adduct the distal femoral shaft.

Anteroposterior (AP) radiograph exhibiting a comminuted subtrochanteric femur fracture with shaft extension. Note the proximal fragment in abduction, external rotation, and flexion, the typical appearance of this fracture pattern
Biomechanically, the forces about the proximal femur are some of the highest seen in the human body. The earliest studies by Koch first analyzed the mechanical stresses on the femur during weight bearing. He showed that up to 1200 lb/inch2 of force could be generated in a 200-lb man. Compression stress exceeds 1200 lb/inch [2] in the medial subtrochanteric area 1–3 inches distal to the level of the lesser trochanter. Lateral tensile stresses are approximately 20% less [12]. While Koch’s analysis was correct for the forces on the femur, he did not take into account the additional stress from the muscle forces [20]. Frankel and Burstein demonstrated a significant force on the hip and proximal part of the femur from flexion and extension of the hip while lying in bed, thus indicating continuous stress on a proximal femoral fixation device even with the patient at bedrest [21]. An analysis by Fielding et al. demonstrated that a medial cortical buttress was required to minimize local stress in the subtrochanteric region. They showed that nonunion results from fatigue failure of a fixation device and that nonunion is actually the cause of implant failure [22]. Higher bending forces are applied to an extramedullary device on the lateral femur than an intramedullary device, which is closer to the line of joint reaction force [23]. Froimson’s description of muscle forces aids our understanding of subtrochanteric fracture displacement and also suggests how such fractures can be reduced [24]. These deforming forces create the obstacles to gaining appropriate reduction. Proper application of tools and implants has helped individuals gain successful reduction of these complex fractures.
Classification
There are over 15 described classifications of subtrochanteric fractures in the literature [25]; however, the Russell and Taylor and the AO/OTA classifications have historically been the most widely reproducible [26, 27]. The Russell and Taylor classification was historically used to differentiate fractures that could be fixed with an intramedullary nail (Type I) or whether a lateral fixed angle device would be required (Type II). Type I fractures do not extend into the piriformis fossa (Type IA, no extension into the lesser trochanter; Type IB, extension to the lesser trochanter). Type II fractures extend into the piriformis fossa (Type IIA, no comminution of lesser trochanter; Type IIB, comminution of lesser trochanter) [26]. This classification has since lost favor due to the development of interlocking nails utilizing both trochanteric and piriformis starting points allowing (Table 9.1). These operative modifications have allowed Type II fractures to be treated with intramedullary devices.
The AO/OTA classification , typically the most widely used, takes into account the bone, the location, the energy of the trauma, and the mechanism [27]. Conventionally subtrochanteric fractures are categorized along with other diaphyseal femur fractures (Table 9.2). The AO/OTA classification is the most widely used in the literature for research; however, in practice, subtrochanteric fractures are typically described by its location and any fracture extension and/or severity of comminution.
Initial Evaluation, Work-Up, and Management
Subtrochanteric fractures, especially in the young patient, typically involve high-energy mechanisms and must be evaluated for other associated injuries. A primary survey under the ATLS guidelines is essential [28, 29]. Life-threatening injuries must be identified and resuscitative measures initiated. The secondary survey should be performed later as part of a more detailed head to toe examination. Critically ill, multiply injured patients should be evaluated and temporarily stabilized and resuscitated.
In the older individual with a lower mechanism of injury, a detailed history of how the accident occurred should be performed to uncover any possible comorbidities leading to injury. If the patient had a syncopal episode resulting in a fall, then an appropriate work-up must be conducted before the patient can be cleared for any surgical intervention. The patient’s medication history must be evaluated for the use of bisphosphonates. Recent studies have shown that chronic bisphosphonate therapy for more than 3–5 years may increase the risk of atypical femoral fractures [6,7,8]. In regard to bisphosphonates, prodromal thigh pain as well as contralateral imaging should be performed. Concern for insufficiency fracture can be diagnosed further with advanced imaging such as magnetic resonance imaging, CT, or bone scan [30,31,32,33,34].
On physical examination when the fracture is displaced, the injured extremity is most often shortened and externally rotated. The thigh may be swollen and can at times have a bony prominence from the deforming forces acting on the proximal fragment. Patients are unable to actively flex their hip or tolerate any range of hip motion. The patient is usually neurologically intact without vascular deficit. Penetrating injuries, on the other hand, can cause neurovascular injury to the surrounding structures and must be carefully evaluated. Initial diagnostic studies should include plain radiographs consisting of anteroposterior (AP) and cross-table views of the hip along with full-length femur views. An AP pelvis view (typically obtained during the trauma work-up) can be helpful in assessing femoral neck/shaft morphology of the uninjured side.
The characteristics of an atypical fracture due to long-term bisphosphonate use on radiographic evaluation include lateral cortical thickening, transverse fracture orientation, lack of comminution, and medial cortical spike [7]. Diagnostic studies on the contralateral side are indicated if the patient has any history of thigh pain on the contralateral side of the injury. A recent retrospective study by Saleh et al. suggested that if a symptomatic patient taking long-term bisphosphonate therapy presents with lateral cortical thickening and no radiolucent line, then discontinuation of bisphosphonate treatment and conservative treatment with teriparatide can resolve the fracture [35]. When a radiolucent line is visible along with lateral cortical thickening, then surgical prophylaxis is recommended to prevent propagation to a complete fracture [7, 8, 35]. Identification of an occult fracture will change the clinical course of the patient providing a definitive medical management and a shorter hospital stay [36].
Initial management includes proper evaluation and hemodynamic resuscitation, if needed. Skeletal traction via a distal femoral or proximal tibial traction pin not only restores length but also can provide considerable pain relief. Skin traction (i.e., Buck’s traction) is also an alternative [37] but will not restore femoral length. Medical optimization prior to operative intervention is of paramount importance.
Nonoperative Management
Due to the high morbidity and mortality, nonoperative management is truly reserved for those in severe extremis that will likely succumb to other organ injuries [38]. Alternatively, those patients in end-of-life care that choose not to undergo operative fixation may opt for nonoperative management but should only do so after a long discussion with the patient and the family. Even in those patient populations (and even in those nonambulatory), operative stabilization of the femur can offer benefits not only in regard to pain relief but also to their caregivers, as it will facilitate easier hygiene care and the ability to transfer.
Operative Management
Intramedullary Locked Nail
The intramedullary locked nail is the gold standard for fixation of acute subtrochanteric femur fractures. Biomechanically, there are several advantages when using the intramedullary nail compared to plate and screws. The nail provides increased rigidity, shorter moment arm, and bending stiffness [39]. The intramedullary nail provides more efficient shared load transfer while resisting deforming forces of medialization from the adductor muscles [11, 40, 41].
There are several IM nail types available for treatment of subtrochanteric fractures. The cephalomedullary hip nail (Fig. 9.2a, b) is most often used in older patients or those with poor bone stock; it utilizes a large threaded screw for stability and protection of the femoral neck. In the younger patient, with healthy bone, a smaller diameter (reconstruction) intramedullary nail (Fig. 9.2c, d) with two smaller screws into the femoral neck can be used to avoid a large screw tract while providing rotational stability of the proximal fragment. Some reconstruction nails incorporate a proximal crossing screw configuration, which has one screw up through the femoral neck and one screw from the greater trochanter to the lesser trochanter. A biomechanical study by Grisell et al. comparing the cross-screw configuration to the parallel screw configuration showed greater axial failure loads and significantly higher stiffness in the cross-screw technique [10].

(a, b) In the elderly, cephalomedullary IMN utilizing a single lag screw can be sufficiently utilized, while in the younger patient, (c, d) smaller bore reconstruction-type screws can offer less bone loss and more rotational control with two points of fixation
There are several options for positioning of the patient for IM nailing. Placing the patient supine on or off a fracture table allows for easier imaging and intraoperative traction of extremities for polytrauma mechanisms. The patient can also be placed lateral on a fracture table or a radiolucent flat table. Placing a patient lateral will allow the distal fragment to flex matching the proximal fragment. This position allows for easier access to the starting point in heavier people with adduction allowing for access.
An important step in ensuring proper fracture reduction is achieving the ideal starting point in either the piriformis fossa or trochanteric tip [14, 42]. Historically, the piriformis starting point was used with straight intramedullary nails. However, an improper piriformis start point can lead to fracture malalignment and increased fracture comminution, and if too anterior, increased hoop stresses can lead to femoral bursting of the proximal femoral fragment [40].
More recently manufactured intramedullary nails were designed for use through a trochanteric starting point . These intramedullary nails have a built-in proximal bend of 4–6° to help prevent varus malreduction. Although the starting point allows for a more subcutaneous landmark, a perfect starting point is still vital for a successful outcome [43, 44]. The starting point needs to be slightly more medial in order to avoid varus malreduction, which can still occur despite the proximal bend [43]. A cadaveric study analyzing the greater trochanters in 100 specimens found that only 63% had an unobstructed ideal entry point, whereas the remaining 37% all had some degree of obscuring of the entry portal [9].
After the ideal starting point is obtained, there are a number of strategies that can be used to further help achieve proper alignment of the fracture (Fig. 9.3a–c). While traction can restore femoral length, the powerful deforming forces of the proximal femoral segment can result in varus and flexion malalignment. In two-part subtrochanteric fractures, the “finger” or cannulated reduction tool can be passed down the canal to provide stabilization and allow passage of the guide wire down an ideal path [45]. Blocking screws can be placed in the concavity of the fracture in comminuted fractures that span longer distances in the subtrochanteric region [45]. A small open incision can be made for any fracture pattern to allow room for clamps to provide efficient fixation while reaming and placement of the intramedullary nail [46,47,48]. Despite using an open technique for fracture reduction, union rates have remained high with intramedullary locked nails [46, 47].

Reduction aids include the use of the (a) “finger,” which is a stiff reduction aid that can help temporarily align the fracture to help pass the guide wire; (b) blocking screws (or a blocking drill bit or Schanz pin) can aid in maintaining nail position as well as reduction; (c) a small, open incision (often the same used for the cephalomedullary screws) can be utilized to place a clamp which can reduce the fracture and facilitate facile IMN placement
The most common pitfalls in operative management of subtrochanteric femur fractures include varus malreduction, rotational malreduction, leg length discrepancy, and missed ipsilateral injury. Obtaining anatomical reduction is required prior to placement of any IMN. The standard construct is an anterograde, long, reamed, statically locked cephalomedullary nail [10, 19, 49]. While there lacks high-level evidence, this construct is widely accepted as the standard due to its inherent biomechanical strength aided by a locked, long working length which allows for reliable, immediate weight bearing. Biomechanically, dual cephalomedullary screws (crossing or parallel) are stronger than a single screw, and two distal locking screws are stronger than one; there is no clinical evidence to support one or the other [10, 19, 49]. When postoperative radiographs demonstrated malreduction greater than or equal to 10° in any plane, there was a statistically significant higher rate of delayed or nonunion [50]. In comminuted fractures, preoperative imaging of the contralateral leg can help avoid leg length mismatch and rotational malreduction. The femoral neck should be heavily scrutinized with fluoroscopy at the beginning and end of the case to prevent missed ipsilateral injuries. A proper knee exam before leaving the operating room is necessary to avoid missing ipsilateral knee injuries.
Overall the use of intramedullary locking nails for these fractures have a high rate of union and low rate of reoperation. The outcomes can be further divided in the high-energy mechanism group primarily involving younger individuals. An early series by Wiss showed 99% fracture union with the use of a piriformis start IM nail [13]. A more recent study by Starr et al. showed 100% union rate without the need for bone graft or a secondary procedure when using a cephalomedullary nail for young patients in high-energy mechanism accidents [14]. The second group of outcomes can be categorized by low-energy mechanisms most commonly seen in the elderly. The current approach is using a trochanteric entry point with a cephalomedullary hip nail. The elderly have an increased level of social dependence and far more comorbidities that predispose them to higher rates of reoperation, and an increase in mortality is seen at the 1-year mark postoperatively [51].
Fixed Angle Blade Plates
Fixed angle blade plates (Fig. 9.4a, b) have historically been successful in treating severely comminuted subtrochanteric fractures [52,53,54]. Kinast showed that using indirect reduction techniques significantly reduced nonunion rates to 0% when compared to direct reduction group [55]. Unfortunately, these results have not been reproducible as Brien et al. showed a nonunion rate of 32% when comparing the blade plate to interlocked IM nails [15]. Plate and screw techniques rely on obtaining compression and thus primary bone healing at the fracture site. The indirect reduction technique is predicated on accurate proximal fixation to ensure a proper neck shaft angle and adequate compression at the fracture site. Compared to IMN, blade plates are more technically difficult to use, and trainees are not exposed to the technique during training and thus have fallen out of favor for use as an initial treatment.

Traditionally, blade plates have been excellent options for treating subtrochanteric femur fractures in the acute period. (a) An AP hip radiograph exhibiting a subtrochanteric femur fracture, restoring length alignment and rotation with a (b) blade plate. With the advent of IMN, however, acute treatment with blade plates has fallen out of favor, avoiding the necessary excessive exposure (Images courtesy of Kenneth A. Egol, MD)
In most cases, the 95° blade plate fixation is reserved for fracture malunion or nonunion. Varus malalignment in subtrochanteric fractures can cause leg length discrepancies and decreases abductor working length. The corrective procedure is an osteotomy at the apex of the deformity with the use of a blade plate. Multiple studies have demonstrated that successful union can be obtained as long as there is stable proximal fragment fixation [52, 53].
Proximal Femoral Locking Compression Plates
The newest plate technology that is available for subtrochanteric femur fractures is the proximal femoral locking compression plate (PFL). This is another type of fixed angle plate. Biomechanical studies have shown that the PFL plate has more axial stiffness, less torsional stiffness, and equivalent irreversible deformation to cyclic axial loading when compared with the blade plate [56].
Comparison of PFL plate to intramedullary nail fixation showed no difference in the number of complications, onset of complications incidence, and time of full-weight bearing. Although the Harris Hip Score among patients improved in both methods of treatment, there was no difference between the two groups [57]. However, subsequent studies have not been able to reproduce similar results when comparing the PFL plate and locked intramedullary nails.
El-Desouky et al. showed PFL plate provided a strong construct for fixation of comminuted subtrochanteric fractures either by open or biological techniques. Unfortunately, low patient compliance was an influential factor for implant failure in both types [58]. While locked proximal femoral plates were created to address the technical difficulty associated with other fixed angle blade plates and provide a more rigid construct, the results following their use have demonstrated high rates of failure (Fig. 9.5) [59]. Fractures with posteromedial comminution [60] and atypical femoral fractures [61] treated with these implants have also had poor outcomes and high failure rates.

While early results and biomechanical studies were promising in regard to PFL plates, recent reports of hardware failure have increased concern for stricter indications and use (Images courtesy of Nirmal C. Tejwani, MD)
Only one study has demonstrated favorable outcomes with established nonunions of subtrochanteric femur fractures using the PFL plate [62]. However, due to the more recent evidence regarding high failure rates, surgeons’ use of the PFL plate is waning; higher-level studies or, perhaps, more specific criterion and/or technique must be set forth prior to more widespread use. More reliably, subtrochanteric nonunions without malalignment have shown high rates of fracture union and functional improvement with exchange nailing (with reduction) with or without bone grafting [53].
Special Consideration: Atypical Femoral Fractures
The operative management of patients with atypical femoral fractures introduces a few more issues that cannot be overlooked. Review of the radiographs for a lateral cortical thickening, transverse fracture orientation, lack of comminution, and medial cortical spike is essential [7]. These atypical fracture patterns have a higher rate of intraoperative femoral shaft comminution during nail insertion and a higher rate of iatrogenic fracture during nail placement [61]. There is also a higher rate of delayed union leading to higher rates of revision surgery [63]. Care must be taken to evaluate the patient for contralateral thigh as there is a high association with bilateral insufficiency fractures [64]. Comparing nonoperative versus operative management with prophylactic fixation of femoral stress fractures showed a decreased average hospital stay for those undergoing fixation [7]. Many of the femoral fractures in the nonoperative group eventually went on to completion and required operative fixation leading to a longer hospital stay [36].
Complications
Complications include nonunion, malunion, and infection. In regard to nonunion and malunion, typical causes are related to failure to obtain an anatomic reduction. These can occur for a myriad of reasons, which include utilizing an incorrect starting point and accepting too much flexion and/or varus, which occurs from a lack of reduction aid utilization [65]. Postoperative malunion can be problematic as any degree of external rotation causes a posterior shift of the weight-bearing axis in the sagittal plane and may lead to a change in gait mechanics [66]. One cannot emphasize the importance of obtaining an acceptable reduction prior to implant placement; placing the IMN in a malreduced fracture is the most common cause of malunion and nonunion. The IMN will not reduce the fracture and increases risk for nonunion and subsequent implant failure with loss of fixation. Nonunions and malunions can typically be treated via exchange nail (with re-reduction) or via corrective osteotomy and blade plate placement (Fig. 9.6a–d).

Subtrochanteric femur fracture nonunions (a, b) can be treated via exchange nail or via blade plate. (a) Here, a subtrochanteric femur fracture treated with a retrograde IMN went onto nonunion. (b) Exchange with an antegrade cephalomedullary nail and distal fixation provided the necessary environment for healing. Similarly, a failed cephalomedullary nail (c) construct left in varus was successfully treated via ORIF and (d) blade plate fixation (Images courtesy of Kenneth A. Egol, MD)
As with any surgery, infection is also a potential complication. Increased risk for infection can arise from host factors (i.e., diabetic, smoker, immunocompromised, etc.) and can occur in the acute postoperative period. Superficial infection and deep infection can occur, with increased risk associated with excessive soft tissue stripping, which can typically occur with large open exposures while attempting to obtain anatomic reduction. Treatment of deep infection depends on the amount of fracture healing. Although rare, a completely healed fracture with evidence of deep infection likely requires IMN removal. In the setting of a non-healed fracture, initial irrigation and debridement with an intravenous antibiotic course can be tried until the fracture heals. In the event of a deep infection and persistent nonunion, complete infection eradication is required for healing. Temporizing fixation can be obtained by utilizing an antibiotic-coated IMN. Laboratory markers are used after the completion of the antibiotic therapy to check for normalization of inflammatory levels. Once the infection has been eradicated, definitive fixation is then performed. Debridement of the bone can be supplemented with bone grafting to further enhance healing potential [67, 68].
Summary
Subtrochanteric fractures are generally treated with operative management. Occurring in a bimodal distribution, both high-energy mechanisms in the young and low-energy, possible bisphosphonate-related etiologies in the elderly must be evaluated and treated. Powerful deforming forces in the proximal femur that historically caused high rates of malreduction, shortening and nonunion, can be overcome via several reduction tools and techniques, including clamps, cerclage cables, blocking screws, and fragment controlling pins. Today, the standard treatment for subtrochanteric femur fractures is anterograde, reamed, statically locked, long, cephalomedullary nails. Biomechanically, two cephalomedullary screws along with two distal locking screws are the strongest. Blade plates and exchange nails are reliable treatments for nonunions/malunions, while recent reports exhibiting high failure rates have limited the use of PFL plate. Future research, involving higher-level evidence, is required to truly determine even more specific, ideal constructs and treatment algorithms for these difficult to treat fractures.
References
Boyd HB, Griffin LL. Classification and treatment of trochanteric fractures. Arch Surg. 1949;58(6):853–66.
Bergman GD, Winquist RA, Mayo KA, Hansen ST. Subtrochanteric fracture of the femur. Fixation using the Zickel nail. J Bone Joint Surgery Am. 1987;69(7):1032–40.
Robey LR. Intertrochanteric and subtrochanteric fractures of the femur in the Negro. J Bone Joint Surg Am. 1956;38-A(6):1301–12.
Velasco RU, Comfort TH. Analysis of treatment problems in subtrochanteric fractures of the femur. J Trauma. 1978;18(7):513–23.
Waddell JP. Subtrochanteric fractures of the femur: a review of 130 patients. J Trauma. 1979;19(8):582–92.
Goh SK, Yang KY, Koh JS, et al. Subtrochanteric insufficiency fractures in patients on alendronate therapy: a caution. J Bone Joint Surg Br. 2007;89(3):349–53.
Kwek EB, Goh SK, Koh JS, Png MA, Howe TS. An emerging pattern of subtrochanteric stress fractures: a long-term complication of alendronate therapy? Injury. 2008;39(2):224–31.
Lenart BA, Neviaser AS, Lyman S, et al. Association of low-energy femoral fractures with prolonged bisphosphonate use: a case control study. Osteoporos Int. 2009;20(8):1353–62.
Grechenig W, Pichler W, Clement H, Tesch NP, Grechenig S. Anatomy of the greater femoral trochanter: clinical importance for intramedullary femoral nailing. Anatomic study of 100 cadaver specimens. Acta Orthop. 2006;77(6):899–901.
Grisell M, Moed BR, Bledsoe JG. A biomechanical comparison of trochanteric nail proximal screw configurations in a subtrochanteric fracture model. J Orthop Trauma. 2010;24(6):359–63.
Kraemer WJ, Hearn TC, Powell JN, Mahomed N. Fixation of segmental subtrochanteric fractures. A biomechanical study. Clin Orthop Relat Res. 1996;332:71–9.
Koch JC. The laws of bone architecture. Am J Anat. 1917;21:177–298.
Wiss DA, Brien WW. Subtrochanteric fractures of the femur. Results of treatment by interlocking nailing. Clin Orthop Relat Res. 1992;(283):231–6.
Starr AJ, Hay MT, Reinert CM, Borer DS, Christensen KC. Cephalomedullary nails in the treatment of high-energy proximal femur fractures in young patients: a prospective, randomized comparison of trochanteric versus piriformis fossa entry portal. J Orthop Trauma. 2006;20(4):240–6.
Brien WW, Wiss DA, Becker V, Lehman T. Subtrochanteric femur fractures: a comparison of the Zickel nail, 95 degrees blade plate, and interlocking nail. J Orthop Trauma. 1991;5(4):458–64.
Forward DP, Doro CJ, OʼToole RV, et al. A biomechanical comparison of a locking plate, a nail, and a 95° angled blade plate for fixation of subtrochanteric femoral fractures. J Orthop Trauma. 2012;26(6):334–40.
French BG, Tornetta P. Use of an interlocked cephalomedullary nail for subtrochanteric fracture stabilization. Clin Orthop Relat Res. 1998;348:95–100.
Kummer FJ, Olsson O, Pearlman CA, Ceder L, Larsson S, Koval KJ. Intramedullary versus extramedullary fixation of subtrochanteric fractures. A biomechanical study. Acta Orthop Scand. 1998;69(6):580–4.
Pugh KJ, Morgan RA, Gorczyca JT, Pienkowski D. A mechanical comparison of subtrochanteric femur fracture fixation. J Orthop Trauma. 1998;12(5):324–9.
Rydell NW. Forces acting on the femoral head-prosthesis. A study on strain gauge supplied prostheses in living persons. Acta Orthop Scand. 1966;37(Suppl 88):81–132.
Frankel VH, Burstein AH. Orthopaedic biomechanics. Philadelphia: Lea & Febiger; 1970.
Fielding JW, Cochran GV, Zickel RE. Biomechanical characteristics and surgical management of subtrochanteric fractures. Orthop Clinics N Am. 1974;5(3):629–50.
Rybicki EF, Simonen FA, Weis EB. On the mathematical analysis of stress in the human femur. J Biomech. 1972;5(2):203–15.
Froimson AI. Treatment of comminuted subtrochanteric fractures of the femur. Surg Gynecol Obstet. 1970;131(3):465–72.
Loizou CL, McNamara I, Ahmed K, Pryor GA, Parker MJ. Classification of subtrochanteric femoral fractures. Injury. 2010;41(7):739–45.
Russell T, Taylor J. Subtrochanteric fractures of the femur. In: Browner BD, Jupiter JB, Levine AM, Trafton PG, editors. Skeletal trauma. Fractures, dislocations, ligamentous injuries. 1st ed. Philadephia: Saunders; 1992. p. 1485–524.
Muller ME, Nazarian S, Koch P. J. S. The AO classification of fractures of long bones. Berlin, Heidelberg: Springer-Verlag; 1990.
Hussmann B, Lendemans S. Pre-hospital and early in-hospital management of severe injuries: changes and trends. Injury. 2014;45(Suppl 3):S39–42.
Radvinsky DS, Yoon RS, Schmitt PJ, Prestigiacomo CJ, Swan KG, Liporace FA. Evolution and development of the advanced trauma life support (ATLS) protocol: a historical perspective. Orthopedics. 2012;35(4):305–11.
Yoon RS, Hwang JS, Beebe KS. Long-term bisphosphonate usage and subtrochanteric insufficiency fractures: a cause for concern? J Bone Joint Surg Br. 2011;93(10):1289–95.
Yoon RS, Beebe KS, Benevenia J. Prophylactic bilateral intramedullary femoral nails for bisphosphonate-associated signs of impending subtrochanteric hip fracture. Orthopedics. 2010;33(4). doi: 10.3928/01477447-20100225-21. Epub 2010 Apr 16. Epub 2010 Apr 16.
Kao CM, Huang PJ, Chen CH, Chen SJ, Cheng YM. Atypical femoral fracture after long-term alendronate treatment: report of a case evidenced with magnetic resonance imaging. Kaohsiung J Med Sci. 2012;28(10):555–8.
Bush LA, Chew FS. Subtrochanteric femoral insufficiency fracture following bisphosphonate therapy for osseous metastases. Radiol Case Rep. 2008;3(4):232.
Probst S, Rakheja R, Stern J. Atypical bisphosphonate-associated subtrochanteric and femoral shaft stress fractures: diagnostic features on bone scan. Clin Nucl Med. 2013;38(5):397–9.
Saleh A, Hegde VV, Potty AG, Schneider R, Cornell CN, Lane JM. Management strategy for symptomatic bisphosphonate-associated incomplete atypical femoral fractures. HSS J. 2012;8(2):103–10.
Banffy MB, Vrahas MS, Ready JE, Abraham JA. Nonoperative versus prophylactic treatment of bisphosphonate-associated femoral stress fractures. Clin Orthop Relat Res. 2011;469(7):2028–34.
Resch S, Thorngren KG. Preoperative traction for hip fracture: a randomized comparison between skin and skeletal traction in 78 patients. Acta Orthop Scand. 1998;69(3):277–9.
Zickel RE. Subtrochanteric femoral fractures. Orthop Clinics N Am. 1980;11(3):555–68.
Brumback RJ, Toal TR, Murphy-Zane MS, Novak VP, Belkoff SM. Immediate weight-bearing after treatment of a comminuted fracture of the femoral shaft with a statically locked intramedullary nail. J Bone Joint Surgery Am. 1999;81(11):1538–44.
Johnson KD, Tencer AF, Sherman MC. Biomechanical factors affecting fracture stability and femoral bursting in closed intramedullary nailing of femoral shaft fractures, with illustrative case presentations. J Orthop Trauma. 1987;1(1):1–11.
Wang J, Ma XL, Ma JX, et al. Biomechanical analysis of four types of internal fixation in subtrochanteric fracture models. Orthop Surg. 2014;6(2):128–36.
Ricci WM, Schwappach J, Tucker M, et al. Trochanteric versus piriformis entry portal for the treatment of femoral shaft fractures. J Orthop Trauma. 2006;20(10):663–7.
Ostrum RF, Marcantonio A, Marburger R. A critical analysis of the eccentric starting point for trochanteric intramedullary femoral nailing. J Orthop Trauma. 2005;19(10):681–6.
Ostrum RF, Levy MS. Penetration of the distal femoral anterior cortex during intramedullary nailing for subtrochanteric fractures: a report of three cases. J Orthop Trauma. 2005;19(9):656–60.
Yoon RS, Donegan DJ, Liporace FA. Reducing subtrochanteric femur fractures: tips and tricks, do’s and don’ts. J Orthop Trauma. 2015;29(Suppl 4):S28–33.
Afsari A, Liporace F, Lindvall E, Infante A Jr, Sagi HC, Haidukewych GJ. Clamp-assisted reduction of high subtrochanteric fractures of the femur. J Bone Joint Surg Am. 2009;91(8):1913–8.
Beingessner DM, Scolaro JA, Orec RJ, Nork SE, Barei DP. Open reduction and intramedullary stabilisation of subtrochanteric femur fractures: a retrospective study of 56 cases. Injury. 2013;44(12):1910–5.
Hoskins W, Bingham R, Joseph S, et al. Subtrochanteric fracture: the effect of cerclage wire on fracture reduction and outcome. Injury. 2015;46(10):1992–5.
Joglekar SB, Lindvall EM, Martirosian A. Contemporary management of subtrochanteric fractures. Orthop Clinics N Am. 2015;46(1):21–35.
Riehl JT, Koval KJ, Langford JR, Munro MW, Kupiszewski SJ, Haidukewych GJ. Intramedullary nailing of subtrochanteric fractures--does malreduction matter? Bull Hosp Joint Dis. 2014;72(2):159–63.
Robinson CM, Houshian S, Khan LA. Trochanteric-entry long cephalomedullary nailing of subtrochanteric fractures caused by low-energy trauma. J Bone Joint Surg Am. 2005;87(10):2217–26.
Barquet A, Mayora G, Fregeiro J, López L, Rienzi D, Francescoli L. The treatment of subtrochanteric nonunions with the long gamma nail: twenty-six patients with a minimum 2-year follow-up. J Orthop Trauma. 2004;18(6):346–53.
Haidukewych GJ, Berry DJ. Nonunion of fractures of the subtrochanteric region of the femur. Clin Orthop Relat Res. 2004;419:185–8.
Whatley JR, Garland DE, Whitecloud T, Whickstrom J. Subtrochanteric fractures of the femur: treatment with ASIF blade plate fixation. South Med J. 1978;71(11):1372–5.
Kinast C, Bolhofner BR, Mast JW, Ganz R. Subtrochanteric fractures of the femur. Results of treatment with the 95 degrees condylar blade-plate. Clin Orthop Relat Res. 1989;(238):122–30.
Crist BD, Khalafi A, Hazelwood SJ, Lee MA. A biomechanical comparison of locked plate fixation with percutaneous insertion capability versus the angled blade plate in a subtrochanteric fracture gap model. J Orthop Trauma. 2009;23(9):622–7.
Mirbolook A, Siavashi B, Jafarinezhad AE, et al. Subtrochanteric fractures: comparison of proximal femur locking plate and intramedullary locking nail fixation outcome. Indian J Surg. 2015;77(Suppl 3):795–8.
El-Desouky II, Mohamed MM, Kandil AE. Clinical outcome of conventional versus biological fixation of subtrochanteric fractures by proximal femoral locked plate. Injury. 2016;47(6):1309–17.
Glassner PJ, Tejwani NC. Failure of proximal femoral locking compression plate: a case series. J Orthop Trauma. 2011;25(2):76–83.
Wieser K, Babst R. Fixation failure of the LCP proximal femoral plate 4.5/5.0 in patients with missing posteromedial support in unstable per-, inter-, and subtrochanteric fractures of the proximal femur. Arch Orthop Trauma Surg. 2010;130(10):1281–7.
Prasarn ML, Ahn J, Helfet DL, Lane JM, Lorich DG. Bisphosphonate-associated femur fractures have high complication rates with operative fixation. Clin Orthop Relat Res. 2012;470(8):2295–301.
Balasubramanian N, Babu G, Prakasam S. Treatment of non unions of subtrochanteric fractures using an anatomical proximal femur locked compression plate – a prospective study of 13 patients. J Orthop Case Rep. 2016;6(1):65–8.
Shroeder JE, Mosheiff R, Khoury A, Liebergall M, Weil YA. The outcome of closed, intramedullary exchange nailing with reamed insertion in the treatment of femoral shaft nonunions. J Orthop Trauma. 2009;23(9):653–7.
Isaacs JD, Shidiak L, Harris IA, Szomor ZL. Femoral insufficiency fractures associated with prolonged bisphosphonate therapy. Clin Orthop Relat Res. 2010;468(12):3384–92.
Broos PL, Reynders P, Vanderspeeten K. Mechanical complications associated with the use of the unreamed AO femoral intramedullary nail with spiral blade: first experiences with thirty-five consecutive cases. J Orthop Trauma. 1998;12(3):186–9.
Gugenheim JJ, Probe RA, Brinker MR. The effects of femoral shaft malrotation on lower extremity anatomy. J Orthop Trauma. 2004;18(10):658–64.
Giannoudis PV, Ahmad MA, Mineo GV, Tosounidis TI, Calori GM, Kanakaris NK. Subtrochanteric fracture non-unions with implant failure managed with the “Diamond” concept. Injury. 2013;44(Suppl 1):S76–81.
Qvick LM, Ritter CA, Mutty CE, Rohrbacher BJ, Buyea CM, Anders MJ. Donor site morbidity with reamer-irrigator-aspirator (RIA) use for autogenous bone graft harvesting in a single centre 204 case series. Injury. 2013;44(10):1263–9.
Author information
Authors and Affiliations
Corresponding authors
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2018 Springer International Publishing AG
About this chapter
Cite this chapter
Koval, K.J., Rezaie, N., Yoon, R.S. (2018). Subtrochanteric Femur Fractures. In: Egol, K., Leucht, P. (eds) Proximal Femur Fractures. Springer, Cham. https://doi.org/10.1007/978-3-319-64904-7_9
Download citation
DOI: https://doi.org/10.1007/978-3-319-64904-7_9
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-319-64902-3
Online ISBN: 978-3-319-64904-7
eBook Packages: MedicineMedicine (R0)