
Abstract
Interstitial Lung Disease (ILD); Diffuse Parenchymal Lung Disease (DPLD); Diffuse Infiltrative Lung Disease (DILD)
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Name and Synonyms
Interstitial Lung Disease (ILD); Diffuse Parenchymal Lung Disease (DPLD); Diffuse Infiltrative Lung Disease (DILD)
Incidence/Epidemiology
-
The interstitial lung diseases encompass more than 200 individual diseases, all with unique incidences and epidemiology.
-
The incidence of specific disorders depends upon many factors, including age, sex, smoking status, environmental and occupational exposures, medications used, exposure to radiation, and medical history.
-
Most are rare diseases.
-
The most common of these disorders, idiopathic pulmonary fibrosis (IPF), accounts for about 55 % of all ILD diagnoses. It has an incidence that ranges from 10–25/100,000 in the population between 40 and 50 years old, to >175/100,000 in those over age 75.
-
All of these disorders are associated with considerable morbidity and mortality.
Differential Diagnosis
-
The differential diagnosis is broad and encompasses all diseases that can present primarily with dyspnea and cough, such as asthma, COPD, CHF, and bronchiectasis, among others.
-
The differential diagnosis within this class of disorders is also very broad, with over 200 individual diseases to consider.
Pathophysiology and Etiology
-
ILD is a broad category of diseases that share pathologic involvement of the lung parenchyma and common clinical, radiologic, and physiologic manifestations.
-
These are all non-malignant and non-infectious diseases.
-
There are several different classification schemes for these diseases. Some schemes classify based upon whether there is a known cause. Some classify based upon primary underlying histopathology (inflammation with fibrosis versus granulomatous.) Some systems classify based upon a combination of both known cause and underlying histopathology.
-
Inflammation and fibrosis. This pathophysiologic process starts with some injury or insult to the epithelial surface of the lung that leads to a diffuse inflammatory response in the air spaces and alveoli. This may remit or become chronic. If the inflammatory becomes chronic, the inflammation spreads to the lung interstitium and vasculature, which can lead to permanent interstitial fibrosis and scarring. This then leads to progressive and permanent impairment in physiologic parameters such as gas exchange and ventilation. Most of these disorders are difficult to treat and resistant to treatment.

A schematic drawing of pathogenetic mechanism of alveolar epithelial cells (AEC) in lung injury alveolitis and fibrosis. An initial injury of known or unknown etiology provokes an unresolved inflammation or AEC damage and alveolitis. Alveolitis is an initial event in the pathogenesis of lung fibrosis. A fibrin clot forms early and serves as a provisional matrix for the migration and proliferation of endogenous AEC stem cells. Bone marrow-derived stem cells, HSCs, can also contribute to the populations of AECs. Activated epithelial cells secrete numerous mediators that create a strong profibrotic microenvironment in lung fibrosis inducing AEC injury, alveolitis and apoptosis. Also injured AEC exhibit a defect in the release of some antifibrotic mediators such as prostaglandinE-2 (PGE2). Epithelial cell damage and cell death during alveolitis induce the formation of gaps in the epithelial basement membrane. Progression from the acute phase of lung injury is accompanied by abnormal alveolar reepitalization, tissue repair and remodeling, which may result in progressive fibrosis. AEC produce MMPs that increase basement membrane disruption and allow fibroblast migration, proliferation and differentiation to myofibroblasts. Myofibroblasts secrete extracellular matrix proteins, mainly collagens. An imbalance between MMPs and TIMPs provokes the progressive deposit of the extracellular matrix (ECM) and abnormal collagen accumulation and promotes fibrosis. Alveolar macrophages and AEC secrete TGF-β1, which induces epithelial mesenchymal transition (EMT), and this may contribute to fibroblast/myoflbroblast accumulation in the processes of fibrosis. [Gharaee-Kermani M, Gyetko MR, Hu B, Phan SH. New Insights into the Pathogenesis and Treatment of Idiopathic Pulmonary Fibrosis: A Potential Role for Stem Cells in the Lung Parenchyma and Implications for Therapy. Pharmaceutical Research. 2007 Apr 12;24(5):819–41.] Caption from original


Idiopathic pulmonary fibrosis (interstitial lung disease, idiopathic interstitial pneumonias) with varying alveolar and interstitial inflammatory infiltrates, progressive interstitial fibrosis, secondary hypertensive vascular disease, and a final stage with honeycombing of the lungs. Note the fleshy gross appearance of the lungs in earlier stages (a), with various microscopic interstitial infiltrates (b–d) and gross honeycombing at the end stage (e). The etiology of these diseases is inhomogeneous, as demonstrated by the large variety of terms in use. In many cases, these diseases appear to be autoimmune, either primary or secondary in the course of other systemic autoimmune disorders, but frequently the etiology remains obscure. These disorders are grouped together because of similar clinical manifestations, including severe shortness of breath, diffuse abnormalities of lung mechanics and gas exchange, and diffuse abnormalities in chest radiographs and CT scans, as well as similar clinical outcomes [Krueger GRF, Wagner M, Oldham SAA. Pathology of the Respiratory Tract. In: Krueger GRF, Buja LM, editors. Atlas of Anatomic Pathology with Imaging [Internet]. London: Springer London; 2013 [cited 2015 May 28]. p. 105–89. Available from: http://springerlink.bibliotecabuap.elogim.com/10.1007/978-1-4471-2846-5_3] Caption adapted from original
-
The granulomatous disorders are marked by the pathologic accumulation of inflammatory cells and epithelial cells into granulomas within lung tissue. Many of these patients can remain with mild-to-moderate symptoms, and many may improve with treatment.
-
A helpful schema clinically is to group these disorders as to whether the cause is known or unknown.
-
Known causes: Inflammatory pathology unless otherwise labeled.
-
Associated with connective-tissue diseases (most commonly rheumatoid arthritis, scleroderma, and polymyositis).
-
Hypersensitivity pneumonitis (e.g., farmer’s lung and bird fancier’s lung). Granulomatous.
-
Pneumonoconioses (asbestosis, silicosis, coal miner’s lung).
-
Drug-induced (chemotherapeutic agents, amiodarone, methotrexate).
-
Smoking-related.
-
Pulmonary Langerhans cell histiocytosis.
-
Respiratory bronchiolitis ILD.
-
Desquamative interstitial pneumonia.
-
Acute eosinophilic pneumonia.
-
Radiation-induced.
-
Toxic-inhalation induced (e.g., cocaine, ammonia, etc.).
-
-
Unknown Causes: Inflammatory pathology unless labeled otherwise.
-
Idiopathic pulmonary fibrosis.
-
Sarcoidosis. Granulomatous.
-
Other idiopathic interstitial pneumonias.
-
Cryptogenic organizing pneumonia (bronchiolitis obliterans organizing pneumonia).
-
Nonspecific interstitial pneumonia.
-
Lymphocytic interstitial pneumonia.
-
Acute interstitial pneumonia.
-
Eosinophilic pneumonias.
-
Pulmonary vasculitides. Mostly granulomatous.
-
Pulmonary lymphangioleiomyomatosis.
-
Pulmonary alveolar proteinosis.
-
Many other rare disorders.
-
Presentation
Typical/“Classic”
-
Dyspnea is the most common and prominent complaint in ILD.
-
Classically, patients will have dyspnea with a persistent, non-productive cough associated with diffuse, interstitial infiltrates on chest x-ray.
-
Often, patients will have been treated with one or several courses of antibiotics for typical and atypical pneumonia. This non-response to antibiotics should raise suspicion for an ILD.
-
The most common time course of presentation is chronic, with symptoms ongoing over months-to-years. A sub-acute presentation over weeks-to-months is also common.
-
A detailed history is very important in the evaluation of a patient with a suspected ILD. It can help to narrow the differential to a manageable number of conditions. The history should include detailed questioning as to the pattern and timing of symptoms, smoking history, a detailed environmental and occupational history, and a family history.
-
Patients with inflammatory/fibrotic disorders will often have bibasilar “dry” crackles on physical exam. These are often also called “Velcro” crackles as they sound like Velcro being pulled apart.
-
Cyanosis and clubbing can occur with advanced disease, and are noted in up to 30% of patients with advanced idiopathic pulmonary fibrosis.

Clubbing of the fingers [Karkucak M, Erturk E, Capkin E, Akyazi H, Ozden G, Tosun M. Primary hypertrophic osteoarthropathy (pachydermoperiostosis): a case report. Rheumatology International. 2007 Jan 11;27(4):403–5.] Caption from original
https://www.youtube.com/watch?v=9C5RFb1qWT8
Audio recording of crackles, including late inspiratory crackles.
Atypical
-
An acute presentation is unusual, happening mostly in disorders with an allergic basis.
-
Some disorders will present in an episodic fashion with acute exacerbations that improve with treatment (sarcoidosis).
-
Wheezing and chest pain are not common presenting complaints/findings, except in sarcoidosis.
-
Hemoptysis is uncommon, but may be seen in the alveolar hemorrhage syndromes.
Primary Differential Considerations
-
Early consideration should be given to
-
ARDS
-
Sarcoidosis
-
Pneumoconiosis
-
Hypersensitivity or drug-induced pneumonitis
-
Pulmonary edema
-
Pneumonia
-
History and Physical Exam
Findings That Confirm Diagnosis
-
There are no historical or physical exam findings that can confirm the diagnosis.
-
The diagnosis is confirmed with appropriate findings on high-resolution CT of the lungs, or by specific pathologic findings on lung biopsy.
Factors That Suggest Diagnosis
-
A classic presentation as described, with slowly progressive dyspnea, a chronic non-productive cough, and diffuse infiltrates on chest x-ray, with symptoms that don’t improve with antibiotic treatment, should clearly raise suspicion for an ILD.
-
A careful physical examination can help to identify related systemic processes such as any evidence of a connective-tissue disease.
Factors That Exclude Diagnosis
-
There are no historical or physical exam findings that can exclude the diagnosis.
-
A normal high-resolution CT scan of the lungs would essentially rule out the diagnosis.
Ancillary Studies
Laboratory
-
Most patients will have had routine laboratory studies (CBC, basic chemistries) checked, but they are unlikely to be helpful.
-
Specific laboratory evaluation for specific disorders being considered should be performed.
-
A raised lactate dehydrogenase (LDH) level is a common, non-specific finding in many ILDs.
-
The serum level of angiotensin-converting enzyme (ACE) is commonly elevated in sarcoidosis.
-
Anti-nuclear Ab and anti-immunoglobulin Ab (rheumatoid factor) can be found even in patients without an obvious connective-tissue disease.
-
If a vasculitis is suspected, it may be helpful to check for the presence of anti-neutrophil cytoplasmic Ab’s and anti-basement membrane Ab.
Imaging
-
Most evaluations for ILD are initiated and suspected based upon an abnormal chest x-ray But plain CXRs are neither sensitive nor specific for a diagnosis of ILD. In fact, up to 20% of patients with ILD can have a CXR that is read as normal. CXR findings correlate poorly with clinical findings, and also with the histopathologic stage of the disease.
-
High-resolution CT (HRCT) of the chest is the imaging study of choice for the diagnosis of any diffuse interstitial process. The classic “honeycombing” of lung tissue is an end-stage finding.
-
HRCT can narrow the differential diagnosis, and in some cases can confirm the diagnosis.
-
The pattern of abnormalities, distribution of abnormalities, and associated findings (pleural effusions, lymphadenopathy) found on HRCT, used in conjunction with the clinical context, can sometimes confirm the diagnosis. This can obviate the need for a lung biopsy.

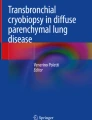
Interstitial lung disease in polymyositis. Magnification lateral‐view chest radiograph showing lower zonal reticular interstitial lung disease. [Berney S, Heldmann M. Chapter 14. In: Crapo J, editor. Bone's atlas of pulmonary and critical care medicine. 3rd ed. Philadelphia: Current Medicine; 2005. ISBN: 1-57340-211-7] Caption from original

High-resolution computed tomography images from a patient with respiratory bronchiolitis interstitial lung disease demonstrating areas of faint, patchy ground glass opacification and reticular thickening. [Coley CJ, Tolle LB, Hasvold J, Schmidt LA, Flaherty KR. Non-specific, Unclassifiable, and Rare Idiopathic Interstitial Pneumonia: Acute Interstitial Pneumonia, Respiratory Bronchiolitis Interstitial Pneumonia, Desquamative Interstitial Pneumonia, Nonspecific Interstitial Pneumonia. In: Cottin V, Cordier J-F, Richeldi L, editors. Orphan Lung Diseases [Internet]. London: Springer London; 2015 [cited 2015 May 28]. p. 349–62. Available from: http://springerlink.bibliotecabuap.elogim.com/10.1007/978-1-4471-2401-6_23] Caption from original

High-resolution computed tomography from the mid (panel a) and lower (panel b) lung fields of patient with nonspecific interstitial pneumonia. The images demonstrate patchy areas of ground glass opacification, reticular thickening and traction bronchiectasis. Some subpleural sparing of disease can be appreciated. Honeycombing is absent. [Coley CJ, Tolle LB, Hasvold J, Schmidt LA, Flaherty KR. Non-specific, Unclassifiable, and Rare Idiopathic Interstitial Pneumonia: Acute Interstitial Pneumonia, Respiratory Bronchiolitis Interstitial Pneumonia, Desquamative Interstitial Pneumonia, Nonspecific Interstitial Pneumonia. In: Cottin V, Cordier J-F, Richeldi L, editors. Orphan Lung Diseases [Internet]. London: Springer London; 2015 [cited 2015 May 28]. p. 349–62. Available from: http://springerlink.bibliotecabuap.elogim.com/10.1007/978-1-4471-2401-6_23] Caption from original

CT diffuse interstitial lung disease with honeycombing. [Teixeira Moreira Almeida M do S, Dias LT, Fernandes SJS, Almeida JVM. Spontaneous pneumomediastinum and subcutaneous emphysema in systemic sclerosis. Rheumatology International. 2007 Apr 10;27(7):675–7.] Caption from original
Pulmonary Function Tests
-
Spirometry is helpful in evaluating the extent of disease.
-
Most forms of ILD will produce a restrictive pattern of PFTs (COPD gives an obstructive pattern). This includes a reduced total lung capacity (TLC), functional residual capacity (FRC), and residual volume (RV).
-
Forced expiratory volume in one second (FEV1) and functional vital capacity (FVC) are often reduced, but their ratio is usually normal or increased, as opposed to COPD, where there is a reduced ratio.
-
Lung volumes continue to decrease as the disease progresses and lung compliance worsens (the lungs become “stiff”).
-
The rate of decline of PFTs can have prognostic significance.
-
The diffusing capacity to carbon monoxide (DLCO) is reduced in most ILDs, but this is a nonspecific finding and does not correlate with disease stage.
-
Arterial blood gases can be normal, but may also show hypoxia from ventilation perfusion mismatch. Ventilation perfusion mismatch occurs because as the fibrosis worsens, lung compliance reduces (the lungs become more stiff). This reduces ventilation in these areas of the lung, but perfusion in these areas remains the same. This leads to blood that has not been adequately oxygenated returning to the heart, which allows this “venous” blood to mix with oxygenated blood in the left heart.
-
Carbon dioxide retention is uncommon in ILD (it is more common in COPD), but if present it indicates severe, end-stage disease.
-
Exercise pulmonary testing can be used to follow disease progression.
Lung Biopsy
-
Lung biopsy may be necessary if the diagnosis is in question after work-up, including HRCT.
-
Lung biopsy is the most effective method for diagnosis and assessment of disease severity.
-
If possible, a biopsy should be performed prior to the initiation of treatment.
-
Bronchoscopy with transbronchial biopsy is usually the first approach to obtaining lung tissue for biopsy. However, this approach gives small tissue samples, and often cannot lead to a definitive diagnosis.
-
In these cases it may be necessary to perform a surgical lung biopsy. Surgical lung biopsy has a diagnostic yield of nearly 90%.
-
Surgical lung biopsy is usually performed under video-assisted thorascopic surgery (VATS). However, this approach can have a mortality of 2% and a complication rate of 5–10%.
-
Bronchoalveolar lavage during bronchoscopy is not useful in the diagnosis of ILD, but may help offer alternative diagnoses (cancer or infections), or assess for complications of ILD (also cancer and infections).
Special Populations
Age
Infants and Children
-
Interstitial lung disease does occur in infants and children. It is marked by pulmonary symptoms with diffuse pulmonary infiltrates on lung imaging.
-
It is very rare in this age group, with a reported incidence between 1.5–3.6 cases per 1 million in those under the age of 16.
-
Many of the causes of ILD in children are similar to the causes in adults, but there are syndromes unique to infants and neonates. These include:
-
Diffuse developmental disorders. This includes alveolar capillary dysplasia with misalignment of the pulmonary veins (ACD-MPV), and acinar dysplasia.
-
Disorders of lung growth and development. This group includes pulmonary hypoplasia and chronic neonatal lung disease with bronchopulmonary dysplasia.
-
Neuroendocrine cell hyperplasia of infancy (NEHI). This is a very rare disorder with an unknown etiology.
-
Pulmonary interstitial glycogenolysis (PIG).
-
Genetic disorders of surfactant production and metabolism.
-
-
In neonates and infants, ILD often presents with unexplained respiratory failure.
-
In older infants and children the presentation can be non-specific and includes persistent and unexplained tachypnea, chronic cough, hypoxemia, exercise intolerance, and clubbing of the digits. ILD can also present as failure to thrive and unexplained feeding difficulties. Children above age 2 are more likely to present with exercise intolerance and clubbing.
-
The work-up should begin with a complete history and physical examination. The evaluation should initially focus on assessing and excluding the more common causes of respiratory symptoms with diffuse infiltrates. These include: infectious causes, congenital heart disease, and cystic fibrosis. Other rare causes can include immunodeficiencies and structural lung and airway abnormalities.
-
The evaluation can then follow as described above for adults.
-
An important addition to the evaluation of ILD in children, especially in neonates with respiratory failure and children with suspected ILD and another affected sibling, is genetic testing for mutations of surfactant production and metabolism. Finding one of these mutations can be diagnostic and obviate the need for lung biopsy.
-
Treatment is often supportive (avoiding respiratory irritants, nutritional support, oxygen for hypoxemia, appropriate vaccinations, and appropriate treatment of intercurrent infections), and should be guided by the specific syndrome.
-
The prognosis greatly depends upon the specific disorder. Some will spontaneously remit.
-
The prognosis is generally poor with ACD-MPV, surfactant mutations, and if pulmonary hypertension complicates ILD.
-
Lung transplantation can be considered for end-stage disease not responding to therapy.
Adults
-
ILD can present across the spectrum of age groups. The age at presentation can be a significant help in narrowing the differential.
Co-morbidities
-
The presence of other or multiple co-morbidities can make the diagnosis and management of ILD more challenging. Of particular concern would be the presence of cancer, heart disease, congestive heart failure, diabetes mellitus, and renal failure.
Pitfalls in Diagnosis
Critical Steps Not to Miss
-
Consideration of the diagnosis is the first critical step. Strong consideration of the diagnosis should be given when a patient has not responded to several courses of antibiotics for presumed infectious pneumonia when there are diffuse infiltrates on the CXR.
-
When considering the diagnosis, it is critical to take an exhaustive history that should include a complete occupational, travel, and hobby/leisure activity history.
-
HRCT is a critical test in the evaluation of suspected ILD.
Mimics
-
With several hundred different forms of ILD, any of these may mimic another.
-
Other diseases that can present with a cough, dyspnea, and diffuse infiltrates include: primary or metastatic cancer, atypical pneumonias, congestive heart failure, and bronchiectasis.
Time-Dependent Interventions
-
Most ILDs are insidious and progress slowly.
-
Diagnosis often requires months, and symptoms may have been ongoing and worsening for months to years.
-
Some of these diseases may present in an acute fashion, developing over days to weeks. These can include allergy, vasculitides, acute interstitial pneumonia, eosinophilic pneumonia, and hypersensitivity pneumonitis.
-
In patients with known ILD, acute respiratory worsening, especially if over 4 weeks or less, is usually due to either acute infection or pulmonary edema.
Overall Principles of Treatment
-
Treatment should be tailored to the specific disorder if possible.
-
The course can be highly variable, but most ILDs are chronic and progressive.
-
There is no therapy to reverse fibrosis once present, so the goal of therapy is usually to reduce inflammation to limit any further damage.
-
Oxygen should be used if the patient is hypoxemic (resting PaO2 <55 mmHg)
-
Pulmonary rehabilitation has been shown to improve quality of life.
-
Glucocorticoids are the most commonly used pharmacologic agents in the majority of ILDs. They are commonly started at high doses, up to 1 mg/kg/day, and continued for 1–3 months. If there has been a response, they are slowly tapered over 3–12 months. Too rapid tapering can lead to recurrence. Many patients will require a maintenance dose of steroids. However, the overall response rate is low.
-
If patients on glucocorticoids don’t improve, or if their condition worsens, second-line agents include cyclophosphamide and azathioprine. These agents can be used alone or in combination with glucocorticoids.
Disease Course
-
Most cases are chronic, slowly progressive, and resistant to most treatments.
-
Lung transplant can be considered for end-stage disease.
Related Evidence
Papers of particular interest have been highlighted as:
** Of key importance
Practice Guideline
Cottin V, Crestani B, Valeyre D, Wallaert B, Cadranel J, Dalphin JC, Delaval P, Israel-Biet D, Kessler R, Reynaud-Gaubert M, Aguilaniu B, Bouquillon B, Carré P, Danel C, Faivre JB, Ferretti G, Just N, Kouzan S, Lebargy F, Marchand-Adam S, Philippe B, Prévot G, Stach B, Thivolet-Béjui F, Cordier JF; French National Reference Centre; Network of Competence Centres for Rare Lung Diseases. Diagnosis and management of idiopathic pulmonary fibrosis: French practical guidelines. Eur Respir Rev. 2014 Jun;23(132):193-214. doi: 10.1183/09059180.00001814. PMID: 24881074. http://www.ncbi.nlm.nih.gov/pubmed/24881074 **
Travis WD, Costabel U, Hansell DM, King TE Jr, Lynch DA, Nicholson AG, Ryerson CJ, Ryu JH, Selman M, Wells AU, Behr J, Bouros D, Brown KK, Colby TV, Collard HR, Cordeiro CR, Cottin V, Crestani B, Drent M, Dudden RF, Egan J, Flaherty K, Hogaboam C, Inoue Y, Johkoh T, Kim DS, Kitaichi M, Loyd J, Martinez FJ, Myers J, Protzko S, Raghu G, Richeldi L, Sverzellati N, Swigris J, Valeyre D; ATS/ERS Committee on Idiopathic Interstitial Pneumonias. An official American Thoracic Society/European Respiratory Society statement: Update of the international multidisciplinary classification of the idiopathic interstitial pneumonias. Am J Respir Crit Care Med. 2013 Sep 15;188(6):733-48. doi: 10.1164/rccm.201308-1483ST. PMID: 24032382. http://www.ncbi.nlm.nih.gov/pubmed/24032382 **
Diagnosis and Management of Suspected Idiopathic Pulmonary Fibrosis: Idiopathic Pulmonary Fibrosis. National Clinical Guideline Centre (UK). London: Royal College of Physicians (UK); 2013 Jun. PMID: 25340234.http://www.ncbi.nlm.nih.gov/pubmed/25340234 **
Meyer KC, Raghu G, Baughman RP, Brown KK, Costabel U, du Bois RM, Drent M, Haslam PL, Kim DS, Nagai S, Rottoli P, Saltini C, Selman M, Strange C, Wood B; American Thoracic Society Committee on BAL in Interstitial Lung Disease. An official American Thoracic Society clinical practice guideline: the clinical utility of bronchoalveolar lavage cellular analysis in interstitial lung disease. Am J Respir Crit Care Med. 2012 May 1;185(9):1004-14. doi: 10.1164/rccm.201202-0320ST. PMID: 22550210. http://www.ncbi.nlm.nih.gov/pubmed/22550210 **
Bradley B, Branley HM, Egan JJ, Greaves MS, Hansell DM, Harrison NK, Hirani N, Hubbard R, Lake F, Millar AB, Wallace WA, Wells AU, Whyte MK, Wilsher ML; British Thoracic Society Interstitial Lung Disease Guideline Group, British Thoracic Society Standards of Care Committee; Thoracic Society of Australia; New Zealand Thoracic Society; Irish Thoracic Society. Interstitial lung disease guideline: the British Thoracic Society in collaboration with the Thoracic Society of Australia and New Zealand and the Irish Thoracic Society. Thorax. 2008 Sep;63 Suppl 5:v1-58. doi: 10.1136/thx.2008.101691. PMID: 18757459. http://www.ncbi.nlm.nih.gov/pubmed/18757459 **
Review
Oldham JM, Noth I. Idiopathic pulmonary fibrosis: early detection and referral. Respir Med. 2014 Jun;108(6):819-29. doi: 10.1016/j.rmed.2014.03.008. PMID: 24746629. http://www.ncbi.nlm.nih.gov/pubmed/24746629 **
Kuo CS, Young LR. Interstitial lung disease in children. Curr Opin Pediatr. 2014 Jun;26(3):320-7. doi: 10.1097/MOP.0000000000000094. PMID: 24752172. http://www.ncbi.nlm.nih.gov/pubmed/24752172 **
Antoniou KM, Margaritopoulos GA, Tomassetti S, Bonella F, Costabel U, Poletti V. Interstitial lung disease. Eur Respir Rev. 2014 Mar 1;23(131):40-54. doi: 10.1183/09059180.00009113. PMID: 24591661. http://www.ncbi.nlm.nih.gov/pubmed/24591661 **
Walsh SL, Hansell DM. High-resolution CT of interstitial lung disease: a continuous evolution. Semin Respir Crit Care Med. 2014 Feb;35(1):129-44. doi: 10.1055/s-0033-1363458. PMID: 24481766. http://www.ncbi.nlm.nih.gov/pubmed/24481766 **
Soares JJ, Deutsch GH, Moore PE, Fazili MF, Austin ED, Brown RF, Sokolow AG, Hilmes MA, Young LR. Childhood interstitial lung diseases: an 18-year retrospective analysis. Pediatrics. 2013 Oct;132(4):684-91. doi: 10.1542/peds.2013-1780. PMID: 24081995. http://www.ncbi.nlm.nih.gov/pubmed/24081995 **
Hilman BC, Amaro-Galvez R. Diagnosis of interstitial lung disease in children. Paediatr Respir Rev. 2004 Jun;5(2):101-7. PMID: 15135119. http://www.ncbi.nlm.nih.gov/pubmed/15135119
Use PubMed Clinical Queries to find the most recent evidence. Use this search strategy:
“Lung Diseases, Interstitial”[Mesh] OR “Interstitial Lung Disease”
Author information
Authors and Affiliations
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2019 Springer Nature Switzerland AG
About this chapter

Cite this chapter
Rees, C.J., Pollack Jr., C.V., Riese, V.G. (2019). Interstitial Lung Disease. In: Pollack Jr., C. (eds) Differential Diagnosis of Cardiopulmonary Disease. Springer, Cham. https://doi.org/10.1007/978-3-319-63895-9_40
Download citation
DOI: https://doi.org/10.1007/978-3-319-63895-9_40
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-319-63894-2
Online ISBN: 978-3-319-63895-9
eBook Packages: MedicineMedicine (R0)