
Abstract
The effects of environmental agents on cerebellar development are profound, and this organ has not been given the attention that is deserving of it, based on its importance in motor, cognitive, and behavioral functions. This chapter will review select agents associated with teratogenic effects on cerebellar structure and function. Mechanisms of teratogenesis and genetic influences will be addressed. The emerging role of effects of environmental agents and effect on the epigenetic mechanisms and gene expression are discussed. Prenatal alcohol exposure and fetal alcohol spectrum disorder will be discussed in greater detail, as this disorder is the most common teratogenic disorder affecting humans. Indeed, many of the phenotypic effects of FASD are the result of cerebellar injury and dysfunction.
Access provided by CONRICYT-eBooks. Download chapter PDF
Similar content being viewed by others


Keywords
- Teratogenesis
- Brain imaging
- Birth defects
- Prenatal exposures
- Viral infections
- Zika virus
- Rubella
- Anticonvulsants
- Valproic acid
- Alcohol
- Genetic factors
- Epigenetics
- Fetal alcohol spectrum disorder
Introduction
Teratology can be defined as science dealing with causes, mechanisms, and manifestations of developmental deviations of either structural or functional nature [1, 2]. A teratogen is any agent that compromises a healthy intrauterine environment and results in altering normal development during the period of embryonic or fetal development resulting in abnormal structure or function, restriction of growth, or death of the embryo or fetus [3]. Known teratogenic agents include infectious agents (e.g., rubella virus, Zika virus, cytomegalovirus, toxoplasmosis, varicella, etc.), a chemical or drug (most anticonvulsant medications such as phenobarbital, diphenylhydantoin, valproic acid, retinoic acid, warfarin, etc.), heavy metals and environmental poisons (mercury, lead, manganese, and toluene/benzene derivatives), excessive radiation, maternal conditions (drug and alcohol abuse or addiction to illicit drugs, smoking, nutritional deficiencies, metabolic disorders in the mother such as phenylketonuria, diabetes, mental and emotional stress, etc.), invasive medical interventions (such as amniocentesis, chorionic villus sampling, etc.), and changes in the environment (elevated core temperature for an extended period of time such as febrile illness, sauna or hot tub use, etc.) [4,5,6].
Teratogens in humans have certain characteristics that include evidence of an increase in the frequency of a known abnormal phenotypic effect , such as neurobehavioral changes or structural changes leading to birth defects , a dose response relationship with a threshold effect, critical periods of significant risk, established mechanism of action, biological plausibility of teratogenicity, and genetic and/or epigenetic predisposing risk factors. Identifying and confirming the etiological origins of birth defects can lead to better treatment and prevention and, in the case of infectious diseases, the development of effective vaccines to reduce the risk in the population [2].
The effects of teratogens are variable and dependent on timing of the exposure, the dose of the exposure, the frequency of exposure(s), maternal and fetal genetic factors, and other mitigating or susceptibility factors that modify the effect. The exposure can lead to a variety of outcomes, from apparently normal and unaffected to mild impairment and to severe impairments with multiple malformations, or result in abortion and death.
As with all developing organs, the brain is often the target of teratogenic effects. The resulting impairments from a teratogenic exposure affecting brain development can lead to effects on brain structure (cellular defects, malformations, or disruption) and/or brain function that can manifest as behavioral abnormalities, craniofacial dysmorphology, developmental delays, intellectual impairment, and/or severe physical disability. It is rare for a teratogenic effect to be restricted to a single organ structure or specific region of the brain. However, for the purposes of this chapter, emphasis will be placed on the teratogenic effect on the cerebellum and the clinical consequences.
The cerebellum is relatively small, but it has established functional connections to many other regions of the brain. Prenatal and postnatal injuries due to a variety of toxins result in neurologic deficits, including ataxia, hypotonia, dysarthria, and ocular motility problems. These exposures can present with impairments in movement, motor coordination, sensory function, cognition, affect regulation, or mood. Dysfunction of the cerebellum and its effects on connectivity to other brain regions have been correlated with a number of neurodevelopmental disorders that include autism, attention deficit hyperactivity disorder, dyslexia, as well as psychiatric diseases such as schizophrenia and bipolar diseases [7]. Many inherited disorders involving abnormal development and function of the cerebellum including cerebellar hypoplasia have been described [8].
The nature of the injury or exposure would be dependent on the subregions of the cerebellum involved and determined by alterations in the corresponding cerebro-cerebellar circuitry [9]. Recent studies exploring the role of speech and language have demonstrated an important role of the cerebellum in communication in health and disease. Mariën et al. [10], in a consensus review of this topic, summarized their findings to date “cerebellar involvement in language extends far beyond the pure motor domain to a variety of high-level non-motor linguistic processes at both the expressive and receptive language level. In general the role of the cerebellum in language adds evidence to the view that timing and sequencing processing, sensorimotor adaptation and cognitive skill automatization act as the overall operational modes of the cognitive cerebellum.”
Developmental abnormalities of the cerebellum have been induced by several teratogenic agents, including therapeutic agents such as 13-cis retinoic acid (Accutane©) and misoprostol (Cytotec©)l. [11,12,13]. Many early studies, prior to the 1970s, were limited in describing cerebellar abnormalities since techniques to visualize this organ were crude or not yet available for wide clinical use. Evaluation of the brain in the 1960s and 1970s was restricted to investigations such as electroencephalograms (EEG), pneumoencephalograms, ultrasound, and the earlier generation computed tomography (CT) or autopsy findings. The list of disorders with identifiable cerebellar lesions is growing particularly with the advent and ubiquitous use of newer imaging techniques. With the advent of newer imaging modalities, brain imaging has been enhanced. Single-photon emission computed tomography (SPECT) can provide 3D information, and positron emission tomography (PET) can help assess functional abnormalities in the brain before anatomical changes occur in many diseases of the brain. Using magnetic resonance imaging (MRI), structural CNS defects and malformations are more readily and accurately defined, or in the case of functional MRI analysis, brain activation responses to a variety of external stimuli can be visualized. Magnetic resonance spectroscopy (MRS) can identify disturbances in the neurochemistry of the brain. Diffusion tensor imaging (DTI) assesses the integrity of the white matter and maps normal and aberrant white matter tracts and brain circuitry. In this chapter some examples of teratogenic agents with effects on the developing cerebellum will be presented.
Intrauterine Infections
There are scores of infectious agents associated with intrauterine viral and parasitic infections. Most can cause a variety of developmental defects in exposed fetuses. Examples include the classical group of teratogenic pathogens, the so-called “TORCH” (Toxoplasma gondii, Others like Treponema pallidum, Rubella virus, Cytomegalovirus, Herpes simplex virus ), and other agents including Parvovirus B19, Varicella zoster virus, and plasmodium falciparum to name a few. In this chapter reviews of Rubella and the Zika virus are presented for illustration purposes, and readers are referred to recent reviews on intrauterine infections for further information [14, 15].
Congenital Rubella
As noted, several infectious agents have been implicated in causing birth defects and brain abnormalities [16]. The first report of a teratogenic agent in humans was made in 1941 by an Australian ophthalmologist Normal Gregg, who described children with cataracts as a result of rubella in the children’s mothers during the pregnancy [17]. Congenital rubella is typically associated with other CNS abnormalities, microcephaly, growth retardation, congenital hepatitis, deafness, cataracts, retinopathy, and cardiovascular defects. The mechanisms of teratogenesis have included inhibited cell growth, impaired blood flow, direct effects of the ongoing infection with cytopathic effects, and immunopathological mechanisms [18, 19].
Townsend et al. [20] reported on a case of progressive panencephalitis in a child who was born with congenital rubella. Neuropathologic studies showed findings in the brain which included diffuse destruction of white matter with perivascular inflammatory cells and gliosis, moderate neuronal loss, numerous amorphous vascular deposits in the white matter, and severe generalized cerebellar atrophy. Recently Cluver et al. [21] reported on an infant with confirmed early prenatal rubella infection born with agenesis of the inferior cerebellar vermis. The authors suggest that the cerebellar defect was likely the result of spread of the virus through the vascular system causing vasculitis and endothelial necrosis [22]. There are only rare reports of cerebellar defects in congenital rubella syndrome.
It is likely that most viral and other infectious agents causing intrauterine infections have similar mechanisms of teratogenesis affecting the developing cerebellum [16, 23, 24]. Further investigations could clarify the role of viral infections in overstimulation of excitatory amino acid receptors, excess production of angiogenesis, pro-inflammatory cytokine neurotrophic factors , and apoptotic-inducing factors [25].
Congenital Zika Infection
Recently, the Aedes species mosquito-borne Zika virus has been confirmed to be causative of congenital microcephaly and other birth defects including arthrogryposis and sensorineural hearing loss [26,27,28,29,30,31,32]. The Zika virus belongs to a family of related arthropod-borne (arbovirus) that includes dengue, yellow fever, West Nile encephalitis, and Japanese encephalitis viruses and another virus from a different family, Chikungunya virus [30]. The virus was first recognized in the Zika forest of Uganda from a rhesus monkey with an acute febrile illness in 1947 [33] with human infections first reported in Nigeria in 1954 [34]. Subsequent spread to the Yap Islands of Micronesia, the Pacific Islands, and Polynesia showed that this was not a benign disease in humans [30]. From mid-2015 to 2016, over 30,000 cases were reported in Brazil [29] and subsequently as far north as Florida [35]. Several cases have been imported to European countries and North America including Canada [36]. In a series of 23 infants from Brazil, de Fatima et al. [27] and Hazin et al. [37] identified common findings in the brain of these children through CT and MRI techniques. The abnormalities included brain calcifications in the junction between cortical and subcortical white matter; malformations of cortical development with simplified gyral patterns, pachygyria, or polymicrogyria in the frontal lobes; enlarged cisterna magna; abnormalities of corpus callosum; ventriculomegaly; delayed myelinization; and hypoplasia of the cerebellum and brainstem [37]. Garcez et al. [38] experimental studies on human brain culture confirm that the Zika virus abrogates neurogenesis during human brain development. Tang et al. [39] showed that there is a downregulation of genes involved in cell-cycle pathways, dysregulation of cell proliferation, and upregulation of genes involved in apoptotic pathways resulting in cell death. Clearly until an effective vaccine is developed [40], better treatment and diagnostic capabilities need to be developed and priority given to vector control. Outcomes of children born with congenital Zika virus infection show major CNS abnormalities and have features of severe delays in development and severe neurological dysfunction [27, 41].
Congenital Anticonvulsant Syndrome
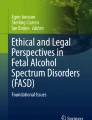
It is estimated that well over a million women of childbearing age in the United States have epilepsy, the vast majority of whom are on drug therapy for management of this common disorder [42]. This is a concern since almost all antiepileptic drugs have potential risks for causing fetal anomalies and later developmental delay. This was first confirmed a reality in the early 1970s and 1980s with reports of children born to epileptic mothers on drugs that included phenobarbital, phenytoin, and carbamazepine presenting with recurrent patterns of birth defects that included major malformations, such as microcephaly, growth retardation, and minor craniofacial and digital/limb anomalies [43,44,45,46,47,48,49,50] (Fig. 1). Holmes et al. [50] showed that the risk of malformations was higher in women taking one anticonvulsants over women delivering babies who were on no anticonvulsants (odds ratio 2.8), and the risk when women were taking two or more anticonvulsants was even higher (odds ratio 4.2). Women with epilepsy who were not on medication in the pregnancy showed no increase in major congenital anomalies than the controls. Morrow et al. [51] studied pregnant women with a diagnosis of epilepsy in UK centers using a prospective, observational, registration, and follow-up approach. They found 4.2% of women delivered infants with major congenital malformations with a history of taking anticonvulsant medication. For polytherapy use, the rate was 6.0%, for monotherapy it was 3.7%, and for women with epilepsy taking no medication, the rate was 3.5%. Valproic acid demonstrated the highest rate of major congenital malformations at 6.2%. This is compared with the expected “background” rate of major congenital malformations as between 1% and 2% in the general population at birth [52, 53]. It has been suggested that some of the difference may be due to genetic factors that increase the frequency of anomalies in some children. This seems to be borne out by studies that show differences in activity of the detoxifying enzyme epoxide hydrolase, with deficiency of the enzyme in infants, presenting with clinical features of hydantoin embryopathy [54, 55]. It has been hypothesized that anticonvulsants increase the production of free radicals resulting in vulnerability to malformations as a potential etiological factor [56].

Infant with typical facial features and distal digital hypoplasia with fetal hydantoin syndrome (From Buehler et al. NEJM. 1998. With permission)
There are several anticonvulsants in common use today. The list of anticonvulsants is long, and the most commonly used drugs include valproic acid, phenobarbital, phenytoin, carbamazepine, gabapentin, lamotrigine, levetiracetam, topiramate, vigabatrin, and benzodiazepines. A detailed review of the effects of valproic acid on human development including the cerebellum is presented below.
Valproic Acid
Valproic acid (VPA) is a widely used and effective anticonvulsant medication that is also used in the treatment of mood disorders, schizophrenia, and migraine headaches. Animal and human studies show that VPA is associated with a predictably higher rate of major congenital malformations that is dose dependent [57]. The risk is two to three times that of the expected rates of malformations in the population, and it is associated with a higher risk than are other anticonvulsants.
The risk of adverse outcomes following the use of VPA includes major congenital malformation including spina bifida, atrial septal defects of the heart, craniosynostosis, cleft palate, hypospadias, and polydactyly [53]. In 1984, DiLiberti et al. [58] described a consistent constellation of dysmorphic features that they called fetal valproate syndrome which has been confirmed subsequently in many reports [59, 60]. Although periconceptional use of folic acid is recommended for all women, those using anticonvulsants may benefit by using a higher dose of this vitamin, although evidence suggests that folic acid may not be protective in preventing spina bifida from occurring after exposure to VPA. This then begs the question what is the mechanism of the malformations in VPA and other anticonvulsants [44, 61]. VPA is also associated with neurodevelopmental and cognitive impairments [62] and is a known risk for autism spectrum disorders [63,64,65]. Christiansen et al. [64] confirmed in their prospective study that maternal use of VPA was associated with a significantly increased risk of autism spectrum disorder even after adjusting for maternal epilepsy. It is of interest and perhaps not coincidental that one of the effects of prenatal exposure to VPA is an increased risk for autism as well as cerebellar anomalies. A subgroup of children with autism and a subgroup of children exposed to VPA both demonstrate structural cerebellar anomalies. The most common model used in environmentally induced ASD models in rodents is the one induced by VPA [66].
Not infrequent and severe consequences of long-term postnatal use of phenytoin and VPA include cerebellar atrophy [67,68,69,70]. Although the mechanism of both prenatal and acquired postnatal effects on the cerebellum may be different, genetic studies suggest that the risk of cerebellar complications may be determined by variations in enzyme activities that metabolize drugs. Buehler et al. [54] showed this to be a fact. They studied infants with fetal hydantoin syndrome and confirmed reduced activity of epoxide hydrolase in those exposed and affected compared to both those exposed and unaffected and normal controls. CYP2C9 mutation (*2 or *3) reduces phenytoin metabolism by 25–50% and can increase the risk of phenytoin-related side effects. CYP2C9 polymorphism has been associated with a reduction in cerebellar white matter volume in epileptic users of phenytoin [69]. Animal studies confirmed that prenatal exposure to VPA is associated with loss of volume in the vermis and hemispheres. Ingram et al. [64] identified reduced Purkinje cells in the vermis with greater loss in the posterior lobe with parallel in some human autistic populations.
As newer and safer drugs become available for the treatment of epilepsy and other seizure disorders in women of childbearing age, the use of drugs such as VPA will likely continue to be reduced. It is important that women on these drugs need to be advised of the risks in pregnancy and screening measures and ongoing surveillance to assess fetal well-being be instituted.
Prenatal Alcohol Effects and Fetal Alcohol Sepctrum Disorder
Whether prenatal alcohol exposure (PAE) can harm the human embryo and fetus has been a contentious issue over the past century. Following seminal studies by Lemoine et al. [71] in France in 1968 and Jones et al. [72, 73] in the United States in 1973 did the irrefutable evidence of the harmful effects of alcohol in pregnancy become clear, and PAE is considered the most common teratogenic agent in humans. Based on extensive research in animals and humans, PAE has been demonstrated to cause a variety of structural and/or functional deficits in the developing fetus, even after a single binge episode or equivalent use in experimental situations [74,75,76].
In humans, the first reports were on infants and young children born to mothers who were known alcoholics. These children typically presented with intrauterine growth retardation, microcephaly, characteristic facial dysmorphic features of short palpebral fissure lengths of the eyes, abnormal and short midface with a smooth poorly formed philtrum and a thin vermilion border of the upper lip, risk to various birth defects including cleft palate, cardiac malformations, limb anomalies, and an increase in minor anomalies, with cognitive impairment and behavioral problems (Fig. 2). This presentation was called fetal alcohol syndrome (FAS) [73, 74, 77, 78]. Subsequently less visible signs of the prenatal effects of alcohol were identified in which affected children showed few or little of the facial and growth features but presented with cognitive and behavioral difficulties. The use of other terminologies such as fetal alcohol effects (FAE) , partial fetal alcohol syndrome (pFAS) , and alcohol-related neurodevelopmental disorder (ARND) was applied [79,80,81,82,83,84,85]. The term fetal alcohol spectrum disorder has often been used to include the whole spectrum of effects of PAE. Cook et al. [84] recently updated the fetal alcohol spectrum disorder (FASD) diagnostic guidelines in Canada, and the terminology has been changed to include two diagnostic categories, FASD with sentinel facial features (FAS) and FASD without sentinel facial features (previously called partial FAS and ARND).

The typical facial features of fetal alcohol syndrome in two infants
The diagnosis of FASD requires multidisciplinary team assessments to identify behavioral, cognitive, neurological, and dysmorphic features congruent with FASD [82]. This means that referrals for suspected cases are sent to the multidisciplinary team for a thorough evaluation by other specialists that includes specialist physicians (developmental pediatricians, geneticists, psychologists, speech and language therapists, occupational therapists, education specialists, and social work case workers). Details of the referral process, evaluations and steps in the diagnosis, and management recommendations are described in detail elsewhere [82, 84].
Evaluation of the brain is an important component of diagnosis. This includes an in-depth assessment of brain function using standardized testing of (1) cognition, (2) memory, (3) language, (4) academic achievement, (5) executive function (including impulse control and hyperactivity, adaptive behavior, social behavior, social skills or social communication, attention, affect regulation, motor skills, and neurological assessment of brain size, neuroanatomy, and neurophysiology (including neurologic examination and in some cases imaging)) [84].
There are many other conditions that can mimic FASD with an extensive differential diagnosis [86], and many comorbid conditions are often co-occurring in FASD individuals, some conditions at rates greater than 100 times the general population based on US data [87]. These children need to be identified as early as possible if therapy and interventions are to make a difference in their long-term prognosis, and so screening programs need to be introduced to afford early detection [88]. Many affected children and adults who are not identified or diagnosed until later in life can experience what has been referred to as secondary disabilities [89]. They can be lost in society and can experience apprehension by social service agents and foster care, school failure with early dropout, addiction problems, mental health difficulties, limited employment opportunities, homelessness, and involvement with crime and the justice system with frequent incarceration [89, 90].
The prevalence of fetal alcohol spectrum disorder (FASD) is estimated to be between 2.4% and 4.8% in a school-age population in the United States [91] and similar high rates of prevalence in a school-age population in Italy [92]. The highest rates at 18–26% were estimated in an at risk rural and lower socioeconomic community in South Africa [93]. Because of the high prevalence in most populations studied and the high costs to society of the condition, prevention of drinking in pregnancy should be a high priority of governments, social and health care professionals, and the alcohol industry [87, 94,95,96,97,98,99].
It is relevant that several of the brain domain impairments observed in PAE and FASD individuals exhibit these difficulties, in part, because of teratogenic effects of alcohol on the cerebellum and their respective connections to other regions of the brain. For example, the functions of motor and balance, eye tracking and visual–spacial perception, cognitive abilities, learning, language, emotional responses, and attention pathways are connected to the cerebellum. Many children with FASD have impairments in these functions. Many research reports and clinical descriptions in the literature to support the above association of cerebellar dysfunction and FASD are presented in the following pages.
Mechanisms for Alcohol Teratogenesis
Ethanol is toxic to the developing embryo and fetus. Alcohol readily crosses the placenta and the blood–brain barrier. Alcohol can affect normal placental function and cause altered blood flow, ischemia, and hypoxia to the fetus. There is also an interaction between the direct toxic effects and indirect or maternally mediated effects of alcohol [100].The mechanisms are complex and involve variables in the timing, frequency, and dose of exposure. Alcohol is known to act on or modulate many different target molecules’ multiple mechanisms, activated at different stages of embryonic and fetal development or at different dose thresholds of exposure and stages of development, resulting in diverse phenotypes [101,102,103]. The earlier the exposure of teratogenic factors during organogenesis , the greater the harm that is likely to occur [74, 103,104,105].
Molecular Pathways and Genetic Factors
PAE and FASD are perhaps best considered to be a prototypical multifactorial teratogenic disorder whereby both genetic predisposing factors and environmental exposures combine to have a variable phenotype (Fig. 3). It is evident that alcohol alone can be directly toxic to the embryo and fetus, but other factors also can either contribute to the risk (as aggravating factors) or have protective effects to some degree (a mitigating factor). PAE is both dose dependent (acute vs chronic exposure; frequency of exposure) and sensitive to critical periods of developmental stage. Factors shown to be protective include good nutrition prenatally and after birth [106], consistent and nurturing child care, early diagnosis with earlier interventions, and favorable genetic factors (particularly those involved in alcohol metabolism). According to May and Gossage [107], maternal risk is multidimensional, including factors related to quantity, frequency, and timing of alcohol exposure, maternal age, number of pregnancies, number of times the mother has given birth, the mother’s body size, nutrition, socioeconomic status, metabolism, religion, spirituality, depression, other drug use, and social relationships. Some risk factors in the child include poor nutrition; exposure to neglect; physical, emotional, or sexual abuse; repeated changes in caregivers and place of residence ; “unfavorable” genetics; and a diagnosis later in childhood [89]. It is well established that the genetic background of the mother and fetus influences the risk of ethanol-induced malformations [108]. The more efficient alcohol dehydrogenase (ADH) allele, ADH 1B*3, affords protection for FASD outcomes [109], while the maternal and fetal ADH1B*2 allele reduced the risk for FAS in a South African population (in comparison with ADH1B*1) [108]. For more recent reviews relevant to the importance of polymorphisms in the alcohol metabolizing pathway, the reader is referred to other reviews [110, 111] (Figs. 4 and 5).

Variable fetal outcomes from excessive ethanol exposure

A schematic representation of risk factors contributing to FASD

Oxidative pathways of alcohol metabolism . The enzymes alcohol dehydrogenase (ADH), cytochrome P450 2E1 (CYP2E1), and catalase all contribute to oxidative metabolism of alcohol. ADH, present in the fluid of the cell (i.e., cytosol), converts alcohol (i.e., ethanol) to acetaldehyde. This reaction involves an intermediate carrier of electrons, nicotinamide adenine dinucleotide (NAD+), which is reduced by two electrons to form NADH. Catalase, located in cell bodies called peroxisomes, requires hydrogen peroxide (H2O2) to oxidize alcohol. CYP2E1, present predominantly in the cell’s microsomes, assumes an important role in metabolizing ethanol to acetaldehyde at elevated ethanol concentrations. Acetaldehyde is metabolized mainly by aldehyde dehydrogenase 2 (ALDH2) in the mitochondria to form acetate and NADH (From Chudley [187])
A recent population-based prospective children’s health and development study from Britain confirmed a genetic risk to some children genetically predisposed to the effects of alcohol exposure in pregnancy [112]. The authors found four ADH genetic variants in alcohol metabolizing genes in 4,167 children which were strongly related to lower IQ at age 8, as was a risk allele score based on these four variants. All the mothers of these children took moderate amounts of alcohol during the pregnancy. The authors suggest that, even among women drinking moderate amounts of alcohol, subtle changes in exposure to alcohol due to an ability to metabolize the substrate may be important and offer some support to the hypothesis that even small amounts of alcohol in utero have an effect on future cognitive outcomes .
Alterations in a number of molecular pathways have been suggested as candidates responsible for the range of FASD phenotypes [101, 113, 114]. These include (1) alterations in the regulation of gene expression (e.g., reduced retinoic acid signaling [115, 116], homeobox gene expression, altered DNA methylation [117]); (2) interference with mitogenic and growth factor responses involved in neural stem cell proliferation, migration, and differentiation [118]; (3) disturbances in molecules that mediate cell–cell interactions (L1, NCAM, loss of trophic support, e.g., [119, 120]); (4) activation of molecular signaling controlling cell survival or death (growth factor deprivation, oxidative stress, apoptotic signaling and caspase-3 activation, suppression of NMDA glutamate and GABAA receptors, withdrawal-induced glutamatergic excitotoxicity), [121, 122]; (5) and derangements in glial proliferation, differentiation, and functioning [123].
Lombard et al. [124] utilized a computational candidate gene selection method that identified genes that may play a role in alcohol teratogenesis. Using a modification of the methodology called convergent functional genomics which combines data from human and animal studies, this group identified a short list of high-probability candidate genes, with the inclusion of additional lines of evidence in the presence of limited expression studies in an animal model and the absence of FAS linkage studies. From a list of 87 genes, the group prioritized key biological pathways significantly overrepresented among the top-ranked candidate genes. These pathways include the TGF-β signaling pathway, MAPK signaling pathway, and the Hedgehog signaling pathway.
The genes in the TGF-β signaling pathway may play pivotal roles during embryogenesis and development and have a potential role in the distinct characteristics associated with FAS, i.e., CNS dysfunction, craniofacial abnormalities, and growth retardation. CNS dysfunction is the most severe and permanent consequence of in utero alcohol exposure and the only feature present in all diagnostic categories in FASD. These observations make the TGF-β signaling pathway an important consideration, as it is essential in fetal and CNS development. Alcohol inhibits TGF-β-regulated processes such as cortical cell proliferation and neuronal migration, disrupts axonal (the major extension of a nerve cell) growth, and upregulates cell adhesion molecule expression [125]. TGF-β signaling pathway interacts with alcohol , and/or its metabolic breakdown products, and alcohol may have a detrimental effect on the efficiency of this developmentally essential pathway.
The MAPK pathway transmits many signals, leading to growth, differentiation, inflammation, and apoptosis responses [126]. This pathway is very complex and includes many protein components. MAPK pathway components are involved in the regulation of meiosis, mitosis, and postmitotic functions and in cell differentiation. The MAPK signaling pathway can be activated by a variety of stimuli as well as external stress factors, such as alcohol [127]. Using a mouse model of FAS, experimental manipulation of second-messenger pathways (that also impact on the MAPK pathway) completely reversed the action of ethanol on neuronal migration in vitro as well as in vivo [128].
The Hedgehog signaling pathway was also identified to contain several genes within the candidate list. This signaling pathway is a highly conserved and key regulator of embryonic development. Knockout mouse models lacking components of this pathway have been observed to develop malformations in the CNS, musculoskeletal system, gastrointestinal tract, and lungs [129]. FAS animal models have a similar craniofacial phenotype to mouse models treated with antibodies that block Hedgehog signaling components, specifically the sonic Hedgehog (Shh) molecule [130, 131 132]. Alcohol resulted in a significant decrease in Shh levels in the developing embryo, as well as a decrease in the level of other transcripts involved in Shh signaling. Addition of Shh after alcohol exposure led to fewer apoptotic (dead or dying) cranial neural crest cells and a decrease in craniofacial anomalies [131]. Altered function of genes in the Hedgehog signaling pathway may thus contribute to the brain malformations and dysfunction in FASD.
Epigenetics
Epigenetic mechanism as a cause of the diverse effect of PAE and FASD is emerging as a potentially important mediator of the FASD phenotype [133,134,135,136]. Epigenetics refers to modifications of DNA and its packaging that alter the accessibility of DNA to potentially regulate gene expression and cellular function without changes to the underlying genomic sequences [135, 137]. There are several mechanisms in which gene expression can be controlled, and the most studied epigenetic modification in human populations is DNA methylation. DNA methylation generally represses gene expression, but this relationship is less well defined for CpGs located within gene bodies and intergenic regions [138]. Furthermore, DNA methylation is closely associated with several key developmental processes, including genomic imprinting, tissue specification, and differentiation [139]. Prenatal alcohol exposure has been shown in animal studies to alter methylation which is predicted to alter gene expression and thus alter developmental processes [134, 140, 141].
There have been few human studies to test the role of changes in methylation and relationship to FASD. Several studies have demonstrated the effect of PAE on the H19 imprinted gene in both mice and humans [142, 143]. Altered expression of the H19 gene could interfere with normal growth mediated through the Igf2 gene. A smaller human study characterized the DNA methylation profile in buccal epithelial cells (BECs) from a small cohort of human FASD samples, identifying alterations in the epigenome of children with FASD, particularly within the protocadherin gene clusters, which are involved in producing proteins involved in cell adhesion [144]. A genome-wide DNA methylation study in mouse embryos exposed to ethanol also identified significant changes within several imprinted genes including both H19 and SLC22A18 [145]). The SLC22A18 gene is located in an imprinted region and plays a role in tumor suppression with other genes in the region mediating growth. A recent comparatively large study compared a cohort of FASD and alcohol-exposed children with controls through genome-wide DNA methylation patterns of BECs which were analyzed (Portales). Results from the study by Portales-Casamar et al. [146] further confirmed these findings, as five down-methylated probes in H19 and six in SLC22A18 were altered in the FASD cohort. With validation, these findings provide initial insight into the molecular mechanisms underlying the effects of PAE on children and present a potential role for DNA methylation in the etiology of FASD . It may also be possible to define a biomarker for alcohol exposure that may aid in the earlier diagnosis, referral, and treatment of this common disorder.
FASD and the Cerebellum
The earliest autopsy studies described in humans diagnosed with FAS and PAE identified errors in cell migration, agenesis or thinning of the corpus callosum, and anomalies in the cerebellum and brain stem [73, 147,148,149]. Subsequent imaging studies with newer technology and resolution were consistent with autopsy findings [150]. These showed overall volume reductions in the cranial, cerebral, and cerebellar vaults in FASD [151,152,153,154,155,156]. Furthermore, other studies have suggested that this decrease is not uniform but rather that the parietal lobe [153,154,155, 157], portions of the frontal lobe [154], and specific areas of the cerebellum [156, 158, 159] appear to be especially sensitive to alcohol insult (Fig. 6).

A MRI demonstrating a small cerebellum and vermis hypoplasia (arrow) in a child with FAS (From Fig. 1 in Autti-Rämö et al. [156].)
Studies of effects on brain volume using imaging techniques have reported disproportionate size reductions in the cerebellum [153, 156, 160,161,162]. Cardenas et al. [162] studied PAE individuals using a cerebellar parcellation tool kit with T1-weighted MRI to assess cerebellar size. They concluded that (1) PAE-related microcephaly is strongly related to cerebellar hemispheric volumes and (2) smaller cerebellar measures in FASD are not fully explained by microcephaly and suggest an additional direct effect of prenatal alcohol exposure on the cerebellum.
Experimental studies on animals confirmed that PAE targets certain areas of the brain, particularly the cerebellum and the craniofacial structures [74, 163, 164]. Nathaniel et al. [165, 166] showed that the cerebellum and the area and circumference of the vermal cerebellum were significantly reduced in ethanol-exposed pups compared with the pair-fed controls. Studies in rats showed that synaptic density of the molecular layer of the cerebellar lobule VI was decreased in 28-day-old animals which were exposed prenatally to ethanol [167].
Studies in the mouse cerebellum showed that microglia promote the death and subsequent engulfment of Purkinje cells that express activated caspase-3 when they are undergoing synaptogenesis [168]. Similar results were observed in a developing nematode C. elegans, where cells in the advanced caspase (CED-3)-dependent stage of degeneration could recover [169]. Sawant et al. [170] assessed fetal cerebellar Purkinje cell counts in an early-maturing region (lobules I–X) and a late-maturing region (lobules VIc–VII) from midsagittal sections of the cerebellar vermis in sheep. Third trimester-equivalent ethanol exposure caused a significant reduction in the fetal cerebellar Purkinje cell volume density and Purkinje cell number only in the early-maturing region, and as expected, the first trimester-equivalent ethanol exposure resulted in significant reductions in both the early- and late-maturing regions. The authors concluded prenatal ethanol exposure in the first trimester interferes with the genesis of Purkinje cells in an unselective manner, whereas exposure during the third trimester selectively kills postmitotic Purkinje cells in specific vermal regions during a vulnerable period of differentiation and synaptogenesis.
Chronic prenatal alcohol exposure on the immature central nervous system (CNS) profoundly inhibits insulin and insulin-like growth factor (IGF) signaling [171, 172]. They conclude that insulin-stimulated central nervous system neuronal survival mechanisms are significantly impaired by chronic gestational exposure to ethanol and that the abnormalities in insulin signaling mechanisms persist in the early postnatal period, which is critical for brain development. The same research group [173] observed ethanol dose-dependent reductions in cerebellar aspartyl (asparaginyl)-β-hydroxylase (AAH) immunoreactivity and significant impairments in insulin- and IGF-I-stimulated directional motility in granule neurons isolated from ethanol-exposed rat pup cerebella . In addition to reduced motility, the authors observed that chronic in vivo ethanol exposure mainly reduced the percentages of migrant adherent cells, consistent with previous reports indicating that ethanol impairs neuronal cell adhesion mechanisms and neuronal migration [102, 120]. Tong et al. [174] showed that abnormalities in cerebellar function following chronic prenatal ethanol exposure were associated with inhibition of insulin/IGF, canonical Wnt, and Notch pathways. Thomas et al. [175] showed that neonatal ethanol exposure induces cerebellar Purkinje and granule cell loss if exposure occurs before postnatal day (PD) 7 and that cerebellar damage may underlie ethanol-induced motor deficits. Exposure during PD 4/5 produced significantly more severe motor deficits and significantly more severe reductions in cerebellar and brainstem weights than did exposure later in life.
Another mechanism of disrupted development of the cerebellum involves synaptic defects. A recent study that showed reduced N-acetylaspartate NAA levels in children with PAE using MRS suggests impairment in the early developmental formation of dendritic arborizations and synaptic connections [176]. The study showed that additional finding of lower choline points to disrupted choline metabolism of membrane phospholipids with potentially reduced content of dendrites and synapses . The alcohol-related alterations in glutamate plus glutamine that was identified suggested a disruption of the glutamate–glutamine cycling involved in glutamatergic excitatory neurotransmission.
Fan et al. [177] have confirmed abnormalities in eyeblink conditioning and FASD using the MRI and DTI analyses. Using DTI (which is used to assess integrity of the white matter) they demonstrated a lower response (as measured by fractional anisotropy) bilaterally in the superior cerebellar peduncles and higher diffusivity in the left middle peduncle in the alcohol-exposed children compared to controls, and the findings correlated with poorer EBC performance. This may reflect poorer myelination in these large bundles of myelinated nerve fibers that connect the cerebellum to the brain stem. The authors conclude that FASD deficits in EBC are likely attributed to poorer myelinization in key regions of the cerebellar peduncles.
Clinical Consequences to Cerebellar Dysfunction in PAE and FASD
Many of the behavioral deficits seen in individuals with FASD, including spatial recognition, motor learning, and fine motor control, are mediated, in part, by the cerebellum [150]. There has been a long-standing recognition and association with cognitive function and cerebellar function [178,179,180,181]. Behavioral changes were clinically prominent in patients with lesions involving the posterior lobe of the cerebellum and the vermis, and in some cases they were the most noticeable aspects of the presentation [178]. As noted previously, there is a frequent occurrence of cerebellar defects in autism [182] and also in ADHD children [183]. Berquin et al. [183] showed vermal volume was significantly less in boys with ADHD. This reduction involved mainly the posterior inferior lobe (lobules VIII–X) but not the posterior superior lobe (lobules VI–VII). A cerebello–thalamo–prefrontal circuit dysfunction may subserve the motor control, inhibition, and executive function deficits encountered in ADHD. It is of interest that FASD children frequently present with attention difficulties, and there may be an overrepresentation of autism in PAE and/or FASD children and adults [184].
In a study of children with heavy prenatal alcohol exposure experience, significant deficits in isometric force production were identified that may impede their ability to perform basic motor skills and activities in everyday tasks [185]. In addition, another study results indicated children with FAS experience deficits in response programming and movement time production [186].
Summary
This chapter summarizes select teratogenic agents to illustrate the importance of the recognition of etiology, mechanisms of teratogenesis, pathogenesis, and clinical impact these agents have on the developing human and particularly cerebellar structural and functional consequences. Where appropriate and relevant, the emerging role and effects of genetic and epigenetic mechanisms are discussed. Emphasis has been given to common conditions and hence the greater attention to PAE and FASD. Because of the nature of teratogens, there is opportunity to prevent the occurrence of phenotypic consequences of these exposures through various prevention strategies.
References
Ujházy E, Mach M, Navarová J, Brucknerová I, Dubovický M. Teratology – past, present and future. Interdiscip Toxicol. 2012;5(4):163–8.
Wilson JG. Environment and birth defects. New York: Academic Press; 1973.
Frías JL, Gilbert-Barness E. Human teratogens: current controversies. Adv Pediatr Infect Dis. 2008;55:171–211.
Holmes LB. Human teratogens: update 2010. Birth Defects Res A Clin Mol Teratol. 2011;91(1):1–7.
Persaud TVN, Chudley AE, Skalko RG. Basic concepts in teratology. New York: Alan R. Liss; 1985.
Brent RL, Beckman DA. Environmental teratogens. Bull N Y Acad Med. 1990;66(2):123–63.
Shakiba A. The role of the cerebellum in neurobiology of psychiatric disorders. Neurol Clin. 2014;32(4):1105–15.
Poretti A, Boltshauser E, Doherty D. Cerebellar hypoplasia: differential diagnosis and diagnostic approach. Am J Med Genet C: Semin Med Genet. 2014;166C(2):211–26.
Stoodley CJ. The cerebellum and neurodevelopmental disorders. Cerebellum. 2016;15(1):34–7.
Mariën P, Ackermann H, Adamaszek M, Barwood CH, Beaton A, Desmond J, De Witte E, Fawcett AJ, Hertrich I, Küper M, Leggio M, Marvel C, Molinari M, Murdoch BE, Nicolson RI, Schmahmann JD, Stoodley CJ, Thürling M, Timmann D, Wouters E, Ziegler W. Consensus paper: language and the cerebellum: an ongoing enigma. Cerebellum. 2014;13(3):386–410.
Holson RR, Gazzara RA, Ferguson SA, Ali SF, Laborde JB, Adams J. Gestational retinoic acid exposure: a sensitive period for effects on neonatal mortality and cerebellar development. Neurotoxicol Teratol. 1997;19(5):335–46.
Pastuszak AL, Schler L, Speck Martins CE, et al. Use of misoprostol during pregnancy and Moebius’ syndrome in infants. N Engl J Med. 1998;338(26):1881–5.
Merlini L, Fluss J, Dhouib A, Vargas MI, Becker M. Mid-hindbrain malformations due to drugs taken during pregnancy. J Child Neurol. 2014;29(4):538–44.
Adams Waldorf KM, McAdams RM. Influence of infection during pregnancy on fetal development. Reproduction. 2013;146(5):151–62.
Neu N, Duchon J, Zachariah P. TORCH infections. Clin Perinatol. 2015;42(1):77–103.
Barkovich AJ, Raybaud C. Pediatric neuroimaging. 5th ed. Philadelphia: Lippincott Williams & Wilkins; 2012.
Gregg NM. Congenital cataract following German measles in the mother. Trans Ophthalmol Soc Aust. 1941;3:35–45.
Rosenberg HS, Oppenheimer EH, Esterly JR. Congenital rubella syndrome: the late effects and their relation to early lesions. Perspect Pediatr Pathol. 1981;6:183–202.
Dudgeon JA. Congenital rubella. J Pediatr. 1975;87:1078–86.
Townsend JJ, Wolinsky JS, Baringer JR. The neuropathology of progressive rubella panencephalitis of late onset. Brain. 1976;99(1):81–90.
Cluver C, Meyer R, Odendaal H, Geerts L. Congenital rubella with agenesis of the inferior cerebellar vermis and total anomalous pulmonary venous drainage. Ultrasound Obstet Gynecol. 2013;42(2):235–7.
Webster WS. Teratogen update: congenital rubella. Teratology. 1998;58:13–23.
Burd I, Balakrishnan B, Kannan S. Models of fetal brain injury, intrauterine inflammation, and preterm birth. Am J Reprod Immunol. 2012 Apr;67(4):287–94.
Sze G, Lee SH. Infectious disease. In: Lee SH, KCVG R, Zimmerman RA, editors. Cranial MRI and CT. 4th ed. New York: Mc Graw-Hill; 1999.
Huleihel M, Golan H, Hallak M. Intrauterine infection/inflammation during pregnancy and offspring brain damages: possible mechanisms involved. Reprod Biol Endocrinol. 2004;2:17.
Rasmussen SA, Jamieson DJ, Honein MA, Petersen LR. Zika virus and birth defects – reviewing the evidence for causality. N Engl J Med. 2016;374(20):1981–7.
de Fatima Vasco Aragao M, van der Linden V, Brainer-Lima AM, Coeli RR, Rocha MA, Sobral da Silva P, Dur Cecosta Gomes de Carvalho M, van der Linden A, Cesario de Holanda A, Valenca MM. Clinical features and neuroimaging (CT and MRI) findings in presumed Zika virus related congenital infection and microcephaly: retrospective case series study. BMJ. 2016;353:i1901.
van der Linden V, Filho EL, Lins OG, van der Linden A, Aragão Mde F, Brainer-Lima AM, Cruz DD, Rocha MA, Sobral da Silva PF, Carvalho MD, do Amaral FJ, Gomes JA, Ribeiro de Medeiros IC, Ventura CV, Ramos RC. Congenital Zika syndrome with arthrogryposis: retrospective case series study. BMJ. 2016;354:i3899.
Faria NR, Azevedo RSS, Kraemer MUG, Souza R, Cunha MS, Hill SC, et al. Zika virus in the Americas: early epidemiological and genetic findings. Science. 2016;352:345–9.
Araujo AQ, Silva MT, Araujo AP. Zika virus-associated neurological disorders: a review. Brain. 2016;139(Pt 8):2122–30.
Soares de Oliveira-Szejnfeld P, Levine D, Melo AS, Amorim MM, Batista AG, Chimelli L, et al. Congenital brain abnormalities and Zika Virus: what the radiologist can expect to see prenatally and postnatally. Radiology. 2016;281:203–18. 161584
Leal MC, Muniz LF, Ferreira TS, et al. Hearing loss in infants with microcephaly and evidence of congenital Zika virus infection – Brazil, November 2015–May 2016. MMWR Morb Mortal Wkly Rep. 2016;65:917–9.
Dick GW, Kitchen SF, Haddow AJ. Zika virus. I. Isolations and serological specificity. Trans R Soc Trop Med Hyg. 1952;46:509–20.
Macnamara FN. Zika virus: a report on three cases of human infection during an epidemic of jaundice in Nigeria. Trans R Soc Trop Med Hyg. 1954;48:139–45.
Russell K, Oliver SE, Lewis L, Barfield WD, Cragan J, Meaney-Delman D, et al. Update: interim guidance for the evaluation and Management of Infants with possible congenital Zika virus infection – United States, August 2016. MMWR Morb Mortal Wkly Rep. 2016;65(33):870–8.
Paixão ES, Barreto F, Teixeira Mda G, Costa Mda C, Rodrigues LC. History, epidemiology, and clinical manifestations of Zika: a systematic review. Am J Public Health. 2016;106(4):606–12.
Hazin AN, Poretti A, Turchi Martelli CM, Huisman TA, Microcephaly Epidemic Research Group. Computed tomographic findings in microcephaly associated with Zika virus. N Engl J Med. 2016;374(22):2193–5.
Garcez PP, Loiola EC, Madeiro da Costa R, Higa LM, Trindade P, et al. Zika virus impairs growth in human neurospheres and brain organoids. Science. 2016;352(6287):816–8.
Tang H, Hammack C, Ogden SC, Wen Z, Qian X, Li Y, et al. Zika virus infects human cortical neural progenitors and attenuates their growth. Cell Stem Cell. 2016;18(5):587–90.
Durbin AP. Vaccine development for Zika virus-timelines and strategies. Semin Reprod Med. 2016 Sep;8
Barreto ML, Barral-Netto M, Stabeli R, Almeida-Filho N, Vasconcelos PF, Teixeira M, et al. Zika virus and microcephaly in Brazil: a scientific agenda. Lancet. 2016;387:919–21.
Chang SI, McAuley JW. Pharmacotherapeutic issues for women of childbearing age with epilepsy. Ann Pharmacother. 1998;32(7–8):794–801.
Speidel BD, Meadow SR. Maternal epilepsy and abnormalities of the fetus and the newborn. Lancet. 1972;2:839–43.
Hill RM, Verniaud WM, Horning MG, McCulley LB, Morgan NF. Infants exposed in utero t antiepileptic drugs: a prospective study. Am J Dis Child. 1974;127:645–53.
Hanson JW, Smith DW. The fetal hydantoin syndrome. J Pediatr. 1975;87:285–90.
Hanson JW, Myrianthopoulos NC, Harvey MA, Smith DW. Risks to the offspring of women treated with hydantoin anticonvulsants, with emphasis on the fetal hydantoin syndrome. J Pediatr. 1976;89(4):662–8.
Seip M. Growth retardation, dysmorphic facies and minor malformations following massive exposure to phenobarbitone in utero. Acta Paediatr Scand. 1976;65:617–21.
Jones KL, Lacro RV, Johnson KA, Adams J. Pattern of malformations in the children of women treated with carbamazepine during pregnancy. N Engl J Med. 1989;320:1661–6.
Lindhout D, Hoppener RJEA, Meinardi H. Teratogenicity of antiepilepticdrug combinations with special emphasis on epoxidation (of carbamazepine). Epilepsia. 1984;25:77–83.
Holmes LB, Harvey EA, Coull BA, et al. The teratogenicity of anticonvulsant drugs. N Engl J Med. 2001;344(15):1132–8.
Morrow J, Russell A, Guthrie E, Parsons L, Robertson I, Waddell R, et al. Malformation risks of antiepileptic drugs in pregnancy: a prospective study from the UK epilepsy and pregnancy register. J Neurol Neurosurg Psychiatry. 2006;77(2):193–8.
Dansky LV, Finnell RH. Parental epilepsy, anticonvulsant drugs, and reproductive outcome: epidemiologic and experimental findings spanning three decades; 2: human studies. Reprod Toxicol. 1991;5(4):301–35.
Jentink J, Loane MA, Dolk H, Barisic I, Garne E, Morris JK, de Jong-van den Berg LT, EUROCAT Antiepileptic Study Working Group. Valproic acid monotherapy in pregnancy and major congenital malformations. N Engl J Med. 2010;362(23):2185–93.
Buehler BA, Delimont D, van Waes M, Finnell RH. Prenatal prediction of risk of the fetal hydantoin syndrome. N Engl J Med. 1990;322(22):1567–72.
Strickler SM, Dansky LV, Miller MA, Seni M-H, Andermann E, Spielberg SP. Genetic predisposition to phenytoin-induced birth defects. Lancet. 1985;2:746–9.
Wells PG, Winn LM. Biochemical toxicology of chemical teratogenesis. Clin Rev Biochem Mol Biol. 1996;31:1–40.
Hill DS, Wlodarczyk BJ, Palacios AM, Finnell RH. Teratogenic effects of antiepileptic drugs. Expert Rev Neurother. 2010;10(6):943–59.
DiLiberti JH, Farndon PA, Dennis NR, Curry CJ. The fetal valproate syndrome. Am J Med Genet. 1984;19(3):473–81.
Ardinger HH, Atkin JF, Blackston RD, Elsas LJ, Clarren SK, Livingstone S, et al. Verification of the fetal valproate syndrome phenotype. Am J Med Genet. 1988;29(1):171–85.
Winter RM, Donnai D, Burn J, Tucker SM. Fetal valproate syndrome: is there a recognisable phenotype? J Med Genet. 1987;24(11):692–5.
Morrow JI, Hunt SJ, Russell AJ, et al. Folic acid use and major congenital malformations in offspring of women with epilepsy: a prospective study from the UK epilepsy and pregnancy register. J Neurol Neurosurg Psychiatry. 2009;80(5):506–11.
Christianson AL, Chesler N, Kromberg JG. Fetal valproate syndrome: clinical and neuro-developmental features in two sibling pairs. Dev Med Child Neurol. 1994;36(4):361–9.
Christensen J, Grønborg TK, Sørensen MJ, Schendel D, Parner ET, Pedersen LH, Vestergaard M. Prenatal valproate exposure and risk of autism spectrum disorders and childhood autism. JAMA. 2013;309(16):1696–703.
Ingram JL, Peckham SM, Tisdale B, Rodier PM. Prenatal exposure of rats to valproic acid reproduces the cerebellar anomalies associated with autism. Neurotoxicol Teratol. 2000;22(3):319–24.
Kim KC, Kim P, Go HS, Choi CS, Park JH, Kim HJ, et al. Male-specific alteration in excitatory post-synaptic development and social interaction in pre-natal valproic acid exposure model of autism spectrum disorder. J Neurochem. 2013;124(6):832–43.
Ergaz Z, Weinmstein-Fudim L, Ornoy A. Genetic and non-genetic animal models for autism spectrum disorders (ASD). Reprod Toxicol. 2016;64:116–40.
Ghosh VB, Kapoor S, Prakash A, Bhatt S. Cerebellar atrophy in a child with valproate toxicity. Indian J Pediatr. 2011;78(8):999–1001.
Papazian O, Cañizales E, Alfonso I, Archila R, Duchowny M, Aicardi J. Reversible dementia and apparent brain atrophy during valproate therapy. Ann Neurol. 1995;38(4):687–91.
Twardowschy CA, Werneck LC, Scola RH, Borgio JG, De Paola L, Silvado C. The role of CYP2C9 polymorphisms in phenytoin-related cerebellar atrophy. Seizure. 2013;22(3):194–7.
Ney GC, Lantos G, Barr WB, Schaul N. Cerebellar atrophy in patients with long-term phenytoin exposure and epilepsy. Arch Neurol. 1994;51(8):767–71. Mar;42(1):77–103
Lemoine P, Harousseau H, Borteyru JP, Menuet JC. Les enfants de parents alcooliques. Ouest Med. 1968;21:476–82.
Jones KL, Smith DW, Ulleland CN, Streissguth P. Pattern of malformation in offspring of chronic alcoholic mothers. Lancet. 1973;1(7815):1267–71.
Jones KL, Smith DW. Recognition of the fetal alcohol syndrome in early infancy. Lancet. 1973;302(7836):999–1001.
Sulik KK, Johnston MC, Webb MA. Fetal alcohol syndrome: embryogenesis in a mouse model. Science. 1981;214(4523):936–8.
Valenzuela CF, Morton RA, Diaz MR, Topper L. Does moderate drinking harm the fetal brain? Insights from animal models. Trends Neurosci. 2012;35(5):284–92.
Sadrian B, Lopez-Guzman M, Wilson DA, Saito M. Distinct neurobehavioral dysfunction based on the timing of developmental binge-like alcohol exposure. Neuroscience. 2014;280:204–19.
Clarren SK. Recognition of fetal alcohol syndrome. J Am Med Assoc. 1981;245(23):2436–9.
Clarren SK, Smith DW. The fetal alcohol syndrome. Lamp. 1978;35(10):4–7.
Stratton K, Howe C. Battaglia. Fetal alcohol syndrome: diagnosis, epidemiology, prevention, and treatment. Institute of Medicine (IOM). Washington, DC: National Academy Press; 1996.
Aase JM, Jones KL, Clarren SK. Do we need the term “FAE”? Pediatrics. 1995;95(3):428–30.
Astley SJ, Clarren SK. Diagnosing the full spectrum of fetal alcohol-exposed individuals: introducing the 4-digit diagnostic code. Alcohol Alcohol. 2000;35(4):400–10.
Chudley AE, Conry J, Cook JL, Loock C, Rosales T, LeBlanc N, Public Health Agency of Canada’s National Advisory Committee on Fetal Alcohol Spectrum Disorder. Fetal alcohol spectrum disorder: Canadian guidelines for diagnosis. CMAJ. 2005;172(5 Suppl):S1–S21.
Hoyme HE, May PA, Kalberg WO, Kodituwakku P, Gossage JP, Trujillo PM, et al. A practical clinical approach to diagnosis of fetal alcohol spectrum disorders: clarification of the 1996 Institute of Medicine criteria. Pediatrics. 2005;115(1):39–47.
Cook JL, Green CR, Lilley CM, Anderson SM, Baldwin ME, Chudley AE, Canada Fetal Alcohol Spectrum Disorder Research Network, et al. Fetal alcohol spectrum disorder: a guideline for diagnosis across the lifespan. CMAJ. 2016;188(3):191–7.
Hoyme HE, Kalberg WO, Elliott AJ, Blankenship J, Buckley D, Marais AS, et al. Updated clinical guidelines for diagnosing fetal alcohol spectrum disorders. Pediatrics. 2016;138(2) pii: e20154256. doi: 10.1542/peds.2015-4256. Epub 2016 Jul 27.
Leibson T, Neuman G, Chudley AE, Koren G. The differential diagnosis of fetal alcohol spectrum disorder. J Popul Ther Clin Pharmacol. 2014;21(1):e1–e30.
Popova S, Lange S, Shield K, Mihic A, Chudley AE, Mukherjee RA, Bekmuradov D, Rehm J. Comorbidity of fetal alcohol spectrum disorder: a systematic review and meta-analysis. Lancet. 2016;387(10022):978–87.
Goh YI, Chudley AE, Clarren SK, Koren G, Orrbine E, et al. Development of Canadian screening tools for fetal alcohol spectrum disorder. Can J Clin Pharmacol. 2008;15(2):e344–66.
Streissguth A, Barr H, Kogan J, Bookstein F. Primary and secondary disabilities in fetal alcohol syndrome. In: Streissguth AP, Kanter J, editors. The challenge of fetal alcohol syndrome: overcoming secondary disabilities. Seattle: University of Washington Press; 1997.
Streissguth AP, Bookstein FL, Barr HM, Sampson PD, O’Malley K, Young JK. Risk factors for adverse life outcomes in fetal alcohol syndrome and fetal alcohol effects. J Dev Behav Pediatr. 2004;25(4):228–38.
May PA, Baete A, Russo J, Elliott AJ, Blankenship J, Kalberg WO, et al. Prevalence and characteristics of fetal alcohol spectrum disorders. Pediatrics. 2014;134(5):855–66.
May PA, Fiorentino D, Coriale G, Kalberg WO, Hoyme HE, Aragon AS, et al. Prevalence of children with severe fetal alcohol spectrum disorders in communities near Rome, Italy: new estimated rates are higher than previous estimates. Int J Environ Res Public Health. 2011;8(6):2331–51.
May PA, de Vries MM, Marais AS, Kalberg WO, Adnams CM, Hasken JM, et al. The continuum of fetal alcohol spectrum disorders in four rural communities in South Africa: prevalence and characteristics. Drug Alcohol Depend. 2016;159:207–18.
Astley SJ, Bailey D, Talbot C, Clarren SK. Fetal alcohol syndrome (FAS) primary prevention through FAS diagnosis: I. Identification of high-risk birth mothers through the diagnosis of their children. Alcohol Alcohol. 2000;35(5):499–508.
Sulik KK, O’Leary-Moore SK, Riley EP. Better safe than sorry. BJOG. 2012;119(10):1159–61.
Avery MR, Droste N, Giorgi C, Ferguson A, Martino F, Coomber K, Miller P. Mechanisms of influence: alcohol industry submissions to the inquiry into fetal alcohol spectrum disorders. Drug Alcohol Rev. 2016;35:665.
Popova S, Lange S, Burd L, Rehm J. Canadian children and youth in care: the cost of fetal alcohol spectrum disorder. Child Youth Care Forum. 2014;43:83–96.
Popova S, Lange S, Burd L, Rehm J. The economic burden of fetal alcohol spectrum disorder in Canada in 2013. Alcohol Alcohol. 2016;51(3):367–75.
Riley EP, Clarren S, Weinberg J, Johnsson E, editors. Fetal alcohol spectrum disorder: management and policy perspectives of FASD. New York: Wiley-Blackwell; 2011.
Randall CL, Ekblad U, Anton RF. Perspectives on the pathophysiology of fetal alcohol syndrome. Alcohol Clin Exp Res. 1990;14(6):807–12.
Goodlett CR, Gilliam DM, Nichols JM, West JR. Genetic influences on brain growth restriction induced by development exposure to alcohol. Neurotoxicology. 1989;10(3):321–34.
Goodlett CR, Horn KH, Zhou FC. Alcohol teratogenesis: mechanisms of damage and strategies for intervention. Exp Biol Med (Maywood). 2005;230:394–406.
Sulik KK. Fetal alcohol spectrum disorder: pathogenesis and mechanisms. Handb Clin Neurol. 2014;125:463–75.
Parnell SE, O’Leary-Moore SK, Godin EA, Dehart DB, Johnson BW, Allan Johnson G, et al. Magnetic resonance microscopy defines ethanol-induced brain abnormalities in prenatal mice: effects of acute insult on gestational day 8. Alcohol Clin Exp Res. 2009;33(6):1001–11.
Parnell SE, Holloway HT, O’Leary-Moore SK, Dehart DB, Paniaqua B, et al. Magnetic resonance microscopy-based analyses of the neuro-anatomical effects of gestational day 9 ethanol exposure in mice. Neurotoxicol Teratol. 2013;39:77–83.
Young JK, Giesbrecht HE, Eskin MN, Aliani M, Suh M. Nutrition implications for fetal alcohol spectrum disorder. Adv Nutr. 2014;5(6):675–92.
May PA, Gossage JP. Maternal risk factors for fetal alcohol spectrum disorders: not as simple as it might seem. Alcohol Res Health. 2011;34(1):15–26.
Warren KR, Li TK. Genetic polymorphisms: impact on the risk of fetal alcohol spectrum disorders. Birth Defects Res A Clin Mol Teratol. 2005;73(4):195–203.
McCarver DG, Thomasson HR, Martier SS, Sokol RJ, Li T. Alcohol dehydrogenase-2*3 allele protects against alcohol-related birth defects among African Americans. J Pharmacol Exp Ther. 1997;283(3):1095–101.
Chudley AE. Genetic factors contributing to fetal alcohol spectrum disorder. In: Riley EP, Clarren S, Weinberg J, Johnsson E, editors. Fetal alcohol spectrum disorder: management and policy perspectives of FASD. Weinheim: Wiley; 2011.
Corkery T, Chudley AE. A review of genetic and epigenetic factors in Fetal Alcohol Spectrum Disorder (FASD). XLIIIèmes Journées Nationales de Néonatologie 2013. 33 Progress en Néonatologie. Jarreau P-H et Moriette G coord. Paris.
Lewis SJ, Zuccolo L, Davey Smith G, Macleod J, Rodriguez S, Draper ES, et al. Fetal alcohol exposure and IQ at age 8: evidence from a population-based birth-cohort study. PLoS One. 2012;7(11):e49407.
Guerri C. Mechanisms involved in central nervous system dysfunctions induced by prenatal ethanol exposure. Neurotox Res. 2002;4(4):327–35.
Guerri C, Bazinet A, Riley EP. Foetal alcohol spectrum disorders and alterations in brain and behaviour. Alcohol Alcohol. 2009;44(2):108–14.
Kot-Leibovich H, Fainsod A. Ethanol induces embryonic malformations by competing for retinaldehyde dehydrogenase activity during vertebrate gastrulation. Dis Model Mech. 2009;2(5–6):295–305.
Shabtai Y, Jubran H, Nassar T, Hirschberg J, Fainsod A. Kinetic characterization and regulation of the human retinaldehyde dehydrogenase 2 enzyme during production of retinoic acid. Biochem J. 2016;473(10):1423–31.
Deltour L, Ang HL, Duester G. Ethanol inhibition of retinoic acid synthesis as a potential mechanism for fetal alcohol syndrome. FASEB J. 1996;10(9):1050–7.
Miranda RC, Santillano DR, Camarillo C, Dohrman D. Modeling the impact of alcohol on cortical development in a dish: strategies from mapping neural stem cell fate. Methods Mol Biol. 2008;447:151–68.
Wilkemeyer MF, Menkari CE, Charness ME. Novel antagonists of alcohol inhibition of l1-mediated cell adhesion: multiple mechanisms of action. Mol Pharmacol. 2002;62(5):1053–60.
Minana R, Climent E, Barettino D, Segui JM, Renau-Piqueras J, Guerri C. Alcohol exposure alters the expression pattern of neural cell adhesion molecules during brain development. J Neurochem. 2000;75:954–64.
Guerri C, Montoliu C, Renau-Piqueras J. Involvement of free radical mechanism in the toxic effects of alcohol: implications for fetal alcohol syndrome. Adv Exp Med Biol. 1994;366:291–305.
Miller L, Shapiro AM, Wells PG. Embryonic catalase protects against ethanol-initiated DNA oxidation and teratogenesis in acatalasemic and transgenic human catalase-expressing mice. Toxicol Sci. 2013;134(2):400–11.
Guerri C, Pascual M, Renau-Piqueras J. Glia and fetal alcohol syndrome. Neurotoxicology. 2001;22(5):593–9.
Lombard Z, Tiffin N, Hofmann O, Bajic VB, Hide W, Ramsay M. Computational selection and prioritization of candidate genes for fetal alcohol syndrome. BMC Genomics. 2007;8:389.
Miller MW, Luo J. Effects of ethanol and transforming growth factor beta (TGF beta) on neuronal proliferation and nCAM expression. Alcohol Clin Exp Res. 2002;26(8):1281–5.
Krens SF, Spaink HP, Snaar-Jagalska BE. Functions of the MAPK family in vertebrate-development. FEBS Lett. 2006;580(21):4984–90.
Aroor AR, Shukla SD. MAP kinase signaling in diverse effects of ethanol. Life Sci. 2004;74(19):2339–64.
Kumada T, Jiang Y, Cameron DB, Komuro H. How does alcohol impair neuronal migration? J Neurosci Res. 2007;85(3):465–70.
Ingham PW, McMahon AP. Hedgehog signaling in animal development: paradigms and principles. Genes Dev. 2001;15(23):3059–87.
Chen SY, Periasamy A, Yang B, Herman B, Jacobson K, Sulik KK. Differential sensitivity of mouse neural crest cells to ethanol-induced toxicity. Alcohol. 2000;20(1):75–81.
Ahlgren SC, Bronner-Fraser M. Inhibition of sonic hedgehog signaling in vivo results in craniofacial neural crest cell death. Curr Biol. 1999;9(22):1304–14.
Ahlgren SC, Thakur V, Bronner-Fraser M. Sonic hedgehog rescues cranial neural crest from cell death induced by ethanol exposure. Proc Natl Acad Sci U S A. 2002;99(16):10476–81.
Feil R, Fraga MF. Epigenetics and the environment: emerging patterns and implications. Nat Rev Genet. 2012;13:97–109.
Haycock PC. Fetal alcohol spectrum disorders: the epigenetic perspective. Biol Reprod. 2009;81:607.
Kobor MS, Weinberg J. Focus on: epigenetics and fetal alcohol spectrum disorders. Alcohol Res Health. 2011;34(1):29–37.
Liyanage VR, Curtis K, Zachariah RM, Chudley AE, Rastegar M. Overview of the genetic basis and epigenetic mechanisms that contribute to FASD pathobiology. Curr Top Med Chem. 2016;17:808.
Bird A. Perceptions of epigenetics. Nature. 2007;447:396–8.
Jones PA. Functions of DNA methylation: islands, start sites, gene bodies and beyond. Nat Rev Genet. 2012;13(7):484–92.
Smith ZD, Meissner A. DNA methylation: roles in mammalian development. Nat Rev Genet. 2013;14:204–20.
Garro AJ, McBeth DL, Lima V, Lieber CS. Ethanol consumption inhibits fetal DNA methylation in mice: implications for the fetal alcohol syndrome. Alcohol Clin Exp Res. 1991;15(3):395–8.
Kaminen-Ahola N, Ahola A, Maga M, Mallitt KA, Fahey P, Cox TC, Whitelaw E, Chong S. Maternal ethanol consumption alters the epigenotype and the phenotype of offspring in a mouse model. PLoS Genet. 2010;6(1):e1000811.
Haycock PC, Ramsay M. Exposure of mouse embryos to ethanol during preimplantation development: effect on DNA methylation in the h19 imprinting control region. Biol Reprod. 2009;81:618–27.
Stouder C, Somm E, Paoloni-Giacobino A. Prenatal exposure to ethanol: a specific effect on the H19 gene in sperm. Reprod Toxicol. 2011;31:507–12.
Laufer BI, Kapalanga J, Castellani CA, Diehl EJ, Yan L, Singh SM. Associative DNA methylation changes in children with prenatal alcohol exposure. Epigenomics. 2015;7(8):1259–74.
Liu Y, Balaraman Y, Wang G, Nephew KP, Zhou FC. Alcohol exposure alters DNA methylation profiles in mouse embryos at early neurulation. Epigenetics. 2009;4:500–11.
Portales-Casamar E, Lussier AA, Jones MJ, MacIsaac JL, Edgar RD, Mah SM, et al. DNA methylation signature of human fetal alcohol spectrum disorder. Epigenetics Chromatin. 2016;9:25.
Clarren SK. Central nervous system malformations in two offspring of alcoholic women. Birth Defects-Orig. 1977;13:151–3.
Wizniewski K. A clinical neuropathological study of the fetal alcohol syndrome. Neuropediatrics. 1998;14:197–201.
Pfeiffer J, Majewski F, Fischbach H, Bierich JR, Volk B. Alcohol embryo- and fetopathy. J Neurol Sci. 1979;41:125–37.
Guerri C. Neuroanatomical and neurophysiological mechanisms involved in central nervous system dysfunctions induced by prenatal alcohol exposure. Alcohol Clin Exp Res. 1998;22:304–12.
Mattson SN, Riley EP, Jernigan TL, Ehlers CL, Delis DC, Jones KL, et al. Fetal alcohol syndrome: a case report of neuropsychological, MRI and EEG assessment of two children. Alcohol Clin Exp Res. 1992;16(5):1001–3.
Swayze VW 2nd, Johnson VP, Hanson JW, Piven J, Sato Y, Giedd JN, Mosnik D, Andreasen NC. Magnetic resonance imaging of brain anomalies in fetal alcohol syndrome. Pediatrics. 1997;99(2):232–40.
Archibald SL, Fennema-Notestine C, Gamst A, Riley EP, Mattson SN, Jernigan TL. Brain dysmorphology in individuals with severe prenatal alcohol exposure. Dev Med Child Neurol. 2001;43:148–54.
Sowell ER, Thompson PM, Mattson SN, et al. Regional brain shape abnormalities persist into adolescence after heavy prenatal alcohol exposure. Cereb Cortex. 2002;12:856–65.
Sowell ER, Thompson PM, Peterson BS, Mattson SN, Welcome SE, Henkenius AL, et al. Mapping cortical gray matter asymmetry patterns in adolescents with heavy prenatal alcohol exposure. NeuroImage. 2002;17(4):1807–19.
Autti-Rämö I, Autti T, Korkman M, Kettunen S, Salonen O, Valanne L. MRI findings in children with school problems who had been exposed prenatally to alcohol. Dev Med Child Neurol. 2002;44(2):98–106.
Sowell ER, Thompson PM, Mattson SN, Tessner KD, Jernigan TL, Riley EP, Toga AW. Voxel-based morphometric analyses of the brain in children and adolescents prenatally exposed to alcohol. Neuroreport. 2001;12(3):515–23.
Sowell ER, Jernigan TL, Mattson SN, Riley EP, Sobel DF, Jones KL. Abnormal development of the cerebellar vermis in children prenatally exposed to alcohol: size reduction in lobules I–V. Alcohol Clin Exp Res. 1996;20(1):31–4.
O’Hare ED, Kan E, Yoshii J, et al. Mapping cerebellar vermal morphology and cognitive correlates in prenatal alcohol exposure. Neuroreport. 2005;16:1285–90.
Bookstein FL, Streissguth AP, Connor PD, Sampson PD. Damage to the human cerebellum from prenatal alcohol exposure: the anatomy of a simple biometrical explanation. Anat Rec B New Anat. 2006;289(5):195–209.
Chen X, Coles CD, Lynch ME, Hu X. Understanding specific effects of prenatal alcohol exposure on brain structure in young adults. Hum Brain Mapp. 2012;33:1663–76.
Cardenas VA, Price M, Infante MA, Moore EM, Mattson SN, Riley EP, Fein G. Automated cerebellar segmentation: validation and application to detect smaller volumes in children prenatally exposed to alcohol. Neuroimage Clin. 2014;4:295–301.
Sulik KK, Lauder JM, Dehart DB. Brain malformations in prenatal mice following acute maternal ethanol administration. Int J Dev Neurosci. 1984;2(3):203–14.
Sulik KK. Genesis of alcohol-induced craniofacial dysmorphism. Exp Biol Med (Maywood). 2005;230(6):366–75.
Nathaniel EJ, Nathaniel DR, Mohamed S, Nathaniel L, Kowalzik C, Nahnybida L. Prenatal ethanol exposure and cerebellar development in rats. Exp Neurol. 1986;93(3):601–9.
Nathaniel EJ, Nathaniel DR, Mohamed SA, Nahnybida L, Nathaniel L. Growth patterns of rat body, brain, and cerebellum in fetal alcohol syndrome. Exp Neurol. 1986;93(3):610–20. te
Lancaster F, Samorajski T. Prenatal ethanol exposure decreases synaptic density in the molecular layer of the cerebellum. Alcohol Alcohol Suppl. 1987;1:477–80.
Marin-Teva JL, Dusart I, Colin C, Gervais A, van Rooijen N, Mallat M. Microglia promote the death of developing Purkinje cells. Neuron. 2004;41:535–47.
Reddien PW, Cameron S, Horvitz HR. Phagocytosis promotes programmed cell death in C. elegans. Nature. 2001;412:198–202.
Sawant OB, Lunde ER, Washburn SE, Chen WJ, Goodlett CR, Cudd TA. Different patterns of regional Purkinje cell loss in the cerebellar vermis as a function of the timing of prenatal ethanol exposure in an ovine model. Neurotoxicol Teratol. 2013;35:7–13.
de la Monte SM, Wands JR. Chronic gestational exposure to ethanol impairs insulin-stimulated survival and mitochondrial function in cerebellar neurons. Cell Mol Life Sci. 2002;59(5):882–93.
de la Monte SM, Wands JR. Role of central nervous system insulin resistance in fetal alcohol spectrum disorders. J Popul Ther Clin Pharmacol. 2010;17(3):e390–404. Epub 2010 Oct 26
de la Monte SM, Tong M, Carlson RI, Carter JJ, Longato L, Silbermann E, Wands JR. Ethanol inhibition of aspartyl-asparaginyl-beta-hydroxylase in fetal alcohol spectrum disorder: potential link to the impairments in central nervous system neuronal migration. Alcohol. 2009;43(3):225–40.
Tong M, Ziplow J, Chen WC, Nguyen QG, Kim C, de la Monte SM. Motor function deficits following chronic prenatal ethanol exposure are linked to impairments in insulin/IGF, notch and Wnt signaling in the cerebellum. J Diabetes Metab. 2013;4(1):238.
Thomas JD, Wasserman EA, West JR, Goodlett CR. Behavioral deficits induced by bingelike exposure to alcohol in neonatal rats: importance of developmental timing and number of episodes. Dev Psychobiol. 1996;29(5):433–52.
du Plessis L, Jacobson JL, Jacobson SW, Hess AT, van der Kouwe A, Avison MJ, et al. An in vivo 1H magnetic resonance spectroscopy study of the deep cerebellar nuclei in children with fetal alcohol spectrum disorders. Alcohol Clin Exp Res. 2014;38(5):1330–8.
Fan J, Meintjes EM, Molteno CD, Spottiswoode BS, Dodge NC, Alhamud AA, Stanton ME, Peterson BS, Jacobson JL, Jacobson SW. White matter integrity of the cerebellar peduncles as a mediator of effects of prenatal alcohol exposure on eyeblink conditioning. Hum Brain Mapp. 2015;36(7):2470–82.
Schmahmann JD, Sherman JC. The cerebellar cognitive affective syndrome. Brain. 1998;121(Pt 4):561–79.
Steinlin M. The cerebellum in cognitive processes: supporting studies in children. Cerebellum. 2007;6(3):237–41.
Bloedel JR, Bracha V. Duality of cerebellar motor and cognitive functions. Int Rev Neurobiol. 1997;41:613–34.
Van Overwalle F, Mariën P. Functional connectivity between the cerebrum and cerebellum in social cognition: a multi-study analysis. NeuroImage. 2016;124(Pt A):248–55.
Fatemi SH, Aldinger KA, Ashwood P, Bauman ML, Blaha CD, Blatt GJ, et al. Consensus paper: pathological role of the cerebellum in autism. Cerebellum. 2012;11(3):777–807.
Berquin PC, Giedd JN, Jacobsen LK, Hamburger SD, Krain AL, Rapoport JL, Castellanos FX. Cerebellum in attention-deficit hyperactivity disorder: a morphometric MRI study. Neurology. 1998;50(4):1087–93.
Ornoy A, Weinstein-Fudim L, Ergaz Z. Genetic syndromes, maternal diseases and antenatal factors associated with autism spectrum disorders (ASD). Front Neurosci. 2016;10:316.
Simmons RW, Nguyen TT, Levy SS, Thomas JD, Mattson SN, Riley EP. Children with heavy prenatal alcohol exposure exhibit deficits when regulating isometric force. Alcohol Clin Exp Res. 2012;36(2):302–9.
Simmons RW, Thomas JD, Levy SS, Riley EP. Motor response programming and movement time in children with heavy prenatal alcohol exposure. Alcohol. 2010;44(4):371–8.
Chudley AE. Genetic factors in fetal alcohol spectrum disorder. In: Riley E, Clarren S, Weinberg J, Jonsson E, editors. Fetal alcohol syndrome disorder. Management and policy perspectives of FASD. New York: Wiley/Blackwell; 2011. p. 109–26.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2017 Springer International Publishing AG
About this chapter
Cite this chapter
Chudley, A.E. (2017). Teratogenic Influences on Cerebellar Development. In: Marzban, H. (eds) Development of the Cerebellum from Molecular Aspects to Diseases. Contemporary Clinical Neuroscience. Springer, Cham. https://doi.org/10.1007/978-3-319-59749-2_14
Download citation
DOI: https://doi.org/10.1007/978-3-319-59749-2_14
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-319-59748-5
Online ISBN: 978-3-319-59749-2
eBook Packages: Biomedical and Life SciencesBiomedical and Life Sciences (R0)