
Abstract
Uterine leiomyomas (fibroids) can lead to a variety of different symptoms, depending on their location, size and number. Submucous fibroids can cause abnormal uterine bleeding (AUB), heavy menstrual bleeding, recurrent pregnancy loss (RPL) and subfertility. Various treatment options include medical or surgical treatments such as hysteroscopic myomectomy, excision by laparoscopy or laparotomy. Additionally, interventional radiological techniques like uterine artery embolization (UAE) or magnetic resonance (MR)-guided focused ultrasound (MR-FU) ablation can be utilized. The wide range of possible treatments warrants an appropriate assessment of patients in choosing suitable intervention. A thorough patient history and examination with ultrasound and/or other imaging is fundamental in the assessment of patients. Hysteroscopic myomectomy has been demonstrated to reduce AUB, increase pregnancy rates and can reduce first and second trimester abortion rates. It is the preferred treatment of choice for many submucous myomas due to its minimally invasive approach and efficacy. To fully restore intracavitary anatomy, the knowledge of hysteroscopic resection techniques as a main surgical treatment option is pivotal. This chapter will present symptoms and disease patterns of submucous myomas, imaging methods, classification of myomas, surgical outcomes of hysteroscopic myomectomy and will highlight possible complications of hysteroscopic surgery for myomas.
Access provided by CONRICYT-eBooks. Download chapter PDF
Similar content being viewed by others

Keywords
1 Preoperative Imaging and Patient Selection
Advances in imaging techniques such as transvaginal sonography (TVS) and MRI have increased the diagnostic accuracy and detection rates of uterine fibroids. In many patients, a combination of submucosal myomas and intramural myomas can be found. Imaging plays an important role in localizing and classifying uterine fibroids in determining correct treatment. The knowledge of fibroid characteristics prior to any type of surgery is essential to patient and treatment selection. Optimized and individual treatment decisions can only be made with detailed knowledge of the patient’s history, symptoms and depend on fertility issues and presence of other pathologies [1]. Hysteroscopic myomectomy is a minimally invasive procedure, which is the treatment of choice for mid-sized submucosal fibroids. The detection of submucosal myomas is usually accomplished by TVS. Hysteroscopy or magnetic resonance imaging (MRI) can also aid diagnosis. However, in comparing different imaging modalities, it is important to note that TVS, hysterosonography and hysteroscopy are equally dependent on the skill of the clinician in contrast to MRI [2]. Nevertheless, due to its availability, cost efficacy and high accuracy for the detection of endometrial polyps and submucous uterine leiomyomas, recent evidence suggests that TVS-based saline contrast sonohysterography is a potential first-line diagnostic tool in the preoperative evaluation of premenopausal patients AUB [3]. Hysterosalpingography (HSG) and computed tomography (CT) have a limited role in locating fibroids [4].
1.1 Transvaginal Sonography (TVS)
Transvaginal ultrasound (TVS) is an easy and highly available method to define pathologies of the uterus. Evaluation of the uterus and cervix for fibroids of any location or other pathologies like adenomyosis and endometrial polyps that may cause similar symptoms is obligatory prior to any kind of intervention. In uteri less than 10 gestational weeks’ size TVS shows a high accuracy for detection of fibroids in various locations [5]. Comparable to MRI, TVS is effective in diagnosing the presence of myomas; however, TVS has limitations in larger uteri (>375 ml) and those with multiple fibroids (>4) [5, 6]. Efforts should be made to reduce inter-observer discrepancies and thus increase the efficacy of TVS [7]. A double-blinded study of women undergoing hysterectomy for benign disease found MRI and TVS comparable in detecting the presence of fibroids [5]. MRI had a sensitivity of 0.99 and specificity of 0.86 and TVS had a sensitivity of 0.99 and specificity of 0.91. However, MRI was superior to TVS with other features like assessing location, in cases of increasing number of fibroids and in assessing proportion of myomas into the endometrial cavity.
1.2 Saline Infusion Sonography
Saline infusion sonography (SIS) also referred to as sonohysterography is a simple method that allows sonographic visualization of the uterine cavity and its changes caused by benign and malignant lesions of mucosal and myometrial origin. The examination is carried out inserting saline into the uterine cavity to enhance the contrast of intrauterine pathologies and surrounding tissues and fluids. If the percentage of an intracavitary leiomyoma is not clearly ascertained, saline infusion sonography may be used to evaluate the uterine cavity. It is a useful tool before planning hysteroscopic excision of myomas or to assess infertility issues with presenting fibroids.
A systematic review of 2-D transvaginal scan with SIS concluded that it has a high diagnostic accuracy in assessing uterine cavity abnormalities in patients with subfertility issues [8]. In diagnosing all intrauterine abnormalities, i.e. uterine polyps, submucous myomas, uterine anomalies and intrauterine adhesions, SIS had a pooled sensitivity of 0.88 and pooled specificity of 0.94. SIS as a method of detecting submucous myomas showed a sensitivity and specificity of 0.82 and 0.99, respectively. Another review [9] supports that SIS is highly accurate in uterine cavity diagnosis in a different patient population with pre- and postmenopausal women complaining of AUB with pooled sensitivity of 0.95 and specificity 0.88. A recent meta-analysis supports these data by demonstrating pooled sensitivity and specificity of 94 and 81% for detection of submucosal uterine leiomyomas by SIS [3]. SIS has a low cost compared to hysteroscopy with a short learning curve [8] and is well tolerated [10].
1.3 Hysteroscopy
Diagnostic hysteroscopy gives a clear visualization of endometrial macroscopic anatomy. It is an excellent tool for diagnosing submucous myomas and can map the extent of protrusion of submucous or intramural myomas into the uterine cavity. However, hysteroscopy is not as good as TVS and sonohysterography in assessing the size of myomas [6]. Hysteroscopy has the advantage of being possible to perform as an outpatient procedure [11, 12]. Despite the heterogeneity of the studies in a systematic review comparing TVS, sonohysterography and hysteroscopy in premenopausal women with AUB found SIS and hysteroscopy superior to TVS in diagnosing submucous myomas [13].
1.4 Magnetic Resonance Imaging
Magnetic resonance imaging (MRI) is a valuable diagnostic tool for visualizing size, number and location of all uterine myomas and can distinguish among leiomyomas and adenomyosis [2, 14]. MRI, hysterosonography and hysteroscopy were found to be as effective and somewhat superior to TVS in evaluation of the uterine cavity in a double-blinded study of women undergoing hysterectomy for benign disease [15]. In a study of 51 premenopausal women undergoing hysterectomy for benign disease, MRI carried less inter-observer variation in evaluation of abnormalities in the uterine cavity, submucous myomas, number of myomas and adenomyosis than for TVS, hysterosonography and hysteroscopy [2]. However, one must consider that MRI is costly and is not as readily available as the other imaging techniques. MRI should be considered in complicated cases with large uteri, multiple myomas or to distinguish myomas from other solid pelvic masses [16]. In a research setting, MRI may be superior to TVS in terms of better sensitivity and less measurement errors [17].
2 Symptoms and Disease Pattern Associated with Uterine Fibroids
Symptoms caused by fibroids are related to number, size and location of the myometrial tumour. In many women, fibromas may be asymptomatic and are diagnosed incidentally on clinical examination or imaging. However, they can cause significant morbidity including menstrual abnormalities like heavy, irregular and prolonged uterine bleeding, iron deficiency anaemia, abdominal pain symptoms with increasing fibroid size and fertility issues [18]. Especially submucous fibroids often cause one or a combination of symptoms [19]. An internet survey of more than 21,000 women in eight countries found that women diagnosed with fibroids reported more bleeding symptoms and pain symptoms than those without a diagnosis of uterine fibroids [20]. Uterine fibroids appeared to have a significant negative impact on these women’s lives in the past 12 months affecting their sexual life (43%), performance at work (28%), and relationship, and family (27%). It is still discussed to what extent acquired uterine cavity anomalies influence fertility and endometrial receptivity, and embryo implantation processes [21].
2.1 Abnormal Uterine Bleeding
Abnormal uterine bleeding (AUB) in non-pregnant, premenopausal women is a very common gynaecological symptom. AUB has been defined as an abnormality in the frequency, cycle regularity, duration and volume of menstrual blood loss in the reproductive years that has been present for over six months [22, 23]. The mechanism that makes submucous leiomyomas a common cause of AUB and heavy menstrual bleeding is not fully understood. The widespread use of different terminologies to describe AUB symptoms has led to difficulties in clinical and research communication and documentation. The International Federation of Gynecology and Obstetrics (FIGO) has developed definitions and terminology for AUB symptoms and classification of AUB aetiologies in the reproductive years. Design and interpretation of basic and clinical research and attempts to conduct multicentre or multinational clinical trials are difficult due to the use of different classification systems [22, 24, 25]. This led to the formation of the Menstrual Disorders Working Group in 2005 within FIGO. Since 2012, this working group has become a standing committee of FIGO, the FIGO Menstrual Disorders Committee (MDC). The group has developed internationally supported recommendations on definitions and terminology for AUB symptoms [22,23,24,25,26] as well as a new classification of underlying causes of AUB in the reproductive years [23]. This terminology and classification systems provide the tools to increase precision in communicating aetiologies, symptoms, diagnosis and treatment of AUB. Where possible, definitions were based on data derived from population-based studies. Results and recommendations have been published as the PALM-COEIN classification of AUB aetiologies [23].
2.2 Recurrent Pregnancy Loss
Recurrent pregnancy loss (RPL) is defined as three or more consecutive miscarriages before 10 weeks gestation [27]. Fibroids, particularly those that impinge upon the endometrium, may affect fertility by interfering with implantation near the lesion, rapid distension of the uterine cavity in early pregnancy or impairment of uterine contractility [28, 29]. It is unknown how uterine fibroids affect pregnancy outcome in patients with RPL. However, a meta-analysis found a significantly higher spontaneous abortion rates in women with submucous myomas (RR 1.68) [30]. A systematic review on the prevalence of submucosal and cavity-distorting myomas in women with two or more abortions found three relevant studies, none of them with a control group [31]. The prevalence of fibroids affecting the cavity was 4% for women with two or more losses, while women with three or more losses had a slightly higher prevalence of these lesions (6%). Cavity-distorting fibroids have been associated with spontaneous miscarriage [32] and may also contribute to RPL since recent evidence has shown that their prevalence in the RPL population is slightly higher compared to women with subfertility of unknown cause [33].
2.3 Subfertility
The management of women with uterine leiomyomas depends upon several factors, including patient’s age and symptoms, her obstetrical history and future childbearing plans. Prophylactic therapy to avoid future complications from myomas is debated [34]. Fibroids have been associated with decreased implantation rates, especially those impairing the endometrium. In addition, abnormal distension of the uterine myometrium in early pregnancy or changes in uterine contractility have been associated as causes for decreased conception rates and increased abortion rates [28,29,30]. There is a lack of good-quality data on whether leiomyomas adversely affect pregnancy outcome. The available information consists largely of observational case series and case reports that are limited by different patient populations, different criteria regarding the size, location, and number of leiomyomas, small numbers of adverse events, ascertainment bias in selecting study participants and inadequate adjustment of confounders. Uterine myomas are found in 5–10% of women with infertility and fibroids are the only abnormal findings in 1.0–2.4% of all infertile women [35,36,37].
3 Classification Systems of Uterine Fibroids
Categorization and classification of fibroids is of major importance when considering and estimating the effect of therapeutic options including medical, interventional guided or surgical therapies for patients in a clinical setting and in research. To date, several classification systems have been described. However, there is no consensus in the use of various classifications. Currently, there is insufficient data to suggest which system provides the best combination of acceptance for clinical and research utility.
3.1 Three-Stage Classification System
The classification consists of three parts and is associated with the FIGO classification of uterine fibroids [23]. The primary classification system only describes the presence or absence of one or more myomas, regardless of number, location or size (Fig. 37.1).

The three-stage classification system for leiomyomas
The secondary classification system reflects on distortion of the uterine cavity. Based on their relationship to the uterine cavity, fibroids are related to submucous or other i.e. intramural or subserosal origin (Fig. 37.2). The tertiary classification system describes several types of fibroids according to their relationship to the endometrium, myometrium and serosa. They are referred to as submucous, intramural or subserosal. Also, it describes those of the cervix and detached from the uterus like intraligamentary-situated myomas.

Illustration of the secondary part of the three-stage classification system describing the relationship to the uterus
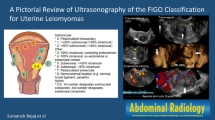
3.2 FIGO Leiomyoma Classification System
The FIGO system for classification of leiomyomas is in accordance with European Society of Gynaecological Endoscopy (ESGE) system for categorization of submucous myomas but adds a number of other categories including intramural and subserous lesions [23] (Fig. 37.3). In addition to the ESGE classification, this system describes the relationship of the fibroid to the uterine serosa. Type 2–5 lesions are not candidates for operative hysteroscopy as they impact both endometrium and serosa, so called hybrid leiomyomas. FIGO type 3, 4 and 5 are intramural lesions located within the uterine wall. They may enlarge the uterus and distort the uterine cavity or serosal surface. FIGO type 6 and 7 myomas originate from the myometrium involving the serosal surface of the uterus. They can occur with broad or pedunculated base and may be situated intraligamentarily thereby extending between the folds of the broad ligament. Type 8 lesions are myomas that do not have any relation to the myometrium e.g. cervical lesions, lesions that exist around the round or broad ligament without direct attachment to the uterus and other “parasitic” lesions.

FIGO leiomyoma sub-classification system
3.3 PALM-COEIN Classification
The PALM-COEIN classification is a classification of AUB aetiologies in non-gravid women of reproductive age [23]. Standard practice includes obtaining a structured patient history and appropriately using the diagnostic tools necessary in identifying potential causes and contributors to AUB. The classification system is divided into nine basic categories that are arranged in the acronym PALM-COEIN: Polyp, Adenomyosis, Leiomyoma, Malignancy and Hyperplasia—Coagulopathy, Ovulatory Dysfunction, Endometrial dysfunction, Iatrogenic, and “Not otherwise classified” (Fig. 37.4).

PALM-COEIN classification system for AUB in non-gravid women of reproductive age
The PALM entities are either measurable visually using imaging techniques and/or diagnosed via histology. The COEIN group is related to entities that are not defined by imaging or histopathology. These entities can be organized in the form of a table to facilitate documentation of clinical evaluation and results. The categories are designed to facilitate the development of sub-classification systems. The system was constructed since any patient could have one or more entities that cause or contribute to AUB and that these structural entities could be asymptomatic and thus not be the cause of AUB (Fig. 37.5).

PALM-COEIN classification is divided in to structural and non-structural causes of AUB
4 ESGE Classification
A classification system for describing the extent of myometrial involvement of submucosal myomas visualized by hysteroscopy was initially described by Wamsteker and colleagues [38]. It has been adopted by ESGE (European Society of Gynaecological Endoscopy) and is associated with the FIGO system (Figs. 37.3 and 37.6). According to the degree of myometrial penetration, submucosal myomas are referred to as Type 0, I and II. Type 0 lesions lie within the endometrial cavity, are easier to remove, and require less operative time and less fluid deficit and blood loss than the other types [39]. Type I lesions extend less than 50% into the myometrium. Type II lesions extend 50% or more within the myometrium, which is associated with higher risk of excessive intraoperative fluid absorption and risk of bleeding, increased operative time and likelihood of additional procedures due to incomplete resection [38, 39].

ESGE classification of submucous leiomyomas
4.1 LASMAR Classification System/STEP-W System
The LASMAR, also called the STEP-W (size, topography, extension, penetration, and wall) system, is a pre-surgical classification [40] to evaluate the viability of hysteroscopic surgical treatment of submucous myomas (Fig. 37.7). In addition, the system aims to estimate degree of difficulty of hysteroscopic myomectomy and suggest appropriate treatment. It helps the surgeon in identifying which patients will have a complete myomectomy and which patients will have more complex surgery. The ESGE classification only evaluates degree of penetration of the myoma into the myometrium, not giving a complete guidance on degree of difficulty of hysteroscopic myomectomy. The system gives a score, maximum of 9, for the following parameters as in the abbreviation:

The LASMAR/STEP-W scoring system for submucous myomas
4.2 STEP-W
-
Size is the largest diameter of the nodule in centimetres.
-
Topography at the uterine cavity, which part of the uterine cavity the myoma is situated.
-
Extension of base of the fibroid to the wall of the myoma in relation to the uterine wall i.e. if the myoma covers the uterine wall by <1/3, between <1/3 and 2/3 or >2/3.
-
Degree of P enetration of the fibroid into the myometrium, which uses the same classification as ESGE, see above under 5.
-
Wall, if the myoma is attached to the lateral wall.
The score is used to divide myomas into group I, II and III estimating the likelihood of successful removal. A patient can have more than one submucous myoma, each myoma is scored individually and the submucous myoma with the highest score guides the recommended treatment. Score 0–4, also referred to as group I, suggests a low complexity of hysteroscopic myomectomy. Score 5–6, referred to as group II, suggests a complex hysteroscopic myomectomy, and the authors recommend considering preparation with GnRH analogue and/or two-stage surgery. Score 7–9, group III, suggests non-hysteroscopic treatment of fibroids [40, 41]. Lasmar and colleagues compared their new classification system to ESGE in 55 patients with 57 myomas in a prospective study [40]. They found that their classification is more accurate in predicting complete procedures.
The suggested system uses hysteroscopy to define parameters [40]. A prospective study of 34 women with submucous fibroids scheduled for hysteroscopic surgery investigated if 2-D and 3-D ultrasound alone could obtain the same STEP-W score as the original hysteroscopic technique described by Lasmar in 2005 [42]. Inter-observer concordance between the methods was high (Cohen’s ƙ = 0.77). However, patient numbers were limited and patients only had a maximum of two submucous fibroids.
The PALM-COEIN classification looks directly at the aetiology behind AUB divided into structural causes, i.e. that can be evaluated, diagnosed by imaging and/or taken a biopsy from, and non-structural causes, i.e. underlying medical conditions. This can be a useful clinical tool in the evaluation of patients, providing structure in clinical training/research allowing a clear illustration that patients can have more than one condition contributing to AUB. It was created to support further development of sub-classification systems. However, it differs from the other classifications as it does not describe myomas further to aid the clinician for hysteroscopic management. The FIGO classification provides a standardized nomenclature for all types of myomas, not only submucosal myomas as the ESGE and STEP-W classifications, but their location and changes in uterine anatomy. However, size and number of leiomyomas are not described in the FIGO classification system. It offers simplified and unified terminology to the benefit of clinical research and collaboration. Both ESGE and STEP-W classifications were both developed to guide the clinician in assessing the level of difficulty of hysteroscopic resection of submucous myomas. The STEP-W classification considers more parameters than ESGE, not only extent of myometrial involvement of the lesion but also size of the largest myoma, location of the lesion in the uterine cavity, extent of the myoma base on the uterine wall and whether the lesion is on the lateral uterine wall. This provides an optimal classification tool for preoperative assessment of submucous fibroids and clear terminology to be used in research. The disadvantage of the STEP-W classification is that the score is primarily given at hysteroscopy, thereby excluding non-invasive imaging techniques such as TVS. However, 2-D and 3-D ultrasound scoring may be more feasible and require less resources and discomfort for the patient [42]. Although there are many classifications for leiomyomas, they all have a different value in daily practice and in a research/education setting. However, simplifying and unifying terminology can improve evaluation, (preoperative) management, teaching and research to the benefit of patients.
5 Surgical Outcome of Hysteroscopic Myomectomy
Outcomes after hysteroscopic surgery have been difficult to compare due to the lack of consistency across studies regarding classification systems, type of myoma treated, menopausal status, objective measurement of fluid and blood loss, complication rates and duration of follow-up. In addition, data on rates of subsequent reoperation or fertility outcome are sparse [43]. A retrospective study of 235 patients with AUB or infertility problems who underwent hysteroscopic resection for myomas found the intraoperative complication rate to be limited (2.6%). Long-term follow-up of patients (range 18–66 months) showed favourable outcome and patient satisfaction in 94.4% [44]. Two large national studies found an incidence of adverse events associated with hysteroscopy to be below 1% [45, 46]. Crucial issues in hysteroscopic myomectomy are size and type of fibroid, risk of incomplete excision, surgical experience and risk of possible complications. Complete resection of fibroids depends on the extent of myometrial penetration. The rate of incomplete resection ranges from 5 to 17% in retrospective case series [44, 47].
A recent Cochrane review of women with otherwise unexplained subfertility and submucous fibroids found no gain with hysteroscopic myomectomy compared to regular fertility-oriented intercourse during 12 months for clinical pregnancy (odds ratio (OR) 2.4, p = 0.06) and miscarriage (OR 1.5, p = 0.47, 94 women); however, the evidence was of low quality [48]. Due to the lack of good evidence, one should be extra vigilant in the management of patients with RPLs in the recommendation of treatment options for fibroids.
5.1 Surgical Outcome: Complications of Hysteroscopic Surgery
Hysteroscopic resection of large fibroids may confer perioperative complications and might require more than one procedure for complete resection and symptom relief. A prospective observational study of 122 women investigated patient characteristics affecting outcome of hysteroscopic myomectomy [49]. The relative risk (RR) for fibroid-related surgery within four years of follow-up was significantly lower in women with fibroids that measured <3 cm in diameter with RR 0.21 compared to fibroids >3 cm in diameter and mainly intracavitary lesions (type 0 and I) with RR 0.26 compared to intramural lesions (type II). Increasing size and extension of fibroid requires a high level surgical skill [38, 47]. Typical complications of hysteroscopic resection include perforation, incomplete resection, fluid loss, bleeding and intrauterine adhesions.
A retrospective study found that intraoperative complications, defined as uterine perforation, excessive glycine absorption (1 l or more), hyponatremia, haemorrhage (500 ml or more), bowel and bladder injury, ability to dilate the cervix and procedure-related hospital admissions, occurred in 25 of 925 interventions (2.7%) [50]. Excessive fluid absorption was the most common complication (0.76%), followed by uterine perforation (0.43%). The authors found that type of hysteroscopic procedure performed is related to risk of complications. Hysteroscopic myomectomy was the procedure associated with the highest odds of complications (OR 7.4), followed by resection of uterine septum (OR 4.0) compared to polypectomy (OR 0.1) and endometrial ablation (OR 0.4). Similarly, Jansen and colleagues found operative-resectoscopic procedures such as intrauterine adhesiolysis to be associated with a higher incidence of complications (4.48%) compared to endometrial resection (0.81%), myomectomy 0.75% and polyp removal 0.38% (p < 0.001) [46].
First described during urological resection procedures (TUR), extensive loss of fluids during hysteroscopy does account for severe imbalances of electrolytes [51]. The OHIA syndrome (operative hysteroscopy intravascular absorption syndrome) may occur due to excessive fluid overload, similar to TUR syndrome [52, 53]. Hypotonic solutions such as glycine are used in combination with monopolar resection loops, whereas bipolar loops are used in combination with isotonic fluids. Excessive fluid absorption occurring in cases of extensive endometrial or myometrial resection potentially results in hyponatremia and volume overload [44]. The pressure in myometrial venous vessels is 10–15 mmHg, while the intrauterine pressure for distention is kept above 40–60 mmHg in order to facilitate visualization of intracavitary architecture. As a consequence, rapid intravasation, hyponatremia, metabolic acidosis, pulmonary and cerebral oedema may develop [53]. A common reason for termination of a technically difficult procedure is excessive absorption of distension fluid [38, 54]. The volume of fluid absorbed during the procedure has been shown to significantly correlate with the degree of myometrial penetration of the fibroid. Critical volumes for type 0 fibroma as described by the ESGE classification were 450 ml, for type I and type II fibroids 957 ml and 1682 ml, respectively [39]. In fact, absorption of small amounts (1–2 l) occurs in 5–10% of patients with a mild OHIA syndrome, while the classic syndrome develops in <1% with intravascular absorption in excess of 2 l. Intravasation of over 2 l (1.5% glycine) may cause severe OHIA and has been associated with a mortality of 25% [53]. Hence, continuous fluid monitoring and awareness of a threshold of fluid loss of about 1.5–2 l are pivotal in hysteroscopic surgery. Due to the inconsistent results on OHIA published so far, a recent guideline (BSGE/ESGE) on the management of fluid distension media in hysteroscopy refers to an upper threshold for isotonic media of 2500 ml in healthy women [55]. However, in patients with comorbidities and advanced age, lower thresholds should be applied with upper fluid deficit levels of 750 ml for hypotonic solutions and 1500 ml for isotonic solutions [55].
Several complications have been shown to be related to insufficient cervical dilatation, suggesting that cervical ripening agents may prevent this problem. Administration of misoprostol before hysteroscopy can facilitate the procedure and thus reduce the risk of procedure-related complications. One randomized controlled trial of 92 nulliparous women undergoing hysteroscopy due to suspected intrauterine abnormalities received 200mcg of misoprostol vaginally or placebo 9–10 h before the procedure [56]. Mean cervical width was significantly higher in the misoprostol vs. placebo group (7 mm vs 4 mm). Mean duration of the hysteroscopy was significantly lower in the misoprostol group vs. placebo group (90 and 142 s). The same group supported these findings with a randomized controlled trial of 152 women but also found that cervical tears occurred more often in the placebo vs. the misoprostol group (11.4% vs. 1.4%) [57].
The relationship of submucous myomas to the uterine serosa is another important factor, since hysteroscopic resection is not considered appropriate in cases of contact with the serosa which has been strongly associated with an increased risk of perforation and serious injury. If perforation occurs with an activated electrode, bowel injury has to be assumed until proven otherwise [50]. Laparoscopic exploration should be considered in these cases [54].
However, incomplete resection does not necessarily lead to reoperation. In a series of 41 women with incomplete hysteroscopic resection of fibroids, only 44 percent underwent further fibroid-related and symptom-associated surgery within three years [47]. In another series, at three-month follow-up, saline infusion sonohysterography revealed that incompletely resected fibroids had regressed in 21 of 38 patients [58]. Several observational studies support the ability of the ESGE classification system to predict complete fibroid resection. Type 0 fibroids were reported to be completely resected in over 95%, type I in 86–90%, and type II in 61–83% [47].
Finally, formation of intrauterine adhesions can interfere with fertility or menstruation. Studies in which second-look hysteroscopy was performed after the initial hysteroscopic myomectomy report, found that the rates of adhesions varied widely, from 0 to 46% [59]. The rate appears to be higher if more than one fibroid is resected with adhesion rates of 31% for single versus 46% for multiple fibroids [44, 59].
5.2 Surgical Outcome: Reduction of AUB
Among symptomatic women with uterine fibroids, AUB is a common symptom. The prevalence of submucous myomas in women with AUB was identified in a systematic review of 11 studies and reached 23.4% [60]. Furthermore, submucous myomas can be found in 23.4% of premenopausal women and 4.5% of postmenopausal women with AUB [1, 60]. It is difficult to evaluate how far submucous fibroids do cause AUB. The mechanisms that contribute to AUB are unclear and may involve dysregulation of endometrial haemostasis and/or mechanical irritation of the endometrium by fibroids extending into the junctional zone (JZ). However, to our knowledge, no studies have clearly evaluated these pathomechanisms to date. The correlation between local irritation by myomas and AUB may be answered by the effect of hysteroscopic surgery in women with those lesions and AUB. The long-term results of trans-cervical hysteroscopic myomectomy (TCRM) for AUB where the procedure was carried out without other interventions such as endometrial ablation demonstrate success rates of 60–90% defined as time periods not requiring further interventions post resection [1]. Patient satisfaction and reduction of AUB rates warrant appropriate selection of patients and accurate pre-surgical diagnostic workup including knowledge of size, type and number of submucous fibroids. An observational study with a period of three years found that TCRM of type 2 myomas could eventually be performed but required a larger number of repeat procedures than the more superficial types 0 and 1 myomas, which almost always were completed with a single operation [38]. Analysing factors that might help to predict the need for further surgery, the authors identified two subgroups of patients: women with a normal-sized uterus and not more than two submucous fibroids identified at hysteroscopy were found to have a risk of undergoing additional procedures within 3 years of only 9.7%. In contrast, the presence of an enlarged uterus and three or more submucous myomas lead to further surgery in 35% [38]. Aiming to limit the number of hysteroscopic interventions for AUB, TCRM may be combined with additional procedures such as endometrial ablation (EA). A retrospective study comparing the outcomes of women undergoing TCRM alone with those undergoing a combination therapy of resection and EA showed a significantly higher success rate when ablation was added. In cases of complete resection of fibroids, bleeding could be controlled in 96.7% of those women with combined EA compared to 84.4% undergoing TCRM only [61]. In cases of incomplete resection, 92.3% of women achieved control after concurrent ablation in contrast to 70.4% if ablation was not performed additionally. Although no RCTs have been performed to compare these techniques, a combination of TCRM and EA should be considered in patients with submucous fibroids and AUB. As stated above, subsequent surgical interventions following TCRM have been associated with increasing uterine size and number of myomas. In addition, it should be noted that concomitant pathologies such as adenomyosis appear to decrease success rates of TCRM in patients with AUB [61]. Preoperative measures to increase success rates of TCRM include the administration of GnRH analogues or ulipristal acetate (UPA) due to their potential to induce amenorrhea and improve anaemia. Both may reduce electrolyte imbalances and thereby complications such as OHIA [55]. Both agents appear to be equally efficient as demonstrated by a retrospective cohort study of patients receiving GnRH or UPA for 3 months prior to TCRM [62]. Whether these agents should be used routinely prior to TRCM is debated since data have shown benefits regarding reduced fluid loss and induction of amenorrhea but have also demonstrated conflicting results regarding operation time and improvement in rates of complete excision [19].
5.3 Surgical Outcome: Fertility and Recurrent Pregnancy Loss (RPL)
Fibroids of all types have been observed in 10% of women with subfertility. In up to 2.4% of women with subfertility, fibroids are the only detectable pathology [19]. How far fibroids and especially submucous lesions do affect fertility and pregnancy outcome has been discussed in previous chapters. Current evidence suggests a significant reduction of implantation and ongoing pregnancy rates in women with fibroids changing the intracavitary architecture [30].
Based on these assumptions, TCRM is a highly valuable tool for removal of submucous myomas to increase live births and decrease abortion rates. A systematic review by Pritts and colleagues [30] clearly supports excision of submucosal myomas with an increase in post-surgical pregnancy rates compared to non-treated patients. The degree of cavitary distortion and its correction appears to influence outcome. Fertility rates at a mean of 41 months following TCRM have been reported to be 49%, 36%, and 33% in type 0, 1 and 2 myomas, respectively [63]. An RCT of 215 women with submucosal fibroids and infertility randomly assigned to surgery (TCRM) or diagnostic hysteroscopy only conceived spontaneously in 63% post intervention versus 28% in the diagnostic group [64]. Similarly, Casini and colleagues [65] investigated the effect of myomectomy of submucosal and intramural fibroids in subfertility patients observing spontaneous pregnancy rates of 43% following TCRM versus 27% in the non-treatment group. To date, no studies have evaluated the effect of TCRM in patients undergoing ART/IVF (artificial reproductive techniques, in vitro fertilization).
However, TCRM should also be indicated in the light of possible complications negatively affecting fertility since the impact of extensive resection of endometrium covering submucosal fibroids on fertility remains unclear. At present, high-quality evidence from systematic reviews [48, 66] suggests a favourable effect of TCRM in subfertility patients in experienced hands and following a detailed pre-surgical workup.
References
Emanuel MH, Wamsteker K, Hart AA, Metz G, Lammes FB. Long-term results of hysteroscopic myomectomy for abnormal uterine bleeding. Obstet Gynecol. 1999;93(5 Pt 1):743–8.
Dueholm M, Lundorf E, Sorensen JS, Ledertoug S, Olesen F, Laursen H. Reproducibility of evaluation of the uterus by transvaginal sonography, hysterosonographic examination, hysteroscopy and magnetic resonance imaging. Hum Reprod. 2002;17(1):195–200.
Bittencourt CA, Simoes RD, Bernardo WM, Fuchs LF, Soares Junior JM, Pastore AR, et al. Accuracy of saline contrast sonohysterography in detection of endometrial polyps and submucosal leiomyoma in women at reproductive age with abnormal uterine bleeding: a systematic review and meta-analysis. Ultrasound Obstet Gynecol. 2016;PubMed:27862503.
Bradley LD, Falcone T, Magen AB. Radiographic imaging techniques for the diagnosis of abnormal uterine bleeding. Obstet Gynecol Clin N Am. 2000;27(2):245–76.
Dueholm M, Lundorf E, Hansen ES, Ledertoug S, Olesen F. Accuracy of magnetic resonance imaging and transvaginal ultrasonography in the diagnosis, mapping, and measurement of uterine myomas. Am J Obstet Gynecol. 2002;186(3):409–15.
Cicinelli E, Romano F, Anastasio PS, Blasi N, Parisi C, Galantino P. Transabdominal sonohysterography, transvaginal sonography, and hysteroscopy in the evaluation of submucous myomas. Obstet Gynecol. 1995;85(1):42–7.
Valentin L. High-quality gynecological ultrasound can be highly beneficial, but poor-quality gynecological ultrasound can do harm. Ultrasound Obstet Gynecol. 1999;13(1):1–7.
Seshadri S, El-Toukhy T, Douiri A, Jayaprakasan K, Khalaf Y. Diagnostic accuracy of saline infusion sonography in the evaluation of uterine cavity abnormalities prior to assisted reproductive techniques: a systematic review and meta-analyses. Hum Reprod Update. 2015;21(2):262–74.
de Kroon CD, de Bock GH, Dieben SW, Jansen FW. Saline contrast hysterosonography in abnormal uterine bleeding: a systematic review and meta-analysis. BJOG. 2003;110(10):938–47.
van Dongen H, de Kroon CD, van den Tillaart SA, Louwe LA, Trimbos-Kemper GC, Jansen FW. A randomised comparison of vaginoscopic office hysteroscopy and saline infusion sonography: a patient compliance study. BJOG. 2008;115(10):1232–7.
Di Spiezio Sardo A, Bettocchi S, Spinelli M, Guida M, Nappi L, Angioni S, et al. Review of new office-based hysteroscopic procedures 2003-2009. J Minim Invasive Gynecol. 2010;17(4):436–48.
Royal College of Obstetricians and Gynaecologists. Hysteroscopy, Best Practice in Outpatient (Green top Guideline No. 59). 2011. https://www.rcog.org.uk/en/guidelines-research-services/guidelines/gtg59. Accessed 18 Jan 17.
Farquhar C, Ekeroma A, Furness S, Arroll B. A systematic review of transvaginal ultrasonography, sonohysterography and hysteroscopy for the investigation of abnormal uterine bleeding in premenopausal women. Acta Obstet Gynecol Scand. 2003;82(6):493–504.
Dueholm M, Lundorf E, Hansen ES, Sorensen JS, Ledertoug S, Olesen F. Magnetic resonance imaging and transvaginal ultrasonography for the diagnosis of adenomyosis. Fertil Steril. 2001;76(3):588–94.
Dueholm M, Lundorf E, Hansen ES, Ledertoug S, Olesen F. Evaluation of the uterine cavity with magnetic resonance imaging, transvaginal sonography, hysterosonographic examination, and diagnostic hysteroscopy. Fertil Steril. 2001;76(2):350–7.
Weinreb JC, Barkoff ND, Megibow A, Demopoulos R. The value of MR imaging in distinguishing leiomyomas from other solid pelvic masses when sonography is indeterminate. AJR Am J Roentgenol. 1990;154(2):295–9.
Levens ED, Wesley R, Premkumar A, Blocker W, Nieman LK. Magnetic resonance imaging and transvaginal ultrasound for determining fibroid burden: implications for research and clinical care. Am J Obstet Gynecol. 2009;200(5):537 e1–7.
Khan AT, Shehmar M, Gupta JK. Uterine fibroids: current perspectives. Int J Women Health. 2014;6:95–114.
American Association of Gynecologic Laparoscopists: Advancing Minimally Invasive Gynecology W. AAGL practice report: practice guidelines for the diagnosis and management of submucous leiomyomas. J Minim Invasive Gynecol. 2012;19(2):152–71.
Zimmermann A, Bernuit D, Gerlinger C, Schaefers M, Geppert K. Prevalence, symptoms and management of uterine fibroids: an international internet-based survey of 21,746 women. BMC Womens Health. 2012;12:6.
Singh M, Chaudhry P, Asselin E. Bridging endometrial receptivity and implantation: network of hormones, cytokines, and growth factors. J Endocrinol. 2011;210(1):5–14.
Fraser IS, Critchley HO, Munro MG, Broder M. Can we achieve international agreement on terminologies and definitions used to describe abnormalities of menstrual bleeding? Hum Reprod. 2007;22(3):635–43.
Munro MG, Critchley HO, Broder MS, Fraser IS, Disorders FWGM. FIGO classification system (PALM-COEIN) for causes of abnormal uterine bleeding in nongravid women of reproductive age. Int J Gynaecol Obstet. 2011;113(1):3–13.
Fraser IS, Critchley HO, Munro MG, Broder M, Writing Group for this Menstrual Agreement P. A process designed to lead to international agreement on terminologies and definitions used to describe abnormalities of menstrual bleeding. Fertil Steril. 2007;87(3):466–76.
Woolcock JG, Critchley HO, Munro MG, Broder MS, Fraser IS. Review of the confusion in current and historical terminology and definitions for disturbances of menstrual bleeding. Fertil Steril. 2008;90(6):2269–80.
Jensen JT, Parke S, Mellinger U, Machlitt A, Fraser IS. Effective treatment of heavy menstrual bleeding with estradiol valerate and dienogest: a randomized controlled trial. Obstet Gynecol. 2011;117(4):777–87.
Stephenson M, Kutteh W. Evaluation and management of recurrent early pregnancy loss. Clin Obstet Gynecol. 2007;50(1):132–45.
Klatsky PC, Tran ND, Caughey AB, Fujimoto VY. Fibroids and reproductive outcomes: a systematic literature review from conception to delivery. Am J Obstet Gynecol. 2008;198(4):357–66.
Orisaka M, Kurokawa T, Shukunami K, Orisaka S, Fukuda MT, Shinagawa A, et al. A comparison of uterine peristalsis in women with normal uteri and uterine leiomyoma by cine magnetic resonance imaging. Eur J Obstet Gynecol Reprod Biol. 2007;135(1):111–5.
Pritts EA, Parker WH, Olive DL. Fibroids and infertility: an updated systematic review of the evidence. Fertil Steril. 2009;91(4):1215–23.
Russo M, Suen M, Bedaiwy M, Chen I. Prevalence of uterine myomas among women with 2 or more recurrent pregnancy losses: a systematic review. J Minim Invasive Gynecol. 2016;23(5):702–6.
Sheiner E, Bashiri A, Levy A, Hershkovitz R, Katz M, Mazor M. Obstetric characteristics and perinatal outcome of pregnancies with uterine leiomyomas. J Reprod Med. 2004;49(3):182–6.
Saravelos SH, Yan J, Rehmani H, Li TC. The prevalence and impact of fibroids and their treatment on the outcome of pregnancy in women with recurrent miscarriage. Hum Reprod. 2011;26(12):3274–9.
Parker WH. Uterine myomas: management. Fertil Steril. 2007;88(2):255–71.
Buttram VC Jr, Reiter RC. Uterine leiomyomata: etiology, symptomatology, and management. Fertil Steril. 1981;36(4):433–45.
Verkauf BS. Myomectomy for fertility enhancement and preservation. Fertil Steril. 1992;58(1):1–15.
Donnez J, Jadoul P. What are the implications of myomas on fertility? A need for a debate? Hum Reprod. 2002;17(6):1424–30.
Wamsteker K, Emanuel MH, de Kruif JH. Transcervical hysteroscopic resection of submucous fibroids for abnormal uterine bleeding: results regarding the degree of intramural extension. Obstet Gynecol. 1993;82(5):736–40.
Emanuel MH, Hart A, Wamsteker K, Lammes F. An analysis of fluid loss during transcervical resection of submucous myomas. Fertil Steril. 1997;68(5):881–6.
Lasmar RB, Barrozo PR, Dias R, Oliveira MA. Submucous myomas: a new presurgical classification to evaluate the viability of hysteroscopic surgical treatment--preliminary report. J Minim Invasive Gynecol. 2005;12(4):308–11.
Lasmar RB, Xinmei Z, Indman PD, Celeste RK, Di Spiezio Sardo A. Feasibility of a new system of classification of submucous myomas: a multicenter study. Fertil Steril. 2011;95(6):2073–7.
Camanni M, Bonino L, Tessarolo M, Migliaretti G, Ferrero B, Deltetto F. Is it possible to obtain a presurgical Lasmar score for hysteroscopic myomectomy by ultrasound alone? Ultrasound Obstet Gynecol. 2012;40(1):106–11.
Myers ER, Barber MD, Gustilo-Ashby T, Couchman G, Matchar DB, McCrory DC. Management of uterine leiomyomata: what do we really know? Obstet Gynecol. 2002;100(1):8–17.
Polena V, Mergui JL, Perrot N, Poncelet C, Barranger E, Uzan S. Long-term results of hysteroscopic myomectomy in 235 patients. Eur J Obstet Gynecol Reprod Biol. 2007;130(2):232–7.
Aydeniz B, Gruber IV, Schauf B, Kurek R, Meyer A, Wallwiener D. A multicenter survey of complications associated with 21,676 operative hysteroscopies. Eur J Obstet Gynecol Reprod Biol. 2002;104(2):160–4.
Jansen FW, Vredevoogd CB, van Ulzen K, Hermans J, Trimbos JB, Trimbos-Kemper TC. Complications of hysteroscopy: a prospective, multicenter study. Obstet Gynecol. 2000;96(2):266–70.
Van Dongen H, Emanuel MH, Smeets MJ, Trimbos B, Jansen FW. Follow-up after incomplete hysteroscopic removal of uterine fibroids. Acta Obstet Gynecol Scand. 2006;85(12):1463–7.
Bosteels J, Kasius J, Weyers S, Broekmans FJ, Mol BW, D'Hooghe TM. Hysteroscopy for treating subfertility associated with suspected major uterine cavity abnormalities. Cochrane Database Syst Rev. 2013;1:CD009461.
Hart R, Molnar BG, Magos A. Long term follow up of hysteroscopic myomectomy assessed by survival analysis. Br J Obstet Gynaecol. 1999;106(7):700–5.
Propst AM, Liberman RF, Harlow BL, Ginsburg ES. Complications of hysteroscopic surgery: predicting patients at risk. Obstet Gynecol. 2000;96(4):517–20.
Hahn RG. Early detection of the TUR syndrome by marking the irrigating fluid with 1% ethanol. Acta Anaesthesiol Scand. 1989;33(2):146–51.
Hahn RG. Fluid absorption in endoscopic surgery. Br J Anaesth. 2006;96(1):8–20.
Sethi N, Chaturvedi R, Kumar K. Operative hysteroscopy intravascular absorption syndrome: A bolt from the blue. Indian J Anaesth. 2012;56(2):179–82.
Munro MG, Christianson LA. Complications of hysteroscopic and uterine resectoscopic surgery. Clin Obstet Gynecol. 2015;58(4):765–97.
Umranikar S, Clark TJ, Saridogan E, Miligkos D, Arambage K, Torbe E, et al. BSGE/ESGE guideline on management of fluid distension media in operative hysteroscopy. Gynecol Surg. 2016;13(4):289–303.
Preutthipan S, Herabutya Y. A randomized controlled trial of vaginal misoprostol for cervical priming before hysteroscopy. Obstet Gynecol. 1999;94(3):427–30.
Preutthipan S, Herabutya Y. Vaginal misoprostol for cervical priming before operative hysteroscopy: a randomized controlled trial. Obstet Gynecol. 2000;96(6):890–4.
Dueholm M, Forman A, Ingerslev J. Regression of residual tissue after incomplete resection of submucous myomas. Gynaecol Endosc. 1998;7:309–14.
Taskin O, Sadik S, Onoglu A, Gokdeniz R, Erturan E, Burak F, et al. Role of endometrial suppression on the frequency of intrauterine adhesions after resectoscopic surgery. J Am Assoc Gynecol Laparosc. 2000;7(3):351–4.
van Dongen H, de Kroon CD, Jacobi CE, Trimbos JB, Jansen FW. Diagnostic hysteroscopy in abnormal uterine bleeding: a systematic review and meta-analysis. BJOG. 2007;114(6):664–75.
Loffer FD. Improving results of hysteroscopic submucosal myomectomy for menorrhagia by concomitant endometrial ablation. J Minim Invasive Gynecol. 2005;12(3):254–60.
Sancho JM, Delgado VS, Valero MJ, Soteras MG, Amate VP, Carrascosa AA. Hysteroscopic myomectomy outcomes after 3-month treatment with either ulipristal acetate or GnRH analogues: a retrospective comparative study. Eur J Obstet Gynecol Reprod Biol. 2016;198:127–30.
Vercellini P, Zaina B, Yaylayan L, Pisacreta A, De Giorgi O, Crosignani PG. Hysteroscopic myomectomy: long-term effects on menstrual pattern and fertility. Obstet Gynecol. 1999;94(3):341–7.
Shokeir T, El-Shafei M, Yousef H, Allam AF, Sadek E. Submucous myomas and their implications in the pregnancy rates of patients with otherwise unexplained primary infertility undergoing hysteroscopic myomectomy: a randomized matched control study. Fertil Steril. 2010;94(2):724–9.
Casini ML, Rossi F, Agostini R, Unfer V. Effects of the position of fibroids on fertility. Gynecol Endocrinol. 2006;22(2):106–9.
Di Spiezio Sardo A, Mazzon I, Bramante S, Bettocchi S, Bifulco G, Guida M, et al. Hysteroscopic myomectomy: a comprehensive review of surgical techniques. Hum Reprod Update. 2008;14(2):101–19.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2018 Springer International Publishing AG
About this chapter
Cite this chapter
Kirchner, L., Aas-Eng, K., Hudelist, G. (2018). Classification of Uterine Fibroids and Correlation with Surgical Outcome. In: Tinelli, A., Alonso Pacheco, L., Haimovich, S. (eds) Hysteroscopy. Springer, Cham. https://doi.org/10.1007/978-3-319-57559-9_37
Download citation
DOI: https://doi.org/10.1007/978-3-319-57559-9_37
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-319-57558-2
Online ISBN: 978-3-319-57559-9
eBook Packages: MedicineMedicine (R0)