
Abstract
Fine-needle aspiration (FNA) biopsies with cellblock preparation have become a primary modality to achieve a definitive diagnosis of a mass-like lesion of the thyroid. This chapter delineated cytologic and histologic features of common and rare neoplastic and nonneoplastic lesions of the thyroid. The newly introduced Bethesda System for Classification of Thyroid Lesions was applied. The utilities and pitfalls of commonly used diagnostic immunohistochemical (IHC) stains such as TROP2, CK19, HBME1, galectin 3, and PAX8, and small diagnostic IHC panels were described. Multiple challenging and yet practical cases at the end of the chapter were used to reemphasize important points illustrated throughout the chapter.
Access provided by CONRICYT-eBooks. Download chapter PDF
Similar content being viewed by others



Keywords
- Thyroid
- Parathyroid
- Acute thyroiditis
- Granulomatous thyroiditis
- Subacute thyroiditis
- Nodular goiter
- Graves’ disease
- Atypical follicular cells of undetermined significance
- Follicular neoplasms
- Follicular adenoma
- Follicular carcinoma
- Hurthle cell neoplasms
- Hurthle cell adenoma
- Hurthle cell carcinoma
- Papillary carcinoma (follicular variant, tall cell variant, columnar cell variant, diffuse sclerosing variant, cribriform variant, Warthin-like variant, macrofollicular variant, oncocytic variant)
- Papillary microcarcinoma
- Poorly differentiated (insular) carcinoma
- Medullary carcinoma
- Undifferentiated (anaplastic) carcinoma
- Hyalinizing trabecular neoplasm
- Carcinoma
- Sarcoma
- Lymphoma
- Plasmacytoma
- Melanoma
- Metastasis
- CK7
- CK20
- CK19
- HBME1
- TROP2
- Galectin-3
- Chromogranin
- Synaptophysin
- MIB-1 (Ki67)
- PTH
- GATA3
- Calcitonin
- CEA
- TTF1
- PAX8
- Beta-catenin
- BRAF
-
Based on the Bethesda System for Reporting Thyroid Cytopathology, the terminology “follicular lesion” is no longer recommended in routine practice. Instead, a distinct subcategory of “Atypia of Undetermined Significance/Follicular Lesion of Undetermined Significance” (AUS/FLUS) was recommended.
-
Focal nuclear pleomorphism of the follicular cells is frequently seen in a lymphocytic/Hashimoto’s thyroiditis; one should avoid overdiagnosing this change as “Atypia of Undetermined Significance.”
-
When a fine-needle aspiration (FNA) smear is composed of a mixture of epithelioid and spindle cells singly and in loosely cohesive groups, and absence of colloid, regardless of the cellularity, a medullary carcinoma should be included in the diagnostic consideration.
-
Hyalinizing trabecular neoplasm is an uncommon lesion and shares many important cytological features with papillary carcinoma of the thyroid, including nuclear grooves and intranuclear pseudoinclusions. When the follicular cells appear to be elongated and a hyaline matrix-like material between cellular components is present, it is necessary to exclude a hyalinizing trabecular neoplasm before a definitive diagnosis of papillary carcinoma is rendered. An immunostain for mindbomb E3 ubiquitin protein ligase 1 (MIB-1 clone[Ki-67]) with distinctive membranous staining pattern is useful in confirming the diagnosis.
-
If abundant acute inflammation is present, in addition to an acute inflammatory process, undifferentiated (anaplastic) carcinoma of the thyroid should be included in the diagnostic consideration. Paired box gene 8 (PAX8 ) is positive in 50% of the tumors; in contrast, both thyroid transcription factor 1 (TTF1 ) and thyroglobulin are usually negative.
-
The vast majority of cystic lesions of the thyroid are benign; however, cystic papillary carcinoma of the thyroid or metastatic squamous cell carcinoma with cystic degeneration may mimic a benign cystic lesion.
-
Parathyroid adenoma/neoplasm should be excluded if colloid is absent and numerous small naked nuclei and vascular-rich stroma are seen. Clear cell or oncocytic changes are common.
-
If the neoplastic cells are morphologically unlike follicular cells and colloid is absent in the background, a rare primary tumor or a metastasis should be considered. The most common metastases in the thyroid are renal cell (clear cell) carcinoma, melanoma , and adenocarcinoma of the lung, breast, and stomach.
-
If a mixture of histiocyte-like cells and lymphoid cells is present, Langerhans cell histiocytosis, follicular dendritic cell tumors, and other rare histiocytic lesions should be considered.
Modified from the 2004 World Health Organization (WHO) Classification of Thyroid and Parathyroid Tumors
Modified with permission from DeLellis RA, Williams ED. Tumors of the thyroid and parathyroid. In: DeLellis RA, Lloyd RV, Heitz PU, Eng C, editors. WHO classification of tumours. Pathology and genetics tumours of endocrine organs. Lyon, France: IARC Press; 2004:49–136.
Thyroid
Benign Nonneoplastic Lesions
-
Acute thyroiditis
-
Granulomatous thyroiditis/subacute thyroiditis
-
Hashimoto’s thyroiditis/lymphocytic thyroiditis
-
Nodular goiter
-
Graves’ disease
Neoplasms
Follicular Neoplasms
-
Follicular adenoma
-
Follicular carcinoma
Hurthle Cell Neoplasms
-
Hurthle cell adenoma
-
Hurthle cell carcinoma
Other Neoplasms
-
Papillary carcinoma
-
Medullary carcinoma
-
Poorly (insular) differentiated carcinoma
-
Undifferentiated (anaplastic) carcinoma
-
Hyalinizing trabecular neoplasm
Uncommon and Rare Lesions
-
Squamous cell carcinoma
-
Mucoepidermoid carcinoma
-
Sclerosing mucoepidermoid carcinoma with eosinophilia
-
Mucinous carcinoma
-
Spindle cell tumor with thymus-like differentiation
-
Carcinoma showing thymus-like differentiation
-
Lymphoma and plasmacytoma
-
Angiosarcoma
-
Smooth muscle tumor
-
Peripheral nerve sheath tumor
-
Solitary fibrous tumor
-
Follicular dendritic cell tumor
-
Langerhans cell histiocytosis
-
Teratoma
-
Ectopic thymoma
-
Second tumors
-
Kidney
-
Skin (melanoma )
-
Lung adenocarcinoma
-
Breast carcinoma
-
Gastric adenocarcinoma
-
Squamous cell carcinoma of the head and neck
-
Parathyroid
Parathyroid adenoma
Parathyroid carcinoma
The Bethesda System for Reporting Thyroid Cytopathology
FNA biopsy plays a crucial role in the assessment and triage of a thyroid nodule, and it has resulted in a significant reduction in unnecessary surgeries for patients with a benign lesion. However, some of the diagnostic categories and terminologies are inconsistent from one laboratory to another, which has created ambiguity and confusion among pathologists and clinicians. To clarify the potential misunderstanding and improve clarity of communication, the Bethesda System for Reporting Thyroid Cytopathology was introduced and published as an atlas in 2010. Six diagnostic categories and the associated risk of malignancy and recommended clinical management for each category were recommended as summarized in Table 3.1 below.
Perhaps the most important change was to introduce a distinct subcategory of “Atypia of Undetermined Significance/Follicular Lesion of Undetermined Significance.” This subcategory of lesions was defined as cellular components (follicular cells, lymphoid cells, and others) with architectural and/or nuclear atypia that is not sufficient to be classified as suspicious for a follicular neoplasm/Hurthle cell neoplasm, suspicious for malignancy, or malignancy. Also, the atypia cannot be confidently classified as benign change. The risk of malignancy in this category is about 5–15%, and a repeat FNA in a reasonable interval was suggested.
Normal Thyroid
Colloid
Colloid is the key diagnostic component for thyroid disease. Colloid appears to be light blue or blue-purple on a Diff-Quik (DQ)-stained slide (Fig. 3.1) and light purple to pink on Papanicolaou (Pap) stain (Fig. 3.2). Comparing the two staining methods, colloid is easier to observe on DQ stain. In the presence of blood and the absence of follicular cells, thin colloid can be difficult to differentiate from serum. The finding of even few follicular cells is an important clue to confirm the presence of thin or watery colloid. In general, two types of colloid are seen: one is thin or watery colloid (Fig. 3.3) and the other is thick or inspissated colloid (Fig. 3.4). When watery colloid falls off the slide, it resembles a spider web (Fig. 3.5).

Watery colloid on DQ stain

Watery colloid on Pap stain

Colloid on DQ stain with cracked glass window appearance

Thick colloid with dark blue staining on DQ stain

Colloid fell off the slide, with spiderweb appearance on DQ stain
Follicular Cells
Follicular cells are cuboids and uniform in size, with a honeycomb arrangement. Nuclei are round, 6–9 um, with small to inconspicuous nucleoli, fine nuclear chromatin with even distribution, and a smooth nuclear contour (Fig. 3.6).

Benign follicular cells with uniform size and orderly arrangement on DQ stain
In general, an adequate specimen should contain a minimum of six groups of well-visualized follicular cells with at least ten cells per group, preferably on a single slide, with the exception of these special circumstances: (1) colloid nodule, (2) solid nodules with cytologic atypia, and (3) solid nodules with inflammation such as lymphocytic thyroiditis or abscess .
Hurthle Cells
A subtype of follicular cells, slightly larger than normal follicular cells, with abundant granular cytoplasm, small to conspicuous nucleoli, and binucleation; they appear light purple on DQ stain and orange to pink on Pap stain (Fig. 3.7).

Hurthle cells with large nuclei and abundant eosinophilic granular cytoplasm
Flame Cells
A subtype of follicular cells, with abundant cytoplasm with cytoplasmic fine vacuoles; they appear purple-pink on DQ stain (Fig. 3.8). They reflect the hyperfunctional status of the thyroid, such as in Graves’ disease . They can be seen in nodular goiter and subacute thyroiditis as well .

Flame cells frequently seen in nodular goiter with hyperthyroid function
Respiratory Epithelial Cells
During the aspiration procedure, the needle may accidentally enter the trachea, and the aspirate may contain respiratory epithelial cells (Fig. 3.9).

Ciliated columnar respiratory epithelial cells when a needle accidentally enters the trachea
Benign Thyroid Lesions
Acute Thyroiditis
Clinical Features
-
Rare, caused by bacteria and fungus.
-
Fever and neck pain.
-
Biopsy is generally unnecessary because of the obvious clinical presentation. If a nodular lesion is formed, then a neoplastic lesion, especially an anaplastic carcinoma, should be included in the diagnostic consideration.
Cytological Features
-
Numerous acute inflammatory and histiocytes (Fig. 3.10a, b)
Fig. 3.10 
Acute inflammatory cells , histiocytes, and necrotic debris in acute thyroiditis (Pap stain)
-
Only few follicular cells
-
Necrotic debris or granulomatous inflammation
-
Fungus or bacteria can be seen on a special stain (Fig. 3.11)
Fig. 3.11 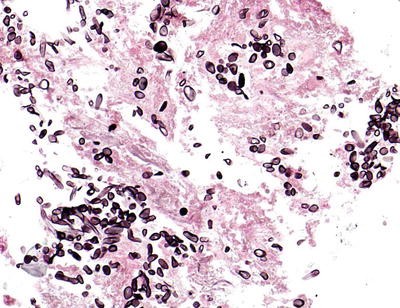
Fungal elements in acute thyroiditis (Grocott’s methenamine silver [GMS] stain)


Histologic Features
-
Acute inflammation with abscess formation and tissue necrosis
Differential Diagnosis
-
Anaplastic carcinoma
Granulomatous (de Quervain) Thyroiditis/Subacute Thyroiditis
Clinical Features
-
Caused by viral infection and a self-limiting process
-
More common in young female
-
Painful or painless diffuse thyroid enlargement
Cytological Features
-
Granulomatous inflammation with multinucleated giant cells; some giant cells may engulf colloid.
-
Many giant cells may contain many nuclei (many more nuclei than multinucleated giant cells seen in PTC).
-
Acute and chronic inflammatory cells.
-
Few follicular cells.
Histologic Features
-
Usually multiple non-caseating granulomas associated with marked inflammation
-
Granulomas containing foreign-body giant cells, which may engulf colloid (Figs. 3.12 and 3.13)
Fig. 3.12 
A large multinucleated giant cell in subacute thyroiditis
Fig. 3.13 
Epithelioid histiocytes in chronic granulomatous inflammation (DQ stain)
-
Thyroid follicles surrounded by granulomas and inflammation
-
Patchy fibrosis


Differential Diagnosis
-
Tuberculosis
-
Sarcoidosis
-
Mycoses
Hashimoto’s Thyroiditis/Lymphocytic Thyroiditis
Clinical Features
-
An autoimmune-related disease.
-
More common in middle-aged women.
-
Present with firm and diffuse enlargement of the thyroid.
-
Normal thyroid function in early stage and hypothyroidism in late stage.
-
Serological tests are positive for anti-thyroglobulin, anti-mitochondrial antibody, and anti-oxidase antibody.
Cytological Features
-
Infiltration of lymphocytes in Hurthle cells (Fig. 3.14a, b).
Fig. 3.14 
Infiltration of lymphoid cells within Hurthle cells in Hashimoto’s thyroiditis (Pap stain and DQ stain)
-
Acute and chronic inflammatory cells with plasma cells.
-
Multinucleated giant cells.
-
Granulomatous inflammation.
-
Reduced numbers of follicular cells dependent upon of the stage of the disease. It can be divided into three phases: (1) florid lymphoid phase, predominately a mixed population of lymphoid cells with sparse Hurthle cells and follicular cells; (2) cellular phase, proliferation of Hurthle cells; and (3) fibrotic phase, fibrotic tissue, scant Hurthle cells and lymphoid cells, and squamous cells (squamous metaplasia).
-
Reactive atypical follicular cells /Hurthle cells; may mimic papillary carcinoma.
-
May coexist with papillary carcinoma, especially papillary microcarcinoma .

Histologic Features
-
Typically diffuse involvement of the thyroid both grossly and microscopically but can be a localized process with a distinct nodular involvement.
-
Thyroid follicles with oncocytic changes and epithelial atrophy.
-
Lymphoplasmacytic infiltration of the stroma with many large lymphoid follicles, which contain prominent germinal centers (Fig. 3.15a–c).
Fig. 3.15 
Histologic sections of Hashimoto’s thyroiditis with oncocytic follicular cells with lymphoid cell infiltration (a, b), prominent germinal center (c) and Hurthle cell/follicular cells with reactive atypia (d)
-
Lymphoplasmacytic cells infiltrating oncocytic follicular cells.
-
Lymphoid cells, plasma cells, histiocytes, and scattered granulomas.
-
Patchy fibrosis or extensive fibrosis with dense hyaline-type collagens.
-
Squamous metaplasia is common.
-
Cystic formation may be present.
-
Reactive atypical follicles , which may mimic PTC (Fig. 3.15d).

Immunohistochemistry
-
Reactive oncocytic follicular cells may be positive for galectin-3 and Hector Battifora mesothelial epitope-1 (HBME-1) but usually negative for cytokeratin (CK) 19 and tumor-associated calcium signal transducer 2 (TROP2 ).
Differential Diagnosis
-
Papillary carcinoma
-
Hurthle cell neoplasm
-
Lymphoma
-
Riedel’s thyroiditis
Nodular Goiter
Clinical Features
-
The most common benign lesion
-
More common in middle-aged women
-
Normal thyroid function; sometimes hyper- or hypothyroidism
-
Goiter with multiple nodules
Cytological Features
-
Abundant colloid and small amount of follicular cells (Figs. 3.16, 3.17, 3.18, 3.19, 3.20, and 3.21).
Fig. 3.16 
Nodular goiter /hyperplasia with abundant watery colloid, benign follicular cells, and histiocytes (Pap stain)
Fig. 3.17 
Benign follicular cells in a nodular goiter/hyperplasia (DQ stain)
Fig. 3.18 
Hurthle cells in a nodular goiter/hyperplasia (Pap stain)
Fig. 3.19 
Hurthle cells in a nodular goiter (Pap stain)
Fig. 3.20 
Hurthle cells in a nodular goiter/hyperplasia (DQ stain)
Fig. 3.21 
Histiocytes in a nodular goiter/hyperplasia with degenerative change (DQ stain)
-
Mixed population of follicular cells, Hurthle cells, and histiocytes.
-
Pigment-laden histiocytes, foamy histiocytes, and stromal cells.
-
Follicular cells are arranged in a honeycomb pattern with follicles of variable sizes.
-
Focal reactive atypical follicular cells can be seen .






Histologic Features
-
A wide spectrum of histologic changes can be seen (Fig. 3.22a–c).
Fig. 3.22 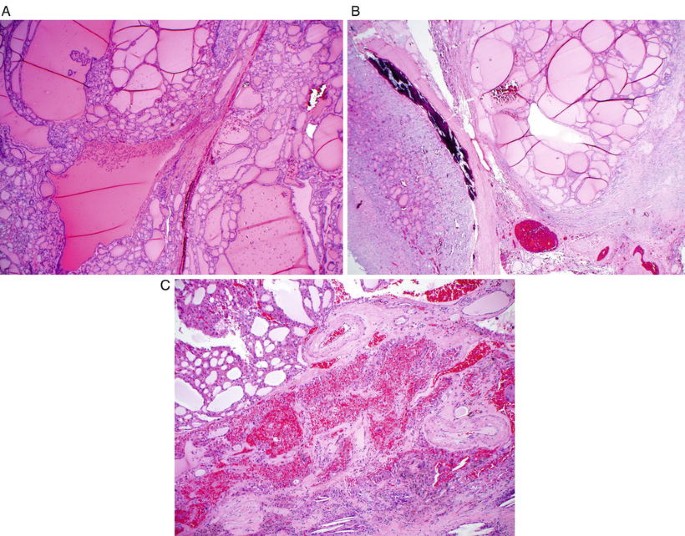
Histologic sections of nodular goiter with Hurthle cells changes, calcification, and degenerative and regenerative changes
-
Multiple nodules, some surrounded by partial or even complete capsules.
-
Huge follicles lined by flattened follicular epithelium, a mixture of follicles of variable sizes, cellular nodules with microfollicles, or cellular nodules with hyperplastic changes, including papillary formations.
-
Focal or diffuse Hurthle cell changes.
-
Secondary changes such as hemorrhage, cystic degeneration, fibrosis, calcification, or even ossification.
-
Rupture of follicles with granulomatous reaction, foreign body-type multinucleated giant cells, and variable numbers of chronic inflammatory cells .

Differential Diagnosis
-
Follicular neoplasm
-
Hurthle cell neoplasm
-
Papillary carcinoma
Neoplastic Thyroid Lesions
Follicular Neoplasm
-
Including follicular adenoma and follicular carcinoma
Follicular Adenoma
Clinical Features
-
Common benign neoplasm
-
More common in women
-
Usually present with a solitary, well-circumscribed, mass
Cytological Features
-
Hypercellular specimen with numerous groups of follicular cells and little or no colloid (Figs. 3.23 and 3.24).
Fig. 3.23 
Follicular neoplasm (DQ stain) with microfollicular growth pattern and lack of colloid in the background
Fig. 3.24 
Follicular neoplasm (DQ stain) with microfollicular growth pattern, nuclear enlargement, and nuclear crowding
-
Microfollicular growth pattern (defined as 6–12 crowded follicular cells in a ring or rosette-like structure, with or without colloid in the center).
-
Relatively uniform population of follicular cells without other types of cells, such as Hurthle cells and histiocytes.
-
Follicular cells are enlarged in size with round nuclei.
-
Focal nuclear atypia can be present .


Histologic Features
-
A follicular nodule enclosed by a fibrous capsule of variable thickness (Fig. 3.25a).
Fig. 3.25 
Histologic sections of follicular adenoma with thin fibrous capsule (a), microfollicular and solid pattern (b), trabecular pattern (c), macrofollicular (d), clear cell changes (e), and bizarre nuclei (f)
-
Absence of capsular or vascular invasion.
-
The architectural patterns may include microfollicular and solid (Fig. 3.25b), trabecular (Fig. 3.25c), normofollicular, and macrofollicular architectures (Fig. 3.25d).
-
The tumor cells are cuboidal, columnar or polygonal, and frequently with uniform, dark, round nuclei.
-
Foci of large nuclei or atypical nuclei with degenerative changes can be seen.
-
Mitotic figures are rare.
-
Many histologic variants have been described, such as clear cell follicular adenoma (Fig. 3.25e), oncocytic follicular adenoma, signet-ring cell follicular adenoma, lipoadenoma, mucinous follicular adenoma, follicular adenoma with bizarre nuclei (Fig. 3.25f), follicular adenoma with papillary hyperplasia, and hyperfunctioning follicular adenoma.
-
Secondary changes, such as myxoid change, cyst formation, fibrosis, hyalinization, hemorrhage, cartilaginous metaplasia, ossification, and calcifications, can be seen .

Immunohistochemistry
-
Positive for TTF1 , PAX8 , and thyroglobulin
-
Negative for calcitonin and neuroendocrine markers
-
Can be positive for HBME-1 and galectin-3 ; usually negative for CK19 and TROP2
Differential Diagnosis
-
Cellular nodular goiter
-
AUS/FLUS
-
Follicular variant of papillary carcinoma
Follicular Carcinoma
Clinical Features
-
More common in 40- to 60-year-old women.
-
Accounts for 10% of thyroid carcinomas.
-
A slow-growing neoplasm.
-
Can be divided into two types: minimally invasive type which is rarely going for distant metastasis ; another type is widely invasive type which is frequently goes for a distant metastasis and has a worse prognosis than papillary carcinoma of the thyroid .
Cytological Features (Figs. 3.26, 3.27, and 3.28)
-
In general, there are no definitive criteria to separate follicular adenoma from follicular carcinoma on an FNA sample.
-
Crowded and three-dimensional follicular structures.
-
Microfollicles with irregular shapes and many single cells.
-
Nuclear pleomorphism.
-
Nuclear enlargement (three to four times that of normal follicular cells).
-
Coarse and irregular nuclear chromatin.
-
High nuclear-to-cytoplasmic ratio.
-
Prominent and multiple nucleoli.
-
Mitoses can be seen .

Nuclear enlargement , crowding, and pleomorphism, suggestive of follicular carcinoma

Marked nuclear atypia , suggestive of follicular carcinoma (DQ stain)

Follicular carcinoma on Pap stain
Histologic Features
-
A follicular nodule enclosed by a thick fibrous capsule showing definite capsular and/or vascular invasion.
-
Lack of diagnostic nuclear features of PTC.
-
Can have variable architectural patterns and cytological features.
-
Classically, it can be divided into two categories: (1) minimally invasive follicular carcinoma with limited capsular invasive and vascular invasion (less than four vessels) and (2) widely invasive follicular carcinoma with widespread capsular and vascular invasion (greater than four vessels).
-
Fig. 3.29a–g shows some examples of capsular and vascular invasion.
Fig. 3.29 

Histology section of follicular carcinoma with capsular invasion (e) and vascular invasion (f, g)
-
Oncocytic variant and clear cell variant have been described .


Immunohistochemistry
-
Similar to follicular adenoma
-
Can be positive for HBME-1 and galectin-3 ; usually negative for CK19 and TROP2
Differential Diagnosis
-
Follicular adenoma
-
Follicular variant of papillary carcinoma
Hurthle Cell Neoplasm (Figs. 3.30, 3.31, 3.32, and 3.33a–c)
-
May be considered a subtype of follicular neoplasm
-
Uniform population of Hurthle cells in small clusters and single cells
-
Little or no colloid
-
Prominent or small nucleoli
-
Three-dimensional or crowded structures
-
Features suggestive for Hurthle cell carcinoma , including nuclear pleomorphism, multiple and prominent nucleoli, high nuclear-to-cytoplasmic ratio, nuclear crowding, and mitoses

Hurthle cell neoplasm with groups of Hurthle cells and absence of colloid in the background (DQ)

Histology section of Hurthle cell adenoma

Hurthle cell carcinoma on FNA smear (DQ)

Histologic sections of Hurthle cell carcinoma (a) with capsular (b) and vascular invasion (c)
Hyalinizing Trabecular Neoplasm
Clinical Features
-
A rare tumor of follicular cell origin.
-
The nuclear features of the tumor suggest that it may be related to PTC.
-
Rearranged during transfection (RET)/PTC rearrangements have been reported in some tumors.
-
Much more common in middle-aged women .
Cytological Features (Fig. 3.34a–d)
-
Similar cytological features to papillary carcinoma.
-
Hyalinizing material may be present between tumor cells.
-
Tumor cells may be more elongated or even spindle.
-
Nuclear grooves and intranuclear inclusions are frequent findings.
-
Psammoma bodies can be seen .

Hyalinizing trabecular adenoma with many cytological features of PTC, including intranuclear inclusion. Note that eosinophilic hyalinizing material between cells (a, DQ) and cellblock (d)
Histologic Features
-
A solid neoplasm with or without thin fibrous capsule.
-
Trabecular or alveolar growth pattern.
-
Polygonal or spindle tumor cells, with granular to clear cytoplasm, with a prominent hyaline stroma between nests or trabeculae of tumors.
-
Elongated nuclei, centrally located, with nuclear grooves and intranuclear pseudoinclusion (Fig. 3.35a, b).
Fig. 3.35 
Hyalinizing trabecular adenoma . Histologic sections showing elongated nuclei, centrally located with nuclear grooves and intranuclear pseudoinclusion (a, b). Note that MIB-1 (Ki-67) immunostain on histology section showing distinct membranous staining pattern (c)
-
Mitotic figures are rarely seen; psammoma bodies may be present.
-
Usually absence of colloid .

Immunohistochemistry
-
MIB-1 (a specific clone for Ki-67) staining showing distinctive membranous staining pattern in the majority of cases (Fig. 3.35c)
-
Frequently positive for galectin-3 ; can be positive for CK19
-
Positive for TTF1 and PAX8 and negative for calcitonin and neuroendocrine markers
Differential Diagnosis
-
Papillary carcinoma
-
Medullary carcinoma
-
Table 3.2 below summarizes useful markers for the distinction among these three tumors.
Table 3.2 Differentiation of hyalinizing trabecular neoplasm, papillary carcinoma, and medullary carcinoma by immunostains
PTC (Papillary Thyroid Carcinoma)
Clinical Features
-
Accounts for about 70% of malignant thyroid neoplasms.
-
More common in young females, with female-to-male ratio of 4:1, especially under age 40.
-
Slow growing; patient may survive for many years even after local lymph node metastasis .
-
Papillary microcarcinoma is defined as a tumor 1 cm or less in diameter.
-
Tall cell variant , columnar cell variant , diffuse sclerosing variant , and solid variant tend to show a more aggressive clinical behavior than a conventional PTC .
Cytological Features of Conventional PTC (Figs. 3.36, 3.37, 3.38, 3.39, 3.40, 3.41, 3.42, 3.43, 3.44, 3.45, 3.46, 3.47, and 3.48)
-
Hypercellular specimen with three-dimensional or two-dimensional papillary structures
-
Nuclear enlargement, overlapping, open nuclear chromatin, small and marginated nucleoli, nuclear grooves, and intranuclear cytoplasmic inclusions
-
Squamoid cytoplasm, oncocytic cytoplasm, or cytoplasm with small vacuoles
-
Thick colloid or gummy colloid
-
Multinucleated giant cells
-
Psammoma bodies

Papillary carcinoma with two-dimensional papillary structure (DQ stain)

Papillary carcinoma with three-dimensional papillary fronds (DQ stain)

Papillary carcinoma with nuclear enlargement and squamoid cytoplasm (DQ stain)

Papillary carcinoma with nuclear enlargement, overlapping, nuclear grooves, and intranuclear inclusions (Pap stain)

Papillary carcinoma with squamoid cytoplasm and septated cytoplasmic vacuoles and intranuclear cytoplasmic inclusion (DQ stain)

Papillary carcinoma with open nuclear chromatin, grooves, and intranuclear cytoplasmic inclusions (Pap stain)

Papillary carcinoma . Cytoplasmic vacuoles (Pap stain)

Papillary carcinoma . Squamoid cytoplasm (Pap stain)

Papillary carcinoma . Multinucleated giant cells (Pap stain)

Papillary carcinoma . Psammoma body (Pap stain)

Papillary carcinoma . Psammoma body (DQ stain)

Papillary carcinoma . Gummy/sticky colloid (DQ stain)

Papillary carcinoma . Multinucleated giant cells (DQ stain)
Cytologic Features for Variants of PTC
-
Follicular Variant
-
Resembles an FNA smear of follicular neoplasm.
-
Tumor cells mostly arranged in microfollicles with absence or near absence of papillary structures.
-
Nuclear features for PTC tend to be subtle when comparing to a classical PTC.
-
Less intranuclear pseudoinclusions.
-
Multinucleated giant cells, psammoma bodies, and cystic changes are usually absent.
-
Follicular neoplasm and parathyroid neoplasm are included in the diagnostic consideration .
-
-
Tall Cell Variant
-
Resembles a classic PTC.
-
The tumor cells have an elongated shape, with a height-to-width ratio of 3:1 or greater (Fig. 3.49a, b).
Fig. 3.49 
Cytologic features of some variants, tall cell variant (a, b), cystic variant (c), and Warthin-like variant (d)
-
Classic nuclear features are needed to render a definitive diagnosis.
-
-
Columnar Cell Variant
-
The neoplastic cells are arranged in papillae, groups, and sheets.
-
The nuclei are elongated and stratified.
-
The nuclear chromatin tends to be more hyperchromatic than open chromatin.
-
The intranuclear inclusions are less prominent.
-
Definitive nuclear changes for PTC are required to render a diagnosis.
-
-
Macrofollicular Variant
-
Resembles a benign colloid nodule on a low-power view with a mixture of sheets of follicular cells, some with microfollicular patterns, and abundant colloid.
-
Diagnosis is based on the observation of nuclear changes for PTC at higher magnification. In general, these tend to be subtle.
-
-
Oncocytic Variant
-
Resembles Hurthle cell proliferation, including Hurthle cell neoplasm.
-
The majority of tumor cells contain abundant oncocytic cytoplasm and are isolated or arranged in sheets or papillae.
-
Classic nuclear changes for PTC, including intranuclear inclusions.
-
Absence of lymphoid cells.
-
Nucleoli tend to be more conspicuous than in a conventional PTC; however, prominent nucleoli, frequently seen in a Hurthle cell neoplasm, are not typical features for an oncocytic variant of PTC .
-
-
Cystic Variant
-
Resembles a colloid cyst with very low cellularity or mainly hemosiderin-laden histiocytes and clear background.
-
Only a few groups of neoplastic follicular cells are present, and they are usually arranged in a small groups, sheets, papillae, or follicles (Fig. 3.49c).
-
The tumor cells may show “histiocytoid” features with cytoplasmic vacuoles.
-
Identification of diagnostic nuclear features for PTC, including intranuclear inclusions, is required to render a diagnosis .
-
-
Warthin-Like Variant
-
Resembles Hashimoto’s thyroiditis.
-
Oncocytic tumor cells arranged in sheets, groups, and papillary and follicular structures.
-
Lymphoplasmacytic background with lymphoid cells and plasma cells intimately associated with tumor cells (Fig. 3.49d).
-
Classic nuclear features for PTC are required to render a diagnosis .
-

Histologic Features
-
The characteristic nuclear features mentioned above are the key to making a diagnosis.
-
Complex papillary architectures with branching and squamous metaplasia are commonly seen.
-
The papillae may have markedly edematous changes.
-
Cystic changes are frequent.
-
Psammoma is frequently present.
-
Many histologic variants are present: (1) follicular variant (Fig. 3.50a), (2) oncocytic variant , (3) tall cell variant (Fig. 3.50b, c), (4) columnar cell variant , (5) diffuse sclerosing variant , (6) clear cell variant, (7) solid variant, (8) cystic variant (Fig. 3.50d, e), (9) cribriform variant (Fig. 3.50f, g), (10) macrofollicular variant , and (11) Warthin-like variant (Fig. 3.50h).
Fig. 3.50 

Histologic sections of follicular variant (a), tall cell variant (b, c), cystic variant (d, e), cribriform variant (f, g), and Warthin-like variant (h)
-
A small proportion of papillary carcinomas may show a combination of histologic variants, with focus/foci of (1) insular carcinoma, (2) squamous cell carcinoma, (3) mucoepidermoid carcinoma, (4) spindle cell and giant cell carcinoma, (5) and medullary carcinoma .


Immunohistochemistry
-
Positive for thyroglobulin, TTF1 , vimentin, and PAX8 ; negative for neuroendocrine markers and calcitonin .
-
Calectin-3, CK19 , HBME-1, and TROP2 are a useful panel of markers for the diagnosis of papillary carcinoma as summarized in Table 3.3. However, no single marker in this panel is entirely sensitive or specific for papillary carcinoma.
Table 3.3 Differentiation of PTC, follicular variant PTC, follicular adenoma, and reactive atypia by immunostains -
Antibodies to RET/PTC rearrangement and BRAF mutation can be useful as well.
-
An example of micropapillary PTC on FNA smear, CB, and positive for CK19 , HBME-1, and TROP2 was shown in Fig. 3.51a–e. The histologic section was shown in Fig. 3.51f, g.
Fig. 3.51 

Example of micropapillary carcinoma on FNA smear (a), cellblock (b), positive for CK19 (c), HBME-1 (d), and TROP2 (e), and the histologic section (f, g)


Molecular Alterations of Thyroid Tumors of Follicular Cell Origin
Table 3.4 summarizes the common genetic alterations reported in thyroid tumors of follicular cell origin .
Differential Diagnosis
-
Atypical follicular cells in nodular goiter or Hashimoto’s thyroiditis
-
Hyalinizing trabecular neoplasm
-
Medullary carcinoma
-
Follicular carcinoma
Medullary Carcinoma
Clinical Features
-
Accounts for 5–10% of malignant thyroid neoplasms.
-
More common in ages 40–60, male-to-female ratio is 2:3.
-
Most cases are associated with RET oncogene in chromosome 10 q11.2.
-
Associated with autosomal dominant trait in some patients.
-
Over 90% of tumors secrete calcitonin .
-
Painless thyroid mass.
-
C-cell hyperplasia is the precursor of heritable medullary carcinoma .
Cytological Features (Fig. 3.52a–i)
-
Mixed population of epithelioid and spindle neoplastic cells.
-
The tumor cells can be predominately single or in clusters, including sheets, follicles, microfollicles, rosettes, cords, or papillae.
-
Plasmacytoid cells with binucleation or multinucleation or bizarre cells.
-
Small to inconspicuous nucleoli.
-
Salt-and-pepper nuclear chromatin.
-
Intranuclear cytoplasmic inclusions.
-
Intracytoplasmic inclusions can be seen.
-
Amyloid in the background .


Cytologic features of medullary carcinoma with epithelioid and spindle cells (a, b), plasmacytoid cells and binucleation (c), spindle cells (d), intracytoplasmic inclusion (e), foamy cytoplasm (f), amyloid stroma (g), amyloid on Congo-red stain (h), and positive for calcitonin on cellblock (i)
Histologic Features (Fig. 3.53a–d)
-
Variable histologic growth patterns and architectures, including sheets, nests, trabeculae, pseudopapillary, follicular, and solid.
-
Polygonal, epithelioid, oncocytic, clear, spindle, melanotic, and small tumor cells or a mixture of different types of cells.
-
Salt-and-pepper chromatin, granular cytoplasm, and small nucleoli are common.
-
Prominent nucleoli are observed in oncocytic variant .
-
Intranuclear inclusions are frequently seen.
-
Intracytoplasmic lumen and mucin production have been reported.
-
Amyloid stroma has been reported in 80% of cases; giant cell reaction and calcification may be present.
-
Tumor necrosis and hemorrhage are uncommon.
-
Focal nuclear pleomorphism may be present but does not indicate a more clinical aggressiveness .

Histologic pattern of medullary carcinoma
Immunohistochemistry
-
95% of cases positive for calcitonin .
-
Over 95% of cases positive for carcinoembryonic antigen (CEA ).
-
Usually weakly positive for TTF1 .
-
Positive for chromogranin and synaptophysin .
-
Negative for thyroglobulin and PAX8 .
-
An example of IHC is shown in Fig. 3.54a–c.
Fig. 3.54 
Example of medullary carcinoma weakly positive for TTF1 (a) and positive for calcitonin (b) and chromogranin (c)

Differential Diagnosis
-
Insular carcinoma/poorly differentiated carcinoma of the thyroid
-
Anaplastic carcinoma of the thyroid
-
Hyalinizing trabecular neoplasm
-
Metastasis
Poorly Differentiated (Insular) Carcinoma
Clinical Features
-
More common in elderly patients
-
Prognosis better than anaplastic carcinoma but worse than papillary and follicular carcinoma
Cytological Features (Fig. 3.55a–c)
-
Relatively uniform population of neoplastic cells.
-
Single or small clusters of neoplastic cells.
-
Round to oval nuclei with hyperchromatic chromatin and high nuclear cytoplasmic ratio.
-
Little or absence of colloid.
-
Tumor necrosis can be seen .

Poorly differentiated (insular) carcinoma showing relatively uniform population of neoplastic cells with round to oval nuclei with hyperchromatic chromatin and high nuclear cytoplasmic ratio (a, DQ stain) and (b, c, Pap stain)
Histologic Features
-
Variable histologic growth patterns and insular, trabecular, solid, peritheliomatous, and infiltrating growth (Fig. 3.56a–c).
Fig. 3.56 
Histologic sections showing insular and trabecular growth and follicular patterns
-
Small uniform tumor cells with round, hyperchromatic to vesicular nuclear chromatin and small nucleoli.
-
Mitotic figures, vascular invasion, and tumor necrosis are common.
-
A small proportion of papillary carcinoma or follicular carcinoma may be present.
-
Regardless of the percentage, the presence of undifferentiated carcinoma component should be reported .

Immunohistochemistry
-
Positive for TTF1 , PAX8 , and thyroglobulin
-
Focal p53 positivity
-
Increased MIB-1 proliferative index
-
Negative for calcitonin and neuroendocrine markers
Differential Diagnosis
-
Medullary carcinoma
-
Follicular carcinoma
-
Metastasis
Undifferentiated (Anaplastic) Carcinoma
Clinical Features
-
Rare, accounting for 5% of malignant thyroid neoplasms
-
Usually occur after age 50, more common in women
-
Rapid growth in months
-
Diffuse enlargement of the thyroid with firm nodules and masses
-
Can be a painful or painless mass
Cytological Features (Fig. 3.57a–d)
-
Epithelioid, spindle, or giant neoplastic cells, singly or in small clusters
-
Marked nuclear pleomorphism, bizarre nuclei, with single or multiple prominent nucleoli
-
Frequent mitotic figures with abnormal mitoses
-
Extensive tumor necrosis and acute inflammatory cells in the background

Cytologic features of undifferentiated (anaplastic) carcinoma with a mixture of epithelioid, spindle, or giant neoplastic cells (a), numerous acute inflammatory cells (b, c), and abnormal mitosis (d)
Histologic Features
-
Admixture of spindle cells, pleomorphic giant cells, and epithelioid cells (Fig. 3.58a–d).
Fig. 3.58 
Undifferentiated (anaplastic) carcinoma showing histologic sections with pleomorphic giant cells, and epithelioid cells (a), exclusively spindle cells (b), squamoid changes (c), and transformation from PTC (d)
-
Tumor may show predominately or exclusively spindle cells with a sarcomatoid appearance.
-
Squamoid changes are common.
-
Prominent neutrophilic infiltrate can be seen.
-
Vascular invasion may be present.
-
Several histologic variants have been described: osteoclastic variant, paucicellular variant, and lymphoepithelioma-like variant.
-
A focus of well-differentiated or poorly differentiated thyroid carcinoma may be identified following an extensive sampling .

Immunohistochemistry
-
Most cases are negative for TTF1 and thyroglobulin.
-
About 50% of cases are positive for PAX8 (Fig. 3.59d) as shown in a needle core biopsy case (Fig. 3.59a–d).
Fig. 3.59 
An example of anaplastic carcinoma with spindle cell morphology on needle core biopsy specimen (a and b). Note tumor cell is positive for PAX8 (c) and high MIB1 proliferative index (d)
-
Strong p53 positivity is common.
-
Over 80% of cases are positive for one of the cytokeratins (AE1/3, CAM5.2, CK5/6, and 34betaE12).
-
Epithelial membrane antigen (EMA) is positive in less than 50% cases .

Differential Diagnosis
-
Medullary carcinoma
-
Soft tissue sarcomas
-
Metastasis , especially from the lung and pancreas
Uncommon and Rare Thyroid Lesions
Lymphoma and Plasmacytoma
-
Most cases are non-Hodgkin’s lymphoma with secondary involvement of the thyroid (Fig. 3.60a, b).
Fig. 3.60 
A diffuse large B-cell lymphoma on FNA smear
-
Approximately 15–20% of lymphomas may involve the thyroid.
-
Account for 1–3% of all malignant neoplasms of the thyroid
-
Plasmacytoma/multiple myeloma as a primary presentation in the thyroid (Fig. 3.61a, b).
Fig. 3.61 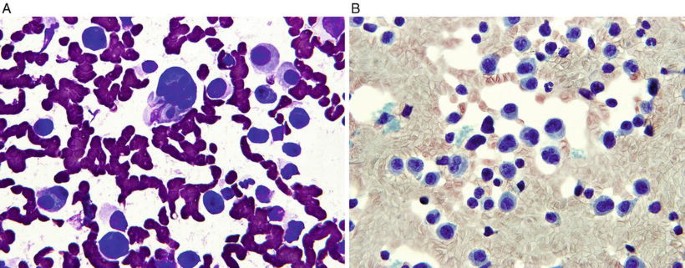
A plasmacytoma involving the thyroid as a primary presentation


Squamous Cell Carcinoma
-
Primary squamous cell carcinoma of the thyroid accounts for less than 1% of the malignant neoplasms of the thyroid. A metastasis especially from the head and neck, lung, and esophagus should be excluded.
Many other rare primary thyroid neoplasms have been recognized and reported in the literature. Table 3.5 summarizes the clinical, cytologic, and histologic features of these neoplasms and any ancillary tests which are potentially useful in making a diagnosis.
Metastases
-
The most common metastases are from the kidney, skin (melanoma ), lung, breast, stomach, and head and neck. Lymphomas and leukemias account for 15% of the cases.
-
Can be a solitary mass or multiple nodules; 80% of cases involve a single lobe.
-
Table 3.6 summarizes the useful IHC markers for the most common differential diagnosis.
Table 3.6 Summary of useful IHC markers for the common differential diagnoses -
Several examples of secondary tumors including metastatic renal cell carcinoma (Fig. 3.62a), breast carcinoma (Fig. 3.62b), and lung squamous cell carcinoma (Fig. 3.62c) are shown.
Fig. 3.62 
Examples of secondary tumors with metastatic renal cell carcinoma (a), breast carcinoma (b), and squamous cell carcinoma (c)

Parathyroid Adenoma/Neoplasm and Carcinoma
Parathyroid Adenoma/Neoplasm
Clinical Features
-
Clinical hypercalcemia is very helpful.
-
Usually involve a single parathyroid gland.
-
More common in patients 50–60 years of age.
-
Female-to-male ratio of approximately 3:1.
Cytologic Features (Fig. 3.63a–g)
-
Hypercellular specimen with similar features to follicular neoplasm.
-
Neoplastic cells tend to be smaller than follicular cells.
-
Numerous naked nuclei in the background.
-
Vascular-rich stroma.
-
Neuroendocrine nuclear chromatin.
-
Fine cytoplasmic vacuoles.
-
Oncocytic cytoplasm resembling Hurthle cell neoplasm.
-
Clear cell change is a frequent finding.
-
Focal marked nuclear pleomorphism may be present .


Cytologic features of parathyroid neoplasm are similar to follicular neoplasm with neoplastic cells smaller than follicular cells, numerous naked nuclei in the background, vascular-rich stroma, and oncocytic changes (a–e). Note the cellblock section (f) and positive for PTH (g)
Histologic Feature (Fig. 3.64a–g)
-
With or without a well-defined fibrous capsule.
-
Proliferation of chief cells, oncocytic cells, or a mixture of different cell types.
-
Many growth patterns such as solid sheets, nodular, trabecular, follicular, and acinar patterns; a mixture of growth patterns is common.
-
Cystic degeneration may be present.
-
Richly vascular stroma with limited fibrotic areas or fibrous bands.
-
Calcification or even ossification can occur.
-
The neoplastic chief cells show round nuclei, neuroendocrine chromatin, and small nucleoli.
-
Focal nuclear pleomorphism with giant hyperchromatic and multilobar nuclei may be seen.
-
A thin rim of normal parathyroid tissue at the periphery.
-
Mitotic figures are generally absent.
-
Massive infarction following an FNA can occur, but tumor necrosis is absent.
-
Three histologic variants have been described: oncocytic adenoma, water-clear cell adenoma, and lipoadenoma.
-
Absence or marked reduction of intracellular and extracellular neutral lipid by oil red O stain.
-
Atypical parathyroid adenoma has been used to describe an adenoma with broad fibrous bands and lack of other malignant features, such as vascular invasion, capsular invasion, increased mitoses, and tumor necrosis .


Histologic sections of parathyroid adenoma with different growth patterns and cell changes. Note that a rim of normal parathyroid tissue (b), clear cell changes (c), oncocytic changes (d), cystic changes (e), follicular-like structures (f), and positive for PTH (g)
Immunohistochemistry
-
Table 3.7 summarizes a panel of useful IHC markers in the differential diagnosis.
Table 3.7 Summary of useful IHC markers for differential diagnosis of follicular neoplasm/Hurthle cell neoplasm, parathyroid adenoma, and medullary carcinoma
Differential Diagnosis
-
Follicular neoplasm
-
Hurthle cell neoplasm
-
Medullary carcinoma
-
Papillary carcinoma
Parathyroid Carcinoma
Clinical Features
-
Rare; accounting for less than 1% of patients with primary hyperparathyroidism
-
Male-to-female ratio of approximately 1:1
-
High serum PTH and hypercalcemia
Cytologic Features
-
Tumor cells with large nuclei and prominent nucleoli, diffuse nuclear atypia, tumor necrosis, and increased mitoses are suggestive of malignancy.
Histologic Features (Fig. 3.65a–c)
-
Usually solid sheets, trabecular, follicular, rosette-like, and spindle cell growth patterns.
-
Can be chief cells, oncocytic cells, clear cells, or a mixture.
-
Broad fibrous bands and focal coagulative necrosis are commonly seen.
-
Enlarged nuclei with prominent nucleoli may be present.
-
Mitotic activity is extremely variable but often more than 5 per 50 high-power fields.
-
For a definitive malignancy, one of these features must be seen: (1) vascular invasion in the fibrous capsule or the surrounding soft tissue, (2) capsular penetration with invasion into the adjacent tissues, or (3) metastasis .

Histologic sections of parathyroid carcinoma with thick fibrous bands (a), trabecular growth pattern, nuclear atypia, tumor necrosis (b), and many mitoses (c)
Immunohistochemistry
-
Positive for PTH , chromogranin , and GATA3 .
-
Negative for calcitonin , TTF1 , PAX8 , and thyroglobulin.
-
Table 3.8 summarizes a panel of useful IHC markers in distinction of parathyroid carcinoma from parathyroid adenoma.
Table 3.8 Summary of IHC markers in distinction between parathyroid carcinoma from adenoma
Differential Diagnosis
-
Thyroid carcinoma
-
Medullary carcinoma
-
Metastasis







Abbreviation List
Abbreviation | Full text |
|---|---|
AUS/FLUS | Atypia of Undetermined Significance/Follicular Lesion of Undetermined Significance |
Bcl2 | B-cell CLL/lymphoma 2 |
CASTLE | Carcinoma showing thymus-like differentiation |
CD | Cluster of differentiation |
CDX2 | Caudal type homeobox 2 |
CEA | Carcinoembryonic antigen |
CK | Cytokeratin |
CRCC | Clear cell renal cell carcinoma |
DQ | Diff-Quik |
EMA | Epithelial membrane antigen |
ERG | ETS-related gene |
FDCT | Follicular dendritic cell tumor |
FNA | Fine-needle aspiration |
GATA3 | GATA-binding protein 3 |
GFAP | Glial fibrillary acidic protein |
GMS | Grocott’s methenamine silver |
HBME-1 | Hector Battifora mesothelial epitope-1 |
IHC | Immunohistochemical |
LCH | Langerhans cell histiocytosis |
MIB-1 | Mindbomb E3 ubiquitin protein ligase 1 |
MPNST | Malignant peripheral nerve sheath tumor |
MUC2 | Mucin 2 |
NSE | Neuron-specific enolase |
Pap | Papanicolaou |
PAX8 | Paired box gene 8 |
PNST | Peripheral nerve sheath tumor |
PTC | Papillary thyroid carcinoma |
PTH | Parathyroid hormone |
pVHL | von Hippel-Lindau tumor suppressor gene protein |
RCCma | Renal cell carcinoma marker |
RDD | Rosai-Dorfman disease |
RET | Rearranged during transfection |
SCC | Squamous cell carcinoma |
SETTLE | Spindle epithelial tumor with thymus-like differentiation |
SFT | Solitary fibrous tumor |
SMA | Smooth muscle actin |
SMECE | Sclerosing mucoepidermoid carcinoma with eosinophils |
SMT | Smooth muscle tumor |
STAT6 | Signal transducer and activator of transcription 6 |
TROP2 | Tumor-associated calcium signal transducer 2 |
TTF1 | Thyroid transcription factor 1 |
WHO | World Health Organization |
Suggested Reading
Cytology/Fine-Needle Aspiration
Aggarwal SK, Jayaram G, Kakar A, Goel GD, Prakash R, Pant CS. Fine needle aspiration cytologic diagnosis of the solitary cold thyroid nodule. Comparison with ultrasonography, radionuclide perfusion study and xeroradiography. Acta Cytol. 1989;33(1):41–7.
Ali SZ, Cibas ES, editors. The bethesda system for reporting thyroid cytopathology. New York: Springer Science+Business Media; 2010.
Baloch ZW, LiVolsi VA. Cytologic and architectural mimics of papillary thyroid carcinoma. Diagnostic challenges in fine-needle aspiration and surgical pathology specimens. Am J Clin Pathol. 2006a;125(Suppl):S135–44.
Baloch ZW, LiVolsi VA. Warthin-like papillary carcinoma of the thyroid. Arch Pathol Lab Med. 2000a;124(8):1192–5.
Baloch ZW, LiVolsi VA, Asa SL, Rosai J, Merino MJ, Randolph G, et al. Diagnostic terminology and morphologic criteria for cytologic diagnosis of thyroid lesions: a synopsis of the National Cancer Institute thyroid fine-needle aspiration state of the science conference. Diagn Cytopathol. 2008;36(6):425–37.
Barroeta JE, Baloch ZW, Lal P, Pasha TL, Zhang PJ, LiVolsi VA. Diagnostic value of differential expression of CK19, galectin-3, HBME-1, ERK, RET, and p16 in benign and malignant follicular-derived lesions of the thyroid: an immunohistochemical tissue microarray analysis. Endocr Pathol. 2006a;17(3):225–34.
Bhatia A, Rajwanshi A, Dash RJ, Mittal BR, Saxena AK. Lymphocytic thyroiditis--is cytological grading significant? A correlation of grades with clinical, biochemical, ultrasonographic and radionuclide parameters. Cytojournal. 2007;4:10.
Bongiovanni M, Bloom L, Krane JF, Baloch ZW, Powers CN, Hintermann S, et al. Cytomorphologic features of poorly differentiated thyroid carcinoma: a multi-institutional analysis of 40 cases. Cancer. 2009a;117(3):185–94.
Bongiovanni M, Crippa S, Baloch Z, Piana S, Spitale A, Pagni F, et al. Comparison of 5-tiered and 6-tiered diagnostic systems for the reporting of thyroid cytopathology: a multi-institutional study. Cancer Cytopathol. 2012;120(2):117–25.
Bongiovanni M, Triponez F, McKee TA, Kumar N, Matthes T, Meyer P. Fine-needle aspiration of the diffuse sclerosing variant of papillary thyroid carcinoma masked by florid lymphocytic thyroiditis; a potential pitfall: a case report and review of the literature. Diagn Cytopathol. 2009b;37(9):671–5.
Bose S, Kapila K, Verma K. Medullary carcinoma of the thyroid: a cytological, immunocytochemical, and ultrastructural study. Diagn Cytopathol. 1992;8(1):28–32.
Cameselle-Teijeiro J, Chan JK. Cribriform-morular variant of papillary carcinoma: a distinctive variant representing the sporadic counterpart of familial adenomatous polyposis-associated thyroid carcinoma? Mod Pathol. 1999;12(4):400–11.
Casey MB, Sebo TJ, Carney JA. Hyalinizing trabecular adenoma of the thyroid gland identification through MIB-1 staining of fine-needle aspiration biopsy smears. Am J Clin Pathol. 2004;122(4):506–10.
Cersosimo E, Gharib H, Suman VJ, Goellner JR. “Suspicious” thyroid cytologic findings: outcome in patients without immediate surgical treatment. Mayo Clin Proc. 1993;68(4):343–8.
Chan JK, Saw D. The grooved nucleus. A useful diagnostic criterion of papillary carcinoma of the thyroid. Am J Surg Pathol. 1986;10(10):672–9.
Chang TC, Lai SM, Wen CY, Hsiao YL. Three-dimensional cytomorphology in fine needle aspiration biopsy of subacute thyroiditis. Acta Cytol. 2004;48(2):155–60.
Collins BT, Cramer HM, Tabatowski K, Hearn S, Raminhos A, Lampe H. Fine needle aspiration of medullary carcinoma of the thyroid. Cytomorphology, immunocytochemistry and electron microscopy. Acta Cytol. 1995;39(5):920–30.
DeLellis RA. Orphan Annie eye nuclei: a historical note. Am J Surg Pathol. 1993;17(10):1067–8.
DeMay RM. Thyroid. In:The art and science of cytopathology. 2nd ed. Chicago: ASCP Press; 2010. p. 841–95.
Deveci MS, Deveci G, LiVolsi VA, Baloch ZW. Fine-needle aspiration of follicular lesions of the thyroid. Diagnosis and follow-up. Cytojournal. 2006;3:9.
Dugan JM, Atkinson BF, Avitabile A, Schimmel M, LiVolsi VA. Psammoma bodies in fine needle aspirate of the thyroid in lymphocytic thyroiditis. Acta Cytol. 1987;31:330–4.
Gamboa-Domínguez A, Candanedo-González F, Uribe-Uribe NO, Angeles-Angeles A. Tall cell variant of papillary thyroid carcinoma. A cytohistologic correlation. Acta Cytol. 1997;41(3):672–6.
Gharib H, Goellner JR, Johnson DA. Fine-needle aspiration cytology of the thyroid. A 12-year experience with 11,000 biopsies. Clin Lab Med. 1993;13(3):699–709.
Giorgadze T, Rossi ED, Fadda G, Gupta PK, Livolsi VA, Baloch Z. Does the fine-needle aspiration diagnosis of “Hurthle-cell neoplasm/follicular neoplasm with oncocytic features” denote increased risk of malignancy? Diagn Cytopathol. 2004;31:307–12.
Goellner JR. Problems and pitfalls in thyroid cytology. Monogr Pathol. 1997;39:75–93.
Guarda LA, Peterson CE, Hall W, Baskin HJ. Anaplastic thyroid carcinoma: cytomorphology and clinical implications of fine-needle aspiration. Diagn Cytopathol. 1991;7(1):63–7.
Gutman PD, Henry M. Fine needle aspiration cytology of the thyroid. Clin Lab Med. 1998;18(3):461–82.
Jayaram G. Fine needle aspiration cytologic study of the solitary thyroid nodule. Profile of 308 cases with histologic correlation. Acta Cytol. 1985;29(6):967–73.
Kini SR, Miller JM, Hamburger JI. Cytopathology of Hürthle cell lesions of the thyroid gland by fine needle aspiration. Acta Cytol. 1981;25(6):647–52.
Kumarasinghe MP, De Silva S. Pitfalls in cytological diagnosis of autoimmune thyroiditis. Pathology. 1999;31(1):1–7.
Luze T, Tötsch M, Bangerl I, Hittmair A, Sandbichler P, Ladurner D, et al. Fine needle aspiration cytodiagnosis of anaplastic carcinoma and malignant haemangioendothelioma of the thyroid in an endemic goitre area. Cytopathology. 1990;1(5):305–10.
Oertel YC. Fine-needle aspiration and the diagnosis of thyroid cancer. Endocrinol Metab Clin North Am. 1996;25(1):69–91.
Oertel YC, Miyahara-Felipe L, Mendoza MG, Yu K. Value of repeated fine needle aspirations of the thyroid: an analysis of over ten thousand FNAs. Thyroid. 2007;17(11):1061–6.
Oertel YC, Oertel JE. Diagnosis of malignant epithelial thyroid lesions: fine needle aspiration and histopathologic correlation. Ann Diagn Pathol. 1998;2(6):377–400.
Papaparaskeva K, Nagel H, Droese M. Cytologic diagnosis of medullary carcinoma of the thyroid gland. Diagn Cytopathol. 2000;22(6):351–8.
Pérez F, Llobet M, Garijo G, Barceló C, Castro P, Bernadó L. Fine-needle aspiration cytology of columnar-cell carcinoma of the thyroid: report of two cases with cytohistologic correlation. Diagn Cytopathol. 1998;18(5):352–6.
Renshaw AA, Wang E, Haja J, Wilbur D, Henry MR, Hughes JH, Cytopathology Committee, College of American Pathologists. Fine-needle aspiration of papillary thyroid carcinoma: distinguishing between cases that performed well and those that performed poorly in the College of American Pathologists Nongynecologic Cytology Program. Arch Pathol Lab Med. 2006a;130(4):452–5.
Renshaw AA, Wang E, Wilbur D, Hughes JH, Haja J, Henry MR, College of American Pathologists Cytopathology Committee. Interobserver agreement on microfollicles in thyroid fine-needle aspirates. Arch Pathol Lab Med. 2006b;130(2):148–52.
Söderström N, Biörklund A. Intranuclear cytoplasmic inclusions in some types of thyroid cancer. Acta Cytol. 1973;17(3):191–7.
Wong LQ, LiVolsi VA, Baloch ZW. Diagnosis of atypia/follicular lesion of undetermined significance: an institutional experience. Cytojournal. 2014;11:23.
Yang GC, LiVolsi VA, Baloch ZW. Thyroid microcarcinoma: fine-needle aspiration diagnosis and histologic follow-up. Int J Surg Pathol. 2002;10:133–9.
Histology
Ahuja AT, Chan ES, Allen PW, Lau KY, King W, Metreweli C. Carcinoma showing thymiclike differentiation (CASTLE tumor). AJNR Am J Neuroradiol. 1998;19(7):1225–8.
Albores-Saavedra J, Gould E, Vardaman C, Vuitch F. The macrofollicular variant of papillary thyroid carcinoma: a study of 17 cases. Hum Pathol. 1991;22(12):1195–205.
Albores-Saavedra J, LiVolsi VA, Williams ED. Medullary carcinoma. Semin Diagn Pathol. 1985;2(2):137–46.
Aldinger KA, Samaan NA, Ibanez M, Hill CS Jr. Anaplastic carcinoma of the thyroid: a review of 84 cases of spindle and giant cell carcinoma of the thyroid. Cancer. 1978;41(6):2267–75.
Apel RL, Asa SL, LiVolsi VA. Papillary Hürthle cell carcinoma with lymphocytic stroma. “Warthin-like tumor” of the thyroid. Am J Surg Pathol. 1995;19(7):810–4.
Asa SL. My approach to oncocytic tumours of the thyroid. J Clin Pathol. 2004;57(3):225–32.
Baloch ZW, LiVolsi VA. Microcarcinoma of the thyroid. Adv Anat Pathol. 2006b;13(2):69–75.
Baloch ZW, LiVolsi VA. Our approach to follicular-patterned lesions of the thyroid. J Clin Pathol. 2007;60(3):244–50.
Baloch ZW, LiVolsi VA. Warthin-like papillary carcinoma of the thyroid. Arch Pathol Lab Med. 2000b;124(8):1192–5.
Baloch ZW, Solomon AC, LiVolsi VA. Primary mucoepidermoid carcinoma and sclerosing mucoepidermoid carcinoma with eosinophilia of the thyroid gland: a report of nine cases. Mod Pathol. 2000;13(7):802–7.
Ben Romdhane K, Khattech R, Ben Othman M, Gamoudi A, Ammar A, Cammoun M. Melanin production in medullary thyroid carcinoma. Histopathology. 1995;27(6):569–71.
Berho M, Suster S. The oncocytic variant of papillary carcinoma of the thyroid: a clinicopathologic study of 15 cases. Hum Pathol. 1997;28(1):47–53.
Bronner MP, LiVolsi VA. Spindle cell squamous carcinoma of the thyroid: an unusual anaplastic tumor associated with tall cell papillary cancer. Mod Pathol. 1991;4(5):637–43.
Cameselle-Teijeiro J. Mucoepidermoid carcinoma and solid cell nests of the thyroid. Hum Pathol. 1996;27(8):861–3.
Cameselle-Teijeiro J, Varela-Duran J, Fonseca E, Villanueva JP, Sobrinho-Simoes M. Solitary fibrous tumor of the thyroid. Am J Clin Pathol. 1994;101(4):535–8.
Carcangiu ML, Bianchi S. Diffuse sclerosing variant of papillary thyroid carcinoma. Clinicopathologic study of 15 cases. Am J Surg Pathol. 1989;13(12):1041–9.
Carcangiu ML, Steeper T, Zampi G, Rosai J. Anaplastic thyroid carcinoma. A study of 70 cases. Am J Clin Pathol. 1985;83(2):135–58.
Carcangiu ML, Zampi G, Rosai J. Poorly differentiated (“insular”) thyroid carcinoma. A reinterpretation of Langhans’ “wuchernde Struma”. Am J Surg Pathol. 1984;8(9):655–68.
Carney JA, Ryan J, Goellner JR. Hyalinizing trabecular adenoma of the thyroid gland. Am J Surg Pathol. 1987;11(8):583–91.
Chan JK, Albores-Saavedra J, Battifora H, Carcangiu ML, Rosai J. Sclerosing mucoepidermoid thyroid carcinoma with eosinophilia. A distinctive low-grade malignancy arising from the metaplastic follicles of Hashimoto’s thyroiditis. Am J Surg Pathol. 1991;15(5):438–48.
JKC C. Tumors of thyroid and parathyroid glands. In: Fletcher CDM, editor. Diagnostic histopathology of tumors. 4th ed. London: Churchill Livingstone; 2013. p. 1177–293.
Chem KT, Rosai J. Follicular variant of thyroid papillary carcinoma: a clinicopathologic study of six cases. Am J Surg Pathol. 1977;1(2):123–30.
Chetty R, Clark SP, Dowling JP. Leiomyosarcoma of the thyroid: immunohistochemical and ultrastructural study. Pathology. 1993;25(2):203–5.
Cheung CC, Boerner SL, MacMillan CM, Ramyar L, Asa SL. Hyalinizing trabecular tumor of the thyroid: a variant of papillary carcinoma proved by molecular genetics. Am J Surg Pathol. 2000;24(12):1622–6.
Chow SM, Law SC, Chan JK, Au SK, Yau S, Lau WH. Papillary microcarcinoma of the thyroid-prognostic significance of lymph node metastasis and multifocality. Cancer. 2003;98(1):31–40.
DeLellis RA, Williams ED. Tumors of the thyroid and parathyroid. In: DeLellis RA, Lloyd RV, Heitz PU, Eng C, editors. WHO classification of tumours. Pathology and genetics tumours of endocrine organs. Lyon: IARC Press; 2004. p. 49–136.
Dotto J, Nose V. Familial thyroid carcinoma: a diagnostic algorithm. Adv Anat Pathol. 2008;15(6):332–49.
Evans HL. Columnar-cell carcinoma of the thyroid. A report of two cases of an aggressive variant of thyroid carcinoma. Am J Clin Pathol. 1986;85(1):77–80.
Fenton PA, Clarke SE, Owen W, Hibbert J, Hodgson SV. Cribriform variant papillary thyroid cancer: a characteristic of familial adenomatous polyposis. Thyroid. 2001;11(2):193–7.
Flynn SD, Forman BH, Stewart AF, Kinder BK. Poorly differentiated (“insular”) carcinoma of the thyroid gland: an aggressive subset of differentiated thyroid neoplasms. Surgery. 1988;104(6):963–70.
Franssila KO, Ackerman LV, Brown CL, Hedinger CE. Follicular carcinoma. Semin Diagn Pathol. 1985;2(2):101–22.
Ghossein R. Problems and controversies in the histopathology of thyroid carcinomas of follicular cell origin. Arch Pathol Lab Med. 2009;133(5):683–91.
Hazard JB, Kenyon R. Atypical adenoma of the thyroid. AMA Arch Pathol. 1954a;58(6):554–63.
Hazard JB, Kenyon R. Encapsulated angioinvasive carcinoma (angioinvasive adenoma) of the thyroid gland. Am J Clin Pathol. 1954b;24(7):755–66.
Hiltzik D, Carlson DL, Tuttle RM, Chuai S, Ishill N, Shaha A, et al. Poorly differentiated thyroid carcinomas defined on the basis of mitosis and necrosis: a clinicopathologic study of 58 patients. Cancer. 2006;106(6):1286–95.
Hunt JL, Barnes EL. Non-tumor-associated psammoma bodies in the thyroid. Am J Clin Pathol. 2003;119(1):90–4.
Iwasa K, Imai MA, Noguchi M, Tanaka S, Sasaki T, Katsuda S, et al. Spindle epithelial tumor with thymus-like differentiation (SETTLE) of the thyroid. Head Neck. 2002;24(9):888–93.
Kirby PA, Ellison WA, Thomas PA. Spindle epithelial tumor with thymus-like differentiation (SETTLE) of the thyroid with prominent mitotic activity and focal necrosis. Am J Surg Pathol. 1999;23(6):712–6.
Landon G, Ordonez NG. Clear cell variant of medullary carcinoma of the thyroid. Hum Pathol. 1985;16(8):844–7.
Lang W, Georgii G. Minimal invasive cancer in the thyroid. Clin Oncol. 1982;1:527–37.
Mendelsohn G, Baylin SB, Bigner SH, Wells SA Jr, Eggleston JC. Anaplastic variants of medullary thyroid carcinoma: a light-microscopic and immunohistochemical study. Am J Surg Pathol. 1980;4(4):333–41.
Mills SE, Gaffey MJ, Watts JC, Swanson PE, Wick MR, LiVolsi VA. Angiomatoid carcinoma and “angiosarcoma” of the thyroid gland. A spectrum of endothelial differentiation. Am J Clin Pathol. 1994;102(3):322–30.
Montone KT, Baloch ZW, LiVolsi VA. The thyroid Hurthle (oncocytic) cell and its associated pathologic conditions: a surgical pathology and cytopathology review. Arch Pathol Lab Med. 2008;132(8):1241–50.
Nikiforov YE, Erickson LA, Nikiforova MN, Caudill CM, Lloyd RV. Solid variant of papillary thyroid carcinoma: incidence, clinical-pathologic characteristics, molecular analysis, and biologic behavior. Am J Surg Pathol. 2001;25(12):1478–84.
Ostrowski M, Merino MJ. Tall cell variant of papillary thyroid carcinoma: a reassessment and immunohistochemical study with comparison to usual type of papillary carcinoma of the thyroid. Am J Surg Pathol. 1996;20(8):964–74.
Rosai J, Saxén EA, Woolner L. Undifferentiated and poorly differentiated carcinoma. Semin Diagn Pathol. 1985;2(2):123–36.
Rosai J, Tallini G. Thyroid gland. In: Rosai J, editor. Rosai and Ackerman’s surgical pathology. 10th ed. London: Mosby Elsevier; 2011. p. 487–564.
Sambade C, Baldaque-Faria A, Cardoso-Oliveira M, Sobrinho-Simões M. Follicular and papillary variants of medullary carcinoma of the thyroid. Pathol Res Pract. 1988;184(1):98–107.
Schmid KW, Mesewinkel F, Böcker W. Hyalinizing trabecular adenoma of the thyroid--morphology and differential diagnosis. Acta Med Austriaca. 1996;23(1–2):65–8.
Schmidt RJ, Wang CA. Encapsulated follicular carcinoma of the thyroid: diagnosis, treatment, and results. Surgery. 1986;100(6):1068–77.
Sobrinho-Simoes M, Sambade C, Nesland JM, Johannessen JV. Tall cell papillary carcinoma. Am J Surg Pathol. 1989;13(1):79–80.
Thieblemont C, Mayer A, Dumontet C, Barbier Y, Callet-Bauchu E, Felman P. Primary thyroid lymphoma is a heterogeneous disease. J Clin Endocrinol Metab. 2002;87(1):105–11.
Volante M, Collini P, Nikiforov YE, Sakamoto A, Kakudo K, Katoh R, et al. Poorly differentiated thyroid carcinoma: the Turin proposal for the use of uniform diagnostic criteria and an algorithmic diagnostic approach. Am J Surg Pathol. 2007;31(8):1256–64.
Wang SA, Rahemtullah A, Faquin WC, Roepke J, Harris NL, Hasserjian RP. Hodgkin’s lymphoma of the thyroid: a clinicopathologic study of five cases and review of the literature. Mod Pathol. 2005;18(12):1577–84.
Wenig BM, Adair CF, Heffess CS. Primary mucoepidermoid carcinoma of the thyroid gland: a report of six cases and a review of the literature of a follicular epithelial-derived tumor. Hum Pathol. 1995;26(10):1099–108.
Wenig BM, Thompson LD, Adair CF, Shmookler B, Heffess CS. Thyroid papillary carcinoma of columnar cell type. A clinicopathologic study of 16 cases. Cancer. 1998;82(4):740–53.
Zaatari GS, Saigo PE, Huvos AG. Mucin production in medullary carcinoma of the thyroid. Arch Pathol Lab Med. 1983;107(2):70–4.
Ancillary Tests: Immunohistochemistry
Abrosimov A. Histologic and immunohistochemical characterization of medullary thyroid carcinoma. Arkh Patol. 1996;58(4):43–8. Russian.
Barroeta JE, Baloch ZW, Lal P, Pasha TL, Zhang PJ, LiVolsi VA. Diagnostic value of differential expression of CK19, galectin-3, HBME-1, ERK, RET, and p16 in benign and malignant follicular-derived lesions of the thyroid: an immunohistochemical tissue microarray analysis. Endocr Pathol. 2006b;17(3):225–34.
Cheung CC, Ezzat S, Freeman JL, Rosen IB, Asa SL. Immunohistochemical diagnosis of papillary thyroid carcinoma. Mod Pathol. 2001;14(4):338–42.
DeLilles RA, Rule AH, Spiler I, Nathanson L, Tashjian AH Jr, Wolfe HJ. Calcitonin and carcinoembryonic antigen as tumor markers in medullary thyroid carcinoma. Am J Clin Pathol. 1978;70(4):587–94.
Hirokawa M, Carney JA, Ohtsuki Y. Hyalinizing trabecular adenoma and papillary carcinoma of the thyroid gland express different cytokeratin patterns. Am J Surg Pathol. 2000;24(6):877–81.
Lin F, Liu H. Immunohistochemistry in undifferentiated neoplasm/tumor of uncertain origin. Arch Pathol Lab Med. 2014;138(12):1583–610.
Liu H, Lin F. Application of immunohistochemistry in thyroid pathology. Arch Pathol Lab Med. 2015;139(1):67–82.
Liu H, Shi J, Lin F. The potential diagnostic utility of TROP-2 in thyroid neoplasms. Appl Immunohistochem Mol Morphol. 2016. Epub 2016 Feb 9.
Liu H, Wilkerson M, Lin F. Thyroid, parathyroid and adrenal glands. In: Lin F, Prichard JW, Liu H, Wilkerson M, Chen ZE, editors. Handbook of practical immunohistochemistry – frequently asked questions. 2nd ed. New York: Springer Science+Business Media; 2015. p. 255–86.
LiVolsi VA, Brooks JJ, Arendash-Durand B. Anaplastic thyroid tumors. Immunohistology. Am J Clin Pathol. 1987;87(4):434–42.
Nonaka D, Tang Y, Chiriboga L, Rivera M, Ghossein R. Diagnostic utility of thyroid transcription factors Pax8 and TTF-2 (FoxE1) in thyroid epithelial neoplasms. Mod Pathol. 2008;21(2):192–200.
Ordóñez NG, El-Naggar AK, Hickey RC, Samaan NA. Anaplastic thyroid carcinoma. Immunohistochemical study of 32 cases. Am J Clin Pathol. 1991;96(1):15–24.
Rosai J. Immunohistochemical markers of thyroid tumors: significance and diagnostic applications. Tumori. 2003;89(5):517–9.
Williams ED, Ponder BJ, Craig RK. Immunohistochemical study of calcitonin gene-related peptide in human medullary carcinoma and C cell hyperplasia. Clin Endocrinol (Oxf). 1987;27(1):107–14.
Ancillary Tests: Molecular Testing
Barzon L, et al. Characterization of a novel complex BRAF mutation in a follicular variant papillary thyroid carcinoma. Eur J Endocrinol. 2008;159:77–80.
Capella G, Matias-Guiu X, Ampudia X, de Leiva A, Perucho M, Prat J. Ras oncogene mutations in thyroid tumors: polymerase chain reaction-restriction-fragment-length polymorphism analysis from paraffin-embedded tissues. Diagn Mol Pathol. 1996;5(1):45–52.
Cohen Y, Xing M, Mambo E, Guo Z, Wu G, Trink B, et al. BRAF mutation in papillary thyroid carcinoma. J Natl Cancer Inst. 2003;95(8):625–7.
Elisei R, Romei C, Vorontsova T, Cosci B, Veremeychik V, Kuchinskaya E, et al. RET/PTC rearrangements in thyroid nodules: studies in irradiated and not irradiated, malignant and benign thyroid lesions in children and adults. J Clin Endocrinol Metab. 2001;86(7):3211–6.
Eng C, Mulligan LM, Smith DP, Healey CS, Frilling A, et al. Mutation of the RET protooncogene in sporadic medullary thyroid carcinoma. Genes Chromosomes Cancer. 1995;12(3):209–12.
Esapa CT, Johnson SJ, Kendall-Taylor P, Lennard TW, Harris PE. Prevalence of Ras mutations in thyroid neoplasia. Clin Endocrinol (Oxf). 1999;50(4):529–35.
Fabien N, Paulin C, Santoro M, Berger N, Grieco M, Galvain D. Detection of RET oncogene activation in human papillary thyroid carcinomas by in situ hybridisation. Br J Cancer. 1992;66(6):1094–8.
Frank-Raue K, Rondot S, Raue F. Molecular genetics and phenomics of RET mutations: impact on prognosis of MTC. Mol Cell Endocrinol. 2010;322(1–2):2–7.
Giordano TJ, Kuick R, Thomas DG, Misek DE, Vinco M, Sanders D, et al. Molecular classification of papillary thyroid carcinoma: distinct BRAF, RAS, and RET/PTC mutation-specific gene expression profiles discovered by DNA microarray analysis. Oncogene. 2005;24(44):6646–56.
Inaba M, Umemura S, Satoh H, Abe Y, Kurokawa K, Sakai H, et al. Expression of RET in follicular cell-derived tumors of the thyroid gland: prevalence and implication of morphological type. Pathol Int. 2003;53(3):146–53.
Jhiang SM, Fithian L, Weghorst CM, Clark OH, Falko JM, O’Dorisio TM, et al. RET mutation screening in MEN2 patients and discovery of a novel mutation in a sporadic medullary thyroid carcinoma. Thyroid. 1996;6(2):115–21.
Kimura ET, Nikiforova MN, Zhu Z, Knauf JA, Nikiforov YE, Fagin JA. High prevalence of BRAF mutations in thyroid cancer: genetic evidence for constitutive activation of the RET/PTC-RAS-BRAF signaling pathway in papillary thyroid carcinoma. Cancer Res. 2003;63(7):1454–7.
Kroll TG. Molecular events in follicular thyroid tumors. Cancer Treat Res. 2004;122:85–105.
Marques AR, Espadinha C, Catarino AL, Moniz S, Pereira T, Sobrinho LG, et al. Expression of PAX8-PPAR gamma 1 rearrangements in both follicular thyroid carcinomas and adenomas. J Clin Endocrinol Metab. 2002;87(8):3947–52.
Motomura T, Nikiforov YE, Namba H, Ashizawa K, Nagataki S, Yamashita S, et al. Ret rearrangements in Japanese pediatric and adult papillary thyroid cancers. Thyroid. 1998;8(6):485–9.
Mulligan LM, Eng C, Healey CS, Clayton D, Kwok JB, Gardner E, et al. Specific mutations of the RET proto-oncogene are related to disease phenotype in MEN 2A and FMTC. Nat Genet. 1994;6(1):70–4.
Nikiforov M, Biddinger PW, Caudill CM, Kroll TG, Nikiforov YE. PAX8-PPAR g rearrangement in thyroid tumors: RT-PCR and immunohistochemical analysis. Am J Surg Pathol. 2002;26(8):1016–23.
Nikiforov YE. Molecular analysis of thyroid tumors. Mod Pathol. 2011;24(Suppl 2):S34–43.
Nikiforov YE. RET/PTC rearrangement in thyroid tumors. Endocr Pathol. 2002;13(1):3–16.
Nikiforov YE. Thyroid carcinoma: molecular pathways and therapeutic targets. Mod Pathol. 2008;21(Suppl 2):S37–43.
Nikiforov YE, Steward DL, Robinson-Smith TM, Haugen BR, Klopper JP, Zhu Z, et al. Molecular testing for mutations in improving the fine-needle aspiration diagnosis of thyroid nodules. J Clin Endocrinol Metab. 2009;94(6):2092–8.
Nikiforova MN, Caudill CM, Biddinger P, Nikiforov YE. Prevalence of RET/PTC rearrangements in Hashimoto’s thyroiditis and papillary thyroid carcinomas. Int J Surg Pathol. 2002;10(1):15–22.
Papotti M, Volante M, Giuliano A, Fassina A, Fusco A, Bussolati G, et al. RET/PTC activation in hyalinizing trabecular tumors of the thyroid. Am J Surg Pathol. 2000;24(12):1615–21.
Williams GH, Rooney S, Thomas GA, Cummins G, Williams ED. RET activation in adult and childhood papillary thyroid carcinoma using a reverse transcriptase-n-polymerase chain reaction approach on archival-nested material. Br J Cancer. 1996;74(4):585–9.
Wirtschafter A, et al. Expression of the RET/PTC fusion gene as a marker for papillary carcinoma in Hashimoto’s thyroiditis. Laryngoscope. 1997;107(1):95–100.
Xing M. BRAF mutation in thyroid cancer. Endocr Relat Cancer. 2005;12(2):245–62.
Xing M, Tufano RP, Tufaro AP, Basaria S, Ewertz M, Rosenbaum E, et al. Detection of BRAF mutation on fine needle aspiration biopsy specimens: a new diagnostic tool for papillary thyroid cancer. J Clin Endocrinol Metab. 2004;89(6):2867–72.
Author information
Authors and Affiliations
Rights and permissions
Copyright information
© 2018 Springer International Publishing AG
About this chapter
Cite this chapter
Lin, F., Liu, H., Zhang, J. (2018). Thyroid and Parathyroid Glands. In: Handbook of Practical Fine Needle Aspiration and Small Tissue Biopsies. Springer, Cham. https://doi.org/10.1007/978-3-319-57386-1_3
Download citation
DOI: https://doi.org/10.1007/978-3-319-57386-1_3
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-319-57384-7
Online ISBN: 978-3-319-57386-1
eBook Packages: MedicineMedicine (R0)