
Abstract
Fine needle aspiration (FNA) biopsies with cellblock preparation or small tissue biopsies have become a primary modality to achieve a definitive diagnosis of a mass-like lesion of the superficial and deep-seated organs. This chapter (1) provided an overview of application of FNA; (2) delineated fundamental approach to an FNA sample; (3) summarized major and minor cytological criteria for some common entities encountered in daily practice; (4) illustrated some of the most effective yet small diagnostic IHC panels for tumor of unknown primary/undifferentiated neoplasm; (5) described some chromosomal translocations which are highly specific for certain solid tumors; and (6) highlighted the most frequently used molecular techniques on FNA and small tissue biopsy specimens.
Access provided by CONRICYT-eBooks. Download chapter PDF
Similar content being viewed by others



Keywords
- Sensitivity
- Specificity
- Spindle cells
- Epithelioid cells
- Small round cells
- Giant cells
- Intranuclear inclusion
- Nuclear grooves
- Parotid gland
- Benign mixed tumor
- Adenoid cystic carcinoma
- Liver
- Hepatocellular carcinoma
- Ductal carcinoma
- Pancreas
- Breast
- Lobular carcinoma
- Adenocarcinoma
- Lung
- Squamous cell carcinoma
- Renal cell carcinoma
- Hodgkin’s lymphoma
- Lymphoma
- Sarcoma
- Melanoma
- Germ cell tumor
- Mesothelioma
- Langerhans cell histiocytosis
- Granular cell tumor
- Papillary thyroid carcinoma
- Thyroid medullary carcinoma
- Colloid carcinoma
- Oncocytoma
- Acinar cell carcinoma
- Neuroendocrine tumor
- Small-cell carcinoma
- Merkel cell carcinoma
- Fine-needle aspiration biopsy
- In-situ hybridization
- Polymerase chain reaction
- Reverse transcription-polymerase chain reaction (RT-PCR )
- Southern blotting
- Gene microarrays
- Genomics
- HER2/neu for gene amplification in breast and gastric cancer
- Detection of clonality in hematopoietic neoplasms
- Specific chromosomal translocations
- CK7
- CK20
- AE1/3
- CAM5.2
- EMA
- Vimenti n
- MOC31
- BerEP4
- CEA
- Calretini n
- WT-1
- CK5/6
- D2-40
- p40
- p63
- S100
- CD10
- Napsin A
- ER
- GATA3
- PAX8
- CDX2
- SATB2
- PSA
- NKX3.1
- P504S
- PSAP
- pVHL
- RCC
- Chromograni n
- SOX10
- Mart-1
- HMB45
- SALL4
- OCT4
- CD30
- Glypican-3
- CD117
- NKX2.2
- STAT6
- CD99
- Myogenin
- MyoD1
- Desmin
- SMA
Indications for Fine Needle Aspiration (FNA) Biopsy
-
Mass lesion with a clinical suspicion of malignant tumor – palpable or deep-seated
-
Infections – virus, fungus
-
Granulomatous inflammation
-
Infiltration – amyloidosis
Complications of FNA
-
Pain
-
Bleeding
-
Faintness
-
Hematoma
-
Pneumothorax
-
Seeding of tumor cells
Advantages of FNA
-
FNA is SAFE.
-
Simple
-
Accurate
-
Fast
-
Economic
-
Primary Applications of FNA
-
Primary diagnosis of a malignant tumor.
-
Confirm a reactive/benign condition.
-
Metastatic tumor of unknown primary.
-
Deep-seated organ/tumor.
-
Confirm a recurrent tumor .
Target Organs of FNA
Superficial Organs
-
Thyroid
-
Lymph node
-
Salivary gland
-
Soft tissue
-
Breast
Deep-Seated Organs
-
Liver
-
Pancreas
-
Lung/mediastinum
-
Kidney/adrenal
-
Retroperitoneum
Sensitivity and Specificity of FNA (Table 1.1)
How to Perform an FNA
Supplies
-
23- or 25-gauge, 1.0-inch or 1.5-inch needle
-
Syringes – 10 mL
-
Syringe holder (Fig. 1.1)
Fig. 1.1 
Showing an aspiration gun (Cameco AB, Tägy, Sweden)

Procedure
-
Stabilize the target lesion.
-
Pass needle through the skin and advance into the lesion.
-
Apply suction.
-
Move the needle back and forth for 10 s.
-
Release suction.
-
Remove the needle from patient.
-
Detach the needle from the syringe.
-
Fill the syringe with air and replace needle on syringe.
-
Express the specimen onto microscopic slides.
-
Prepare air-dried and fixed smears .
How to Interpret an FNA
Overall Cellularity
-
High – lymphoma , melanoma , neuroendocrine tumor (NET ) (Fig. 1.2)
Fig. 1.2 
Hypercellularity in melanoma
-
Low – lobular carcinoma , schwannoma (Fig. 1.3)
Fig. 1.3 
Low cellularity in breast lobular carcinoma


Cellular Architectures
-
Papillary (Fig. 1.4)
Fig. 1.4 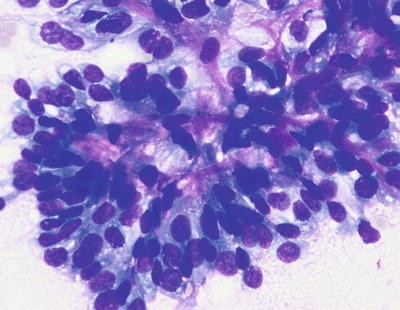
Papillary structure in papillary RCC
-
Tightly cohesive groups (Fig. 1.5)
Fig. 1.5 
Cohesive cellular group in medullary carcinoma of the breast
-
Loosely cohesive groups (Fig. 1.6)
Fig. 1.6 
Loosely cohesive group in breast carcinoma
-
Acinar (Fig. 1.7)
Fig. 1.7 
Acinar formation in acinar cell carcinoma of the pancreas
-
Glandular (Fig. 1.8)
Fig. 1.8 
Glandular formation in colonic ADC





Cell Shapes
-
Epithelial (Fig. 1.9)
Fig. 1.9 
Epithelial cells in well-differentiated ADC of the pancreas
-
Epithelioid (Fig. 1.10)
Fig. 1.10 
Epithelioid cells in melanoma
-
Spindle (Fig. 1.11)
Fig. 1.11 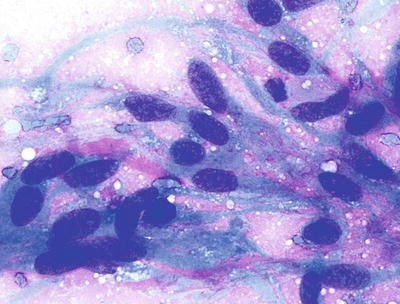
Spindle cell in gastrointestinal stromal tumor
-
Bizarre
-
Small round cell (Fig. 1.12)
Fig. 1.12 
Small blue cell in Ewing’s sarcoma
-
Giant cell (Fig. 1.13)
Fig. 1.13 
Giant tumor cells in rhabdomyosarcoma on Diff-Quik (DQ)





Naked Nuclei
-
Hepatocellular carcinoma (HCC) (Fig. 1.14)
Fig. 1.14 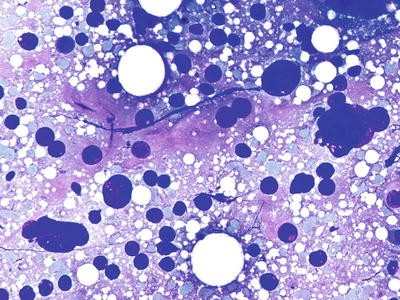
Naked nuclei in HCC
-
Acinar cell carcinoma
-
Granular cell tumor
-
Lactating adenoma
-
Fibroadenoma

Nuclear Details
-
Intranuclear inclusion – melanoma (Fig. 1.15), renal cell carcinoma (RCC ), papillary thyroid carcinoma , HCC, and paraganglioma
Fig. 1.15 
Intranuclear inclusion in a melanoma
-
Nuclear grooves – papillary thyroid carcinoma , adult granulosa cell tumor, histiocytosis X (Fig. 1.16), solid-pseudopapillary tumor of pancreas
Fig. 1.16 
Nuclear grooves in Langerhans cell histiocytosis
-
Anisonucleosis – high-grade neoplasms (Figs. 1.17 and 1.18)
Fig. 1.17 
Nuclear pleomorphism in a melanoma
Fig. 1.18 
Anaplastic carcinoma of the thyroid with marked nuclear pleomorphism
-
Nuclear chromatin clearing – pancreatic carcinoma
-
Prominent nucleoli – melanoma , high-grade lymphoma, HCC, high-grade RCC , adenocarcinoma (ADC) , and sarcoma




Cytoplasm
-
Clear – clear cell RCC (Fig. 1.19), clear cell carcinoma of the ovary and the uterus, melanoma , ADC with clear cell changes (such as pancreas), and squamous cell carcinoma (SCC) with clear cell changes
Fig. 1.19 
Clear cytoplasm in a clear cell RCC
-
Granular – oncocytoma (Fig. 1.20), HCC, granular cell tumor (Fig. 1.21), high-grade RCC , medullary carcinoma of the thyroid, and other NETs/carcinomas
Fig. 1.20 
Oncocytic cytoplasm in an oncocytoma
Fig. 1.21 
Coarse, granular cytoplasm in a granular cell tumor
-
Foamy – RCC , carcinoma of the breast, lung, and pancreas, melanoma
-
Squamoid/dense – SCC (Figs. 1.22 and 1.23) , papillary thyroid carcinoma , carcinoma of the lung and pancreas, and high-grade mucoepidermoid carcinoma
Fig. 1.22 
Squamous tumor cell in a SCC on DQ
Fig. 1.23 
Keratinizing squamous tumor cell in an SCC on Papanicolaou (Pap) stain
-
Intracytoplasmic lumen – lobular carcinoma and low-grade ductal carcinoma of the breast (Fig. 1.24), signet-ring cell carcinoma, and melanoma
Fig. 1.24 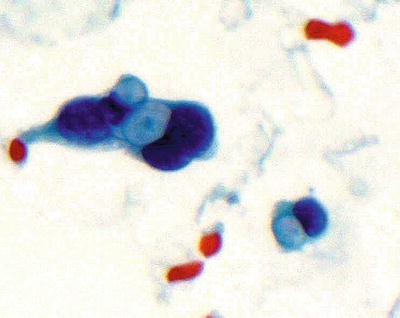
Intracytoplasmic lumen in a breast lobular carcinoma






Background Material
-
Abundant mucin – colloid carcinoma of breast and pancreas (Figs. 1.25 and 1.26) and mucoepidermoid carcinoma
Fig. 1.25 
Mucinous background in a colloid carcinoma of the breast on DQ
Fig. 1.26 
Mucinous background in a colloid carcinoma of the breast on Pap stain
-
Abundant colloid – thyroid nodular goiter
-
Myxoid/chondroid – benign mixed tumor , chondrosarcoma, and myxoid and chondroid neoplasms (Figs. 1.27 and 1.28)
Fig. 1.27 
Chondroid background in a chodorma on DQ
Fig. 1.28 
Chondroid background in a chodorma on Pap stain
-
Amyloid – medullary carcinoma of the thyroid, NET , and endocrine tumor of the pancreas
-
Necrosis – colorectal ADC, small-cell undifferentiated carcinoma, lymphoma , and high-grade carcinoma or sarcoma
-
Crushed artifact – small blue cell tumor, lymphoma , and lymphoid tissue
-
Acute inflammation – infection, inflammatory process, anaplastic carcinoma of the thyroid, anaplastic large-cell lymphoma, and SCC with cystic degeneration




Single Cell Population
-
NET (Figs. 1.29)
Fig. 1.29 
Single cell population in a carcinoid tumor of lung on DQ
-
Lymphoma /plasmacytoma/myeloid sarcoma (Fig. 1.30)
Fig. 1.30 
Single cell population in a plasmacytoma on Pap stain
-
Melanoma
-
Sarcoma


Two Populations of Cells


How to Report an FNA
Category
-
1.
Positive for malignant cells/malignant
-
2.
Suspicious for malignant cells
-
3.
Atypical cytology/atypical cells of undetermined significance
-
4.
Negative for malignant cells/benign
-
5.
Indeterminate
Specimen Adequacy
-
1.
Adequate/satisfactory
-
2.
Inadequate/unsatisfactory
-
3.
Suboptimal/limited
An Example of a Formal Report of an FNA of the Thyroid
-
Thyroid, right, FNA
-
Positive for malignant cells
-
Papillary thyroid carcinoma
-
Adequately cellular specimen
Comment: Tall cell variant of papillary carcinoma of the thyroid is suspected.
Cytological Criteria of Common Neoplasms
-
1.
Papillary Carcinoma of Thyroid
-
Major Criteria (Fig. 1.33)
-
Nuclear enlargement
-
Nuclear overlapping
-
Nuclear clearing
-
Nuclear grooving
-
Intranuclear inclusion
Fig. 1.33 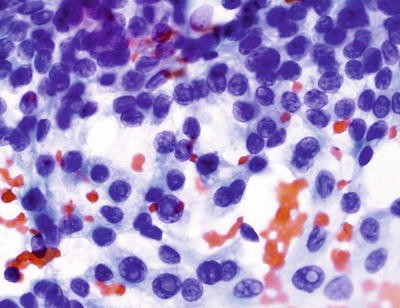
Classic nuclear changes in a papillary carcinoma of the thyroid on Pap stain
-
-
Minor Criteria
-
Squamoid cytoplasm
-
Cytoplasmic vacuoles
-
Psammoma body
-
Thick colloid
-
Multinucleated giant cells
-
-

-
2.
Medullary Carcinoma of the Thyroid
-
Major Criteria (Fig. 1.34)
-
Two populations of cells, epithelioid and spindle cells
-
Salt-pepper chromatin
-
Small to inconspicuous nucleoli
-
Plasmacytoid features
Fig. 1.34 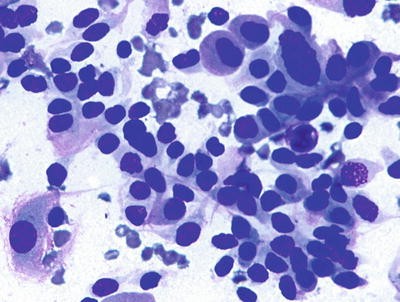
Classic cytological features for a medullary carcinoma of the thyroid on DQ
-
-
Minor Criteria
-
Intranuclear inclusion
-
Granular and dense cytoplasm
-
Amyloid
-
Hyaline globules
-
-
-
3.
Adenoid Cystic Carcinoma of Salivary Gland
-
Major Criteria (Fig. 1.35)
-
Small uniform, basaloid cells with high nuclear-to-cytoplasmic ratio, bland nuclei, but hyperchromatic chromatin
-
Hyaline globules
Fig. 1.35 
Diagnostic hyalinizing globules in an adenoid cystic carcinoma on DQ
-
-
Minor Criteria
-
Usually absence of myoepithelial cells
-
Few stromal fragments
-
Exclude other entities
-
-
-
4.
Benign Mixed Tumor of the Salivary Gland
-
Major Criteria (Fig. 1.36)
-
Epithelial cells
-
Stromal cells
-
Metachromatic stroma
-
Spindle stromal cells
-
Plasmacytoid myoepithelial cells
Fig. 1.36 
Showing an example of benign mixed tumor on DQ
-
-
Minor Criteria
-
Epithelial cell dominant
-
Stromal cell dominant
-
Stromal acellular component dominant
-
Myoepithelial cell dominant
-
Extensive squamous metaplasia
-
-
-
5.
ADC of the Pancreas
-
Major Criteria (Fig. 1.37)
-
Variation in nuclear size in the same group (1:4)
-
Nuclear enlargement (>2 red blood cells [RBCs])
-
Nuclear overlapping/three dimensionality
-
Nuclear membranous irregularity
Fig. 1.37 
Showing an example of well-diff ADC of the pancreas on Pap stain
-
-
Minor Criteria
-
Single atypical cells
-
Tumor necrosis
-
Prominent nucleoli
-
Mitosis
-
Chromatin clearing
-
Giant tumor cells
-
Hyperchromatic nuclei
-
-
-
6.
NET of the Pancreas
-
Major Criteria (Fig. 1.38)
-
A mixture of small cohesive groups and single cells
-
Round nuclei with salt-pepper nuclear chromatin
-
Small nucleoli
-
Plasmacytoid features
-
Binucleation
Fig. 1.38 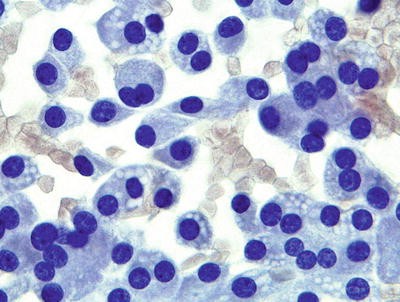
Showing an example of pancreatic NET
-
-
Minor Criteria
-
Occasional large atypical cells
-
Crushed artifact
-
Focal necrosis
-
Multinucleated giant cells
-
Granular cytoplasm
-
Striped nuclei
-
-
-
7.
HCC
-
Major Criteria (Fig. 1.39)
-
Trabecular fragment >3 cells thick and wrapped by endothelial cells or pseudoglandular formation with production of bile
-
Special stain for reticulin and an immunostain for cluster of differentiation (CD)34 performed on the cell block section or core biopsy are useful
Fig. 1.39 
Showing an example of HCC producing bile on Pap stain
-
-
Minor Criteria
-
Hypercellularity
-
Many single cells
-
Naked nuclei
-
High nuclear-to-cytoplasmic ratio
-
Few ductal cells
-
-
-
8.
Ductal Carcinoma of the Breast
-
Major Criteria (Fig. 1.40)
-
Hypercellularity
-
Nuclear enlargement (>2.5 RBCs)
-
Disordered, loosely cohesive epithelial group
-
Single atypical cells
-
Nuclear chromatin changes
Fig. 1.40 
Showing an example of breast ductal carcinoma on Pap stain
Minor Criteria
-
Marked nuclear atypia
-
Tumor necrosis
-
Mitosis
-
Prominent nucleoli
-
Intracytoplasmic lumens
-
Foamy cytoplasm
-
-
-
9.
Small-Cell Carcinoma of the Lung
-
Major Criteria (Figs. 1.41 and 1.42 )
-
Pleomorphic nuclei with salt-and-pepper nuclear chromatin
-
Very high nuclear-to-cytoplasmic ratio
-
Single cell necrosis and mitosis
-
Inconspicuous nucleoli
Fig. 1.41 
Showing an example of small-cell carcinoma of the lung on DQ
Fig. 1.42 
Showing nuclear molding in a small-cell carcinoma on DQ
-
-
Minor Criteria
-
Crushed artifact
-
Hypercellularity
-
Many single cells
-
Blue body
-
Nuclear molding
-
Extensive necrosis
-
Marked atypical cells
-
-
-
10.
ADC of the Lung
-
Major Criteria
-
Three dimensional groups
-
Glandular, tubular, acinar, or papillary formation
-
Nuclear enlargement
-
Chromatin clearing and clumping
-
Irregular nuclear membrane
-
Prominent nucleoli
-
Mucinous material in the background
-
-
Minor Criteria
-
Single atypical cells with plasmacytoid features
-
Mitosis
-
Vacuoles in cytoplasm
-
-
-
11.
SCC of the Lung
-
Major Criteria (Fig. 1.43 )
-
Two or three dimensional groups
-
Keratinization
-
Single atypical cells with dense cytoplasm
-
Nuclear enlargement
-
Small nucleoli
-
Irregular nuclear membrane
-
No glandular, tubular, acinar, or papillary formation
-
Mucinous material in the background
Fig. 1.43 
Showing an example of well-differentiated SCC of the lung on Pap stain
-
-
Minor Criteria
-
Tumor necrosis
-
Mitosis
-
Marked pleomorphic cells
-
Bizarre cell sharps
-
-
-
12.
Melanoma
-
Major Criteria (Fig. 1.44)
-
Large epithelioid cells
-
Abundant cytoplasm
-
Large nuclei
-
Prominent nucleoli
-
Binucleation
-
Intranuclear inclusion
Fig. 1.44 
Showing an example of melanoma with clear cytoplasm on Pap stain
-
-
Minor Criteria
-
Two populations of cells – epithelioid and spindle
-
Plasmacytoid appearance
-
Marked pleomorphic cells
-
Pigments
-
-
-
13.
Clear Cell RCC
-
Major Criteria (Fig. 1.45)
-
Clusters of tumor cells with vascular-rich network
-
Low nuclear-to-cytoplasmic ratio
-
Clear or granular cytoplasm
-
Small to prominent nucleoli
-
Intranuclear inclusion
Fig. 1.45 
Showing an example of clear cell RCC on Pap stain
-
-
Minor Criteria
-
Naked nuclei
-
Mixed neutrophils, RBCs, and pigment-laden histiocytes with tumor cells
-
-
-
14.
Non-Hodgkin’s Lymphomas
-
Major Criteria (Fig. 1.46)
-
Uniform population of lymphoid cells
-
Classified into small, medium, and large cell size using histiocytes as a reference
-
Lymphoglandular body
Fig. 1.46 
Showing an example of lymphoblastic lymphoma on DQ
-
-
Minor Criteria
-
Cleaved or noncleaved nuclei
-
Fine granular chromatin
-
Many mitoses
-
Single cell or extensive necrosis
-
Prominent nucleoli
-
Cytoplasmic vacuoles
-
-
-
15.
Hodgkin’s Lymphoma
-
Major Criteria (Fig. 1.47)
-
Reed-Sternberg cells
-
Hodgkin’s cells
-
Mixed population of small lymphoid cells, histiocytes, plasma cells, and eosinophils in the background
Fig. 1.47 
Showing an example of Hodgkin lymphoma with Reed-Sternberg cells on DQ
-
-
Minor Criteria
-
Granulomas
-
Fibrosis
-
Necrosis
-
-














Diagnosis of lymphomas should not solely rely on cytological features; instead, it should include (1) cytomorphology, (2) immunohistochemistry (IHC), (3) flow cytometry, and (4) FISH/molecular diagnosis.
Ancillary Studies
IHC
In this section, the focus will be on the application of IHC to undifferentiated neoplasms if a cell block or a small tissue biopsy sample is available, especially carcinoma of unknown origin. The utilities of IHC on other specific entities on each organ will be delineated in each organ-based chapter.
How to Approach Undifferentiated Neoplasms /Tumors of Uncertain Origin
-
Review hematoxylin- and eosin (H&E)-stained slides .
Morphologic features are fundamental. The very first step is to determine if the lesion is malignant. If a benign/reactive condition is included in the differential diagnosis, caution should be taken when applying any immunostains, since IHC may or may not contribute to this process or may lead one to come to the wrong conclusion. If the lesion is malignant, it is important to review the slides and generate a broad differential diagnosis based on the morphologic features alone. One can be misled by incomplete or inaccurate clinical information .
-
Consider the basic clinical information such as age, sex, tumor location, and prior malignancy.
After formulating the initial differential diagnostic categories, it is time to consider the patient’s age, sex, tumor location, and any prior malignancy. One should follow the statistics and focus on the common entities in that particular age group of patients and tumor location. Jumping to a conclusion of an uncommon entity in the initial diagnostic workup is not a wise choice .
-
Re-evaluate morphologic features of the tumor and predict the most likely category, such as carcinoma, melanoma , sarcoma , lymphoma , or germ cell tumor .
Based on the patient’s age, sex, tumor location, prior malignancy, and morphologic features, one should narrow down the initial differential diagnosis to one to three options, if possible. For example: Is this a carcinoma? Is this an ADC? If it is an ADC, what is the likely primary site? Based on the tumor morphology, patient’s age, and tumor location, the literature demonstrated that pathologists were able to correctly identify the tumor origin as their first choice in 50–55% of cases or as their first, second, or third choice in 67–74% of cases .
-
Determine the first diagnostic IHC panel to order .
There are two likely scenarios. In the first, there is a clear lineage differentiation, such as an ADC/carcinoma. The next question will be: What is the likely primary site? A broad-spectrum cytokeratin cocktail (AE1/3 and CAM5.2 ), cytokeratin (CK)7, CK20 , plus relatively organ-specific markers are recommended .
Determination of a Broad Category of Neoplasm
A cocktail of AE1/AE3 and CAM 5.2 is an effective panel of markers for identifying an epithelial lineage. AE1/AE3 by itself is insufficient to exclude an epithelial lineage. Other broad-spectrum cytokeratins containing keratin 8 and keratin 18, such as clones KL1, OSCAR, MAK6, and 5D3/LP3, are also excellent choices as a screening cytokeratin.
Leukocyte common antigen (LCA) itself is insufficient to exclude a potential diagnosis of hematopoietic neoplasm. Some diffuse large B-cell lymphomas, plasmablastic lymphomas, and anaplastic lymphomas can be negative for LCA. A combination of LCA and CD43 will cover a broad spectrum of lymphomas/myeloid sarcomas .
Vimentin is a non-specific marker; however, a vimentin-negative tumor is unlikely to be a sarcoma (with the exception of alveolar soft part sarcoma), lymphoma, or melanoma . Some carcinomas frequently co-express vimentin. A combination of S100 and sex-determining region Y-box (SOX)10 will detect nearly 100% of melanomas and greater than 80% of spindle cell /desmoplastic melanomas.
Sal-like protein 4 (SALL4 ) and lin-28 homolog A (LIN28) are highly sensitive and specific markers for identifying a tumor of germ cell origin. The markers for determination of a broad category of neoplasms are summarized in Table 1.2.
Tissue-Specific Markers
No single antibody is absolutely sensitive and specific for a particular tumor; however, some are especially useful when used in a small panel. Frequently used tissue-specific biomarkers are summarized in Table 1.3.
Co-expression of Cytokeratin and Vimentin
Follicular, papillary, and medullary thyroid carcinomas are nearly 100% positive for vimentin. Metaplastic breast carcinoma usually expresses both cytokeratin and vimentin in addition to high molecular weight cytokeratins and myoepithelial markers. Alveolar soft part sarcoma is a rare sarcoma which has no immunoreactivity for vimentin. Tumors that express both cytokeratin and vimentin are described in Table 1.4.
Expression of Epithelial Markers in Non-epithelial Neoplasms
Expression of cytokeratin is not restricted to epithelial neoplasms. Keratin is commonly expressed in some tumors with evidence of epithelial differentiation, such as synovial sarcomas, epithelioid sarcomas, desmoplastic small round cell tumors, chordomas, adamantinoma, and myoepithelial carcinomas. Other mesenchymal tumors can also express cytokeratin, although with a low frequency, including angiosarcomas, epithelioid hemangioendotheliomas, epithelioid leiomyosarcomas, and meningiomas. Aberrant expression of cytokeratin, which tends to be focal, has been reported in other tumors, including undifferentiated pleomorphic sarcomas, rhabdomyosarcomas, malignant rhabdoid tumors, and peripheral nerve sheath tumors, clear cell sarcomas, plasmacytomas, diffuse large B-cell lymphomas, anaplastic large-cell lymphomas, and melanomas .
Expression of Hematopoietic Markers in Non-hematopoietic Neoplasms
CD5 has been reported in thymic carcinoma, breast carcinoma, colonic ADC, pancreatic ADC, and lung ADC. CD138 is also frequently positive in SCC and can be positive in breast carcinoma, ovarian carcinoma, adrenal cortical carcinoma, and RCC .
CD56 is the most sensitive but not an entirely specific marker for neuroendocrine neoplasms, including some small-cell carcinomas which may lose expression of cytokeratins and other neuroendocrine markers but still show expression of CD56. A significant percentage of thyroid carcinomas are immunoreactive for CD56 as well, as reported in the literature. Hematopoietic markers expressed in non-hematopoietic neoplasms are listed in Table 1.5.
Review of Selected Antibodies
The following selected antibodies are either recently described or frequently used in identifying a tumor of uncertain origin/undifferentiated neoplasm, especially a carcinoma. As well documented, every antigen can demonstrate an aberrant expression in a certain tumor. Table 1.6 summarizes the common application of these antibodies. The antibody information for the frequently used antibodies is summarized in Table 1.7.
Recommended Diagnostic IHC Panels
As aforementioned, this section will focus on carcinomas of uncertain origin, which can be separated into four main diagnostic groups: CK7 +/CK20 -, CK7+/CK20+, CK7-/CK20+, and CK7-/CK20-.
-
Differential diagnosis of CK7 + and CK7+/focal CK20 + carcinomas .
When working on a tumor of unknown primary, CK7 + or CK7+/CK20 + carcinomas are nearly always included in the diagnostic consideration. The differential diagnosis usually encompasses a broad spectrum of organs and entities, such as the breast, lung, ovary, uterus, urinary bladder, upper GI tract, pancreatobiliary tract, thyroid, kidney (papillary RCC ), and mesothelioma. Table 1.8 summarizes the frequently used markers in the differential diagnosis of these common entities. A significant portion of these CK7+ carcinomas also express ER , and the major differential diagnosis of CK7+/ER+ carcinomas, including tumors from the breast and gynecologic tract, is summarized in Table 1.9.
Table 1.8 Summary of CK7 + and CK7+/CK20 + epithelial neoplasms Table 1.9 Summary of CK7 +/ER + carcinomas and useful markers In real practice, each individual case will have a unique presentation; therefore, it is impractical and impossible to create a specific IHC panel for every diagnostically challenging case here. However, a few potentially useful IHC panels are recommended in Tables 1.10, 1.11, 1.12, 1.13, 1.14, and 1.15.
Table 1.10 Lung ADC vs. breast carcinoma Table 1.11 Lung ADC vs. mesothelioma Table 1.12 Lung vs. upper GI, pancreatobiliary primary, and urinary bladder Table 1.13 Breast carcinoma vs. upper GI, pancreatobiliary primary, and urinary bladder Table 1.14 Lung ADC vs. gynecologic primaries Table 1.15 PRCC vs. UC vs. CDC vs. PADC Caution should be taken when using a polyclonal antibody to napsin A . A significant percentage of esophageal ADCs and some pancreatic ADCs can be positive for napsin A . Less than 10% of pancreatic ADCs may show focal positivity for GATA3 .
In addition to the entities mentioned in Tables 1.9, 1.10, 1.11, 1.12, 1.13, and 1.14, many other entities can present as CK7 + or CK7+/focally CK20 + carcinomas, including anal/rectal ADCs, ampullary ADCs, common bile duct ADCs, gallbladder ADCs, small bowel ADCs, renal collecting duct carcinomas, renal medullary carcinomas, medullary thyroid carcinomas, thymic carcinomas, salivary gland carcinomas, ovarian mucinous carcinoma, and SCCs of the uterine cervix.
-
Differential diagnosis of CK7 +/ER + carcinomas .
ER is one of the most critical immunomarkers when working on a tumor of uncertain origin or undifferentiated neoplasm, especially in a woman. ER is frequently positive in breast carcinomas and gynecologic primaries. Therefore, ER itself plays a limited role in differential diagnosis among these carcinomas. Table 1.9 includes the most common ER-positive carcinomas when working on a tumor of uncertain origin. GATA3 and TFF1 are two recently described sensitive markers for identifying a breast origin, which is rarely positive in other gynecologic carcinomas, including endometrial ADCs, endocervical ADCs, ovarian serous carcinomas, and clear cell carcinomas. TFF1 is expressed in 80% and 90% of breast and colorectal carcinomas, respectively, whereas other carcinomas, including those of the lung, endometrium, and ovary, are rarely positive. Vimentin is expressed in 90% of endometrial ADCs and negative in other gynecologic carcinomas, with the exception in ovarian endometrioid ADCs, which showed immunoreactivity for vimentin in over 90% of cases. p16 is a useful marker in distinguishing between endometrial ADC and endocervical ADC; it tends to be diffusely and strongly positive in endocervical ADC (nearly every tumor cell) with only patchy immunoreactivity in endometrial ADC. Human papilloma virus (HPV) in situ hybridization (ISH) demonstrated positivity in the majority of endocervical ADCs. pVHL and hepatocyte nuclear factor 1 beta (HNF-1B) are helpful markers in distinguishing ovarian serous carcinoma from ovarian clear cell carcinoma. Additionally, p53 is usually diffusely and strongly positive or completely negative in serous carcinomas and only focally and weakly positive in ovarian clear cell carcinomas. KIM-1, which is not currently commercially available, is a sensitive and relatively specific marker for ovarian and uterine clear cell carcinomas; pVHL plays a similar role. No reliable immunomarkers are available for differentiating a uterine serous carcinoma from an ovarian serous carcinoma .
-
Differential diagnosis of CK20 +/CK7 - carcinomas .
Predominately CK20 + carcinomas include colorectal ADC (CRADC), small intestinal ADC (SADC), bladder ADC (BADC), appendiceal ADC (APADC), Merkel cell carcinoma , and salivary gland small-cell carcinoma. Perinuclear dot-staining patterns are seen in both Merkel cell carcinoma and salivary gland small-cell carcinoma. Merkel cell polyomavirus (MCPyV) was detected in approximately 80% of Merkel cell carcinomas but not in other high-grade neuroendocrine carcinomas, including salivary gland small-cell carcinomas; therefore, MCPyV is a potentially sensitive and highly specific marker for identification of Merkel cell carcinoma of the skin. CK20+ carcinomas and useful markers are summarized in Table 1.16.
Table 1.16 Summary of CK20 + carcinomas and useful markers -
Differential diagnosis of CK7 −/CK20 - carcinomas .
The following neoplasms usually present as CK7 −/CK20 - carcinomas, and some relatively tissue-specific markers may be helpful in reaching a definitive diagnosis. These tumors include but are not limited to (1) medullary carcinomas of the colon, (2) some neuroendocrine neoplasms, (3) clear cell RCCs, (4) HCCs, (5) adrenal cortical neoplasm/carcinomas, (6) germ cell tumors , (7) prostatic ADCs, and (8) SCCs. A subset of small-cell carcinomas of the lung, gastric ADCs, esophageal ADCs, and mesotheliomas can be CK7−/CK20-.
Medullary carcinoma of the colon frequently shows loss of microsatellite instability (MSI) markers, especially MutL homolog 1 (MLH1) and postmeiotic segregation increased 2 (PMS2), and is commonly positive for CDH17, SATB2 , calretinin, trefoil factor (TFF)3, and mucin 4 (MUC4). CDX2 expression tends to be weak and focal. Focal positivity (<25% of the tumor cells stained) for neuroendocrine markers such as synaptophysin can be seen. Approximately 70% of medullary carcinomas of the large bowel can be positive for calretinin .
Neuroendocrine neoplasms/carcinomas are positive for chromogranin , synaptophysin, and CD56. Chromogranin is expressed in well to moderately differentiated neuroendocrine neoplasms/carcinomas and tends to be only focally positive in poorly differentiated neuroendocrine carcinomas/small-cell carcinomas. CD56 is a highly sensitive marker for small-cell carcinoma; however, its expression is only seen in approximately 50% of pancreatic NETs. Additionally, CD56 can be positive in non-neuroendocrine carcinomas. More recently, preliminary studies showed that approximately 50% of pancreatic NETs showed loss of expression of anti-ATRX or anti-DAXX. The expression of ATRX/DAXX is usually present in NETs from other organs . To differentiate the tissue origin of a given neuroendocrine neoplasm/carcinoma, the following markers are useful and are summarized in Table 1.17.
Table 1.17 Markers for NETs Germ cell tumors are frequently negative for CK7 and CK20 . SALL4 and LIN28 are excellent screening markers for germ cell tumors , which are positive in nearly 100% of seminomas, embryonal carcinomas, and yolk sac tumors, 70% of choriocarcinomas, and 50% of teratomas. D2-40 and CD117 are specific markers for seminoma; AFP and glypican-3 are specific markers for yolk sac tumors; SOX2, NANOG, and CD30 are relatively specific markers for embryonal carcinomas, although NANOG is also positive in seminomas and SOX2 may be positive in yolk sac tumors; and CD10 and beta-human chorionic gonadotropin (B-HCG) are specific markers for choriocarcinomas. GATA3 are frequently positive in choriocarcinomas and yolk sac tumors. The useful markers are summarized in Table 1.18.
Table 1.18 Markers for germ cell tumors Over 90% of clear cell RCCs are negative for both CK7 and CK20 . Co-expression of cytokeratin/vimentin is one of the important features for clear cell RCC . Five markers (PAX8 , pVHL , RCCma, CD10 , and KIM-1) are helpful in confirming the diagnosis of clear cell RCC. PAX8 is likely the most sensitive marker among these five markers; however, it also expresses in tumors from the thyroid, gynecologic tract, thymus, and others. RCCma has a low sensitivity of approximately 50% in detecting a high-grade clear cell RCC. Both pVHL and KIM-1 are also expressed in clear cell carcinomas of the uterus and ovary; however, KIM-1 is not commercially available yet. CD10 is a highly sensitive but not very specific marker for clear cell RCC. In general, a small panel of antibodies consisting of CAM5.2 , vimentin, PAX8, pVHL, and RCCma can serve as an initial panel to confirm a metastatic clear cell RCC. When it comes to a sarcomatoid RCC, an extended panel of antibodies including cytokeratins, vimentin, PAX8, pVHL, RCCma, CD10, KIM-1, and alpha-methylacyl-CoA racemase (P504S ) is recommended to increase the diagnostic sensitivity .
A majority of HCCs are negative for CK7 and CK20 , with the exception of fibrolamellar HCC, which is usually CK7+/CK20-. Approximately 10% of HCCs may show positive staining for both CK7 and CK20. AE1/AE3 is only positive in approximately 30% of HCCs, whereas over 90% of HCCs are positive for CAM5.2 which contains keratin 8. Other cytokeratins such as 5D3, 5D3/LP34, and KL1 (containing both keratins 8 and 18) are good screening markers for HCC. Many markers are useful for identifying HCC, including arginase-1, glypican-3 , HepPar-1, CD10 , and polyclonal carcinoembryonic antigen (CEA ). Arginase-1 is the most sensitive and specific marker for HCC, including poorly differentiated HCC, whereas HepPar-1 is a sensitive but not very specific marker for HCC since its immunoreactivity has been reported in many other carcinomas. The diagnostic sensitivity of both arginase-1 and HepPar-1 for identifying liver cell origin is over 90%. Glypican-3 is a good marker for both well-differentiated and poorly differentiated HCC, with a diagnostic sensitivity of approximately 85%. In addition, glypican-3 is not expressed in benign or reactive hepatocytes; in contrast, both arginase-1 and HepPar-1 are expressed in both benign and neoplastic hepatocytes. Both CD10 and polyclonal CEA demonstrate a canalicular staining pattern in HCC and benign liver. AFP has limited utility due to its low sensitivity of approximately 25%, but AFP is a highly sensitive marker for hepatoblastoma. Nearly all HCCs are negative for MOC-31.
Adrenal cortical neoplasm/carcinoma is another group of epithelial tumors which is usually negative for both CK7 and CK20 . Mart-1 , calretinin, SF-1, and inhibin-alpha are a group of sensitive and relatively specific markers for identifying adrenal cortical neoplasm/carcinomas. They are usually negative for hepatocellular markers (arginase-1, HepPar-1, and glypican-3 ) and RCC markers (PAX8 , RCCma, CD10 , CAIX, and pVHL ) .
Over 90% of prostatic acinar ADCs are negative for CK7 and CK20 , with the exception of prostatic ductal ADC, which is usually positive for CK7. Prostate-specific antigen (PSA ) and prostate-specific acid phosphatase (PSAP ) are highly sensitive and specific markers for identifying over 90% of metastatic prostatic ADCs. NK3 homeobox 1 (NKX3.1 ) is a highly sensitive and specific nuclear staining marker for both primary and metastatic prostatic ADCs and has been reported in virtually 100% of prostatic ADCs. NKX3.1 is a marker of choice for a metastatic prostatic ADC in a decalcified specimen. P504S is another very sensitive but not totally specific marker for prostatic ADC. ERG is a recently described specific but not very sensitive marker for prostatic ADC, with a diagnostic sensitivity of approximately 40–50%. ERG is the most sensitive marker for benign and malignant vascular tumors.
SCCs frequently showed no immunoreactivity for CK7 or CK20 . Many markers such as p40 , CK5/6 , p63 , CK903, and SOX2 are indicative of squamous differentiation. CK5/6 and p40 are the most reliable markers to confirm squamous cell differentiation; however, a majority of urothelial carcinomas is also positive for both p40 and CK5/6.
Diagnostic IHC Panels Based on Histomorphology
If based on the histomorphology alone, four major morphologic types of neoplasms are usually encountered, including epithelioid cells (Table 1.19), small round cells (Table 1.20), spindle cells (Table 1.21), and pleomorphic cells (Table 1.22). Each morphologic category encompasses a wide differential diagnosis. Tables 1.19, 1.20, and 1.21 summarize the useful markers in the differential diagnosis of each category of tumor.
Alveolar soft part sarcoma may be positive for transcription factor E3 (TFE3) but negative for vimentin. Epithelioid sarcoma frequently shows loss of INI1 expression. PEComas can be patchy positive for S100 and usually positive for HMB45 and Mart-1 as well .
Application of Molecular Techniques on FNA Specimens
As our understanding of the molecular genetics of tumors is growing, the application of molecular tests on FNA specimens is accelerating. Most molecular techniques include:
-
In-situ hybridization (ISH)
-
Polymerase chain reaction (PCR)
-
Reverse transcription-polymerase chain reaction (RT-PCR )
-
Southern blotting
-
Gene microarrays
-
Transcriptional profiling
These techniques can be performed with FNAB specimens including direct smears, Thin Prep, or Surepath and have been used with different organ systems and different objectives to:
-
Detect cancer cells.
-
Render a specific diagnosis.
-
Distinct benign from malignant disease.
-
Determine the genetic abnormalities and genetic makeup of tumors.
-
Predict response to chemotherapy.
-
Perform risk assessment.
-
Select patients for targeted therapy.
Interphase cytogenetic studies by ISH techniques, unlike metaphase karyotyping, allow analysis of cytogenetic alterations of individual cells independent of their ability to proliferate. ISH with chromogenic or fluorescent signals has distinct advantages over other molecular techniques because it allows comparison of cellular morphology with chromosomal alterations in cells. FNA specimens, unlike cell block sections or tissue sections, are particularly suitable for ISH. The availability of intact cells makes it possible to count hybridized signals in the nuclei without nuclear transection and the associated inaccuracy in signal counting that can occur with cell block or tissue sections. With the availability of the commercial DNA probes, fluorescence in-situ hybridization (FISH) has several clinical applications for FNA specimens.
PCR can be performed using aspirated material collected solely for molecular analysis, from cells scraped from cellular smears, or from 10-micron tissue sections of cell blocks prepared from FNAB samples. The success of the test depends on the amount of viable material available for analysis:
-
PCR amplification , which allows automated enzymatic in-vitro synthesis of a target DNA sequence in millions of copies for subsequent sequence analysis, is one of the most commonly used molecular technique to demonstrate molecular alterations in FNA specimens.
-
RT-PCR analysis allows for amplification of very limited quantities of transcripts. This technique is suitable for molecular analysis of limited amounts of material, such as that procured by FNA.
-
Multiplex PCR allows for amplification of several target sequences simultaneously and is increasingly used for molecular analysis .
Microarray analysis has been used on FNA specimens. DNA chip or microarray technology relies on the accurate binding or hybridization of strands of DNA with their precise complementary copies where the known sequences are bound onto a solid-state substrate. These are hybridized with probes of fluorescent cDNAs or genomic sequences from test material. By analyzing the intensity of fluorescence on the chip, the expression of several thousands of genes can be determined simultaneously. The bioinformatics statistical programs were used to analyze the data generated in microarray experiments. And transcriptional profiling of using the currently available gene chips has been reported on FNA specimens from sites such as breast, lymph node, and lung.
Although some molecular tests are used for patient care, such as assessment of human epidermal growth factor receptor 2 (HER2/neu) for gene amplification in breast cancer, detection of clonality in hematopoietic neoplasms , and specific chromosomal translocations in the diagnosis of soft tissue sarcoma and hematopoietic neoplasms, most are currently investigational only.
Breast Cancer
-
The FISH assay for HER2/neu gene amplification can be performed on FNAB air-dried cytology smears or cell block sections of metastatic tumors because the HER2/neu status is usually concordant among primary tumor, locoregional, and distant metastasis.
-
Two kits approved by the US Food and Drug Administration (FDA) are either using an HER2/neu probe alone (Oncor, Gaithersburg, MD) or using an HER2/neu probe and a centromere 17 probe (Path Vysion, Vysis, Downers Grove, IL) .
Soft Tissue Tumors
-
The specific cytogenetic alterations can be detected using karyotypic analysis, PCR, or ISH. Touch preparations of core needle biopsy and cytospin or monolayer preparations of FNA specimens of primary or recurrent sarcomas are excellent specimens for FISH testing because of the availability of single cells for analysis.
-
Common and specific translocations can lead to recombination of coding sequences of different genes and result in the formation of pathologic fusion genes and expression of pathologic gene fusion products, which is valuable for making accurate diagnosis of soft tissue tumors.
-
The chromosomal translocation (11;22) (q24;q12) is specific for Ewing sarcoma, peripheral neuroepithelioma, and Askin’s tumor. When EWS gene is fused with the ATF-1 gene resulting from t(12;22)(q13;q12), it is specific for clear cell sarcoma; when it is fused with the WT-1 gene in t(11;22)(p13;q12), it is specific for desmoplastic small round cell tumor; when it is fused with the CHN gene in t(9;22)(q22;q12), it is specific for myxoid chondrosarcoma.
-
Alveolar rhabdomyosarcoma is characterized by two tumor-specific chromosomal translocations, t(2;13)(q35;q14) and t(1;13)(p36;q14), resulting in fusions of the PAX3 and PAX7 genes, which are members of the PAX transcription factor gene family mapped to 2q35 and 1p36 with the FKRH gene mapped to 13q14.
-
Synovial sarcoma is characterized by specific t(X;18)(p11;q11) translocation involving the SYT gene on chromosome 18 and 1 of the SSX genes on chromosome X, leading to functional fusion (SYT-SSX). These translocations are specific for synovial sarcoma and are particularly valuable for diagnosis of the small-cell and monophasic variants of synovial sarcoma.
-
Molecular analysis of c-kit mutations can be successfully performed using FNA samples for making a diagnosis of primary and recurrent gastrointestinal stromal tumors (GIST) .
Hematopoietic Neoplasms
-
In many cases cytomorphologic features in conjunction with immunophenotyping of aspirated material using flow cytometry and/or immunocytochemistry (ICC) alone may be sufficient for making a specific diagnosis.
-
In selected cases of malignant lymphoma where immunophenotyping using flow cytometry and/or ICC produces confusing results, molecular tests such as Southern blotting , PCR, and FISH can be used with FNA to demonstrate the clonality.
-
PCR is the most widely used for detection of immunoglobulin (Ig) heavy-chain and T-cell receptor gene rearrangements.
-
FISH and PCR can be used to detect bcl-1 and bcl-2 gene rearrangements in aspirates.
-
FISH performed on FNA smears using cyclin D1 and immunoglobulin heavy chain probes to demonstrate t(11;14)(q13;q32) chromosomal translocation in mantle cell lymphoma .
-
FISH performed on FNA smears using bcl-2 and immunoglobulin heavy chain probes indicating t(14;18)9q32;q21) chromosomal translocation .
Thyroid Neoplasms
-
FNA is routinely used to guide management of patients in the preoperative evaluation of thyroid nodules.
-
In 5–10% of cases, the results are inadequate; and in 20% of cases, the findings could be indeterminate for malignancy would require thyroidectomy.
-
Telomerase, RET/PTC rearrangements, and BRAF mutation have been studied with FNA of the thyroid.
-
More than half of all papillary thyroid carcinomas (PTC) harbor at least one of several chimeric oncogenes, called RET/PTC, which results from gene rearrangements involving the ret. proto-oncogene on chromosome 10 resulting in the generation of novel fusion transcripts.
-
Study supports the usefulness of RET/PTC RT-PCR and Southern hybridization as an ancillary test to cytology in selected cases for a definitive diagnosis of PTC.
-
BRAF mutations by RT-PCR are found in 70–72% of PTC cases and highly specific; they have not been noted in benign nodules or in other thyroid malignancies and has been investigated as an adjunct to cytology for making a definitive diagnosis of PTC. BRAF mutations also established the presence of malignancy in 16% of carcinomas that could not be diagnosed conclusively by FNA alone. The use of FNA sample in evaluating RET/PTC and BRAF mutations for making a diagnosis of PTC in indeterminate and suspicious cases of thyroid malignancies will require validation in future studies.
-
The telomerase activity has been investigated in thyroid FNA samples and archival Diff-Quik stained smears to distinguish malignant from benign lesions. Telomeres are highly conserved hexameric nucleotide repeats at the ends of chromosomes. Telomerase activity and hTERT gene expression by RT-PCR are noted in malignancy and in lymphocytic thyroiditis and 40% of follicular adenomas. The occurrence of telomerase activity in benign tumors decreases the specificity of the test in the preoperative diagnosis of thyroid nodules on FNA specimens.
-
Gene expression profiling by extracellular matrix and adhesion molecule cDNA arrays and real-time quantitative RT-PCR for FNA samples has been studied for the preoperative distinction of benign and malignant thyroid nodules from FNA samples and is promising and still needed to be validated in prospective trials .
Pulmonary Neoplasms
-
The sensitivity of lung FNA in the diagnosis of bronchogenic carcinoma is around 80%. The need for ancillary molecular testing with lung FNA samples arises in some cases with indeterminate or suspicious cytology findings where corresponding core needle biopsy (CNB) are unavailable or when CNB could not be performed either because of technical reasons or because of the development of pneumothorax. In de-stained Papanicolaou (Pap)-stained smears (the exfoliative and transbronchial FNA cases), the multitarget FISH assay (La Vysion, Vysis), which includes probes for chromosome 6p11-q11, 7p12 (EGFR), 8q24 (myc), and 5p15.2-chromosomal loci commonly affected in non-small-cell lung carcinoma (NSCLC), has been investigated to distinguish benign from malignant lesions. The test has been reported with an overall sensitivity and specificity of 79% and 100% and has potential in clinical practice for making a definite diagnosis in selected cases of lung FNA cases.
-
The c-myc E2F-1/p21 WAF1/Cip1 interactive gene expression index has been used for standardized RT-PCR testing of lung FNA with a sensitivity of 100% and specificity of 94%. The contribution of these molecular tests as an adjunct to cytology needs further validation.
-
The echinoderm microtubule-associated protein-like 4-anaplastic lymphoma kinase (ALK) re-arrangements and epidermal growth factor receptor (EGFR) mutations have emerged as a leading target for the treatment of patients with NSCLC, which are commonly mutually exclusive. If there is an EGFR mutation, the presence of KRAS mutation needs to be evaluated since its presence will negate the effect of EGFR inhibitors downstream and render the treatment ineffective. RT-PCR -based assays that target specific mutations in the EGFR gene have been reported to predict good response to tyrosine kinase (TK) inhibitors and can be easily performed on FNA material to aid in the selection of patients with advanced NSCLC for therapy with EGFR inhibitors. There are reports indicating the utility of assessing EGFR gene amplification for selecting patients for EGFR inhibitor therapy; and the gene amplification tests can be performed on FNAB samples.
-
The gene expression profiling of advanced NSCLC using RNA from lung FNA samples was performed and showed that transcriptional profiles were comparable with that from surgically excised tissue .
Metastatic Tumor in Lymph Node
-
The ancillary molecular tests can be used to detect small metastases and is considered currently investigational.
-
PCR for selected markers has been used to detect hypermethylation of CpG islands in promoter regions of MGMT, p16, and p14 as markers for micrometastases in EUS-guided lymph node FNA samples from patients with gastrointestinal and lung cancer.
-
RT-PCR has also been reported to detect levels of human telomerase reverse transcriptase mRNA to identify metastasis in the lymph nodes in patients with NSCLC.
-
Numerical aberrations in cyclin D1 gene copy numbers by FISH on FNA have been done in patients with previously untreated stage I and II oral squamous cell carcinoma who had not undergone radical neck dissection and showed independently predicted late cervical lymph node metastasis and that the results of such an analysis could be a valuable marker for poor prognosis, tumor aggressiveness, recurrence, and for selecting patients for elective cervical lymph node dissection.
-
RT-PCR for tyrosinase, a tissue-specific enzyme that regulates melanin biosynthesis, has been done in lymph node FNAB samples to detect metastasis of melanoma .
Pancreatic Neoplasms
-
K-ras oncogene mutations by mutant-enriched PCR have been investigated using FNA samples as a possible adjunct to conventional cytology for making a definite diagnosis of pancreatic adenocarcinoma. The K-ras oncogene is activated by point mutations in 75–90% of pancreatic adenocarcinoma with typical localization in codon 12. And K-ras mutations have been described in few proven cases of chronic pancreatitis.
-
Semiquantitative PCR for assessment of telomerase activity as a possible ancillary test to increase the sensitivity of pancreatic FNA in patients with pancreatic adenocarcinomas.
-
Comparative genomic hybridization (CGH) enables the study of global chromosomal aberrations in patient tissues without the need to culture the constituent cells. Target mutant DNA and normal DNA are tagged with different fluorescent signals and are mixed and applied to the normal metaphase chromosome preparations. The normal and mutant DNAs compete to hybridize with their complementary chromosomal loci. Digital image scanning is then used to quantify and compare the relative amounts of differentially colored signals indicating loss or gain of DNA in a given chromosomal locus.
-
The differentially expressed genes, lipocalin 2 (LCN2) and PLAT (tissue-type plasminogen activator or tPA), have been validated by RT-PCR in FNA samples and reported to be significantly increased in all pancreatic adenocarcinoma. Lipocalins are small extracellular proteins with an important role in cell proliferation and differentiation. PLAT is important in tumor angiogenesis and in the development of exocrine pancreatic cancer, contributing to the invasive phenotype. The utility of evaluating markers, such as lipocalin 2 and PLAT by RT-PCR using FNA of the pancreas for the diagnosis of pancreatic adenocarcinoma, needs further validation in future studies .
Renal Neoplasms
-
MN/CA9, carbonic anhydrase family member, is up-regulated by hypoxia-inducible factor 1 alpha in many cancers in response to hypoxic conditions. Its gene expression by RT-PCR in kidney FNA samples have been investigated as potential ancillary aids for making a definite diagnosis of malignancy on renal FNA. It has been established as a reliable biomarker for RCC and is present in almost all clear RCCs and in about 56% of papillary RCCs but is absent from chromophobe RCCs, oncocytomas, and normal tissue. The overall sensitivity and specificity were 68% and 100%, respectively. MN/CA9 protein expression can also be demonstrated by ICC.
-
FISH was performed on kidney tumors using centromere-specific probes for chromosome Y, 7, 17, 16, 12, 8, and 3 to study chromosomal alterations in FNA and effusions of primary and metastatic renal cell carcinoma and found numerical aberrations of chromosome 3 to be most frequent in RCC .
Infectious Disease
-
There are few reports discussing PCR on FNA samples from lymph nodes as an adjunct to conventional methods for the diagnosis of tuberculous lymphadenitis. An RT-PCR assay was developed to diagnose and identify the causative agent of suspected mycobacterial lymphadenitis using primers to detect M. avium and M. tuberculosis. This assay detected mycobacterial infections in 71.6% of patients; auramine staining and culture were positive in 46.3% and 41.2% of patients, respectively.
-
A PCR method for the amplification of Bartonella henselae DNA was developed, and showed that the results of this test can be useful for making an accurate diagnosis of cat-scratch disease in FNA specimens of the lymph nodes and primary lesion in comparison to Warthin-Starry silver impregnation stains and culture and can obviate the need for excisional biopsy.
-
The detection of HPV DNA in metastatic squamous cell carcinoma by PCR or in-situ hybridization can be used in selected cases to support a possible anogenital origin of the tumor, if the differential diagnosis includes tumors reported to have a low prevalence of HPV DNA such as from lung, esophagus, and skin in non-immunocompromised patients. The presence of high-risk HPV type in that case would suggest either an anogenital or a head-and-neck origin of the carcinoma .
The literature reports the excellent potential of material procured from FNA for applications in almost any type of molecular analysis, but few of the tests alone are used for patient care. However, some of these tests have the potential for clinical use in the coming years. The possible integration of molecular tests with current practice for the distinction of benign from malignant lesions in selected cases, determining the genetic makeup of tumors, and identifying specific molecular targets for typing, diagnosis, determining prognosis, and response to therapy are some of the anticipated uses of molecular tests as applied to FNA in the near future. Combining the stringent cytological criteria with ancillary molecular testing is expected to yield more discrete and diagnostic categories for research and reporting.
Abbreviations List
Abbreviation | Full Text |
|---|---|
ADC | Adenocarcinoma |
AFP | Alpha-fetoprotein |
APADC | Appendiceal adenocarcinoma |
Appen | Appendix |
AR | Androgen receptor |
AR | Antigen retrieval |
Arg-1 | Arginase-1 |
ATRX | Anti-transcriptional regulator |
BADC | Breast carcinoma |
BADC | Bladder adenocarcinoma |
Bcl2 | B-cell CLL/lymphoma 2 |
Beta-HCG | Beta human chorionic gonadotropin |
C | Cytoplasmic |
CA | Carcinoma |
CAIX | Carbonic anhydrase IX |
CC1 | Cell conditioning solution 1 (Ventana) |
CD | Cluster of differentiation |
CDC | Collecting duct carcinoma |
CDH17 | Cadherin-17 |
CDK4 | Cyclin-dependent kinase 4 |
CDX2 | Caudal-type homeobox 2 |
CEA | Carcinoembryonic antigen |
ChorioCA | Choriocarcinoma |
CK | Cytokeratin |
CNS | Central nervous system |
CRADC | Colorectal adenocarcinoma |
D2-40 | Podoplanin |
DAXX | Anti-death domain-associated protein 6 |
DFSP | Dermatofibrosarcoma protuberans |
DOG1 | Discovered on GIST-1 |
DPSRCT | Desmoplastic small round cell tumor |
Duo | Duodenum |
ECADC | Endocervical adenocarcinoma |
EMADC | Endometrial adenocarcinoma |
ER | Estrogen receptor |
ERG | ETS-related gene |
ESS | Endometrial stromal sarcoma |
FISH | Fluorescence in site hybridization |
Fli-1 | Friend leukemia virus integration 1 |
FNA | Fine needle aspiration |
FOXL2 | Forkhead box L2 |
GATA3 | GATA binding protein 3 |
GCDFP-15 | Gross cystic disease fluid protein 15 |
GI | Gastrointestinal |
GIST | Gastrointestinal stroma tumor |
H&E | Hematoxylin and eosin |
HCC | Hepatocellular carcinoma |
HepPar-1 | Hepatocyte paraffin-1 |
HMB45 | Human melanoma black 45 |
HNF-1B | Hepatocyte nuclear factor 1 beta |
HPV | Human papilloma virus |
ICC | Intrahepatic cholangiocarcinoma |
IHC | Immunohistochemistry |
IMP3 | Insulin-like growth factor II messenger RNA-binding protein-3 |
INI1 | Integrase interactor 1 |
ISH | In situ hybridization |
KIM-1 | Kidney injury molecule 1 |
LADC | Lung adenocarcinoma |
LC | Left colon |
LCA | Leukocyte common antigen |
LIN28 | Lin-28 homolog A |
Loc | Localization |
LYM | Lymphoblastic lymphoma |
M | Membranous |
Mart-1 | Melanoma-associated antigen recognized by T cells |
Maspin | Mammary serine protease inhibitor |
MCPyV | Merkel cell polyomavirus |
MDM2 | Mouse double minute 2 homolog |
MGB | Mammaglobin |
MIB-1 | Mindbomb homolog 1 |
MiTF | Microphthalmia-associated transcription factor |
MLH1 | MutL homolog 1 |
MOC-31 | Epithelial-related antigen clone MOC-31 |
MPNST | Malignant peripheral nerve sheath tumor |
MPO | Myeloperoxidase |
MS | Mesothelioma |
MSA | Muscle-specific actin |
MSI | Microsatellite instability |
MUC | Mucin |
MUC4 | Mucin 4 |
MUC5AC | Mucin 5 AC |
Myo | Myogenin |
MyoD1 | Myogenic differentiation 1 |
N | Nuclear |
NANOG | NANOG homeobox |
NB | Neuroblastoma |
NET | Neuroendocrine tumor |
NKX2.2 | NK2 homeobox 2 |
NKX3.1 | NK3 homeobox 1 |
NSE | Neuron-specific enolase |
NY-ESO-1 | Cancer/testis antigen 1B |
OCCCA | Ovarian clear cell carcinoma |
OCT4 | Octamer-binding transcription factor 4 |
OSCA | Ovarian serous carcinoma |
P504S | Alpha-methylacyl-CoA racemase |
PADC | Pancreatic adenocarcinoma |
PADC | Prostatic adenocarcinoma |
Pan | Pancreas |
PAX | Paired box gene |
PC | Plasmacytoma |
PDX1 | Pancreatic duodenal homeobox 1 |
PECOMa | Perivascular epithelioid cell tumor |
PMS2 | Postmeiotic segregation increased 2 |
PNET | Primitive neuroectodermal tumor |
PNL2 | Melanoma-associated antigen PNL2 |
PR | Progesterone receptor |
PRCC | Papillary renal cell carcinoma |
PSA | Prostate-specific antigen |
PSAP | Prostate-specific acid phosphatase |
PTC | Papillary thyroid carcinoma |
pVHL | Von Hippel-Lindau tumor suppressor |
RBC | Red blood cell |
RCC | Renal cell carcinoma |
RCCma | Renal cell carcinoma marker |
Rec | Rectum |
RHMS | Rhabdomyosarcoma |
S100P | Placental S00 |
SADC | Small bowel adenocarcinoma |
SADC | Small intestinal adenocarcinoma |
SALL4 | Sal-like protein 4 |
SATB2 | Special AT-rich sequence-binding protein 2 |
SCC | Squamous cell carcinoma |
SF-1 | Steroidogenic factor 1 |
SFT | Solitary fibrous tumor |
SMA | Smooth muscle actin |
SmCC | Small-cell carcinoma |
SOX | Sex-determining region Y-box |
SSCC | Salivary gland small-cell carcinoma |
Stoma | Stomach |
TFE3 | Transcription factor E3 |
TFF1 | Trefoil factor 1 |
TLE1 | Transducin-like enhancer of split 1 |
TTF1 | Thyroid transcription factor 1 |
UC | Urothelial carcinoma |
UGI | Upper gastrointestinal tract |
UP | Uroplakin |
WT1 | Wilms’ tumor 1 |
Suggested Reading
Cytology/FNA
DeMay RM. Chapter 8. Building blocks of cytodiagnosis. In:The art and science of cytopathology, vol. 2. 2nd ed. Chicago: ASCP Press; 2010a. p. 562–619.
DeMay RM. Chapter 7. Introduction to FNA biopsy. In:The art and science of cytopathology, vol. 2. 2nd ed. Chicago: ASCP Press; 2010b. p. 536–61.
Ancillary Study: IHC
Bahrami A, Truong LD, Ro JY. Undifferentiated tumor: true identity by immunohistochemistry. Arch Pathol Lab Med. 2008;132(3):326–48.
Barbareschi M, Murer B, Colby TV, Chilosi M, Macri E, Loda M, et al. CDX-2 homeobox gene expression is a reliable marker of colorectal adenocarcinoma metastases to the lungs. Am J Surg Pathol. 2003;27(2):141–9.
Baumhoer D, Tornillo L, Stadlmann S, Roncalli M, Diamantis EK, Terracciano LM. Glypican 3 expression in human nonneoplastic, preneoplastic, and neoplastic tissues: a tissue microarray analysis of 4,387 tissue samples. Am J Clin Pathol. 2008;129(6):899–906.
Bishop JA, Sharma R, Illei PB. Napsin a and thyroid transcription factor-1 expression in carcinomas of the lung, breast, pancreas, colon, kidney, thyroid, and malignant mesothelioma. Hum Pathol. 2010;41(1):20–5.
Cao D, Guo S, Allan RW, Molberg KH, Peng Y. SALL4 is a novel sensitive and specific marker of ovarian primitive germ cell tumors and is particularly useful in distinguishing yolk sac tumor from clear cell carcinoma. Am J Surg Pathol. 2009a;33(6):894–904.
Cao D, Humphrey PA, Allan RW. SALL4 is a novel sensitive and specific marker for metastatic germ cell tumors , with particular utility in detection of metastatic yolk sac tumors. Cancer. 2009b;115(12):2640–51.
Chang A, Brimo F, Montgomery EA, Epstein JI. Use of PAX8 and GATA3 in diagnosing sarcomatoid renal cell carcinoma and sarcomatoid urothelial carcinoma. Hum Pathol. 2013;44(8):1563–8.
Chu PG, Weiss LM. Modern immunohistochemistry. New York: Cambridge University Press; 2009.
Dabbs DJ. Diagnostic immunohistochemistry. 3rd ed. Philadelphia: Churchill Livingstone Elsevier; 2010.
Dejmek A, Naucler P, Smedjeback A, Kato H, Maeda M, Yashima K, et al. Napsin a (TA02) is a useful alternative to thyroid transcription factor-1 (TTF-1) for the identification of pulmonary adenocarcinoma cells in pleural effusions. Diagn Cytopathol. 2007;35(8):493–7.
Dennis JL, Hvidsten TR, Wit EC, Komorowski J, Bell AK, Downie I, et al. Markers of adenocarcinoma characteristic of the site of origin: development of a diagnostic algorithm. Clin Cancer Res. 2005;11(10):3766–72.
DeYoung BR, Wick MR. Immunohistologic evaluation of metastatic carcinomas of unknown origin: an algorithmic approach. Semin Diagn Pathol. 2000;17(3):184–93.
Erickson LA, Papouchado B, Dimashkieh H, Zhang S, Nakamura N, Lloyd RV. Cdx2 as a marker for neuroendocrine tumors of unknown primary sites. Endocr Pathol. 2004;15(3):247–52.
Higgins JP, Kaygusuz G, Wang L, Montgomery K, Mason V, Zhu SX, et al. Placental S100 (S100P) and GATA3 : markers for transitional epithelium and urothelial carcinoma discovered by complementary DNA microarray. Am J Surg Pathol. 2007;31(5):673–80.
Hornick JL, Dal Cin P, Fletcher CD. Loss of INI1 expression is characteristic of both conventional and proximal-type epithelioid sarcoma. Am J Surg Pathol. 2009;33(4):542–50.
Jones TD, Ulbright TM, Eble JN, Baldridge LA, Cheng L. OCT4 staining in testicular tumors: a sensitive and specific marker for seminoma and embryonal carcinoma. Am J Surg Pathol. 2004;28(7):935–40.
Krishna M. Diagnosis of metastatic neoplasms: an immunohistochemical approach. Arch Pathol Lab Med. 2010;134(2):207–15.
Liu A, Cheng L, Du J, Peng Y, Allan RW, Wei L, et al. Diagnostic utility of novel stem cell markers SALL4 , OCT4 , NANOG, SOX2, UTF1, and TCL1 in primary mediastinal germ cell tumors . Am J Surg Pathol. 2010;34(5):697–706.
Lin F, Liu H. Immunohistochemistry in undifferentiated neoplasm/tumor of uncertain origin. Arch Pathol Lab Med. 2014;138(12):1583–610.
Lin F, Liu H. Unknown primary/undifferentiated neoplasm. In: Lin F, Prichard JW, Liu H, Wilkerson M, Chen ZM, editors. Handbook of practical immunohistochemistry – frequently asked questions. 2nd ed. New York: Springer Science+Business Media; 2015. p. 119–64.
Lin F, Shi J, Liu H, Zhang J, Zhang PL, Wang HL, et al. Immunohistochemical detection of the von Hippel-Lindau gene product (pVHL ) in human tissues and tumors: a diagnostic marker for metastatic renal cell carcinoma and clear cell carcinoma of the ovary and uterus. Am J Clin Pathol. 2008;129(4):592–605.
Liu H, Shi J, Wilkerson ML, Lin F. Immunohistochemical evaluation of GATA3 expression in tumors and normal tissues: a useful immunomarker for breast and urothelial carcinomas. Am J Clin Pathol. 2012;138(1):57–64.
Liu H, Shi J, Wilkerson M, Yang XJ, Lin F. Immunohistochemical evaluation of ERG expression in various benign and malignant tissues. Ann Clin Lab Sci. 2013;43(1):3–9.
Long KB, Srivastava A, Hirsch MS, Hornick JL. PAX8 expression in well-differentiated pancreatic endocrine tumors: correlation with clinicopathologic features and comparison with gastrointestinal and pulmonary carcinoid tumors. Am J Surg Pathol. 2010;34(5):723–9.
Magnusson K, de Wit M, Brennan DJ, Johnson LB, McGee SF, Lundberg E, et al. SATB2 in combination with cytokeratin 20 identifies over 95% of all colorectal carcinomas. Am J Surg Pathol. 2011;35(7):937–48.
Miettinen M, Wang ZF, Paetau A, Tan SH, Dobi A, Srivastava S, et al. ERG transcription factor as an immunohistochemical marker for vascular endothelial tumors and prostatic carcinoma. Am J Surg Pathol. 2011;35(3):432–41.
Ordóñez NG. Napsin a expression in lung and kidney neoplasia: a review and update. Adv Anat Pathol. 2012a;19(1):66–73.
Ordóñez NG. Thyroid transcription factor-1 is not expressed in squamous cell carcinomas of the lung: an immunohistochemical study with review of the literature. Appl Immunohistochem Mol Morphol. 2012b;20(6):525–30.
Ordóñez NG. Value of PAX 8 immunostaining in tumor diagnosis: a review and update. Adv Anat Pathol. 2012c;19(3):140–51.
Ordóñez NG. Value of PAX8 , PAX2, napsin a, carbonic anhydrase IX, and claudin-4 immunostaining in distinguishing pleural epithelioid mesothelioma from metastatic renal cell carcinoma. Mod Pathol. 2013;26(8):1132–43.
Ordóñez NG. Value of thyroid transcription factor-1 immunostaining in tumor diagnosis: a review and update. Appl Immunohistochem Mol Morphol. 2012d;20(5):429–44.
Panarelli NC, Yantiss RK, Yeh MM, Liu Y, Chen YT. Tissue-specific cadherin CDH17 is a useful marker of gastrointestinal adenocarcinomas with higher sensitivity than CDX2 . Am J Clin Pathol. 2012;138(2):211–22.
Park SY, Kim BH, Kim JH, Lee S, Kang GH. Panels of immunohistochemical markers help determine primary sites of metastatic adenocarcinoma. Arch Pathol Lab Med. 2007;131(10):1561–7.
Timek DT, Shi J, Liu H, Lin F. Arginase-1, HepPar-1, and Glypican-3 are the most effective panel of markers in distinguishing hepatocellular carcinoma from metastatic tumor on fine-needle aspiration specimens. Am J Clin Pathol. 2012;138(2):203–10.
Varadhachary GR, Abbruzzese JL, Lenzi R. Diagnostic strategies for unknown primary cancer. Cancer. 2004;100(9):1776–85.
Wang HL, Anatelli F, Zhai QJ, Adley B, Chuang ST, Yang XJ. Glypican-3 as a useful diagnostic marker that distinguishes hepatocellular carcinoma from benign hepatocellular mass lesions. Arch Pathol Lab Med. 2008;132(11):1723–8.
Wennerberg AE, Nalesnik MA, Coleman WB. Hepatocyte paraffin 1: a monoclonal antibody that reacts with hepatocytes and can be used for differential diagnosis of hepatic tumors. Am J Pathol. 1993;143(4):1050–4.
Yan BC, Gong C, Song J, Krausz T, Tretiakova M, Hyjek E, et al. Arginase-1: a new immunohistochemical marker of hepatocytes and hepatocellular neoplasms. Am J Surg Pathol. 2010;34(8):1147–54.
Ancillary Study: Molecular Analysis
Betz BL, Dixon CA, Weigelin HC, Knoepp SM, Roh MH. The use of stained cytologic direct smears for ALK gene rearrangement analysis of lung adenocarcinoma. Cancer Cytopathol. 2013;121:489–99.
Bofin AM, Ytterhus B, Martin C, O’Leary JJ, Hagmar BM. Detection and quantitation of HER-2 gene amplification and protein expression in breast carcinoma. Am J Clin Pathol. 2004;122:110–9.
Cheng L, Zhang S, Alexander R, Yao Y, MacLennan GT, Pan CX, et al. The landscape of EGFR pathways and personalized management of non-small-cell lung cancer. Future Oncol. 2011;7:519–41.
Cheung CC, Carydis B, Ezzat S, Bedard YC, Asa SL. Analysis of ret/PTC gene rearrangements refines the fine needle aspiration diagnosis of thyroid cancer. J Clin Endocrinol Metab. 2006;86:2187–90.
Cibas E, Ducatman B. Thyroid. In:Text cytology diagnostic principles and clinical correlates. 3rd ed. Philadelphia: Saunders Elsevier; 2009. p. 255.
Cohen Y, Rosenbaum E, Clark DP, et al. Mutational analysis of BRAF in fine needle aspiration biopsies of the thyroid: a potential application for the preoperative assessment of thyroid nodules. Clin Cancer Res. 2004;10:2761–5.
Dimashkieh H, Wolff DJ, Smith TM, Houser PM, Nietert PJ, Yang J. Evaluation of UroVysion and cytology for bladder cancer detection: a study of 1835 paired urine samples with clinical and histologic correlation. Cancer Cytopathol. 2013;121:591–7.
Frostad B, Martinsson T, Tani E, et al. The use of fine-needle aspiration cytology in the molecular characterization of neuroblastoma in children. Cancer (Cancer Cytopathol). 1999;87:60–8.
Kebebew E, Peng M, Reiff E, Targ O, Clark OH, McMillan A. ECM1 and TMPRSS4 are diagnostic markers of malignant thyroid neoplasms and improve the accuracy of fine needle aspiration biopsy. Ann Surg. 2005;242:353–61.
Kipp BR, Fritcher EG, del Rosario KM, Stevens CL, Sebo TJ, Halling KC. A systematic approach to identifying urothelial cells likely to be polysomic by fluorescence in situ hybridization. Anal Quant Cytol Histol. 2005;27:317–22.
Krishnamurthy S. Applications of molecular techniques to fine-needle aspiration. Biopsy Cancer (Cancer Cytopathol). 2007;111:106–22.
Mezzelani A, Alasio L, Bartoli C, et al. C-erbB2/neu gene and chromosome 17 analysis in breast cancer by FISH on archival cytological fine-needle aspirates. Br J Cancer. 1999;80:519–25.
Nikiforov YE. Molecular diagnostics of thyroid tumors. Arch Pathol Lab Med. 2011;135:569–77.
Nikiforova MN, Khalid A, Fasanella KE, McGrath KM, Brand RE, Chennat JS, et al. Integration of KRAS testing in the diagnosis of pancreatic cystic lesions: a clinical experience of 618 pancreatic cysts. Mod Pathol. 2013;26:1478–87.
Nizzoli R, Bozzetti C, Crafa P, et al. Immunocytochemical evaluation of HER-2/neu on fine-needle aspirates from primary breast carcinomas. Diagn Cytopathol. 2003;28:142–6.
Rhyu MS. Telomeres, telomerase and immortality. J Natl Cancer Inst. 1995;87:884–94.
Rosell R, Moran T, Queralt C, Porta R, Cardenal F, Camps C, et al. Screening for epidermal growth factor receptor mutations in lung cancer. N Engl J Med. 2009;361:958–67.
Santoro M, Carlomagno F, Hay ID, et al. Ret oncogene activation in human thyroid neoplasms is restricted to the papillary cancer subtype. J Clin Invest. 1992;89:1517–22.
Siddiqui MT, Greene KL, Clark DP, et al. Human telomerase reverse transcriptase expression in diff-Quik stained FNA samples from thyroid nodules. Diagn Mol Pathol. 2001;10:123–9.
Willmore-Payne C, Layfield LJ, Holden JA. C-KIT mutation analysis for diagnosis of gastrointestinal stromal tumors in fine needle aspiration specimens. Cancer (Cancer Cytopathol). 2005;105:165–70.
Yoder BJ, Skacel M, Hedgepeth R, Babineau D, Ulchaker JC, Liou LS, et al. Reflex UroVysion testing of bladder cancer surveillance patients with equivocal or negative urine cytology: a prospective study with focus on the natural history of anticipatory positive findings. Am J Clin Pathol. 2007;127:295–301.
Author information
Authors and Affiliations
Rights and permissions
Copyright information
© 2018 Springer International Publishing AG
About this chapter
Cite this chapter
Lin, F., Zhang, J., Liu, H. (2018). Introduction and Application of Fine Needle Aspiration Biopsy. In: Handbook of Practical Fine Needle Aspiration and Small Tissue Biopsies. Springer, Cham. https://doi.org/10.1007/978-3-319-57386-1_1
Download citation
DOI: https://doi.org/10.1007/978-3-319-57386-1_1
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-319-57384-7
Online ISBN: 978-3-319-57386-1
eBook Packages: MedicineMedicine (R0)