
Abstract
Hidden hunger, referring to micronutrient deficiencies often not apparent through distinct clinical symptoms, is known to be highly prevalent in many developing countries: The prevalence of such inadequacies in developed countries has been less discussed, even though it is worryingly high for some micronutrients even in affluent countries such as the U.S. Therefore the aim of this chapter is to review and discuss the available data on micronutrient intakes and status in affluent societies in general and in sub populations that are particularly at risk. As discussing all nutrients systematically would exceed the scope of this article, this chapter concentrates on nutrients of particular concern for the general population or during specific periods in the life cycle. It concludes that in affluent countries, micronutrient inadequacies are widespread, and that intakes of vitamins E, D and A and folate are particularly critical, pointing out that improving nutrition could help alleviate the social and financial burden of nutrition deficiency diseases. Better knowledge concerning their nutritional status might encourage people to improve their diet and consequently their long-term health.
Access provided by CONRICYT-eBooks. Download chapter PDF
Similar content being viewed by others


Keywords
- Hidden hunger
- Nutrition deficiency diseases
- Micronutrient intakes
- Micronutrient status
- Micronutrient deficiency
- Developed countries
- Affluent societies
1 Is the Developed World Micronutrient-Secure?
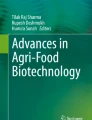
Hidden hunger, referring to micronutrient deficiencies often not apparent through distinct clinical symptoms, is known to be highly prevalent in many developing countries: The recent Lancet series on maternal and child nutrition reports on the widespread occurrence of insufficient supply with a range of micronutrients in low- and middle-income countries (LMIC) [1]. For example, around 30% of school-aged children and 15% of pregnant women were reported to be vitamin A-deficient in countries with GDP < US$15,000 [2]. The prevalence of such inadequacies in developed countries has been less discussed, even though it is worryingly high for some micronutrients even in affluent countries such as the U.S. (Fig. 11.1) [3].

Proportion of U.S. population aged ≥4 years with intakes below the Estimated Average Requirement or Adequate Intake (Food only [dark blue] or food and multiple micronutrient supplements [light blue], % ± standard error of the mean) (Adapted from Wallace et al. [3])
2 Vitamin D Status
A review of studies assessing serum 25-hydroxyvitamin D levels globally found that nearly 40% of the population had inadequate (<50 nmol/L) and approximately 7% deficient (<25 nmol/L) levels [4]. A similar picture is shown by the map of 25-hydroxyvitamin D levels in adults compiled by Wahl et al. [5] (Figure 11.2). The most recent European Nutrition and Health Report showed that average vitamin D intakes for women were below recommendations in all countries surveyed, and for men, in around two thirds of them [6]. In line with this, it was reported that between 50 and 100% of adults in various European countries had inadequate intakes of this vitamin [7]. Also in the U.S., more than 90% of adults were reported to have intakes of vitamin D below the Estimated Average Requirement in 2007–2010 [3]. Prevalence of 25-hydroxvitamin D levels below 30 nmol/L was ~18% in Europeans assessed between October and March, but only ~9% for those studied in April to September, reflecting the body’s capacity for endogenous production during the summer months, and dark-skinned persons had a significantly higher risk of inadequate levels [8]. The high prevalence of low vitamin D levels is thought to be highly relevant for public health, as it has been estimated that the risk ratio for all-cause mortality in the lowest compared with the highest quintiles of serum 25-hydroxyvitamin D is around 1.6 (95% confidence interval from 1.36 to 1.81) [9]. Unsurprisingly, it has been suggested that doubling serum levels could reduce all-cause mortality rates by about 17% in Europe, resulting in an increase in life expectancy of approximately two years [10].

Vitamin D status in adults (>18 years) around the world (Wahl et al. [5])
At the same time, calcium intakes were found to be low for around 20% of adults in a range of European countries [7] and for more than 40% in the U.S. [3] (Fig. 11.1). Vitamin D plays an important role in calcium absorption and bone re-modelling, and insufficiency can accelerate age-related loss of bone and increase the risk of fracture [11]. The elderly seem to be particularly at risk of vitamin D inadequacy or even deficiency [4], and it has been proposed that nutritional supplements with 700–1000 IU or more per day should ideally be taken by this age group to prevent fractures resulting from falls [12], combined with regular intakes of dairy products to assure adequate intakes of calcium and protein [13]. Intakes of vitamin K, an additional key player for bone health, have also been reported as inadequate for large segments of the population [3, 14] (Fig. 11.1). Bone health seems to be further affected by lack of other micronutrients such as vitamins C and E, highlighting the important role that nutrition as a whole plays in reducing the risk of osteoporosis [15]. Worryingly, these are also frequently reported to be low in a significant proportion of the population (see below).
3 Vitamin C Status
The European Nutrition and Health Survey [6] reports mean vitamin C intakes ranging from ~60 to ~153 mg. However, despite the comparatively high mean intake reported for Germany (153 mg/d for adults) [6], half the adult population has a vitamin C intake below the current German recommendation of 100 mg per day [16, 17]. Using lower cut-off of 60 and 50 mg/d for men and women, respectively, the European survey reports 8–40% of adults with inadequate intakes [7]. Similar rates of inadequate intakes relative to recommendations were reported from the U.S. [3] (Fig. 11.1), even though the cut-offs used there are slightly higher at 75 and 60 mg/d for men and women, respectively [18]. Unfortunately, dietary surveys frequently only report mean or median intakes, which do not give an indication of the proportion of the population with intakes below the recommendations. Given the similarities of the mean intakes, it can be assumed that the same problem exists in many, also affluent, parts of the world: In Japan, median intakes increase from around 60 mg in the age group of 15–49 to above 100 mg in people aged ≥50 years [19], and mean intakes in South Korea were 116 mg in men and 105 mg in women [20].
4 Vitamin E Status
Vitamin E seems to be another nutrient of concern even in affluent countries, as high proportions of inadequate intakes have been reported from the U.S., some European countries, and also some countries in the Asia Pacific region [3, 21] (Fig. 11.1). A recent review showed that, globally, 82 and 61% of adults aged ≥14 years had intakes below 15 and 12 mg/day, respectively (Fig. 11.3), [22]. The former level corresponds to the Recommended Daily Allowance and the latter to the Estimated Average Requirement defined by the Institute of Medicine [18]. Even more worryingly, recent evidence, as yet mostly from epidemiologic studies, on cardiovascular health and immune function indicates that optimal plasma alpha-tocopherol levels might be higher than previously assumed [23].

Vitamin E intakes (total of all 8 isomers) reported as mean (black) or median (blue) by region and country from studies with persons aged ≥14 years. Red low intake (≤5 mg/d); yellow moderate intake (6–14 mg/d); green recommended intake or above (≥15 mg/d) (n = 128 studies); for more details, see Péter et al. [22]
5 Vitamin A Status
Vitamin A intakes from food are also low for more than 40% of Americans above the age of 13 years [3], while this is the case for ~15% of men and ~10% of women in Germany [17]. The differences are partially due to the conversion factor of 1:12 used in the U.S. [24], whereas 1:6 is used in Germany [16]. This is due to different interpretations of the evidence for the relative absorption of pro-vitamin A and its conversion by the β-carotene monooxygenase by the Institute of Medicine [25] and DACH [16]. As beta-carotene contributes significantly to total vitamin A intakes [26], using the same conversion factor as in the U.S. would considerably increase the proportion of Germans with total vitamin A intakes below the recommendations. The accuracy of the conversion and the assessment of adequacy of vitamin A intakes is further complicated by the existence of various common polymorphisms for genes encoding enzymes involved in the conversion of beta-carotene to vitamin A: Carriers of these polymorphism can have an up to 50% reduction in enzyme activity, and therefore have an impaired ability to convert beta-carotene to vitamin A [27]. Consequently, such polymorphisms make it more difficult to achieve adequate intakes, and specific recommendations might be needed for these at-risk groups [28].
6 B-Vitamins Status
B-vitamins appear at first glance to be less of an issue in developed countries such as the U.S. [3] (Fig. 11.1). However, the proportion of adults with inadequate intakes of vitamin B12 reached 20% and 40% in Finland and Greece, respectively [7]. In Canada, it has been reported that between 3 and 9% of non-pregnant women had deficient or marginal serum concentrations for vitamin B12, respectively, which increased to 10 and 21% at week 16 and 23 and 35% at week 36 of gestation [29]. This is in line with a meta-analysis of global prevalence of vitamin B12 insufficiency during pregnancy, which found 21, 19 and 29% in the first, second and third trimester, respectively [30]. Moreover, comparison of intakes from 2005 to 2007 and 2012 to 2013 showed a small but significant downward trend for some of the B-vitamins in Germany, which might be linked to decreased intakes of fruits and fruit products [31].
For folate, the situation is even more critical, with proportions of intakes below recommendations ranging from 20 to 40% in some European countries [7]. In German women, folate intakes remained stable, albeit at a relatively low median with intakes of 200 µg/d [31], and only 8 and 3% of women aged 19–45 years and 15–19 years, respectively, reporting that they take folate-containing supplements [17]. A review of nutritional intakes in pregnant women in other affluent countries showed folate intakes of 75, 64 and 37% of Estimated Average Requirements for pregnant women in Japan, the U.S. and Australia, respectively [32]. Periconceptual folate use is generally low in Europe, with only the Netherlands and Denmark achieving levels around 40 and 30% of periconceptual folate use, respectively, while the other countries monitored (Belgium, Croatia, Germany, Ireland Italy, Portugal, Spain and Switzerland) had levels below 10%—in some cases, considerably so [33]. This is despite the fact that a clear dose response has been shown for maternal folate status and the risk of developing neural tube defects in the offspring [34]. Moreover, perinatal folic acid supplementation can significantly reduce the risk and poses no risk to the mother or the baby [35]. Each year, ~300,000 children are born with neural tube defects globally, and in Europe, more than 4,500 pregnancies are affected [36]. Moreover, low folate status during early pregnancy was found to be associated with smaller total brain volume, poorer language performance, reduction in memory and learning, and a decrease in visuo-spatial domains in Dutch children [37].
In addition, the availability of B-vitamins and other nutrients implicated in the one-carbon metabolism and consequently DNA methylation due to maternal nutrition during pregnancy seems to play an important role in epigenetic changes in the offspring [38]. Even though the mechanisms are not well understood, processes such as DNA methylation in the offspring as a result of maternal or even paternal diet have been shown in a range of studies in animals and humans [39]. A recent study in the Gambia, for example, showed different DNA methylation pattern in the blood of infants whose mothers had received periconceptional micronutrient supplements compared with those whose mothers received a placebo [40]. It has been suggested that these epigenetic alterations might have long-lasting consequences for cognition and health [41].
7 The Vitamin Status of Pregnant Women
While it was reported that the prevalence of low iron intakes was around or below 10% in European countries, these figures only include male adults, as data on woman were excluded for methodological reasons [7]. A study of the nutritional status of pregnant women in affluent countries reports intakes to be 49, 55, 60, 72 and 107% of the Estimated Average Requirement in Japan, Australia and New Zealand, Europe, the U.S. and Canada and the UK, respectively [32]. In the U.S., 18% of pregnant women were classified as iron-deficient, and the prevalence increased as gestation progressed [42].
A review of vitamin D intakes in pregnant women in affluent countries reported intakes at 24, 43, 74 and 78% of the Estimated Average Requirement or Adequate Intake for Japan, U.S. and Canada, Australia and the UK, respectively [32]. Comparison of pregnant and non-pregnant age-matched controls showed significantly lower level in the former [43]. Even though pregnancy-related adaptations such as hemodilution raise some questions regarding optimal levels [44], this is still worrying, given the importance of vitamin D for early development [45]. A recent meta-analysis concluded that supplementation with vitamin D was effective in raising serum 25-hydroxy levels during pregnancy and might have a beneficial effect on the risk of pre-eclampsia, low birth weight and preterm birth—even though some questions remain to be resolved, particularly with respect to co-supplementation with calcium [46]. Currently, even recently revised recommendations contain no additional provision for vitamin D during pregnancy and lactation [47, 48]. However, it has been proposed that significantly higher amounts, in the range of 1500–2000 IU per day, are necessary to avoid deficiency during this highly demanding period [49]. Adequate maternal vitamin D levels are particularly important, as neonates were identified as a further group that is particularly at risk of vitamin D deficiency, [4] and low levels at birth are thought to have long-lasting consequences: low levels in cord blood were, for example, linked to increased risk of respiratory infection and wheezing five years later [50]. In addition to increasing vitamin D levels in maternal and cord blood, supplementation during pregnancy also led to an increase in birth weight and length [51]. It has been shown that achieving adequate maternal levels of vitamin D via supplements had a beneficial effect on neonatal status [52].
8 The Vitamin Status of Infants
During lactation, adequate intakes are also crucial, as the nutrient content of breast milk—particularly for iodine, specific fatty acids including DHA, thiamine, riboflavin, as well as vitamins A, B6, B12, C and D—are influenced by maternal diet and reserves [53]. In Germany, a significant proportion of infants was reported to have intakes below recommendations, those for vitamin D, E, C and folate being particularly low [54]. However, even with a balanced, nutrient-dense diet, it is difficult to meet the requirements for some nutrients during this crucial period: Even though the vitamin D content of breast milk can be increased by maternal supplementation, it has been shown that breast milk only covered around one fifth of the recommended daily dose for this age group [55], unless daily high-dose supplements were taken [56]. A study in Swedish infants showed that without the addition of vitamin D drops to the diet, many of these healthy-term infants would have had intakes associated with the risk of developing rickets [57]. Consequently, daily supplementation with drops of 400 IU/d are recommended for infants, starting at birth [58]. However, compliance with this supplementation was found to be low, and exclusively breast-fed infants in particular had difficulties meeting the recommended intakes in the U.S. due to the relatively low levels in human milk [59].
A study evaluating the nutritional adequacy of children aged one to three years in Brazil, Germany, Russia and the United States reported vitamins A, D, calcium, and folate only in Germany as nutrients of concern in this age group [60]. Moreover, nearly 60% of young children (12–24 months) in a study in the U.S. were found to have vitamin E intakes below the recommendations [61]. Swiss school children were reported to have inadequate intakes of various vitamins [62]. Intakes of calcium, as well as of vitamins D and E, were identified as critical in U.S. children who did not take supplements, while inadequate intakes of magnesium and vitamin A were found in a lower, but still substantial, proportion [63].
In addition to vitamins and minerals, intakes of other essential nutrients appear to be still rather low: Even though polyunsaturated fat intake has increased globally compared to the 1990s, it is still lower than what is generally regarded as optimal (Fig. 11.4) [64]. Only limited information on docosahexaenoic acid (DHA) and eicosaenoic acid (EPA) intakes is available, but a study in the U.S. found that on average, adults had intakes of 63 and 23 mg/d respectively, which slightly increased to 72 and 41 mg/day if supplements were included [65]. This is well below the >250 mg DHA and EPA that were proposed as optimal for healthy individuals [66].

Global and regional mean consumption levels of dietary seafood and plant omega-3 fat in 2010 for adults ≥20 years of age [64]
9 The Vitamin Status of the Elderly
Malnutrition among the elderly is a significant and somewhat neglected public health problem that is thought to affect approximately 10% of people over the age of 65 years in the UK [67]. Even though frequently only protein-energy malnutrition is assessed, a study in the US showed that intakes below the Estimated Average Requirements were widespread for a range of micronutrients [68]. A review of the available data in Europe, Canada and the U.S. showed that vitamin D, thiamine, riboflavin, calcium, magnesium and selenium were identified as micronutrients of concern in the elderly [69]. Data from Germany shows that the situation is even more critical for elderly people living in care homes due to their physical or mental impairments [70] (Fig. 11.5). The situation is similar in Canada, where intakes of folate (before mandatory fortification was implemented), magnesium, zinc, vitamin E and B6 were low for ≥70% of elderly inhabitants of various care centers [71].

10 Dietary Supplements
The situation is somewhat improved by the use of dietary supplements: In one study, >80% of adults aged >50 years met the Estimated Average Requirements for vitamins A, B6, B12, C and E, folate, iron and zinc, thanks to supplementation [72]. In general, the use of dietary supplements in the elderly in Europe and Northern America seems to be gaining impetus and contributes significant amounts to their habitual intakes for a range of micronutrients (as reviewed by ter Borg et al. [69]). It has been suggested that regular use of dietary supplements is a promising way to improve micronutrient intakes in the elderly [73]. The same applies to the population as a whole: Data on dietary intake between 2007 and 2010 shows that around 50% of persons aged ≥4 years consumed dietary supplements with at least three vitamins and one mineral, which was an increase from the approximately 30% reported in previous surveys [3]. Figure 11.1 shows that, thanks to such supplements, the proportion of the population with intakes below recommendations decreases somewhat, but remains critically high for some nutrients [3]. In Europe, their use is somewhat less common, and a strong north-to-south gradient, with 40 and 5% users, respectively, was reported [7]. This gradient was observed in dietary patterns in general in Europe, as the diets of southern countries were found to provide adequate intakes of vitamin E, but were poor in vitamin A and D, while Nordic countries showed a near-opposite trend [74].
11 Food Fortification
Another commonly used approach to improve nutrient intakes is food fortification: In the case of vitamin D, for example, it has been shown that the fortification of products such as yoghurt, orange juice and bread had a significant effect on 25-hydroxyvitamin D levels [75]. Vitamin D-fortified foods were consumed by around three quarters of Irish children assessed in one study, and they made a significant contribution to their diet, which was otherwise fairly low in vitamin D [76]. The fortification of milk and margarine led to a significant improvement in vitamin D status in preschool children in Finland [77]. Fortified milk was also the main source of vitamin D in Finnish schoolchildren, and milk consumption was consequently the main determinant of vitamin D status in that population [78]. It has been shown that pregnant woman who consumed fortified cereals regularly had significantly higher intakes of folate, iron, zinc and calcium, as well as of vitamins A, C, D and E, and this reduced the risk of inadequate nutrient intakes by 60–90% [79].
12 Micronutrient Deficiency and Obesity
The problem of inadequate nutrient intakes is aggravated by the fact that the micronutrient status of the obese is frequently lower. This is not just due to lower intakes, but also because for some nutrients, such as iron, the low-level inflammation that accompanies obesity seems to reduce absorption [80]. The lower serum levels of 25-hydroxyvitamin D found in overweight and obese subjects compared to their normal-weight counterparts [81] might at least partially be due to increased sequestration of the vitamin in adipose tissue [82]. This effect is increasingly relevant, as obesity rates have doubled globally since 1980, resulting in 1.4 billion overweight adults in 2008 and more than 40 million overweight children under the age of five in 2011 [83]. It has been suggested that the recent increase in the prevalence of inadequate vitamin D status in the U.S. is predominantly attributable to the parallel increase in obesity [84]. While the development of obesity is complex and facilitated by a range of lifestyle and environmental factors, it appears that energy density is crucial [85]. There is mounting evidence that food insecurity contributes to the development of, or at least coexists with, obesity, particularly in situations where food insecurity leads to a disruption of normal eating patterns [86]. This is especially worrying as in 2012 in the U.S. alone, nearly 18 million and 7 million households were classified as food-insecure or even very food-insecure, respectively [87]. According to the authors, these figures had been relatively stable since the marked increase in 2008 following the global economic crisis of that year [87]. Economic constraints were frequently identified as a main driver encouraging consumption of an energy-dense, micronutrient-poor diet [88].
13 Micronutrient Deficiency and Non-communicable Diseases
It is widely accepted that inadequate nutrition during early life increases the risk of developing non-communicable diseases [89]. However, inadequate nutrition affects health at all stages of the life-course, and needs to be addressed accordingly [90]. Prolonged illness frequently dominates the final decade of life [91], which has a detrimental effect on the quality of life [92] and places a heavy burden on the economy due to its chronic nature [93]. This becomes even more important in light of the increasing prevalence of non-communicable diseases in low- and middle-income countries whose health budgets are even more limited than those of more affluent countries [93]. In times of increased financial austerity, the cost of health care is increasingly transferred from the state to the individual [94], further reducing the household budget available for food.
Consequently, affordable diets rich in essential nutrients, whether due to their natural composition or to fortification, have the potential to improve health and quality of life, and to help alleviate some of the pressure on the ever-increasing cost of health care. However, this will only improve nutrition if the general population understands the importance of eating such a diet, and adherence to dietary guidelines is notoriously poor [95]. If individuals were aware of their nutritional status in general or in respect of specific nutrients, they might see the relevance of adjusting their diets: A recent study found that giving people dietary guidance based on information about their genetic profile led to an improvement in nutritional habits [96]. For this to work, reliable, minimally invasive, cheap and quick methods to measure the nutrients level are needed. One example of such a method is the measurement of 25-hydroxyvitamin D levels via dried blood spots: For this, two drops of blood obtained by a finger prick are collected on a special card, dried and sent to a laboratory for analysis. The method has been validated according to the guidelines of the US FDA guidance for Industry and the EMA guidance on bioanalytical method validation. This method was used at a charity event in Heerlen, the Netherlands, and showed that of the people volunteering to participate, 8 and 29% had deficient (<30 nmol/L) or inadequate (31–50 nmol/L) vitamin D levels, respectively (unpublished data).
Another option is that the status of specific nutrients should be routinely assessed by general practitioners, pediatricians and gynecologists, as is the case for hemoglobin for women of reproductive age in some countries. Voluntary testing could also be offered by companies for their employees: Such an initiative, as an example, showed prevalence of inadequate (25–49 nMol/L) and even deficient (<24 nMol/L) levels of 25-hydroxyvitamin D in just below 50 and 21%, respectively. In addition, less than 6% had an omega-3 index in the desirable range (>8%), while 72 and 12% had intermediate (4–8%) or even undesirable (<4%) levels, respectively. The omega-3 index is a measure of docosahexaenoic and eicosapentaenoic acid as percentage of total fatty acids in the membranes of red blood cells and gives an indication of long-term intakes of these [97]. Widespread availability of such services could improve people’s understanding of their own nutritional status and thereby empower them to improve their diet and simultaneously their long-term health.
14 Summary: Key Messages
-
In affluent countries, micronutrient inadequacies are widespread, and intakes of vitamins E, D and A and folate are particularly critical.
-
Vulnerable periods along the life-course, such as pregnancy, infancy or old age, require special attention.
-
Obesity, inadequate micronutrient intake and food insecurity are interrelated, and often co-exist.
-
Poor diet throughout the life-course is a risk factor for the development of non-communicable diseases.
-
Given the difficulties of achieving adequate intakes through diet alone, fortification or supplementation should be considered for specific nutrients for the whole population or groups at increased risk.
-
Improving nutrition could help alleviate the social and financial burden of such diseases.
-
Better knowledge concerning their nutritional status might encourage people to improve their diet and consequently their long-term health.
References
Black, R.E., et al., Maternal and child undernutrition and overweight in low-income and middle-income countries. The Lancet, 2013.
World Health Organization, Global prevalence of vitamin A deficiency in populations at risk 1995–2005, in WHO Global Database on Vitamin A Deficiency. 2009: Geneva.
Wallace, T.C., M. McBurney, and V.L. Fulgoni, Multivitamin/Mineral Supplement Contribution to Micronutrient Intakes in the United States, 2007–2010. Journal of the American College of Nutrition, 2014. 33(2): p. 94–102.
Hilger, J., et al., A systematic review of vitamin D status in populations worldwide. British Journal of Nutrition, 2014. 111(01): p. 23–45.
Wahl, D.A., et al., A global representation of vitamin D status in healthy populations. Archives of Osteoporosis, 2012. 7: p. 155–72.
Elmadfa, I., et al., European nutrition and health report 2009. 2010/02/06 ed. Forum of Nutrition, ed. I. Elmadfa. Vol. 62. 2009, Basel: Karger.
Roman Vinas, B., et al., Projected prevalence of inadequate nutrient intakes in Europe. Ann Nutr Metab, 2011. 59(2–4): p. 84-95.
Cashman, K.D., et al., Vitamin D deficiency in Europe: pandemic? The American Journal of Clinical Nutrition, 2016. 103(4): p. 1033–1044.
Schöttker, B., et al., Vitamin D and mortality: meta-analysis of individual participant data from a large consortium of cohort studies from Europe and the United States. British Medical Journal, 2014. 348: p. g3656.
Grant, W.B., An estimate of the global reduction in mortality rates through doubling vitamin D levels. European Journal of Clinical Nutrition, 2011. 65(9): p. 1016–1026.
Sahota, O., Osteoporosis and the role of vitamin D and calcium-vitamin D deficiency, vitamin D insufficiency and vitamin D sufficiency. Age Ageing, 2000. 29(4): p. 301–4.
Bischoff-Ferrari, H., Vitamin D: What is an adequate vitamin D level and how much supplementation is necessary? Best Practice & Research Clinical Rheumatology, 2009. 23(6): p. 789–795.
Bischoff-Ferrari and Staehelin, Importance of Vitamin D and Calcium at Older Age. International Journal for Vitamin and Nutrition Research, 2008. 78(6): p. 286–292.
Maresz, K., Proper Calcium Use: Vitamin K(2) as a Promoter of Bone and Cardiovascular Health. Integrative Medicine: A Clinician’s Journal, 2015. 14(1): p. 34–39.
Ahmadieh, H. and A. Arabi, Vitamins and bone health: beyond calcium and vitamin D. Nutrition Reviews, 2011. 69(10): p. 584–598.
Deutsche Gesellschaft für Ernährung, et al., Referenzwerte für die Nährstoffzufuhr. 2008, Frankfurt/ Main: Umschau Verlag.
Deutsche Gesellschaft für Ernährung e. V., 12. Ernährungsbericht 2012. 2012, Bonn: Deutsche Gesellschaft für Ernährung e. V.
Institute of Medicine, Dietary reference intakes of vitamin C, vitamin E, selenium, and carotenoids. 2000, Washington, DC: National Academic Press.
Ministry of Health Labour and Welfare (Japan), The Japan National Health and Nutrition Survey 2008. 2008.
Kim, J. and Y.-H. Choi, Physical activity, dietary vitamin C, and metabolic syndrome in the Korean adults: the Korea National Health and Nutrition Examination Survey 2008 to 2012. Public Health, 2016.
Troesch, B., et al., Dietary surveys indicate vitamin intakes below recommendations are common in representative Western countries. British Journal of Nutrition, 2012. 108(4): p. 692–698.
Péter, S., et al., A systematic review of global alpha-tocopherol status as assessed by nutritional intake levels and blood serum concentrations. International Journal for Vitamin and Nutrition Research, 2016. 14: p. 1–21.
Péter, S., et al., The Challenge of Setting Appropriate Intake Recommendations for Vitamin E: Considerations on Status and Functionality to Define Nutrient Requirements. International Journal for Vitamin and Nutrition Research, 2013. 83(2): p. 129–136.
Food and Nutrition Board and Institute of Medicine, Dietary reference intakes of vitamin A, vitamin K, arsenic, boron, chromium, copper, iodine, iron, manganese, molybdenum, nickel, silicon, vanadium, and zinc. 2001, Washington, DC: National Academic Press.
Institute of Medicine, Dietary reference intakes of vitamin A, vitamin K, arsenic, boron, chromium, copper, iodine, iron, manganese, molybdenum, nickel, silicon, vanadium, and zinc. 2001, Washington, DC: National Academic Press.
Max Rubner-Institut, Nationale Verzehrsstudie II. Ergebnisbericht Teil 2. Die bundesweite Befragung zur Ernährung von Jugendlichen und Erwachsenen. 2008 (http://www.was-esse-ich.de/uploads/media/NVSII_Abschlussbericht_Teil_2.pdf) (Accessed 02.07.2011): Karlsruhe.
Lietz, G., et al., Single Nucleotide Polymorphisms Upstream from the β-Carotene 15,15’-Monoxygenase Gene Influence Provitamin A Conversion Efficiency in Female Volunteers. The Journal of Nutrition, 2012. 142: p. 161S-165S.
Grune, T., et al., Beta-carotene is an important vitamin A source for humans. J Nutr, 2010. 140(12): p. 2268S–2285S.
Wu, B.T., et al., Low plasma vitamin B-12 is associated with a lower pregnancy-associated rise in plasma free choline in Canadian pregnant women and lower postnatal growth rates in their male infants. The American Journal of Clinical Nutrition, 2013. 98(5): p. 1209–1217.
Sukumar, N., et al., Prevalence of vitamin B-12 insufficiency during pregnancy and its effect on offspring birth weight: a systematic review and meta-analysis. The American Journal of Clinical Nutrition, 2016.
Gose, M., et al., Trends in food consumption and nutrient intake in Germany between 2006 and 2012: results of the German National Nutrition Monitoring (NEMONIT). British Journal of Nutrition, 2016. 115(Supplement 08): p. 1498–1507.
Blumfield, M.L., et al., Micronutrient intakes during pregnancy in developed countries: Systematic Review and Meta-Analysis. Nutrition Reviews, 2013. 71(2): p. 118–132.
EUROCAT, Special Report: Prevention of Neural Tube Defects by Periconceptual Folic Acid Supplementation in Europe—December 2009. 2009 (http://www.eurocat-network.eu/pagecontent.aspx?pageid=115) (Accessed 04.07.2011), EUROCAT Central Registry, University of Ulster.
Daly, L.E., et al., Folate levels and neural tube defects: Implications for prevention. JAMA, 1995. 274(21): p. 1698–1702.
De-Regil, L.M., et al., Effects and safety of periconceptional folate supplementation for preventing birth defects. The Cochrane database of systematic reviews, 2010(10): p. CD007950-CD007950.
Holzgreve, W., et al., Adding folate to the contraceptive pill: a new concept for the prevention of neural tube defects. The Journal of Maternal-Fetal & Neonatal Medicine, 2012. 25(9): p. 1529–1536.
Ars, C.L., et al., Prenatal folate, homocysteine and vitamin B12 levels and child brain volumes, cognitive development and psychological functioning: the Generation R Study. British Journal of Nutrition, 2016. FirstView: p. 1–9.
Dominguez-Salas, P., et al., Maternal nutrition at conception modulates DNA methylation of human metastable epialleles. Nature Communications, 2014. 5: p. 3746.
Lillycrop, K.A. and G.C. Burdge, Epigenetic mechanisms linking early nutrition to long term health. Best Practice & Research Clinical Endocrinology & Metabolism, 2012. 26(5): p. 667–676.
Khulan, B., et al., Periconceptional maternal micronutrient supplementation is associated with widespread gender related changes in the epigenome: a study of a unique resource in the Gambia. Human Molecular Genetics, 2012. 21(9): p. 2086–2101.
McGarel, C., et al., Emerging roles for folate and related B-vitamins in brain health across the lifecycle. Proceedings of the Nutrition Society, 2015. 74(01): p. 46–55.
Mei, Z., et al., Assessment of iron status in US pregnant women from the National Health and Nutrition Examination Survey (NHANES), 1999–2006. The American Journal of Clinical Nutrition, 2011. 93(6): p. 1312–1320.
Holmes, V.A., et al., Vitamin D deficiency and insufficiency in pregnant women: a longitudinal study. British Journal of Nutrition, 2009. 102(06): p. 876–881.
Gernand, A.D., et al., Micronutrient deficiencies in pregnancy worldwide: health effects and prevention. Nat Rev Endocrinol, 2016. advance online publication.
Hart, P.H., et al., Vitamin D in Fetal Development: Findings From a Birth Cohort Study. Pediatrics, 2015. 135(1): p. e167–e173.
Brough, L., et al., Effect of multiple-micronutrient supplementation on maternal nutrient status, infant birth weight and gestational age at birth in a low-income, multi-ethnic population. British Journal of Nutrition, 2010. 104(03): p. 437–445.
Institute of Medicine, Dietary reference intakes for calcium and vitamin D. DRI—Dietary Reference Intakes, ed. A.C. Ross, et al. 2011, Washington: The National Academies Press.
Deutsche Gesellschaft für Ernährung. Referenzwerte für die Nährstoffzufuhr- Vitamin D (Calciferole). 2012 17. Jan. 2012 17. Jan. 2012]; Available from: http://www.dge.de/modules.php?name=Content&pa=showpage&pid=4&page=12.
Bischoff-Ferrari, H.A., Vitamin D – Role in Pregnancy and Early Childhood. Annals of Nutrition and Metabolism, 2011. 59(1): p. 17–21.
Camargo, C.A., Jr., et al., Cord-blood 25-hydroxyvitamin D levels and risk of respiratory infection, wheezing, and asthma. Pediatrics, 2011. 127(1): p. e180–7.
Nandal, R., et al., Comparison of cord blood vitamin D levels in newborns of vitamin D supplemented and unsupplemented pregnant women: a prospective, comparative study. The Journal of Maternal-Fetal & Neonatal Medicine, 2016. 29(11): p. 1812–1816.
Kovacs, C.S., Vitamin D in pregnancy and lactation: maternal, fetal, and neonatal outcomes from human and animal studies. The American Journal of Clinical Nutrition, 2008. 88(2): p. 520S–528S.
Valentine, C.J. and C.L. Wagner, Nutritional Management of the Breastfeeding Dyad. Pediatric Clinics of North America, 2013. 60(1): p. 261–274.
Deutsche Gesellschaft für Ernährung e. V., Verzehrsstudie zur Ermittlung der Lebensmittelaufnahme von Säuglingen und Kleinkindern (VELS), in Ernährungsbericht 2008. 2008, Deutsche Gesellschaft für Ernährung e. V.: Bonn. p. 53–60.
Streym, S.v., et al., Vitamin D content in human breast milk: a 9-mo follow-up study. 2016, American Society for Clinical Nutrition, Inc. p. 107.
Thiele, D.K., J.L. Senti, and C.M. Anderson, Maternal Vitamin D Supplementation to Meet the Needs of the Breastfed Infant: A Systematic Review. Journal of Human Lactation, 2013. 29(2): p. 163–170.
Blomquist, H.K., et al., Dietary intake of vitamin D during the second half of infancy in Swedish infants. Scandinavian Journal of Nutrition, 2004. 48(4): p. 173–177.
Ziegler, E.E., S.E. Nelson, and J.M. Jeter, Vitamin D supplementation of breastfed infants: a randomized dose-response trial. Pediatr Res, 2014. 76(2): p. 177–83.
Perrine, C.G., et al., Adherence to vitamin D recommendations among US infants. Pediatrics, 2010. 125(4): p. 627–32.
Hilger, J., et al., Micronutrient Intake in Healthy Toddlers: A Multinational Perspective. Nutrients, 2015. 7(8): p. 6938–6955.
Devaney, B., et al., Nutrient intakes of infants and toddlers. J Am Diet Assoc, 2004. 104(1 Suppl 1): p. s14–21.
Decarli, B., C. Cavadini, and P.A. Michaud, Habitudes alimentaires et ingestats de nutriments d’un groupe d’adolescents vaudois de 9 à 19 ans, in Fünfter Schweizer Ernährungsbericht, M. Eichholzer, et al., Editors. 2005, Bundesamt für Gesundheit: Bern. p. 133–150.
Bailey, R.L., et al., Do Dietary Supplements Improve Micronutrient Sufficiency in Children and Adolescents? The Journal of Pediatrics, 2012. 161(5): p. 837–842.e3.
Micha, R., et al., Global, regional, and national consumption levels of dietary fats and oils in 1990 and 2010: a systematic analysis including 266 country-specific nutrition surveys. BMJ, 2014. 348.
Papanikolaou, Y., et al., U.S. adults are not meeting recommended levels for fish and omega-3 fatty acid intake: results of an analysis using observational data from NHANES 2003–2008. Nutrition Journal, 2014. 13(1): p. 31.
Aranceta, J. and C. Pérez-Rodrigo, Recommended dietary reference intakes, nutritional goals and dietary guidelines for fat and fatty acids: a systematic review. British Journal of Nutrition, 2012. 107(SupplementS2): p. S8-S22.
Elia, M., et al., The cost of disease-related malnutrition in the UK and economic considerations for the use of oral nutritional supplements (ONS) in adults, M. Elia, Editor. 2006, British Association for Parenteral and Enteral Nutrition: Redditch, UK.
Marriott, B.P., et al., Intake of Added Sugars and Selected Nutrients in the United States, National Health and Nutrition Examination Survey (NHANES) 2003—2006. Critical Reviews in Food Science and Nutrition, 2010. 50(3): p. 228–258.
ter Borg, S., et al., Micronutrient intakes and potential inadequacies of community-dwelling older adults: a systematic review. British Journal of Nutrition, 2015. 113(08): p. 1195–1206.
Deutsche Gesellschaft für Ernährung e. V., Ernährung älterer Menschen in stationären Einrichtungen (ErnSTES-Studies), in Ernährungsbericht 2008. 2008, Deutsche Gesellschaft für Ernährung e. V.: Bonn. p. 157–204.
Lengyel, C.O., S.J. Whiting, and G.A. Zello, Nutrient inadequacies among elderly residents of long-term care facilities. Can J Diet Pract Res, 2008. 69(2): p. 82–8.
Sebastian, R.S., et al., Older adults who use vitamin/mineral supplements differ from nonusers in nutrient intake adequacy and dietary attitudes. Journal of the American Dietetic Association, 2007. 107(8): p. 1322–32.
Fabian, E., et al., Vitamin status in elderly people in relation to the use of nutritional supplements. The Journal of Nutrition, Health & Aging, 2012. 16: p. 206–212.
Freisling, H., et al., Region-specific nutrient intake patterns exhibit a geographical gradient within and between European countries. J Nutr, 2010. 140(7): p. 1280–6.
Black, L.J., et al., An Updated Systematic Review and Meta-Analysis of the Efficacy of Vitamin D Food Fortification. The Journal of Nutrition, 2012. 142(6): p. 1102–1108.
Hennessy, Á., et al., The role of fortified foods and nutritional supplements in increasing vitamin D intake in Irish preschool children. European Journal of Nutrition, 2016: p. 1–13.
Piirainen, T., K. Laitinen, and E. Isolauri, Impact of national fortification of fluid milks and margarines with vitamin D on dietary intake and serum 25-hydroxyvitamin D concentration in 4-year-old children. Eur J Clin Nutr, 2007. 61(1): p. 123–128.
Soininen, S., et al., Determinants of serum 25-hydroxyvitamin D concentration in Finnish children: the Physical Activity and Nutrition in Children (PANIC) study. British Journal of Nutrition, 2016. 115(06): p. 1080–1091.
Snook Parrott, M., et al., Maternal cereal consumption and adequacy of micronutrient intake in the periconceptional period. Public Health Nutrition, 2009. 12(08): p. 1276–1283.
Cepeda-Lopez, A.C., I. Aeberli, and M.B. Zimmermann, Does obesity increase risk for iron deficiency? A review of the literature and the potential mechanisms. International Journal for Vitamin and Nutrition Research, 2010. 80(4–5): p. 263–70.
Samuel, L. and L.N. Borrell, The effect of body mass index on optimal vitamin D status in U.S. adults: the National Health and Nutrition Examination Survey 2001–2006. Ann Epidemiol, 2013. 23(7): p. 409–14.
Wortsman, J., et al., Decreased bioavailability of vitamin D in obesity. The American Journal of Clinical Nutrition, 2000. 72(3): p. 690–693.
World Health Organization. Fact sheet N° 311: Obesity and overweight. 2014 March 2014 May 02, 2014]; Available from: http://www.who.int/mediacentre/factsheets/fs311/en/.
Ganji, V., X. Zhang, and V. Tangpricha, Serum 25-Hydroxyvitamin D Concentrations and Prevalence Estimates of Hypovitaminosis D in the U.S. Population Based on Assay-Adjusted Data. The Journal of Nutrition, 2012. 142(3): p. 498–507.
Prentice, A.M. and S.A. Jebb, Fast foods, energy density and obesity: a possible mechanistic link. Obesity Reviews, 2003. 4(4): p. 187–194.
Martin-Fernandez, J., et al., Food insecurity, a determinant of obesity?—An analysis from a population-based survey in the paris metropolitan area, 2010. Obesity Facts, 2014. 7(2): p. 120–129.
Coleman-Jensen, A., M. Nord, and A. Singh, Household Food Security in the United States in 2012. 2013, U.S. Department of Agriculture, Economic Research Service.
Drewnowski, A. and N. Darmon, The economics of obesity: dietary energy density and energy cost. Am J Clin Nutr, 2005. 82(1 Suppl): p. 265S–273S.
Plagemann, A., et al., Early postnatal life as a critical time window for determination of long-term metabolic health. Best Practice & Research Clinical Endocrinology & Metabolism, 2012. 26(5): p. 641–653.
World Health Organization, WHO global status report on noncommunicable diseases 2010, W. Press, Editor. 2010: Geneva, Switzerland.
Lunenfeld, B., An aging world – demographics and challenges. Gynecological Endocrinology, 2008. 24(1): p. 1–3.
Beaglehole, R., et al., Priority actions for the non-communicable disease crisis. The Lancet, 2011. 377(9775): p. 1438–1447.
Adeyi, O., O. Smith, and S. Robles, Public policy and the challenge of chronic noncommunicable diseases, ed. W. Bank. 2007, Washington, DC.
Burke, S., et al., Indicators of health system coverage and activity in Ireland during the economic crisis 2008–2014—From ‘more with less’ to ‘less with less’. Health Policy, 2014 epub(0).
Krebs-Smith, S.M., et al., Americans Do Not Meet Federal Dietary Recommendations. The Journal of Nutrition, 2010. 140(10): p. 1832–1838.
Nielsen, D.E. and A. El-Sohemy, Disclosure of Genetic Information and Change in Dietary Intake: A Randomized Controlled Trial. PLoS ONE, 2014. 9(11): p. e112665.
Harris, W.S. and C. von Schacky, The Omega-3 Index: a new risk factor for death from coronary heart disease? Preventive Medicine, 2004. 39(1): p. 212–220.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2017 Springer International Publishing AG
About this chapter
Cite this chapter
Troesch, B. (2017). Micronutrient Status in Affluent Societies. In: Biesalski, H., Drewnowski, A., Dwyer, J., Strain, J., Weber, P., Eggersdorfer, M. (eds) Sustainable Nutrition in a Changing World. Springer, Cham. https://doi.org/10.1007/978-3-319-55942-1_11
Download citation
DOI: https://doi.org/10.1007/978-3-319-55942-1_11
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-319-55940-7
Online ISBN: 978-3-319-55942-1
eBook Packages: Chemistry and Materials ScienceChemistry and Material Science (R0)