
Abstract
Fibrohistiocytic lesions represent an assortment of soft tissue neoplasms in which the constitutive cells have histologic features of both fibroblasts and macrophages. The fibroblastic-appearing cells typically have elongated and spindled nuclei and are arranged in a streaming pattern (Fig. 6.1a). Cells with a more histiocytic appearance are less organized and have a “foamy” cytoplasm (Fig. 6.1b) [1].
Access provided by CONRICYT-eBooks. Download chapter PDF
Similar content being viewed by others



Keywords
- Fibrohistiocytic lesions
- Fibrous histiocytoma
- Neurofibroma
- Solitary xanthogranuloma
- Tenosynovial giant cell tumor

(a) Spindle fibrous-like cells in a fibrous histiocytoma. (b) Histiocytic-appearing cells in a fibrous histiocytoma
6.1 Fibrous Histiocytoma
Fibrous histiocytoma, otherwise referred to as dermatofibroma , typically arises as a skin lesion in the extremities of adults between the second and fourth decades of life [2]. These clinically present as elevated and sometimes pigmented lesions that are usually less than 1 cm in diameter [3]. Approximately a third of affected patients can have multiple lesions, which have been reported to sometimes occur in patients who are immunosuppressed [4]. Rarely, benign fibrous histiocytomas can present as deeper lesions in the subcutaneous or soft tissue that are several centimeters in size [5]. These deep fibrous histiocytomas have been noted to occur at any age [6].
Pathology
Cutaneous fibrous histiocytomas are usually centered in the dermis and are composed of haphazardly arranged cells with fibrous and histiocytic features that percolate between dense sclerotic collagen fibers (Figs. 6.2 and 6.3). Scattered foamy histiocytes and multinucleated giant cells can be identified. There is typically only limited extension into the underlying subcutaneous adipose tissue [1].

Cutaneous fibrous histiocytoma containing cells with a fibrohistiocytic appearance

At the periphery of this fibrous histiocytoma , the cells percolate in between dense collagen fibers
The less frequent deep fibrous histiocytomas are more circumscribed. Microscopically, these neoplasms are typically cellular and can exhibit a more organized fascicular arrangement. Prominent branching vessels, similar to solitary fibrous tumor, can be identified (Fig. 6.4) [6].

Deep fibrous histiocytoma with a branching vascular pattern
Histologic Variants
-
Cellular fibrous histiocytoma —The cells in cellular fibrous histiocytoma show increased cellularity with a more organized fascicular arrangement (Fig. 6.5) [7].
Fig. 6.5 
Cellular fibrous histiocytoma with fascicles of spindle cells
-
Aneurysmal fibrous histiocytoma —This variant of fibrous histiocytoma has central blood-filled spaces with associated hemosiderin deposition (Fig. 6.6) [8].
Fig. 6.6 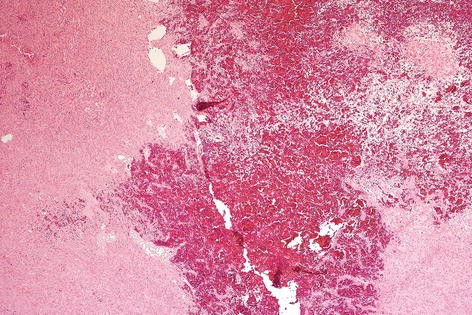
Aneurysmal fibrous histiocytoma with cells surrounding a central pool of blood


Ancillary Studies
-
Although neither sensitive nor specific, fibrous histiocytomas are often positive for Factor XIIIa and lack significant staining for CD34.
Differential Diagnosis
-
Dermatofibrosarcoma protuberans
-
Leiomyoma
-
Neurofibroma
Comments
-
1.
Fibrous histiocytoma can sometimes be difficult to distinguish from dermatofibrosarcoma protuberans, which is a more aggressive neoplasm.
-
2.
Dermatofibrosarcoma protuberans extensively infiltrates into the underlying subcutaneous adipose tissue.
-
3.
If the morphologic features are ambiguous, immunohistochemical stains for CD34 and Factor XIIIa can be helpful, as dermatofibrosarcoma protuberans is frequently strongly positive for CD34 and negative for Factor XIIIa.
-
4.
FISH studies can exclude dermatofibrosarcoma protuberans by confirming the absence of the COL1A-PDGFB fusion transcript.
-
5.
Fibrous histiocytoma can be confused with other dermal-based spindle cell lesions, such as neurofibroma or leiomyoma. Fibrous histiocytoma lacks the S100 or SOX-10 staining found in neurofibroma, or the desmin staining found in leiomyoma.
-
6.
Fibrous histiocytomas are benign neoplasms and are treated with conservative surgical resection. Once excised, they rarely recur [1].
-
7.
Cellular fibrous histiocytoma and aneurysmal fibrous histiocytoma have increased rates (26% and 19%, respectively) of recurrence following excision [7, 8].
-
8.
Deep fibrous histiocytomas recur in approximately 20% of cases.
6.2 Solitary Xanthogranuloma
Solitary xanthogranuloma often occurs in children (sometimes referred to as juvenile xanthogranuloma ) but can also be seen in adults. These most commonly present as dermal lesions that frequently arise in the head and neck or trunk as skin papules. In occasional cases (particularly in very young children), patients can have multiple lesions arising on the skin and even organ involvement, such as the eye [9].
Pathology
Histologically, a solitary xanthogranuloma is composed of a dermal concentration of cells with eosinophilic or foamy cytoplasm that extends up to the epidermis and around associated adnexal structures (Fig. 6.7). Characteristic giant cells with peripherally arranged nuclei (Touton giant cells ) are present (Fig. 6.8). Associated inflammatory cells can also be identified [9, 10].

Solitary xanthogranuloma with foamy histiocytic cells centered in the dermis

Touton giant cells (arrow) with peripherally arranged nuclei in a solitary xanthogranuloma
Ancillary Studies
-
Although not specific, solitary xanthogranulomas are positive for CD68, a stain that highlights histiocytes.
-
They are negative for S100 and CD1a immunohistochemical stains.
Differential Diagnosis
-
Langerhans cell histiocytosis
-
Xanthoma
-
Fibrous histiocytoma
Comments
-
1.
Solitary xanthogranuloma can mimic other histiocytic-appearing neoplasms, such as Langerhans cell histiocytosis, xanthoma, or fibrous histiocytoma.
-
2.
Unlike solitary xanthogranuloma, Langerhans cell histiocytosis is positive for S100 and CD1a immunohistochemical stains.
-
3.
Xanthomas contain cells that are consistently foamy in appearance.
-
4.
Fibrous histiocytoma typically contains less foamy cells and Touton giant cells and usually manifests a more prominent population of spindle cells.
-
5.
Dermal solitary xanthogranulomas are benign lesions. Excision is curative in over 80% of cases. Lesions that are incompletely excised often regress [9].
-
6.
The prognosis is much more concerning in patients who have systemic involvement by xanthogranulomas , as young patients with organ involvement can die of disease. These patients are often treated with chemotherapy [1, 11].
6.3 Tenosynovial Giant Cell Tumor, Localized Type
Tenosynovial giant cell tumor, localized type, otherwise known as giant cell tumor of the tendon sheath (localized type) is a well-circumscribed benign lesion that occurs in adults between the fourth and sixth decade of life. These lesions arise in the hands or feet, typically close to the interphalangeal joints or synovium of the tendon sheath [6, 12, 13].
Pathology
Grossly, these tumors are well circumscribed and lobulated. The microscopic sections show mononuclear cells with eosinophilic cytoplasm, osteoclast-like giant cells, and foamy histiocytes (Figs. 6.9 and 6.10). Hemosiderin pigment can be identified [12].


Multinucleated giant cells and associated mononuclear cells with eosinophilic cytoplasm in tenosynovial giant cell tumor, localized type.
Ancillary Studies
-
The cells can stain for CD68 and desmin, but this is rarely used for diagnosis.
Differential Diagnosis
-
Tenosynovial giant cell tumor, diffuse type
-
Fibroma of tendon sheath
Comments
-
Tenosynovial giant cell tumor, localized type, is distinguished from tenosynovial giant cell tumor, diffuse type by its well-circumscribed border and lack of infiltration into adjacent tissue.
-
These are benign lesions. Approximately 10% will recur following excision [14].
6.4 Tenosynovial Giant Cell Tumor, Diffuse Type
Tenosynovial giant cell tumor, diffuse type, otherwise known as pigmented villonodular tenosynovitis (PVNS) , often occurs in the articular space of the knee or hip in patients less than 40 years old [15]. These tumors can also arise as predominantly soft tissue masses in the wrist, knee, thigh, and foot [16]. They are more aggressive than their localized counterpart and present with swelling and tenderness of the affected joint [3].
Pathology
This type of giant cell tumor is not well circumscribed and often has a sheetlike or villous architecture (Fig. 6.11). Similar to tenosynovial giant cell tumor, localized type, the sections show mononuclear cells with eosinophilic cytoplasm and multinucleated giant cells. Hemosiderin deposition, foamy histiocytes, chronic inflammation, and fibrosis can also be present (Fig. 6.12).

Tenosynovial giant cell tumor, diffuse type, showing a villous-like architecture

Mononuclear cells with hemosiderin deposition in a tenosynovial giant cell tumor, diffuse type
Ancillary Studies
-
Similar to tenosynovial giant cell tumor, localized type, the cells can be positive for CD68.
Differential Diagnosis
-
Undifferentiated high-grade pleomorphic sarcoma
-
Synovial sarcoma
-
Tenosynovial giant celltumor, localized type
Comments
-
1.
The numerous giant cells in a tenosynovial giant cell tumor, diffuse type, can cause concern for a high-grade sarcoma such as undifferentiated pleomorphic sarcoma. Tenosynovial giant cell tumor typically does not contain the nuclear atypia seen in these high-grade malignancies.
-
2.
The intimate association of tenosynovial giant cell tumor with residual synovium in a joint can mimic a synovial sarcoma. However, synovial sarcoma would demonstrate positivity with cytokeratin or TLE-1 immunohistochemical stains.
-
3.
Clinically, the localized type of tenosynovial giant cell tumor is more circumscribed and usually involves the smaller joints of the hands and feet.
-
4.
Tenosynovial giant cell tumor, diffuse type, can recur in 20–60% of cases.
-
5.
The primary treatment is complete surgical excision, as incompletely resected tumors are more likely to recur. Synovectomy is often performed for intra-articular tumors and wide excision is typically performed for extra-articular lesions [3, 13].
Facts to Remember
-
1.
Fibrous histiocytoma is typically a benign cutaneous neoplasm which is composed of fibrous and histiocytic cells. Cellular and aneurysmal fibrous histiocytoma variants have a higher incidence of recurrence.
-
2.
Solitary xanthogranuloma is typically a benign dermal lesion which can affect both children and adults. Patients with systemic solitary xanthogranulomas with organ involvement have a poorer prognosis and may require systemic chemotherapy.
-
3.
Tenosynovial giant cell tumor, localized type, is a benign neoplasm that primarily affects the tendons of the hands and feet. Only a limited number of these neoplasms will recur.
-
4.
Tenosynovial giant cell tumor, diffuse type, can be intra-articular or extra-articular. Intra-articular lesions usually arise in spaces of the larger joints, such as the knees and hips. Recurrence in these tumors is more frequent, and the focus should be on complete excision.
References
Goldblum J, Weiss S, Folpe AL, editors. Enzinger and Weiss’s soft tissue tumors. 6th ed. Philadelphia: Elsevier; 2013.
Gonzalez S, Duarte I. Benign fibrous histiocytoma of the skin. A morphologic study of 290 cases. Pathol Res Pract. 1982;174(4):379–91.
Hornick JL, editor. Practical soft tissue pathology: a diagnostic approach. Philadelphia: Saunders; 2013.
Newman DM, Walter JB. Multiple dermatofibromas in patients with systemic lupus erythematosus on immunosuppressive therapy. N Engl J Med. 1973;289(16):842–3.
Gleason BC, Fletcher CD. Deep “benign” fibrous histiocytoma: clinicopathologic analysis of 69 cases of a rare tumor indicating occasional metastatic potential. Am J Surg Pathol. 2008;32(3):354–62.
Fletcher CDM, Bridge JA, Hogendoorn PC, Mertens F, editors. Pathology and genetics of tumours of soft tissue and bone. 4th ed. Lyon: World Health. Organization; 2013.
Calonje E, Mentzel T, Fletcher CD. Cellular benign fibrous histiocytoma. Clinicopathologic analysis of 74 cases of a distinctive variant of cutaneous fibrous histiocytoma with frequent recurrence. Am J Surg Pathol. 1994;18(7):668–76.
Calonje E, Fletcher CD. Aneurysmal benign fibrous histiocytoma: clinicopathological analysis of 40 cases of a tumour frequently misdiagnosed as a vascular neoplasm. Histopathology. 1995;26(4):323–31.
Janssen D, Harms D. Juvenile xanthogranuloma in childhood and adolescence: a clinicopathologic study of 129 patients from the Kiel pediatric tumor registry. Am J Surg Pathol. 2005;29(1):21–8.
Tahan SR, Pastel-Levy C, Bhan AK, Mihm Jr MC. Juvenile xanthogranuloma. Clinical and pathologic characterization. Arch Pathol Lab Med. 1989;113(9):1057–61.
Dehner LP. Juvenile xanthogranulomas in the first two decades of life: a clinicopathologic study of 174 cases with cutaneous and extracutaneous manifestations. Am J Surg Pathol. 2003;27(5):579–93.
Monaghan H, Salter DM, Al-Nafussi A. Giant cell tumour of tendon sheath (localised nodular tenosynovitis): clinicopathological features of 71 cases. J Clin Pathol. 2001;54(5):404–7.
Ushijima M, Hashimoto H, Tsuneyoshi M, Enjoji M. Giant cell tumor of the tendon sheath (nodular tenosynovitis). A study of 207 cases to compare the large joint group with the common digit group. Cancer. 1986;57(4):875–84.
Williams J, Hodari A, Janevski P, Siddiqui A. Recurrence of giant cell tumors in the hand: a prospective study. J Hand Surg [Am]. 2010;35(3):451–6.
Myers BW, Masi AT. Pigmented villonodular synovitis and tenosynovitis: a clinical epidemiologic study of 166 cases and literature review. Medicine (Baltimore). 1980;59(3):223–38.
Somerhausen NS, Fletcher CD. Diffuse-type giant cell tumor: clinicopathologic and immunohistochemical analysis of 50 cases with extraarticular disease. Am J Surg Pathol. 2000;24(4)
Author information
Authors and Affiliations
Rights and permissions
Copyright information
© 2017 Springer International Publishing AG
About this chapter
Cite this chapter
Perry, K. (2017). Fibrohistiocytic Lesions. In: Soft Tissue Pathology for Clinicians. Pathology for Clinicians. Springer, Cham. https://doi.org/10.1007/978-3-319-55654-3_6
Download citation
DOI: https://doi.org/10.1007/978-3-319-55654-3_6
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-319-55653-6
Online ISBN: 978-3-319-55654-3
eBook Packages: MedicineMedicine (R0)