
Abstract
The interoperability of Electronic Health Records (EHR) and Clinical Decision Support (CDS) systems is a major challenge in the medical informatics field. International initiatives propose the use of ontologies for bridging both types of systems. The next-generation of EHR and CDS systems are supposed to use ontologies, or at least ontologies should be fundamental for enabling their interoperability. This situation makes necessary to analyze if current ontologies are ready for playing such intended role. In this paper we describe and discuss some important issues that need to be solved in order to have optimal ontologies for such a purpose, such as the need for increasing reuse in ontologies, as well as getting axiomatically richer ontologies. We also describe how our recent research results in the areas of ontology enrichment and ontology evaluation may contribute to such a goal.
Access provided by CONRICYT-eBooks. Download conference paper PDF
Similar content being viewed by others


Keywords
- Electronic Health Records
- Clinical decision-support systems
- Semantic interoperability
- Ontology quality
- Ontology enrichment
1 Introduction
Humans have been interested in recording information about patient care for many years and even centuries (see for instance [6, 13]). The development of the information and communication technologies has permitted to store and exchange the medical information in electronic formats, which has generated new opportunities for improving clinical research and the quality of health care.
Two relevant types of medical information systems are Electronic Health Records (EHR) and Clinical Decision Support (CDS). EHR systems provide the means for storing the medical information generated by the interactions of patients with the health system. In the most generic way, the EHR of a patient should provide access to all the medical information of the patient, that is, from all the healthcare institutions in which the patient has received care. Unfortunately, this is not possible due to the lack of interoperability between different EHR systems. CDS systems try to help physicians in the diagnosis and treatment of patients, basically by combining the medical knowledge with the patient data. Consequently, CDS systems should have access to the content of the EHR and, similarly, to have access to the recommendations of CDS systems from the EHR system would be helpful for physicians.
As it will be described in Sect. 2, there has been a significant evolution of EHR and CDS systems, but such evolution has not achieved an effective communication between those systems. The interoperability of EHR and CDS systems is indeed an existing challenge for the medical informatics community and it has been the subject of reports of international efforts and initiatives such as Semantic HealthNet (SHN)Footnote 1.
In the last years, the Semantic Web technologies have gained popularity in the pursuit of the semantic interoperability of health information systems, especially since the Semantic Health project [17] recommended the use of ontologies for supporting semantic interoperability in healthcare. The Semantic Web [4] is a natural space for data integration based on shared meaning [12] in which the shared models of meaning are provided by ontologies. SHN also proposes that ontological formalization should be fundamental for enabling a meaningful exchange and cooperation between EHR and CDS systems. The meaningful exchange between EHR and CDS systems also imposes a series of requirements on biomedical ontologies related to knowledge representation, data retrieval and classification.
In this paper, we examine how current biomedical ontologies meet such requirements, which will determine to what extent current biomedical ontologies are useful for bridging between EHR and CDS systems. Besides, we describe two frameworks developed by our research group that contribute to increase the usefulness of biomedical ontologies. We believe that these frameworks can be part of the solution but additional actions are also required. We believe that this work permits to gain knowledge on the types of actions that will make possible the effective ontology-based interoperability of EHR and CDS systems.
2 Background
In this section we provide an overview of the evolution of EHR and CDS systems, including how the interaction between ontologies and such systems has been addressed in the last years.
2.1 EHR Systems
The first experiences of electronic medical records happened in the sixties, when the Akron Children’s hospital and IBM collaborated to develop a computer-based patient information system [32] with the aim of centralising medical information, sharing information and reducing paperwork. Since then, EHR systems have evolved in many different ways, and today we can see how physicians can input or have access to the patient records by using tablets or smartphones [21]. This is clearly an advance in the way of interacting with the EHR content, but its real impact depends on what can be effectively done from such modern interfaces. Computer-based records share with paper-based ones the heterogeneity in structure and content, which makes difficult for computers to understand and to process the content of the EHR, and so limiting the practical usefulness of EHR systems.
The information architecture of EHR systems is fundamental for the useful exploitation of EHR data, and there has also been an evolution in the architecture of EHR systems in the last decades. EHR systems have been studied as a subsystem of knowledge management [20]. From such perspective, four generations of systems can be distinguished. The first generation did not include any possibility for representing knowledge. The systems from the second generation started to provide some capabilities for knowledge representation. The integration with clinical decision and the availability of purpose-specific knowledge bases started to happen in the third generation. Finally, the fourth generation uses formal knowledge representation languages.
From an information architecture point of view, the early EHR systems followed the single-level methodological approach. In a single-level approach, the medical experts discuss with the software engineers the requirements and needs of the EHR systems, and all the medical knowledge is implemented in the EHR system. In this context, implemented has to be understood as hard-coded, since in most cases the medical knowledge was fixed in the system, and updating the knowledge usually requires major implementation changes in the EHR system. This is obviously a suboptimal decision given the current progress of science and medicine, which requires EHR systems capable to work in a context of dynamic, evolving knowledge.
In the nineties, the Good European Health Record (GEHR) project [14], funded by European Health Telematics research, had as main objective to achieve a generic representation of EHR data that would enable data exchange between EHR systems. Its most popular result was the dual-level methodology for the development of EHR systems. This methodology innovates in the relation between the medical knowledge and the EHR system, because now the EHR system uses the medical knowledge, but this is not hard-coded into the system. This means that the knowledge can be updated without requiring major implementation changes. This architecture has inspired the development of specifications and standards such as openEHRFootnote 2, ISO 13606Footnote 3 or HL7 CDAFootnote 4. This is the architecture of the next generation of EHR systems, which is based on standards.
The dual-level methodology uses two modelling levels: information and knowledge. The information level provides the modeling primitives for representing, storing and exchanging EHR data. The knowledge level provides the clinical models, which define data structures that will be used for capturing the EHR data in a particular scenario. By clinical model we refer to artifacts such as archetypes [3], CEMsFootnote 5, FHIR resourcesFootnote 6 or CIMI modelsFootnote 7, since they are the technological solution for the knowledge level proposed by the different specifications. The clinical models facilitate the meaningful exchange of EHR data between systems, because the meaning of the data captured is provided by means of links to semantic resources. For simplicity, we focus next on archetypes.
Archetypes contain a terminology (formerly ontology) section, which is used to provide the specific meaning to the information. In this section we may define that the valid values for the field “blood phenotype” is a query over SNOMED CTFootnote 8. Such association is described using an archetype constraint. This constraint is a query that would show the user all the SNOMED CT concepts that are the result of the query. However, once the corresponding code is chosen, it is stored and used in the EHR system as a code, since the technologies used in archetypes-based systems are not able to natively exploit the semantics of resources such as SNOMED CT. This situation is not exclusive for archetypes, but it also happens with other types of clinical models. The answer to such semantic limitation provided by a part of the research community has been to propose the use of semantic formalisms, such as the Web Ontology Language (OWL) as the common formalism for expressing the reference model, the clinical information models and the semantic resources used by the former ones [18, 19, 34].
2.2 CDS Systems
The history of computerized clinical decision support (CDS) systems also starts in the late fifties/early sixties. The Warner system [37] was one of the earliest decision support systems, developed for the diagnosis of congenital heart disease using data from more than 1000 patients. The increasing complexity of medical knowledge and the amount and types of information sources needed to support clinical decisions has driven the evolution of CDS systems, with the traditional objective of having the EHR as the reference source of information. In [39], the evolution of CDS systems is described using four phases of evolution: (1) stand-alone systems, which are independent of the EHR system; (2) integrated systems, which are integrated into clinical information systems, but not necessarily with the EHR; (3) standards-based systems, which include the use of standards to represent, encode, store and share knowledge; and (4) service models, in which CDS and EHR are connected through interfaces. The last two phases are the most relevant ones for our purpose because they describe a context in which CDS systems are based on standards and provide ways for communicating and exchanging information. If we focus on computerized clinical guidelines, a series of languages and frameworks such as Arden [1], GLIF [23] or PROForma [11] have been proposed in the last decades. They provide ways for expressing clinical knowledge, expressing and executing clinical guidelines, but they cannot easily be connected with the EHR. One of the main reasons was identified in [15]: “The inclusion of a guideline-based system into an existing electronic medical record system is hard because they are designed as a closed monolithic system with a lack of interoperability methods.” Basically, this means that despite EHR and CDS systems use standards to represent the medical knowledge required, such standards are not really interoperable, which limits the joint operation of EHR and CDS systems.
Recently, the Guideline Definition Language (GDL) [7] was proposed by the openEHR Foundation to palliate this situation. GDL is a formal language for expressing decision support logic, and closely related to the openEHR Reference Model (RM) and Archetype Model (AM). GDL proposes to specify the decision support logic using the entities provided by the openEHR RM and AM. Consequently, the queries described in the guideline would be compatible with the structure of the EHR and, therefore, CDS systems could effectively reuse the EHR data.
In Sect. 2.1 we have mentioned that EHR standards based on archetypes are limited in the processing of the semantics associated with the data and the clinical information models. The logic included in the guidelines may need to perform inferences, which requires to be able to exploit the semantics of all the information involved. Consequently, to date, approaches such as GDL keep having the drawback of their limited exploitation of the semantics of the resources used for providing the meaning to the data.
Ontologies have been used in CDS systems in the last years. In the nineties, ontologies were already used to support protocol-based decisions [36], and we can find a number of papers with related use since then [5, 10, 22, 40]. The specification of guidelines was also approached using ontologies, see for instance [31]. More recently, ontologies have been proposed to drive the execution of the guideline [16], and to mediate between the guideline and the medical knowledge [38]. However, none of them solve the integration of EHR and CDS systems. Interestingly, according to the results of the review presented in [24], the integration of clinical guidelines with the EHR has not been one of the most active areas in the period 2001–2013.
3 Ontologies in the Interface EHR-CDS
The evolution of EHR and CDS systems reveals that ontologies are gaining momentum. This is supported by the fact that clinical models may use ontologies for providing the semantics to the data, the existing experiences in the use of ontologies and semantic web technologies for representing clinical models and EHR data, and that ontologies have been used for modelling and driving the execution of computerized clinical guidelines. However, the integration of EHR and CDS systems remains unsolved.
We could ask ourselves whether ontologies could be an effective bridge for EHR and CDS systems. This question is not novel, since the central role of ontologies for connecting EHR and CDS systems has been proposed ealier. [29] describes the relations between the patient data model (information model), the concept model (ontology), and the guideline model (inference model). This vision proposes that clear interfaces between these models are required in order to get interoperability between EHR and CDS systems. Moreover, an interface between the three models is also needed. Whereas ontologies provide the static domain knowledge, guidelines provide the dynamic one, which means that both should use the same building blocks, and share the same concepts, that is, use a common knowledge model.
[29] makes a statement that reinforces the role of ontologies in the interface EHR-CDS: “The concept model should be capable of classifying the information of the medical record under the abstractions used in the guideline”. A practical interpretation of this statement is that if the medical record contains a blood pressure measurement of an individual of 190/110 and the guideline manages the concept “elevated blood pressure”, then the concept model (ontology) should be capable of classifying that individual as a “person with elevated blood pressure”. Consequently, the ontology would be the bridge between the EHR data and the CDS knowledge.
Semantic HealthNet (SHN)Footnote 9 has been an EU FP7 Network of Excellence which has run in the period 2011–2015. SHN identified four major axes of activity for the “consistent representation, access and interpretation” of health data: (1) data and record structure and content; (2) workflow; (3) terminology systems; and (4) privacy. An analysis of the content of each axe shows a close relation between the first three ones and the models proposed in [29]. The SHN deliverablesFootnote 10 4.4 and 4.5 also contain some statements reinforcing the role of ontologies in the interface EHR-CDS:
-
The information model must hold the patient information necessary to determine whether certain clinical guidelines criteria are satisfied.
-
Clinical models and clinical guidelines must share the same ontology for representing their concepts.
-
Guideline creators should map their non-standardized vocabularies to standardized ontologies.
-
The elements of clinical models should be mapped to standardized ontologies and used in the guidelines.
The potential role of ontologies as a bridge between EHR and CDS systems has been described in previous sections. This helps us to understand the usefulness of an ontology in this context, which we approach as to what extent a given ontology may play such role. Given that bridging between EHR and CDS can be too generic, the following specific requirements for usefulness can be identified:
-
1.
Representation, sharing and reuse of knowledge for information and inference models.
-
2.
Classification of EHR data according to guideline rules.
-
3.
EHR data retrieval according to guideline rules.
-
4.
Quality-assured ontology.
The first three requirements can be drawn from the content of the previous sections, but the fourth one comes from the need of using quality-proof artifacts in legacy health information systems. In the remaining of this section, an analysis of the usefulness of current biomedical ontologies is performed. The results of such analysis will be the input for revising and proposing methods for increasing the usefulness of ontologies.
Performing a systematic analysis of ontologies requires to define, measure and evaluate a series of indicators that would capture our intended meaning of usefulness. The ontology engineering community has not been able to reach a consensus on a series of metrics that should be used for the analysis of a given ontology. The number of classes, properties, axioms, labels, or the visits to the ontology are some indicators that have been traditionally measured and evaluated in ontologies, although they do not generate enough information for our purpose. Initiatives such as the OBO Foundry [33] have proposed a series of good design principles for biomedical ontologies. Among such criteria we can identify three that can be useful for our objective:
-
Delineated content: The OBO Foundry promotes the development of an orthogonal collection of biomedical ontologies. This means that biomedical ontologies should reuse the content from other existing ontologies to avoid overlaps.
-
Relations: There should be a consistent formulation of relational assertions, which is related to the number and types of relations used in biomedical ontologies. This aspect will be approached in a more general way, since the types of axioms, not only relations, will be analyzed.
-
Naming conventions: The labels associated with the concepts in the ontology should be meaningful for humans. Besides, there should be lexical relations between the labels of taxonomically related concepts. Since a taxonomic child concept is a specialization of its parent, then the label of the child concept could be an extension of the label of the parent.
Next, a summary of the results of analyzing more than 200 OWL ontologies retrieved from BioPortal is presented, whereas the complete results can be found in related papers [26, 27].
Reuse. The analysis of how ontology content is being reused by other ontologies has a direct implication on the requirement 1, that is, on the representation, sharing and reuse of knowledge. Besides, reuse can be approached from two different perspectives, namely, effective and potential reuse.
Effective reuse is measured by taking into account how many ontologies are imported and reused. Our results show that only 23% of the ontologies analyzed reuse content from other ontologies, 90% of which reuse only one ontology. Both results are a sign of low effective reuse in biomedical ontologies. However, some positive findings were also obtained in this analysis. The most frequently reused ontologies are the Basic Formal Ontology (BFO)Footnote 11, the OBO Relations OntologyFootnote 12 and the Information Artifact Ontology (IAO)Footnote 13. Those ontologies can be considered top-level or very general knowledge frameworks, so their frequent reuse means that many ontologies are using a common background knowledge, which positively contributes to requirement 1.
Potential reuse identifies content from other ontologies that could be reused in a given ontology by performing lexical matches between the content of the labels of the classes. Three types of matches are taken into account:
-
Internal exact match (IEM): The lexical regularity is the full label of another class of the same ontology. For example, there is an internal exact match between the class “amine binding” and “binding” if both classes are in the same ontology. In this case, reuse would mean that the class “binding” could be used for defining the axioms associated with the class “amine binding”.
-
External exact match (EEM): The lexical regularity is the full label of a class of a different ontology. For example, there is an external exact match between the class “peptide antigen binding” in the Gene Ontology [2] and “antigen” in SNOMED CT. In this case, the class “antigen” could be used for defining the axioms associated with the class “peptide antigen binding”.
-
External regularity match (ERM): The lexical regularity is also a regularity in a different ontology. For example, there is an external regularity match between the class “peptide antigen binding” in the Gene Ontology and “antigen role” in OBI, since “antigen” is a shared regularity. In this case, the semantics associated with “antigen” could be used for defining the axioms associated with the two classes of this ERM.
The first step in the analysis of potential reuse was to calculate the regularities existing in the labels of the classes of our corpus. For this study, only those regularities with frequency greater than 1% were used, in this case, 8175 regularities. Then, we calculated the IEM, EEM and ERM for all the classes in the corpus. The results were that 15.60% of the regularities had IEMs, 36.44% of the regularities had EEMs, and 23.49% of the regularities had ERMs. These results clearly show that there is a huge potential reuse in biomedical ontologies, which is yet to be exploited.
Axioms. The analysis of the axiomatic richness of an ontology is closely related to requirements 2–3, that is, the classification and retrieval of data. It is also related to the fourth one, since the axiomatization of the ontology has traditionally been linked to the quality of ontologies. Besides, it is related to the machine understandability of the content of the ontology.
This study has focused on the analysis of the types of axioms used in the corpus of ontologies analyzed. The results reveal that the most frequently used type of axiom is Annotation Assertion (57.63%), followed by subClassOf (26.84%). Hence, two types of axioms (out of 35 types of axioms in OWL2) cover more than 84% of the axioms defined in this corpus.
Annotation axioms provide content that is basically in natural language such as labels, comments or descriptions, so that content cannot be easily used by the machine. The taxonomic relation provides the hierarchical structure of the ontologies, so most ontologies in this corpus can be described as plain taxonomies rich in natural language content. Consequently, its axiomatic richness is lower than expected to fulfil our usefulness requirements.
Systematic Naming. The analysis of the application of a systematic naming convention is directly related to the understandability of the content of the ontology for humans, but we also see it related to the axiomatization of the ontology due to the potential reuse in biomedical ontologies. There are tools such as Ontocheck [30] that permit to test the application of naming conventions in ontologies. Basically, the application of naming conventions implies that there is an agreement on how to name and label the classes. In practical terms, the application of the naming convention implies that taxonomically related classes should have similar linguistic labels, and the labels of the child concepts should be extensions of the labels of the parent ones. Consequently, the systematic naming of classes must have an impact on the regularity of the content of the labels and on the number of words repeated in different labels. Our study focused on the analysis of the regularities as a sign of the application of a systematic naming convention in our corpus. We found that the percentage of repeated words in the labels was 67.7%, all the ontologies having values over 50% and the maximum reaching 94.7%. The existence of regularities with length over 10 words is also a clear sign of application of naming conventions.
4 Increasing the Usefulness of Ontologies
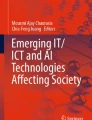
Two main limitations of existing biomedical ontologies can be identified from our usefulness perspective: effective reuse and axiomatization. However, it is worth to study whether the results obtained in terms of potential reuse and systematic naming conventions can be used for overcoming such limitations. For this purpose, we performed a clustering of the ontologies in the corpus described in previous sections. We performed an agglomerative hierarchical clustering (k-means) by taking into account three variables: percentage of classes with regularities, percentage of classes with IEM or EEM matches, and percentage of repeated words. The inspection of the dendrogram suggested the existence of three differentiated groups of ontologies.
Figure 1 shows the spatial distribution of the ontologies and the three clusters. Cluster 1 contains 43% of the ontologies, Cluster 2 33% and Cluster 3 24%. Cluster 1 includes ontologies with many regularities, many repeated words and those ontologies with the highest percentage of matches. Cluster 2 includes those ontologies with many repeated words and high degree of regularity. Cluster 3 includes the ontologies with the lowest values for the three variables. We think that the axiomatic richness and reuse in the ontologies of Clusters 1 and 2 could be addressed by analyzing and exploiting the regularities and matches existing in such ontologies. This conclusion is reinforced by the distance between the clusters depicted in the figure. In the next subsections we describe two frameworks that can contribute to increase the usefulness of biomedical ontologies. First, we need to facilitate the reuse of ontologies. This requires facilitating the task of identifying which ontology provides the best knowledge for the new ontology. This support is needed because the current set of existing biomedical ontologies is not orthogonal. Second, we need to support ontology developers in creating axiomatically-rich ontologies and in evaluating and assuring the quality of their ontologies. These frameworks deal with (1) ontology enrichment and (2) ontology evaluation. The first one has the objective of identifying and analyzing the regularities in the content and structure of the labels in biomedical ontologies, and to find content from other ontologies that could be used for adding or improving existing axioms in ontologies. The second one has the objective of identifying strengths and flaws in ontologies from an engineering perspective.

3D scatterplot of the clusters obtained with more than 200 BioPortal ontologies
4.1 Ontology Enrichment
This process takes advantage of the fact that biomedical ontologies have hidden semantics [35], that is, some content of the ontologies is only expressed in natural language, but not as logical axioms. Consequently, such content is only available for humans, not for machines. This ontology enrichment method, called OntoEnrich, is inspired by the “lexically suggest, logically define” principle [28], which means that what is expressed in natural language for humans should be expressed in the form of axioms for the machines.

Diagram of the different stages of the ontology enrichment framework
Figure 2 shows the stages included in our ontology enrichment approach:
-
Stage 1: Identification and basic characterization of lexical regularities. The content of the labels of the classes of biomedical ontologies is processed using Natural Language Processing techniques to identify the lexical regularities, which are ordered, consecutive words that appear in different labels. This stage selects the regularities whose frequency is over a user-defined threshold. The primary characterization also finds the IEM, EEM, and ERM with the ontologies existing in BioPortal.
-
Stage 2: Advanced characterization of lexical regularities. A series of metrics are calculated for each regularity: locality, modularity and cross-products extensions (CPE). Locality accounts for how close the classes that exhibit a given regularity are in the ontology. The enrichment of the classes associated with regularities with high locality would affect a particular region of the ontology. Modularity analyses the distribution of the regularity in selected modules of the ontology, which permits to identify which modules are associated with the regularity. In this context, a module refers to a subontology, and it is identified by its root class. The CPE analyses to what extent the content of the regularity has matches with classes from the same or different ontologies. For example, if the content of the regularity can be fully decomposed in matching classes, then the axioms associated with the regularity could be defined by reusing existing classes.
-
Stage 3: Filtering lexical regularities. The analysis of the metrics associated with the lexical regularities may help the ontology developer to filter out the regularities less promising for the enrichment of the ontology. Besides filters based on frequency, locality, modality or CPE metrics, the method permits to filter based on the super/subrelations that may hold between regularities. This would permit to focus on the most general or the most specific regularities.
-
Stage 4: Extraction of relations. The method is able to automatically suggest taxonomic links between classes sharing a regularity. This requires that the regularity matches the full label of one class in the ontology, which would be the superclass in those taxonomic links.
-
Stage 5: Design and execution of axioms. The user may define a template axiom for a given regularity, which can be applied to the classes that exhibit such regularity using the OPPL2 languageFootnote 14.
This method has been implemented and made available online in our OntoEnrich platformFootnote 15. There, the results of a series of analyses can be found. The “lexically suggest, logically define” principle has inspired our ontology enrichment process but can also be used with the purpose of quality assurance, that is, to check that the logical axioms have the meaning expressed in the content in natural language. We have actually applied our method with such purpose on SNOMED CT, and this has permitted to identify potential cases of suboptimal axiomatization in SNOMED CT [25], which would lead to queries with incomplete results if issued against EHR datasets.
4.2 Ontology Quality Evaluation: The OQuaRE Framework
Assuring the quality of ontologies requires to perform a series of different types of analyses over them, which would measure different properties of the ontologies. Many ontology evaluation methods have traditionally been applied with the objective of ranking ontologies for a given purpose, although we approach it from the perspective of identifying strengths and flaws in biomedical ontologies. Such findings should help the ontology developers to improve their ontologies, and ontology users to select the ontologies that provides the best match to their requirements. It should be noted that quality evaluation tasks are usually understood as objective evaluations to test to what extent a determined product meets some requirements.
In the last years we have designed and developed an objective, reproducible, quantitative framework for evaluating the quality of ontologies, which is called OQuaRE [8]. OQuaRE is adapted from SQuaREFootnote 16, an international standard for software product quality evaluation. The complete description of the OQuaRE framework can be found in its websiteFootnote 17, although its main features are described next. OQuaRE structures the evaluation of the quality of an ontology using four out of the five divisions proposed by SQuaRE: quality evaluation, quality requirements, quality model (characteristics and subcharacteristics) and quality measurements. OQuaRE uses the eight quality characteristics proposed by SQuaRE for measuring software quality: functional adequacy, reliability, operability, maintainability, compatibility, transferability, performance efficiency and quality in use. Besides, OQuaRE adds the structural characteristic, because of the relevance of structural aspects in the quality of ontologies. Each quality characteristic has a set of associated quality subcharacteristics, which are measured through quality metrics. The values of the quality metrics are automatically calculated.
The current version of OQuaRE includes 9 characteristics, 49 subcharacteristics and 16 metrics. The values of the metrics are scaled to the range [1, 5], which has been traditionally used in quality evaluation frameworks. The weighted mean of the metrics scores associated with each subcharacteristic permits to assign a [1, 5] score to each quality subcharacteristic. The quality scores of each quality characteristic are obtained by the weighted average of the scores of its subcharacteristics. Although it is possible to calculate a quality score for the whole ontology, we think that such score is not relevant for our purpose of showing strengths and flaws, but for the application of the framework with the purpose of ranking ontologies. Consequently, the quality scores could guide the process of deciding which ontology to reuse, since the scores should permit the users to make informed decisions by matching their requirements to the ontologies’ scores.

Radar graph showing the quality scores of seven OQuaRE quality characteristics for both versions of the Cell Type Ontology
It would be expected that an axiomatically richer ontology would have better quality scores for certain properties. This was shown by the application of OQuaRE to two different versions of the Cell Type Ontology [8]. One version, called oCTO, was the original Cell Type Ontology. The second version, called nCTO, was the result of a redesign of the ontology, including more axioms. Figure 3 shows the scores of the quality characteristics for both ontologies. The results show that nCTO obtains higher scores for most characteristics, what has an implication on the practical usefulness of both ontologies. Besides, a method such as OQuaRE should contribute to analyze whether changes in the ontologies have the expected impact on the quality characteristics. Recently, we have developed an extension of the OQuaRE framework which is capable of analyzing the evolution of an ontology [9]. Figure 4 shows the evolution of the values of selected metrics (TMOnto, NOMOnto, RFCOnto, LCOMOnto, RROnto) for a biomedical ontology. In the figure, each line represents the evolution of the quality scores (scale 1–5) of each metric across the eighteen versions of EDAM. We can observe that the quality scores of some metrics vary significantly between the initial versions and the final ones. Besides, it can be seen that version 4 is key because this version triggers most of the major changes in the quality scores. The inspection of that version reveals that there was a change in the modeling style for some properties in the ontology, and such design decision had an impact on the metrics. Frameworks such as OQuaRE permits ontology developers to analyze the changes made in their ontologies from a quality evaluation perspective. This helps them to check whether the effects are in line with the requirements for their ontologies, which contributes to achieve higher quality, more useful biomedical ontologies.

Evolution of the values of the metrics across the different versions of an ontology
5 Discussion and Conclusions
In this paper we have described the evolution of EHR and CDS systems, illustrating why their meaningful communication has not been reached yet. According to the international recommendations, ontologies should play an important role for enabling such meaningful communication, which led us to briefly analyzed how ontologies have been used in EHR and CDS systems, and identifying some requirements ontologies should meet in order to be useful for bridging between EHR and CDS systems. Some results analyzing how existing ontologies meet those requirements were presented, identifying a series of improvements in biomedical ontologies for optimizing their efficacy for playing the intended bridging role: (1) the reuse of content from standardized ontologies, which should help to build the knowledge required to capture and describe EHR data and the clinical guidelines, (2) increasing the axiomatization of ontologies to improve data retrieval and classification; and (3) assuring the quality of ontologies as products.
We have described two frameworks that have demonstrated in the last years that they can help to increase the usefulness of biomedical ontologies. The ontology enrichment framework, implemented in the OntoEnrich platform, pursues to convert the hidden semantics existing in the labels of biomedical ontologies into explicit knowledge, that is, logical axioms. This framework contributes to the reuse of content by identifying matches between classes from different ontologies since it includes algorithms for token-based lexical alignment. Besides, it contributes to the axiomatization of ontologies because its methods permit to design new logical axioms that can be added to a set of classes in the ontology. Finally, this framework can also contribute to quality assurance, since it permits to analyze how principles such as “lexically suggest, logically define” are applied. The ontology evaluation framework, implemented in the OQuaRE platform, contributes to the quality assurance of the ontology by providing quantitative information to ontology developers about the strengths and flaws of the ontologies during their whole development, since it permits to analyze the effects of changes in different versions of an ontology. Moreover, reuse can also be supported by OQuaRE, since its quantitative information can be applied by users for making informed decisions about which content to reuse.
Nevertheless, these are only two of the processes needed to increase the usefulness of biomedical ontologies. For example, one of the requirements for biomedical ontologies is reusing standardized ontologies, including top-level ontologies such as BFOFootnote 18 or BioTopFootnote 19. Despite our results show that BFO is the most reused ontology, the size and modeling style of top-level ontologies is not handled by ontology tools in an optimal way, what makes difficult to explore and find the right classes. We also believe that EHR standards and CDS frameworks should be rethought to be grounded on standardized ontologies. This would help to overcome limitations such as the ones described in current archetype-based technology. That would certainly require agreements on the semantic modeling primitives for both types of systems, which would certainly facilitate their interoperability.
In summary, biomedical ontologies should play a fundamental role for the meaningful exchange of data between EHR and CDS systems, but they need to be improved in a series of ways in order to optimize their efficacy and efficiency. The notion of usefulness applied in this work focuses on making more knowledge available for the machines and in facilitating the reuse of content, but other complementary aspects must also be taken into account. We hope that the work described in this paper contributes to gear up the efforts in this area.
Notes
- 1.
- 2.
- 3.
- 4.
- 5.
- 6.
- 7.
- 8.
- 9.
- 10.
- 11.
- 12.
- 13.
- 14.
- 15.
- 16.
- 17.
- 18.
- 19.
References
Health Level 7.: Arden Syntax for Medical Logic Systems Standard Version 2.6. Ann Arbor, MI: Health Level 7 (2007)
Ashburner, M., Ball, C.A., Blake, J.A., Botstein, D., Butler, H., Cherry, J.M., Davis, A.P., Dolinski, K., Dwight, S.S., Eppig, J.T., et al.: Gene ontology: tool for the unification of biology. Nature Genet. 25(1), 25–29 (2000)
Beale, T.: Archetypes: constraint-based domain models for future-proof information systems. In: OOPSLA 2002 Workshop on Behavioural Semantics, vol. 105 (2002)
Berners-Lee, T., Hendler, J., Lassila, O., et al.: The semantic web. Sci. Am. 284(5), 28–37 (2001)
Bouamrane, M.-M., Rector, A., Hurrell, M.: Using owl ontologies for adaptive patient information modelling and preoperative clinical decision support. Knowl. Inform. Syst. 29(2), 405–418 (2011)
Breasted, J.H.: The Edwin Smith Surgical Papyrus: published in facsimile and hieroglyphic transliteration with translation and commentary in two volumes, vol. 3. Chic. UP (1930)
Chen, R., Corbal, I.: Guideline definition language (gdl). Release 0.9, pp. 1–23 (2013)
Duque-Ramos, A., Fernández-Breis, J.T., Stevens, R., Aussenac-Gilles, R.N., et al.: Oquare: a square-based approach for evaluating the quality of ontologies. J. Res. Pract. Inform. Technol. 43(2), 159 (2011)
Duque-Ramos, A., Quesada-Martínez, M., Iniesta-Moreno, M., Fernández-Breis, J.T., Stevens, R.: Supporting the analysis of ontology evolution processes through the combination of static and dynamic scaling functions in oquare. J. Biomed. Semant. 7(1), 63 (2016)
Farion, K., Michalowski, W., Wilk, S., O’Sullivan, D.M., Rubin, S., Weiss, D.: Clinical decision support system for point of care use: ontology driven design and software implementation. Meth. Inform. Med. 48(4), 381–390 (2009)
Fox, J., Johns, N., Rahmanzadeh, A.: Disseminating medical knowledge: the proforma approach. Artif. Intell. Med. 14(1), 157–182 (1998)
Goble, C., Stevens, R.: Stevens.: state of the nation in data integration for bioinformatics. J. Biomed. Inform. 41(5), 687–693 (2008)
Hawkins, M., Ralley, R., Young, J.: A medical panorama: the casebooks project. Book 2.0 4(1–2), 61–69 (2014)
Ingram, D.: The good european health record. In: Laires, M.F., Ladeira, M.F., Christensen, J.P. (eds.) Health in the New Communication Age, pp. 66–74. IOS (1995)
Isern, D., Moreno, A.: Computer-based execution of clinical guidelines: a review. Int. J. Med. Inform. 77(12), 787–808 (2008)
Isern, D., Sánchez, D., Moreno, A.: Ontology-driven execution of clinical guidelines. Comput. Meth. Programs Biomed. 107(2), 122–139 (2012)
Kalra, D., Lewalle, P., Rector, A., Rodrigues, J.M., Stroetmann, K.A., Surjan, G., Ustun, B., Virtanen, M., Zanstra, P.E.: Semantic interoperability for better health and safer healthcare. Research and Deployment Roadmap for Europe. SemanticHEALTH Project Report, Published by the European Commission (2009). http://ec.europa.eu/information_society/ehealth
Martínez-Costa, C., Menárguez-Tortosa, M., Fernández-Breis, J.T., Maldonado, J.A.: A model-driven approach for representing clinical archetypes for semantic web environments. J. Biomed. Inform. 42(1), 150–164 (2009)
Menárguez-Tortosa, M., Fernández-Breis, J.T.: Owl-based reasoning methods for validating archetypes. J. Biomed. Inform. 46(2), 304–317 (2013)
Montero, M.A., Prado, S.: Electronic health record as a knowledge management tool in the scope of health. In: Riaño, D. (ed.) K4HelP 2008. LNCS (LNAI), vol. 5626, pp. 152–166. Springer, Heidelberg (2009). doi:10.1007/978-3-642-03262-2_12
Mosa, A.S.M., Yoo, I., Sheets, L.: A systematic review of healthcare applications for smartphones. BMC Med. Inform. Decis. Making 12(1), 1 (2012)
Musen, M.A., Middleton, B., Greenes, R.A.: Clinical decision-support systems. In: Shortliffe, E.H., Cimino, J.J. (eds.) Biomedical Informatics, pp. 643–674. Springer, New York (2014)
Ohno-Machado, L., Gennari, J.H., Murphy, S.N., Jain, N.L., Tu, S.W., Oliver, D.E., Pattison-Gordon, E., Greenes, R.A., Shortliffe, E.H., Barnett, G.O.: The guideline interchange format. J. Am. Med. Inform. Assoc. 5(4), 357–372 (1998)
Peleg, M.: Computer-interpretable clinical guidelines: a methodological review. J. Biomed. inform. 46(4), 744–763 (2013)
Quesada-Martínez, M., Fernández-Breis, J.T., Karlsson, D.: Suggesting missing relations in biomedical ontologies based on lexical regularities. Stud. Health Technol. Inform. 228, 384 (2016)
Quesada-Martínez, M., Fernández-Breis, J.T., Stevens, R.: Lexical characterization and analysis of the BioPortal ontologies. In: Peek, N., Marín Morales, R., Peleg, M. (eds.) AIME 2013. LNCS (LNAI), vol. 7885, pp. 206–215. Springer, Heidelberg (2013). doi:10.1007/978-3-642-38326-7_31
Quesada-Martínez, M., Fernández-Breis, J.T., Stevens, R.: Lexical characterisation of bio-ontologies by the inspection of regularities in labels. Curr. Bioinform. 10(2), 165–176 (2015)
Rector, A., Iannone, L.: Lexically suggest, logically define: quality assurance of the use of qualifiers and expected results of post-coordination in snomed ct. J. Biomed. Inform. 45(2), 199–209 (2012)
Rector, A.L., Johnson, P.D., Tu, S., Wroe, C., Rogers, J.: Interface of inference models with concept and medical record models. In: Quaglini, S., Barahona, P., Andreassen, S. (eds.) AIME 2001. LNCS (LNAI), vol. 2101, pp. 314–323. Springer, Heidelberg (2001). doi:10.1007/3-540-48229-6_43
Schober, D., Tudose, I., Svatek, V., Boeker, M.: Ontocheck: verifying ontology naming conventions and metadata completeness in protégé 4. J. Biomed. Semant. 3(2), 1 (2012)
Shahar, Y., Young, O., Shalom, E., Galperin, M., Mayaffit, A., Moskovitch, R., Hessing, A.: A framework for a distributed, hybrid, multiple-ontology clinical-guideline library, and automated guideline-support tools. J. Biomed. Inform. 37(5), 325–344 (2004)
Sherman, R.: Computer system clears up errors, lets nurses get back to nursing: a progress report from children’s hospital, Akron, Ohio. Hosp. Top. 43(10), 44–46 (1965)
Smith, B., Ashburner, M., Rosse, C., Bard, J., Bug, W., Ceusters, W., Goldberg, L.J., Eilbeck, K., Ireland, A., Mungall, C.J., et al.: The obo foundry: coordinated evolution of ontologies to support biomedical data integration. Nature Biotechnol. 25(11), 1251–1255 (2007)
Tao, C., Jiang, G., Oniki, T.A., Freimuth, R.R., Zhu, Q., Sharma, D., Pathak, J., Huff, S.M., Chute, C.G.: A semantic-web oriented representation of the clinical element model for secondary use of electronic health records data. J. Am. Med. Inform. Assoc. 20(3), 554–562 (2013)
Third, A.: Hidden semantics: what can we learn from the names in an ontology? In: Proceedings of the Seventh International Natural Language Generation Conference, pp. 67–75. Association for Computational Linguistics (2012)
Tu, S.W., Eriksson, H., Gennari, J.H., Shahar, Y., Musen, M.A.: Ontology-based configuration of problem-solving methods and generation of knowledge-acquisition tools: application of protege-ii to protocol-based decision support. Artif. Intell. Med. 7(3), 257–289 (1995)
Warner, H.R., Toronto, A.F., Veasey, L.G., Stephenson, R.: A mathematical approach to medical diagnosis: application to congenital heart disease. Jama 177(3), 177–183 (1961)
Wilk, S., Michalowski, W., Michalowski, M., Farion, K., Hing, M.M., Mohapatra, S.: Mitigation of adverse interactions in pairs of clinical practice guidelines using constraint logic programming. J. Biomed. Inform. 46(2), 341–353 (2013)
Wright, A., Sittig, D.F.: A four-phase model of the evolution of clinical decision support architectures. Int. J. Med. Inform. 77(10), 641–649 (2008)
Yao, W., Kumar, A.: Conflexflow: Integrating flexible clinical pathways into clinical decision support systems using context and rules. Decis. Support Syst. 55(2), 499–515 (2013)
Acknowledgements
This work has been partially funded by to the Spanish Ministry of Economy and Competitiveness, the FEDER Programme and by the Fundación Séneca through grants TIN2014-53749-C2-2-R and 19371/PI/14.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2017 Springer International Publishing AG
About this paper
Cite this paper
Fernández-Breis, J.T., Quesada-Martínez, M., Duque-Ramos, A. (2017). Can Existing Biomedical Ontologies Be More Useful for EHR and CDS?. In: Riaño, D., Lenz, R., Reichert, M. (eds) Knowledge Representation for Health Care. ProHealth KR4HC 2016 2016. Lecture Notes in Computer Science(), vol 10096. Springer, Cham. https://doi.org/10.1007/978-3-319-55014-5_1
Download citation
DOI: https://doi.org/10.1007/978-3-319-55014-5_1
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-319-55013-8
Online ISBN: 978-3-319-55014-5
eBook Packages: Computer ScienceComputer Science (R0)