
Abstract
Bleeding in late pregnancy often heralds serious and potentially life-threatening complications. Antepartum hemorrhage is defined as any vaginal bleeding in the second half of pregnancy but before birth, usually considered after 20 weeks’ gestation. Major causes include placenta previa, placental abruption, vasa previa, and uterine rupture. These complications are infrequently managed in the emergency department, but emergency physicians must be prepared to make a swift, accurate diagnosis and to lead resuscitative efforts until definitive obstetric management can be obtained. Prompt, coordinated interdisciplinary care can be lifesaving for both mother and fetus. Ultimate management depends on maternal stability and gestational age, and many patients will require emergent cesarean delivery.
Access provided by CONRICYT-eBooks. Download chapter PDF
Similar content being viewed by others


Keywords
- Placental abruption
- Placenta previa
- Vasa previa
- Uterine rupture
- Late-trimester bleeding
- Antepartum hemorrhage
Introduction
Bleeding in late pregnancy is less common than in early pregnancy and often heralds serious and potentially life-threatening complications. Antepartum hemorrhage is defined as any vaginal bleeding in the second half of pregnancy but before birth, usually considered after 20 weeks’ gestation. Antepartum bleeding complicates approximately 5% of pregnancies [1]. Major causes include “bloody show” associated with labor, placenta previa, placental abruption, and, rarely, uterine rupture and vasa previa. Massive acute hemorrhage and emergency operative delivery are associated with both maternal and fetal morbidity and mortality; therefore, evaluation must be swift and definitive. While late pregnancy complications are infrequently managed in the emergency department (ED), emergency physicians must be prepared to identify the source of late-trimester bleeding and to stabilize mother and fetus until definitive obstetric management can be obtained.
Emergency Department Evaluation
The initial assessment of vaginal bleeding in late pregnancy begins with obtaining maternal vital signs, determining gestational age and fetal well-being, and acquiring a clear history of the onset and description of bleeding. Bleeding that is sudden onset, painless, and bright red points toward placenta previa. Bleeding associated with pain, following trauma, or darker in color points toward placental abruption. Bleeding may vary from spotting to exsanguination.
The physical exam should include an abdominal and external uterus exam. Loss of normal uterine contour or the ability to palpate fetal parts indicates uterine rupture. A uterus that is tender, firm, or rigid may indicate placental abruption. An external genital and sterile speculum exam may be performed, but digital cervical exam is contraindicated until placenta previa has been excluded [2].
Laboratory tests may give helpful objective data to assess the extent of vaginal bleeding, though in acute hemorrhage, the data could be falsely reassuring. A complete blood count (CBC) should be ordered to evaluate for anemia, thrombocytopenia, and platelet consumption. A blood type and screen is required to determine Rh status and to prepare for potential blood transfusion. Women who are Rh negative should receive 300 mcg Rho(D) immune globulin to prevent Rh alloimmunization. In cases of significant bleeding, prothrombin time (PT), partial thromboplastin time (PTT), and fibrinogen levels should be checked, as placenta abruption and uterine rupture may lead to disseminated intravascular coagulation (DIC). A basic metabolic panel, magnesium level, hepatic panel, and urinalysis with urine toxicology may also be considered if there is concern for preeclampsia or substance abuse.
Transabdominal or transvaginal obstetric ultrasound can be helpful to differentiate sources of late-trimester bleeding and should be performed to look for intrauterine and intra-abdominal bleeding, placenta location, and fetal movement.
Continuous fetal monitoring, if available, is highly recommended. Any decelerations and loss of variability on fetal heart rate tracings should be noted, yet some resolve with maternal resuscitation. Persistent decelerations may require emergent cesarean delivery even before the etiology of the hemorrhage is established.
In all cases of late pregnancy vaginal bleeding, an obstetrician should be consulted as early as possible. The ultimate management is based on maternal stability and gestational age. Most patients with late pregnancy bleeding will be admitted for observation and monitoring; those near term are often delivered.
Placenta Previa
Placenta previa is defined as placental implantation in the lower uterine segment, with either complete or partial obstruction of the cervical os [3]. The incidence of placenta previa varies from 3.5 to 4.6 per 1000 births [4]. Placenta previa is often found incidentally during routine second-trimester ultrasound. Previa is noted on about 4% of ultrasound studies performed at 20–24 weeks’ gestation; however, at 37–42 weeks, it is present in only 0.4% of pregnancies [4, 5].
The exact pathogenesis of placenta previa is unknown and the condition appears to be multifactorial. There are a variety of reported risk factors placenta previa, including advanced maternal age (>35 years), infertility treatment, multiparity, multiple gestations, previous placenta previa, and pervious uterine surgery or cesarean delivery [4, 6,7,8,9,10,11,12,13].
The classic clinical presentation of placenta previa is sudden painless bright red vaginal bleeding. Emergency physicians should assume that a pregnant woman past 20 weeks gestation with painless vaginal bleeding has placenta previa until proven otherwise. The uterus usually remains soft, yet 10–20% of women may have associated uterine contractions [14, 15]. In about one-third of affected pregnancies, the initial bleeding episode occurs prior to 30 weeks’ gestation [16].
Bleeding from placenta previa can range from minor to severe. In the absence of cervical instrumentation or cervical digital examination, the sentinel bleed usually is not sufficient to produce hemodynamic instability or to threaten fetal viability [17, 18]. The initial bleeding from placenta previa is thought to occur due to shearing forces between the inelastic placenta and the uterine wall, as gradual changes in the cervix and lower uterine segment lead to partial detachment. Bleeding is primarily thought to be from the maternal side of the placenta, as no fetal vessels are exposed in placenta previa. Sexual intercourse and vaginal exams can also cause bleeding from disruption of the intervillous space, which is the space between the fetal and maternal blood vessels. Because of this, digital cervical examination is contraindicated and should not be performed until placenta previa has been ruled out [1].
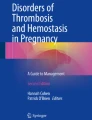
The diagnosis of placenta previa is made by ultrasound (Fig. 5.1). Transabdominal ultrasound (TAUS) is an appropriate initial study. However, several anatomical features can lead to inaccurate results such as a posteriorly located placenta, an over-distended bladder compressing the anterior lower uterine segment, and a low lying fetal head. Transvaginal ultrasonography (TVUS) has been shown to be more sensitive and specific for diagnosis of placenta previa [19,20,21,22,23,24]. One study demonstrated the superiority of TVUS as compared to the TAUS approach: false-positive and false-negative rates of TVUS were 1.0% and 2.0%, vs. 7% and 8%, for TAUS [19]. Similarly, another study found that landmarks were poorly seen in 50% of the cases using TAUS and a definitive diagnosis could not be made due to suboptimal visualization; subsequently, once TVUS was performed, the diagnosis changed in 26% of the cases [20]. TVUS can be safely performed in late pregnancy if the vaginal probe is placed 2–3 cm away from cervical os with optimal angle from os [21].

Placenta previa. Ultrasound image showing placenta covering cervical os (arrowheads). Image courtesy of Ian Suchet
Management of placenta previa depends on gestational age and stability of the mother. Unstable patients require aggressive resuscitation with blood products and emergent cesarean section. For stable patients, the main goal is to prolong pregnancy until fetal lung maturity is adequate for delivery. Patients between 24 and 34 weeks gestation should be given corticosteroids to accelerate fetal lung maturity if delivery within 7 days is anticipated [25]. Forty-four percent of women with placenta previa deliver before 37 weeks [26]. An obstetrician should evaluate all patients with placenta previa. For the majority of patients, admission to an obstetric unit is required.
Placental Abruption
Placental abruption, also known as abruptio placentae, is defined as separation of the placenta from the uterine wall before delivery. This condition occurs in about 1% of all pregnancies, and about 50% of these occur prior to 36 weeks’ gestation [27,28,29]. The presentation of placenta abruption can vary widely, making the diagnosis difficult. Placental abruption is the most common cause of intrapartum fetal death, with neonatal mortality ranging 10–30% of all abruption cases [29, 30]. Risk factors for abruptio placentae include maternal trauma, previous abruption, hypertension, cocaine use, multiparity, and advanced maternal age [29,30,31,32,33,34].
The classic presentation of placental abruption is the acute onset of abdominal pain with or without dark red vaginal bleeding. The hallmark of placental abruption is pain and tenderness, which is found in 70% of patients [33, 35]. The pain may be abdominal, pelvic, or back pain. Contractions in placental abruption are usually high frequency and low amplitude and result in pain worse between contractions [36]. The uterus tends to be firm and rigid, and hypertonia develops as the abruption expands.
Vaginal bleeding occurs in approximately 80–70% of patients with placental abruption [33, 35]. Bleeding can be light to hemorrhagic and may be bright red to dark burgundy. In abruption, maternal spiral arteries rupture, causing blood to accumulate and split the decidua from the uterine wall. A hematoma can develop without vaginal bleeding in 10–20% of abruptions [33]. These “concealed abruptions” are either early in the vessel bleeding phase or there is partial placental separation between the fetal membranes and decidua; hence, these patients present with preterm labor and abdominal pain. However, if bleeding continues, complete dissection of the uterine-placental interface can occur as the hematoma grows. Importantly, the amount of vaginal bleeding does not correlate with the severity of the abruption.
Placental abruption can quickly progress to hemorrhagic shock in the mother, and the lack of gas exchange and nutrients to the fetus causes fetal distress. Indeed, fetal distress is noted in 60% of patients with placenta abruption and may be the only sign that an abruption has occured [35]. When placental separation exceeds 50%, acute disseminated intravascular coagulation (DIC) is common and fetal death is almost certain [37].
Placental abruption is a largely clinical diagnosis. Ultrasound may be used, as a hyperechoic clot or sign of bleeding posterior to the placenta, if visualized, is highly suggestive of placental abruption (Fig. 5.2). Unfortunately, these findings are only present in about 25% of cases [38]. While ultrasound cannot reliably exclude abruption, it can be used to exclude placenta previa.

Ultrasound image showing acute placental abruption with a retroplacental hematoma (arrow) lifting part of the placenta. Meguerdichian, D. “Complications in late pregnancy” Emergency Medicine Clinics of North America. Philadelphia, Elsevier. 2011. Courtesy of Carol Benson, MD, Brigham and Women’s Hospital Department of Radiology, with permission
Management of patients with abruptio placentae should begin with placement of two large bore IVs, resuscitation with intravenous fluids or blood products, reversal of any coagulopathies, and immediate obstetric consultation. Since DIC occurs in about 10% of placenta abruption cases, fibrinogen, PT, and PTT should be sent with standard labs [39]. Blood type and screen should also be sent if this diagnosis is suspected. In most cases of placental abruption, immediate delivery is necessary and tocolytics are contraindicated. One case-control study found that decision to deliver interval of 20 min or less resulted in better neonatal outcomes [40].
Vasa Previa
Vasa previa, from the Latin “vessels before the road,” is the presence of fetal vessels between the cervix and the presenting fetal part. This is a very serious cause of vaginal bleeding in late pregnancy, with greater than 50% perinatal mortality [41]. Rupture of only 100 ml of exposed fetal vessels can cause fetal exsanguination or death [42]. Obstetric consultation should be obtained immediately. The condition is usually diagnosed in the second or third trimester by ultrasound (Fig. 5.3). The incidence of vasa previa is about 1 in 2500 births, yet may be even higher in pregnancies resulting from assisted reproductive technologies [41]. The risk factors for vasa previa include placenta previa, in vitro fertilization, multiple gestations, and velamentous cord insertion (i.e., when the placental end of the umbilical cord consists of divergent umbilical vessels that are not protected by Wharton’s jelly and are at risk for rupture) [41, 43, 44].

Vasa previa. Arrows pointing to fetal vessels between the cervix and presenting fetal part. Image courtesy of Ian Suchet
Patients with vasa previa tend to present with vaginal bleeding immediately after spontaneous rupture of membranes or amniotomy; it is rare for fetal vessels to rupture without rupture of membranes. Without a history of vasa previa on a prior ultrasound, this diagnosis should be suspected if there are fetal heart abnormalities accompanied with sudden vaginal bleeding after rupture of membranes. Fetal heart monitoring in this condition tends to present as sinusoidal or bradycardic pattern [43, 45]. Any non-reassuring fetal monitoring or unstable maternal vital signs is an indication for operative delivery. Upon delivery, focus should be placed on neonatal resuscitation due to the high mortality rate. If there is a reassuring fetal heart rate, stable maternal vital signs, and nonhemorrhagic vaginal bleeding, an Apt test (a qualitative test of vaginal bleeding to determine the absence or presence of fetal blood) may be performed to diagnose vasa previa [46].
Uterine Rupture
Uterine rupture is a life-threatening cause of vaginal bleeding in late pregnancy. The incidence depends on cause of rupture and is difficult to estimate. It is much more common in patients with history of previous cesarean sections, but is still possible in an unscarred uterus. In fact, 13% of uterine ruptures occur in unscarred uteruses, and this group has a higher morbidity and mortality compared to uterine rupture with a previously scarred uterus [47, 48]. One study found a perinatal mortality of 65% in the unscarred uterus [47]. In addition to history of previous cesarean section, risk factors for uterine rupture include trauma, high parity, advanced maternal age, and congenital disorders (e.g., Ehlers-Danlos) [47,48,49,50,51,52,53,54].
The classic presentation of uterine rupture is the sudden onset of abdominal pain, loss of uterine tone, change in uterine shape or contour, vaginal bleeding, and shock. A scarred uterus rupture may have a less severe onset presentation than that of an unscarred uterus due to previously altered vasculature [47]. Vaginal bleeding may be modest to hemorrhagic depending on the site of uterine rupture. These patients have a tender, boggy uterus on exam, and abdominal girth may quickly expand as blood accumulates. Fetal monitoring is more reliable than abdominal pain in diagnosing uterine rupture [53, 55,56,57,58]. Bradycardia is the most common finding on fetal monitoring, but no fetal heart rate pattern is pathognomonic [53, 55,56,57,58].
In any suspicion of uterine rupture, immediate resuscitation and surgical intervention are crucial. In the rare situations where there is only mild abdominal pain, stable fetal heart tracings, and light vaginal bleeding, an ultrasound exam may be performed. An abdomen or focused assessment with sonography for trauma (FAST) ultrasound exam with significant blood or defect in uterine wall can help reach the uterine rupture diagnosis. Studies have noted that a physician has about 10–37 min from frank uterine rupture to intervention before there is significant fetal and maternal morbidity [54, 56, 59]. Therefore, this is a diagnosis that should be immediately considered in antepartum hemorrhage.
Other Causes of Antepartum Hemorrhage
The previously discussed topics are some of the more concerning diagnoses of late-trimester vaginal bleeding, but there are numerous causes and degrees of vaginal bleeding in pregnancy. Vaginal and cervical sources of bleeding include vaginitis, cervicitis, warts, polyps, fissures, and trauma. Fibroids and circumvallate placenta are intrauterine causes of vaginal bleeding. Patients may have mild vaginal bleeding following cervical exams, sexual intercourse, or stripping of membranes by obstetricians near term. Most of these cases presents with spotting or minimal vaginal bleeding. Regardless, all patients with vaginal bleeding in late pregnancy should be evaluated with serious concern, and care should be managed in close consultation with an obstetrician.
Summary
Bleeding in late pregnancy can herald potentially life-threatening conditions such as placenta previa, placental abruption, vasa previa, or uterine rupture. These emergencies are infrequently managed in the ED and can be challenging for the entire team. It is incumbent on the emergency physician to make a swift, accurate diagnosis and to lead resuscitative efforts. Obstetric consultation should be obtained as early as possible. Prompt, coordinated interdisciplinary care can be lifesaving for both the mother and fetus. Ultimately, management depends on maternal stability and gestational age; many patients will require emergent cesarean delivery.
Key Points
-
A pregnant woman past 20 weeks gestation with sudden onset painless vaginal bleeding has placenta previa until proven otherwise.
-
Digital cervical exams are contraindicated until placenta previa has been excluded.
-
Placental abruption may present with or without vaginal bleeding; the amount of bleeding does not correlate with the severity of the abruption.
-
Ultrasound is used to diagnose placenta previa; it cannot reliably exclude placental abruption.
-
Obstetric consultation should be obtained early in the ED course of all patients with late pregnancy bleeding.
References
Hull AD, Resnick R. Placenta previa, placenta accreta, abruptio placentae, and vasa previa. In: Creasy RK, Resnick R, Iams JD, et al editors. Maternal-fetal medicine: Priniciple and practice. 7th ed. Philadelphia, PA: Elsevier Saunders, p. 732–42.
Chilaka VN, Konje JC, Clarke S, Taylor DJ. Practice observed: is speculum examination on admission a necessary procedure in the management of all cases of antepartum haemorrhage? J Obstet Gynaecol. 2000;20:396–8.
Silver RM. Abnormal placentation: placenta previa, vasa previa, and placenta accreta. Obstet Gynecol. 2015;126(3):654–68.
Faiz AS, Ananth CV. Etiology and risk factors for placenta previa: an overview and meta-analysis of observational studies. J Matern Fetal Neonatal Med. 2003;13:175–90.
Mustafa SA, Brizot ML, Carvalho MH, Watanabe L, Kahhale S, Zugaib M. Transvaginal ultrasonography in predicting placenta previa at delivery: a longitudinal study. Ultrasound Obstet Gynecol. 2002;20:356–9.
Marshall NE, Fu R, Guise JM. Impact of multiple cesarean deliveries on maternal morbidity: a systematic review. Am J Obstet Gynecol. 2011;205(3):262.
Ananth CV, Smulian JC, Vintzileos AM. The association of placenta previa with history of cesarean delivery and abortion: a metaanalysis. Am J Obstet Gynecol. 1997;177(5):1071.
Rasmussen S, Albrechtsen S, Dalaker K. Obstetric history and the risk of placenta previa. Acta Obstet Gynecol Scand. 2000;79(6):502–7.
Macones GA, Sehdev HM, Parry S, Morgan MA, Berlin JA. The association between maternal cocaine use and placenta previa. Am J Obstet Gynecol. 1997;177(5):1097–100.
Iyasu S, Saftlas AK, Rowley DL, Koonin LM, Lawson HW, Atrash HK. The epidemiology of placenta previa in the United States, 1979 through 1987. Am J Obstet Gynecol. 1993;168(5):1424–9.
Rosenberg T, Pariente G, Sergienko R, Wiznitzer A, Sheiner E. Critical analysis of risk factors and outcome of placenta previa. Arch Gynecol Obstet. 2011;284(1):47.
Ananth CV, Demissie K, Smulian JC, Vintzileos AM. Placenta previa in singleton and twin births in the United States, 1989 through 1998: a comparison of risk factor profiles and associated conditions. Am J Obstet Gynecol. 2003;188(1):275.
Sheiner E, Shoham-Vardi I, Hallak M, Hershkowitz R, Katz M, Mazor M. Placenta previa: obstetric risk factors and pregnancy outcome. Matern Fetal Med. 2001;10:414–9.
Cotton DB, Read JA, Paul RH, Quilligan EJ. The conservative aggressive management of placenta previa. Am J Obstet Gynecol. 1980;137(6):687.
Silver R, Depp R, Sabbagha RE, Dooley SL, Socol ML, Tamura RK. Placenta previa: aggressive expectant management. Am J Obstet Gynecol. 1984;150(1):15.
Dola CP, Garite TJ, Dowling DD, Friend D, Ahdoot D, Asrat T. Placenta previa: does its type affect pregnancy outcome? Am J Perinatol. 2003;20(7):353–60.
Sakornbut E, Leeman L, Fontaine P. Late pregnancy bleeding. Am Fam Physician. 2007;75(8):1199–206.
Abbrescia K, Sheridan B. Complications of second and third trimester pregnancies. Emerg Med Clin North Am. 2003;21(3):695–710.
Leerentveld RA, Gilberts EC, Arnold MJ, Wladimiroff JW. Accuracy and safety of transvaginal sonographic placental localization. Obstet Gynecol. 1990;(76):759–62.
Smith RS, Lauria MR, Comstock CH, Treadwell MC, Kirk JS, Lee W, Bottoms SF. Transvaginal ultrasonography for all placentas that appear to be low-lying or over the internal cervical os. Ultrasound Obstet Gynecol. 1997;9(1):22.
Timor-Tritsch IE, Yunis R. Confirming the safety of transvaginal sonography in patients suspected of placenta previa. Obstet Gynecol. 1993;81(5Pt 1):742.
Sunna E, Ziadeh S. Transvaginal and transabdominal ultrasound for the diagnosis of placenta praevia. J Obstet Gynaecol. 1999;19(2):152.
Sherman SJ, Carlson DE, Platt LD, Medearis AL. Transvaginal ultrasound: does it help in the diagnosis of placenta previa? Ultrasound Obstet Gynecol. 1992;2(4):256.
Oyelese KO, Holden D, Awadh A, Coates S, Campbell S. Placenta praevia: the case for transvaginal sonography. Contemp Rev Obstet Gynaecol. 1999;11:257–61.
Practice Bulletin No. 159: Management of preterm labor. Obstet Gynecol. 2016;127:29–38.
Bose DA, Assel BG, Hill JB, Chauhan SP. Maintenance tocolytics for preterm symptomatic placenta previa: a review. Am J Perinatol. 2011;28(1):45–50.
Hladky K, Yankowitz J, Hansen WF. Placental abruption. Obstet Gynecol Surv. 2002;57:299–305.
Rasmussen S, Irgens LM, Bergsjo P, Dalaker K. The occurrence of placental abruption in Norway 1967–1991. Acta Obstet Gynecol Scand. 1996;75:222–8.
Tikkanen M. Placental abruption: epidemiology, risk factors and consequences. Acta Obstet Gynecol Scand. 2011;90(2):140–9.
Kyrklund-Blomberg NB, Gennser G, Cnattingius S. Placental abruption and perinatal death. Paediatr Perinat Epidemiol. 2001;15(3):290–7.
Abu-Heija A. Abruptio placentae: risk factors and perinatal outcome. J Obstet Gynaecol Res. 1998;24(2):141–4.
Ananth CV, Smulian JC, Demissie K, Vintzileos AM, Knuppel RA. Placental abruption among singleton and twin births in the United States: risk factor profiles. Am J Epidemiol. 2001;153(8):771.
Oyelese Y, Ananth CV. Placental abruption. Obstet Gynecol. 2006;108(4):1005–16.
Mbah AK, Alio AP, Fombo DW, Bruder K, Dagne G, Salihu HM. Association between cocaine abuse in pregnancy and placenta-associated syndromes using propensity score matching approach. Early Hum Dev. 2012;88(6):333–7.
Tikkanen M, Nuutila M, Hiilesmaa V, et al. Clinical presentation and risk factors of placental abruption. Acta Obstet Gynecol Scand. 2006;85(6):700–5.
Yeo L, Ananth C, et al. Glob. libr. women’s med., (ISSN: 1756–2228). 2008.
Ananth CV, Berkowitz GS, Savitz DA, et al. Placental abruption and adverse perinatal outcomes. JAMA. 1999;282:1646–51.
Glantz C, Purnell L. Clinical utility of sonography in the diagnosis and treatment of placental abruption. J Ultrasound Med. 2002;21:837–40.
Witlin AG, Sibai BM. Perinatal and maternal outcome following abruptio placentae. Hypertens Pregnancy. 2001;20:195–203.
Kayani SI, Walkinshaw SA, Preston C. Pregnancy outcome in severe placental abruption. BJOG. 2003;110:679–83.
Oyalese KO, Turner M, Lees C, Campbell S. Vasa previa: an avoidable obstetric tragedy. Obstet Gynecol Surv. 1999;54:138–45.
Lubin B. Neonatal anaemia secondary to blood loss. Clin Haematol. 1978;7:19–34.
Society of Maternal-Fetal (SMFM) Publications Committee, Sinkey RG, Odibo AO, Dashe JS. #37: Diagnosis and management of vasa previa. Am J Obstet Gynecol. 2015;213(5):615.
Hasegawa J, Nakamura M, Sekizawa A, Matsuoka R, Ichizuka K, Okai T. Prediction of risk for vasa previa at 9-13 weeks’ gestation. J Obstet Gynaecol Res. 2011;37(10):1346–51.
Kruitwagen RF, Nijhuis JG. Ruptured vasa praevia complicated by a sinusoidal fetal heart rate pattern: a case report. Eur J Obstet Gynecol Reprod Biol. 1991;39:147–50.
Odunsi K, Bullough CH, Henzel J, Polanska A. Evaluation of chemical tests for fetal bleeding from vasa previa. Int J Gynaecol Obstet. 1996;55(3):207.
Gibbins KJ, Weber T, Holmgren CM, Porter TF, Varner MW, Manuck TA. Maternal and fetal morbidity associated with uterine rupture of the unscarred uterus. Am J Obstet Gynecol. 2015;213(3):382.
Zwart JJ, Richters JM, Ory F, de Vries JI, Bloemenkamp KW, van Roosmalen J. Uterine rupture in The Netherlands: a nationwide population-based cohort study. BJOG. 2009;116(8):1069.
Al-Zirqi I, Daltveit AK, Forsen L, et al. Risk factors for complete uterine rupture. Am J Obstet Gynecol. 2017;216(2):165e1–165e8
Rageth JC, Juzi C, Grossenbacher H. Delivery after previous cesarean: a risk evaluation. Swiss Working Group of Obstetric and Gynecologic Institutions. Obstet Gynecol. 1999;93(3):332–7.
Rudd NL, Nimrod C, Holbrook KA, Byers PH. Pregnancy complications in type IV Ehlers-Danlos Syndrome. Lancet. 1983;1(8314–5):50.
National Institutes of Health Consensus Development Conference Panel. National Institutes of Health Consensus Development conference statement: vaginal birth after cesarean: new insights March 8–10, 2010. Obstet Gynecol. 2010;115(6):127.
Ozdemir I, Yucel N, Yucel O. Rupture of the pregnant uterus: a 9-year review. Arch Gynecol Obstet. 2005;272(3):229.
Bujold E, Gauthier RJ. Neonatal morbidity associated with uterine rupture: what are the risk factors? Am J Obstet Gynecol. 2002;186(2):311–4.
Bujold E, Mehta SH, Bujold C, Gauthier RJ. Interdelivery interval and uterine rupture. Am J Obstet Gynecol. 2002;187(5):1199–202.
Leung AS, Leung EK, Paul RH. Uterine rupture after previous cesarean delivery: maternal and fetal consequences. Am J Obstet Gynecol. 1993;169(4):945–50.
Rodriguez MH, Masaki DI, Phelan JP, Diaz FG. Uterine rupture: are intrauterine pressure catheters useful in the diagnosis? Am J Obstet Gynecol. 1989;161(3):666–9.
Johnson C, Oriol N. The role of epidural anesthesia in trial of labor. Reg Anesth. 1990;15(6):304–8.
Blanchette H, Blanchette M, McCabe J, Vincent S. Is vaginal birth after cesarean safe? Experience at a community hospital. Am J Obstet Gynecol. 2001;184(7):1478–87.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2017 Springer International Publishing AG
About this chapter
Cite this chapter
Dynin, M., Lane, D.R. (2017). Bleeding in Late Pregnancy. In: Borhart, J. (eds) Emergency Department Management of Obstetric Complications. Springer, Cham. https://doi.org/10.1007/978-3-319-54410-6_5
Download citation
DOI: https://doi.org/10.1007/978-3-319-54410-6_5
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-319-54409-0
Online ISBN: 978-3-319-54410-6
eBook Packages: MedicineMedicine (R0)